as with any system the first thing that should be done before commencing the examination is to...
TRANSCRIPT

Neurological Examination
What comes fi rst?
As with any system the first thing that should be done before commencing the examination is to ___________.For the neurological system the review questions are:
1. Headache or facial pain?2. Fits, faints or funny turns?3. Dizziness or vertigo?4. Disturbances of vision hearing or smell?5. Speech and swallowing difficulties?6. Disturbed sensation?7. Weakness?8. Tremor and involuntary movements?9. Loss of bladder/bowel control?10.Gait disturbances?
It is also vital to note the temporal course of the illness
take a history

Motor SystemInspection:• Look at the overall positioning of the patient, looking especially for hemiplegic positioning (flexion of elbow and wrist with extension of knee and ankle)• Muscle wasting – compare both sides• Look for fasiculations
• Test muscle tone – ensure the patient is relaxed and repeat each movement at different speeds. This can be surprisingly difficult to evaluate.

Motor SystemArms:Basic Screening Examination
Nerve Root Movements Reflex
C5 Shoulder abduction, elbow flexion
Biceps
C6 Elbow flexion (semipronated) Supinator
C7 Finger extension, elbow extension
Triceps
C8 Finger flexors Finger
T1 Small muscles of the hand No reflex

Motor SystemLegs:Basic Screening Examination
Nerve Root Movements Reflex
L1, L2 Hip flexion No reflex
L3, L4 Knee extension Knee
L5 Dorsiflexion of foot, inversion/eversion of ankle, extension of hallux
No reflex
S1 Hip extension, knee flexion, plantarflexion of foot
Ankle

Sensory SystemThere are five basic modalities of sensation:
Modality Tract Fibre Size
Vibration Sense Posterior column
Large
Proprioception Posterior column
Large
Light Touch Posterior column and Spinothalamic tract
Large and Small
Pin Prick Spinothalamic tract
Small
Temperature Spinothalamic tract
Small
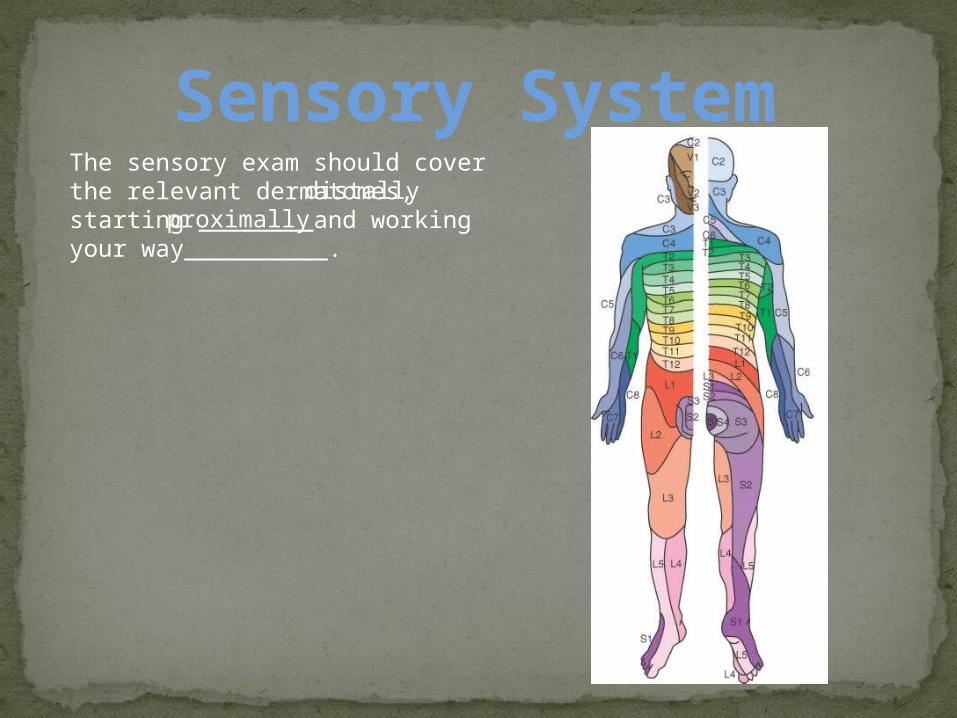
Sensory SystemThe sensory exam should cover the relevant dermatomes, starting ________and working your way__________.
distallyproximally

Sensory SystemThere are four individual nerves which are commonly affected in the upper limb. It is worth knowing their sensory distribution.
Radial
UlnarMedian

Sensory SystemThere are four individual nerves which are commonly affected in the upper limb. It is worth knowing their sensory distribution.
Axillary

Sensory SystemThere are also four individual nerves which are commonly affected in the lower limb. It is worth knowing their sensory distribution.

CoordinationA coordinated series of motor actions is needed to produce a smooth and accurate movement. This requires the integration of sensory feedback and motor output which occurs mainly in the __________.Loss of joint position sense can produce incoordination, especially with the eyes closed, thus it is necessary to test proprioception before coordination.
What to do:• Test the patient’s gait• Finger-nose test• Repeated movements (hand tap)• Heel-shin test• Feet tap
cerebellum

Higher FunctionHigher function is a term used to encompass thought, memory, understanding, perception and intellect. Higher function testing can be divided into the following parts:• Attention• Memory (immediate, short, long)• Calculation• Abstract thought• Spatial• Visual and body perception

Attention and OrientationOrientation:• Time: What day is it? What’s the date? The month, year? What is the season?• Place: What is the name of the place we are at? What is the name of the ward/hospital? What is the name of the city/town?• Person: What is your name? What is your job? Where do you live?
Attention: Digit spanTell the patient you want them to repeat some numbers that you give them. Start with simple sequences of 3 to 4 numbers and increase until the patient makes several mistakes at a certain number of digits. Then ask the patient to repeat the numbers you say backwards.• Normal = seven forward, five backwards.

MemoryImmediate recall:Tell the patient a name and address, e.g. Josh Graham, 18 Bromide Street, Broken Hill. Ask them to repeat it back to you immediately.
Short term recallAfter about 5 minutes ask the patient to recall the name and address.
Long term recallTest factual knowledge that you would expect the patient to have. This varies greatly from patient to patient and needs to be modified carefully. Example general knowledge questions include: Name an American president that was shot dead, what are the colours on the Australian flag, etc?

CalculationSerial sevensAsk the patient to subtract 7 from 100 and to take another seven from what remains. Note the time taken to do the calculations and mistakes made.The premorbid intelligence should also be taken into consideration, for example a mistake made by a maths professor would carry greater significance.
Doubling threesThis should be done if the patient admits to difficulty to calculations. Ask what is two times three. And twice that, and so on. Note how high the patient can go and how long it takes.
Abstract ThoughtThis tests for frontal lobe function and is particularly useful in frontal lobe lesions, dementia and psychiatric illness.
Ask the patient to explain well know proverbs. For example:• A rolling stone gathers no moss• People in glass houses shouldn’t throw stones
The correct interpretation is normal
A physical interpretation such as ‘the stone just rolls down so moss doesn’t stick’ or ‘throwing stones will break the glass’ indicates concrete thinking.
Another useful test is to ask the patient to describe the differences between objects e.g. A table and a chair.

SpatialThis tests for parietal and occipital lobe function.
Clock face:Ask the patient to draw a clock face and fill in the numbers. Ask them to then draw on the hands at a given time, for example quarter past eight.
Five pointed starAsk the patient to copy this five pointed star
Normal= accurate clock and starHalf clock missing= visual inattentionUnable to draw clock or star= constructional apraxia

Visual and body perceptionThis is another test for parietal and occipital lesions. Useful in dementias
Facial recognition: ‘famous faces’Take a bedside newspaper or magazine and ask the patient to identify the faces of famous people. Choose people the patient would be expected to know, e.g. the prime minister, the queen, etc
Normal= faces recognisedFaces not recognised= propagnosia
Body perception:• Patient ignores one side and unable to find hand if asked (Hemi-neglect)• Patient does not recognise left hand if shown it (asomatagnosia)• Patient is unaware of weakness on affected side and will often move the unaffected side when asked to move the affected.

Visual and body perceptionBody perception:Ask the patient to show you their index finger, ring finger and so on. Failure is termed finger agnosia
Ask the patient to touch their left ear with their right hand. Cross their hands and ask which is the right hand. Failure is termed left/right agnosia
Ask the patient to close their eyes and place a familiar object e.g. Coin, pen in their hand and ask them to identify it. Failure is termed astereognosis
Ask the patient to close their eyes and write a number or letter on their palm and ask them what it is. Failure is termed agraphaesthesia

ApraxiaApraxia is an inability to perform a task when there is no weakness, incoordination or movement disorder to prevent it. This tests for parietal function and the premotor cortex of the frontal lobe. It is very useful in dementias.
Ask the patient to perform an imaginary task‘Show me how you would comb your hair, drink a cup of tea, strike a match and blow it out’
The patient is able to perform the action = NormalThe patient is unable to initiate the action, though understanding the command = Ideational apraxiaThe patient performs the task but makes errors = ideomotor apraxia

ApraxiaThe three hand testAsk the patient to copy your movements and demonstrate:1) Make a fist and tap it against the table thumb up2) Straighten your fingers and tap the table with your thumb up3) Place your palm flat on the table
If the patient cannot perform this in the presence of normal motor function = limb apraxia.
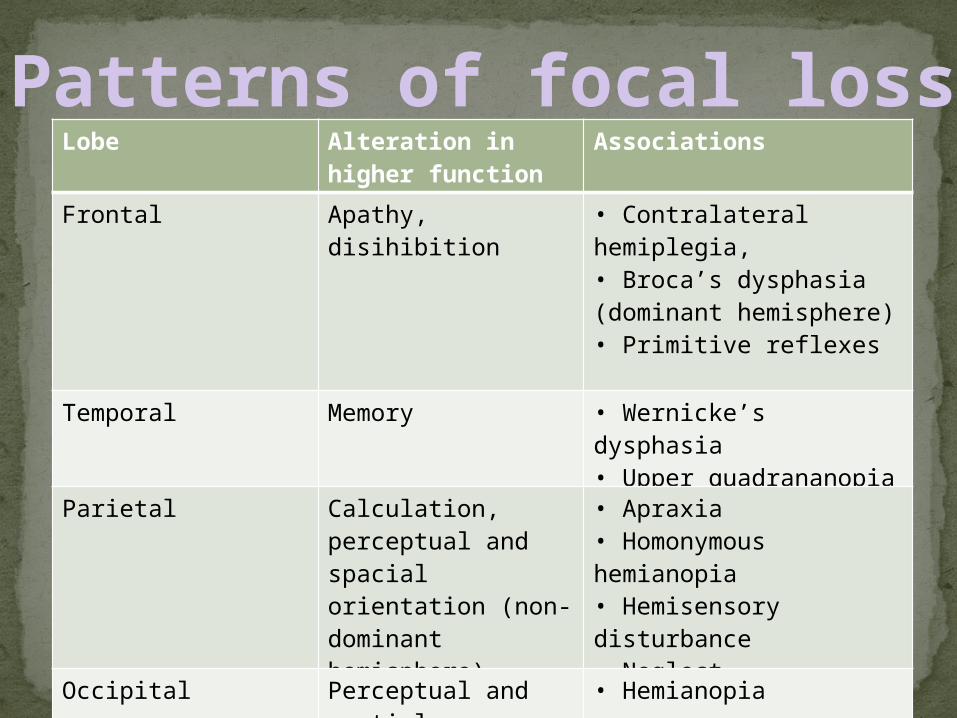
Patterns of focal lossLobe Alteration in
higher functionAssociations
Frontal Apathy, disihibition • Contralateral hemiplegia, • Broca’s dysphasia (dominant hemisphere) • Primitive reflexes
Temporal Memory • Wernicke’s dysphasia• Upper quadrananopia
Parietal Calculation, perceptual and spacial orientation (non-dominant hemisphere)
• Apraxia• Homonymous hemianopia• Hemisensory disturbance• Neglect
Occipital Perceptual and spatial orientation
• Hemianopia