assessing impact and measuring effectiveness of new payment models wedi innovation summit erik pupo...
TRANSCRIPT

Assessing Impact and Measuring Effectiveness of New Payment Models
WEDI Innovation SummitErik Pupo – Senior Manager - Deloitte

• PCMH in New York• “Increased detection and/or
management of previously undetected diseases associated with an increased focus of PCMH providers on assessment and prevention could be driving increased inpatient utilization as is sometimes seen with individuals who are newly insured and have previous unmet need”
• PCMH in Pennsylvania• “Widespread implementation of the
PCMH with limited data may lead to failure”
Assessing New Payment Models

• Administration of government programs can be influenced to greater or lesser degrees by politics
Ponder the following questions:
• What condition or set of conditions is the new payment model targeting?
• Who makes up the pool of patients in the payment model?
• How are payment penalties, bonuses, and discounts applied in the model?
Role of Politics in Assessment

What are we trying to assess?
The problems with measuring payment models:
1. Is care patient-centered?2. Is care safe and effective?3. Is care timely and accessible? 4. Is care efficient?5. Is care coordinated?6. Is care continuous?7. Is care optimized?8. Are patients engaged in their care?9. Is health information flowing as part of care coordination?10. Is the care accountable?11. Is the care innovative?12. Is learning occurring as care is delivered?

Defining Effective

Paul Taylor’s The Next America: Boomers, Millennials, and the Looming Generational Showdown predicts economic battle between Millennials and Baby Boomers:
“Every family, on some level, is a barter between the generations…If I care for you when you’re young so you’ll care for me when I’m old…But many Millennials won’t be able to afford that…The young today are paying taxes to support a level of benefits for the old that they themselves have no prospect of receiving when they become old.”
Role of Population in Effectiveness

Why does assessing matter?
Source – AHIP

Newer payment models have not been fully exposed to levels of variability within the health system – there are a LOT of variables that go into a payment model. Judgments of effectiveness thus are very subjective
Why does effectiveness matter?
Source – StateHealth.org

1. Transitional, partial bundle models
2. Broader competitive pricing
3. Use of predictive modeling
4. Application of hybrid models
A. Working within inefficiencies of multi-payerB. Relaxed reporting requirements/subjective reporting
5. Supply Chain
A. Moving beyond Value Based Purchasing to Value Based Staffing
What newer approaches work?

A physician practice (or health system) would receive a single (severity-adjusted) payment per patient to cover all of the services provided within the practice that would previously have been billed under individual fee codes, e.g., E&M codes, immunizations
Other outpatient services (e.g., lab tests) and inpatient care (hospitalizations) would con- tinue to be paid separately, but the physician practice would receive a pay-for-performance (P4P)-style bonus/penalty payment based on the level of utilization of those services (on a severity-adjusted basis).
Advantage:
Health IT can be focused on specific domains of care and outpatient and inpatient services where health IT effectiveness is more variable
Outpatient OR Inpatient Excluded

The physician practice or health system would receive a single payment to cover all outpatient OR inpatient costs, but the other level of care would still be paid separately. The practice would receive a bonus/penalty payment based on the rate of utili- zation of inpatient services.
Outpatient or Inpatient Only

• Under competitive pricing, providers (who know a lot about the cost of care) tell payers (who unavoidably know much less) about the resources that are required to provide a given product or service. In administrative pricing, information flows in the other direction
Administrative Pricing vs. Competitive Pricing
Source – StateHealth.org

Pricing for the Skewed Level of Conditions
Source – Massachusetts Cost Trends Report 2013

Dealing with Cost Skew
Source – Massachusetts Cost Trends Report 2013
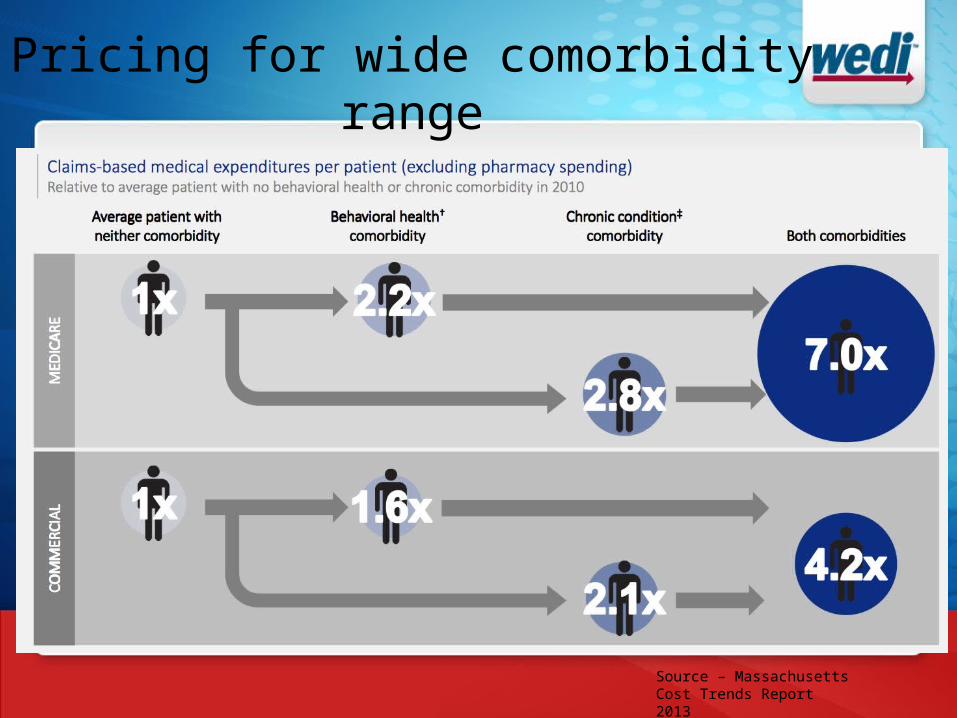
Pricing for wide comorbidity range
Source – Massachusetts Cost Trends Report 2013

Medical homes may be more likely to succeed if they are paired with predictive modeling to proactively identify and intervene on their patients who are most likely to have ambulatory-sensitive hospitalizations most likely to have ambulatory-sensitive hospitalizations
Leveraging Predictive Models
Source – Optum

Assigning a readmissions risk score and estimating resource use based on clinically relevant classifications.
Applying that score throughout the payment model
Applying that score as a measurement for reporting
Triaging (Payment Model as a “Scout”)
Source – JAMA Internal Medicine 2013

“33 required quality measures that are part of the quality performance standard, including the Consumer Assessment of Healthcare Providers and Systems (CAHPS) patient experience survey measures, claims-based measures, the Electronic Health Record (EHR) Incentive Program measure, and the required Group Practice Reporting Option (GPRO) web interface quality measures that are required for purposes of ACO participants earning a Physician Quality Reporting System (PQRS) incentive under the Medicare Shared Savings Program.”
Vs.
Is the patient care “centered”
Patient vs. Bureaucracy Reporting

19
ISSUE Lack of effective coordinated care for patients and their families which prohibits positive recovery.
IMPACT The JourneyMap gives the patient greater control and allows them to be more engaged in their care through real-time feedback, creating unified visibility across multiple providers.
AT A GLANCEThe JourneyMap includes appointment scheduling, education & information sharing, check lists, alerts, social media feeds, dashboards and monitoring to facilitate a positive outcome for the patient on the road to recovery. Providing a coordinated, comprehensive view of the patient, the app provides real-time feedback and enables on-the-go changes to the patient’s care plan.
Patient Journey Maps

20
Supply Chain and Risk
Source – Optum

21
VBP and Risk
Source – Optum

Summary Characteristics for VBP
Source – Optum

• Emphasizing outpatient over inpatient
• Inclusion of staffing levels and/or use of hospital-based staffing plans in VBP programs
• Many of the identified preventable Hospital Acquired Conditions (HACs) - such as falls and nosocomial infections- have been tied, at least in part, to nurse staffing
• Measuring “intensity” in payment models
Value Based Staffing

• Geography matters – innovate to your area• Something that works in one area may not work more broadly
• People matter – don’t ignore behavior in payment innovation• Some doubt on whether the medical home works outside of integrated
delivery settings and with high risk patient populations• Medicare bureaucracy cannot support the introduction and assessment of
multiple payment models
• The innovation angle – target young people for payment model reform• They want a local health care system that’s simple: paperless, treatments
that are necessary and easily understood, prices that are sensible and transparent, and caregivers who listen and connect.
• Little political will to change delivery of care to seniors
Summary Conclusions

1. How can we align our standards work in support of these trends?
2. What is the potential business opportunity for WEDI and its constituents?
3. How can WEDI’s new focus on interoperability fit into payment model assessment and effectiveness (how can WEDI
4. How can WEDI “find its voice” on innovation in payment reform, interoperability
5. How can WEDI promote innovation in its work on healthcare administrative standards?
Takeaways for WEDI