atezolizumab oncology development - food and … oncology development pediatric oncology...
TRANSCRIPT
Atezolizumab Oncology Development Pediatric Oncology Subcommittee of the
Oncologic Drugs Advisory Committee (ODAC) Raphaël Rousseau, M.D., Ph.D.
Global Head, Pediatric Oncology Drug Development Group Genentech, a member of the Roche Group
South San Francisco
1
Outline
• Introduce Roche/Genentech Pediatric Oncology Team
• Cancer Immunotherapy
• Atezolizumab Mechanism of Action
• Atezolizumab Adult Development
• Key Differences Between Adult and Pediatric Cancers
• Atezolizumab Pediatric Development
• Next Steps
2
Genentech/Roche Pediatric Oncology Doing Now What Children Need Next
Provide children with unmet medical needs with innovative, safe, life-saving therapies
• Ensure early access to drugs for children with high unmet medical needs • Improve pediatric patient care through pediatric product labeling • Fulfill pediatric regulatory obligations to enable timely registrations
31 dedicated individuals and growing. Research Scientists, Pediatric Oncologists, Clinical Pharmacologists, Safety Specialists, Regulatory, etc.
Team
Goals
Vision
3
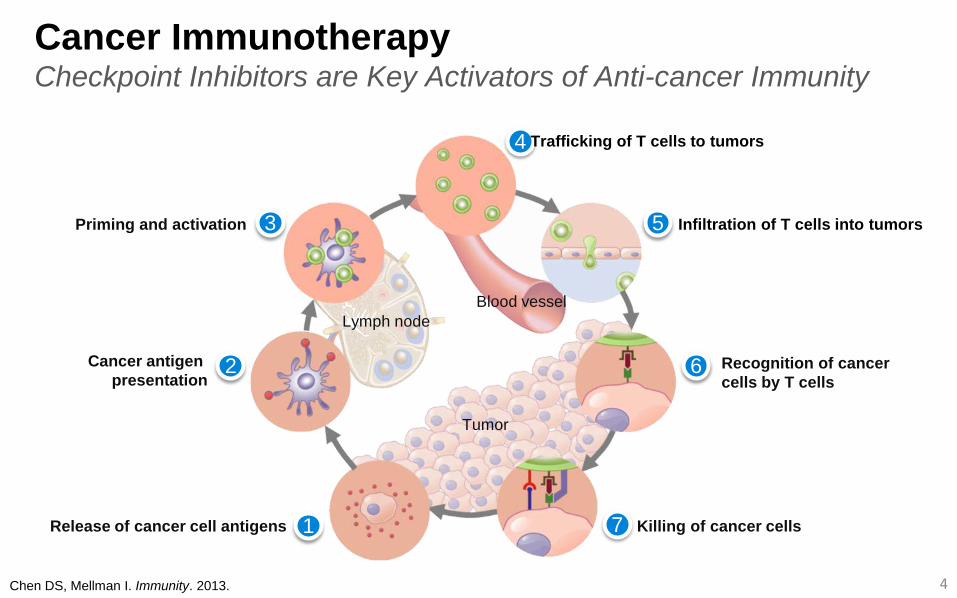
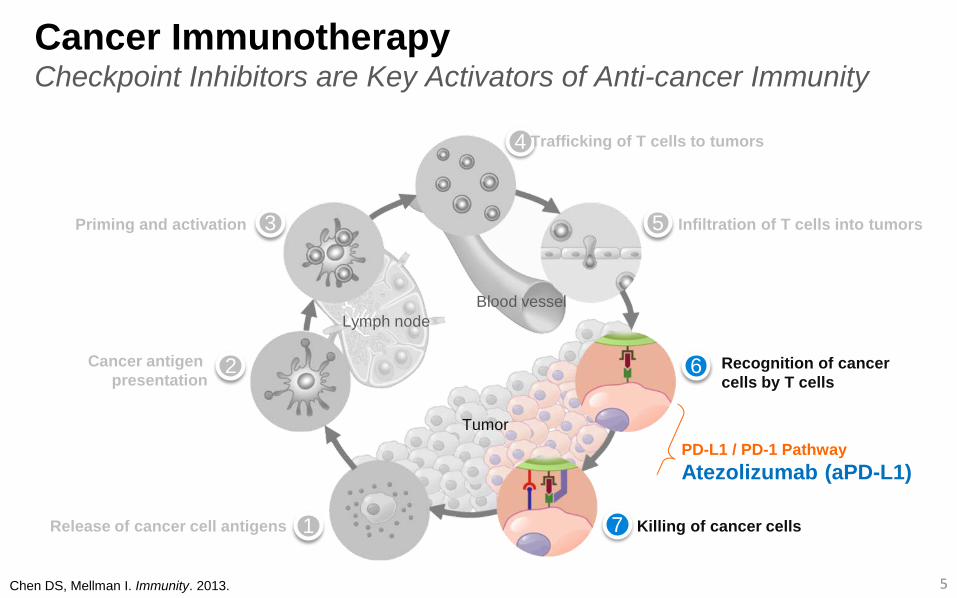
Cancer Immunotherapy Checkpoint Inhibitors are Key Activators of Anti-cancer Immunity
Chen DS, Mellman I. Immunity. 2013.
Cancer antigen presentation
Priming and activation
Recognition of cancer cells by T cells
4
2
3
4
5
6
Lymph node Blood vessel
Tumor
Release of cancer cell antigens 1 7 Killing of cancer cells
Trafficking of T cells to tumors
Infiltration of T cells into tumors
Cancer Immunotherapy Checkpoint Inhibitors are Key Activators of Anti-cancer Immunity
Chen DS, Mellman I. Immunity. 2013.
Release of cancer cell antigens
Cancer antigen presentation
Priming and activation
Recognition of cancer cells by T cells
5
1
2
3
4
5
6
7
Lymph node Blood vessel
Tumor
Killing of cancer cells
PD-L1 / PD-1 Pathway Atezolizumab (aPD-L1)
Trafficking of T cells to tumors
Infiltration of T cells into tumors
6
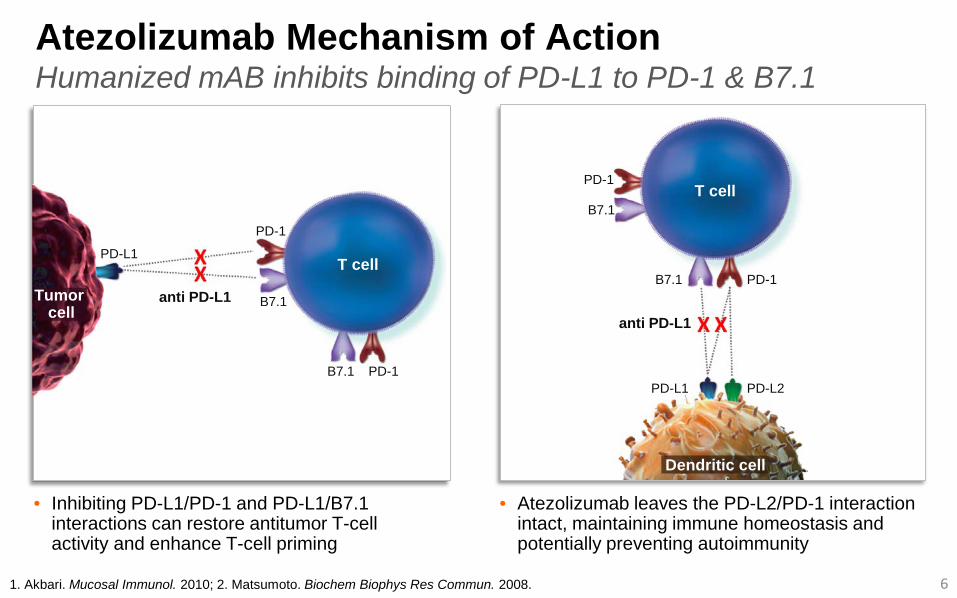
Atezolizumab Mechanism of Action Humanized mAB inhibits binding of PD-L1 to PD-1 & B7.1
1. Akbari. Mucosal Immunol. 2010; 2. Matsumoto. Biochem Biophys Res Commun. 2008.
• Inhibiting PD-L1/PD-1 and PD-L1/B7.1 interactions can restore antitumor T-cell activity and enhance T-cell priming
• Atezolizumab leaves the PD-L2/PD-1 interaction intact, maintaining immune homeostasis and potentially preventing autoimmunity
Tumor cell
T cell PD-L1
PD-1
B7.1
PD-1 B7.1
anti PD-L1
T cell
Dendritic cell
PD-1
B7.1
PD-1 B7.1
PD-L2 PD-L1
anti PD-L1
• ~ 5000 patients have received atezolizumab across clinical trials, as of February 2016
• The key safety risks associated with atezolizumab are immune-related events – Events include pneumonitis, hepatitis, colitis, endocrinopathies, and other
immune-related events including meningitis / encephalitis, motor and sensory neuropathy, and pancreatitis
– Immune-related events are generally grade 1 and 2 in nature and manageable with dose interruption and supportive care, including the use of systemic corticosteroids, where appropriate
• The safety profile appears similar between tumor types and suggests independence from the level of PD-L1 expression
• No apparent dose related trends in the incidence of AEs
Atezolizumab Adult Development Acceptable Safety Profile Across Tumor Types
7
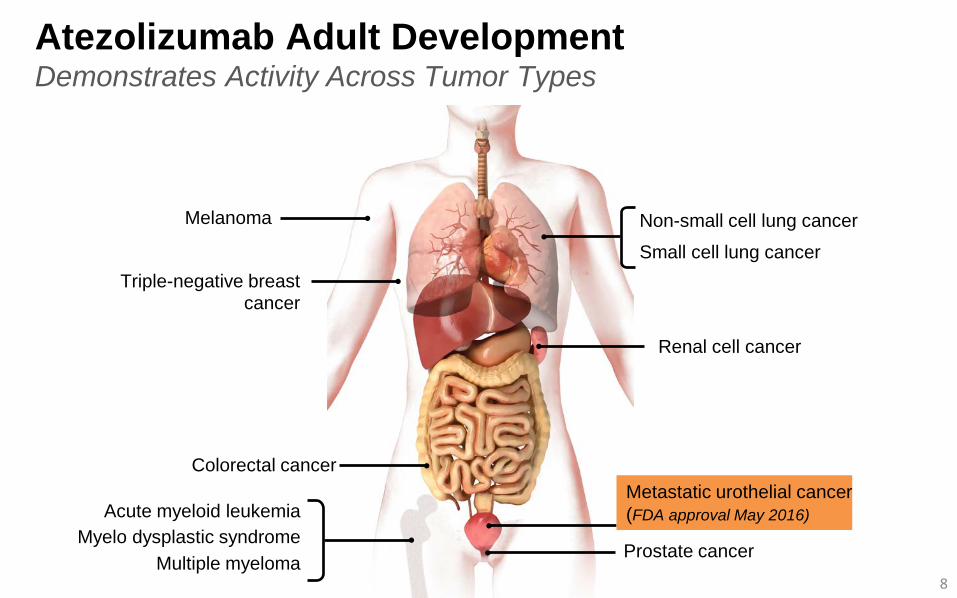
Atezolizumab Adult Development Demonstrates Activity Across Tumor Types
Non-small cell lung cancer
Small cell lung cancer
Renal cell cancer
Prostate cancer
Colorectal cancer
Myelo dysplastic syndrome Multiple myeloma
Acute myeloid leukemia
Triple-negative breast cancer
Melanoma
8
Metastatic urothelial cancer (FDA approval May 2016)
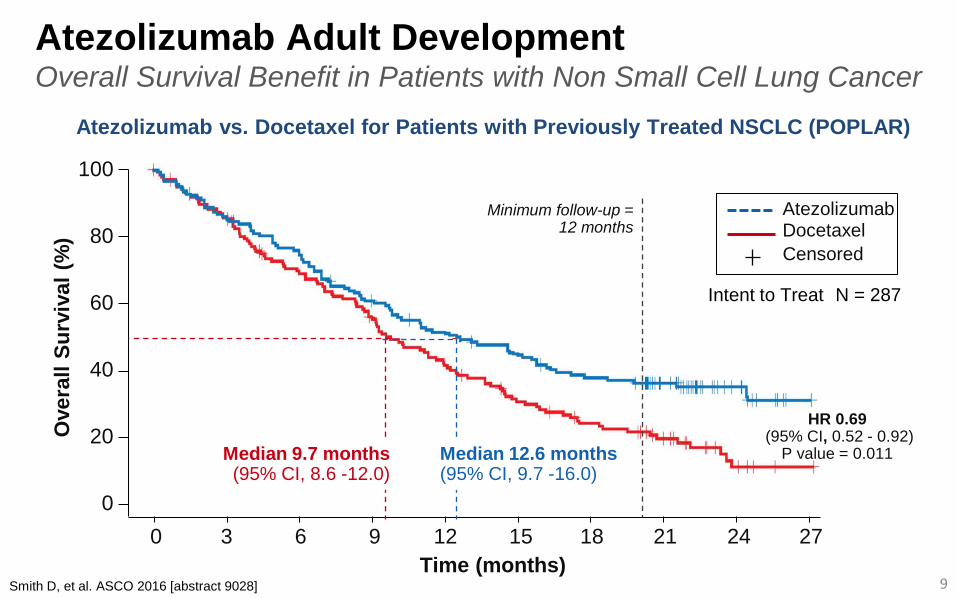
Atezolizumab Adult Development Overall Survival Benefit in Patients with Non Small Cell Lung Cancer
9 Smith D, et al. ASCO 2016 [abstract 9028]
Atezolizumab vs. Docetaxel for Patients with Previously Treated NSCLC (POPLAR)
100
80
60
40
20
0 0 3 6 9 12 15 18 21 24 27
Time (months)
Ove
rall
Surv
ival
(%) Docetaxel
Atezolizumab
Censored
Median 9.7 months (95% CI, 8.6 -12.0)
Median 12.6 months (95% CI, 9.7 -16.0)
HR 0.69 (95% CI, 0.52 - 0.92)
P value = 0.011
Minimum follow-up = 12 months
N = 287 Intent to Treat
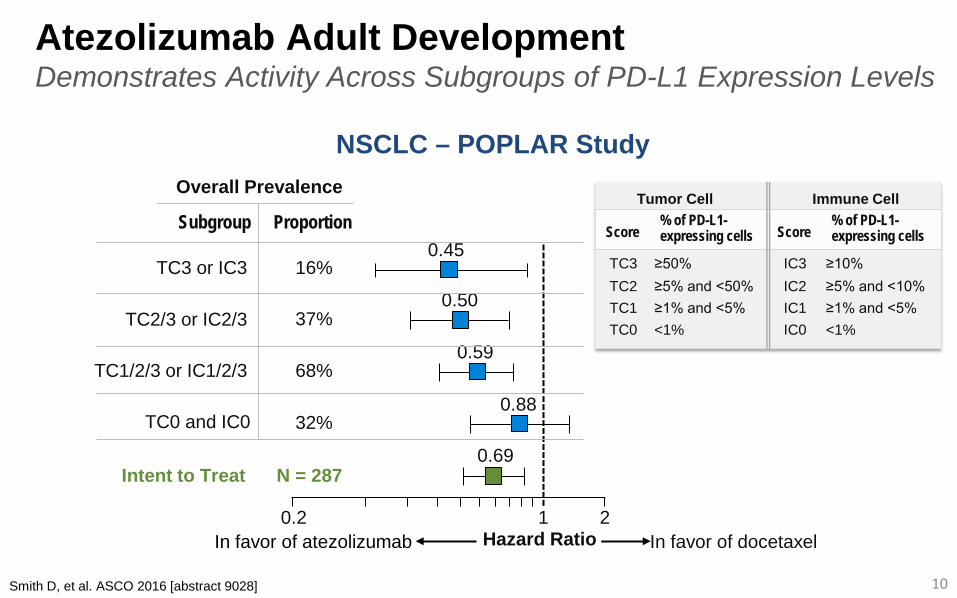
Atezolizumab Adult Development Demonstrates Activity Across Subgroups of PD-L1 Expression Levels
10
NSCLC – POPLAR Study
Tumor Cell % of PD-L1- expressing cells Score
≥50% TC3
TC0 <1% TC1 ≥1% and <5% TC2 ≥5% and <50%
Immune Cell % of PD-L1- expressing cells Score
≥10% IC3
IC0 <1% IC1 ≥1% and <5% IC2 ≥5% and <10%
In favor of docetaxel
0.69
0.88
0.59
0.50
0.45
In favor of atezolizumab
N = 287 Intent to Treat
0.2 1 2 Hazard Ratio
Overall Prevalence
Proportion Subgroup
16% TC3 or IC3
TC0 and IC0 32%
TC1/2/3 or IC1/2/3 68%
TC2/3 or IC2/3 37%
Smith D, et al. ASCO 2016 [abstract 9028]
Antigen release
T cell recognition
T cell killing
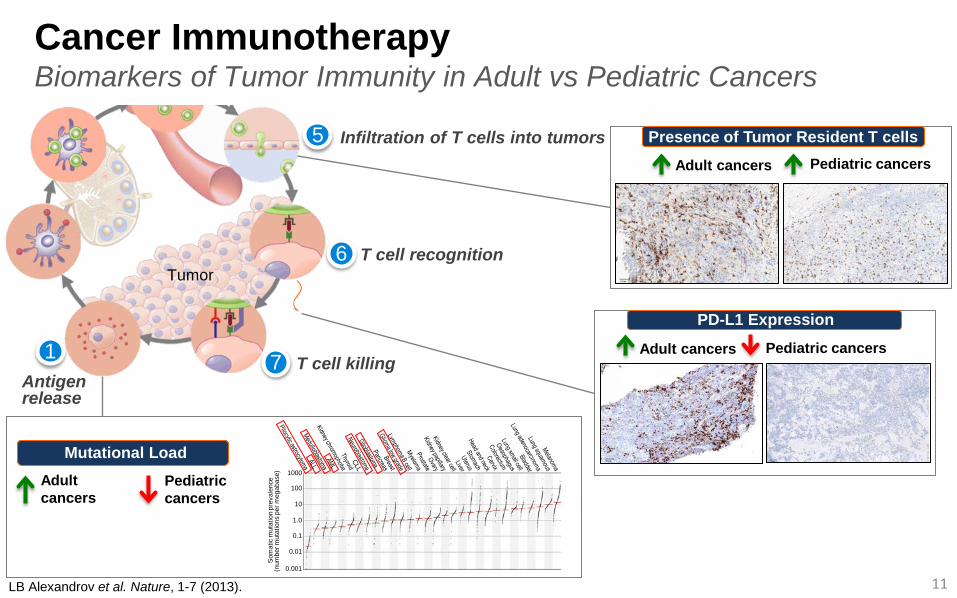
Mutational Load Adult cancers
Pediatric cancers
11
Adult cancers
Presence of Tumor Resident T cells Pediatric cancers
LB Alexandrov et al. Nature, 1-7 (2013).
Cancer Immunotherapy Biomarkers of Tumor Immunity in Adult vs Pediatric Cancers
1 7
6
5 Infiltration of T cells into tumors
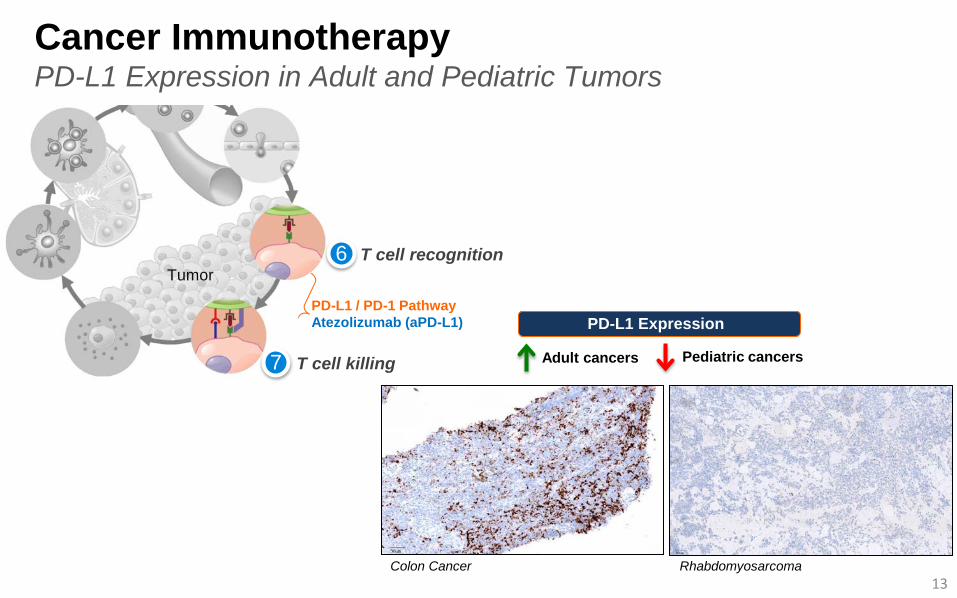
PD-L1 Expression
Adult cancers Pediatric cancers
1000
100
10
1.0
0.1
0.01
0.001
Som
atic
mut
atio
n pr
eval
ence
(n
umbe
r mut
atio
ns p
er m
egab
ase)
Tumor
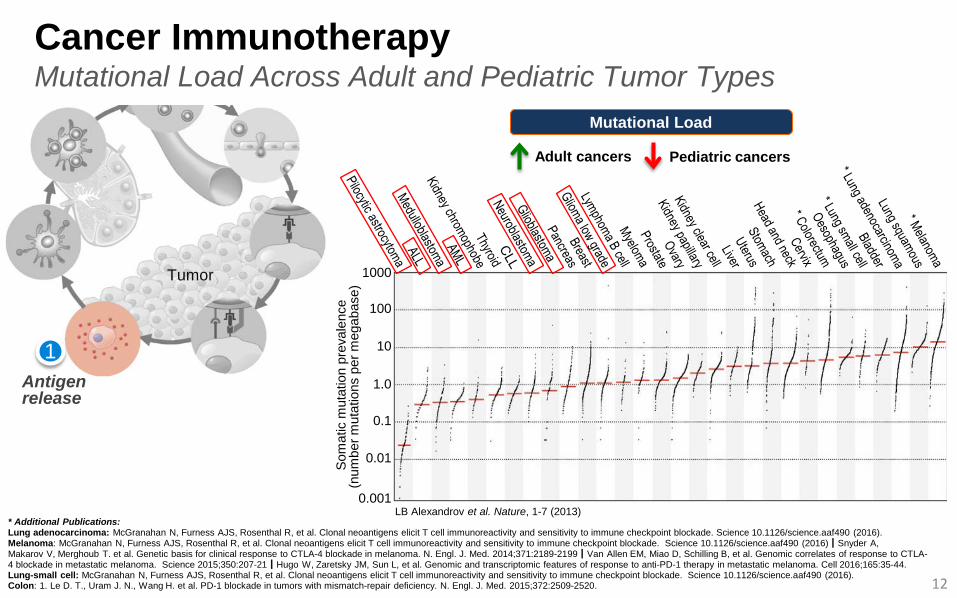
Mutational Load
Adult cancers Pediatric cancers
Cancer Immunotherapy Mutational Load Across Adult and Pediatric Tumor Types
LB Alexandrov et al. Nature, 1-7 (2013)
1000
100
10
1.0
0.1
0.01
0.001
Som
atic
mut
atio
n pr
eval
ence
(n
umbe
r mut
atio
ns p
er m
egab
ase)
* Additional Publications: Lung adenocarcinoma: McGranahan N, Furness AJS, Rosenthal R, et al. Clonal neoantigens elicit T cell immunoreactivity and sensitivity to immune checkpoint blockade. Science 10.1126/science.aaf490 (2016). Melanoma: McGranahan N, Furness AJS, Rosenthal R, et al. Clonal neoantigens elicit T cell immunoreactivity and sensitivity to immune checkpoint blockade. Science 10.1126/science.aaf490 (2016)┃Snyder A, Makarov V, Merghoub T. et al. Genetic basis for clinical response to CTLA-4 blockade in melanoma. N. Engl. J. Med. 2014;371:2189-2199┃Van Allen EM, Miao D, Schilling B, et al. Genomic correlates of response to CTLA-4 blockade in metastatic melanoma. Science 2015;350:207-21┃Hugo W, Zaretsky JM, Sun L, et al. Genomic and transcriptomic features of response to anti-PD-1 therapy in metastatic melanoma. Cell 2016;165:35-44. Lung-small cell: McGranahan N, Furness AJS, Rosenthal R, et al. Clonal neoantigens elicit T cell immunoreactivity and sensitivity to immune checkpoint blockade. Science 10.1126/science.aaf490 (2016). Colon: 1. Le D. T., Uram J. N., Wang H. et al. PD-1 blockade in tumors with mismatch-repair deficiency. N. Engl. J. Med. 2015;372:2509-2520.
Tumor
12
Antigen release
1
PD-L1 Expression
Adult cancers Pediatric cancers
13
Cancer Immunotherapy PD-L1 Expression in Adult and Pediatric Tumors
PD-L1 / PD-1 Pathway Atezolizumab (aPD-L1)
Tumor T cell recognition
T cell killing 7
6
Rhabdomyosarcoma
Colon Cancer
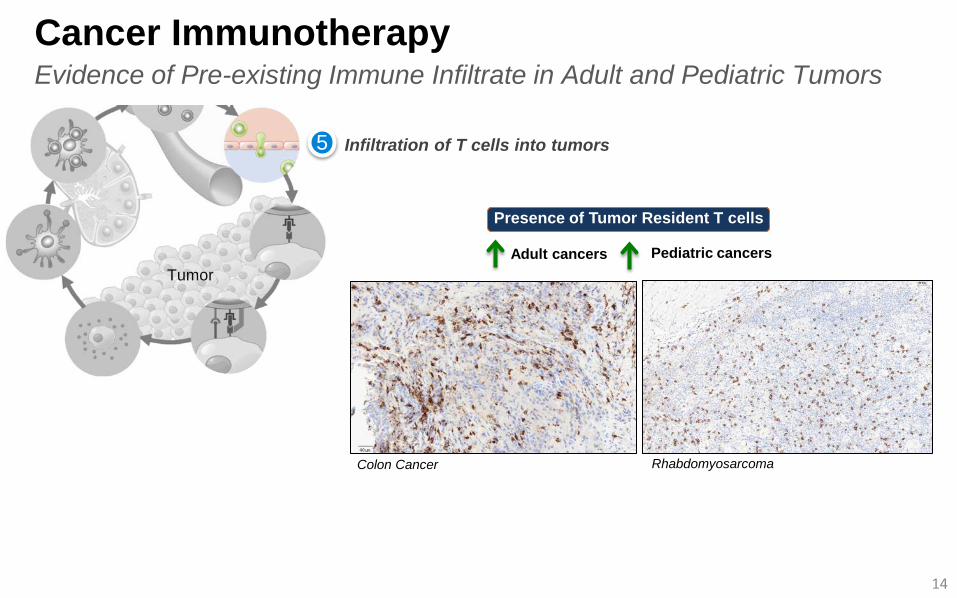
Presence of Tumor Resident T cells
14
Cancer Immunotherapy Evidence of Pre-existing Immune Infiltrate in Adult and Pediatric Tumors
Adult cancers Pediatric cancers Tumor
5 Infiltration of T cells into tumors
Colon Cancer
Rhabdomyosarcoma
Pediatric Biomarker Development
• Unselected pediatric population chosen for Phase I to ensure: – We did not prematurely exclude any children who could potentially benefit – We could collect robust data to optimize our biomarker understanding and development
• Planned evaluation of CD8+ T-cell infiltration PD-L1 expression, and antigen-specific T-cell responses in addition to other immune markers
• Biomarker findings will be utilized to guide amendments to the current protocol, and to the design of future studies
Atezolizumab Pediatric Development Broad Spectrum Biomarker Research Ongoing
15
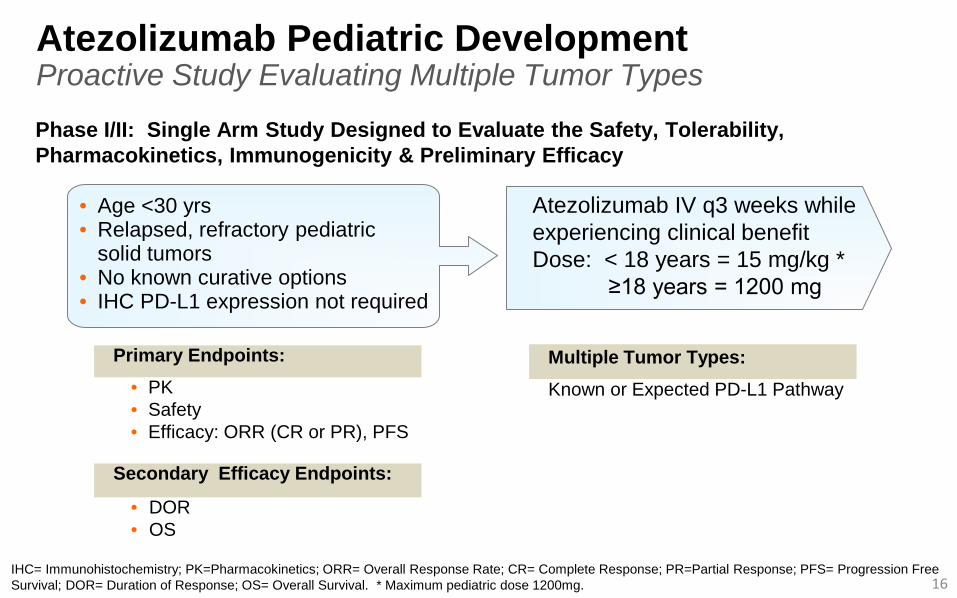
Atezolizumab Pediatric Development Proactive Study Evaluating Multiple Tumor Types
• Age <30 yrs • Relapsed, refractory pediatric
solid tumors • No known curative options • IHC PD-L1 expression not required
Atezolizumab IV q3 weeks while experiencing clinical benefit Dose: < 18 years = 15 mg/kg * ≥18 years = 1200 mg
Primary Endpoints: • PK • Safety • Efficacy: ORR (CR or PR), PFS
Secondary Efficacy Endpoints:
• DOR • OS
Phase I/II: Single Arm Study Designed to Evaluate the Safety, Tolerability, Pharmacokinetics, Immunogenicity & Preliminary Efficacy
16 IHC= Immunohistochemistry; PK=Pharmacokinetics; ORR= Overall Response Rate; CR= Complete Response; PR=Partial Response; PFS= Progression Free Survival; DOR= Duration of Response; OS= Overall Survival. * Maximum pediatric dose 1200mg.
Multiple Tumor Types: Known or Expected PD-L1 Pathway
17
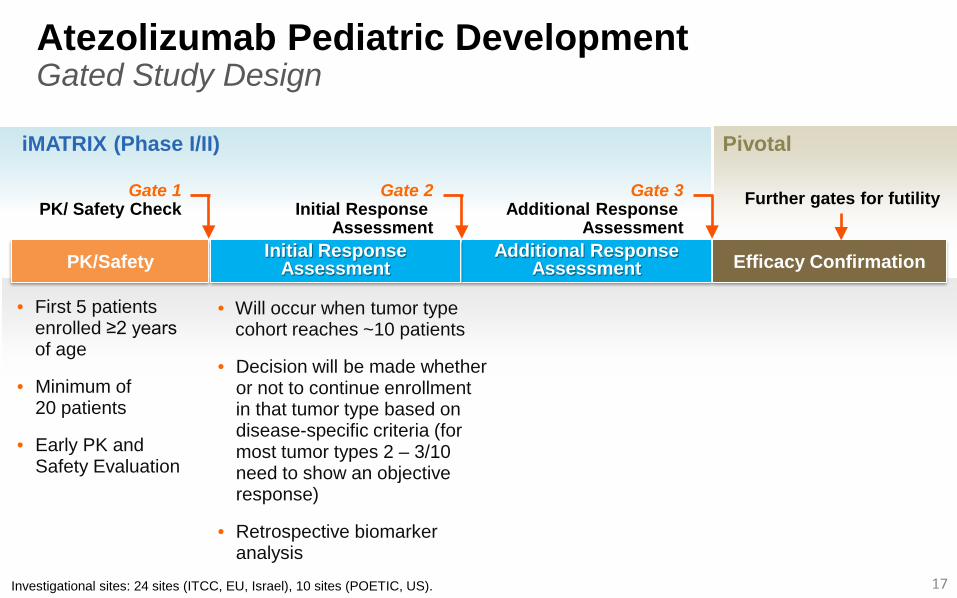
Atezolizumab Pediatric Development Gated Study Design
Gate 1 PK/ Safety Check
PK/Safety Additional Response Assessment Efficacy Confirmation
iMATRIX (Phase I/II) Pivotal
Further gates for futility Gate 2 Initial Response
Assessment
Gate 3 Additional Response
Assessment Initial Response
Assessment
• First 5 patients enrolled ≥2 years of age
• Minimum of 20 patients
• Early PK and Safety Evaluation
• Will occur when tumor type cohort reaches ~10 patients
• Decision will be made whether or not to continue enrollment in that tumor type based on disease-specific criteria (for most tumor types 2 – 3/10 need to show an objective response)
• Retrospective biomarker analysis
Investigational sites: 24 sites (ITCC, EU, Israel), 10 sites (POETIC, US).
18
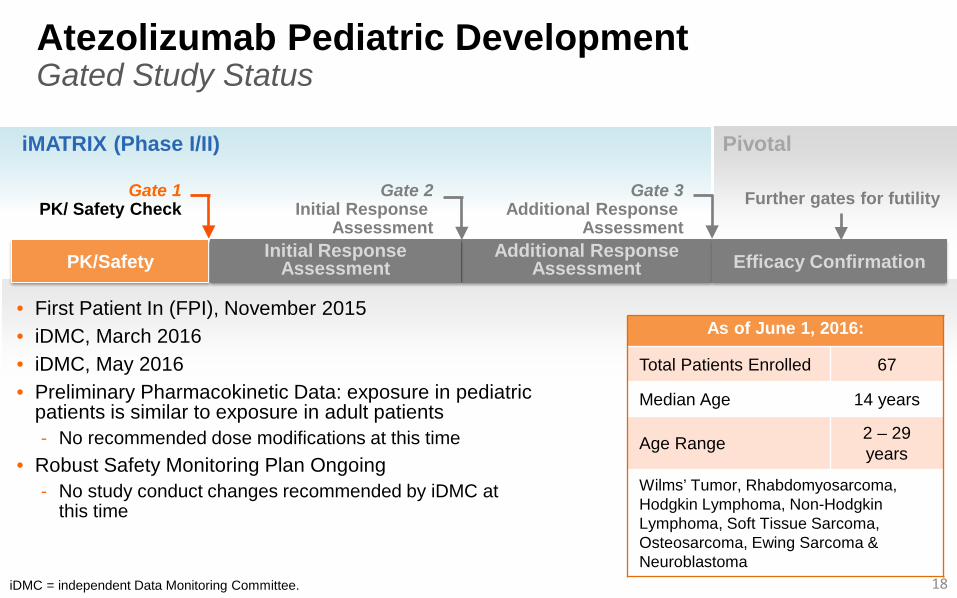
Atezolizumab Pediatric Development Gated Study Status
PK/Safety Additional Response Assessment Efficacy Confirmation
Pivotal
Initial Response Assessment
As of June 1, 2016:
Total Patients Enrolled 67
Median Age 14 years
Age Range 2 – 29 years
Wilms’ Tumor, Rhabdomyosarcoma, Hodgkin Lymphoma, Non-Hodgkin Lymphoma, Soft Tissue Sarcoma, Osteosarcoma, Ewing Sarcoma & Neuroblastoma
• First Patient In (FPI), November 2015 • iDMC, March 2016 • iDMC, May 2016 • Preliminary Pharmacokinetic Data: exposure in pediatric
patients is similar to exposure in adult patients - No recommended dose modifications at this time
• Robust Safety Monitoring Plan Ongoing - No study conduct changes recommended by iDMC at
this time
iMATRIX (Phase I/II)
iDMC = independent Data Monitoring Committee.
Gate 1 PK/ Safety Check Further gates for futility Gate 2
Initial Response Assessment
Gate 3 Additional Response
Assessment
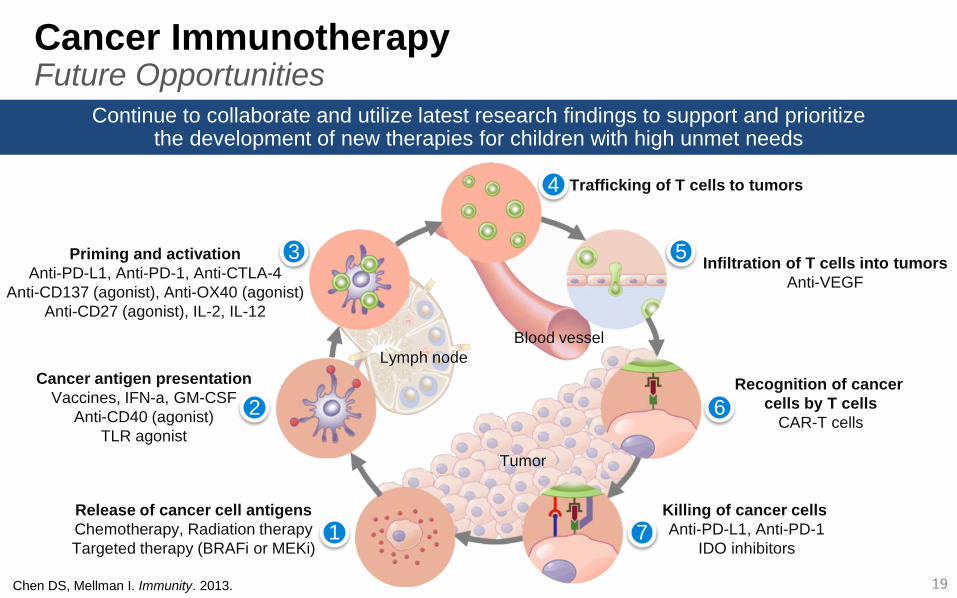
Cancer Immunotherapy Future Opportunities
Chen DS, Mellman I. Immunity. 2013.
Release of cancer cell antigens Chemotherapy, Radiation therapy Targeted therapy (BRAFi or MEKi)
Cancer antigen presentation Vaccines, IFN-a, GM-CSF
Anti-CD40 (agonist) TLR agonist
Priming and activation Anti-PD-L1, Anti-PD-1, Anti-CTLA-4
Anti-CD137 (agonist), Anti-OX40 (agonist) Anti-CD27 (agonist), IL-2, IL-12
Trafficking of T cells to tumors
Infiltration of T cells into tumors Anti-VEGF
Recognition of cancer cells by T cells
CAR-T cells
Killing of cancer cells Anti-PD-L1, Anti-PD-1
IDO inhibitors 1
2
3
4
5
6
7
19
Continue to collaborate and utilize latest research findings to support and prioritize the development of new therapies for children with high unmet needs
Lymph node Blood vessel
Tumor
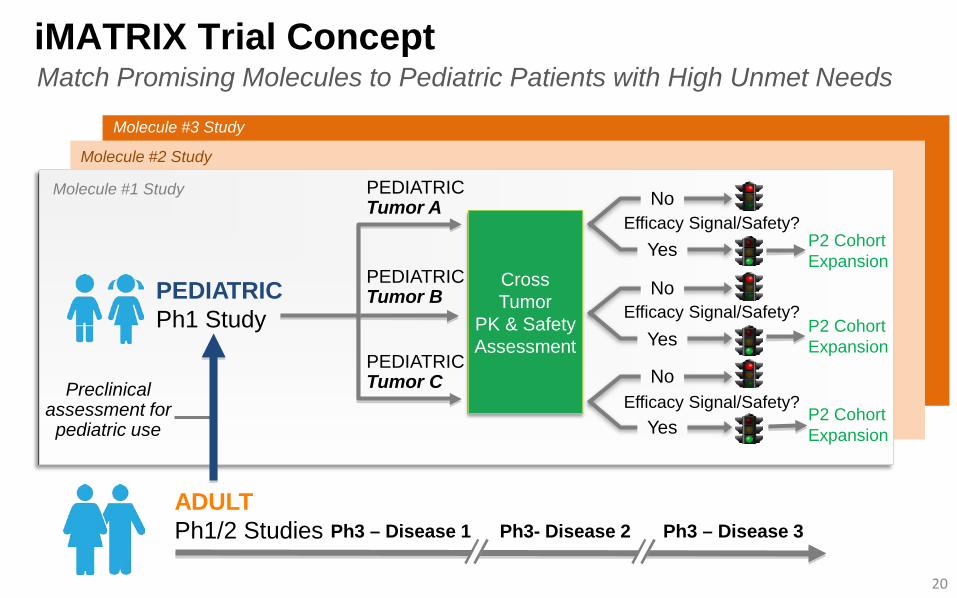
iMATRIX Trial Concept
20
Ph3 – Disease 1 ADULT Ph1/2 Studies Ph3- Disease 2 Ph3 – Disease 3
Preclinical
assessment for pediatric use
PEDIATRIC Tumor A
PEDIATRIC Tumor B
PEDIATRIC Tumor C
Efficacy Signal/Safety? P2 Cohort Expansion Yes
No
Efficacy Signal/Safety? P2 Cohort Expansion Yes
No
Efficacy Signal/Safety? P2 Cohort Expansion Yes
No
PEDIATRIC Ph1 Study
Molecule #1 Study
Molecule #2 Study
Molecule #3 Study
Cross Tumor
PK & Safety Assessment
Match Promising Molecules to Pediatric Patients with High Unmet Needs
Key Conclusions & Next Steps
21
• Atezolizumab is a humanized, monoclonal antibody which binds to PD-L1 to restore the anti-tumor immunity mediated by T cells
• Atezolizumab is well tolerated and demonstrates clinical efficacy across tumor types & subgroups in adults
• Voluntary pediatric study of atezolizumab is ongoing as part of our iMATRIX platform which matches promising molecules to pediatric patients with high unmet medical needs
- Rigorous and consistent PK, safety and efficacy assessment - Comprehensive biomarker evaluation - Strong collaboration with academic consortium and health
authorities

THANK YOU
22
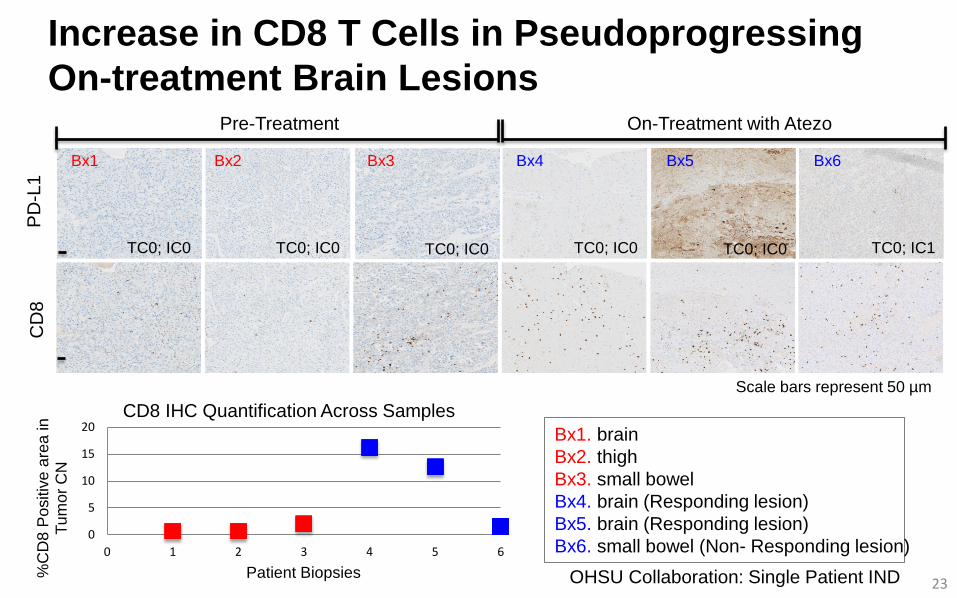
Increase in CD8 T Cells in Pseudoprogressing On-treatment Brain Lesions
Scale bars represent 50 µm
CD
8 P
D-L
1
TC0; IC0 TC0; IC0 TC0; IC0 TC0; IC0 TC0; IC0 TC0; IC1
Pre-Treatment On-Treatment with Atezo
Bx1 Bx2 Bx3 Bx4 Bx5 Bx6
0
5
10
15
20
0 1 2 3 4 5 6
%C
D8
Pos
itive
are
a in
Tu
mor
CN
Patient Biopsies
CD8 IHC Quantification Across Samples Bx1. brain Bx2. thigh Bx3. small bowel Bx4. brain (Responding lesion) Bx5. brain (Responding lesion) Bx6. small bowel (Non- Responding lesion)
OHSU Collaboration: Single Patient IND 23