aravind eye care system - the king's fund · pdf filelow cost wi-fi 802.11b connectivity...
TRANSCRIPT

Aravind
‘Enhancing Access & Affordability’
Aravind Eye Care System
Dr.R.D.Ravindran Chairman
Aravind Eye Hospitals India

Aravind
Blindness Magnitude
• 45 million blind, worldwide
• 12 million blind in India
• 300,000 of them children
Aravind
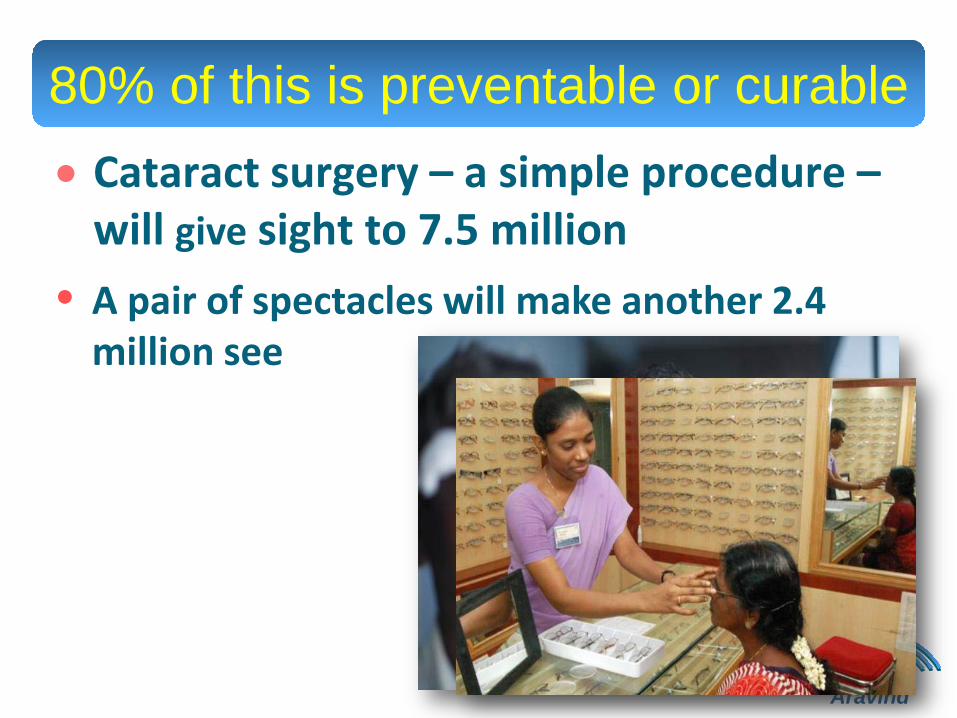
80% of this is preventable or curable • Cataract surgery – a simple procedure –
will give sight to 7.5 million
• A pair of spectacles will make another 2.4 million see

Aravind
Challenges - underserved
population • Managing fluctuating
incomes/low affordability • Difficult living conditions • Unfamiliar with many
products, technologies & procedures
• Seek trusted advice • Demand respect • Face disadvantages in
market
Dr.Venkatasamy, feeling the urgent need, started an eye clinic in 1976 on his retirement with 11 beds, to create
an alternate, sustainable eye care system to supplement the
government’s efforts.
In a developing country with competing demands on limited resources, government alone cannot meet the health needs of all.
Our challenges
• Creating access
• Making it affordable
• Ensuring quality
• Resource scarcity (Capital and HR)
Universal concerns ?? - variable levels
India: Population 1.1 billion
200 million need eye care
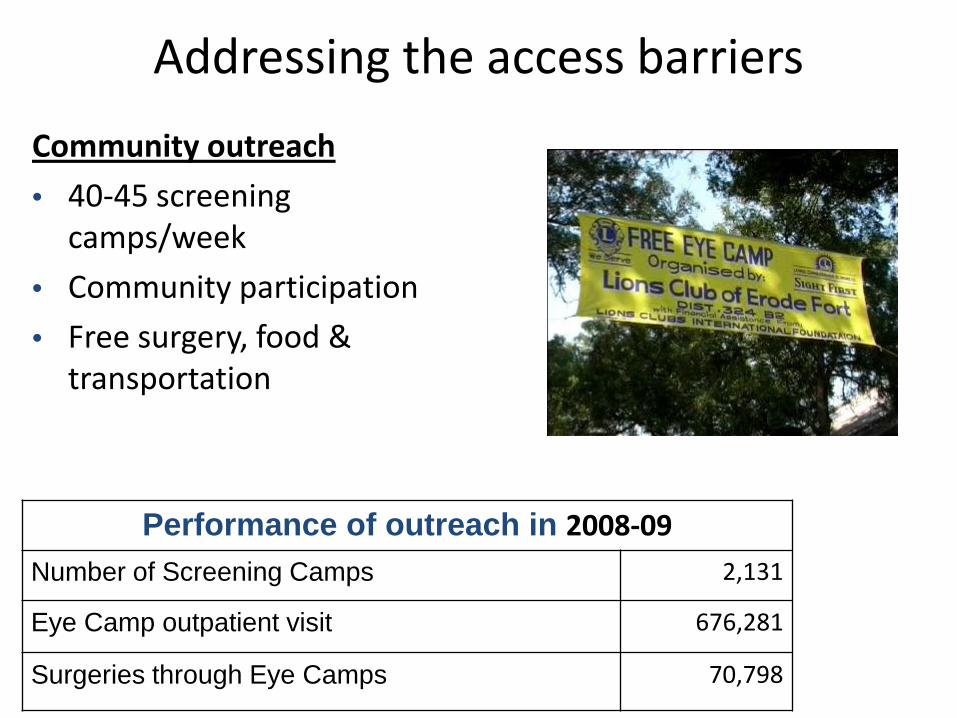
Addressing the access barriers
Community outreach
• 40-45 screening camps/week
• Community participation
• Free surgery, food & transportation
Performance of outreach in 2008-09 Number of Screening Camps 2,131
Eye Camp outpatient visit 676,281
Surgeries through Eye Camps 70,798
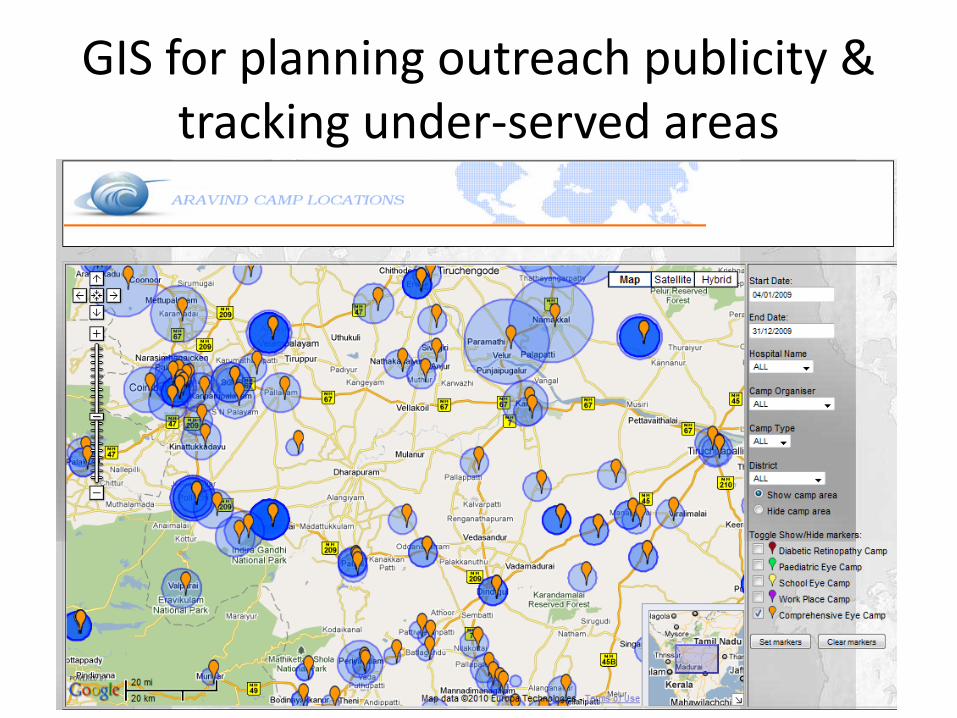
GIS for planning outreach publicity & tracking under-served areas
Camp location : Devadanapatti, Theni District
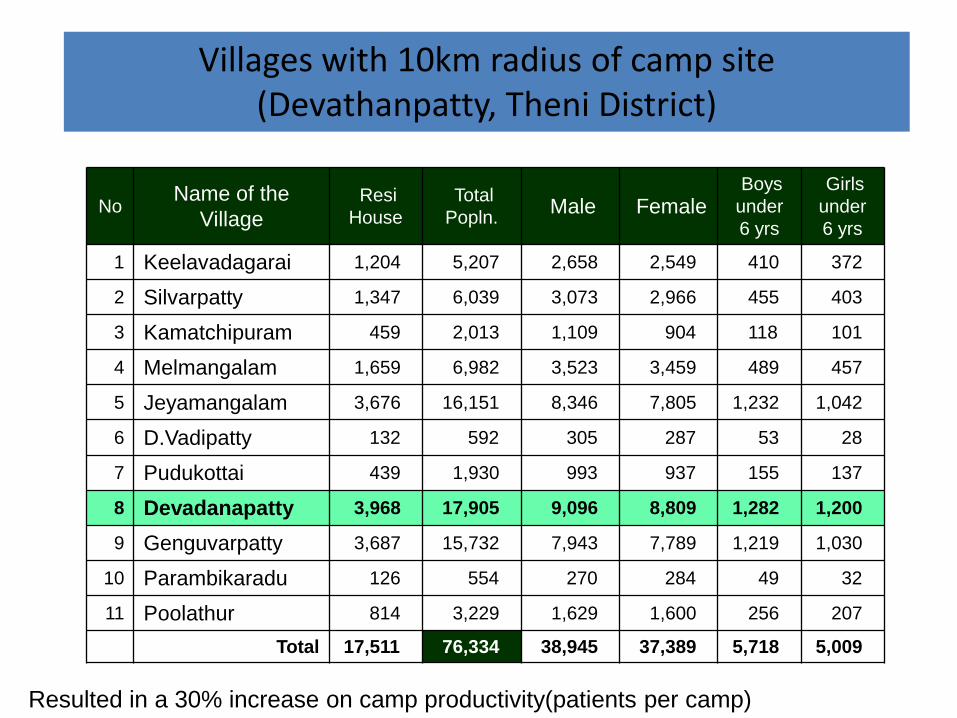
No Name of the Village
Resi House
Total Popln. Male Female
Boys under 6 yrs
Girls under 6 yrs
1 Keelavadagarai 1,204 5,207 2,658 2,549 410 372
2 Silvarpatty 1,347 6,039 3,073 2,966 455 403
3 Kamatchipuram 459 2,013 1,109 904 118 101
4 Melmangalam 1,659 6,982 3,523 3,459 489 457
5 Jeyamangalam 3,676 16,151 8,346 7,805 1,232 1,042
6 D.Vadipatty 132 592 305 287 53 28
7 Pudukottai 439 1,930 993 937 155 137
8 Devadanapatty 3,968 17,905 9,096 8,809 1,282 1,200
9 Genguvarpatty 3,687 15,732 7,943 7,789 1,219 1,030
10 Parambikaradu 126 554 270 284 49 32
11 Poolathur 814 3,229 1,629 1,600 256 207
Total 17,511 76,334 38,945 37,389 5,718 5,009
Villages with 10km radius of camp site (Devathanpatty, Theni District)
Resulted in a 30% increase on camp productivity(patients per camp)
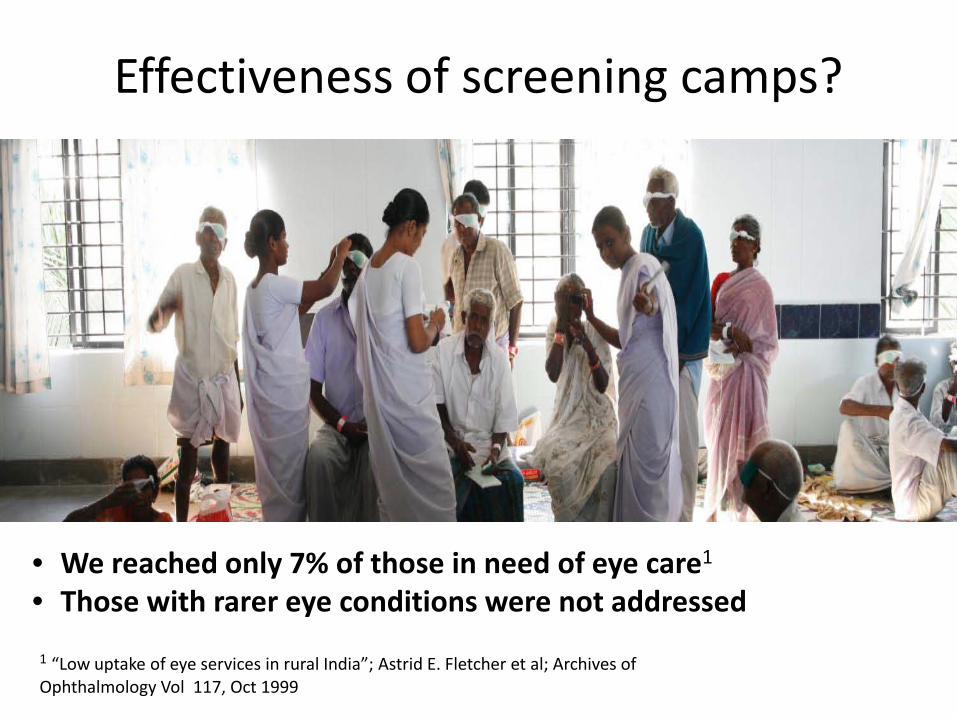
Effectiveness of screening camps?
• We reached only 7% of those in need of eye care1
• Those with rarer eye conditions were not addressed
1 “Low uptake of eye services in rural India”; Astrid E. Fletcher et al; Archives of Ophthalmology Vol 117, Oct 1999
Enhancing access Vision Centers
• Permanent facility in rural areas
• Covering small population - 50,000
• Staffed by technicians (tough to get doctors to work in villages)
Challenge:
• Comprehensive eye exam
• Ensuring quality – right diagnosis & prescription
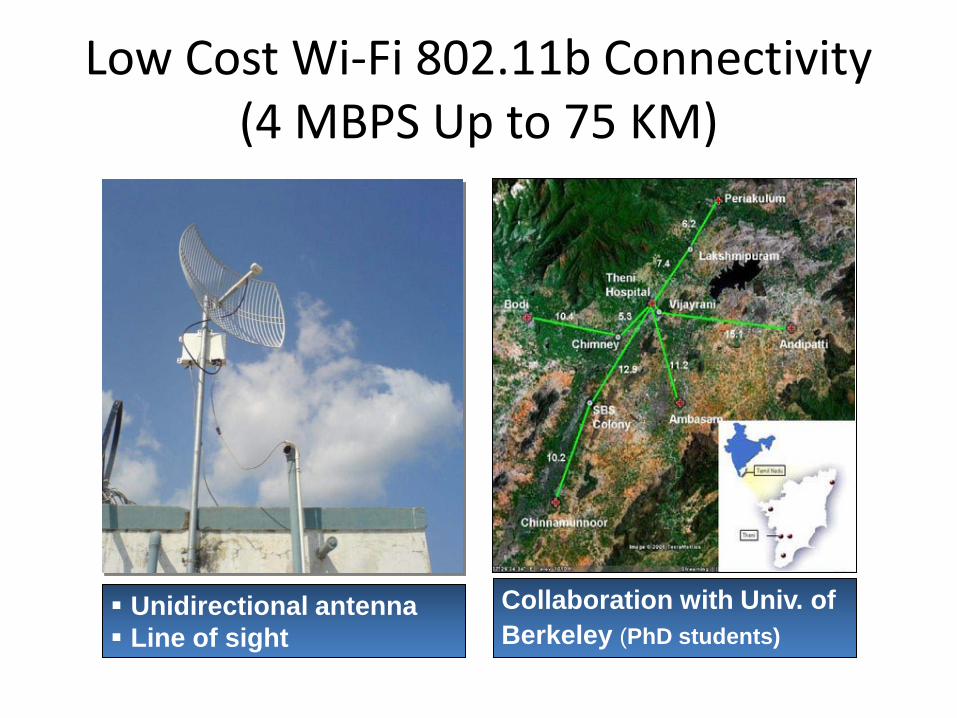
Low Cost Wi-Fi 802.11b Connectivity (4 MBPS Up to 75 KM)
Unidirectional antenna Line of sight
Collaboration with Univ. of Berkeley (PhD students)

Investment: • Digital Camera + Adapter
• US$ 250
Vs. • Digital Fundus Camera:
• US$ 25,000
Innovation: Low-cost imaging
technology
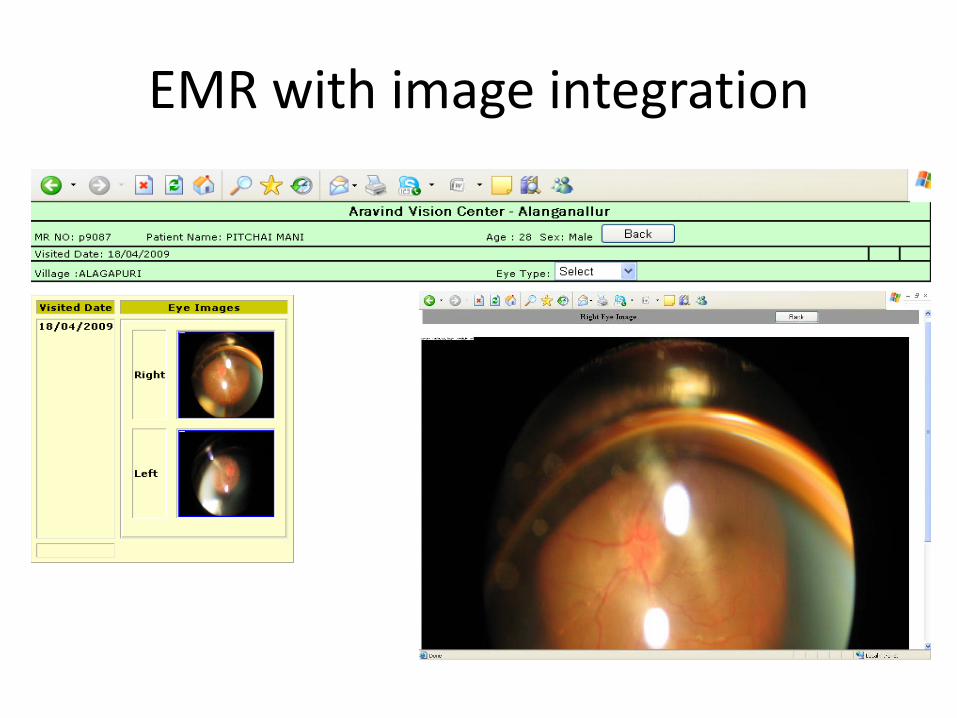
EMR with image integration
Vision Centers – how they work
Performance – 39 Centers
• Every day we video-consult with 700 patients
• 70 to 80 are given corrective glasses • 35 to 40 patients are advised to
have surgery • 35 to 40 diabetics are counselled
regarding DR
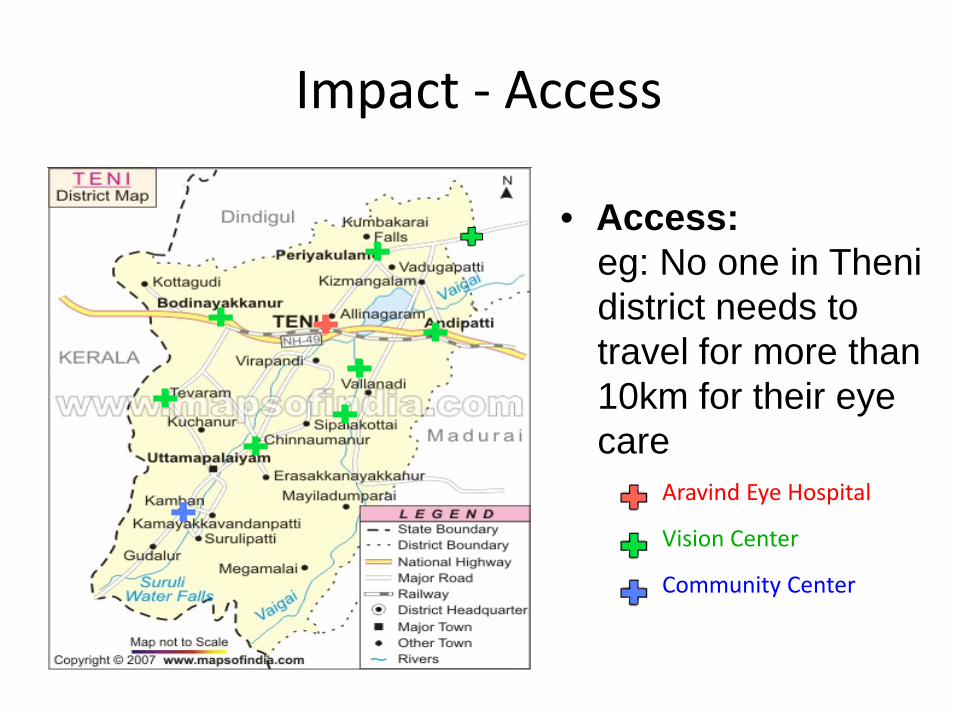
Impact - Access
Aravind Eye Hospital
Vision Center
Community Center
• Access: eg: No one in Theni district needs to travel for more than 10km for their eye care
• Goes to remote places
• Known diabetic pts. Fundus images are taken
• Recorded in a specialized software and transmitted to the Reading Grading Center at the Base Hospital
Solution 2: Taking advanced care to villages
Achieving Universal Access
Key strategies:
• Designing services for the non-customer
• Community involvement
• Monitoring
Impact – reaching the unreached
• Creating access
• Increased awareness
• Influencing health-seeking behaviour
• Community participation
• Growing the market (reaching the unreached)
ARAVIND EYE CARE SYSTEM
Making it affordable
•When most can’t pay
•For the provider with limited resources
Defining costs • Provider perspective - price of service/product
• Customer/community perspective
– Time investment and lost wages – Cost of access – Similar costs incurred by accompanying person – Price of service/product as above – Cost of repeat visits
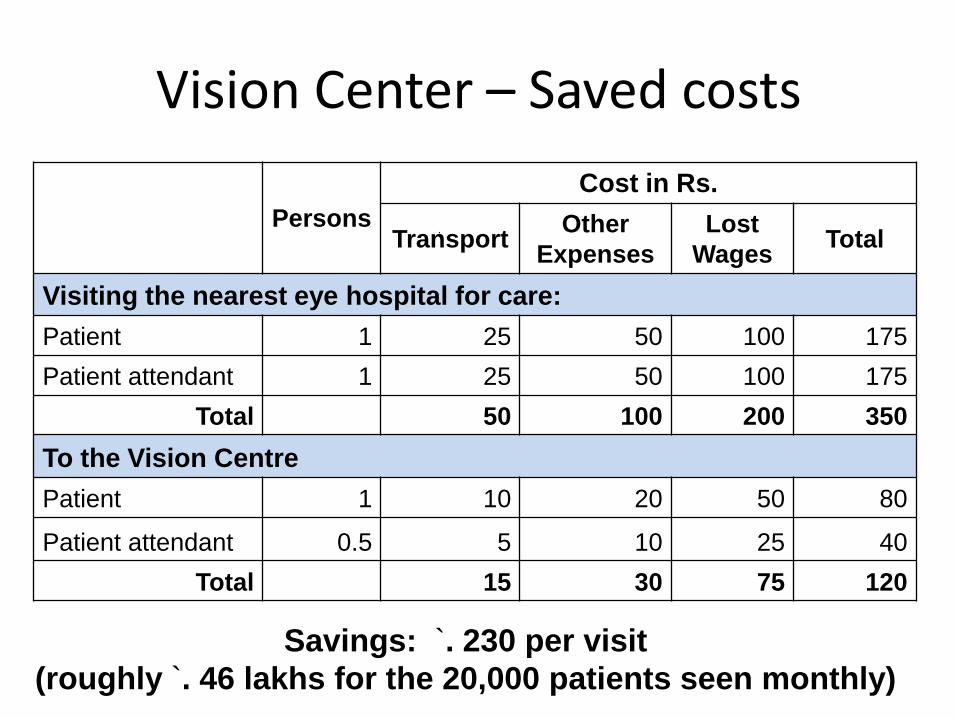
Vision Center – Saved costs
Persons Cost in Rs.
Transport Other Expenses
Lost Wages Total
Visiting the nearest eye hospital for care: Patient 1 25 50 100 175 Patient attendant 1 25 50 100 175
Total 50 100 200 350
To the Vision Centre Patient 1 10 20 50 80
Patient attendant 0.5 5 10 25 40 Total 15 30 75 120
Savings: `. 230 per visit (roughly `. 46 lakhs for the 20,000 patients seen monthly)
Processes to minimize ‘patients’ costs
• Completing all investigations on a single visit
• Eliminating unnecessary tests
• No waiting list
• Minimizing length of stay
Costs of access, lost wages, and incidental expenses can be significant
Costs associated – Patient
• Cost of spectacles - Rs. 175 – Rs. 250
• Cost of getting glasses – Rs.150 to 250 Involves 2 to 4 trips for:
• examination
• ordering the glasses
• getting the glasses
• ensuring that the glasses are right.
• The above costs can be reduced to 0 with the strategy of free examination and on the spot delivery
Provider: Cost-efficiency
• Managing bottlenecks
• Eliminating waste – idling of resources
– inappropriate use of resources
• Ensuring high quality – doing it right every time
– building patient trust and compliance
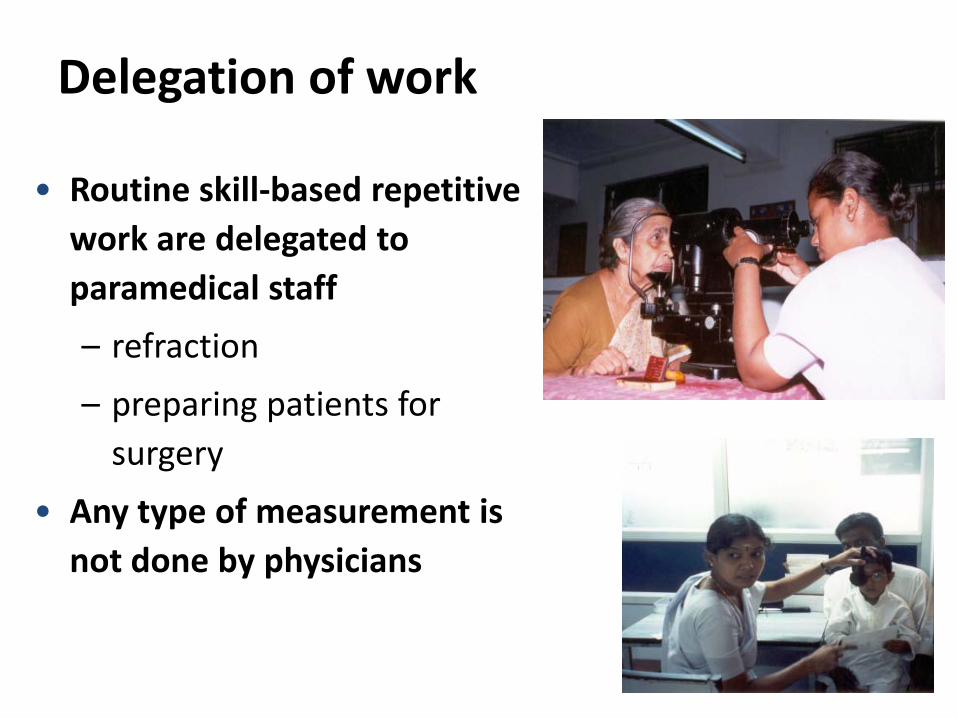
Delegation of work
• Routine skill-based repetitive work are delegated to paramedical staff
– refraction
– preparing patients for surgery
• Any type of measurement is not done by physicians
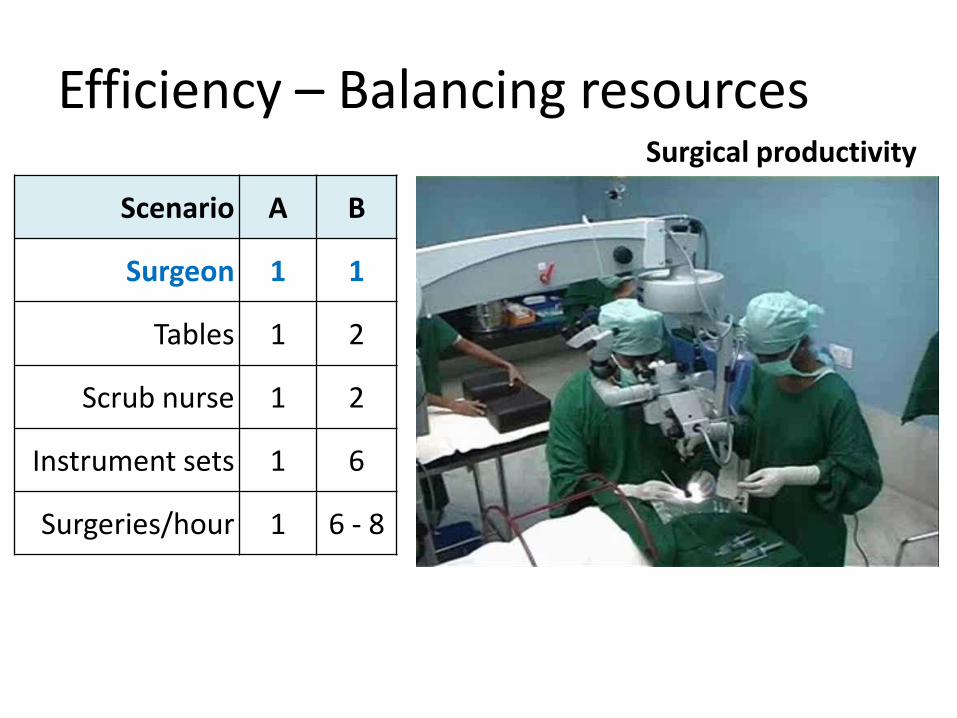
Efficiency – Balancing resources
Scenario A B
Surgeon 1 1
Tables 1 2
Scrub nurse 1 2
Instrument sets 1 6
Surgeries/hour 1 6 - 8
Surgical productivity
Aravind (Wo)manpower
• 400+ village high school girls given job specific training each year
• Perform most of the routine clinical tasks
• Results in higher quality, productivity and lowers cost
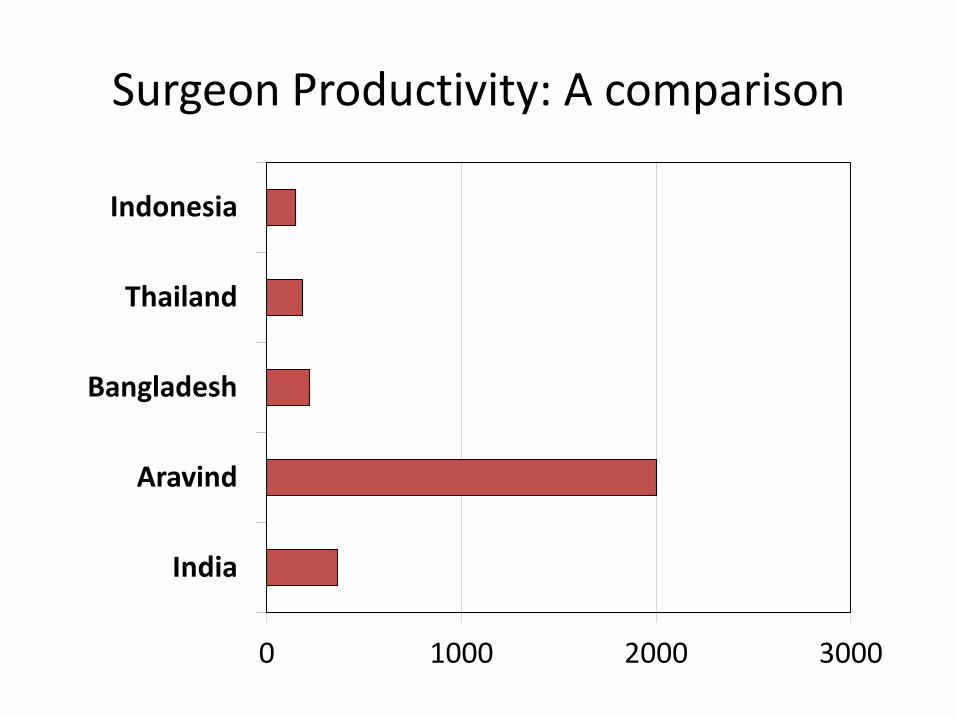
Surgeon Productivity: A comparison
0 1000 2000 3000
India
Aravind
Bangladesh
Thailand
Indonesia
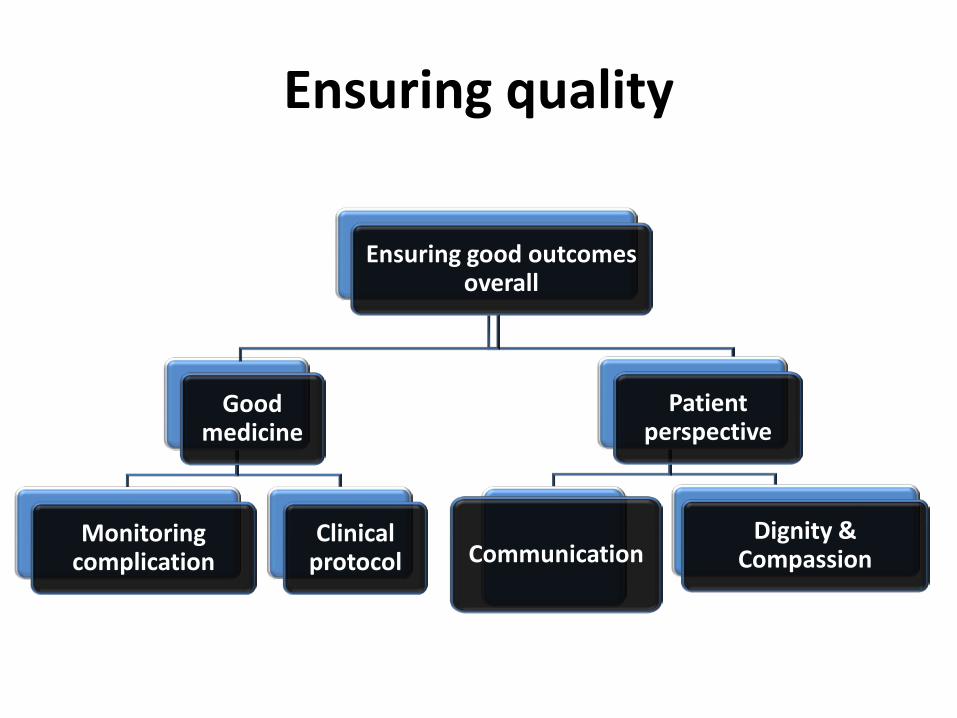
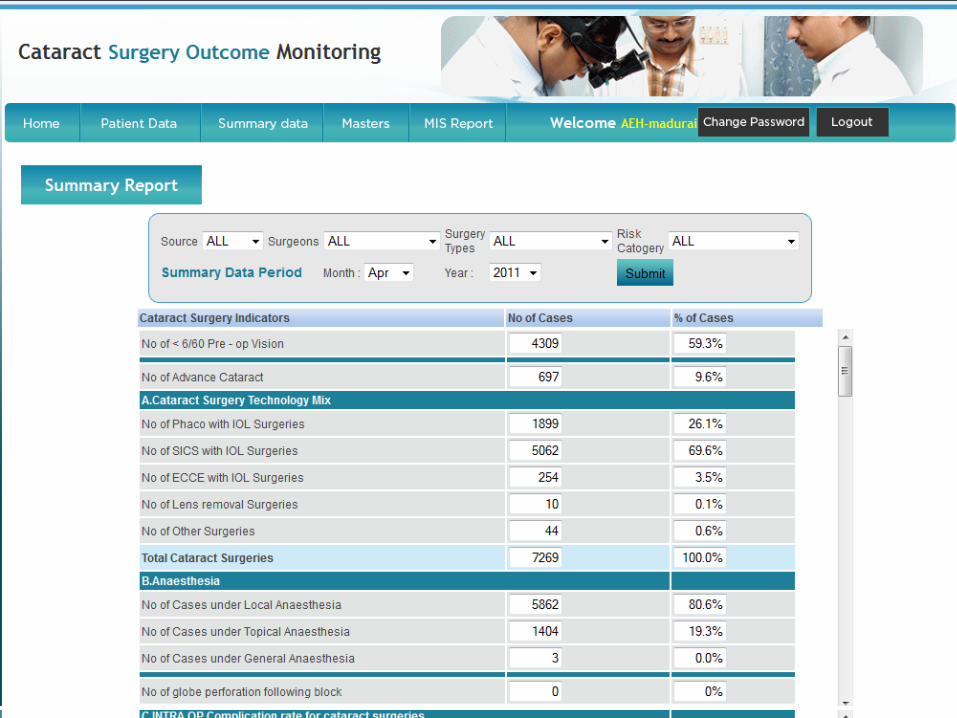
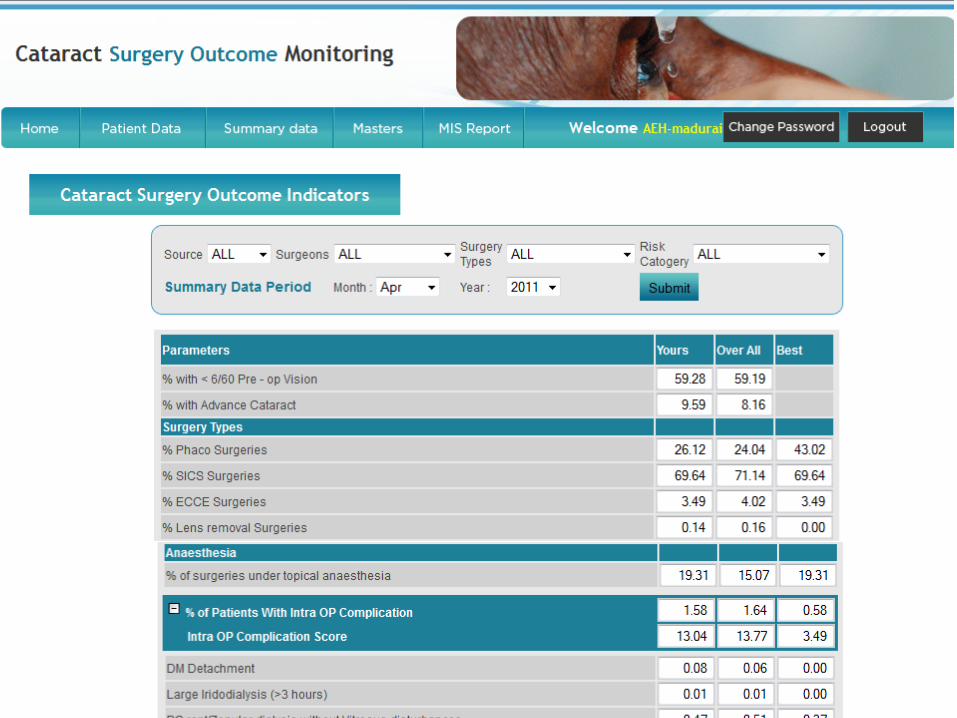
Ensuring quality
Ensuring good outcomes overall
Good medicine
Monitoring complication
Clinical protocol
Patient perspective
Communication Dignity &
Compassion
Clinical protocols
Guidelines for clinical areas: • Guidelines for advising surgery • Post op. follow up guidelines • Treatment/Follow up guidelines for
common disorders (Glaucoma)
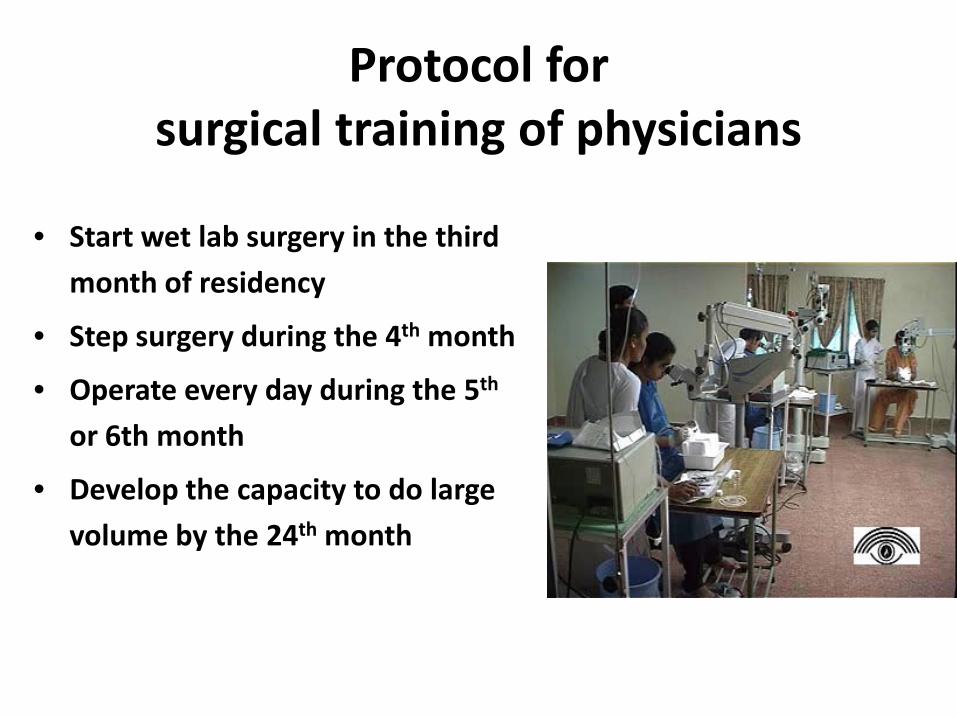
Protocol for surgical training of physicians
• Start wet lab surgery in the third
month of residency
• Step surgery during the 4th month
• Operate every day during the 5th
or 6th month
• Develop the capacity to do large
volume by the 24th month
FOCUS ON
THE
Patient
Patient is an equal partner in the treatment process
Patient counselling • Clinical procedure/
pamphlet • Length of stay and
cost • Post op.
instructions • SMS reminders
Ensuring compliance

Summary
• Addressing these issues: – of access
– ensuring quality, resulting in high productivity
Helped us to bring down the cost and make the eye care affordable in our setting.
Tamil Nadu
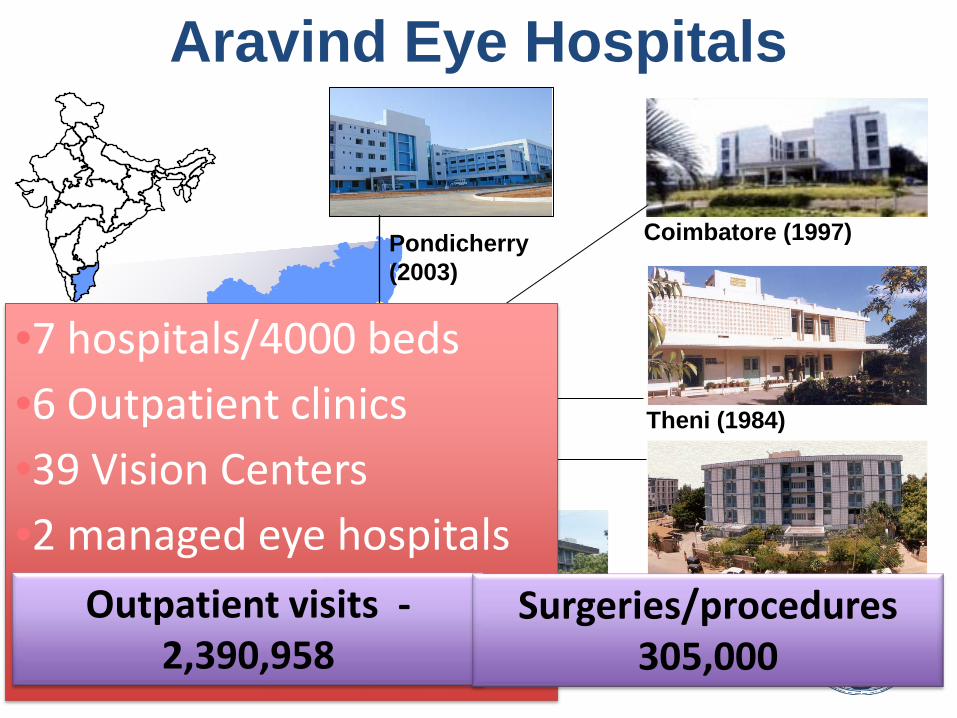
Pondicherry (2003)
Coimbatore (1997)
Theni (1984)
Madurai (1978)
Tirunelveli (1988)
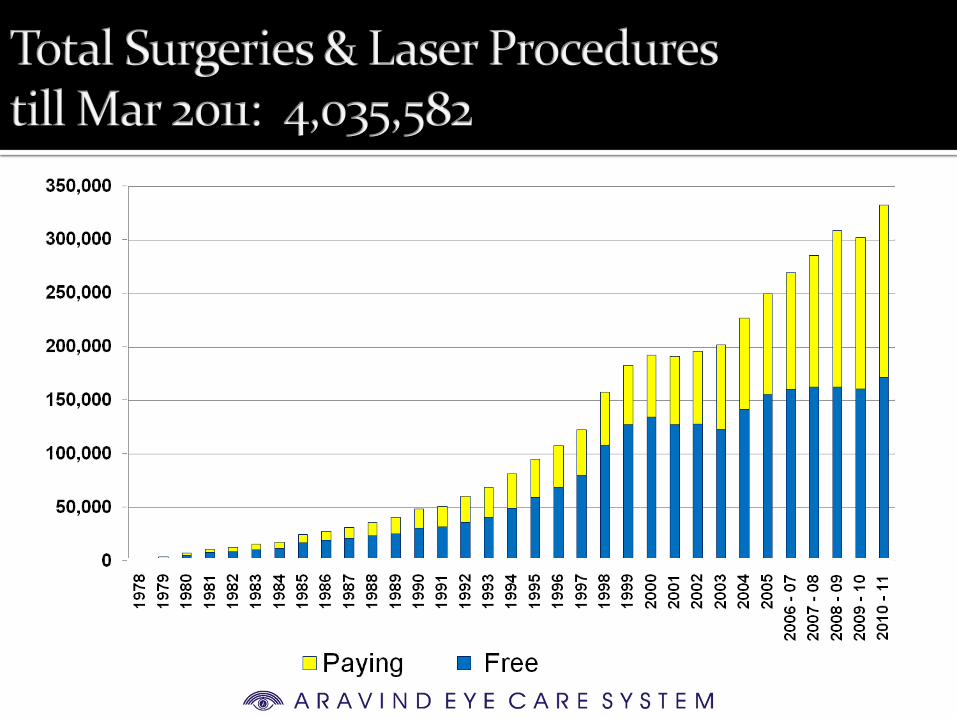
Aravind Eye Hospitals
•7 hospitals/4000 beds •6 Outpatient clinics •39 Vision Centers •2 managed eye hospitals
• Outpatient visits -
2,390,958 Surgeries/procedures
305,000
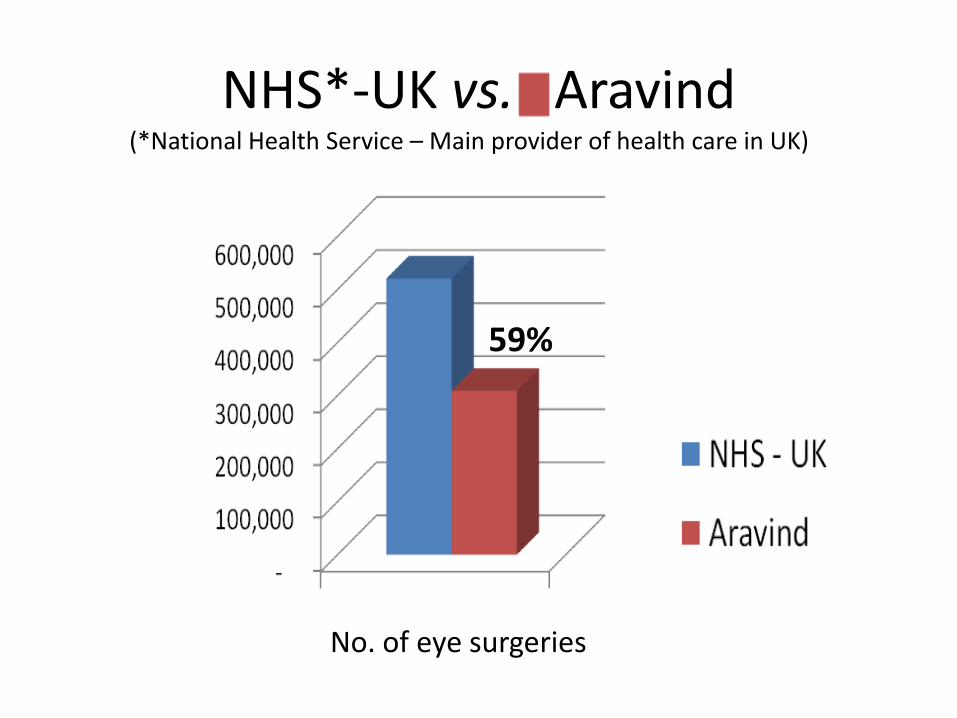
NHS*-UK vs. Aravind
No. of eye surgeries
59%
(*National Health Service – Main provider of health care in UK)
0
5
10
15
20
25
30
80-8
181
-82
82-8
383
-84
84-8
585
-86
86-8
787
-88
88-8
989
-90
90-9
191
-92
92-9
393
-94
94-9
595
-96
96-9
7
97-9
898
-99
99-0
000
-01
01-0
202
-03
03-0
404
-05
'05-
06'0
6-07
07-0
808
-09
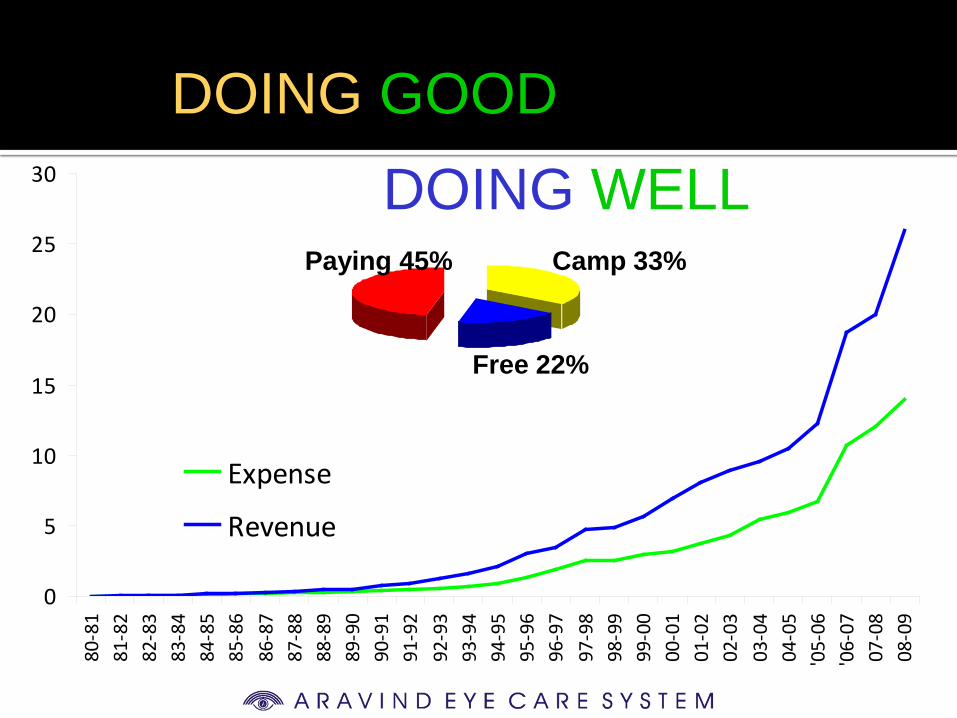
Expense
Revenue
DOING GOOD DOING WELL
Camp 33% Paying 45%
Free 22%
Social entrepreneurism
Vision Developing the right
perspectives Innovation Mindset Leadership
“When you grow in spiritual consciousness, we identify with all that is in the world, so there is no exploitation, it is ourselves we are helping, it is ourselves we are healing” - Dr. G. Venkataswamy