are you ready for your next outbreak? - 2016...
TRANSCRIPT

Antimicrobial Stewardship
Isn’t That Doctor Business?
Janine Carrucan
Nursing Director Infection Prevention & Control

Standard 3: Preventing and controlling
healthcare associated infections
Antimicrobial stewardship
Safe and appropriate antimicrobial prescribing is a
strategic goal of the clinical governance system.

Townsville, North Queensland


Townsville Hospital and Health Service


2013
• Funded AMS program comprising
–1.0 FTE specialist AMS pharmacist
–0.8 FTE clinical nurse
–ID/clinical micro physician from existing
resources


Trial of activities
• 30 bed neurosurgical ward

Antimicrobial IV administration
• Push
• Hang
• Flush
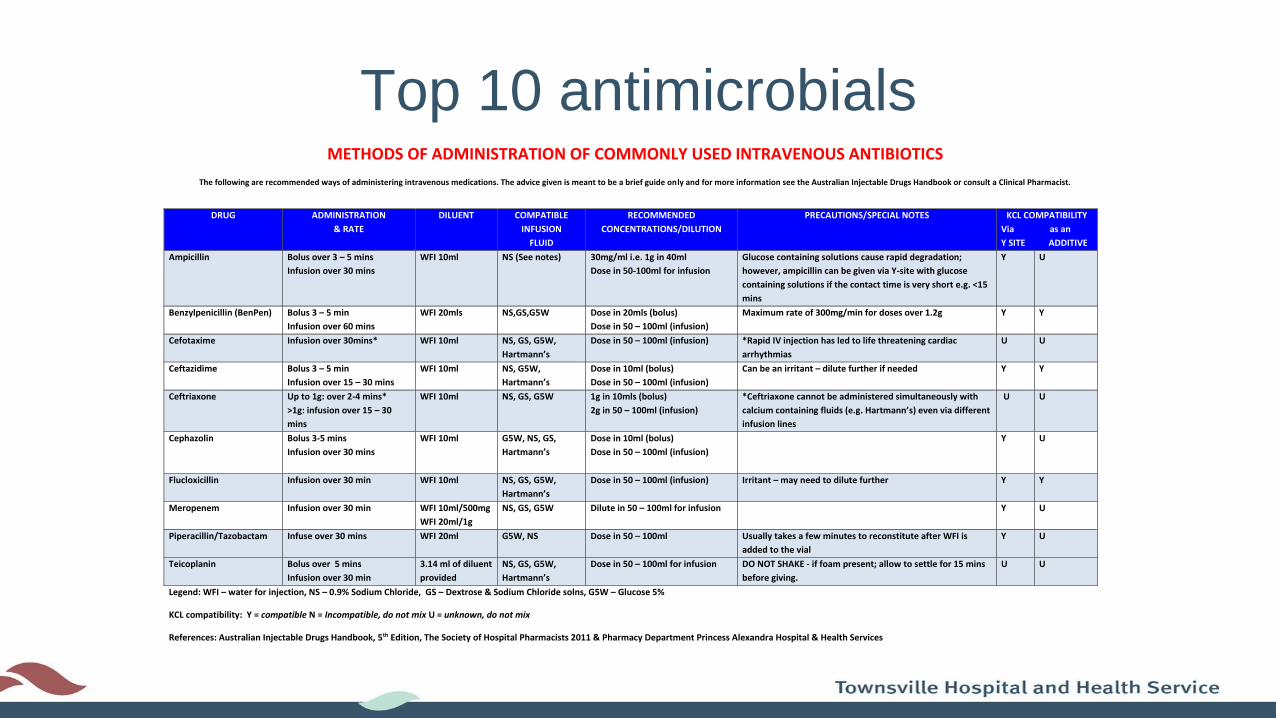
Top 10 antimicrobials
METHODS OF ADMINISTRATION OF COMMONLY USED INTRAVENOUS ANTIBIOTICS
The following are recommended ways of administering intravenous medications. The advice given is meant to be a brief guide only and for more information see the Australian Injectable Drugs Handbook or consult a Clinical Pharmacist.
Legend: WFI – water for injection, NS – 0.9% Sodium Chloride, GS – Dextrose & Sodium Chloride solns, G5W – Glucose 5%
KCL compatibility: Y = compatible N = Incompatible, do not mix U = unknown, do not mix
References: Australian Injectable Drugs Handbook, 5th Edition, The Society of Hospital Pharmacists 2011 & Pharmacy Department Princess Alexandra Hospital & Health Services
DRUG ADMINISTRATION
& RATE
DILUENT COMPATIBLE
INFUSION
FLUID
RECOMMENDED
CONCENTRATIONS/DILUTION
PRECAUTIONS/SPECIAL NOTES KCL COMPATIBILITY
Via as an
Y SITE ADDITIVE
Ampicillin Bolus over 3 – 5 mins
Infusion over 30 mins
WFI 10ml NS (See notes) 30mg/ml i.e. 1g in 40ml
Dose in 50-100ml for infusion
Glucose containing solutions cause rapid degradation;
however, ampicillin can be given via Y-site with glucose
containing solutions if the contact time is very short e.g. <15
mins
Y U
Benzylpenicillin (BenPen) Bolus 3 – 5 min
Infusion over 60 mins
WFI 20mls NS,GS,G5W Dose in 20mls (bolus)
Dose in 50 – 100ml (infusion)
Maximum rate of 300mg/min for doses over 1.2g Y Y
Cefotaxime Infusion over 30mins* WFI 10ml NS, GS, G5W,
Hartmann’s
Dose in 50 – 100ml (infusion) *Rapid IV injection has led to life threatening cardiac
arrhythmias
U U
Ceftazidime Bolus 3 – 5 min
Infusion over 15 – 30 mins
WFI 10ml NS, G5W,
Hartmann’s
Dose in 10ml (bolus)
Dose in 50 – 100ml (infusion)
Can be an irritant – dilute further if needed Y Y
Ceftriaxone Up to 1g: over 2-4 mins*
>1g: infusion over 15 – 30
mins
WFI 10ml NS, GS, G5W 1g in 10mls (bolus)
2g in 50 – 100ml (infusion)
*Ceftriaxone cannot be administered simultaneously with
calcium containing fluids (e.g. Hartmann’s) even via different
infusion lines
U U
Cephazolin Bolus 3-5 mins
Infusion over 30 mins
WFI 10ml G5W, NS, GS,
Hartmann’s
Dose in 10ml (bolus)
Dose in 50 – 100ml (infusion)
Y U
Flucloxicillin Infusion over 30 min WFI 10ml NS, GS, G5W,
Hartmann’s
Dose in 50 – 100ml (infusion) Irritant – may need to dilute further Y Y
Meropenem Infusion over 30 min WFI 10ml/500mg
WFI 20ml/1g
NS, GS, G5W Dilute in 50 – 100ml for infusion Y U
Piperacillin/Tazobactam
Infuse over 30 mins WFI 20ml G5W, NS Dose in 50 – 100ml Usually takes a few minutes to reconstitute after WFI is
added to the vial
Y U
Teicoplanin Bolus over 5 mins
Infusion over 30 min
3.14 ml of diluent
provided
NS, GS, G5W,
Hartmann’s
Dose in 50 – 100ml for infusion DO NOT SHAKE - if foam present; allow to settle for 15 mins
before giving.
U U

Penicillin allergy
mismatch
PENICILLIN ALLERGY
In serious penicillin allergy (e.g. anaphylaxis, bronchospasm, urticaria, angioedema), avoid ALL penicillins, cephalosporins and other beta-lactam antibiotics. In non-severe penicillin allergy (e.g. mild rash) use cephalosporins & carbapenems with caution. Some reactions (e.g. nausea) are not considered allergies and do not warrant prohibiting penicillin use.
Record allergies on the medication chart in the ‘Allergy section’, the yellow alert sheet in the front of the patient notes
(include details of drug and reaction, and the name of the person completing the record). Place an alert sticker on the
front cover of the patient notes.
Contact your ward pharmacist or AMS Pharmacist (31874) for any concerns/queries.
Created by – THHS AMS Team - December 2013. Endorsed: THHS AMS Committee
Acknowledgements: Pharmacy Department, Women’s and Children’s Hospital, Adelaide SA & Counties Manukau District Health Board, Auckland, New Zealand
Ampicillin
Amoxycillin
Amoxycillin/clavulanic acid (Augmentin®)
Benzathine penicillin
Benzylpenicillin (Penicillin G)
Phenoxymethylpenicillin (Penicillin V)
Dicloxacillin
Flucloxacillin
Piperacillin/tazobactam (Tazocin®)
Ticarcillin/clavulanic acid (Timentin®)
Cefaclor
Cefepime
Cefotaxime
Cefoxitin
Ceftazidime
Ceftriaxone
Cefuroxime
Cephalexin
Cephazolin
Doripenem, Ertapenem, Imipenem, Meropenem
Aztreonam
Azithromycin, Erythromycin, Roxithromycin,
Clarithromycin Ciprofloxacin, Norfloxacin, Moxifloxacin
Clindamycin, Lincomycin
Doxycycline, Minocycline, Tigecycline
Gentamicin, Tobramycin, Amikacin
Linezolid
Metronidazole
Trimethoprim/Sulfamethoxazole
Vancomycin

Therapeutic drug monitoring
vancomycin/gentamicin
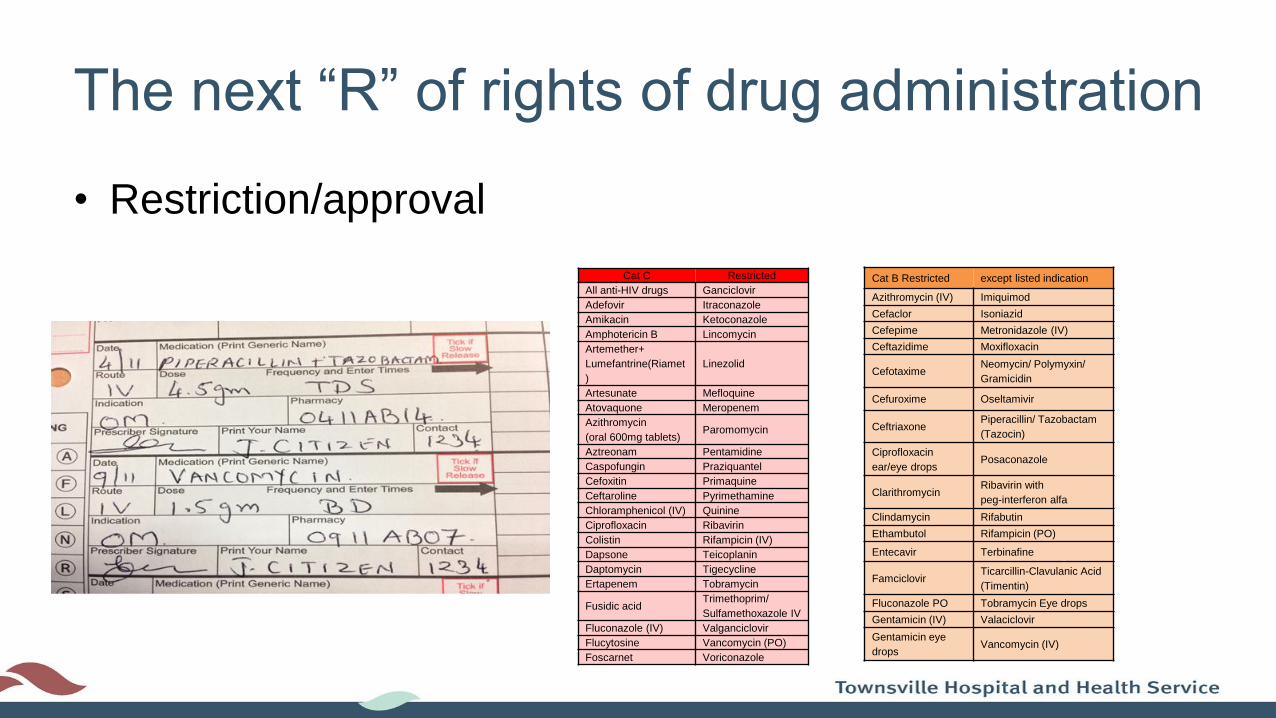
The next “R” of rights of drug administration
• Restriction/approval
Cat C Restricted
All anti-HIV drugs Ganciclovir
Adefovir Itraconazole
Amikacin Ketoconazole
Amphotericin B Lincomycin
Artemether+
Lumefantrine(Riamet
)
Linezolid
Artesunate Mefloquine
Atovaquone Meropenem
Azithromycin
(oral 600mg tablets)Paromomycin
Aztreonam Pentamidine
Caspofungin Praziquantel
Cefoxitin Primaquine
Ceftaroline Pyrimethamine
Chloramphenicol (IV) Quinine
Ciprofloxacin Ribavirin
Colistin Rifampicin (IV)
Dapsone Teicoplanin
Daptomycin Tigecycline
Ertapenem Tobramycin
Fusidic acidTrimethoprim/
Sulfamethoxazole IV
Fluconazole (IV) Valganciclovir
Flucytosine Vancomycin (PO)
Foscarnet Voriconazole
Cat B Restricted except listed indication
Azithromycin (IV) Imiquimod
Cefaclor Isoniazid
Cefepime Metronidazole (IV)
Ceftazidime Moxifloxacin
CefotaximeNeomycin/ Polymyxin/
Gramicidin
Cefuroxime Oseltamivir
CeftriaxonePiperacillin/ Tazobactam
(Tazocin)
Ciprofloxacin
ear/eye dropsPosaconazole
ClarithromycinRibavirin with
peg-interferon alfa
Clindamycin Rifabutin
Ethambutol Rifampicin (PO)
Entecavir Terbinafine
FamciclovirTicarcillin-Clavulanic Acid
(Timentin)
Fluconazole PO Tobramycin Eye drops
Gentamicin (IV) Valaciclovir
Gentamicin eye
dropsVancomycin (IV)

Specimen collection
• Urine
• Faeces
• Respiratory
• Other body fluids
IV to oral switch?

Auditing/educationAuditing
– Sepsis audit
– NAPs audit
– acNAPs audit
– Surgical antibiotic prophylaxis/SSS
Education
– Nursing Grand Rounds
– Nurses education
– Patient focused education
– Shadowing at IV administration times to assess compliance

Evaluation
• Too much for one dedicated FTE
• Included in the ICP role description
• Targeted AMS topics each month
• Ensure goals are achievable within the resources
• All achievements will have positive outcomes for patients
NO!
AMS is NOT just Doctor Business!