assessing adverse reactions - affiliatedphysicians.com
TRANSCRIPT

Assessing Adverse Reactions
Key Symptoms
Assess patient’s airway, breathing, circulation and mental acuity (i.e. alertness, orientation, coherence of thought).
With early onset of anaphylaxis, vital signs may vary. May initially be normal or tachypnic, tachycardic and hypertensive, however, when entering anaphylactic ‘shock’, patient may become hypotensive, bradycardic and hypoxic.
General appearance can vary according to severity of the anaphylactic episode.
Your assessment, observation and vital sign check(s) will help direct your decision with treatment.
*Use Vital Sign Flowcharts for guidance
1 32 4Rule out anaphylaxis Vital SignsCheck the patient’s appearance Treatment
2 sets of vital signs— minimum of
3 minutes apart.
ANAPHYLAXIS
• Autoimmune response• Tachycardia has been reported in ONLY ¼ of anaphylactic cases• Hypotension – is generally a secondary response• Angioedema of tongue and lips• Laryngeal edema – may present with stridor or severe air hunger• Loss of voice, hoarseness, dysphonia (difficulty speaking when alert – not to be confused with difficulty
speaking when loss of consciousness occurs with a vasovagal reaction)• Passing out generally does not take place with anaphylaxis• Bronchospasm• Mucus hypersecretion and/or inability to swallow secretions• Wheezing• Hypoxia – can cause mentation changes• Vomiting and Diarrhea frequently observed in patients experiencing anaphylaxis• Feeling of impending doom
VASOVAGAL
• Hypotension – is generally a primary response in persons experiencing a vasovagal episode• Bradycardia – is more suggestive of a vasovagal reaction vs anaphylaxis• Typically hypotension occurs in conjunction with low heart rate• Decreased perfusion to extremities, which may result in low oxygen saturation level.
ALWAYS correlate manual HR with HR displayed on pulse oximetry.• Cold and clammy• Feeling warm sensation• Sweating• Lightheaded• Pallor• Dizzy• Blurred vision

Key Symptoms continued...
ANXIETY – PANIC ATTACK
• Mental disorder• Chest tightening or pain• Intense fear• Palpitations• Nausea• Numbness or tingling• Chills or hot flash• Shaking• Sweating• Shortness of breath and/or tachypnea• Palpitations and/or tachycardia
LOCAL REACTIONS
A patient may experience localized adverse reactions to vaccines. The following are some common cutaneous reactions that may occur at the injection site:
• Erythema• Edema• Pruritic
Systemic manifestations are less likely to occur when these symptoms are reported, and are not predictive of systemic anaphylaxis with re-exposure.
Anxiety, Panic Attacks, Vasovagal and Anaphylaxis has some similar symptoms. Be aware of the most significant and most urgent symptoms of all that can be a TRUE Anaphylaxis reaction that requires emergency medication and treatment:
1. Throat – Tongue - Lip swelling or closure
2. Wheezing or stridor
3. Diffuse itching, rash or hives
IMPORTANT TAKEAWAY
**the information shared in this document is meant for guidance and not for diagnosing. This should NOT take the place of physical assessments and sound clinical judgement when managing adverse reactions at community clinic events.
911-EMS needs to be
activated
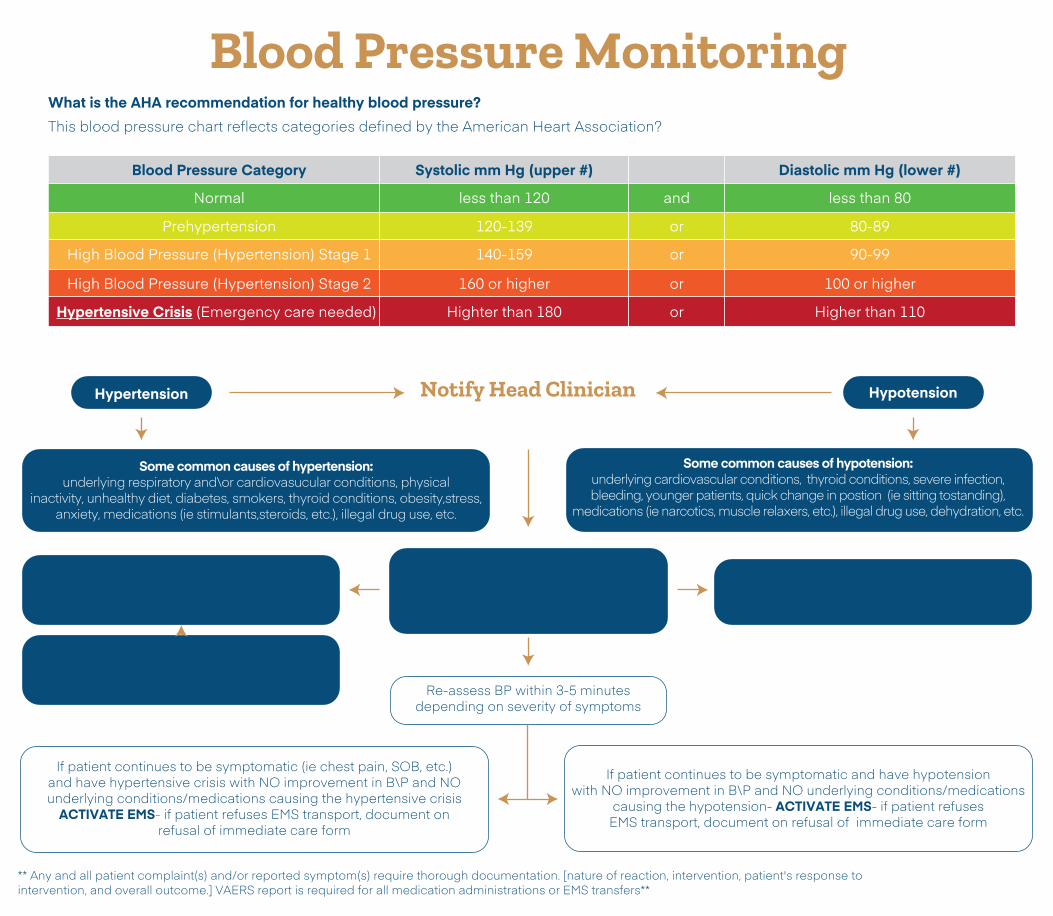
Blood Pressure Monitoring
If patient is symptomatic and hypertensive- Provide comfort, emotionalsupport and re-assurance
If patient has hypertension but is NOT in crisis and/or symptomatic please advise patient
to follow up with PCP or urgent care
Obtain medical and social Hx (cardiac, respiratory diagnosis,
current medications, use of any drugs [recreational and\or OTC], etc)
HypotensionHypertension
If patient is symptomatic andhypotensive- Place patient intrendelenburg position, providecomfort, emotional support and re-assurance
Notify Head Clinician
Re-assess BP within 3-5 minutesdepending on severity of symptoms
What is the AHA recommendation for healthy blood pressure?This blood pressure chart reflects categories defined by the American Heart Association?
If patient continues to be symptomatic (ie chest pain, SOB, etc.) and have hypertensive crisis with NO improvement in B\P and NO underlying conditions/medications causing the hypertensive crisis
ACTIVATE EMS- if patient refuses EMS transport, document on refusal of immediate care form
If patient continues to be symptomatic and have hypotension with NO improvement in B\P and NO underlying conditions/medications
causing the hypotension- ACTIVATE EMS- if patient refuses EMS transport, document on refusal of immediate care form
** Any and all patient complaint(s) and/or reported symptom(s) require thorough documentation. [nature of reaction, intervention, patient's response tointervention, and overall outcome.] VAERS report is required for all medication administrations or EMS transfers**
Some common causes of hypertension:underlying respiratory and\or cardiovasucular conditions, physical
inactivity, unhealthy diet, diabetes, smokers, thyroid conditions, obesity,stress, anxiety, medications (ie stimulants,steroids, etc.), illegal drug use, etc.
Some common causes of hypotension:underlying cardiovascular conditions, thyroid conditions, severe infection, bleeding, younger patients, quick change in postion (ie sitting tostanding),
medications (ie narcotics, muscle relaxers, etc.), illegal drug use, dehydration, etc.
Blood Pressure Category Systolic mm Hg (upper #) Diastolic mm Hg (lower #)
Normal less than 120 and less than 80
Prehypertension 120-139 or 80-89
High Blood Pressure (Hypertension) Stage 1 140-159 or 90-99
High Blood Pressure (Hypertension) Stage 2 160 or higher or 100 or higher
Hypertensive Crisis (Emergency care needed) Highter than 180 or Higher than 110

Heart Rate Monitoring
Common causes for bradycardiamay include: athletes, underlying
cardiovascular conditions including heart blocks, medications (ie narcotics,
beta-blockers, antiarrythmics, etc),recreational drug use, underlying
metabolic , etc.
Obtain medical and social Hx (cardiac, respiratory diagnosis, current medications, use of any
drugs [recreational and\or OTC], etc)
Tachycardia in sympotamtic patient:Maintain patient comfort, provide
emotional support and re-assurance
Bradycardia in symptomatic patient:Place patient in trendelenburg position;
elevate bilateral lower extremities (above heart level). Maintain safety, provide
emotional support and re-assurance.
Common acute reasons forbradycardia that will require
intervention may include:Syncopal vasovagal episodes
Normal Resting HR= 60-100 bpm
Notify HeadClinician
Reassess HR within 3-5 minutes depending on severity of symptoms
and every 5 minutes thereafter until full resolve reported
** Any and all patient complaint(s) and/or reported symptom(s) require thorough documentation. [nature of reaction, intervention, patient's response tointervention, and overall outcome.] VAERS report is required for all medication administrations or EMS transfers**
BradycardiaHR< 60 bpm
No intervention required ifpatient is asymptomatic
No intervention required ifpatient is asymptomatic
TachycardiaHR >100 bpm
If patient continues to be symptomatic and have bradycardia with NO improvement in HR
and NO underlying conditions/medications causing the bradycardia, ACTIVATE EMS
If patient continues to be symptomatic andhave tachycardia with NO improvement
in HR and NO known underlyingconditions/medications, ACTIVATE EMS
Common causes for tachycardia may include: underlying respiratory or
cardiovascular conditions, underlying metabolic conditions, medications (ie
chronic steroid use, etc)
Common acute causes oftachycardia may include:
Anxiety, nervousness, panicattacks, over exertion, medications
(ie antihistamines, steroids, etc.), recreational drug use

Respiratory Rate Monitoring
Common reasons fortachypnea: anxiety,
nervousness, panic attacks,underlying respiratory and\or
cardiovascular conditions,medications (i.e. stimulants),
illegal drug use
Obtain medical and social Hx(cardiac, respiratory diagnosis,current medications, use of any
drugs [recreational and/or OTC], etc)
Reassess RR within 3-5 minutes depending on severity of symptomsand every 5 minutes thereafter until
full resolve of symptoms are reported
Engage in conversation,stimulate patient if needed
via light sternal rub
Encourage deep breathing exercises, provide comfort,
emotional support and re-assurance to patient
Normal Resting RR= 12-20 bpm
Notify HeadClinician
** Any and all patient complaint(s) and/or reported symptom(s) require thorough documentation. [nature of reaction, intervention, patient's response tointervention, and overall outcome.] VAERS report is required for all medication administrations or EMS transfers**
TachypneaRR> 20 bpm
BradypneaRR < 12 bpm
If patient continues to be symptomatic and have tachypnea with NO improvement in RR and NO underlying conditions/medications
causing the tachypnea ACTIVATE EMS
If patient continues to be symptomatic and have bradypnea with NO improvement in RR and NO underlying conditions/medications
causing the bradypnea ACTIVATE EMS
Common reasons for bradypnea: underlying cardiovascular conditions,
medications (ie narcotics, muscle relaxers, etc.), illegal drugs, and
hormonal imbalances

Oxygen Saturation Level Monitoring
common causes of hypoxia:underlying respiratory, metabolic and\or cardiovascular conditions,
anemia, inaccurate saturation secondary to poor circulation and/or nail polish on nail bed
EMS activation not required *unless patient is severely hypoxic and/or symptomatic (i.e. unable to
breath, gasping for air, etc.)
Obtain medical and social Hx (cardiac, respiratory diagnosis,
current medications, use of any drugs [recreational and\or OTC],
etc) Confirm what patient's baseline is.
syncopal/vasovagal reactions:Blood flow is decreased to
peripheral extremeties causing paleness, cool, cold fingers with extended capillary refill times > 3
seconds. This decrease in perfusion causesinaccurate 02 saturation
readings.*Confirm patient is not hypotensive
prior to documenting hypoxia.Alert: hypotension during syncopal
vagovagal episodes can cause decreased perfusion to extremities.)
EMS activation not required*unless patient is severely hypoxic and/or symptomatic (i.e. unable to
breath, gasping for air, etc.)
Acute Hypoxia02 saturation level
< 90%
Notify HeadClinician
Recheck 02 saturation level - If patient continues to be symptomatic and hypoxic ACTIVATE EMS (pulse oximetry should remain on patient's
finger until care of patienthas been transferred safely to EMS).
** Any and all patient complaint(s) and/or reported symptom(s) require thorough documentation. [nature of reaction, intervention, patient's response tointervention, and overall outcome.] VAERS report is required for all medication administrations or EMS transfers**