are we behind? - obstetrics and gynecology are we behind? when i slowly realized that nipt is...
TRANSCRIPT
6/7/2017
1
Early anomaly scansEarly anomaly scans
Ilan Timor‐TritschIlan Timor‐Tritsch
Why are we behind?
When I slowly realized that NIPT is reality:
• I started to have sleepless nights
• I feared that my an almost career long “investment” in first and early second trimester anatomy scan will go down the drain
• But then I learned more about the presumed “threat” and drew some comfort of the virtues an advantages of TVS
• I am convinced that TVS is here to stay and will undoubtedly find its well earned place in 1st trimester diagnosis alongside the NIPT
Background
• In the last decade, prenatal screening and testing have shifted from the 2nd to the 1st trimester.
• US evaluation of the fetus—a large component of fetal testing—is also applied earlier in gestation to provide information to clinicians and patients about the integrity of the pregnancy.

6/7/2017
2
Background
• The shifting of the classic, 2nd ∆ “gold standard” anatomy scan to the 1st ∆ was made possible by the introduction of high‐frequency, high resolution transvaginal transducers and by greater understanding of the early signs of fetal pathology.
• (It is effective transabdominally too!!)
TVS
TVS
TASTAS
Scanning at 13‐16 wks
• Hi frequency transducer• High resolution• Entire fetus fits into FR
• Adequate early scan• Requires a second scan
Focal range (FR)
• Lower frequency transducer• Lower resolution• Potentially less adequate early scan
• May complement TVS scan• Requires second scan
TVS
TVS
TASTAS TASTAS
2nd scan @ 20 – 23 w 1stscan @ 11‐14 (16) w
Advantages:• High resolution images• Can combine with NT scan• Potentially detects up to 80% of detectable/early anomalies• Early assessment of MFP
Alone or in combination Advantages:• Organs adequate for resolution• Potentially detects up to 95% of detectable anomalies• Better for brain, skeletal, heart, diaphragmatic etc.• Assess cervix

6/7/2017
3
Background
• We may witness another extremely possible change in the 1st ∆ prenatal diagnostic paradigm due to the introduction of the Noninvasive Prenatal Testing (NIPT) that may, over time, decrease the number of patients referred for NT screening.
• This may result in missing the opportunity to actually look at the early fetus
Background
• NOW is therefore the best time to reevaluate the value of 1st ∆ anatomy scan and, if found useful, encourage offering it to pregnant patients.
• Performing the early fetal anatomy scan would complement the new NIPT, since they are not mutually exclusive in detecting pathology.
What are the added values of TVS in the first trimester?

6/7/2017
4
Added value of the 1st ∆ US exam?
• First‐trimester ultrasound (FTUS) achieves several important goals: IT CAN
• …detect many pregnancy complications, such as placental abnormalities
• …highlight some chromosomal anomalies
• ….include a detailed fetal anatomy scan, if desired.
But wait…….. there is more!!!
An important application: emergency imaging
• 1st ∆ US can help determine the source of any 1st ∆ vaginal bleeding—specifically, it can differentiate between threatened abortion, early fetal demise, andectopic pregnancy.

6/7/2017
5
Fetal viability can be established
• High‐frequency transvaginalprobes allow earlier and more accurate diagnosis of embryonic and fetal viability, even in the 1st ∆ through the assessment of cardiac activity.
Precise dating can be established• In addition, early pregnancies can be dated accurately by sequential sonographic visualization of the gestational sac, yolk sac, embryonic pole, cardiac activity, and amniotic sac.
• Measurement of the fetal crown‐rump length (CRL) also provides landmark information that aids in dating the pregnancy and managing different aspects of the gestation.
•If the patient is obese this may be her ONLY“shot” at a good structural evaluation
Positive fact about the early anomaly scan
WEIGHT
OVERW
The obese patientThe obese patient
The obese patient
verweight patverweight pat
obeseobeseThe obese patientThe obese patient
The obese patient
The obese patientThe obese patient
The obese
THE OBESE PATIENTThe obese patientThe obese patient
patient
THE OVERWEGHT
PATIENT
THE OVERWEGHT
PATIENT
The overweight patientThe overweight patient
The overweight patient
The overweight patientThe overweight patientThe overweight patientThe overweight patient
The overweight patientThe overweight patient
The overweight patientThe overweight patient
The obese patientThe obese patient
OVERWEIGHTOVERWEIGHT
OVERWEIGHT
OVERWEIGHT OVERWEIGHTOVERWEIGHT
O V E R W E I G H TO V E R W E I G H T
OVERWEIGHT
OVERWEIGHT
OVERWEIGHT
OVERWEIGHTOVERWEIGHTWeight
WeightWeight
Weight
WEIGHT
Weight
Weight
Remember: 30‐40% women in the USA are obese

6/7/2017
6
• The addition of a 14‐16 week transabdominalanatomy scan significantly increased the rate of complete anatomy scans from 42% to 51% (P < .01). It also significantly improved visualization of the head, thorax, and abdomen and significantly increased the mean number of items seen (P < .05).
J Ultrasound Med 2014; 33:1579–1583
Important feature: Definition of MFP
• The 1st ∆ is also the best time to identify, date, and evaluate multifetalgestation in regard to chorionicity and amniocity. These variables, which are important in determining optimal management and potential outcomes, are more difficult to determine later in pregnancy.
Advanced applications include an assessment of fetal anatomy
• At the time of NT assessment, 1st∆ US can be broadened to evaluate the age‐related anatomy of fetal organs and organ systems.
• At 12 weeks, approximately 40% to 50% of common, US discernible anomalies are already present.
•Timor‐TritschI,FuchsK,MonteagudoA,D’altonME.Performingafetalanatomyscanatthetimeoffirst‐trimesterscreening.ObstetGyncol.2009;113(2Pt1):402–407.

6/7/2017
7
Don’t forget the cervix and the adnexae
• It is important to evaluate the cervix in the 1st∆ , keeping the risk of preterm delivery in mind, as well as the maternal uterus and adnexae(looking for pathology) and the placenta (looking for abnormalities).
Best time for aneuploidy screening
• 1st ∆ US and biochemical testing can be used for aneuploidy screening between 11 and 13‐6/7 weeks.
• Sonographic measurement of the nuchal translucency (NT)—is used to determine the likelihood that the fetus is aneuploid Trisomy 21.
Best time for aneuploidy screening
• NT measurement alone has sensitivity of 64% to 70% for the detection of Trisomy 21, as well as a false‐positive rate of 5%.
• When NT assessment is combined with the measurement of maternal serum pregnancy‐associated plasma protein A and free serum hCG, sensitivity increases to 82% to 87%.
• When maternal age is factored into the equation, sensitivity may exceed 90%.

6/7/2017
8
• Assessment of the:
• nasal bones ,
• ductus venous flow,
• tricuspid regurgitation,
• and hepatic artery flow
in combination with NT measurement can also improve sensitivity in the detection of Trisomy 21
•NicolaidesKH.Screeningforfetalaneuploidiesat11to13weeks.PrenatDiagn.2011;31(1):7–15.
•Nicolaides KH.Screeningforfetalaneuploidies at11to13weeks.Prenat Diagn.2011;31(1):7–15.
Best time for aneuploidy screening
Best time for aneuploidy screening
• NT measurement alone has sensitivity of 64% to 70% for the detection of Trisomy 21, as well as a false‐positive rate of 5%.
• When NT assessment is combined with the measurement of maternal serum pregnancy‐associated plasma protein A and free serum hCG, sensitivity increases to 82% to 87%.
• When maternal age is factored into the equation, sensitivity may exceed 90%.
Lately, there is a new threat to the Ob/Gyncommunity:
Cesarean Scar PregnancyIt can be detected early in the 1st ∆!!! Look where the placenta is inserted!!!:
Lately, there is a new threat to the Ob/Gyncommunity:
Cesarean Scar PregnancyIt can be detected early in the 1st ∆!!! Look where the placenta is inserted!!!:
• Timor‐Tritsch I, Monteagudo A. Unforeseen consequences of the increasing rate of cesarean deliveries: early placenta accreta and cesarean scar pregnancy. A review. Am J Obstet Gynecol. 2012;207(1):14–29.
• Timor‐Tritsch I, Monteagudo A, Santos R, Tsymbal T, Pineda G, Arslan AA. The diagnosis, treatment, and follow‐up of cesarean scar pregnancy. Am J ObstetGynecol. 2012;207(1):44.e1–e13.
• Stirnemann J, Chalouhi G, Forner S, et al. First‐trimester uterine scar assessment by transvaginal ultrasound. Am J Obstet Gyncol. 2011;205(6):551.e1–e6.
• Stirnemann J, Mousty E, Chalouhi G, Salomon LJ, Berard JP, Ville Y. Screening for placenta accreta at 11‐14 weeks of gestation. Am J Obstet Gynecol. 2011;205(6):547.e1–e6.

6/7/2017
9
• Cell free DNA testing can be offered to patients but should not be part of routine prenatal laboratory assessment.
• It should be an informed choice after pretest counseling
• Should not be offered to low risk patients or multiple gestations
ACOG Committee Opinion #545 Noninvasive Prenatal Testing for Fetal
Aneuploidy
ACOG Committee Opinion #545 Noninvasive Prenatal Testing for
Fetal Aneuploidy
• In a rather short time NIPT will enter the “routine use” status as this happened with:
–Doppler evaluations
–TVS
–NT
–3D US
ACOG Committee Opinion #545 Noninvasive Prenatal Testing for
Fetal Aneuploidy
• When NIPT will be routine or almost routine, we may have a smaller number of patients to perform anatomy evaluations on
• This will lead to some, obvious, early detectable structural anomalies undetectable by NIPT to be missed

6/7/2017
10
The American Institute of Ultrasound in Medicine (AIUM) recommendation
• “Embryonic/fetal anatomy appropriate for the 1st r should be assessed” during the 1st ∆”
• Although AIUM provides no details about the list of structures to be evaluated, it does provide a guideline for the 2nd ∆ anatomy scan that can be adapted easily for use in the first trimester.
•AmericanInstituteofUltrasoundinMedicine.AIUMPracticeGuidelineforthePerformanceofObstetricUltrasoundExaminations.http://www.aium.org/resources/guidelines/obstetric.pdf.EffectiveOctober1,2007..
The International Society of Ultrasound in Obstetrics and Gynecology (ISUOG)
Published guidelines for 1st∆ US—including its use as an anatomy scan. The ability to assess anatomical structures in the depends on the quality of the equipment as well as the training of the sonographer or sonologist.
UOG 2013;41:102‐113
Second‐trimester follow‐up is recommended
• Because some congenital anomalies cannot be identified in the 1st∆ (or may progress into the 2nd∆), a follow‐up US in the 2nd∆ should always be recommended.
• AIUM guidelines for a 2nd ∆ anatomy work‐up mandate the visualization and documentation of a number of structures and organs

6/7/2017
11
What to look for during 1st ∆ imaging
Before we describe which anatomical structures and fetal anomalies can be assessed during the first trimester, we’d like to recommend 2 articles providing a comprehensive list of anomalies that have been identified in the 1s∆t by Fong et al & by Syngelaki et al.
•SyngelakiA,ChelemenT,DagklisT,AllanL,NicolaidesKH.Challengesinthediagnosisoffetalnon‐chromosomalabnormalitiesat11‐13weeks.Prenat Diagn.2011;31(1):90–102..•FongKW,Toi A,SalemS,etal.DetectionoffetalstructuralabnormalitieswithUSduringearlypregnancy.Radiographics.2004;24(1):157–174.
Anomaly Detection in theFirst Trimester
• When is it a realistic time to perform the anatomy scan?
• What structures should be included in the scan?
• Which anomalies can be detected in the 1st trimester?
• It really means anomaly detection between 11 to 136/7 weeks
• It really means anomaly detection between 11 to 136/7 weeks
Anomaly Detection in theFirst Trimester
• However, many times anomalies can be diagnosed even before 11 weeks
• However, many times anomalies can be diagnosed even before 11 weeks

6/7/2017
12
Majority of > 20 published studies = 2 staged protocols with an 11‐14 wk scan followed by an 18‐22 wk scan
First‐trimester detection rates range 16‐84%
Majority reported detection rates > 50%
After the 2nd trimester ultrasound, two‐stage protocols reported detection rates of 48‐95%
Highest detection rates were achieved in studies screening high‐risk women
113:402.
1∆ Anatomic Survey: Detection Rates
Timor‐Tritsch, Obstet Gynecol 2009Timor‐Tritsch IE1, Fuchs KM, Monteagudo A, D'alton MEPerforming a fetal anatomy scan at the time of first‐trimester screening. ObstetGynecol. 2009 Feb;113(2 Pt 1):402‐7
g yMost fetal organs are formed and
can be imaged by 14 weeks
Weeks NAnt & Post contours
Long bones Fingers
Face Palate
Foot Toes
4 Chamber view
9 17 +F&H ±T&R ‐ ± ‐ ‐ ‐
10 16 +F&H ±T&R ‐ ± ± ‐ ‐
11 17 + + ± ± ± ‐
12 15 + + + + ± ±
13 14 + + + + + ±
14 18 + + + + + +
± : Threshold level (first seen) +: Discriminatory level (always seen)
Timor‐Tritsch IE, Monteagudo A, Peisner DB. High‐frequency transvaginal sonographic examination
for the potential malformation assessment of the 9‐week to 14‐week fetus. JCU 1992;20:231‐8.
The study supports the possibility of searching for specific malformations at or after 9‐14 weeks, or performing a more comprehensive malformation
evaluation after 13 weeks.
The optimal gestational age to examine fetal anatomy and measure nuchaltranslucency in the first trimester
Whitlow BJ, Economides DL. UOG 1998;11:258‐61.
Objective: to determine the optimal gestational age for examining fetal anatomy and nuchal translucency in the first trimester.
Study Design: Prospective cross –sectional study; N=1288
Results: Visualization of fetal anatomy improved with increasing gestational age
10 weeks = 6% 11 weeks = 75% 12 weeks = 96%13 weeks = 98% 14 weeks = 98%

6/7/2017
13
Success rates for visualization of structures (TVS & TAS) (N=1288)
Modified After: Whitlow BJ, Economides DL. The optimal gestational age to examine fetal anatomy and measure nuchal translucency in the first trimester. UO G 1998;11:258‐61.
Conclusions: the optimal gestational age to examine fetal anatomy and measure nuchal
translucency in the first trimester is 13 weeks.
Visualization of fetal organs 11‐14 wks (n=1144)
Souka AP, Pilalis A, Kavalakis Y, Kosmas Y, Antsaklis P, Antsaklis A. Assessment of fetal anatomy at the 11‐14‐week ultrasound examination. UOG 2004;24:730‐4.
Structural evaluation of the fetus at 11‐14 weeks performed by sonographers in the
USA: A feasibility study (N=223)
Timor‐Tritsch IE, Bashiri A, Monteagudo A, Arslan AA. Qualified and trained sonographers in the US can perform early fetal anatomy scans between 11 and 14 weeks. AJOG 2004;191:1247‐52.
Can USA sonographers perform a structural evaluation of the fetus at 11‐14 weeks; with comparable detection rates as those performed in Europe by physicians ???

6/7/2017
14
Visualization rates of structures by wks
Timor‐Tritsch IE, Bashiri, A., Monteagudo, A. et al,. AJ OG 2004; 191(4): 1247‐52.
Visualization rates of structures by wks
Timor‐Tritsch IE, Bashiri, A., Monteagudo, A. et al,. AJ OG 2004; 191(4): 1247‐52.
Visualization rates of structures by wks
Timor‐Tritsch IE, Bashiri, A., Monteagudo, A. et al,. AJ OG 2004; 191(4): 1247‐52.

6/7/2017
15
Visualization rates of structures by wks
Timor‐Tritsch IE, Bashiri, A., Monteagudo, A. et al,. AJ OG 2004; 191(4): 1247‐52.
Conclusion:Anatomic surveys between 11 and 14 weeks can be performed by
sonographers with good detection rates of most structures.
What to look for during 1st∆ US
• Before we describe which anatomical structures and fetal anomalies can be assessed during the 1st∆, I’d like to highlight two articles that provide a comprehensive list of anomalies that have been identified in the 1st∆ by Fong et al and by Syngelaki etal.
•SyngelakiA,ChelemenT,DagklisT,AllanL,NicolaidesKH.Challengesinthediagnosisoffetanon‐chromosomalabnormalitiesat11‐13weeks.Prenat Diagn.2011;31(1):90–102..•FongKW,Toi A,SalemS,etal.DetectionoffetalstructuralabnormalitieswithUSduringearlypregnancy.Radiographics.2004;24(1):157–174.
Which anatomic structures should be included in the scan?
Which anatomic structures should be included in the scan?
• AIUM and ACOG have published a list of fetal structures which constitute the essential elements of the anatomical survey.

6/7/2017
16
What is the role of the gestational age in constructing the list of structures to be scanned at 11‐136/7 weeks?
What is the role of the gestational age in constructing the list of structures to be scanned at 11‐136/7 weeks?
• Due to the developmental timeline of the fetal structure, not all routinely imaged during the 2nd trimester anatomy scan are fully formed at 11‐136/7 weeks
• Therefore the question is: which anatomical structures could and should be assessed at 11‐136/7 weeks??
UOG 2013;41:102‐113

6/7/2017
17
Fetal ImagingFetal Imaging Workshop 2013
• Executive summary of a Joint Eunice Kennedy Shriver National Institute of
Child Health and Human Development, SMFM, AIUM, ACOG,
ACR, SPR, and SRU
Uma M. Reddy, MD, MPH, Alfred Z. Abuhamad, MD, Deborah Levine, MD, George R. Saade, MD for the Fetal Imaging Workshop Invited Participants*
Due to its attributed clinical importance it was published in
the three most important Ob/GynJournals
Am J Obstet Gynecol. 2014 May;210(5):387‐97. Obstet Gynecol. 2014 May;123(5):1070‐82. J Ultrasound Med. 2014 May;33(5):745‐57. .
The single paragraph dealing with 1st
trimester anatomy scan:• “Offering NT screening for aneuploidy assessment at 11 to 13 6/7 weeks’ gestation is part of standard of practice in the U.S.”
“If a late 1st trimester US is performed for dating or NT assessment, evaluation for early detection of severe fetal anomalies such as anencephaly and limb‐body wall complex is reasonable. In some
experienced centers, detection of other major fetal anomalies in the first trimester is possible.”15‐19

6/7/2017
18
Fetal imaging: Executive summary of a Joint Eunice Kennedy Shriver National Institute of Child Health
and Human Development, Society for Maternal‐Fetal Medicine, American Institute of Ultrasound in
Medicine, American College of Obstetricians and Gynecologists, American College of Radiology, Society for Pediatric Radiology, and Society of
Radiologists in Ultrasound Fetal Imaging Workshop.Reddy UM, Abuhamad AZ, Levine D, Saade GR; Fetal
Imaging Workshop Invited Participants.
Am J Obstet Gynecol. 2014 May;210(5):387‐97. Review.Obstet Gynecol. 2014 May;123(5):1070‐82. J Ultrasound Med. 2014 May;33(5):745‐57. .
• Alphabetical Order: Jacques Abramowicz, MD, Rush University Medical Center; Alfred Abuhamad, MD, Eastern Virginia Medical School; Ray Bahado‐Singh, MD, Wayne State University; Beryl Benacerraf, MD, Harvard Medical School; Carol Benson, MD, Harvard Medical School; Dorothy Bulas, MD, Children's National Medical Center; Beverly G. Coleman, MD, University of Pennsylvania; Joshua Copel, MD, Yale University School of Medicine; Mary D'Alton, MD, Columbia University; Jodi Dashe, MD; University of Texas Southwestern Medical Center; Peter Doubilet, MD PhD; Harvard Medical School; Jeffrey L. Ecker, MD, Harvard Medical School; Mary C. Frates, MD, Harvard Medical School; James D. Goldberg, MD, California Pacific Medical Center; Lyndon Hill, MD, University of Pittsburgh; John Hobbins, MD, University of Colorado; Sarah Katel, MD, Kaiser Permanente; Jeffrey A. Kuller, MD, Duke University Medical Center; Deborah Levine, MD, Beth Israel Deaconess Medical Center; George A. Macones, MD, MSCE, Washington University School of Medicine; M. Kathryn Menard, MD, MPH, University of North Carolina School of Medicine; Kenneth J. Moise, Jr., MD, University of Texas Medical School at Houston; Mary Norton, MD, Stanford University School of Medicine; Dan O’Keeffe, MD, Society for Maternal‐Fetal Medicine; Lawrence Platt, MD, University of California, Los Angeles; UmaM. Reddy, MD, MPH, Eunice Kennedy Shriver National Institute of Child Health and Human Development; George Saade, MD, University of Texas Medical Branch at Galveston; Lynn Simpson, MD, MSc, Columbia University Medical Center; Catherine Y. Spong, MD, Eunice Kennedy Shriver National Institute of Child Health and Human Development; Ilan E. Timor Tritsch, MD, New York University Medical Center; Isabelle Wilkins, MD, University of Illinois at Chicago; Honor Wolfe, MD, Case Western Reserve University
First trimester normal and abnormal anatomy. Can we finally match the rest of the
world?
First trimester normal and abnormal anatomy. Can we finally match the rest of the
world?
So, the questions still stands:
We could! We Would! But, sadly enough, we are forced to adopt the
“brass standard”!
We could! We Would! But, sadly enough, we are forced to adopt the
“brass standard”!

6/7/2017
19
Yes, it is….but now I need to provide you
with more evidence !!!
Is the 1st Trimester Screen appointment a realistic time to start performing an anatomical
survey?
The first trimester anatomy should be followed by a complete anatomy scan at 18‐22 weeks to look for anatomic structures or anomalies that cannot be diagnosed at 11‐136/7 weeks.
i.e. agenesis of the corpus callosum
Examples from our practiceAnatomical structures
suggested to be included in the anatomic scan by ISUOG at
11 to 136/7 weeks and beyond …..

6/7/2017
20
Head
• Shape
• Cranial Bones
• Midline Falx
• Choroid Plexus
12 2/7 weeks
12 2/7 weeks
Face
• Profile
• Nasal bone
• Maxilla
• Mandible
Face
Retronasal Triangle View
• Two frontal processes of the maxilla
• Palate
12 0/7 weeks
NEW INFO: Waldo Sepulveda: the use of the retronasaltriangle view to detect the nasal bone in the 1st trimester(UOG 2014)

6/7/2017
21
• Upper lipFace
12 0/7 weeks
Face
12 2/7 weeks
• Orbits
• Lenses
12 5/7 weeks
Face
12 2/7 weeks
• Orbits
• Lenses

6/7/2017
22
Neck
12 2/7 weeks
12 5/7 weeks12 2/7 weeks
Spine
Spine
13 3/7 weeks

6/7/2017
23
GA 11 weeks
Courtesy: Ritsuko Pooh, Japan
Posterior fossa pathology ??
Chest
• Lung fields
• Anterior & posterior fetal body contour
12 2/7 weeks
13 3/7 weeks
• 4 chamber views
Heart
Apical & septal 4Ch views, Doppler flow

6/7/2017
24
• RVOT• LVOT
13 3/7 weeks
Heart
• Aortic arch• Ductal arch
13 3/7 weeks
Heart
Abdomen
13 3/7 weeks
• Stomach• Bladder

6/7/2017
25
13 3/7 weeks
Abdomen • Kidneys•Bladder• Renal Arteries
13 3/7 weeks
Abdomen
• Cord Insertion• Umbilical arteries
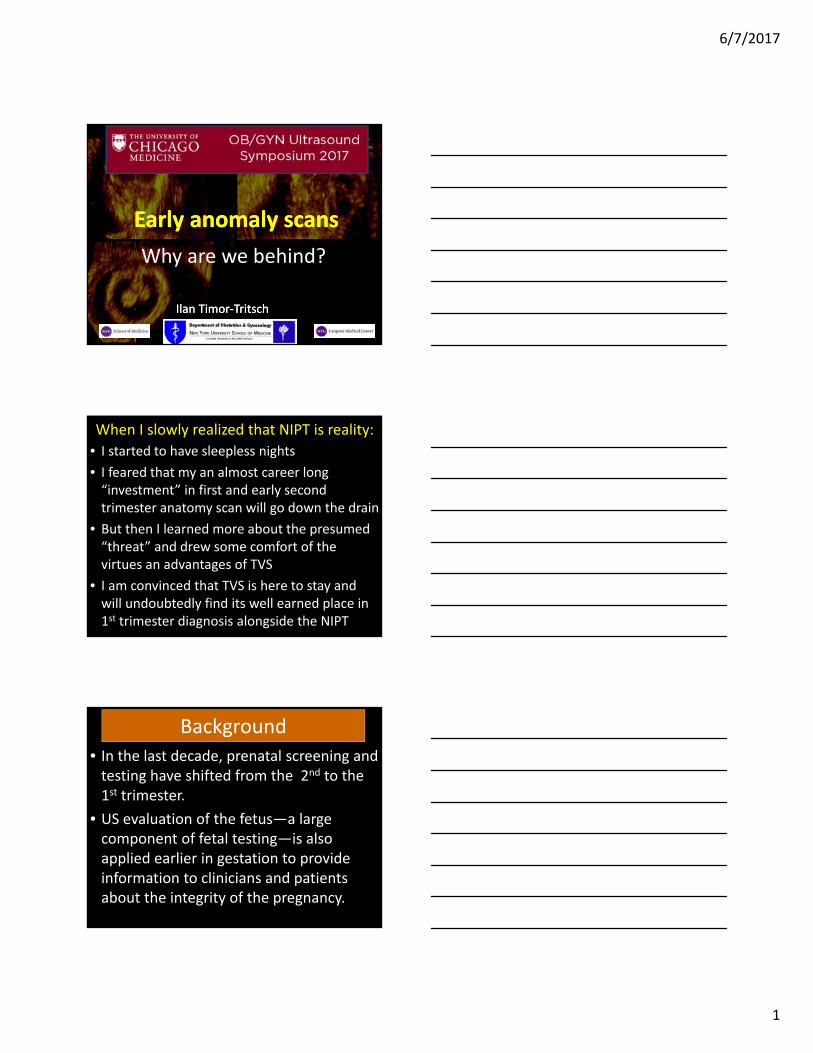
Extremities• Upper
12 5/7 weeks
6/7/2017
26
12 5/7 weeks
• Lower
Extremities
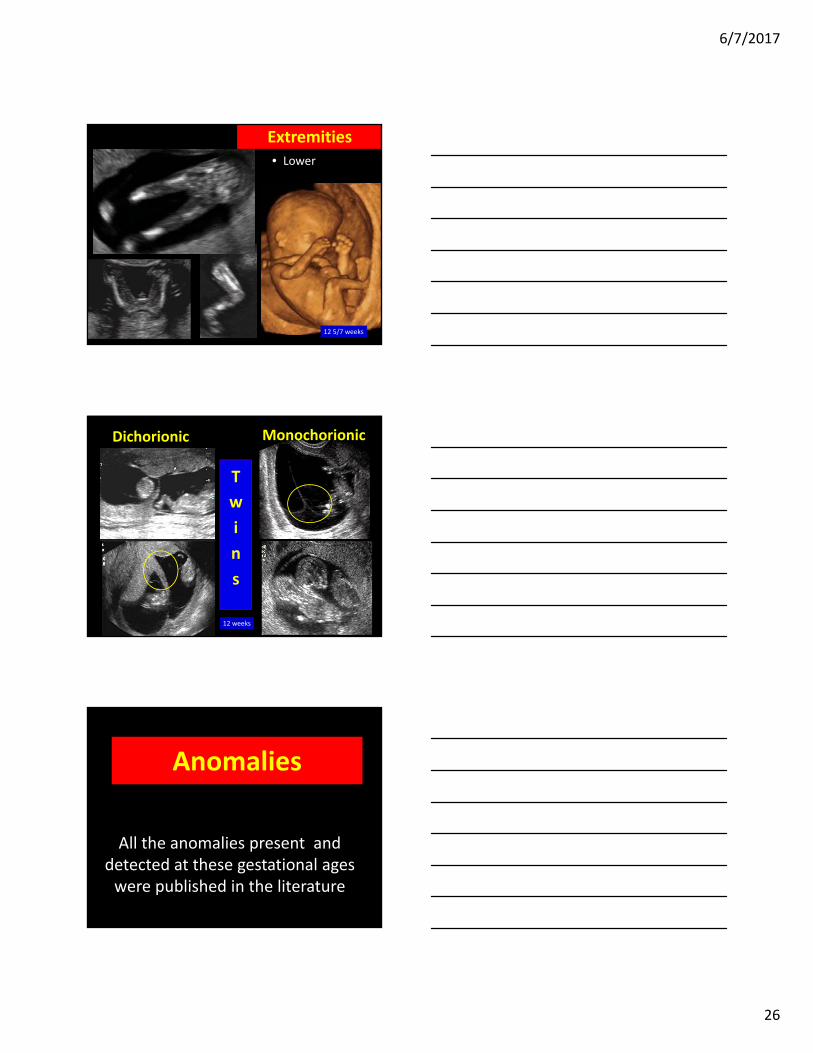
Dichorionic
12 weeks
Monochorionic
T
w
i
n
s
Anomalies
All the anomalies present and detected at these gestational ages were published in the literature

6/7/2017
27
Exencephaly/Anencephaly Sequence
12 w 1d
15 w
??
These are most probably the “skeleton of bloodvessels” left behind after the neural tissue “rubbed off”
Exencephaly/Anencephaly sequence? another proof of the natural hx ?

6/7/2017
28
Holoprosencephaly
11 4/7 weeks 12 1/7 weeks 13 2/7 weeks
9 6/7 weeks
The earliest and easiest detectable brain anomaly

6/7/2017
29
Holoprosencephaly
12 3/7 weeks
Median
Horizontal
Coronal
Inversion
Fused anterior horns of the lateral ventricles
9 weeks 2 days holoprosencephaly
Median
Horizontal
Coronal
Superior view of the “cast” of the ventricles
Fused anterior horns
Posterior
…and this…….
9w 2d Semilobar holoprosencephaly

6/7/2017
30
9w 2d holoprosencephaly
8w NL
al
SagittalCoronal
Fused anterior horns
Fused anterior horns
Fused ThalamiChoroid plexuses
10w 1d holoprosencephaly
Inversion of ventricles: lateral view10w 1d holoprosencephaly10w 1d holoprosencephaly
Inversion renderingInversion rendering

6/7/2017
31
Holoprosencephaly 11 wks
Inversion rendering
Holoprosencephaly 13 wks
Coronal

6/7/2017
32
Sagittal
Axial
Fused anterior horns
Imprint of Falx
Imprint of Falx
Occipital horn
Lateral view
Superior view
Anterior view
Occipital horns
13 weeks holoprosencephaly

6/7/2017
33
3D Inversion rendering of the fused ventricles
Anterior view
Superior view
Lateral view view
Superior view
Comparative images of the anatomy of the anterior horns
Normal brains
Brains with holoprosencephaly
Anterior
Superior view

6/7/2017
34
Thick Nuchal Translucency
11 5/7 weeks
Thick NT’s
NT= 3.4 mm; EGA 12 2/7 wks
NT= 3.5 mm; EGA 12 2/7 wks
Normal Chromosomes
Down syndrome
12 3/7 weeks
Cystic Hygroma

6/7/2017
35
Cystic Hygroma112/7 weeks
Trisomy 18Trisomy 18
Cystic Hygroma 112/7 weeksCystic Hygroma 112/7 weeks
Normal Chromosomes
Posterior Cephalocele
12 4/7 weeks

6/7/2017
36
13 3/7 weeks
Posterior Cephalocele
Exencephaly 112/7 wks
3D Twins discordant for Exencephaly125/7 wks
3D Twins discordant for Exencephaly125/7 wks

6/7/2017
37
Presented at 11w 6d for NT screen CRL= 9w No FH beats

6/7/2017
38
Anterior Cephalocele
13 1/7 weeks
Meckel Syndrome
Brain lesion: ? future cephalocele?
11 3/7 weeks
Micrognathia
13 6/7 weeks

6/7/2017
39
Micrognathia
13 6/7 weeks
Cleft Lip and Palate
12 1/7 weeks
Cleft Lip and Palate
12 1/7 weeks

6/7/2017
40
Histology Courtesy :Dr A. Friedman Mt Sinai NY
15 weeks 4 days
12 weeks 5 days
NL lenses
Congenital cataracts
Monteagudo A, Timor‐Tritsch IE, Friedman AH, Santos R. Autosomal dominant cataracts of the fetus: early detection by transvaginal ultrasound. UOG 1996;8:104‐8.
Spina Bifida
12 3/7 weeks
Spina Bifida
12 3/7 weeks
TH
BS
ITCP
FCM
OB
TH
BS
CP
OB
Non‐visualization of the Intracranial Translucency Normal

6/7/2017
41
The impacted cerebellum obliterating the foramen magnum: “banana sign”
Specimen: Courtesy Dr Bronshtein, IsraelSpecimen: Courtesy Dr Bronshtein, Israel
SPINA BIFIDA14 Weeks 3 days
SPINA BIFIDA14 Weeks 3 days
, Spina bifida at 9 weeks
Courtesy: Ritsuko Pooh, Japan
Pentalogy of Cantrell 13 weeks
Pentalogy of Cantrell 13 weeks
• Large midline defect•Cleft sternum• Ectopia cordis• Pericardial defect• Diaphragmatic defect• Omphalocele

6/7/2017
42
OEIS syndrome
14 weeks 3 days
• Omphalocele• Exstrophy of bladder• Imperforate anus• Spinal defect
•
12 0/7 weeks
OEIS Complex
Omphalocele
Spinal defect

6/7/2017
43
Sacrococcygeal Teratoma
ROMAN AS, MONTEAGUDO A et al. . First‐trimester diagnosis of sacrococcygeal teratoma: the role of 3D ultrasound. UOG 2004; 23: 612–614 12 6/7 weeks
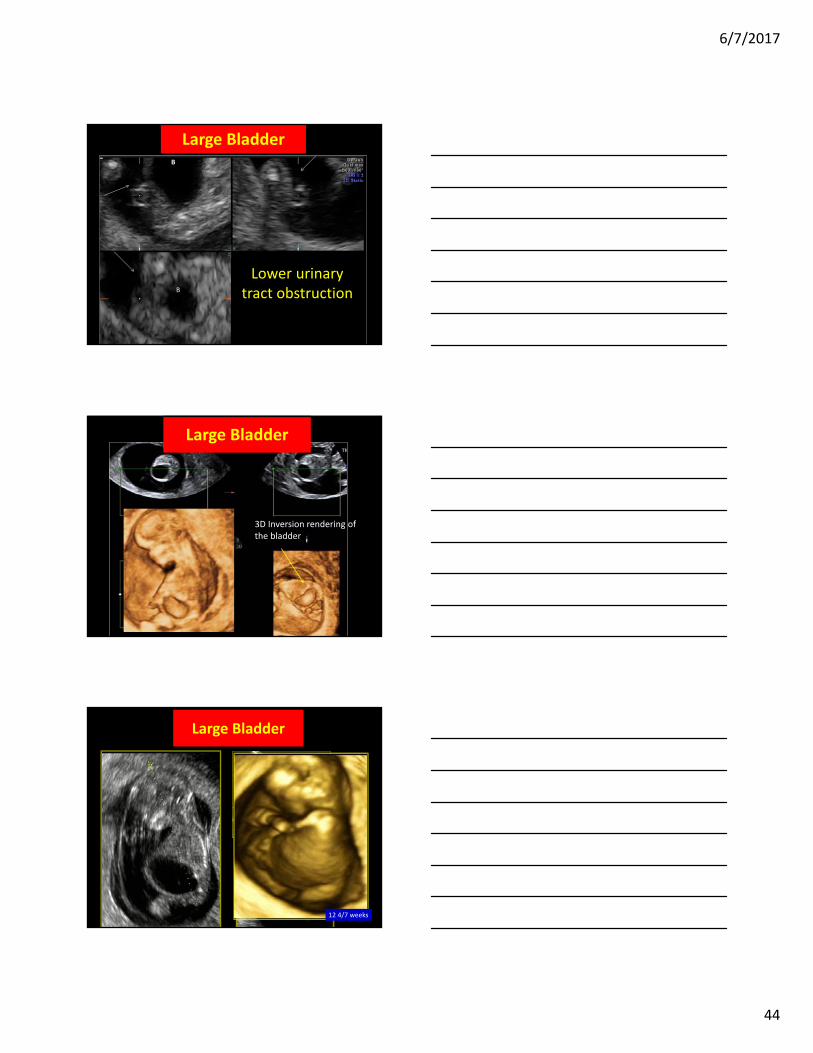
Large Bladder
10 5/7 weeks
12 1/7 weeks
Large Bladder
6/7/2017
44
Lower urinary tract obstruction
B
B
Large Bladder
3D Inversion rendering of the bladder
Large Bladder
Large Bladder
12 4/7 weeks

6/7/2017
45
Single Umbilical Artery
11 6/7 weeks
Exstrophy of the Bladder2V Cord
11 5/7 weeks
Exstrophy of the BladderUmbilical Cord Cyst, 2VC
11 5/7 weeks

6/7/2017
46
11 5/7 weeks
Bladder Exstrophy, Umbilical Cord Cyst and 2VC
Hematoma
Placenta
Cord Insertion
Hematoma
Cord Insertion
Placenta
Monteagudo A, Sfakianaki AK, Timor‐Tritsch IE. Velamentous insertion of the cord in the first trimester.
UOG 2000;16:498‐9.
Velamentous Cord Insertion
11 6/7 weeks
11 4/7 weeks
Omphalocele

6/7/2017
47
Omphalocele
11 6/7 weeks
Omphalocele
12 1/7 weeks
Gastroschisis

6/7/2017
48
Bowel loops on the right side of the cord
11 1/7 weeks
Limb‐Body‐Wall Complex

6/7/2017
49
Polydactyly
14 0/7 weeks
Proximal Femoral Focal Deficiency (PFFD)
Proximal Femoral Focal Deficiency (PFFD)

6/7/2017
50
Extremities‐ Right Hand
12 1/7 weeks
Extremities‐ Right Hand
12 1/7 weeks
Hand Deformity Trisomy 18
11 0/7 weeks

6/7/2017
51
Right Partial Limb Reduction
12 4/7 weeks
3D Rt. Partial Amelia 12w 4d
Absent Hand
Left Right (normal) 15 1/7 weeks

6/7/2017
52
SUA
Monteagudo A, Mayberry P, Rebarber A, Paidas M, Timor‐Tritsch IE. Sirenomelia sequence: first‐trimester diagnosis with both two‐ and three‐dimensional sonography. JUM 2002;21:915‐20.
11 3/7 weeks
Sirenomelia
Sirenomelia
Monteagudo et al JUM 2002;21(8): 915‐20
Sirenomelia
12 0/7 weeks

6/7/2017
53
Anomalies Seen in Twin Pregnancies
Di‐Di Concordance is Uncommon (~10%)Twins Discordant for Exencephaly
Twin A
Twin B
A: NL (NT of 0.7mm)B: Acephalic, had cystic hygroma, no heart,SUA
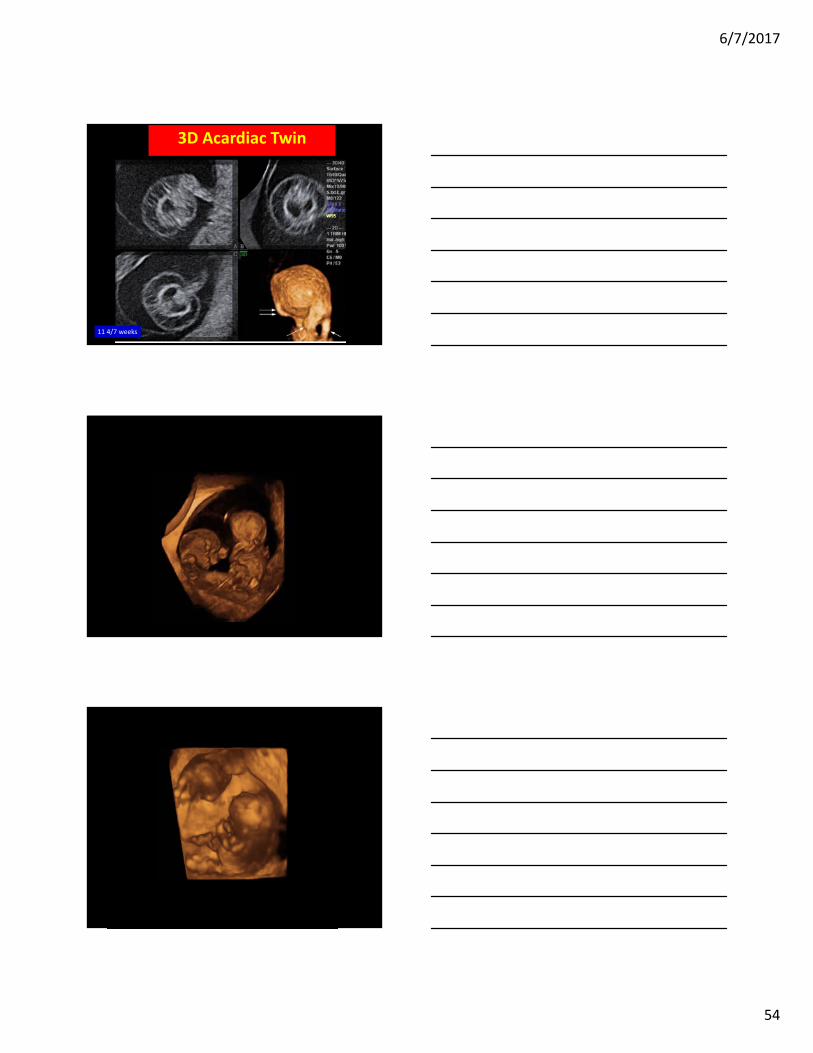
Twin Reversed Arterial Perfusion Sequence (TRAP) “Acardiac Twin”
• A‐to‐A anastomosis• Reversed arterial flow was confirmed 11 4/7 weeks
Bornstein E, Monteagudo A, Dong R, Schwartz N, Timor‐Tritsch IE. Detection of twin reversed arterial perfusion sequence at the time of first‐trimester screening: the added value of 3‐
dimensional volume and color Doppler sonography. JUM 2008;27:1105‐9.
6/7/2017
54
3D Acardiac Twin
11 4/7 weeks

6/7/2017
55
Conjoined Twins
10 5/7 weeks
Bornstein E, Santos R, Timor‐Tritsch IE, Monteagudo A. "Brothers in arms": 3‐dimensional sonographic findings in a first‐trimester thoraco‐omphalopagus conjoined twin pair. JUM 2009;28:97‐9.

6/7/2017
56
Conjoined twins 10 weeks
Courtesy: Yvan Viale MD Lausanne
Courtesy: Yvan Viale MD Lausanne
C
A & BA & B
Timor‐Tritsch IE, Monteagudo A, Horan C, Stangel JJ. Dichorionic triplet pregnancy with the monoamniotictwin pair concordant for omphalocele and bladder exstrophy. UOG 2000;16:669‐71.
Triplet Pregnancy A&B: MoMo Concordant for Bladder Exstrophy &
Omphalocele

6/7/2017
57
T16 at 10 weeks: ectopia cordis
Courtesy: Patricia Mayberry RDMS
Courtesy: Patricia Mayberry RDMS
Summary: I tried to alert you that we should NOT be missing out on 1st trimester US
• It is made possible by high‐frequency transvaginal transducers and better understanding of early signs of fetal pathology.
• It can be performed by TVS and by TAS
• At 12 weeks, about 40% to 50% of common US discernable anomalies are already present
• 2nd ∆ follow‐up US is imperative
• Now that less 1st ∆ screening with NT will be scheduled, it is time for re‐introduction of 1st ∆ anatomy scan Timor‐Tritsch I, Gupta S: Evolving applications of first‐
trimester ultrasound. OBG Management 2012 (Dec).

6/7/2017
58
Conclusions• When is it a realistic time to perform the 1st
trimester anatomy scan?
• At 11 to 13 6/7 weeks
• What structures should be included?
• The ISUOG suggested structures
• Which anomalies can be detected?
• Major anomalies such as anencephaly, HPE, some limb defects and many more…..
• When is it a realistic time to perform the 1st
trimester anatomy scan?
• At 11 to 13 6/7 weeks
• What structures should be included?
• The ISUOG suggested structures
• Which anomalies can be detected?
• Major anomalies such as anencephaly, HPE, some limb defects and many more…..
Conclusions• Do not let this relatively simple and useful diagnostic and in specific cases a screening modality be pushed to the sidelines because of the introduction of NIPT
• They are not mutually exclusive
• They are complementary!
• Do not let this relatively simple and useful diagnostic and in specific cases a screening modality be pushed to the sidelines because of the introduction of NIPT
• They are not mutually exclusive
• They are complementary!
11 2/7 weeks
Thank You