attachments i & j updated as of 11/01/2010 june 1,2010
TRANSCRIPT
Attachments I & J Updated as of 11/01/2010

Policy: 03-522 DBHDD SUBJECT: Physical and Nutritional Supports
Page 2 of 17
2. To enable each individual to experience an optimal balance of quality of life, functional independence, and safety.
3. To meet the physical and nutritional needs of each individual with services delivered by trained and competent staff that consistently provide appropriate interventions which are aligned with assessed individualized needs and preferences.
4. To identify, in a timely manner, all individuals who are at risk for problems such as choking and aspiration, falls, and decubitus ulcers, and to provide appropriate interventions and safety measures to ensure optimal health and safety.
5. To ensure that each individual’s physical and nutritional status is reviewed and updated as clinically indicated and upon change in status due to functional improvement or decline based on focused assessments and interdisciplinary input at a program and/or facility level.
DEFINITIONS Aspiration: The entrance of liquids, foods, and/or secretions into the trachea and/or lungs. Asphyxia: Impaired breathing that causes a severely deficient oxygen supply. Choking: Any episode of airway obstruction by food or foreign object. Dysphagia: Difficulty swallowing. Dehydration: Inadequate intake to or loss of water from the body (e.g., due to diarrhea, vomiting, excessive urination). Complications can include seizures, constipation, urinary tract infection (UTI), and headaches. Obesity: A condition of having too much body fat, which can increase the risk of diabetes, heart disease, stroke, arthritis and some cancers. Obesity is usually associated with a Body Mass Index (BMI) over 30. Underweight: Low body mass, typically associated with a BMI less than 18, which can result in lowered immunity, loss of periods, bone loss, and/or malnutrition. Pica: Eating one or more nonnutritive substances on a persistent basis for a period of at least one month. Fall: An uncontrolled, unintentional, downward displacement of the body to the ground or other object, excluding falls resulting from violent blows, other purposeful actions, stroke, fainting or seizures. Decubitus Ulcer: An open wound associated with compromised circulation to the skin that may form due to several factors including prolonged pressure due to limited
Attachments I & J Updated as of 11/01/2010
Policy: 03-522 DBHDD SUBJECT: Physical and Nutritional Supports
Page 3 of 17
mobility, excessive moisture (e.g., due to incontinence), chronic conditions such as diabetes or peripheral vascular disease (PVD), and/or malnutrition. Decubitus ulcers often occur over bony prominences, and are staged from I (early) to IV (most severe). PROCEDURES A. Criteria for the Development and Implementation of a 24-Hour Support Plan.
Physical and nutritional support is initiated upon admission and continues throughout extended or long-term admissions. The development and implementation of a 24-Hour Support Plan should occur for all individuals who are either identified as high risk for choking, aspiration, falls, nutritional concerns, and/or decubitus ulcers, or who have a need for individualized supports to facilitate independence. 1. Screening is performed upon admission and during hospitalization, as clinically
indicated, in order to identify individuals at potential risk for physical and nutritional concerns that could lead to adverse health events who would benefit from risk assessment. Data gathered by risk assessments are used to assist in determining whether an individual meets the criteria to be included on pertinent facility high-risk list(s). Any individual determined to be at high risk for choking, aspiration, falls, or decubitus ulcers will require the provision of a 24-Hour Support Plan, unless the treatment team is able to provide and document clinical rationale, justification and/or supporting data as to why a 24-Hour Support Plan is not indicated. a. Screening, Assessment, and Evaluation of Choking and Aspiration Risk
i. The “Choking and Aspiration Risk” section of the Physical and Nutritional Support Risk Screen (Attachment A) is completed by a licensed nurse on admission for all individuals, and annually thereafter on all individuals who remain in the hospital who are NOT at high risk for choking and aspiration. This section of the Physical and Nutritional Support Risk Screen is repeated for individuals NOT at high risk anytime there is a related change in physical or functional status (including improvements or declines) that could affect the potential risk for choking and aspiration. This includes observation of possible signs and symptoms of choking, aspiration, and asphyxia, or identification of emerging risk factors. Subsequent to completing this section of the Risk Screen, the clinician who completed the screen will inform the other members of the treatment team of the screening results. If the individual is found to be at potential risk, the physician or advanced practice registered nurse (APRN) and unit charge nurse will be immediately notified. See Hospital Specific Details (Attachment K)
ii. If the “Choking and Aspiration Risk” section of the Physical and Nutritional
Support Risk Screen indicates the need for immediate intervention, a modified diet and medication texture should be immediately ordered by medical staff. In addition, the initial treatment plan should address
Attachments I & J Updated as of 11/01/2010
Policy: 03-522 DBHDD SUBJECT: Physical and Nutritional Supports
Page 4 of 17
positioning during meals, and mealtime supervision and assistance as required by the individual. These interventions will be implemented until full assessment and/or evaluation is completed. (See Details)
iii. The Choking and Aspiration Risk Assessment (Attachment B) is
performed for all individuals identified to be at potential risk through the Physical and Nutritional Support Risk Screen. The Choking and Aspiration Risk Assessment is repeated for individuals at high risk annually and anytime there is a related change in physical or functional status (including improvements or declines) that could affect the potential risk for choking and aspiration. The Choking and Aspiration Risk Assessment is performed by a trained and competent clinician within 24 hours of notification of potential risk by the nurse. Subsequent to completing the Risk Assessment, the clinician who completed the assessment will inform the other members of the treatment team of the assessment results. If the individual is found to be at high risk, the physician or APRN, unit charge nurse, and dietitian will be immediately notified. Attachment B- Instructions provides additional information about completion of the Choking and Aspiration Risk Assessment. (See Details)
iv. Evaluation of Choking and Aspiration Risk: If an individual is determined
to be at high risk, medical staff will order further evaluation and treatments as needed. Recommended assessments may include but are not limited to standardized swallowing assessments (e.g., Mini Nutritional Assessment, Mann’s Assessment of Swallowing), facility bedside swallowing evaluations, and diagnostic procedures such as Modified Barium Swallow study (MBS), Fiberoptic Endoscopic Evaluation of Swallowing (FEES), Upper Gastrointestinal series (UGI), and/or gastric emptying studies. On site evaluations are completed within 24 hours of notification, and scheduling of off-site evaluations utilizing diagnostic tests is completed within 24 hours of notification. (See Details)
b. Screening, Assessment and Evaluation of Fall Risk (See Details) i. The “Fall Risk” section of the Physical and Nutritional Support Risk Screen
is completed by a licensed nurse upon admission for all individuals, and annually thereafter on all individuals who remain in the hospital who are NOT at high risk for falls. This section of the Physical and Nutritional Support Risk Screen is repeated for individuals NOT at high risk anytime there is a related change in physical or functional status (including improvements or declines) that could affect the potential risk for falls. This includes observation of signs and symptoms of unsteady gait or identification of other emerging risk factors. Subsequent to completing this section of the Risk Screen, the clinician who completed the screen will
Attachments I & J Updated as of 11/01/2010

Policy: 03-522 DBHDD SUBJECT: Physical and Nutritional Supports
Page 5 of 17
inform the other members of the treatment team of the screening results. If the individual is found to be at potential risk, the physician or APRN and unit charge nurse will be immediately notified.
ii. If the “Fall Risk” section of the Physical and Nutritional Support Risk
Screen indicates the need for immediate intervention, fall precautions or related supports should be immediately implemented. This should include level of supervision and monitoring and assistance with use of assistive devices as required by the individual. These interventions will be implemented until full assessment and/or evaluation is completed.
iii. The Fall Risk Assessment (Attachment C) is performed for all
individuals identified to be at potential risk through the Physical and Nutritional Support Risk Screen. The Fall Risk Assessment is repeated for individuals at high risk annually and anytime there is a related change in physical or functional status (including improvements or declines) that could affect the potential risk for falls. The Fall Risk Assessment is performed by a trained and competent clinician within 24 hours of notification of potential risk by the nurse. Subsequent to completing the Risk Assessment, the clinician who completed the assessment will inform the other members of the treatment team of the assessment results. If the individual is found to be at high risk, the physician or APRN and unit charge nurse will be immediately notified. Attachment C – Instructions provides additional information about completion of the Fall Risk Assessment.
iv. Evaluation of Fall Risk: If an individual is determined to be at high risk,
medical staff will order further evaluation and treatments as needed. Recommended evaluations should include standardized tools (e.g., Tinetti, Berg balance test) when possible. On site evaluations are completed within 24 hours of notification, and scheduling of off-site evaluations utilizing diagnostic tests is completed within 24 hours of notification.
c. Screening, Assessment and Evaluation of Compromised Skin Integrity Risk (See Details) i. The “Decubitus Ulcer Risk” section of the Physical and Nutritional Support
Risk Screen is completed by a licensed nurse upon admission for all individuals, and annually thereafter on all individuals NOT at high risk for decubitus ulcer who remain in the hospital. This section of the Physical and Nutritional Support Risk Screen is repeated for individuals NOT at high risk anytime there is a related change in physical or functional status (including improvements or declines) that could affect the potential risk for compromised skin integrity. Subsequent to completing this section of the
Attachments I & J Updated as of 11/01/2010

Policy: 03-522 DBHDD SUBJECT: Physical and Nutritional Supports
Page 6 of 17
Risk Screen, the clinician who completed the screen will inform the other members of the treatment team of the screening results. If the individual is found to be at potential risk, the physician or APRN and unit charge nurse will be immediately notified.
ii. If the “Decubitus Ulcer Risk” section of the Physical and Nutritional Support Risk Screen indicates the need for immediate intervention, protective supports should be immediately implemented. This should include supports to address skin moisture, prevention of shear/friction, and positioning as required by the individual. These interventions will be implemented until full assessment and/or evaluation is completed.
iii. The Decubitus Ulcer Risk Assessment (Attachment D) is performed for
all individuals identified to be at potential risk through the Physical and Nutritional Support Risk Screen. The Decubitus Ulcer Risk Assessment is repeated for individuals at high risk annually and anytime there is a related change in physical or functional status (including improvements or declines) that could affect the potential risk for decubitus ulcer. The Decubitus Ulcer Risk Assessment is performed by a trained and competent clinician within 24 hours of notification of potential risk by the nurse. Subsequent to completing the Risk Assessment, the clinician who completed the assessment will inform the other members of the treatment team of the assessment results. If the individual is found to be at high risk, the physician or APRN and unit charge nurse will be immediately notified. Attachment D - Instructions provides additional information about completion of the Decubitus Ulcer Risk Assessment.
iv. Evaluation of Compromised Skin Integrity Risk: If an individual is
determined to be at high risk, medical staff should order further evaluation and treatments (e.g., OT and PT evaluation of seating system and alternate positioning schedule) as needed. On site evaluations are completed within 24 hours of notification.
2. Upon admission, annually, and as clinically indicated, treatment team and
discipline-specific assessments for occupational, physical and speech therapy are completed to identify individuals’ functional status, strengths, preferences, cultural background, and needs for assistance and support in order to engage in activities of daily living. Individuals who are determined to require assistance, supervision, and/or environmental modification within any area of daily living including self care, work, education, and leisure tasks to promote independence and opportunities for learning and engagement will require the provision of a 24-Hour Support Plan.
Attachments I & J Updated as of 11/01/2010

Policy: 03-522 DBHDD SUBJECT: Physical and Nutritional Supports
Page 7 of 17
B. Treatment Planning for Individuals who Require Physical and Nutritional Supports 1. The treatment team assesses any individual who meets criteria for a 24-Hour
Support Plan and implements objectives and interventions to minimize risks and promote optimum independence.
2. Individuals who require nutritional and physical support should have service objectives and interventions (e.g., 24-Hour Support Plan) as well as learning objectives and interventions, as clinically indicated.
Example 1: If an individual is determined to be at risk due to rapid eating, then the treatment team must implement appropriate objectives and interventions to minimize the risk associated with this behavior. This may include a 24-Hour Support Plan to indicate appropriate level of supervision, behavioral techniques, and adaptive equipment (e.g., small bowl spoon), as well as a concomitant learning objective to help the individual learn to eat at a safe pace. Example 2: If an individual requires a 24-Hour Support Plan due to limited independence with mobility, it should list adaptive equipment for mobility, level of function and assistance required, and transfer techniques, as well as a learning objective for improving independence with mobility.
C. Development and Implementation of the 24-Hour Support Plan 1. Nutritional and Physical Support General Guidelines (Attachments E and F)
provide instructions regarding procedures to promote safety, hygiene, and compassionate care and should be followed for all individuals. A 24-Hour Support Plan is developed when an individual requires specific and individualized supports that may extend beyond the scope of the general guidelines.
2. An individualized 24-Hour Support Plan is developed with and reviewed by staff
members who are involved in implementation. The plan shall be accessible to staff at all relevant times throughout the 24-hour day in order to serve as a reference to support accurate implementation of each person’s individualized supports.
3. Designated staff will be responsible for writing the 24-Hour Support Plan following assessment, diagnostic tests, interdisciplinary collaboration, and treatment team input. The plan should be written within 48 hours of notification or upon identification of need by risk or discipline specific assessment. (See Details)
Attachments I & J Updated as of 11/01/2010
Policy: 03-522 DBHDD SUBJECT: Physical and Nutritional Supports
Page 8 of 17
4. The treatment team will approve each plan prior to implementation upon development and/or revision. (See Details)
5. The 24-Hour Support Plan should be individualized and contain only the sections for each individual that are clinically meaningful, required, and indicated by assessed needs.
6. An individualized plan (see Attachment G for plan template) may include any combination of the sections listed below. Responsible disciplines should be determined by the hospital, in accordance with staffing, strengths, competency, and in consideration of scope of practice and Georgia practice acts. a. Mealtime
i. Specific triggers (e.g., recent history of aspiration pneumonia), ii. Target behaviors that increase risk of adverse mealtime event (e.g., food
snatching, pica), and strategies for addressing behaviors, iii. Therapeutic diet prescription, which include nutritional requirements and
allergies, as well as any noted individual food preferences or dislikes, iv. Diet texture and liquid consistency (see Attachment H for list of dysphagia
diets), v. Information regarding special hydration requirements and fluid restrictions, vi. Adaptive equipment, vii. Functional ability and level of assistance required, viii. Special procedures and techniques (e.g., chin tuck, augmentative
communication device to choose beverage, low vision strategies), ix. Type of supervision, and x. Picture of individual with mealtime positioning device and adaptive
equipment
b. Medication Administration i. Medication texture, liquid consistency, and method of presentation (e.g.,
crushed with pudding), ii. Techniques for presentation, and iii. Adaptive equipment (e.g., nosey cut out cup)
c. Oral Hygiene
i. Positioning for oral hygiene, ii. Special techniques (e.g., tongue cleaning, no mouthwash), and iii. Adaptive equipment (e.g., suction toothbrush)
d. Mobility and Transfers
i. Adaptive equipment and/or mobility device, ii. Functional ability and level of assistance and/or supervision, iii. Special techniques and procedures (e.g., visual orientation in mobility),
and
Attachments I & J Updated as of 11/01/2010
Policy: 03-522 DBHDD SUBJECT: Physical and Nutritional Supports
Page 9 of 17
iv. Picture of individual with device
e. Bed and/or Alternate Positioning i. Adaptive equipment and/or positioning device, ii. Special techniques and procedures, and iii. Picture of individual in alternate positioning
f. Bathing i. Functional ability, level of assistance and supervision, ii. Adaptive equipment, iii. Positioning, and iv. Special techniques
g. Dressing and Grooming
i. Functional ability, level of assistance and supervision, ii. Adaptive equipment, iii. Positioning, and iv. Special techniques
h. Work and/or Education
i. Adaptive equipment and ii. Environmental considerations
7. Required components of the 24-Hour Support Plan
a. All individuals at high risk for choking and aspiration must have mealtime, medication administration, and oral hygiene sections completed.
b. If an individual is determined to be at risk for aspiration of secretions (determined via treatment team and/or diagnostic tests), even if NPO, positioning for all activities of daily living, including dressing and bathing must be indicated in the 24-Hour Support Plan.
c. All individuals at risk for decubitus ulcers should have positioning and/or postural supports indicated for all relevant sections of the 24-Hour Support Plan. It should be noted that the individual’s positioning schedule should not determine his or her daily activities, but rather positions should promote activity engagement and support performance.
8. The location of each individual plan is immediately accessible including, but not limited to the dining area or wherever meals are taken, or with the individual during all activities of daily living. (See Details)
9. Special considerations regarding implementation of the 24-Hour Support Plan.
Attachments I & J Updated as of 11/01/2010

Policy: 03-522 DBHDD SUBJECT: Physical and Nutritional Supports
Page 10 of 17
a. Implementation of the 24-Hour Support Plan during visits with family, visitors, and/or significant others: i. Families, visitors, and significant others should be oriented to the
individual’s 24-Hour Support Plan, (See Details) ii. Foods or fluids brought by family, visitors, and significant others that may
not be appropriate for the individual must be cleared with medical staff before being served to the individual, and
iii. Family and significant others should receive training on the individual’s 24-Hour Support Plan prior to extended home visits.
b. The 24-Hour Support Plan should be implemented during hospital sponsored
off-campus activities in which food is involved. i. Staff scheduling the event should notify licensed nursing staff in advance
of the event to ensure any individuals participating in event have proper diets, whether prepared by the hospital or purchased in the community,
ii. Licensed nursing and Activity staff should coordinate such events and, if necessary, advise the medical staff and obtain orders for diet variance,
iii. Escorting staff should provide meals for individuals that incorporate all special needs, safety factors, and appropriate environment and hygiene,
iv. Any problems encountered should be reported to the nurse upon return to the unit, and
v. CPR /First Aid certified staff should be present at all off-campus activities.
c. Admission to an acute care facility: Upon admission of an individual to an acute care facility, the 24-Hour Support Plan should be included among the documents that accompany the individual during transfer.
D. Implications for dental procedures and routine oral care for individuals at high
risk for choking and aspiration 1. Routine Oral Care:
a. Proper oral care plays an important role in physical and nutritional support. Poor oral hygiene can contribute to aspiration of bacteria from the mouth and oropharynx which can lead to respiratory infections such as pneumonia.
b. When possible, standardized measures such as the revised Oral Assessment Guide should be utilized to determine health ratings of all oral areas.
c. For all individuals at high risk, oral hygiene supports should be assessed by
the speech therapist and/or dental providers, as well as other relevant treatment team members, to determine the safest and most effective procedures and techniques for teeth, tongue, and mouth cleaning. Recommendations are incorporated into the individual’s 24-Hour Support Plan.
Attachments I & J Updated as of 11/01/2010

Policy: 03-522 DBHDD SUBJECT: Physical and Nutritional Supports
Page 11 of 17
d. Accelerated dental hygiene care with quarterly cleaning and dental checks will be provided to individuals as clinically indicated.
2. Dental Procedures:
a. For all individuals identified to be at high risk for choking and aspiration, an alert is placed in the dental record addressing this risk, and an updated list of all high risk individuals is sent monthly to dental providers. The updated list will be sent by the Risk Manager and/or the Treatment Team leader.
b. Interventions utilized when providing dental services for individuals at high risk include the following: i. Individuals at high risk for aspiration should never be placed in the supine
position during dental procedures. If certain procedures necessary to ensure optimal oral health (e.g., procedures to the upper posterior teeth) require positioning which differs from the 45 degree guideline, individuals should be reclined no more than is necessary and for no longer than is necessary to complete the dental procedure,
ii. Caution should be exercised when using ultrasonic scalers due to the risk of aspiration of scaled material with the large amount of water required for the procedure, and
iii. Provision of adequate suctioning during dental procedures to prevent aspiration of bacteria.
E. Medication Administration for Individuals at High Risk for Choking and
Aspiration 1. For individuals at high risk for choking and aspiration, the rehabilitation
therapist(s) will recommend how each individual should receive her or his medication based on assessment and information from diagnostic tests, and/or collaboration with nursing.
2. The treatment team will review the recommendation, and the physician and/or pharmacist will review current medications to determine whether modifications may be made (e.g., if current meds are crushable when crushing is recommended; if a liquid medication may be thickened).
3. If a discrepancy is noted between recommendations for safe medication presentation and the physical and/or chemical properties of the medications, the treatment team members must develop alternate recommendations. Medication administration with revised recommendations should then be assessed by the speech therapist and nurse prior to implementation of the revised 24-Hour Support Plan and recorded in the Medication Administration Record (MAR).
4. An updated version of the 24-Hour Support Plan for each individual at high risk should be available in the MAR for nurse reference.
Attachments I & J Updated as of 11/01/2010

Policy: 03-522 DBHDD SUBJECT: Physical and Nutritional Supports
Page 12 of 17
F. Assessing and Monitoring Nutritional Status (See Details)
1. Nutritional Risk: The “Nutritional Risk” section of the Physical and Nutritional Support Risk Screen is completed by a licensed nurse on admission for all individuals, annually thereafter on all individuals who remain in the hospital, and anytime there is a related change in physical or functional status (including improvements or declines) that could result in potential nutritional risk. a. If an individual is found to be at potential nutritional risk, the physician or
APRN, unit charge nurse and dietitian are notified. The dietitian should complete a nutrition assessment within 24 hours of notification.
b. If the “Nutritional Risk” section of the Physical and Nutritional Support Risk Screen indicates the need for immediate intervention, medical staff will immediately order a special diet as clinically indicated. In addition, the initial treatment plan should address monitoring and supervision of intake as required by the individual. These interventions will be implemented until full assessment and/or evaluation is completed.
c. Subsequent to completing the nutrition assessment, the dietitian who
completed the assessment will inform the other members of the treatment team of the assessment results. If the individual is found to be at nutritional risk, the physician or APRN and unit charge nurse will be immediately notified.
2. The following formula and rating of Significant Weight Loss/Gain or Severe
Weight Loss/Gain will be used to assist in determining which individuals are at nutritional risk: % of body weight change = Previous Weight minus Current Weight divided by Previous Weight x 100
Interval Significant Loss/Gain Severe Loss/Gain 1 month 5% Greater than 5% 3 months 7.5% Greater than 7.5% 6 months 10% Greater than 10%
3. Height, weight, and waist circumference measurements should be taken
consistent with established hospital policy. Medical Staff must be notified immediately of weight loss or gain that falls outside of the established parameters for the specific individual, and/or if there is a unintentional significant or severe loss or gain from the previous month. It is the responsibility of the staff member that identifies the weight loss or gain to notify the unit charge nurse who will in turn notify the medical staff and dietitian.
4. Medical staff will refer individuals for evaluation by the Dietitian upon admission and as clinically indicated.
Attachments I & J Updated as of 11/01/2010
Policy: 03-522 DBHDD SUBJECT: Physical and Nutritional Supports
Page 13 of 17
5. Implementation of nutritional recommendations:
Appropriate nursing and dietary interventions, as determined by the treatment team, are to be implemented for each individual identified with nutritional needs and/or nutritional risk. For all individuals determined to be at high risk for choking and aspiration, the therapeutic diet prescription, as well as any food allergies, preferences and/or dislikes should be included on the 24-Hour Support Plan. Adequate hydration (48-64 ounces per day, unless otherwise ordered by Medical Staff) is provided for all individuals. Any special techniques for ensuring optimal hydration (e.g., fluid restrictions, behavioral techniques to encourage fluid consumption) should be included in the 24-Hour Support Plan.
6. Weights are reviewed and trended for any individual with a length of stay that exceeds three months. (See Details)
G. Providing Non-oral Nutrition, Hydration and/or Medication
1. Prior to tube placement, the treatment team must conduct a discussion by which the medical risks (e.g., site infection) and psychosocial risks (e.g., reduced social aspects of mealtime) of enteral nutrition are discussed. Informed consent should be obtained from individuals who have decision making capacity.
2. The treatment team should consider individual needs and develop appropriate interventions for the provision of non-oral nutrition, hydration, and medication administration. This includes not only the type and placement of the tube, but the schedule and rate of nutrition (e.g., bolus, continuous) that promote optimal function and safety.
3. Nutrition assessments and evaluations are requested, as needed, to ensure
nutrition and hydration needs are met.
4. For all individuals who receive nutrition, hydration, and/or medication through alternate methods, the treatment team must conduct a reassessment at least annually to determine if return to oral intake is possible, as well as to justify continued need for non-oral nourishment, hydration, and/or medication administration.
H. Review, Reassessment and Updating of the 24-Hour Support Plan 1. Each individual with a 24-Hour Support Plan should be reassessed at least
quarterly or as clinically indicated to ensure the 24-Hour Support Plan continues to meet the individual’s needs, and is being implemented as indicated. (See Details)
2. Each individual should be reassessed following any change in physical or
functional status (due to improvement or decline). Following reassessment, the
Attachments I & J Updated as of 11/01/2010

Policy: 03-522 DBHDD SUBJECT: Physical and Nutritional Supports
Page 14 of 17
24-Hour Support Plan should be updated accordingly to reflect changes in status (e.g., improvements in functional dining skills) and supports (e.g., liquid thickening due to increased swallow delay). (See Details)
3. Any updates to the diet order by the Dietitian should be communicated to the designated responsible clinician(s) via the treatment team process, email, fax, or phone, so that the 24-Hour Support Plan may be updated in a timely manner. (See Details)
4. Whenever possible, direct care staff input should be utilized in helping to determine appropriate addendums or changes to 24-Hour Support Plans. Direct care and support staff have unique and valuable expertise in many aspects of the individual’s care that can inform treatment decisions.
5. Revised dates should be listed on updated 24-Hour Support Plans.
6. Appropriate staff should receive person-specific training following significant changes to the 24-Hour Support Plan. The need for training following update will be determined by the responsible clinician. (See Details)
I. Training
1. Screening and Assessments All staff (Medical, Nursing, Rehabilitation Therapists, and Dietitians) will be trained to competency on the screening tools and assessments for which they are assigned responsibility.
2. New Employee Training
a. Nurses, Medical staff, Rehabilitation Therapists (OT, PT, SLP), Dietitians, Dentists, Psychologists, Behavior Specialists, QMRP’s (Team Leaders), and Social Workers will receive training regarding Physical and Nutritional Supports for professionals as part of New Employee Orientation.
b. Direct care staff and/or 24-Hour Support Plan end users, including HST’s, CNA’s, FST’s, Instructors, Activity staff, Dental assistants, Paraprofessionals, and Teachers will be trained to competency on concepts related to nutritional and physical support, choking, aspiration, fall and decubitus ulcer risk, nutritional and physical support general guidelines, handling and transfers, and the 24-Hour Support Plan.
3. Person Specific Training a. All direct care staff will be trained to competency by a qualified trainer (i.e.,
trained to competency on both Physical Nutritional Support training for professional staff and end user training materials) on 24-Hour Support Plans for the individuals they will be responsible for assisting prior to assisting these individuals. (See Details)
Attachments I & J Updated as of 11/01/2010

Policy: 03-522 DBHDD SUBJECT: Physical and Nutritional Supports
Page 15 of 17
b. Responsible staff should be trained on new plans prior to plan
implementation. (See Details)
c. All appropriate direct care and end user staff should be trained to competency following changes to plans if clinically indicated by the treatment team. (See Details)
d. For new employees, in vivo return demonstration is required for mealtimes,
assisted mobility, and transfers.
e. The Physical and/or Nutritional Support Plan monitoring form(s) may be used to assess person specific competency.
f. Failure to demonstrate in vivo competency results in referral for immediate didactic retraining and follow-up of in vivo return demonstration until competency is demonstrated to trainer. (See Details)
g. A staff member who does not achieve in vivo competency in assisting individuals with mealtimes, mobility, and/or transfers may not assist individuals with these activities. The Nurse Manager and/or Team Leader must be notified when a staff member does not achieve competency, so that the staff member is not assigned these duties prior to passing the appropriate person specific training tasks. (See Details)
4. Additional training pertaining to areas of the 24-Hour Support Plan training may occur in a group or individualized basis as a result of need identified through the monitoring process, a departmental performance improvement process, or as a corrective action identified through third level facility risk management review.
J. Monitoring and Performance Improvement
1. In vivo monitoring of the 24-Hour Support Plan is completed as follows: a. Monitoring of the 24-Hour Support Plan should be performed at least
quarterly and may be done in conjunction with the 24-Hour Support Plan quarterly reassessment. Monitoring of physical and/or nutritional supports is performed using a standard form. See Attachment I - 24-Hour Support Plan Monitoring Template and Instructions for Nutritional Support. See Attachment J - 24-Hour Support Plan Monitoring Template and Instructions for Physical Support.
b. Sections of the 24-Hour Support Plan to be monitored should include but are
not limited to the mealtime section, mobility section, and any physical support sections for which the individual has an active learning based objective.
Attachments I & J Updated as of 11/01/2010

Policy: 03-522 DBHDD SUBJECT: Physical and Nutritional Supports
Page 16 of 17
c. Monitoring of 24-Hour Support Plans for individuals at mealtimes is performed by staff who have been trained on the 24-Hour Support Plan Monitoring process (i.e., trained to competency on both Physical Nutritional Support training for professional staff and end user training materials) and/or have shown adequate inter-rater agreement. Monitoring should be done in an interactive mealtime observation format. This involves active collaborative assistance by the monitor in the appropriate setting (e.g., dining area) in conjunction with the monitoring of identified plans and documentation of monitoring results. This interactive method creates opportunities for incidental teaching and training, and reduces artifacts of observation in staff performance that tend to occur during a more traditional formal monitoring process.
d. Opportunities for individual performance improvement are identified and addressed at the time of monitoring. If any interaction or action demonstrated during the monitoring is putting an individual at risk, the person conducting the monitoring will intervene in order to ameliorate risk. Any staff member who has been observed to demonstrate an action that has put an individual at risk will be retrained and required to demonstrate competency with person-specific training on the relevant section(s) of the individual’s 24-Hour Support Plan.
e. Systemic opportunities for improvement are identified by trending of aggregate monitoring data. Data should be drilled down (e.g., by shift, unit) and analyzed and reviewed quarterly by facility management, with identified trends tracked and addressed through performance improvement plans.
f. Significant trends in monitoring data that identify general training needs should be utilized to provide input to and inform New Employee Orientation staff training materials.
2. Monitoring of 24-Hour Support Plan components during medication administration and provision of enteral nutrition is completed as follows: The Medication Administration and Enteral Nutrition Observation tools will contain components to assess whether individuals are receiving optimal nutritional and physical supports. Inter-rater agreement may be established between nurses and designated clinicians for these specific components prior to observation implementation.
K. Discontinuation of the 24-Hour Support Plan
The 24-Hour Support Plan shall be discontinued once an individual no longer meets criteria for the provision of a 24-Hour Support Plan.
Attachments I & J Updated as of 11/01/2010

Policy: 03-522 DBHDD Physical and Nutritional Supports
Page 17 of 17 SUBJECT:
L. Dignity of Risk 1. Protection from harm is the clinical goal of providing adequate nutritional and
physical support. Ethical conflicts may arise when an individual or an individual’s guardian or surrogate does not choose to accept the implementation of treatment intervention recommendations.
2. Treatment team review at the program and facility level must be performed for all
individuals with advance directives that are in conflict with treatment team recommendations (e.g., tube placement), and for individuals (or guardians) who elect the withholding or withdrawal of recommended treatments.
3. Reviews may involve planning to provide comprehensive education and informed consent regarding treatment recommendation benefit and risk, as well as the exploration of alternative options to treatment recommendations (e.g., enteral nutrition with pleasure feeding, time-limited trial of recommended intervention).
Attachments I & J Updated as of 11/01/2010

DBHDD Policy: Physical and Nutritional Supports Page 1 of 4
Physical and Nutritional Support Risk Screen
__________________________________________________________________________________________________________
Complete all sections of the Risk Screen (A, B, C, and D) upon admission. Complete sections A, B, and C annually and upon change in status unless the individual is already determined to be at high risk in that area (in which case the appropriate Risk Assessment will be completed instead). Complete section D annually and upon change in status. Mark the “Not applicable” box only if completion of a specific section is not presently indicated. Otherwise, mark “Yes” (Y), “No” (N), or “Unknown” (U) for all risk factors in each section; do not leave any blanks. Use several sources of information, including individual and family/significant other report, other hospital staff, and current and past medical records. Mark “Unknown” only if unable to find information from any available source. Make notifications if the individual is determined to be at potential risk, and document as indicated below each section. A. Choking and Aspiration Risk Not applicable Mark Y (Yes), N (No), or U (Unknown) for each of the following risk factors: (Any) history of aspiration pneumonia Y N U History of choking incident (within the past five years) Y N U History of stroke (within the past year only) Y N U Current dysphagia diagnosis Y N U Drooling with difficulty managing secretions Y N U Edentulous or acute dental issues which may impact chewing Y N U Difficulty swallowing or chewing Y N U Altered level of consciousness Y N U Dysphasia/slurred speech Y N U Currently receives non-oral nutrition, medication, and/or hydration Y N U __________________________________________ ____________ ____________ Signature/title of person completing screen Date Time Is one or more risk factor above marked “yes”? Y (potential risk) N If yes, Choking and Aspiration Risk Assessment is indicated. If yes, immediately notify Physician/APRN and Unit Charge Nurse and document below: __________________________________________ ____________ ____________ Name/title of Physician/APRN notified Date Time __________________________________________ ____________ ____________ Name/title of Unit Charge Nurse notified Date Time __________________________________________ ____________ ____________ Name/title of other staff notified (if applicable) Date Time Stamp Plate
Policy 03-522 Attachment A Version 3-10-2010
DBHDD Policy: Physical and Nutritional Supports Page 2 of 4
Physical and Nutritional Support Risk Screen
__________________________________________________________________________________________________________
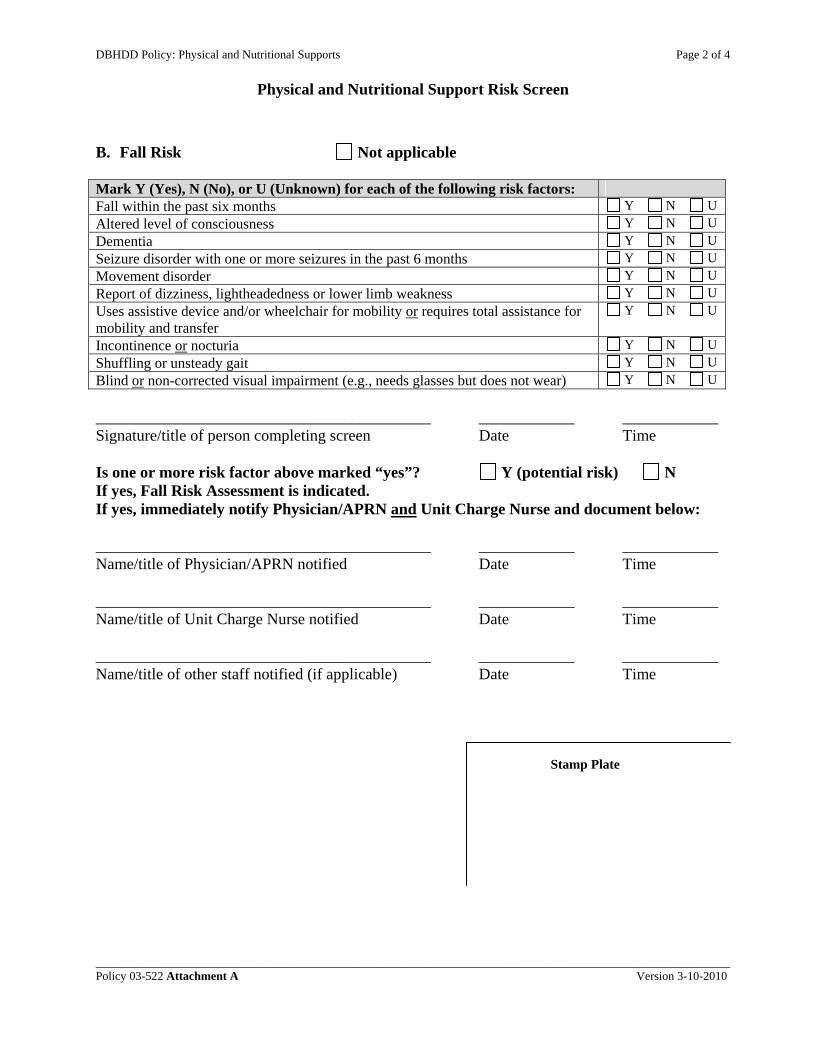
B. Fall Risk Not applicable
Mark Y (Yes), N (No), or U (Unknown) for each of the following risk factors: Fall within the past six months Y N U Altered level of consciousness Y N U Dementia Y N U Seizure disorder with one or more seizures in the past 6 months Y N U Movement disorder Y N U Report of dizziness, lightheadedness or lower limb weakness Y N U Uses assistive device and/or wheelchair for mobility or requires total assistance for mobility and transfer
Y N U
Incontinence or nocturia Y N U Shuffling or unsteady gait Y N U Blind or non-corrected visual impairment (e.g., needs glasses but does not wear) Y N U __________________________________________ ____________ ____________ Signature/title of person completing screen Date Time Is one or more risk factor above marked “yes”? Y (potential risk) N If yes, Fall Risk Assessment is indicated. If yes, immediately notify Physician/APRN and Unit Charge Nurse and document below: __________________________________________ ____________ ____________ Name/title of Physician/APRN notified Date Time __________________________________________ ____________ ____________ Name/title of Unit Charge Nurse notified Date Time __________________________________________ ____________ ____________ Name/title of other staff notified (if applicable) Date Time Stamp Plate
Policy 03-522 Attachment A Version 3-10-2010

DBHDD Policy: Physical and Nutritional Supports Page 3 of 4
Physical and Nutritional Support Risk Screen
__________________________________________________________________________________________________________
C. Decubitus Ulcer Risk Not applicable
Mark Y (Yes), N (No), or U (Unknown) for each of the following risk factors: Confined to bed Y N U Requires use of a wheelchair for mobility Y N U (Any) history of a pressure ulcer Y N U Observation of reddened areas over bony prominences Y N U Incontinence Y N U __________________________________________ ____________ ____________ Signature/title of person completing screen Date Time Is one or more risk factor above marked “yes”? Y (potential risk) N If yes, Decubitus Ulcer Risk Assessment is indicated. If yes, immediately notify Physician/APRN and Unit Charge Nurse and document below: __________________________________________ ____________ ____________ Name/title of Physician/APRN notified Date Time __________________________________________ ____________ ____________ Name/title of Unit Charge Nurse notified Date Time __________________________________________ ____________ ____________ Name/title of other staff notified (if applicable) Date Time Stamp Plate
Policy 03-522 Attachment A Version 3-10-2010

DBHDD Policy: Physical and Nutritional Supports Page 4 of 4
Physical and Nutritional Support Risk Screen
__________________________________________________________________________________________________________ Policy 03-522 Attachment A Version 3-10-2010
D. Nutritional Risk Not applicable Mark Y (Yes), N (No), or U (Unknown) for each of the following risk factors: Diabetes mellitus (new onset or insulin-requiring) or diabetes insipidus Y N U Anorexia or bulimia Y N U Current decubitus ulcer or non-healing wound Y N U Receives dialysis Y N U Severe or multiple food allergies (e.g., rash, difficulty breathing) Y N U Unintentional weight loss/gain of 10 pounds or more in the past month Y N U Receives non-oral nutrition, hydration, and/or medication Y N U Recent unexplained decrease in food/fluid intake Y N U Excessive water intake Y N U Pregnant or lactating Y N U Hallucinations and/or delusions that impact nutritional status (e.g., thinks food is being poisoned; hears voices saying not to eat)
Y N U
__________________________________________ ____________ ____________ Signature/title of person completing screen Date Time Is one or more risk factor above marked “yes”? Y (potential risk) N If yes, Nutrition Assessment is indicated. If yes, immediately notify Physician/APRN, Unit Charge Nurse, and Dietitian and document below: __________________________________________ ____________ ____________ Name/title of Physician/APRN notified Date Time __________________________________________ ____________ ____________ Name/title of Unit Charge Nurse notified Date Time __________________________________________ ____________ ____________ Name/title of Dietitian notified Date Time __________________________________________ ____________ ____________ Name/title of other staff notified (if applicable) Date Time
Stamp Plate

DBHDD Policy: Physical and Nutritional Page 1 of 3
Choking and Aspiration Risk Assessment
______________________________________________________________________________________________________________________ Policy 03-522 Attachment B Version 5-17-2010
DATE DATE DATE DATE
A. Recent Conditions (within the past 6 months): Score (Y/N) Score (Y/N) Score (Y/N) Score (Y/N) *CVA *Traumatic Brain Injury (TBI) *Aspiration Pneumonia *Choking Incident *Evidence of aspiration on diagnostic test (e.g., MBS, FEES) *Intubation or tracheostomy *Head or neck surgery *Chemotherapy and/or radiation to head or neck *Acute Heart Failure *Current Dysphagia diagnosis (within or prior to the past six months) *Receiving non-oral nutrition, hydration and/or medication (within or prior to the past six months)
Total # of Yes responses-Section A B. Current Medical Conditions and/or Treatments: Score (Y/N) Score (Y/N) Score (Y/N) Score (Y/N)
Parkinson’s Disease Developmental Disability Tardive Dyskinesia Tardive Akathesia Multiple Sclerosis Cerebral Palsy Huntington’s Disease Degenerative Neurologic Disease Polyneuropathy Other Movement Disorders Seizure disorder Esophageal stricture Esophageal dysmotility Gastro-esophageal reflux (GERD) COPD, or other chronic respiratory disease Congestive heart failure Dementia, altered level of consciousness Receiving neuroleptic medications Edentulous and/or missing teeth Receiving medications which may cause CNS depression (anticonvulsants, anti-anxiety, antispasmodics, antidepressants)
Receiving medications which may cause dry mouth (antidepressants, antispasmodics, antihypertensives, anticholinergics, antihistamines, bronchodilators, sedatives, muscle relaxants, antineoplastic, anti-Parkinsonism, anticonvulsants, narcotics, antianxiety)
Receiving medications which may cause increased saliva (Anticholinesterase, clonazepam, clozapine)
Receiving medications which may cause immunosuppression (antibiotics, cytotoxic agents)
Receiving medications which may cause neuromuscular junction blockage (aminoglycoside antibiotics, botulinum)
Receiving medications which may cause myopathy (corticosteroids, lipid-lowering agents, colchicine, L-tryptophan)
Receiving medications which may cause reduction in esophageal sphincter tone (antihistamines, diuretics, opiates, ipratroprium bromide, alpha andranergic blocking agents, antihypertensives, anticholinergics)
Stamp Plate
DBHDD Policy: Physical and Nutritional Page 2 of 3
Choking and Aspiration Risk Assessment
______________________________________________________________________________________________________________________ Policy 03-522 Attachment B Version 5-17-2010
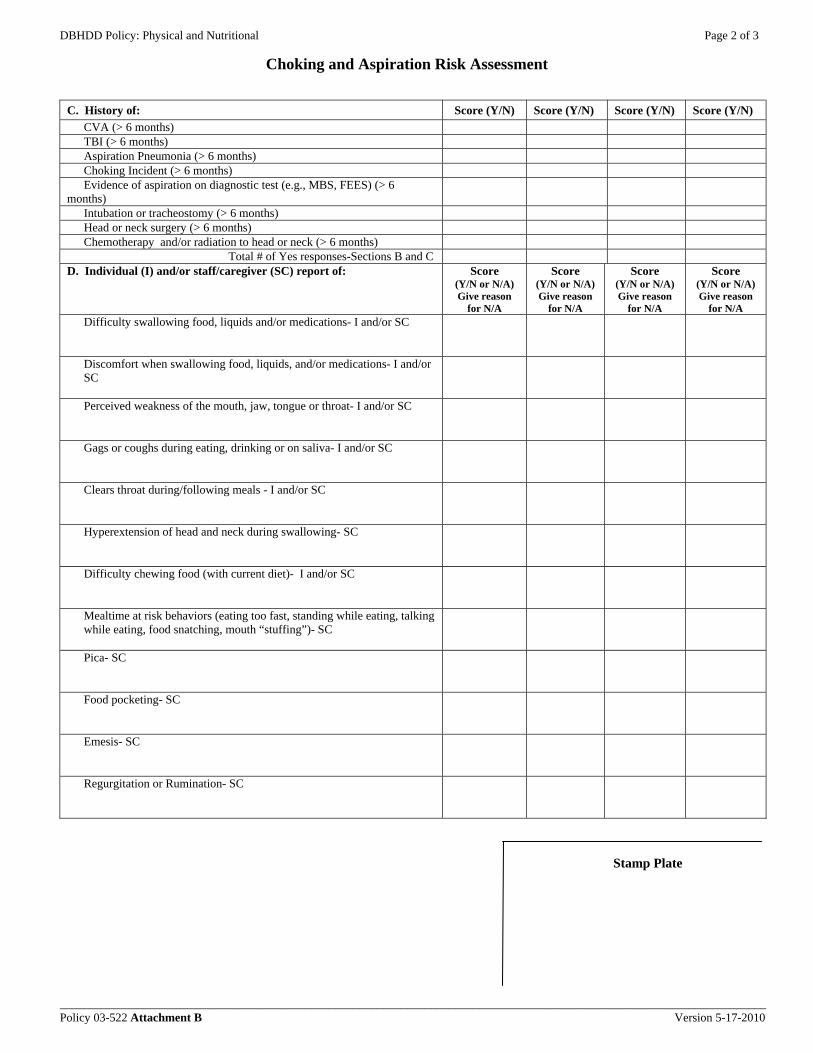
C. History of: Score (Y/N) Score (Y/N) Score (Y/N) Score (Y/N) CVA (> 6 months) TBI (> 6 months) Aspiration Pneumonia (> 6 months) Choking Incident (> 6 months) Evidence of aspiration on diagnostic test (e.g., MBS, FEES) (> 6
months)
Intubation or tracheostomy (> 6 months) Head or neck surgery (> 6 months) Chemotherapy and/or radiation to head or neck (> 6 months)
Total # of Yes responses-Sections B and C D. Individual (I) and/or staff/caregiver (SC) report of: Score
(Y/N or N/A) Give reason
for N/A
Score (Y/N or N/A) Give reason
for N/A
Score (Y/N or N/A) Give reason
for N/A
Score (Y/N or N/A) Give reason
for N/A Difficulty swallowing food, liquids and/or medications- I and/or SC
Discomfort when swallowing food, liquids, and/or medications- I and/or SC
Perceived weakness of the mouth, jaw, tongue or throat- I and/or SC
Gags or coughs during eating, drinking or on saliva- I and/or SC
Clears throat during/following meals - I and/or SC
Hyperextension of head and neck during swallowing- SC
Difficulty chewing food (with current diet)- I and/or SC
Mealtime at risk behaviors (eating too fast, standing while eating, talking while eating, food snatching, mouth “stuffing”)- SC
Pica- SC
Food pocketing- SC
Emesis- SC
Regurgitation or Rumination- SC
Stamp Plate

DBHDD Policy: Physical and Nutritional Page 3 of 3
Choking and Aspiration Risk Assessment
______________________________________________________________________________________________________________________ Policy 03-522 Attachment B Version 5-17-2010
E. Clinical Observation of: Score (Y/N) Score (Y/N) Score (Y/N) Score (Y/N) *Dysarthria (speech is slurred or hard to understand) *Wet voice *Altered level of alertness *Poor postural control and alignment (score as “no” if individual has adequate postural alignment and control with adaptive device and is independent with device)
*Respiratory rate greater than 30 breaths/minute Increased and persistent drooling Extrapyramidal symptoms including involuntary lip, tongue, and/or jaw movements
Delayed swallow Apraxic (poorly coordinated) swallow Hyperextension of head and neck during swallowing Reduced laryngeal elevation Total # of Yes responses-Sections D and E
F. *3 Oz. Water Test *If individual has any conditions listed in section A or if any of the asterisked items in section E are scored as “Yes”, the 3 ounce water test should NOT be performed.
Pass/Fail/ N/A
Give reason for N/A
Pass/Fail/ N/A
Give reason for N/A
Pass/Fail/ N/A
Give reason for N/A
Pass/Fail/ N/A
Give reason for N/A
Signs or symptoms of dysphagia during 3 oz water test
Desaturation during 3 oz water test possibly indicative of silent aspiration > 2% desaturation If baseline reading is below 90%, do not perform 3 ounce water test.
Baseline reading:
_________
Follow-up reading:
__________
Desaturation: __________
Baseline reading:
_________
Follow-up reading:
__________
Desaturation: __________
Baseline reading:
_________
Follow-up reading:
__________
Desaturation: __________
Baseline reading:
_________
Follow-up reading:
__________
Desaturation: __________
Scoring: Answer the following three questions. If you answer “yes” to at least one question, the individual is at high risk for choking and aspiration.
DATE
DATE
DATE
DATE
Is there at least one item in section A scored as a “yes” response?
__Yes (high risk) __ No
__Yes (high risk) __ No
__Yes (high risk) __ No
__Yes (high risk) __ No
Did the individual fail the 3 oz. water test? __Yes (high risk) __ No __ N/A
__Yes (high risk) __ No __ N/A
__Yes (high risk) __ No __ N/A
__Yes (high risk) __ No __ N/A
Is there at least one item in Section B or C scored as a “yes” response AND at least one item in Section D or E scored as a “yes” response?
__Yes (high risk) __ No
__Yes (high risk) __ No
__Yes (high risk) __ No
__Yes (high risk) __ No
SIGNATURE: DATE: _____________________________________________ ________ Stamp Plate
_____________________________________________ ________
_____________________________________________ ________
_____________________________________________ ________
DBHDD Policy: Physical and Nutritional Supports Page 1 of 4
Instructions: Choking and Aspiration Risk Assessment
__________________________________________________________________________________________________________________ Policy 03-522 Attachment B - Instructions Version 5-17-10
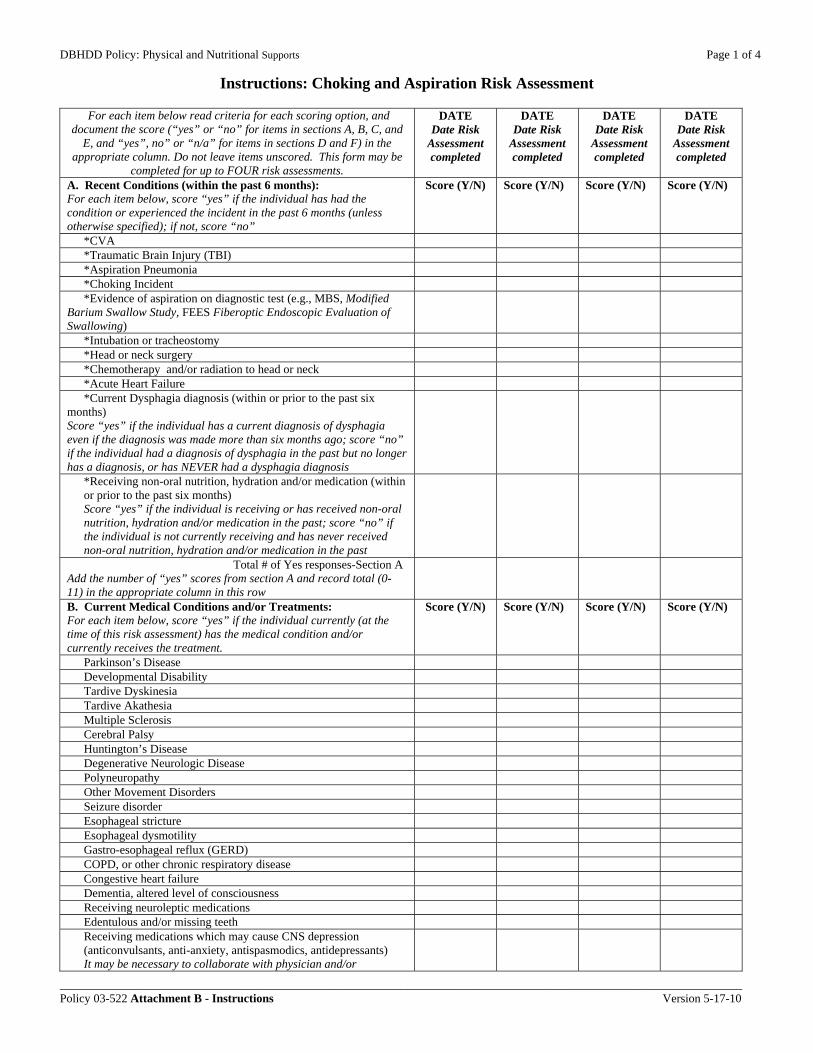
For each item below read criteria for each scoring option, and document the score (“yes” or “no” for items in sections A, B, C, and
E, and “yes”, no” or “n/a” for items in sections D and F) in the appropriate column. Do not leave items unscored. This form may be
completed for up to FOUR risk assessments.
DATE Date Risk
Assessment completed
DATE Date Risk
Assessment completed
DATE Date Risk
Assessment completed
DATE Date Risk
Assessment completed
A. Recent Conditions (within the past 6 months): For each item below, score “yes” if the individual has had the condition or experienced the incident in the past 6 months (unless otherwise specified); if not, score “no”
Score (Y/N) Score (Y/N) Score (Y/N) Score (Y/N)
*CVA *Traumatic Brain Injury (TBI) *Aspiration Pneumonia *Choking Incident *Evidence of aspiration on diagnostic test (e.g., MBS, Modified
Barium Swallow Study, FEES Fiberoptic Endoscopic Evaluation of Swallowing)
*Intubation or tracheostomy *Head or neck surgery *Chemotherapy and/or radiation to head or neck *Acute Heart Failure *Current Dysphagia diagnosis (within or prior to the past six
months) Score “yes” if the individual has a current diagnosis of dysphagia even if the diagnosis was made more than six months ago; score “no” if the individual had a diagnosis of dysphagia in the past but no longer has a diagnosis, or has NEVER had a dysphagia diagnosis
*Receiving non-oral nutrition, hydration and/or medication (within or prior to the past six months) Score “yes” if the individual is receiving or has received non-oral nutrition, hydration and/or medication in the past; score “no” if the individual is not currently receiving and has never received non-oral nutrition, hydration and/or medication in the past
Total # of Yes responses-Section A Add the number of “yes” scores from section A and record total (0-11) in the appropriate column in this row
B. Current Medical Conditions and/or Treatments: For each item below, score “yes” if the individual currently (at the time of this risk assessment) has the medical condition and/or currently receives the treatment.
Score (Y/N) Score (Y/N) Score (Y/N) Score (Y/N)
Parkinson’s Disease Developmental Disability Tardive Dyskinesia Tardive Akathesia Multiple Sclerosis Cerebral Palsy Huntington’s Disease Degenerative Neurologic Disease Polyneuropathy Other Movement Disorders Seizure disorder Esophageal stricture Esophageal dysmotility Gastro-esophageal reflux (GERD) COPD, or other chronic respiratory disease Congestive heart failure Dementia, altered level of consciousness Receiving neuroleptic medications Edentulous and/or missing teeth Receiving medications which may cause CNS depression (anticonvulsants, anti-anxiety, antispasmodics, antidepressants) It may be necessary to collaborate with physician and/or

DBHDD Policy: Physical and Nutritional Supports Page 2 of 4
Instructions: Choking and Aspiration Risk Assessment
__________________________________________________________________________________________________________________ Policy 03-522 Attachment B - Instructions Version 5-17-10
pharmacist for these medication indicators Receiving medications which may cause dry mouth (antidepressants, antispasmodics, antihypertensives, anticholinergics, antihistamines, bronchodilators, sedatives, muscle relaxants, antineoplastic, anti-Parkinsonism, anticonvulsants, narcotics, antianxiety) It may be necessary to collaborate with physician and/or pharmacist for these medication indicators
Receiving medications which may cause increased saliva (Anticholinesterase, clonazepam, clozapine) It may be necessary to collaborate with physician and/or pharmacist for these medication indicators
Receiving medications which may cause immunosuppression (antibiotics, cytotoxic agents) It may be necessary to collaborate with physician and/or pharmacist for these medication indicators
Receiving medications which may cause neuromuscular junction blockage (aminoglycoside antibiotics, botulinum) It may be necessary to collaborate with physician and/or pharmacist for these medication indicators
Receiving medications which may cause myopathy (corticosteroids, lipid-lowering agents, colchicine, L-tryptophan) It may be necessary to collaborate with physician and/or pharmacist for these medication indicators
Receiving medications which may cause reduction in esophageal sphincter tone (antihistamines, diuretics, opiates, ipratroprium bromide, alpha andranergic blocking agents, antihypertensives, anticholinergics) It may be necessary to collaborate with physician and/or pharmacist for these medication indicators
C. History of: For each item below, score “yes” if the individual has had the condition or experienced the incident more than 6 months ago; if not, score “no”.
Score (Y/N) Score (Y/N) Score (Y/N) Score (Y/N)
CVA (> 6 months) TBI (> 6 months) Aspiration Pneumonia (> 6 months) Choking Incident (> 6 months) Evidence of aspiration on diagnostic test (e.g., MBS, FEES) (> 6
months)
Intubation or tracheostomy (> 6 months) Head or neck surgery (> 6 months) Chemotherapy and/or radiation to head or neck (> 6 months)
Total # of Yes responses-Sections B and C Add the number of “yes” scores from sections B and C and record total (0-34) in the appropriate column in this row
D. Individual (I) and/or staff/caregiver (SC) report of: Ask the individual and/or caregiver questions about each of the following items in order to determine whether these factors are present. For each item, score “yes” if the factor is present, and score “no” if it is not. If the individual is unable to answer and the caregiver is not available or does not know an answer, score as “N/A”, and document the reason why N/A response was scored.
Score (Y/N or N/A) Give reason
for N/A
Score (Y/N or N/A) Give reason
for N/A
Score (Y/N or N/A) Give reason
for N/A
Score (Y/N or N/A) Give reason
for N/A
Difficulty swallowing food, liquids and/or medications- I and/or SC
Discomfort when swallowing food, liquids, and/or medications- I and/or SC
Perceived weakness of the mouth, jaw, tongue or throat- I and/or SC
Gags or coughs during eating, drinking or on saliva- I and/or SC Clears throat during/following meals - I and/or SC

DBHDD Policy: Physical and Nutritional Supports Page 3 of 4
Instructions: Choking and Aspiration Risk Assessment
__________________________________________________________________________________________________________________ Policy 03-522 Attachment B - Instructions Version 5-17-10
Hyperextension of head and neck during swallowing- SC Difficulty chewing food (with current diet)- I and/or SC Mealtime at risk behaviors (eating too fast, standing while eating, talking while eating, food snatching, mouth “stuffing”)- SC
Pica- SC Food pocketing- SC Emesis- SC Regurgitation or Rumination- SC
E. Clinical Observation of: For each item below, score “yes” if observed during the risk assessment, otherwise, score “no”
Score (Y/N) Score (Y/N) Score (Y/N) Score (Y/N)
*Dysarthria (speech is slurred or hard to understand) *Wet voice *Altered level of alertness *Poor postural control and alignment (score as “no” if individual has adequate postural alignment and control with adaptive device and is independent with device)
*Respiratory rate greater than 30 breaths/minute Increased and persistent drooling Extrapyramidal symptoms including involuntary lip, tongue, and/or jaw movements
Delayed swallow (may assess during the 3 ounce water test) Apraxic (poorly coordinated) swallow (may assess during the 3 ounce water test)
Hyperextension of head and neck during swallowing (may assess during the 3 ounce water test)
Reduced laryngeal elevation (Score “no” if the hyoid bone moves up and then down during swallowing; score as “yes” if there is no visible up and down movement of the hyoid bone. May assess during the 3 ounce water test)
Total # of Yes responses-Sections D and E Add the number of “yes” scores from sections D and E and record the total (0-23) in the appropriate column in this row
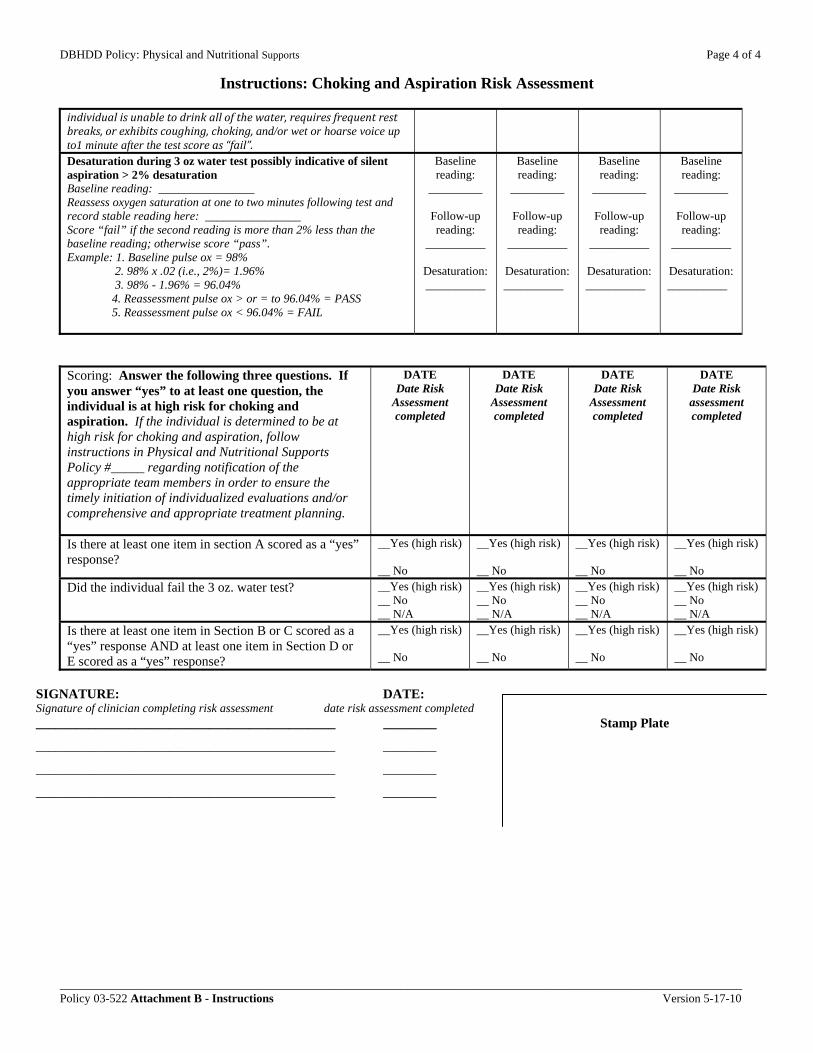
F. *3 Oz. Water Test If individual has any conditions listed in section A, or if any of the asterisked items in section E. are scored as “Yes”, the 3 oz. water test should not be performed. If any asterisked items on this assessment are scored as “yes”, do not perform this test, and mark “N/A” for all boxes in section F. In addition, score N/A if the individual is unable to follow directions for the test due to cognitive and/or communication difficulties. Document the reason why N/A response was scored in each applicable box. If either of the two items in section F. is scored as “fail”, the individual fails the 3 ounce water test and should be considered at high risk for choking and aspiration. Place pulse oximeter probe on the individual’s index finger. Assess O2 saturation prior to test. Record stable baseline reading. If baseline reading is below 90%, do not perform 3 ounce water test. Give the individual 3 ounces of water and ask the individual to drink from a cup or straw without stopping if they can.
Pass/Fail/ N/A
Give reason for N/A
Pass/Fail/ N/A
Give reason for N/A
Pass/Fail/ N/A
Give reason for N/A
Pass/Fail/ N/A
Give reason for N/A
Signs or symptoms of dysphagia during 3 oz water test Score “pass” if the individual is able to drink the entire amount without pausing to rest, coughing or choking, and does not exhibit wet or hoarse vocal quality for up to 1 minute following the test. If the
DBHDD Policy: Physical and Nutritional Supports Page 4 of 4
Instructions: Choking and Aspiration Risk Assessment
__________________________________________________________________________________________________________________ Policy 03-522 Attachment B - Instructions Version 5-17-10
individual is unable to drink all of the water, requires frequent rest breaks, or exhibits coughing, choking, and/or wet or hoarse voice up to1 minute after the test score as “fail”. Desaturation during 3 oz water test possibly indicative of silent aspiration > 2% desaturation Baseline reading: ________________ Reassess oxygen saturation at one to two minutes following test and record stable reading here: ________________ Score “fail” if the second reading is more than 2% less than the baseline reading; otherwise score “pass”. Example: 1. Baseline pulse ox = 98% 2. 98% x .02 (i.e., 2%)= 1.96% 3. 98% - 1.96% = 96.04% 4. Reassessment pulse ox > or = to 96.04% = PASS 5. Reassessment pulse ox < 96.04% = FAIL
Baseline reading:
_________
Follow-up reading:
__________
Desaturation: __________
Baseline reading:
_________
Follow-up reading:
__________
Desaturation: __________
Baseline reading:
_________
Follow-up reading:
__________
Desaturation: __________
Baseline reading:
_________
Follow-up reading:
__________
Desaturation: __________
Scoring: Answer the following three questions. If you answer “yes” to at least one question, the individual is at high risk for choking and aspiration. If the individual is determined to be at high risk for choking and aspiration, follow instructions in Physical and Nutritional Supports Policy #_____ regarding notification of the appropriate team members in order to ensure the timely initiation of individualized evaluations and/or comprehensive and appropriate treatment planning.
DATE Date Risk
Assessment completed
DATE Date Risk
Assessment completed
DATE Date Risk
Assessment completed
DATE Date Risk
assessment completed
Is there at least one item in section A scored as a “yes” response?
__Yes (high risk) __ No
__Yes (high risk) __ No
__Yes (high risk) __ No
__Yes (high risk) __ No
Did the individual fail the 3 oz. water test? __Yes (high risk) __ No __ N/A
__Yes (high risk) __ No __ N/A
__Yes (high risk) __ No __ N/A
__Yes (high risk) __ No __ N/A
Is there at least one item in Section B or C scored as a “yes” response AND at least one item in Section D or E scored as a “yes” response?
__Yes (high risk) __ No
__Yes (high risk) __ No
__Yes (high risk) __ No
__Yes (high risk) __ No
SIGNATURE: DATE: Signature of clinician completing risk assessment date risk assessment completed _____________________________________________ ________ Stamp Plate
_____________________________________________ ________
_____________________________________________ ________
_____________________________________________ ________

DBHDD Policy: Physical and Nutritional Supports Page 1 of 3 Fall Risk Assessment
________________________________________________________________________________________________________________________________ Policy 03-522 Attachment C Version 5-17-2010
Score 0
Score 1
Score 2
Score 3
Date:
Score (0-3/N/A)
A. History of Falls Documented and/or reported history of fall(s)
No fall history in the past 12 months
Fall in the past 6-12 months
Fall in the past 2-6 months Fall within the past two months
B. Current Status Medical and Psychiatric conditions
None of the conditions listed in Score 1, 2, or 3 columns
One of the following: -Arthritis -Osteoporosis -Respiratory condition -Recent substance abuse -Depression with decreased sleeping -Psychosis with suspiciousness, grandiosity, emotional withdrawal -Hypoglycemia -Seizure disorder with no seizure occurrence in the past 12 months
One of the following: -Anemia -CVA or traumatic brain injury in past 6 months -Movement disorder (e.g., Parkinson’s) -Congestive Heart Failure -Diabetic neuropathy -Vertigo (e.g., BPPV) -Psychosis with hallucinations and delusions -Neurologic condition causing LE weakness -Seizure disorder with one or more seizures in the past 6-12 months
One or both of the following: -Dementia -Seizure Disorder with one or more seizures in the past 6 months AND/OR -Two or more medical or psychiatric conditions from Score 1 and/or Score 2 column(s)
Medications
None of the medications listed in Score 1, 2, or 3 columns
One of the following: -Diuretics -Laxatives -Antidepressants -Psychotropics
One of the following: -Anti-hypertensives -Anticonvulsants -Anti-anxiety -Antispasmodics -Narcotics -Sedatives -Hypoglycemics -Antihistamines
-Two or more medications from Score 1 and/or Score 2 column(s) OR -Change in one or more medications listed in Score 1 and/or Score 2 column(s) in the past month
Activities of daily living
Independent with mobility, ambulation and self care tasks
-Requires active supervision and/or repeated prompts to complete activities of daily living
One of the following: -Requires physical assistance with ambulation and mobility -Requires the use of a device for ambulation and mobility (list below) -Requires physical assistance with activities of daily living -Uses wheelchair for mobility but able to assist with transfers
Two or more indicators from Score 1 and/or Score 2 column(s) OR Requires total dependence for mobility and transfers but attempts to get out of bed or chair
Lower extremity orthopedic condition
No lower extremity orthopedic condition
One or more of the following: -Requires unilateral lower extremity orthotic device -Requires unilateral lower extremity prosthetic device -Does not wear shoes
One or more of the following: -Requires bilateral lower extremity orthotic devices -Requires bilateral lower extremity prosthetic devices -Does not wear prescribed orthopedic shoes -Footwear is ill-fitting
Requires but does not wear orthotic or prosthetic device(s)
Urinary and bowel function
No urinary or bowel dysfunction
One or more of the following chronic conditions: -Incontinence (of urine and/or stool) -Increased frequency and/or urgency to urinate
Nocturia
Stamp Plate

DBHDD Policy: Physical and Nutritional Supports Page 2 of 3 Fall Risk Assessment
________________________________________________________________________________________________________________________________ Policy 03-522 Attachment C Version 5-17-2010
Sensory and communicative function
No sensory impairments
One of the following: -Somatosensory disorder -Hearing disorder -Wears corrective lenses
One of the following: -Blurred vision -Cataracts -Glaucoma -Requires corrective lenses but does not wear -Moderate language barrier -Exhibits impaired communication of needs and wants
One or more of the following: -Blind -Severe language barrier -Unable to communicate needs and wants OR -Two or more sensory impairments from Score 1 and/or Score 2 column(s)
Score 0
Score 1
Score 2
Score 3
Date:
Score (0-3/N/A)
C. *Individual report of: (Note: Score this section as N/A if individual is unable to self-report, and document reason)
Lower limb weakness No report of lower limb weakness
Reports weakness that does not impact balance or walking
Reports weakness that does impact balance and/or walking
Lightheadedness when standing or sitting up
No report of lightheadedness
Reports experience of lightheadedness less than once a week
Reports experience of lightheadedness more than once a week
Reports experience of lightheadedness one or more times a day
Dizziness No report of dizziness
Reports experience of dizziness less than once a week
Reports experience of dizziness more than once a week
Reports experience of dizziness one or more times a day
Lower limb and/or back pain
No report of lower limb and/or back pain
Reports pain that does not impact balance or walking
Reports pain that does impact balance and/or walking
Fear of falling
No report of fear of falling
Reports a fear of falling
D. Clinical Observation of:
Balance Not applicable for individual OR Functional balance
One of the following: -holds onto chair in order to keep upright -uses arms to hold onto chair or assistive device to pull or push up -moves forward in chair before attempting to rise -steady when standing, but uses assistive device for support -upon displacement, needs to move feet, but is able to maintain balance
Balance reactions impaired Two or more of the following: -holds onto chair in order to keep upright -uses arms to hold onto chair or assistive device to pull or push up -moves forward in chair before attempting to rise -steady when standing, but uses assistive device for support -upon displacement, needs to move feet, but is able to maintain balance
Significant balance impairment One or more of the following: -leans on chair for support or slides down in chair due to weakness or poor endurance -requires multiple attempts and/or physical assistance to rise from chair -any sign of unsteadiness during standing (e.g., grabbing at object or person for support, staggering, moving feet, swaying)
Balance
Stamp Plate

DBHDD Policy: Physical and Nutritional Supports Page 3 of 3 Fall Risk Assessment
________________________________________________________________________________________________________________________________ Policy 03-522 Attachment C Version 5-17-2010
[if noted DO NOT
perform displacement test] -upon displacement, begins to fall, or requires physical assistance to help maintain balance
Gait Not applicable for individual OR Normal gait
One or more of the following: -Gait is slow -Gait is shuffling
One or more of the following: -Gait is unsteady -Gait is poorly coordinated
Agitation and Anxiety Not observed One or more of the following: -Uses offensive/abrasive language occasionally -Engages in repetitive behaviors (e. g., pacing, rocking) -Yells, frequently complains -Mild symptoms of anxiety: minimal muscle tension, awareness of multiple environmental and internal stimuli, thoughts may be random
One or more of the following: -Verbally aggressive -Engages in property destruction -Threatens others -Moderate symptoms of anxiety: vital signs normal or slightly elevated, tension observed, may be uncomfortable, perception narrowed
One or more of the following: -Physically aggressive or hostile -Severe symptoms of anxiety: vital signs increased, sweating, muscles rigid or tense, perceptions and/or awareness greatly narrowed, feels threatened, startles with new stimuli -Meets Risk Management Policy Attachment B criteria for high risk for aggression
Mental status No observation of impaired mental status
One of the following: -Impaired memory -Impulsivity
One of the following: -Impaired judgment -Impaired ability to understand and follow directions
Two or more indicators from Score 1 and/or Score 2 column(s)
Awareness
Alert and aware of environment and routine
Diminished awareness of environment and routine
Unfamiliar with and unaware of environment and routine
Orthostatic Vital Signs Not applicable for individual OR No significant orthostatic changes in BP or HR
-Significant orthostatic changes in BP or HR
Total score:
Adaptive equipment related to mobility and/or transfers: *Section C. N/A response: ___________________________________________________________________________________________ __________________________________________________________________________________________________________________ Scoring: A score of 25/49 or more indicates high risk for falls *If the individual is unable to report indicators due to limited cognition and/or communication, score as “N/A”. If section C. is marked as “N/A”, a score of 19/37 or more indicates high risk for falls.
SIGNATURE: DATE: _____________________________________________ ________ Stamp Plate

DBHDD Policy: Physical and Nutritional Supports Page 1 of 6
Instructions: Fall Risk Assessment
________________________________________________________________________________________________________________________________ Policy 03-522 Attachment C - Instructions Version 5-17-2010
For each item below read criteria for each scoring option, select the best option that most accurately describes the individual, and document this score in the far right column. Do not leave any scores blank. This form may be completed for ONE risk assessment.
Score 0
Score 1
Score 2
Score 3
Date:
Score (0-3/N/A)
A. History of Falls Documented and/or reported history of fall(s)
No fall history in the past 12 months Score 0 if the individual has not had a fall in the last 12 months
Fall in the past 6-12 months Score 1 if the individual has not had a fall in the last 6 months, but had a fall 6 to 12 months ago
Fall in the past 2-6 months Score 2 if the individual has not had a fall in the last 2 months, but had a fall 2-6 months ago
Fall within the past two months Score 3 if the individual had a fall in the last 2 months
B. Current Status Medical and Psychiatric conditions
None of the conditions listed in Score 1, 2, or 3 columns Score 0 if the individual does not have any of the conditions listed in the Score 1, 2, or 3 columns
Score 1 if the individual has ONLY ONE of the following conditions: -Arthritis -Osteoporosis -Respiratory condition -Recent substance abuse -Depression with decreased sleeping -Psychosis with suspiciousness, grandiosity, emotional withdrawal -Hypoglycemia -Seizure disorder with no seizure occurrence in the past 12 months
Score 2 if the individual has ONLY ONE of the following conditions: -Anemia -CVA or traumatic brain injury in past 6 months -Movement disorder (e.g., Parkinson’s) -Congestive Heart Failure -Diabetic neuropathy -Vertigo (e.g., BPPV, Benign Paroxysmal Positional Vertigo) -Psychosis with hallucinations and delusions -Neurologic condition causing LE (lower extremity) weakness (e.g., spinal cord injury) -Seizure disorder with one or more seizures in the past 6-12 months
Score 3 if the individual has ONE OR BOTH of the following conditions: -Dementia -Seizure Disorder with one or more seizures in the past 6 months AND/OR Score 3 if the individual has: -TWO OR MORE medical or psychiatric conditions from Score 1 and/or Score 2 column(s)
Medications
None of the medications listed in Score 1, 2, or 3 columns Score 0 if the individual does not receive any of the medications listed in the Score 1 or Score 2 columns
Score 1 if the individual receives ONLY ONE of the following medications: -Diuretics -Laxatives -Antidepressants -Psychotropics
Score 2 if the individual receives ONLY ONE of the following medications: -Anti-hypertensives -Anticonvulsants -Anti-anxiety -Antispasmodics -Narcotics -Sedatives -Hypoglycemics -Antihistamines
Score 3 if the individual receives: -TWO OR MORE medications from Score 1 and/or Score 2 column(s) OR Score 3 if the individual has had a: -Change in one or more medications listed in Score 1 and/or Score 2 column(s) in the past month
Activities of daily living
Independent with mobility, ambulation and self care tasks Score 0 if the individual does not require physical
Score 1 if the individual: -Requires active supervision and/or repeated prompts to complete activities of daily living (this pertains to self care
Score 2 if ONLY ONE of the following is true for the individual (may ask individual and/or caregiver to score): -Requires physical assistance with ambulation and mobility -Requires the use of a device for ambulation and mobility (list below)
Score 3 if the individual exhibits: TWO OR MORE indicators from Score 1 and/or Score 2 column(s) OR Score 3 if the individual: Requires total dependence

DBHDD Policy: Physical and Nutritional Supports Page 2 of 6
Instructions: Fall Risk Assessment
________________________________________________________________________________________________________________________________ Policy 03-522 Attachment C - Instructions Version 5-17-2010
assistance or supervision for self care activities; may ask individual and/or caregiver to score
activities of daily living; may ask individual and/or caregiver to score)
-Requires physical assistance with activities of daily living (this pertains to self care activities of daily living) -Uses wheelchair for mobility but able to assist with transfers
for mobility and transfers but attempts to get out of bed or chair
Lower extremity orthopedic condition
No lower extremity orthopedic condition Score 0 if the individual does not have any lower extremity (e.g., foot, ankle, knee, hip) conditions that may cause pain or impaired function
Score 1 if ONE OR MORE of the following is true for the individual: -Requires unilateral lower extremity orthotic device -Requires unilateral lower extremity prosthetic device -Does not wear shoes
Score 2 if ONE OR MORE of the following is true for the individual: -Requires bilateral lower extremity orthotic devices -Requires bilateral lower extremity prosthetic devices -Does not wear prescribed orthopedic shoes -Footwear is ill-fitting
Score 3 if the individual: Requires but does not wear orthotic or prosthetic device(s)
Urinary and bowel function
No urinary or bowel dysfunction Score 0 if individual is continent of bowel and bladder and has no complaints of increased frequency, urgency, or nocturia; may ask individual and/or caregiver to score
Score 2 if the individual has ONE OR MORE of the following chronic conditions; may ask individual and/or caregiver to score: -Incontinence (of urine and/or stool) -Increased frequency and/or urgency to urinate
Score 3 if the individual has nocturia; may ask individual and/or caregiver to score Nocturia
Sensory and communicative function
No sensory impairments Score 0 if the individual has no known visual, hearing, somatosensory (e.g., touch, joint and muscle sensor limitations) or communication impairments
Score 1 if the individual has ONLY ONE of the following: -Somatosensory disorder -Hearing disorder -Wears corrective lenses
Score 2 if the individual has ONLY ONE of the following: -Blurred vision -Cataracts -Glaucoma -Requires corrective lenses but does not wear -Moderate language barrier -Exhibits impaired communication of needs and wants
Score 3 if the individual has ONE OR MORE of the following: -Blind -Severe language barrier -Unable to communicate needs and wants OR Score 3 if the individual has: -Two or more sensory impairments from Score 1 and/or Score 2 column(s)
Score 0
Score 1
Score 2
Score 3
Date:
Score (0-3/N/A)
C. *Individual report of: (Note: Score this section as N/A if individual is unable to self-report, and document reason) If the individual is
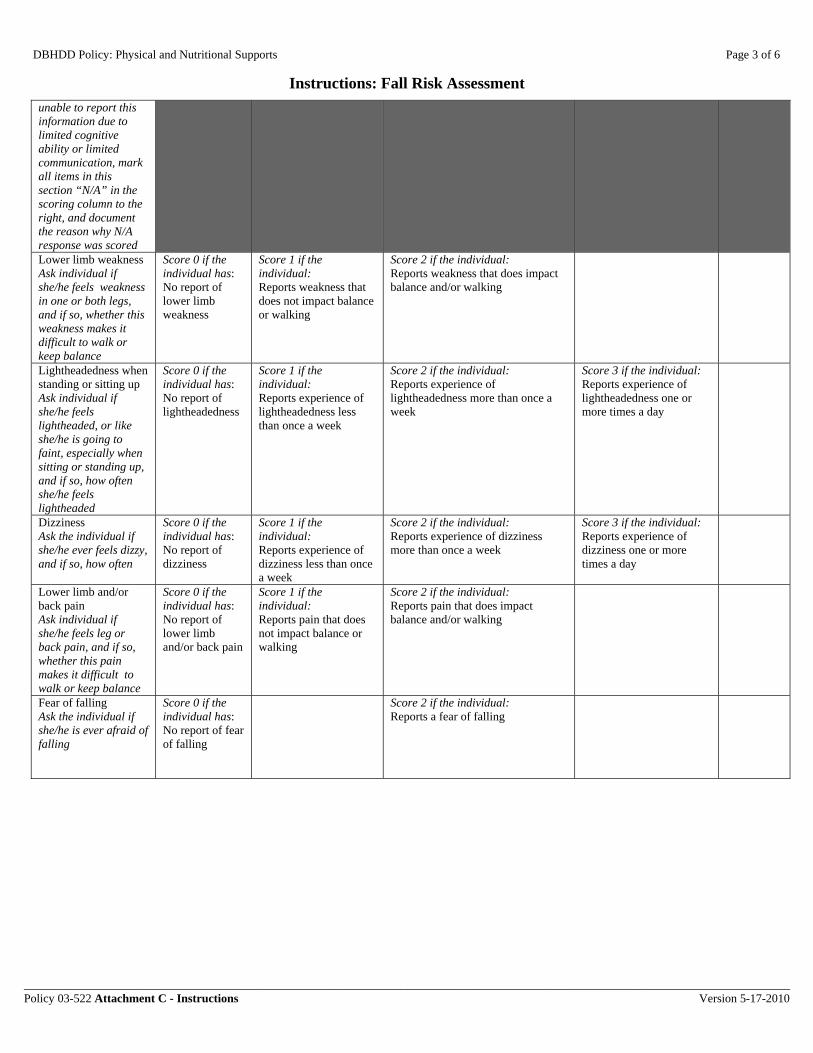
DBHDD Policy: Physical and Nutritional Supports Page 3 of 6
Instructions: Fall Risk Assessment
________________________________________________________________________________________________________________________________ Policy 03-522 Attachment C - Instructions Version 5-17-2010
unable to report this information due to limited cognitive ability or limited communication, mark all items in this section “N/A” in the scoring column to the right, and document the reason why N/A response was scored Lower limb weakness Ask individual if she/he feels weakness in one or both legs, and if so, whether this weakness makes it difficult to walk or keep balance
Score 0 if the individual has: No report of lower limb weakness
Score 1 if the individual: Reports weakness that does not impact balance or walking
Score 2 if the individual: Reports weakness that does impact balance and/or walking
Lightheadedness when standing or sitting up Ask individual if she/he feels lightheaded, or like she/he is going to faint, especially when sitting or standing up, and if so, how often she/he feels lightheaded
Score 0 if the individual has: No report of lightheadedness
Score 1 if the individual: Reports experience of lightheadedness less than once a week
Score 2 if the individual: Reports experience of lightheadedness more than once a week
Score 3 if the individual: Reports experience of lightheadedness one or more times a day
Dizziness Ask the individual if she/he ever feels dizzy, and if so, how often
Score 0 if the individual has: No report of dizziness
Score 1 if the individual: Reports experience of dizziness less than once a week
Score 2 if the individual: Reports experience of dizziness more than once a week
Score 3 if the individual: Reports experience of dizziness one or more times a day
Lower limb and/or back pain Ask individual if she/he feels leg or back pain, and if so, whether this pain makes it difficult to walk or keep balance
Score 0 if the individual has: No report of lower limb and/or back pain
Score 1 if the individual: Reports pain that does not impact balance or walking
Score 2 if the individual: Reports pain that does impact balance and/or walking
Fear of falling Ask the individual if she/he is ever afraid of falling
Score 0 if the individual has: No report of fear of falling
Score 2 if the individual: Reports a fear of falling

DBHDD Policy: Physical and Nutritional Supports Page 4 of 6
Instructions: Fall Risk Assessment
________________________________________________________________________________________________________________________________ Policy 03-522 Attachment C - Instructions Version 5-17-2010
D. Clinical Observation of:
Balance Observe individual transitioning to sitting, during sitting, and while standing. If an individual is able to stand independently, perform standing balance test. While individual is standing, inform individual that you will be testing her/his balance prior to giving gentle nudge to sternum area to cause displacement.
Functional balance Score 0 if individual is able to do all of the following: -sit down in one smooth movement, - remain steady and stable while sitting in chair -stand without swaying or holding object for support -individual remains steady with displacement and is able to withstand pressure OR Score 0 if individual’s physical condition prevents she or he from sitting or standing up (e.g., individual is in a coma)
Score 1 if individual exhibits ONLY ONE of the following: -holds onto chair in order to keep upright -uses arms to hold onto chair or assistive device to pull or push up -moves forward in chair before attempting to rise -steady when standing, but uses assistive device for support -upon displacement, needs to move feet, but is able to maintain balance
Balance reactions impaired Score 2 if the individual exhibits ANY TWO OR MORE of the following: -holds onto chair in order to keep upright -uses arms to hold onto chair or assistive device to pull or push up -moves forward in chair before attempting to rise -steady when standing, but uses assistive device for support -upon displacement, needs to move feet, but is able to maintain balance
Significant balance impairment Score 3 if the individual exhibits ONE OR MORE of the following: -leans on chair for support or slides down in chair due to weakness or poor endurance -requires multiple attempts and/or physical assistance to rise from chair -any sign of unsteadiness during standing (e.g., grabbing at object or person for support, staggering, moving feet, swaying) [if noted DO NOT perform displacement test] -upon displacement, begins to fall, or requires physical assistance to help maintain balance
Gait Observe individual walking upon approach towards and retreat from risk assessment location, or if unable to observe, ask individual to walk a distance of approximately 30 feet (10 meters) and observe gait
Normal gait Score 0 if individual exhibits a normal and steady gait OR Score 0 if individual does not ambulate
Score 1 if ONE OR MORE of the following are observed: -Gait is slow -Gait is shuffling
Score 2 if individual exhibits ONE OR MORE of the following: -Gait is unsteady: trunk leaning to side or back, veers to one side, gait is wide-based, or individual is limping or needs assistive device due to unsteady gait -Gait is poorly coordinated: individual hikes hip, exhibits spastic or stiff legs, or drags one foot
Agitation and Anxiety Not observed Score 0 if neither agitation nor anxiety is observed during risk assessment AND has not been observed in the past month as evidenced by
Score 1 if individual exhibits ONE OR MORE of the following during risk assessment AND/OR ONE OR MORE of the following was observed in the past month as evidenced by documentation or caregiver report: -Uses
Score 2 if individual exhibits ONE OR MORE of the following during risk assessment AND/OR ONE OR MORE of the following was observed in the past month as evidenced by documentation or caregiver report: -Verbally aggressive -Engages in property destruction -Threatens others -Moderate symptoms of anxiety:
Score 3 if individual exhibits ONE OR MORE of the following during risk assessment AND/OR ONE OR MORE of the following was observed in the past month as evidenced by documentation or caregiver report: -Physically aggressive or

DBHDD Policy: Physical and Nutritional Supports Page 5 of 6
Instructions: Fall Risk Assessment
________________________________________________________________________________________________________________________________ Policy 03-522 Attachment C - Instructions Version 5-17-2010
documentation or caregiver report
offensive/abrasive language occasionally -Engages in repetitive behaviors (e. g., pacing, rocking) -Yells, frequently complains -Mild symptoms of anxiety: minimal muscle tension, awareness of multiple environmental and internal stimuli, thoughts may be random
vital signs normal or slightly elevated, tension observed, may be uncomfortable, perception narrowed
hostile -Severe symptoms of anxiety: vital signs increased, sweating, muscles rigid or tense, perceptions and/or awareness greatly narrowed, feels threatened, startles with new stimuli -Meets Risk Management Policy Attachment B criteria for high risk for aggression
Mental status No observation of impaired mental status Score 0 if no observation of impaired mental status is observed during risk assessment AND has not been observed in the past month as evidenced by documentation or caregiver report
Score 1 if individual exhibits ONLY ONE of the following during risk assessment AND/OR ONLY ONE of the following was observed in the past month as evidenced by documentation or caregiver report: -Impaired memory -Impulsivity
Score 2 if individual exhibits ONLY ONE of the following during risk assessment AND/OR ONLY ONE of the following was observed in the past month as evidenced by documentation or caregiver report: -Impaired judgment -Impaired ability to understand and follow directions
Score 3 if individual exhibits TWO OR MORE of the following during risk assessment AND/OR TWO OR MORE of the following were observed in the past month as evidenced by documentation or caregiver report: -Impaired memory -Impulsivity -Impaired judgment -Impaired ability to understand and follow directions
Awareness
Alert and aware of environment and routine Score 0 if individual is alert and aware of environment during risk assessment, AND if not a new admission, individual is aware of daily routine
Diminished awareness of environment and routine Score 2 if individual has partial awareness of environment during risk assessment, AND/OR if not a new admission, individual has partial awareness of daily routine
Unfamiliar with and unaware of environment and routine Score 3 if individual is unaware of environment during risk assessment, OR if not a new admission, individual is unaware of daily routine
Orthostatic Vital Signs Assess orthostatic vital signs as clinically indicated per physician order and hospital procedures
Not applicable for individual OR No significant orthostatic changes in BP or HR Score as 0 if individual does not have a condition which would warrant orthostatic vital sign assessment OR Score as 0 if no significant
Significant orthostatic changes in BP or HR Score as 2 if significant orthostatic changes in BP or HR are observed as evidenced by one or more of the
following: -Standing or sitting heart rate 20 or more beats higher than lying -Standing or sitting systolic BP 20 or more mmHg less than lying -Standing or sitting diastolic BP 10 or more mmHg less than lying
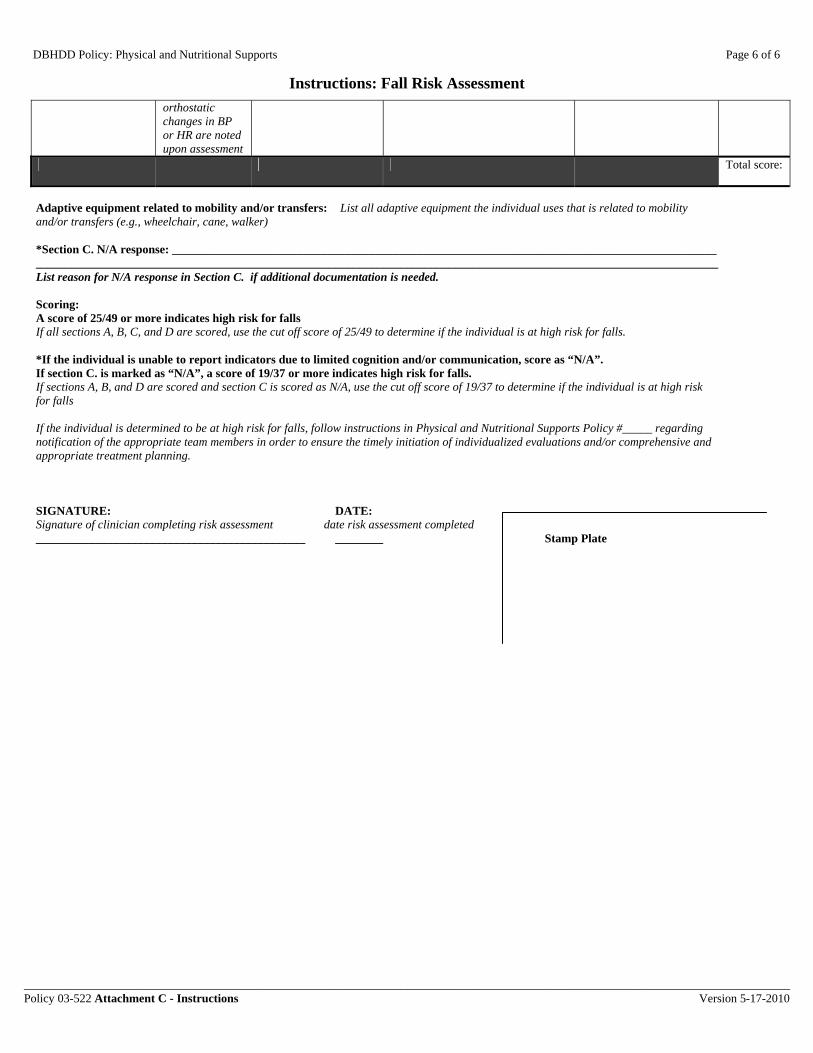
DBHDD Policy: Physical and Nutritional Supports Page 6 of 6
Instructions: Fall Risk Assessment
________________________________________________________________________________________________________________________________ Policy 03-522 Attachment C - Instructions Version 5-17-2010
orthostatic changes in BP or HR are noted upon assessment
Total score:
Adaptive equipment related to mobility and/or transfers: List all adaptive equipment the individual uses that is related to mobility and/or transfers (e.g., wheelchair, cane, walker) *Section C. N/A response: ___________________________________________________________________________________________ __________________________________________________________________________________________________________________ List reason for N/A response in Section C. if additional documentation is needed. Scoring: A score of 25/49 or more indicates high risk for falls If all sections A, B, C, and D are scored, use the cut off score of 25/49 to determine if the individual is at high risk for falls. *If the individual is unable to report indicators due to limited cognition and/or communication, score as “N/A”. If section C. is marked as “N/A”, a score of 19/37 or more indicates high risk for falls. If sections A, B, and D are scored and section C is scored as N/A, use the cut off score of 19/37 to determine if the individual is at high risk for falls If the individual is determined to be at high risk for falls, follow instructions in Physical and Nutritional Supports Policy #_____ regarding notification of the appropriate team members in order to ensure the timely initiation of individualized evaluations and/or comprehensive and appropriate treatment planning.
SIGNATURE: DATE: Signature of clinician completing risk assessment date risk assessment completed _____________________________________________ ________ Stamp Plate
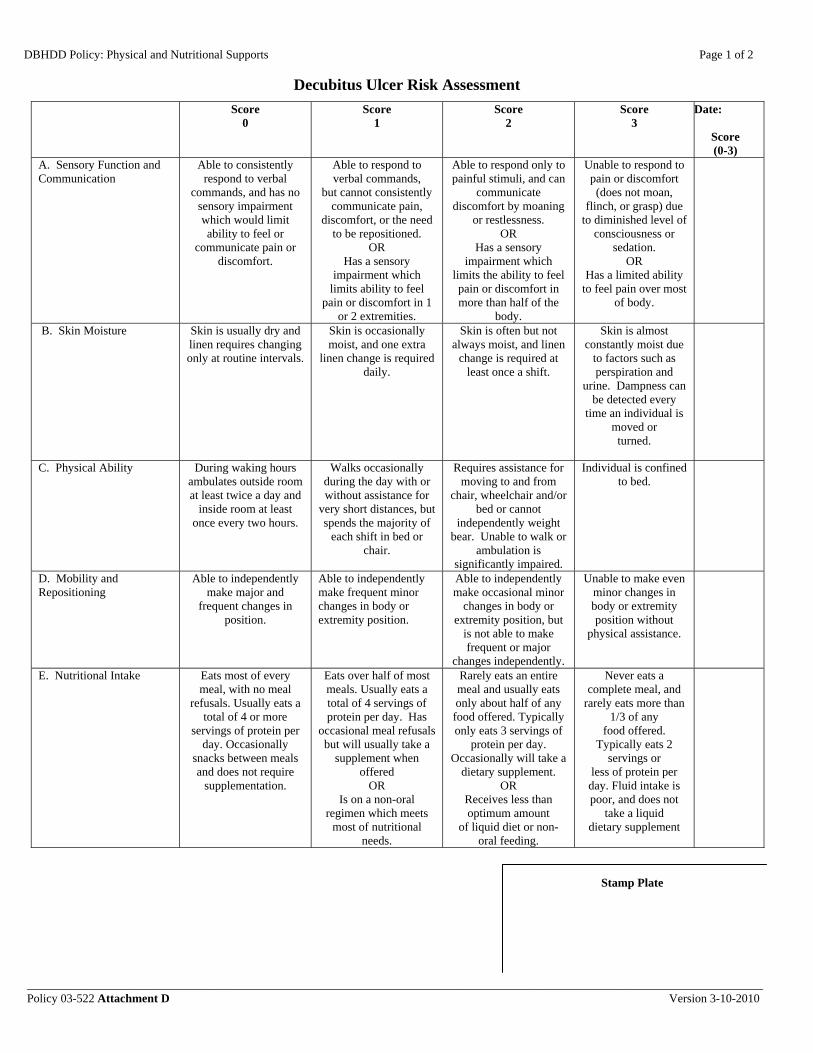
DBHDD Policy: Physical and Nutritional Supports Page 1 of 2
Decubitus Ulcer Risk Assessment
___________________________________________________________________________________________________________________________ Policy 03-522 Attachment D Version 3-10-2010
Score 0
Score 1
Score 2
Score 3
Date:
Score (0-3)
A. Sensory Function and Communication
Able to consistently respond to verbal
commands, and has no sensory impairment which would limit ability to feel or
communicate pain or discomfort.
Able to respond to verbal commands,
but cannot consistently communicate pain,
discomfort, or the need to be repositioned.
OR Has a sensory
impairment which limits ability to feel
pain or discomfort in 1 or 2 extremities.
Able to respond only to painful stimuli, and can
communicate discomfort by moaning
or restlessness. OR
Has a sensory impairment which
limits the ability to feel pain or discomfort in more than half of the
body.
Unable to respond to pain or discomfort (does not moan,
flinch, or grasp) due to diminished level of
consciousness or sedation.
OR Has a limited ability
to feel pain over most of body.
B. Skin Moisture Skin is usually dry and linen requires changing only at routine intervals.
Skin is occasionally moist, and one extra
linen change is required daily.
Skin is often but not always moist, and linen
change is required at least once a shift.
Skin is almost constantly moist due
to factors such as perspiration and
urine. Dampness can be detected every
time an individual is moved or turned.
C. Physical Ability During waking hours ambulates outside room at least twice a day and
inside room at least once every two hours.
Walks occasionally during the day with or without assistance for
very short distances, but spends the majority of
each shift in bed or chair.
Requires assistance for moving to and from
chair, wheelchair and/or bed or cannot
independently weight bear. Unable to walk or
ambulation is significantly impaired.
Individual is confined to bed.
D. Mobility and Repositioning
Able to independently make major and
frequent changes in position.
Able to independently make frequent minor changes in body or extremity position.
Able to independently make occasional minor
changes in body or extremity position, but
is not able to make frequent or major
changes independently.
Unable to make even minor changes in body or extremity position without
physical assistance.
E. Nutritional Intake Eats most of every meal, with no meal
refusals. Usually eats a total of 4 or more
servings of protein per day. Occasionally
snacks between meals and does not require
supplementation.
Eats over half of most meals. Usually eats a total of 4 servings of protein per day. Has
occasional meal refusals but will usually take a
supplement when offered
OR Is on a non-oral
regimen which meets most of nutritional
needs.
Rarely eats an entire meal and usually eats only about half of any food offered. Typically only eats 3 servings of
protein per day. Occasionally will take a
dietary supplement. OR
Receives less than optimum amount
of liquid diet or non-oral feeding.
Never eats a complete meal, and
rarely eats more than 1/3 of any
food offered. Typically eats 2
servings or less of protein per day. Fluid intake is poor, and does not
take a liquid dietary supplement
Stamp Plate

DBHDD Policy: Physical and Nutritional Supports Page 2 of 2
Decubitus Ulcer Risk Assessment
___________________________________________________________________________________________________________________________ Policy 03-522 Attachment D Version 3-10-2010
Score
0 Score
1 Score
2
Score 3
Date:
Score (0-3)
OR Is NPO and/or maintained on
clear liquids or IV’s for more than 5 days.
F. Friction and Shearing Forces
Able to move independently in bed and in chair and has
sufficient strength to lift up completely during
repositioning and moving. Able to
maintain good position and
alignment in bed or chair.
Requires minimum assistance with moving,
or exhibits poor movement. During a move skin probably slides to some extent against sheets, chair,
restraints or other devices. Able to
maintain relatively good position in chair
or bed most of the time but occasionally slides
down.
Requires moderate to maximum
assistance with moving. Unable to
lift individual without sliding on sheets. Requires frequent repositioning with
maximum assistance due to frequent
sliding down in bed or chair.
Friction is almost constant due to
spasticity, contractures or
agitation.
G. Body Build and Height Average (BMI 19-24) Above (BMI 25-29) or Below Average (BMI
15-18.5)
Emaciated (BMI below 15)
Obese (BMI > 30)
H. Skin Type Normal Dry skin Tissue paper-like Edematous Total
score:
Scoring: A score of 13 or more indicates high risk for decubitus ulcer
SIGNATURE: DATE: _____________________________________________ ________ Stamp Plate

DBHDD Policy: Physical and Nutritional Supports Page 1 of 3
Instructions: Decubitus Ulcer Risk Assessment
__________________________________________________________________________________________________________________________ Policy 03-522 Attachment D - Instructions Version 3-10-2010
For each item below read criteria for each scoring
option, select the best option that most accurately
describes the individual, and document this score in
the far right column. Do not leave any scores blank.
This form may be completed for ONE risk
assessment.
Score 0
Score 1
Score 2
Score 3
Date:
Score (0-3)
A. Sensory Function and Communication
Score 0 if the individual exhibits the following
during risk assessment; may also use caregiver
report to assist with scoring
Able to consistently respond to verbal
commands, and has no sensory impairment which would limit ability to feel or
communicate pain or discomfort.
Score 1 if the individual exhibits the following
during risk assessment; may also use caregiver
report to assist with scoring:
Able to respond to verbal commands,
but cannot consistently communicate pain,
discomfort, or the need to be repositioned.
OR Score 1 if the individual:
Has a sensory impairment which
limits ability to feel pain or discomfort in 1
or 2 extremities.
Score 2 if the individual exhibits the following
during risk assessment; may also use caregiver
report to assist with scoring:
Able to respond only to painful stimuli, and can
communicate discomfort by moaning
or restlessness. OR
Score 2 if the individual:
Has a sensory impairment which
limits the ability to feel pain or discomfort in more than half of the
body.
Score 3 if the individual exhibits
the following during risk assessment; may
also use caregiver report to assist with
scoring: Unable to respond to pain or discomfort (does not moan,
flinch, or grasp) due to diminished level of
consciousness or sedation.
OR Score 3 if the individual:
Has a limited ability to feel pain over most
of body.
B. Skin Moisture Score 0 if the following is confirmed by
individual report, caregiver report, and/or nursing documentation: Skin is usually dry and linen requires changing only at routine intervals.
Score 1 if the following is confirmed by
individual report, caregiver report, and/or nursing documentation:
Skin is occasionally moist, and one extra
linen change is required daily.
Score 2 if the following is confirmed by
individual report, caregiver report, and/or nursing documentation:
Skin is often but not always moist, and linen
change is required at least once a shift.
Score 3 if the following is
confirmed by individual report, caregiver report, and/or nursing documentation: Skin is almost
constantly moist due to factors such as perspiration and
urine. Dampness can be detected every
time an individual is moved or turned.
C. Physical Ability Score 0 if the following is confirmed by
individual report, caregiver report, and/or nursing documentation:
During waking hours ambulates outside room at least twice a day and
inside room at least once every two hours.
Score 1 if the following is confirmed by
individual report, caregiver report, and/or nursing documentation:
Walks occasionally during the day with or without assistance for
very short distances, but spends the majority of
each shift in bed or chair.
Score 2 if any of the following are observed
for the individual: Requires assistance for
moving to and from chair, wheelchair and/or
bed or cannot independently weight
bear. Unable to walk or ambulation is
significantly impaired.
Score 3 if: Individual is confined
to bed.
D. Mobility and Repositioning
Score 0 if the individual exhibits the following
during risk assessment; may also use caregiver
Score 1 if the individual exhibits the following during risk assessment; may also use caregiver
Score 2 if the individual exhibits the following
during risk assessment; may also use caregiver
Score 3 if the individual exhibits
the following during risk assessment; may

DBHDD Policy: Physical and Nutritional Supports Page 2 of 3
Instructions: Decubitus Ulcer Risk Assessment
__________________________________________________________________________________________________________________________ Policy 03-522 Attachment D - Instructions Version 3-10-2010
report to assist with scoring
Able to independently make major (e.g., moves
between supine, sidelying and prone
positions in bed independently) and frequent changes in
position.
report to assist with scoring: Able to independently make frequent minor (e.g., can move limbs) changes in body or extremity position.
report to assist with scoring:
Able to independently make occasional minor
changes in body or extremity position, but
is not able to make frequent or major
changes independently.
also use caregiver report to assist with
scoring: Unable to make even
minor changes in body or extremity position without
physical assistance.
E. Nutritional Intake Review intake documentation for the past month, or use individual and/or caregiver report if no documentation is available for a new admission. May collaborate with dietitian for further clarification.
Score 0 if the individual:
Eats most of every meal, with no meal
refusals. Usually eats a total of 4 or more
servings of protein per day. Occasionally
snacks between meals and does not require
supplementation.
Score 1 if the individual:
Eats over half of most meals. Usually eats a total of 4 servings of protein per day. Has
occasional meal refusals but will usually take a
supplement when offered
OR Score 1 if the individual:
Is on a non-oral regimen which meets
most of nutritional needs.
Score 2 if the individual:
Rarely eats an entire meal and usually eats only about half of any food offered. Typically only eats 3 servings of
protein per day. Occasionally will take a
dietary supplement. OR
Score 2 if the individual:
Receives less than optimum amount
of liquid diet or non-oral feeding.
Score 3 if the individual:
Never eats a complete meal, and
rarely eats more than 1/3 of any
food offered. Typically eats 2
servings or less of protein per day. Fluid intake is poor, and does not
take a liquid dietary supplement
OR Score 3 if the individual:
Is NPO and/or maintained on
clear liquids or IV’s for more than 5 days.

DBHDD Policy: Physical and Nutritional Supports Page 3 of 3
Instructions: Decubitus Ulcer Risk Assessment
__________________________________________________________________________________________________________________________ Policy 03-522 Attachment D - Instructions Version 3-10-2010
Score 0
Score 1
Score 2
Score 3
Date:
Score (0-3)
F. Friction and Shearing Forces
Score 1 if the individual exhibits the following
during risk assessment; may also use caregiver
report to assist with scoring:
Able to move independently in bed and in chair and has
sufficient strength to lift up completely during
repositioning and moving. Able to
maintain good position and
alignment in bed or chair.
Score 2 if the individual exhibits the following
during risk assessment; may also use caregiver
report to assist with scoring:
Requires minimum assistance with moving,
or exhibits poor movement. During a move skin probably slides to some extent against sheets, chair,
restraints or other devices. Able to
maintain relatively good position in chair
or bed most of the time but occasionally slides
down.
Score 3 if the individual exhibits
the following during risk assessment; may
also use caregiver report to assist with
scoring: Requires moderate to
maximum assistance with
moving. Unable to lift individual without
sliding on sheets. Requires frequent repositioning with
maximum assistance due to frequent
sliding down in bed or chair.
Friction is almost constant due to
spasticity, contractures or
agitation.
G. Body Build and Height Refer to appropriate most recent assessment in medical record to determine BMI; score 0 if individual BMI is: Average (BMI 19-24)
Refer to appropriate most recent assessment in medical record to determine BMI; score 1 if BMI is:
Above Average (BMI 25-29) or Below
Average (BMI 15-18.5)
Refer to appropriate most recent assessment in medical record to determine BMI; score 2 if BMI indicates that individual is: Emaciated (BMI below 15)
Refer to appropriate most recent assessment in medical record to determine BMI; score 3 if BMI indicates that individual is:
Obese (BMI > 30)
H. Skin Type Score 0 if skin appears: Normal
Score 1 if the individual has:
Dry skin
Score 2 if the individual has skin that is:
Tissue paper-like
Score 3 if swelling or edema is noted
Edematous
Total score:
Scoring: A score of 13 or more indicates high risk for decubitus ulcer If the individual is determined to be at high risk for decubitus ulcers, follow instructions in Physical and Nutritional Supports Policy #_____ regarding notification of the appropriate team members in order to ensure the timely initiation of individualized evaluations and/or comprehensive and appropriate treatment planning.
SIGNATURE: DATE: Signature of clinician completing risk assessment date risk assessment completed
_____________________________________________ ________ Stamp Plate

DBHDD Policy: Physical and Nutritional Supports Page 1 of 2
Nutritional Support General Guidelines
If any equipment is broken or missing, contact your supervisor or the Therapy department to request replacement equipment.
Always wash hands before assisting individuals to eat and remind or assist individuals to wash their hands as well.
Hands should be re-washed before helping another individual. Clean eating surfaces prior to each meal and/or individual assisted to eat. Individuals should be as upright as possible for all meals, snacks, oral hygiene,
tube feeding, and medication. People with reflux should remain upright for one hour following meals; they
should never lie flat. People with any swallowing difficulty should remain upright at least 30 minutes
following oral intake; they should never lie flat. All individuals who use wheelchairs or need help to sit upright must be
repositioned before meals, snacks, oral hygiene, medication administration, and/or non oral nutrition.
Repositioning should also occur throughout meals, snacks, oral hygiene, and non-oral nutrition as needed.
Head position- neutral or tucked, NEVER bent back! Staff helping individuals should sit at eye level. Pelvis position- level and back in the seat; seatbelt fastened if present Foot position- supported on floor, foot rests, or foot stool If a lap tray is not being used as an eating surface, remove tray to let the
individual sit close to the table. Helmets should be removed prior to meals, snacks, and oral hygiene, unless
otherwise indicated. Lock wheelchair brakes prior to meals, oral hygiene, and medication
administration. Individuals should be encouraged to sit in a regular chair at the table if they are
safe to do so. When assisting individuals:
Present all food at or below chin level. A safe bite size is one level TEASPOON. Offer liquids throughout the meal after every 4-6 bites of food. Watch for the up and down movement of the throat to check for a swallow
before giving another bite or sip. Make sure all food or liquid is cleared out of the mouth before presenting
another bite or sip. If food or liquid remains in the mouth, give an empty spoon to encourage
an additional swallow. When supervising individuals who can eat by themselves:
Provide assistance toward the end of the meal if the person becomes tired or has difficulty with eating.
________________________________________________________________________________________________ Policy 03-522 Attachment E Version 3-10-2010
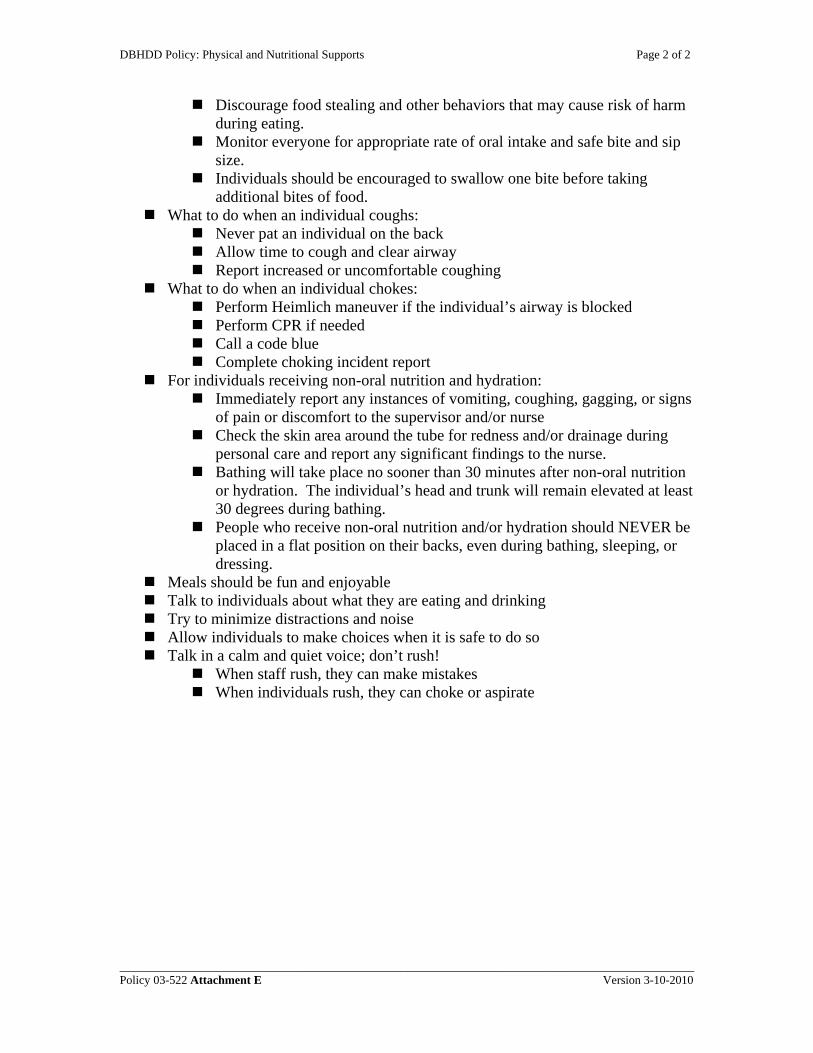
DBHDD Policy: Physical and Nutritional Supports Page 2 of 2
________________________________________________________________________________________________ Policy 03-522 Attachment E Version 3-10-2010
Discourage food stealing and other behaviors that may cause risk of harm during eating.
Monitor everyone for appropriate rate of oral intake and safe bite and sip size.
Individuals should be encouraged to swallow one bite before taking additional bites of food.
What to do when an individual coughs: Never pat an individual on the back Allow time to cough and clear airway Report increased or uncomfortable coughing
What to do when an individual chokes: Perform Heimlich maneuver if the individual’s airway is blocked Perform CPR if needed Call a code blue Complete choking incident report
For individuals receiving non-oral nutrition and hydration: Immediately report any instances of vomiting, coughing, gagging, or signs
of pain or discomfort to the supervisor and/or nurse Check the skin area around the tube for redness and/or drainage during
personal care and report any significant findings to the nurse. Bathing will take place no sooner than 30 minutes after non-oral nutrition
or hydration. The individual’s head and trunk will remain elevated at least 30 degrees during bathing.
People who receive non-oral nutrition and/or hydration should NEVER be placed in a flat position on their backs, even during bathing, sleeping, or dressing.
Meals should be fun and enjoyable Talk to individuals about what they are eating and drinking Try to minimize distractions and noise Allow individuals to make choices when it is safe to do so Talk in a calm and quiet voice; don’t rush!
When staff rush, they can make mistakes When individuals rush, they can choke or aspirate
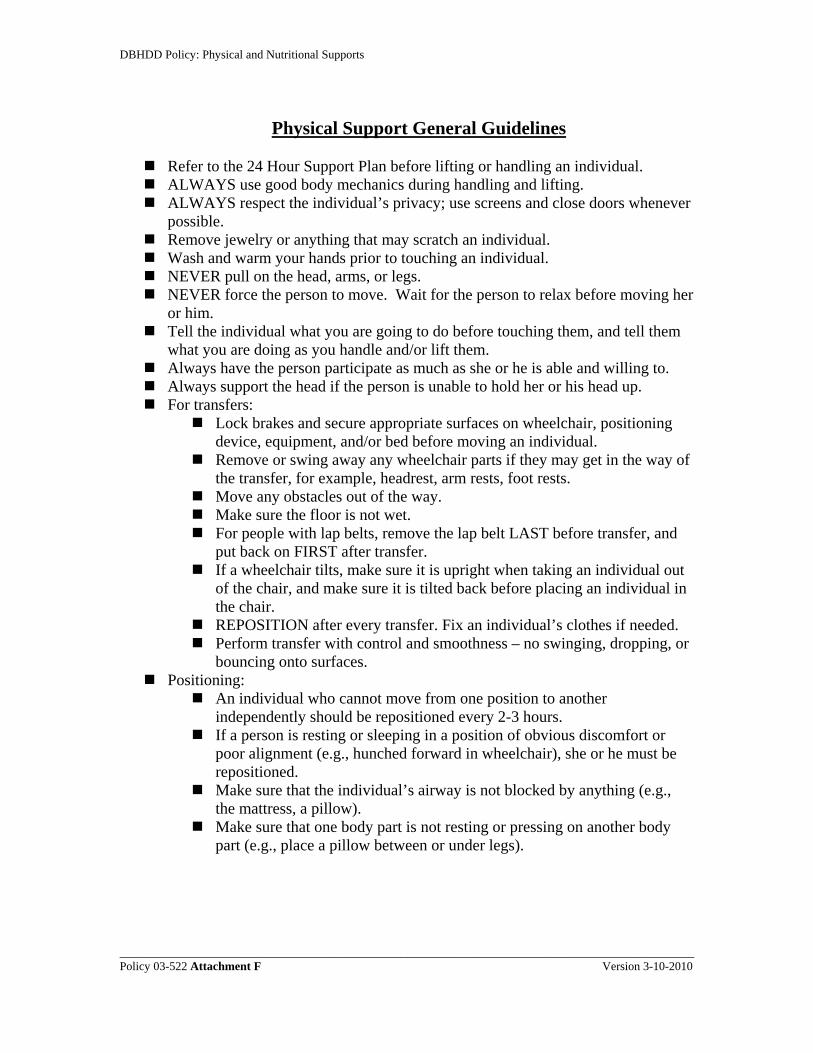
DBHDD Policy: Physical and Nutritional Supports
Physical Support General Guidelines
Refer to the 24 Hour Support Plan before lifting or handling an individual. ALWAYS use good body mechanics during handling and lifting. ALWAYS respect the individual’s privacy; use screens and close doors whenever
possible. Remove jewelry or anything that may scratch an individual. Wash and warm your hands prior to touching an individual. NEVER pull on the head, arms, or legs. NEVER force the person to move. Wait for the person to relax before moving her
or him. Tell the individual what you are going to do before touching them, and tell them
what you are doing as you handle and/or lift them. Always have the person participate as much as she or he is able and willing to. Always support the head if the person is unable to hold her or his head up. For transfers:
Lock brakes and secure appropriate surfaces on wheelchair, positioning device, equipment, and/or bed before moving an individual.
Remove or swing away any wheelchair parts if they may get in the way of the transfer, for example, headrest, arm rests, foot rests.
Move any obstacles out of the way. Make sure the floor is not wet. For people with lap belts, remove the lap belt LAST before transfer, and
put back on FIRST after transfer. If a wheelchair tilts, make sure it is upright when taking an individual out
of the chair, and make sure it is tilted back before placing an individual in the chair.
REPOSITION after every transfer. Fix an individual’s clothes if needed. Perform transfer with control and smoothness – no swinging, dropping, or
bouncing onto surfaces. Positioning:
An individual who cannot move from one position to another independently should be repositioned every 2-3 hours.
If a person is resting or sleeping in a position of obvious discomfort or poor alignment (e.g., hunched forward in wheelchair), she or he must be repositioned.
Make sure that the individual’s airway is not blocked by anything (e.g., the mattress, a pillow).
Make sure that one body part is not resting or pressing on another body part (e.g., place a pillow between or under legs).
________________________________________________________________________________________________ Policy 03-522 Attachment F Version 3-10-2010

DBHDD Policy: Physical and Nutritional Supports Page 1 of 2
24 Hour Support Plan Template and Guidelines
Date Initiated: Date(s) Revised:
Mealtime and Snacks: Triggers: list risk factors, e.g., h/o choking Target behaviors: list risk behaviors (e.g., fast eating pace, mouth “stuffing”) Diet prescription: should include therapeutic diet order, allergies, food preferences and/or food dislikes, special diet issues (e.g., religious fasting) Diet texture and liquid consistency: list food texture, liquid consistency, and any special instructions to ensure optimal or adequate hydration (e.g., fluid restrictions) Adaptive equipment: list hand preference and all adaptive equipment related to eating. Functional ability, level of assistance, and type of supervision: list supervision, level of assistance required as well as any specific abilities (e.g.; Mr. A. requires 1:1 supervision and staff assistance to scoop food- Mr. A is able to bring a loaded spoon to mouth independently) Special procedures and techniques: list any special techniques (e.g., chin tuck, offer communication device to allow for beverage choices, behavioral techniques, low vision strategies) for mealtime implementation. Individual and staff positioning: e.g., Mr. A should be seated upright in his custom wheelchair for all meals/snacks. Staff should be seated and positioned on his right side.
Medication Administration Medication texture, liquid consistency, and method of presentation: List how medications should be provided, including texture, liquid consistency and presentation Techniques for presentation: List any special techniques or precautions (e.g., provide medication by spoon using downward pressure on the middle of the tongue) Adaptive equipment: list any equipment specific to medication administration (e.g., nosey cup, small bowl spoon)
Oral Hygiene: Individual and Staff Positioning for oral hygiene: Special techniques: list any special procedures for provision of oral hygiene (e.g., no mouthwash, tongue scraping) Adaptive equipment: list any equipment specific to oral hygiene (e.g., built up handle toothbrush, suction toothbrush)
Picture of individual during eating activities (mealtime, snacks) - should include positioning and/or adaptive equipment
Please report any observed concerns to your immediate supervisor, and request assistance if you have any questions about this plan.
____________________________________________________________________________________________________________________ Policy 03-522 Attachment G Version 3-10-2010

DBHDD Policy: Physical and Nutritional Supports Page 2 of 2
____________________________________________________________________________________________________________________ Policy 03-522 Attachment G Version 3-10-2010
Mobility and transfers: Adaptive equipment and/or mobility device(s): Type of Transfer: Functional ability, level of assistance, and type of supervision: list supervision, level of assistance required as well as any specific abilities (e.g.; Mr. A. requires 1:1 supervision and total staff assistance x1 to transfer- Mr. A is able to place his arms on armrests independently prior to transfer) Special techniques and procedures: e.g., visual orientation in mobility, extra assistance with changes in surface due to poor depth perception
Bathing: Functional ability, level of assistance, and type of supervision: (e.g.; Mr. A. requires 1:1 supervision and maximum staff assistance for bathing- Mr. A is able to place wash his stomach with a prepared washcloth) Adaptive equipment: e.g., long handled sponge Positioning: Special techniques: include bathing strategies, and special techniques (e.g., behavioral, communication techniques)
Dressing and Grooming: Functional ability, level of assistance, and type of supervision: (e.g.; Mr. A. requires 1:1 supervision and total staff assistance x1 to transfer- Mr. A is able to place lift his arms independently prior to UB dressing) Adaptive equipment: e.g., long handled sponge Positioning: Special techniques: include dressing strategies, and special techniques (e.g., behavioral,
Picture of individual in seating system or with mobility device
Bed and/or alternate positioning: Equipment: e.g., bolster, elevated sidelyer Procedures:
Work and/or Education: Adaptive equipment: e.g., weighted pencil Environmental considerations: e.g., works best when visual distractions are minimized Picture of individual in bed or alternate positioning
Additional pictures as needed
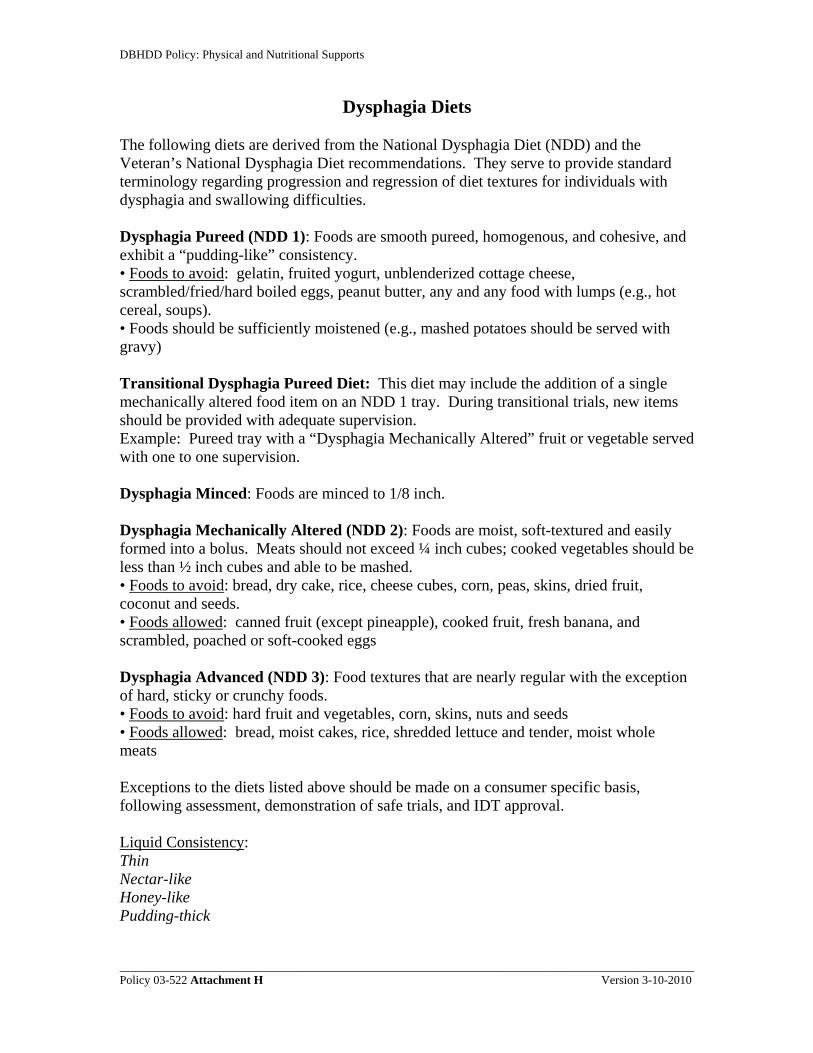
DBHDD Policy: Physical and Nutritional Supports
Dysphagia Diets
The following diets are derived from the National Dysphagia Diet (NDD) and the Veteran’s National Dysphagia Diet recommendations. They serve to provide standard terminology regarding progression and regression of diet textures for individuals with dysphagia and swallowing difficulties. Dysphagia Pureed (NDD 1): Foods are smooth pureed, homogenous, and cohesive, and exhibit a “pudding-like” consistency. • Foods to avoid: gelatin, fruited yogurt, unblenderized cottage cheese, scrambled/fried/hard boiled eggs, peanut butter, any and any food with lumps (e.g., hot cereal, soups). • Foods should be sufficiently moistened (e.g., mashed potatoes should be served with gravy) Transitional Dysphagia Pureed Diet: This diet may include the addition of a single mechanically altered food item on an NDD 1 tray. During transitional trials, new items should be provided with adequate supervision. Example: Pureed tray with a “Dysphagia Mechanically Altered” fruit or vegetable served with one to one supervision. Dysphagia Minced: Foods are minced to 1/8 inch. Dysphagia Mechanically Altered (NDD 2): Foods are moist, soft-textured and easily formed into a bolus. Meats should not exceed ¼ inch cubes; cooked vegetables should be less than ½ inch cubes and able to be mashed. • Foods to avoid: bread, dry cake, rice, cheese cubes, corn, peas, skins, dried fruit, coconut and seeds. • Foods allowed: canned fruit (except pineapple), cooked fruit, fresh banana, and scrambled, poached or soft-cooked eggs Dysphagia Advanced (NDD 3): Food textures that are nearly regular with the exception of hard, sticky or crunchy foods. • Foods to avoid: hard fruit and vegetables, corn, skins, nuts and seeds • Foods allowed: bread, moist cakes, rice, shredded lettuce and tender, moist whole meats Exceptions to the diets listed above should be made on a consumer specific basis, following assessment, demonstration of safe trials, and IDT approval. Liquid Consistency: Thin Nectar-like Honey-like Pudding-thick
________________________________________________________________________________________________ Policy 03-522 Attachment H Version 3-10-2010
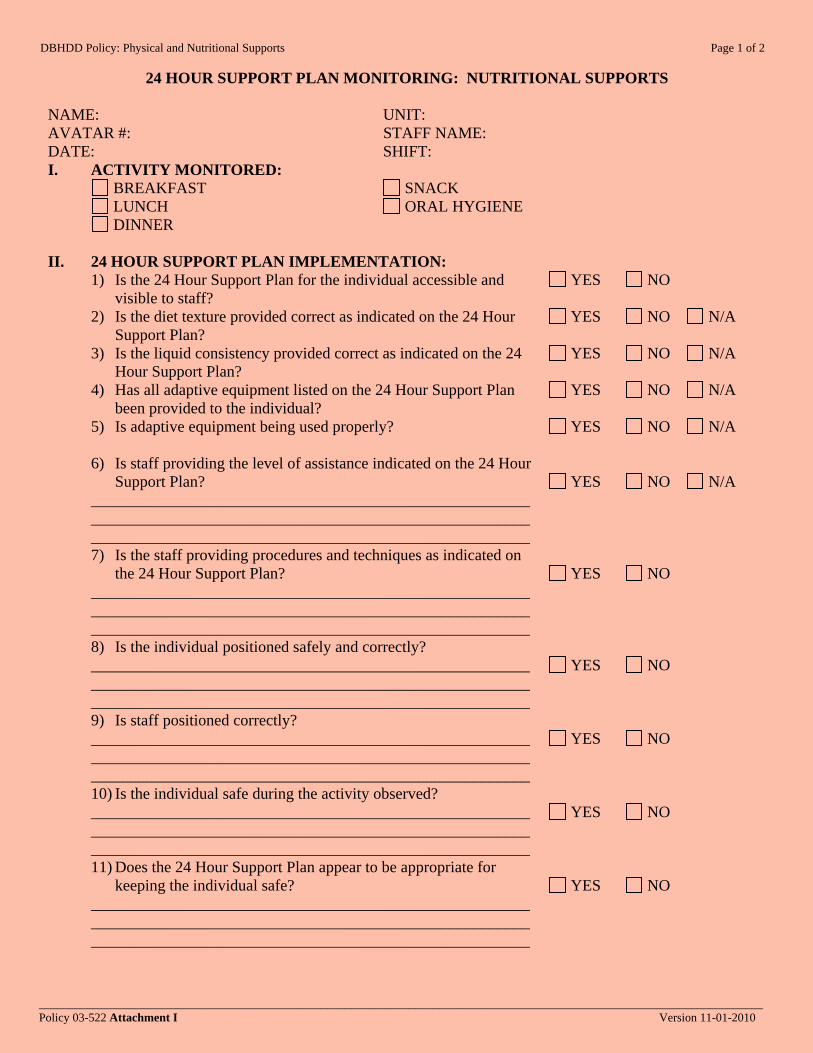
DBHDD Policy: Physical and Nutritional Supports Page 1 of 2
24 HOUR SUPPORT PLAN MONITORING: NUTRITIONAL SUPPORTS
_________________________________________________________________________________________________________________________ Policy 03-522 Attachment I Version 11-01-2010
NAME: UNIT: AVATAR #: STAFF NAME: DATE: SHIFT: I. ACTIVITY MONITORED: BREAKFAST
LUNCH DINNER
SNACK ORAL HYGIENE
II. 24 HOUR SUPPORT PLAN IMPLEMENTATION: 1) Is the 24 Hour Support Plan for the individual accessible and
visible to staff? 2) Is the diet texture provided correct as indicated on the 24 Hour
Support Plan? 3) Is the liquid consistency provided correct as indicated on the 24
Hour Support Plan? 4) Has all adaptive equipment listed on the 24 Hour Support Plan
been provided to the individual? 5) Is adaptive equipment being used properly? 6) Is staff providing the level of assistance indicated on the 24 Hour
Support Plan? _____________________________________________________________________________________________________________________________________________________________________ 7) Is the staff providing procedures and techniques as indicated on
the 24 Hour Support Plan? _____________________________________________________________________________________________________________________________________________________________________ 8) Is the individual positioned safely and correctly? _____________________________________________________________________________________________________________________________________________________________________ 9) Is staff positioned correctly? _____________________________________________________________________________________________________________________________________________________________________ 10) Is the individual safe during the activity observed? _____________________________________________________________________________________________________________________________________________________________________ 11) Does the 24 Hour Support Plan appear to be appropriate for
keeping the individual safe? _____________________________________________________________________________________________________________________________________________________________________
YES NO
YES NO N/A
YES NO N/A
YES NO N/A
YES NO N/A
YES NO N/A
YES NO
YES NO
YES NO
YES NO
YES NO

DBHDD Policy: Physical and Nutritional Supports Page 2 of 2
24 HOUR SUPPORT PLAN MONITORING: NUTRITIONAL SUPPORTS
_________________________________________________________________________________________________________________________ Policy 03-522 Attachment I Version 11-01-2010
12) Does the 24 Hour Support Plan appear to be appropriate for promoting optimal independence?
_____________________________________________________________________________________________________________________________________________________________________
YES NO
III. INDIVIDUALIZED OUTCOME IMPLEMENTATION: 1) Is the learning based objective associated with nutritional
support being implemented as indicated during observation? 2) Is data being consistently recorded for learning based objective?
YES NO N/A
YES NO N/A
IV. INCIDENTAL TEACHING AND CORRECTIVE ACTION 1) Was staff able to implement plan without incidental teaching?
2) Was staff able to implement plan without intervention by the
monitor in order to keep the individual safe?
YES NO
YES NO
Describe incidental teaching opportunity and/or reason for intervention: _________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ Plan of correction: _____________________________________________________________________________________________________________________________________________________________________ __________________________________________________________________________________
As appropriate, provide praise and positive reinforcement for staff actions that reflect good practice and facilitate a positive and enjoyable dining environment. __________________________________ ____________________________ ___________________ Printed Name Signature Date and Time

DBHDD Policy: Physical and Nutritional Supports Page 1 of 3
________________________________________________________________________________________________________________________ Policy 03-522 Attachment I – Instructions Version 11-01-2010
INSTRUCTIONS: 24 HOUR SUPPORT PLAN - NUTRITIONAL SUPPORTS NAME: UNIT: AVATAR #: STAFF NAME: DATE: SHIFT: I. ACTIVITY MONITORED: BREAKFAST
LUNCH DINNER
SNACK ORAL HYGIENE
II. 24 HOUR SUPPORT PLAN IMPLEMENTATION: 1) Is the 24 Hour Support Plan for the individual accessible and
visible to staff? Score as “yes” if the plan is accessible AND visible to staff; otherwise, score as “no”. 2) Is the diet texture provided correct as indicated on the 24 Hour
Support Plan? Score as “yes” if the diet texture is provided as indicated on the 24 Hour Plan OR the staff is able to identify that texture is incorrect and obtain the correct texture from food services; otherwise, score as “no”. If observing oral hygiene, score as “n/a”. 3) Is the liquid consistency provided correct as indicated on the 24
Hour Support Plan? Score as “yes” if staff is able to serve AND/OR accurately prepare the liquid consistency indicated on the 24 Hour Plan AND adjust liquids that have been altered in consistency throughout the meal (e.g., due to change in temperature); otherwise, score as “no”. If observing oral hygiene, score as “n/a”. 4) Has all adaptive equipment listed on the 24 Hour Support Plan
been provided to the individual? Score as “yes” if ALL adaptive equipment listed on the 24 Hour Support Plan for activity being monitored has been provided, AND is set up according to the picture provided on the 24 Hour Support Plan; otherwise, score as “no”. 5) Is adaptive equipment being used properly? Score as “yes” if ALL adaptive equipment listed on the 24 Hour Support Plan for activity being monitored is being used as indicated (including correct hand preference); otherwise, score as “no”. 6) Is staff providing the level of assistance indicated on the 24 Hour
Support Plan? Score as “yes” if staff is providing the level of assistance indicated on the 24 Hour Support Plan for activity being monitored AND encouraging the optimal level of independence based on functional ability listed on plan; otherwise, score as “no”. In the space provided, document reason for “no” response (e.g., staff providing too much or inadequate assistance). 7) Is the staff providing procedures and techniques as indicated on
the 24 Hour Support Plan? Score as “yes” if staff is implementing ALL procedures and techniques indicated on the 24 Hour Support Plan for activity being monitored; otherwise, score as “no”. In the space provided, document reason for “no” response (e.g., staff used an improper
YES NO
YES NO N/A
YES NO N/A
YES NO N/A
YES NO N/A
YES NO
YES NO

DBHDD Policy: Physical and Nutritional Supports Page 2 of 3
________________________________________________________________________________________________________________________ Policy 03-522 Attachment I – Instructions Version 11-01-2010
lifting technique). 8) Is the individual positioned safely and correctly? Score as “yes” if individual is positioned as indicated by the picture listed on the 24 Hour Support Plan AND safely repositioned as needed; otherwise, score as “no”. In the space provided, document reason for “no” response (e.g., individual is not adequately aligned for eating or oral hygiene). 9) Is staff positioned correctly? Score as “yes” if staff is positioned as indicated on the 24 Hour Support Plan; otherwise, score as “no”. In the space provided, document reason for “no” response (e.g., staff positioned on the wrong side on the individual). 10) Is the individual safe during the activity observed? Score as “yes” if individual is not placed at risk during the activity observed; otherwise, score as “no”. In the space provided, document reason for “no” response (e.g., individual hyper-extended neck during eating and staff did not intervene to correct). 11) Does the 24 Hour Support Plan appear to be appropriate for
keeping the individual safe? Score as “yes” if the 24 Hour Support Plan, when implemented as written, is adequate to ensure individual safety during the activity being monitored; otherwise, score as “no”. In the space provided, document reason for “no” response (e.g., individual needs additional staff assistance for activity observed to ensure safety). 12) Does the 24 Hour Support Plan appear to be appropriate for
promoting optimal independence? Score as “yes” if the 24 Hour Support Plan, when implemented as written, is adequate to ensure that optimal functional engagement is supported during the activity being monitored; otherwise, score as “no”. In the space provided, document reason for “no” response (e.g., individual is able to perform task at a higher functional level than is listed on plan).
YES NO
YES NO
YES NO
YES NO
YES NO
III. INDIVIDUALIZED OUTCOME IMPLEMENTATION: 1) Is the learning based objective associated with nutritional
support being implemented as indicated during observation? Score as “yes” if implementation of learning based objective linked to activity being monitored is observed; otherwise, score as “no”. If a learning based objective is not clinically indicated for task being monitored, score as “n/a”. 2) Is data being consistently recorded for learning based objective? Score as “yes” if data has been consistently collected for learning based objective linked to the activity being monitored; otherwise, score as “no”. If a learning based objective is not clinically indicated for task being monitored, score as “n/a”.
YES NO N/A
YES NO N/A
IV. INCIDENTAL TEACHING AND CORRECTIVE ACTION 1) Was staff able to implement plan without incidental teaching?
Score as “yes” the staff member observed implemented the plan as indicated and did not require incidental teaching to improve compliance or performance; otherwise, score as “no”.
YES NO
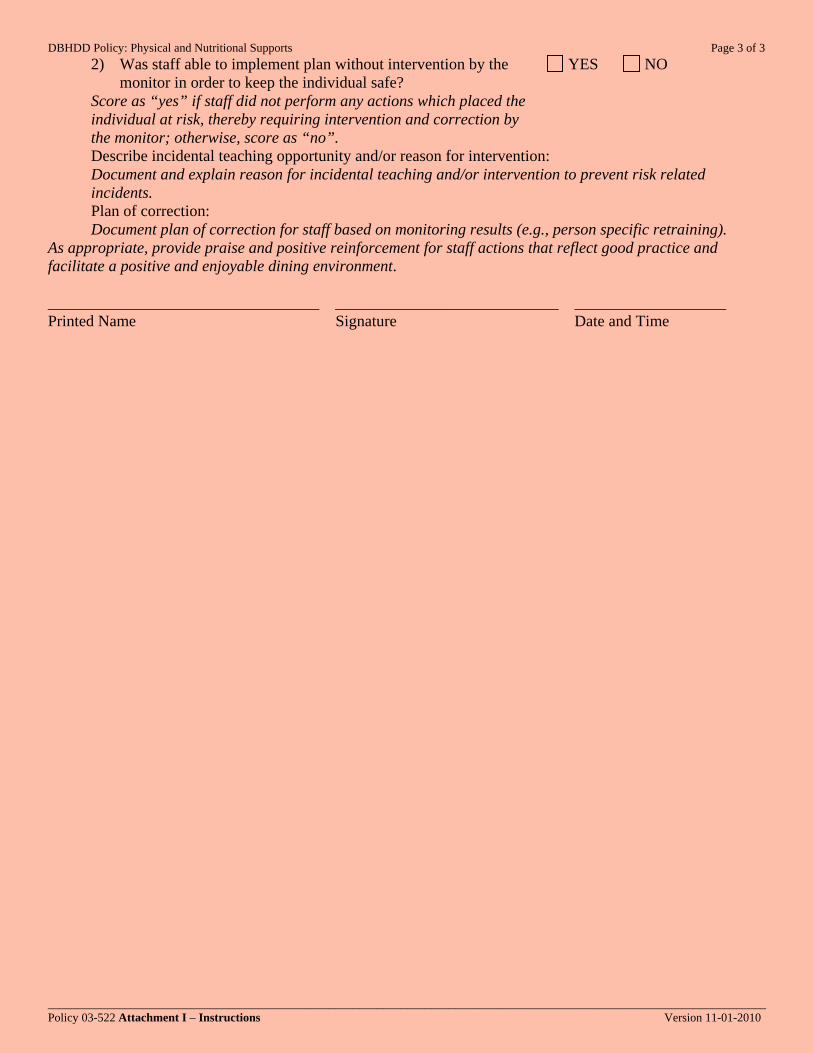
DBHDD Policy: Physical and Nutritional Supports Page 3 of 3
________________________________________________________________________________________________________________________ Policy 03-522 Attachment I – Instructions Version 11-01-2010
2) Was staff able to implement plan without intervention by the monitor in order to keep the individual safe?
Score as “yes” if staff did not perform any actions which placed the individual at risk, thereby requiring intervention and correction by the monitor; otherwise, score as “no”.
YES NO
Describe incidental teaching opportunity and/or reason for intervention: Document and explain reason for incidental teaching and/or intervention to prevent risk related incidents. Plan of correction: Document plan of correction for staff based on monitoring results (e.g., person specific retraining).
As appropriate, provide praise and positive reinforcement for staff actions that reflect good practice and facilitate a positive and enjoyable dining environment. __________________________________ ____________________________ ___________________ Printed Name Signature Date and Time

DBHDD Policy: Physical and Nutritional Supports Page 1 of 2
24 HOUR SUPPORT PLAN MONITORING - PHYSICAL SUPPORTS
_________________________________________________________________________________________________________________________ Policy 03-522 Attachment J Version 11-01-2010
NAME: UNIT: AVATAR #: STAFF NAME(S): DATE: SHIFT: I. ACTIVITY MONITORED: Select only one activity to be monitored at a time MOBILITY
TRANSFER ALTERNATE POSITIONING
BATHING DRESSING OR GROOMING WORK AND/OR EDUCATION
II. 24 HOUR SUPPORT PLAN IMPLEMENTATION: 1) Is the 24 Hour Support Plan for the individual accessible to staff?
2) Has all adaptive equipment listed on the 24 Hour Support Plan
been provided to the individual? 3) Is adaptive equipment being used properly? 4) Is staff providing the level of assistance indicated on the 24 Hour
Support Plan? _____________________________________________________________________________________________________________________________________________________________________ 5) Is the staff providing procedures and techniques as indicated on
the 24 Hour Support Plan? _____________________________________________________________________________________________________________________________________________________________________ 6) Is the individual positioned and repositioned safely and
correctly? _____________________________________________________________________________________________________________________________________________________________________ 7) Does staff use appropriate body mechanics? 8) Is the individual safe during the activity observed? _____________________________________________________________________________________________________________________________________________________________________ 9) Does the 24 Hour Support Plan appear to be appropriate for
keeping the individual safe? _____________________________________________________________________________________________________________________________________________________________________ 10) Does the 24 Hour Support Plan appear to be appropriate for
promoting optimal independence? _____________________________________________________________________________________________________________________________________________________________________
YES NO
YES NO N/A
YES NO N/A
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO

DBHDD Policy: Physical and Nutritional Supports Page 2 of 2
24 HOUR SUPPORT PLAN MONITORING - PHYSICAL SUPPORTS
_________________________________________________________________________________________________________________________ Policy 03-522 Attachment J Version 11-01-2010
III. INDIVIDUALIZED OUTCOME IMPLEMENTATION: 1) Is the learning based objective associated with physical support
being implemented as indicated during observation? 2) Is data being consistently recorded for the learning based
objective?
YES NO N/A
YES NO N/A
IV. INCIDENTAL TEACHING AND CORRECTIVE ACTION 1) Was staff able to implement plan without incidental teaching?
2) Was staff able to implement plan without intervention by the
monitor in order to ensure that the individual is safe?
YES NO
YES NO
Describe incidental teaching opportunity and/or reason for intervention: _________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________ Plan of correction: _________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
As appropriate, provide praise and reinforcement for staff actions that reflect good practice and a positive, compassionate and encouraging attitude. __________________________________ ____________________________ ___________________ Printed Name Signature Date and Time

DBHDD Policy: Physical and Nutritional Supports Page 1 of 2
________________________________________________________________________________________________________________________ Policy 03-522 Attachment J – Instructions Version 11-01-2010
INSTRUCTIONS: 24 HOUR SUPPORT PLAN - PHYSICAL SUPPORTS NAME: UNIT: AVATAR #: STAFF NAME(S): DATE: SHIFT: I. ACTIVITY MONITORED: Select only one activity to be monitored at a time MOBILITY
TRANSFER ALTERNATE POSITIONING
BATHING DRESSING OR GROOMING WORK AND/OR EDUCATION
II. 24 HOUR SUPPORT PLAN IMPLEMENTATION: 1) Is the 24 Hour Support Plan for the individual accessible to staff?
Score as “yes” if the plan is accessible and/or staff can verbalize where the plan is located; otherwise, score as “no”. 2) Has all adaptive equipment listed on the 24 Hour Support Plan
been provided to the individual? Score as “yes” if ALL adaptive equipment listed on the 24 Hour Support Plan for activity being monitored has been provided, AND is set up according to the picture provided (if picture is indicated) on the 24 Hour Support Plan; otherwise, score as “no”. 3) Is adaptive equipment being used properly? Score as “yes” if ALL adaptive equipment listed on the 24 Hour Support Plan for activity being monitored is used as indicated; otherwise, score as “no”. 4) Is staff providing the level of assistance indicated on the 24 Hour
Support Plan? Score as “yes” if staff is providing the level of assistance indicated on the 24 Hour Support Plan for activity being monitored AND encouraging the optimal level of independence based on functional ability listed on plan; otherwise, score as “no”. In the space provided, document reason for “no” response (e.g., staff providing too much or inadequate assistance). 5) Is the staff providing procedures and techniques as indicated on
the 24 Hour Support Plan? Score as “yes” if staff is implementing ALL procedures and techniques indicated on the 24 Hour Support Plan for activity being monitored; otherwise, score as “no”. In the space provided, document reason for “no” response (e.g., staff used an improper lifting technique). 6) Is the individual positioned and repositioned safely and
correctly? Score as “yes” if individual is positioned as indicated by the picture listed on the 24 Hour Support Plan (if applicable) for the activity being monitored AND safely repositioned as needed; otherwise, score as “no”. In the space provided, document reason for “no” response (e.g., individual not repositioned when pelvis slid forward in seat, leaning to left, etc.). 7) Does staff use appropriate body mechanics? Score as “yes” if staff is using appropriate body mechanics during handling AND/or lifting tasks; otherwise, score as “no”. In the space provided, document reason for “no” response. 8) Is the individual safe during the activity observed? Score as “yes” if individual is not placed at risk during the activity
YES NO
YES NO N/A
YES NO N/A
YES NO
YES NO
YES NO
YES NO
YES NO
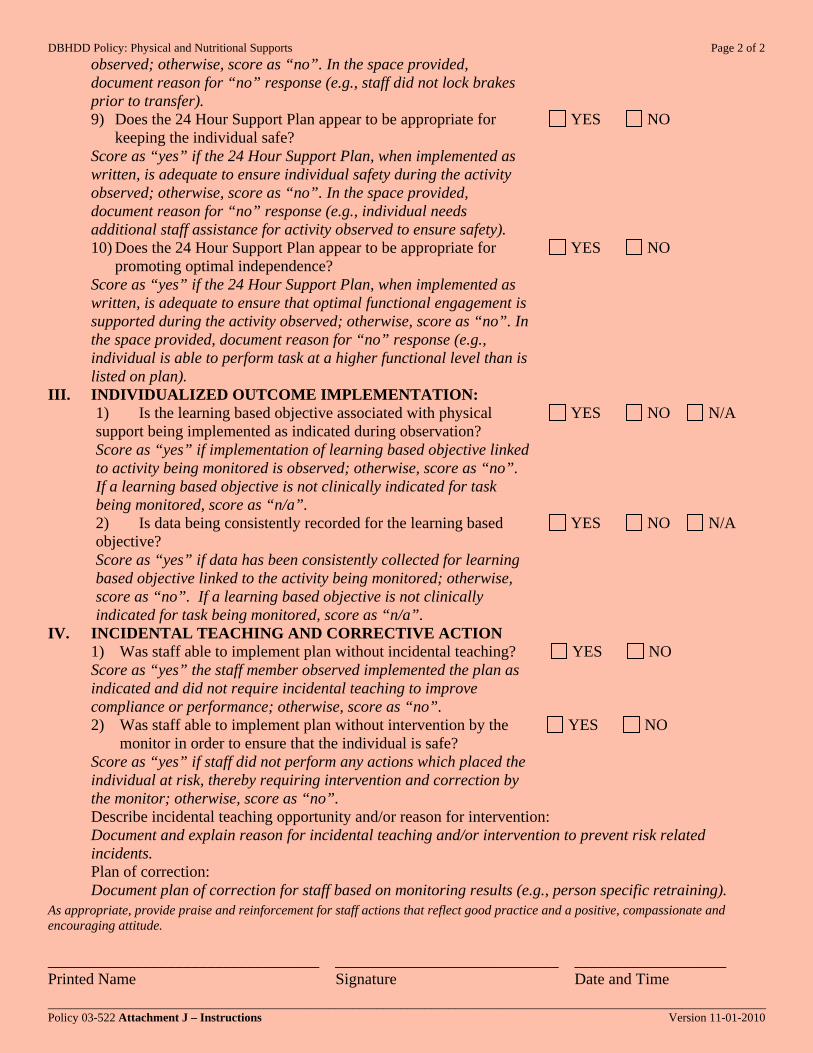
DBHDD Policy: Physical and Nutritional Supports Page 2 of 2
________________________________________________________________________________________________________________________ Policy 03-522 Attachment J – Instructions Version 11-01-2010
observed; otherwise, score as “no”. In the space provided, document reason for “no” response (e.g., staff did not lock brakes prior to transfer). 9) Does the 24 Hour Support Plan appear to be appropriate for
keeping the individual safe? Score as “yes” if the 24 Hour Support Plan, when implemented as written, is adequate to ensure individual safety during the activity observed; otherwise, score as “no”. In the space provided, document reason for “no” response (e.g., individual needs additional staff assistance for activity observed to ensure safety). 10) Does the 24 Hour Support Plan appear to be appropriate for
promoting optimal independence? Score as “yes” if the 24 Hour Support Plan, when implemented as written, is adequate to ensure that optimal functional engagement is supported during the activity observed; otherwise, score as “no”. In the space provided, document reason for “no” response (e.g., individual is able to perform task at a higher functional level than is listed on plan).
YES NO
YES NO
III. INDIVIDUALIZED OUTCOME IMPLEMENTATION: 1) Is the learning based objective associated with physical
support being implemented as indicated during observation? Score as “yes” if implementation of learning based objective linked to activity being monitored is observed; otherwise, score as “no”. If a learning based objective is not clinically indicated for task being monitored, score as “n/a”. 2) Is data being consistently recorded for the learning based objective? Score as “yes” if data has been consistently collected for learning based objective linked to the activity being monitored; otherwise, score as “no”. If a learning based objective is not clinically indicated for task being monitored, score as “n/a”.
YES NO N/A
YES NO N/A
IV. INCIDENTAL TEACHING AND CORRECTIVE ACTION 1) Was staff able to implement plan without incidental teaching?
Score as “yes” the staff member observed implemented the plan as indicated and did not require incidental teaching to improve compliance or performance; otherwise, score as “no”. 2) Was staff able to implement plan without intervention by the
monitor in order to ensure that the individual is safe? Score as “yes” if staff did not perform any actions which placed the individual at risk, thereby requiring intervention and correction by the monitor; otherwise, score as “no”.
YES NO
YES NO
Describe incidental teaching opportunity and/or reason for intervention: Document and explain reason for incidental teaching and/or intervention to prevent risk related incidents. Plan of correction: Document plan of correction for staff based on monitoring results (e.g., person specific retraining).
As appropriate, provide praise and reinforcement for staff actions that reflect good practice and a positive, compassionate and encouraging attitude. __________________________________ ____________________________ ___________________ Printed Name Signature Date and Time

Policy #03-522: Physical and Nutritional Supports
Attachment K: Hospital Specific Details for PNS Policy Implementation
Click on a hospital to view details
Central State Hospital
East Central Regional Hospital
Georgia Regional Hospital – Atlanta
Georgia Regional Hospital – Savannah
Northwest Georgia Regional Hospital
Southwestern State Hospital
West Central Georgia Regional Hospital
Click here to return to Policy

DBHDD: Physical and Nutritional Support Page 1of 8
Central State Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
The left-hand column of this table lists the section(s) of the policy for which these details are relevant (policy page # and outline letter/number). I. PNS notification (i.e., referral) process: A. Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
1. How will clinicians be notified to do risk assessments for choking and aspiration, fall and decubitus ulcer?
DDS LTC & FS 1. The nurse (LPN or RN) who did the
screen will immediately inform the medical staff via phone call or page. If the risk assessment is indicated outside of the screening process, the ranking nurse on that unit will immediately inform the medical staff via phone call or page.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
2. Who will do the notification? DDS LTC & FS 2. The ranking nurse or the nurse who
completed the screen. Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
3. Will notification be done by email, phone, and/or paper referral, and how will receipt of referral be documented?
DDS LTC & FS 3. Via phone call or page, with
documentation of the call in the progress notes.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
DDS & LTC 4. 24/7. If the On Duty Physician does the
Risk Assessment, the Attending Medical Staff must review that assessment and co-sign the assessment if he/she is in agreement, or document in the progress notes his/her disagreement with the assessment, including why, and immediately complete a reassessment. The physician identifies appropriate team members who need to respond according to circumstances. The on-duty Unit Nurse will call the team leader who will notify the individual(s) who should report to develop the 24 Hour Plan.
Forensics 4. 24/7. If the On Duty Physician does the
Risk Assessment, the Attending Medical Staff must review that assessment and co-sign the assessment if he/she is in agreement, or document in the progress notes his/her disagreement with the assessment, including why, and immediately complete a reassessment. The Attending Physician identifies appropriate team members who need to respond according to circumstances and notifies the Unit Nurse/Charge Nurse or Unit Clerk. The Unit Nurse/Charge Nurse or Unit Clerk will then notify the individual(s) who should report to develop the 24 Hour Plan.
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 2of 8
Central State Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
5. Would staff be on call in the event that a risk assessment needs to be performed?
DDS, LTC & FS 5. Yes- Medical staff and nurses will be
available 24/7. Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
6. How quickly will notification occur? (e.g., If potential risk identified Friday at 10 p.m., when will designee be notified?)
DDS, LTC & FS 6. Upon identification of potential risk.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
7. How will notification be logged? DDS, LTC & FS 7. In the progress notes to include the time,
date, to whom the contact was made, and outcome of the conversation.
Pg. 3-4 a.ii Pg. 5 b.ii Pg. 6 c.ii
8. If an individual is identified to be at potential risk for choking and aspiration, falls, and/or decubitus, who will be responsible for ordering the initial treatment plan to protect the individual until risk assessment and/or evaluations are completed?
DDS, LTC & FS 8. The Physician responding to the request
for completion of a risk assessment.
B. Pg. 12 F.i.a 1. How will dietitians be notified to
do assessments for individuals at potential nutritional risk?
DDS, LTC & FS 1. The dietitian and other treatment team
members needed to ensure safety will be notified by the Physicians or the Physician’s designee ( such as the ranking or Unit Nurse, Charge Nurse or Unit Clerk).
Pg. 12 F.i.a 2. Who will do the notification?
DDS LTC & FS 2. The ranking nurse who completed the
screen.
Pg. 12 F.i.a 3. Will notification be done by email, phone, and/or paper referral, and how will receipt of referral be documented?
DDS, LTC & FS 3. Phone call or pro-page with
documentation of the calls or pro-pages in the progress notes.
Pg. 12 F.i.a 4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
DDS, LTC & FS 4. 24/7. The unit dietitian will be called or
pro-paged during typical business hours; otherwise, on-call dietitian is called or pro-paged.
Pg. 12 F.i.a 5. Would staff be on call in the event that a 24 hour assessment needs to be performed?
DDS, LTC & FS 5. Yes.
Pg. 12 F.i.a 6. How quickly will notification occur? (e.g., If potential risk identified Friday at 10 p.m., when will designee be notified?)
DDS, LTC & FS 6. Upon identification of potential risk.
Pg. 12 F.i.a 7. How will notification be logged? DDS, LTC & FS 7. In the progress notes to include the time,
date, to who the contact was made, and outcome of the conversation.
DBHDD Policy 03-522 Attachment K Version 5-4-2010
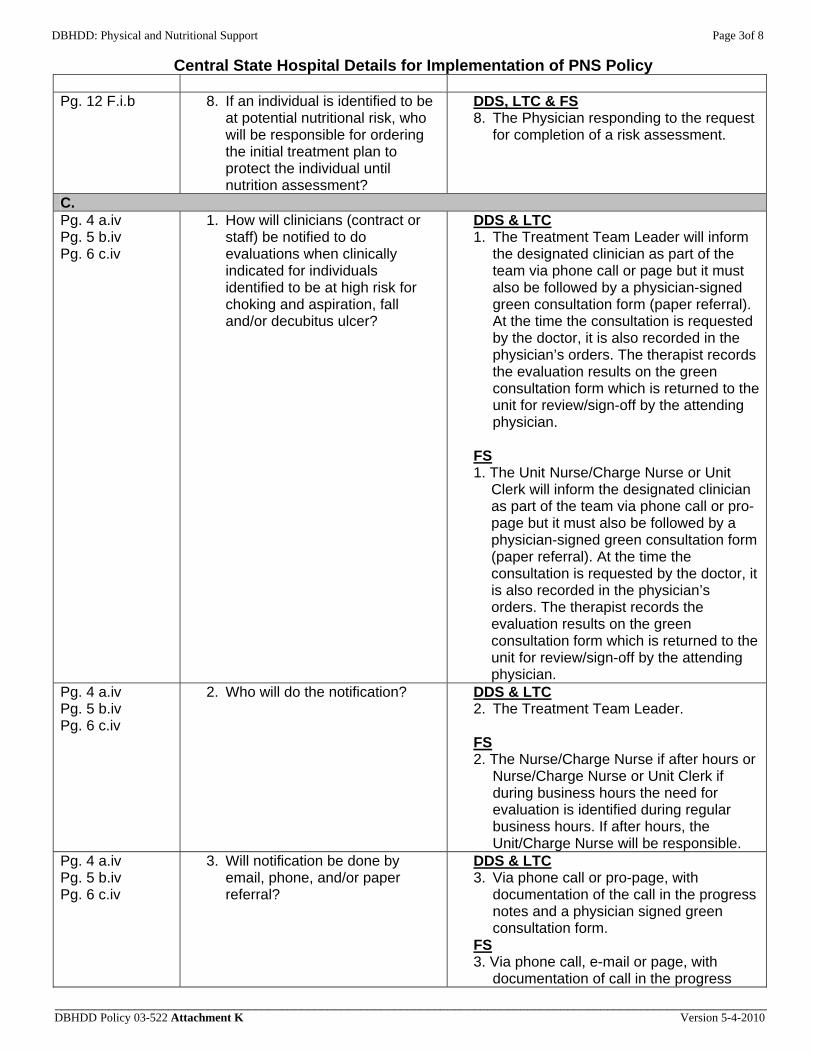
DBHDD: Physical and Nutritional Support Page 3of 8
Central State Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
Pg. 12 F.i.b 8. If an individual is identified to be
at potential nutritional risk, who will be responsible for ordering the initial treatment plan to protect the individual until nutrition assessment?
DDS, LTC & FS 8. The Physician responding to the request
for completion of a risk assessment.
C. Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
1. How will clinicians (contract or staff) be notified to do evaluations when clinically indicated for individuals identified to be at high risk for choking and aspiration, fall and/or decubitus ulcer?
DDS & LTC 1. The Treatment Team Leader will inform
the designated clinician as part of the team via phone call or page but it must also be followed by a physician-signed green consultation form (paper referral). At the time the consultation is requested by the doctor, it is also recorded in the physician’s orders. The therapist records the evaluation results on the green consultation form which is returned to the unit for review/sign-off by the attending physician.
FS 1. The Unit Nurse/Charge Nurse or Unit
Clerk will inform the designated clinician as part of the team via phone call or pro-page but it must also be followed by a physician-signed green consultation form (paper referral). At the time the consultation is requested by the doctor, it is also recorded in the physician’s orders. The therapist records the evaluation results on the green consultation form which is returned to the unit for review/sign-off by the attending physician.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
2. Who will do the notification? DDS & LTC 2. The Treatment Team Leader. FS 2. The Nurse/Charge Nurse if after hours or
Nurse/Charge Nurse or Unit Clerk if during business hours the need for evaluation is identified during regular business hours. If after hours, the Unit/Charge Nurse will be responsible.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
3. Will notification be done by email, phone, and/or paper referral?
DDS & LTC 3. Via phone call or pro-page, with
documentation of the call in the progress notes and a physician signed green consultation form.
FS 3. Via phone call, e-mail or page, with
documentation of call in the progress
DBHDD Policy 03-522 Attachment K Version 5-4-2010
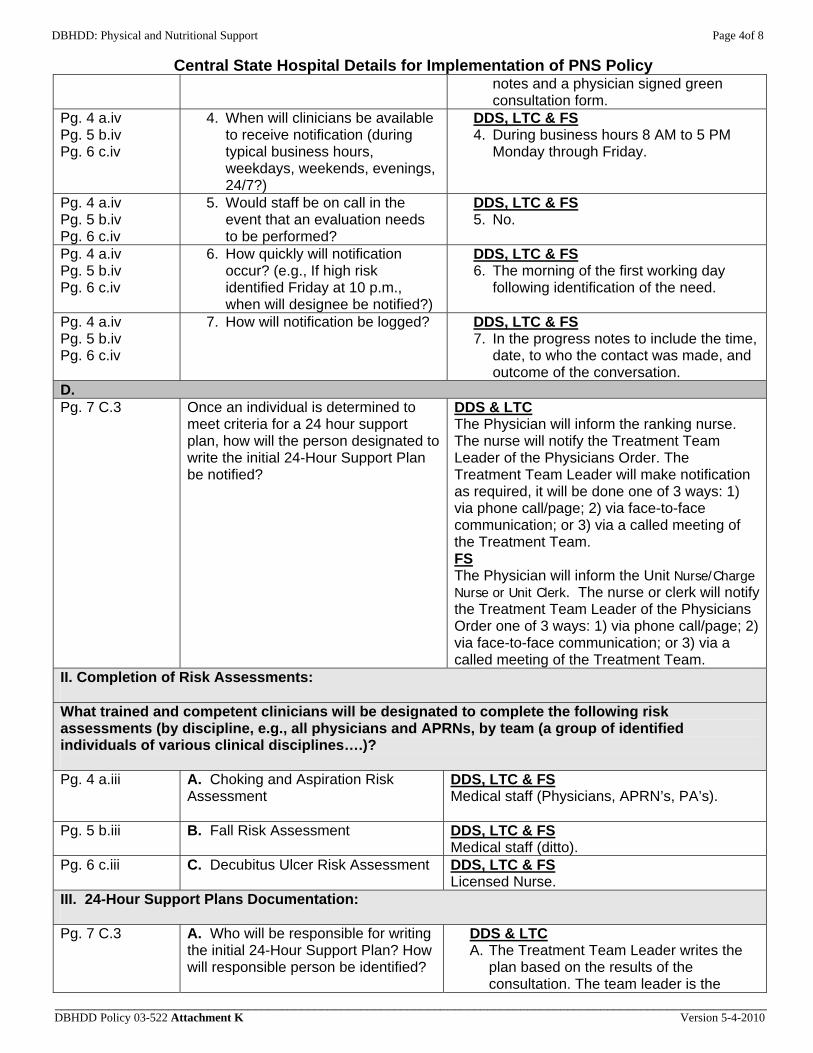
DBHDD: Physical and Nutritional Support Page 4of 8
Central State Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
notes and a physician signed green consultation form.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
DDS, LTC & FS 4. During business hours 8 AM to 5 PM
Monday through Friday.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
5. Would staff be on call in the event that an evaluation needs to be performed?
DDS, LTC & FS 5. No.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
6. How quickly will notification occur? (e.g., If high risk identified Friday at 10 p.m., when will designee be notified?)
DDS, LTC & FS 6. The morning of the first working day
following identification of the need.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
7. How will notification be logged?
DDS, LTC & FS 7. In the progress notes to include the time,
date, to who the contact was made, and outcome of the conversation.
D. Pg. 7 C.3 Once an individual is determined to
meet criteria for a 24 hour support plan, how will the person designated to write the initial 24-Hour Support Plan be notified?
DDS & LTC The Physician will inform the ranking nurse. The nurse will notify the Treatment Team Leader of the Physicians Order. The Treatment Team Leader will make notification as required, it will be done one of 3 ways: 1) via phone call/page; 2) via face-to-face communication; or 3) via a called meeting of the Treatment Team. FS The Physician will inform the Unit Nurse/Charge Nurse or Unit Clerk. The nurse or clerk will notify the Treatment Team Leader of the Physicians Order one of 3 ways: 1) via phone call/page; 2) via face-to-face communication; or 3) via a called meeting of the Treatment Team.
II. Completion of Risk Assessments:
What trained and competent clinicians will be designated to complete the following risk assessments (by discipline, e.g., all physicians and APRNs, by team (a group of identified individuals of various clinical disciplines….)? Pg. 4 a.iii A. Choking and Aspiration Risk
Assessment
DDS, LTC & FS Medical staff (Physicians, APRN’s, PA’s).
Pg. 5 b.iii B. Fall Risk Assessment
DDS, LTC & FS Medical staff (ditto).
Pg. 6 c.iii C. Decubitus Ulcer Risk Assessment DDS, LTC & FS Licensed Nurse.
III. 24-Hour Support Plans Documentation:
Pg. 7 C.3 A. Who will be responsible for writing the initial 24-Hour Support Plan? How will responsible person be identified?
DDS & LTC A. The Treatment Team Leader writes the
plan based on the results of the consultation. The team leader is the
DBHDD Policy 03-522 Attachment K Version 5-4-2010
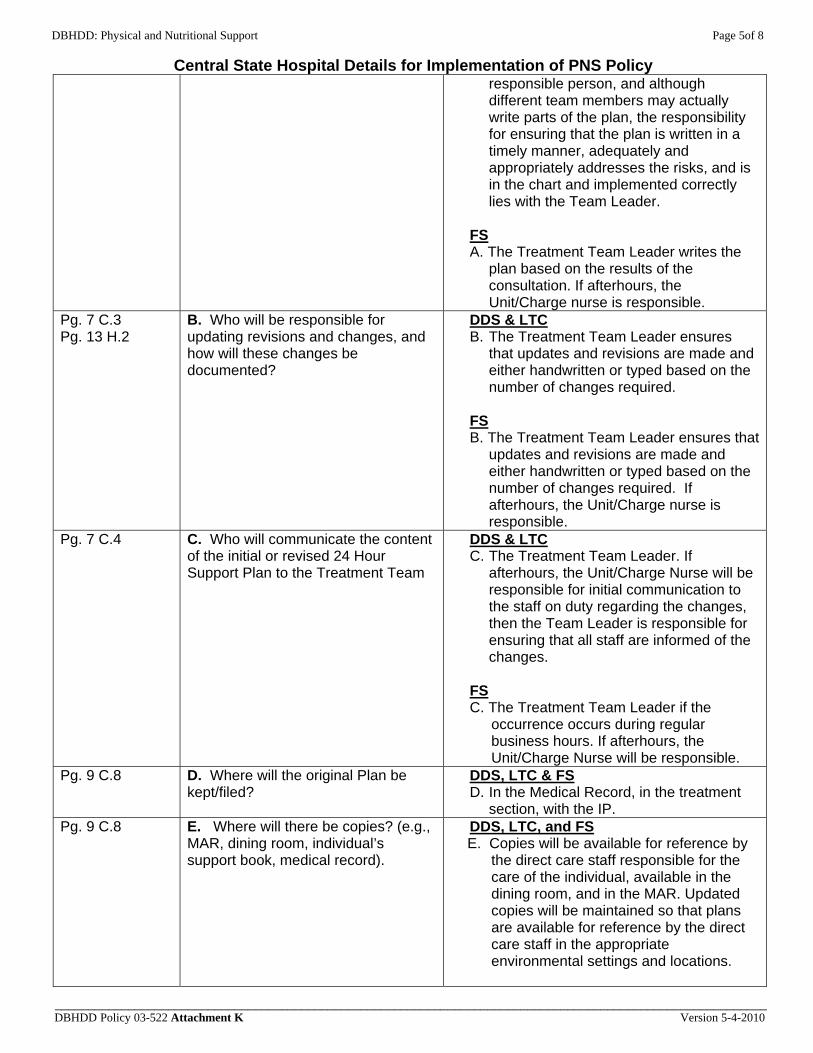
DBHDD: Physical and Nutritional Support Page 5of 8
Central State Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
responsible person, and although different team members may actually write parts of the plan, the responsibility for ensuring that the plan is written in a timely manner, adequately and appropriately addresses the risks, and is in the chart and implemented correctly lies with the Team Leader.
FS A. The Treatment Team Leader writes the
plan based on the results of the consultation. If afterhours, the Unit/Charge nurse is responsible.
Pg. 7 C.3 Pg. 13 H.2
B. Who will be responsible for updating revisions and changes, and how will these changes be documented?
DDS & LTC B. The Treatment Team Leader ensures
that updates and revisions are made and either handwritten or typed based on the number of changes required.
FS B. The Treatment Team Leader ensures that
updates and revisions are made and either handwritten or typed based on the number of changes required. If afterhours, the Unit/Charge nurse is responsible.
Pg. 7 C.4 C. Who will communicate the content of the initial or revised 24 Hour Support Plan to the Treatment Team
DDS & LTC C. The Treatment Team Leader. If
afterhours, the Unit/Charge Nurse will be responsible for initial communication to the staff on duty regarding the changes, then the Team Leader is responsible for ensuring that all staff are informed of the changes.
FS C. The Treatment Team Leader if the
occurrence occurs during regular business hours. If afterhours, the Unit/Charge Nurse will be responsible.
Pg. 9 C.8 D. Where will the original Plan be kept/filed?
DDS, LTC & FS D. In the Medical Record, in the treatment
section, with the IP. Pg. 9 C.8 E. Where will there be copies? (e.g.,
MAR, dining room, individual’s support book, medical record).
DDS, LTC, and FS E. Copies will be available for reference by
the direct care staff responsible for the care of the individual, available in the dining room, and in the MAR. Updated copies will be maintained so that plans are available for reference by the direct care staff in the appropriate environmental settings and locations.
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 6of 8
Central State Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
Pg. 9 C.8 F. Who is responsible for distributing copies and ensuring copies are updated with any change to the Plan?
DDS & LTC F. The Treatment Team Leader. FS F. The Treatment Team Leader for distribution during regular business hours. If afterhours, the Unit/Charge Nurse or Unit Clerk will be responsible.
IV. Protocol for communication with the TREATMENT TEAM:
A. TREATMENT TEAM approval of the 24-Hour Support Plans (new and revised):
Pg. 7 C.4 1. What is the process by which the Treatment Team approves initial and revised plans?
DDS, LTC & FS 1. The Treatment Team will have a meeting
that includes the core team members and any others who are responsible for the development and ensuring the proper utilization of the Plan.
Pg. 7.C.4 2. Can approval be done by email, verbally, or may it require a special team meeting when clinically appropriate?
DDS, LTC & FS 2. A Special face to face Team Meeting
must be held. The meeting will be documented in the medical record.
Pg. 4 a.iii. Pg. 4 a.iv Pg. 5 b.iii Pg. 5 b.iv Pg. 6 c.iii Pg. 6 c.iv Pg. 12 F.i.c Pg. 14 H.3
How and when will clinicians doing the PNS Risk Screen, Risk Assessments, and/or evaluations report their findings to the other members of the Treatment Team (besides those immediately notified according to PNS procedure)? (e.g., At the next regularly scheduled Treatment Team meeting? At morning unit meetings? Email? etc.)
DDS, LTC & FS All outcomes of screenings and risk assessments for individuals who do not meet criteria for a 24 hour support plan will be discussed at the next regularly scheduled Treatment Team meeting. If the risk assessment determines that the individual is at high risk and a 24 Hour Support Plan needs to be immediately implemented, a called meeting of the Treatment Team will be held. The Treatment Team will be notified via phone, e-mail or pro-page and the notification documented to include the time, date, team members contacted and outcome(s) of the conversation(s).
V. Who will train family, visitors, and significant others on the 24-Hour Support Plan?
Pg. 9.C.9.a.i DDS, LTC & FS The licensed nurse and Treatment Team Leader will ensure that family, etc., who regularly visit or take the client home for visits are trained on the Plan and/or changes in the Plan at the first opportunity following formulation/change. The Ranking Nurse who is providing hand-off communication prior to a visit (home, TV) will ensure that the family or staff receiving the client has been or is trained at the time of transfer of responsibility. This training is documented on the Trial Visit Temporary Leave Instruction Form CSH # 365 or 385 which is filed in the Medical Record , and an entry is made in the progress notes.
VI. Dietitian vs. Nurse: Who trends weights and enters/tracks the data?
Pg. 13 F.6 DDS, LTC & FS The Dietitian quarterly. The Licensed Nurse monthly or more often if clinically indicated. Both disciplines are responsible for a progress note, and notification of the medical staff of identified concerns.
DBHDD Policy 03-522 Attachment K Version 5-4-2010
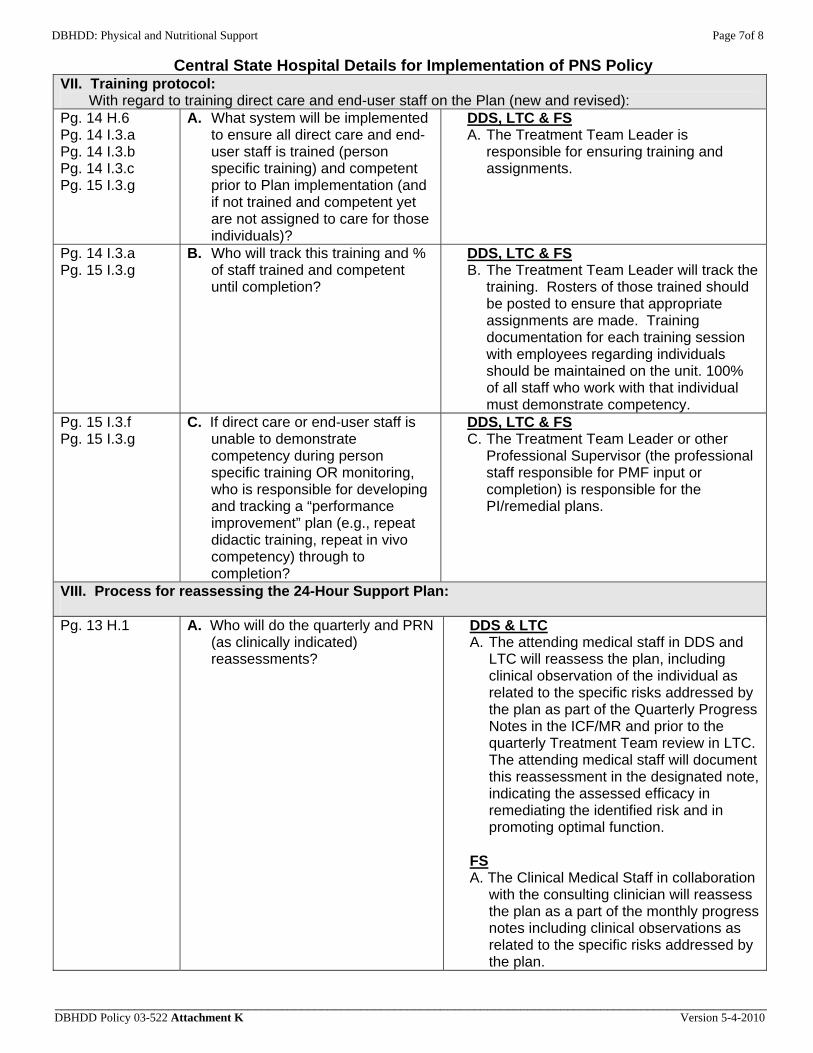
DBHDD: Physical and Nutritional Support Page 7of 8
Central State Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
VII. Training protocol: With regard to training direct care and end-user staff on the Plan (new and revised): Pg. 14 H.6 Pg. 14 I.3.a Pg. 14 I.3.b Pg. 14 I.3.c Pg. 15 I.3.g
A. What system will be implemented to ensure all direct care and end-user staff is trained (person specific training) and competent prior to Plan implementation (and if not trained and competent yet are not assigned to care for those individuals)?
DDS, LTC & FS A. The Treatment Team Leader is
responsible for ensuring training and assignments.
Pg. 14 I.3.a Pg. 15 I.3.g
B. Who will track this training and % of staff trained and competent until completion?
DDS, LTC & FS B. The Treatment Team Leader will track the
training. Rosters of those trained should be posted to ensure that appropriate assignments are made. Training documentation for each training session with employees regarding individuals should be maintained on the unit. 100% of all staff who work with that individual must demonstrate competency.
Pg. 15 I.3.f Pg. 15 I.3.g
C. If direct care or end-user staff is unable to demonstrate competency during person specific training OR monitoring, who is responsible for developing and tracking a “performance improvement” plan (e.g., repeat didactic training, repeat in vivo competency) through to completion?
DDS, LTC & FS C. The Treatment Team Leader or other
Professional Supervisor (the professional staff responsible for PMF input or completion) is responsible for the PI/remedial plans.
VIII. Process for reassessing the 24-Hour Support Plan:
Pg. 13 H.1 A. Who will do the quarterly and PRN (as clinically indicated) reassessments?
DDS & LTC A. The attending medical staff in DDS and
LTC will reassess the plan, including clinical observation of the individual as related to the specific risks addressed by the plan as part of the Quarterly Progress Notes in the ICF/MR and prior to the quarterly Treatment Team review in LTC. The attending medical staff will document this reassessment in the designated note, indicating the assessed efficacy in remediating the identified risk and in promoting optimal function.
FS A. The Clinical Medical Staff in collaboration
with the consulting clinician will reassess the plan as a part of the monthly progress notes including clinical observations as related to the specific risks addressed by the plan.
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 8of 8
Central State Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________ DBHDD Policy 03-522 Attachment K Version 5-4-2010
Pg. 13 H.1 B. Who will track when they are due and how will it be tracked?
DDS, LTC & FS B. The Treatment Team Leader will use a
database.
Pg. 13 H.1 Pg. 13 H.2
C. What will these reassessments consist of and how will they be documented (e.g., IDN, progress notes) and communicated to the Treatment Team, along with recommendations (i.e., revise Plan or continue with no changes?).
DDS, LTC & FS C. The reassessment will include a clinical
observation of the individual to assess the plan’s efficacy in remediating risk and promoting function. The team will review for the occurrence of any related triggers, any changes in condition, general health changes (gradual or acute), and review reports of problems by the direct care staff. If any of these are positive, the Medical Staff will revise the related re-assessment and, immediately upon completion, report the results back to the Treatment Team through the Team Leader. Any changes in the 24-hour Support Plan that are indicated will be made and implemented immediately, via the process delineated above.

DBHDD: Physical and Nutritional Support Page 1of 7
East Central Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
The left-hand column of this table lists the section(s) of the policy for which these details are relevant (policy page # and outline letter/number). I. PNS notification (i.e., referral) process: A. Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
1. How will clinicians be notified to do risk assessments for choking and aspiration, fall and decubitus ulcer?
The Registered Nurse completing the initial screening (admission, annual and upon change in status) will notify the Physician and the Nurse Manager or Charge Nurse by telephone, immediately upon completion of the Physical and Nutritional Supports Risk Screen. The Nurse Manager or Charge Person will notify Dietitian.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
2. Who will do the notification? The Registered Nurse completing the initial screening will notify the Physician by telephone immediately upon completion of the Physical and Nutritional Supports Risk Screen.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
3. Will notification be done by email, phone, and/or paper referral, and how will receipt of referral be documented?
Notification by telephone. Documentation by Progress Note.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
A Physician will be available to receive notification 24 hours a day, 7 days a week.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
5. Would staff be on call in the event that a risk assessment needs to be performed?
A Physician will be available to receive notification 24 hours a day, 7 days a week.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
6. How quickly will notification occur? (e.g., If potential risk identified Friday at 10 p.m., when will designee be notified?)
Immediately upon completion of the Physical and Nutritional Supports Risk Screen.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
7. How will notification be logged?
The Nurse will document on Physical and Nutritional Supports Risk Screening of notification and on Progress Note form in the individual’s record on the Gracewood Campus and in the Progress Note on the Augusta Campus.
Pg. 3-4 a.ii Pg. 5 b.ii Pg. 6 c.ii
8. If an individual is identified to be at potential risk for choking and aspiration, falls, and/or decubitus, who will be responsible for ordering the initial treatment plan to protect the individual until risk assessment and/or evaluations are completed?
The Physician and/or Physician Assistant
B. Pg. 12 F.i.a 1. How will dietitians be notified
to do assessments for individuals at potential
The Registered Nurse completing the initial screening (admission, annual and upon change in status) will notify the Nurse Manager
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 2of 7
East Central Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
nutritional risk?
or Charge Nurse by telephone, immediately upon completion of the Physical and Nutritional Supports Risk Screen. The Nurse Manager or Charge Person will notify Dietitian via e-mail Monday – Friday between the hours of 8:00 a.m. – 4:30 pm.
Pg. 12 F.i.a 2. Who will do the notification?
Nurse Manager or Charge Nurse in the absence of Nurse Manager.
Pg. 12 F.i.a 3. Will notification be done by email, phone, and/or paper referral, and how will receipt of referral be documented?
Via e-mail Monday – Friday between 8:00a.m.– 4:30pm The Nurse will document on Physical and Nutritional Supports Risk Screening of notification. Additionally, the Nurse will document notification on PROGRESS NOTES form in the individual’s record. Documentation of receipt of referral will be on PROGRESS NOTES.
Pg. 12 F.i.a 4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
Monday – Friday between 8:00a.m.– 4:30pm
Pg. 12 F.i.a 5. Would staff be on call in the event that a 24 hour assessment needs to be performed?
No
Pg. 12 F.i.a 6. How quickly will notification occur? (e.g., If potential risk identified Friday at 10 p.m., when will designee be notified?)
Notification will be sent immediately upon Physician’s Orders. Dietitians will receive notification of the need for evaluation upon the start of the first working day following notification.
Pg. 12 F.i.a 7. How will notification be logged?
The Nurse will document notification on Physical and Nutritional Supports Risk Screening and on PROGRESS NOTES. Documentation of receipt of referral will be on PROGRESS NOTES.
Pg. 12 F.i.b 8. If an individual is identified to be at potential nutritional risk, who will be responsible for ordering the initial treatment plan to protect the individual until nutrition assessment?
In the event the Risk Screen Assessment indicates the potential for nutritional risk, the Physician will order interventions that will be implemented until a full assessment and/or evaluation is completed.
C. Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
1. How will clinicians (contract or staff) be notified to do evaluations when clinically indicated for individuals identified to be at high risk for choking and aspiration, fall and/or decubitus ulcer?
OT/PT, Speech Therapists, Dietitians, and Statistical Technician will be notified via e-mail immediately upon Physician’s order by the Nurse Manager or Charge Nurse in the absence of Nurse Manager.
Pg. 4 a.iv 2. Who will do the notification? Nurse Manager or Charge Nurse in the
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 3of 7
East Central Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
Pg. 5 b.iv Pg. 6 c.iv
absence of Nurse Manager.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
3. Will notification be done by email, phone, and/or paper referral?
E-mail Physician’s referral/consult not required. Physician’s order for Speech Therapy Bedside Swallow Study will be written as needed.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
Monday – Friday between 8:00a.m – 4:30pm.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
5. Would staff be on call in the event that an evaluation needs to be performed?
Clinicians (OT/PT, Speech Therapists, Dietitians) will not be on call outside of normal business hours (i.e., Monday – Friday between 8:00am – 4:30pm).
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
6. How quickly will notification occur? (e.g., If high risk identified Friday at 10 p.m., when will designee be notified?)
Notification will be sent immediately upon Physician’s Orders. Clinicians (OT/PT, Speech Therapists, Dietitians) will receive notification of the need for evaluation upon the start of the first working day following notification.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
7. How will notification be logged?
The Nurse will document on PROGRESS NOTES form on the Gracewood Campus and in the Progress Note in the individual’s record on the Augusta Campus. Documentation of receipt of referral will be on PROGRESS NOTES on the Gracewood Campus and in the Progress Note in the individual’s record on the Augusta Campus. Notifications will be logged and tracked by the Statistical Technician on the Gracewood campus and by the designated Program Assistant on the Augusta Campus.
D. Pg. 7 C.3 Once an individual is determined to
meet criteria for a 24 hour support plan, how will the person designated to write the initial 24-Hour Support Plan be notified?
The clinicians completing the assessment and/or evaluation will email the information for the 24 Hour Support Plan to the assigned QMRP/Team Leader (DD) or Registered Nurse (MH).
II. Completion of Risk Assessments:
What trained and competent clinicians will be designated to complete the following risk assessments (by discipline, e.g., all physicians and APRNs, by team (a group of identified individuals of various clinical disciplines….)? Pg. 4 a.iii A. Choking and Aspiration Risk
Assessment The Physician and/or the Physician’s Assistant will be responsible
Pg. 5 b.iii B. Fall Risk Assessment
The Physician and/or the Physician’s Assistant will be responsible
Pg. 6 c.iii C. Decubitus Ulcer Risk Assessment
The Physician and/or the Physician’s Assistant will be responsible
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 4of 7
East Central Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
III. 24-Hour Support Plans Documentation:
Pg. 7 C.3 A. Who will be responsible for writing the initial 24-Hour Support Plan? How will responsible person be identified?
The assigned QMRP/Team Leader(DD) and Registered Nurse (MH) will be the main authors, and be responsible for gathering and incorporating information from discipline specific assessments and evaluations. Write access will be given to QMRP/Team Leader and Program Assistant (DD) and Nurse Manager and Program Assistant (MH).
Pg. 7 C.3 Pg. 13 H.2
B. Who will be responsible for updating revisions and changes, and how will these changes be documented?
The assigned QMRP/Team Leader (DD) and Registered Nurse (MH). Write access will be given to QMRP/Team Leader and Program Assistant (DD) and Nurse Manager and Program Assistant (MH). Revisions/changes will be documented directly on the 24 Hour Support Plan. Plans will be handwritten initially until typed.
Pg. 7 C.4 C. Who will communicate the content of the initial or revised 24 Hour Support Plan to the Treatment Team?
Clinicians responsible for completing assessments will be responsible communicating information to the QMRP/Team Leader and the Treatment Team.
Pg. 9 C.8 D. Where will the original Plan be kept/filed? Where will there be copies (e.g., MAR, dining room, individual’s support book, medical record). Who is responsible for distributing copies and ensuring copies are updated with any change to the Plan?
Original hard copy will be in the individual’s medical record. Copies will be posted in each Dining Room (Dining room copy needs to be laminated), MAR, Group book. Copy of the 24-Hour Support Plan will be saved on the facility server. QMRP/Team Leaders (DD) and Registered Nurse (MH) will be responsible for distributing and updating the plans.
IV. Protocol for communication with the TREATMENT TEAM:
A. TREATMENT TEAM approval of the 24-Hour Support Plans (new and revised):
Pg. 7 C.4 1. What is the process by which the Treatment Team approves initial and revised plans?
Team meeting with documented minutes. Upon completion of the discipline specific assessments, discipline specific summaries will be sent to the assigned QMRP/Team Leader (DD) and Registered Nurse (MH) to compile into the “Physical & Nutritional Team Summary”. The Physical & Nutritional Team Summary will be reviewed/discussed as part of the Interdisciplinary Team Meeting.
Pg. 7.C.4 2. Can approval be done by email, verbally, or may it require a special team meeting when clinically appropriate?
Revisions are based on prioritization: Minor Changes, such as changes in type of adaptive eating equipment, diet, can be approved verbally in Morning Report (DD) and Treatment Team Meeting (MH) and documented by the initiating professional on the DD425 form (DD) and progress note (MH). Major Changes involving multiple Team
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 5of 7
East Central Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
Members in development of the interventions will require a Treatment Team Meeting.
B. Pg. 4 a.iii. Pg. 4 a.iv Pg. 5 b.iii Pg. 5 b.iv Pg. 6 c.iii Pg. 6 c.iv Pg. 12 F.i.c Pg. 14 H.3
How and when will clinicians doing the PNS Risk Screen, Risk Assessments, and/or evaluations report their findings to the other members of the Treatment Team (besides those immediately notified according to PNS procedure)? (e.g., At the next regularly scheduled Treatment Team meeting? At morning unit meetings? Email? etc.)
During morning report, with documentation in the minutes on the Gracewood Campus and during Treatment Team meetings with documentation in the progress note in the individual’s record on the Augusta Campus.
V. Who will train family, visitors, and significant others on the 24-Hour Support Plan?
Pg. 9.C.9.a.i A copy of the 24-Hour Support Plan will be sent to families as part of the annual Post-Staffing packet; however initially a letter explaining the Physical and Nutritional Support Plan will be sent to all families by the assigned Social Services Provider. During family visits with individuals, the assigned nurse will review the 24-Hour Support Plan and provide a copy to the family. The nurse will document this process on the Family Education Form.
VI. Dietitian vs. Nurse: Who trends weights and enters/tracks the data?
Pg. 13 F.6 The Dietitian trends weight data and findings are discussed at each quarterly Periodic Health Review (DD) and during Treatment Teams (MH).
VII. Training protocol: With regard to training direct care and end-user staff on the Plan (new and revised): Pg. 14 H.6 Pg. 14 I.3.a Pg. 14 I.3.b Pg. 14 I.3.c Pg. 15 I.3.g
A. What system will be implemented to ensure all direct care and end-user staff is trained (person specific training) and competent prior to Plan implementation (and if not trained and competent yet are not assigned to care for those individuals)?
Policy Training for Current Employees: A training schedule for PNS will be published by the Training Program Administrator hospital-wide monthly until all current staff are trained. Training Program Administrator will send out the list of staff that has not completed and did not pass the course. Managers/Supervisor will register staff based on the list. New Employee Training: New employee will be training during Statewide Basic orientation. PNS Instructors indicated on the training roster if the staff does not pass the PNS Course. Those staff does not receive credit for the course and remains on the incomplete list. To pass the course staff must pass all the return demonstrations (if applies) and PNS exam. The Training Program Administrator will track this training and % of staff training until completion. Person Specific Training: ECRH recommends mini teams for each living area. Mini teams will consist of, but not limited
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 6of 7
East Central Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
to: Team Leader, Shift Supervisor, Night Shift Supervisor Monitor, OT staff, PT, Speech, Dietitian, and Nurse. The mini teams will work together to ensure all staff are trained on each living area. Team Leader will ensure that only trained staff are assigned to individuals. Documentation will be on Direct Care Competency Assessment Form: 24-Hour Support Plan Training. This is a separate form. Training will be filed per individual employee competency file.
Pg. 14 I.3.a Pg. 15 I.3.g
B. Who will track this training and % of staff trained and competent until completion?
The Shift Supervisor Trainers (DD) and the Nurse Manager or designee (MH) will track training and competency for staff.
Pg. 15 I.3.f Pg. 15 I.3.g
C. If direct care or end-user staff is unable to demonstrate competency during person specific training OR monitoring, who is responsible for developing and tracking a “performance improvement” plan (e.g., repeat didactic training, repeat in vivo competency) through to completion?
The Shift Supervisor Trainers (DD) and the Nurse Manager or Charge Nurse in the absence of Nurse manager (MH) will track training and competency for staff. Team Leaders will follow through on PI plans.
VIII. Process for reassessing the 24-Hour Support Plan:
Pg. 13 H.1 A. Who will do the quarterly and PRN (as clinically indicated) reassessments?
ECRH staff who received the training provided by the experts (Occupational Therapists, Physical Therapist, Speech Therapists, Dietitian and Nurse).
Pg. 13 H.1 B. Who will track when they are due and how will it be tracked?
On the Gracewood Campus, QMRP/Team Leader in accordance with the Periodic Health Review Schedule. Upcoming due dates for Periodic Health Reviews are indicated on the Treatment Team Staffing Schedule/ Calendar. Team Leader will review reassessment list to ensure that reassessments are completed in a timely manner, prior to PHR meeting. On the Augusta Campus, the Nurse Manager and/or designated Charge Nurse will track due dates for the quarterly reassessment of the Twenty-four hour Support Plan.
Pg. 13 H.1 Pg. 13 H.2
C. What will these reassessments consist of and how will they be documented (e.g., IDN, progress notes) and communicated to the Treatment Team, along with recommendations (i.e., revise Plan or continue with no changes?).
Reassessments will consist of completing the Physical Supports Monitoring and the Nutritional Supports Monitoring. Reassessments will be documented during Periodic Health Review (PHR) and documented on PHR forms and Progress Notes. The note indicates whether the current plan is adequate or needs revising. It shall be the responsibility of the QMRP Team Leader on the Gracewood Campus and the
DBHDD Policy 03-522 Attachment K Version 5-4-2010
DBHDD: Physical and Nutritional Support Page 7of 7
East Central Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________ DBHDD Policy 03-522 Attachment K Version 5-4-2010
Nurse Manager/Charge Nurse on the Augusta Campus to forward the Physical Supports Monitoring and the Nutritional Supports Monitoring to Data Management for aggregation of data/to identify trends and areas of improvement. The 24-Hour Support Plans will be updated as appropriate. Treatment Team members not present at PHR will be notified during Morning report (DD) and Treatment Team Meeting (MH).
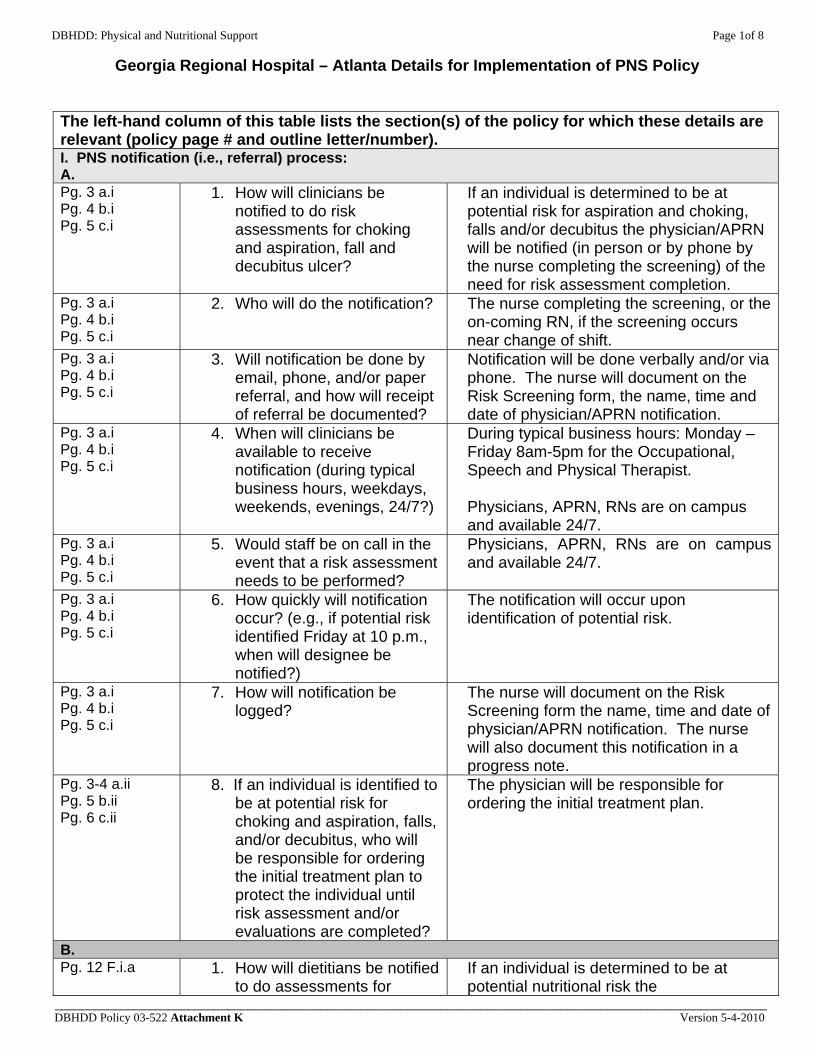
DBHDD: Physical and Nutritional Support Page 1of 8
Georgia Regional Hospital – Atlanta Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
The left-hand column of this table lists the section(s) of the policy for which these details are relevant (policy page # and outline letter/number). I. PNS notification (i.e., referral) process: A. Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
1. How will clinicians be notified to do risk assessments for choking and aspiration, fall and decubitus ulcer?
If an individual is determined to be at potential risk for aspiration and choking, falls and/or decubitus the physician/APRN will be notified (in person or by phone by the nurse completing the screening) of the need for risk assessment completion.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
2. Who will do the notification? The nurse completing the screening, or the on-coming RN, if the screening occurs near change of shift.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
3. Will notification be done by email, phone, and/or paper referral, and how will receipt of referral be documented?
Notification will be done verbally and/or via phone. The nurse will document on the Risk Screening form, the name, time and date of physician/APRN notification.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
During typical business hours: Monday – Friday 8am-5pm for the Occupational, Speech and Physical Therapist.
Physicians, APRN, RNs are on campus and available 24/7.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
5. Would staff be on call in the event that a risk assessment needs to be performed?
Physicians, APRN, RNs are on campus and available 24/7.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
6. How quickly will notification occur? (e.g., if potential risk identified Friday at 10 p.m., when will designee be notified?)
The notification will occur upon identification of potential risk.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
7. How will notification be logged?
The nurse will document on the Risk Screening form the name, time and date of physician/APRN notification. The nurse will also document this notification in a progress note.
Pg. 3-4 a.ii Pg. 5 b.ii Pg. 6 c.ii
8. If an individual is identified to be at potential risk for choking and aspiration, falls, and/or decubitus, who will be responsible for ordering the initial treatment plan to protect the individual until risk assessment and/or evaluations are completed?
The physician will be responsible for ordering the initial treatment plan.
B. Pg. 12 F.i.a 1. How will dietitians be notified
to do assessments for If an individual is determined to be at potential nutritional risk the
DBHDD Policy 03-522 Attachment K Version 5-4-2010
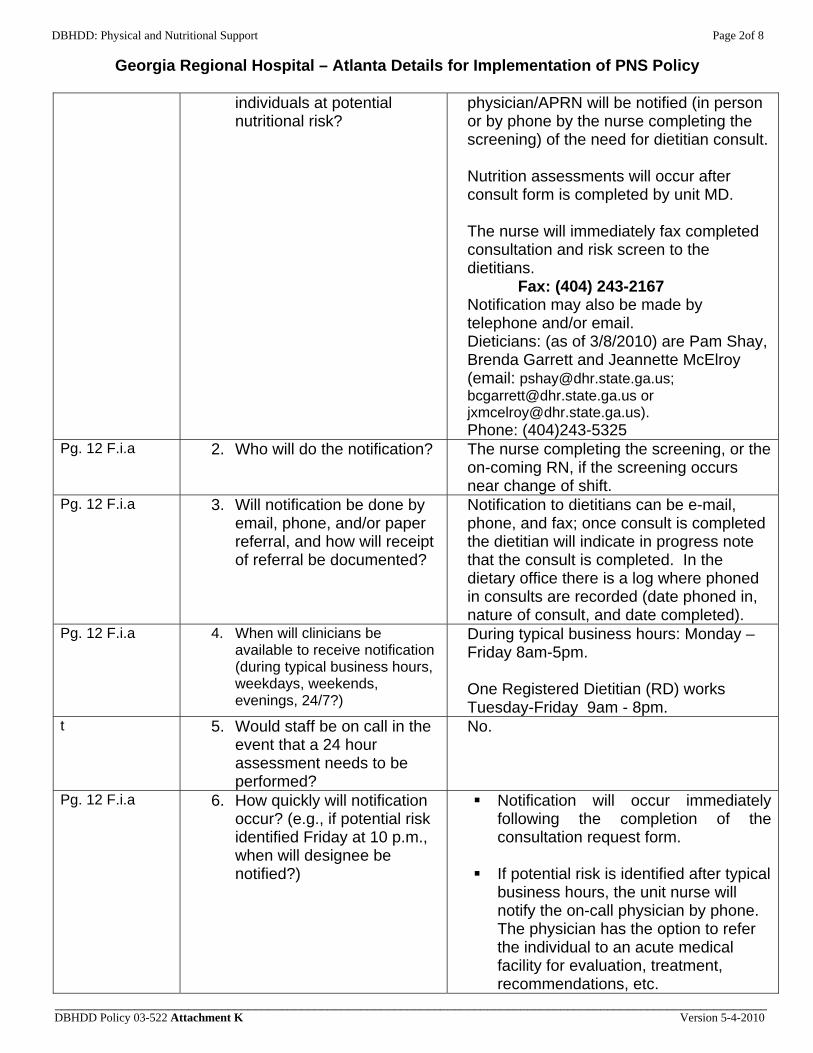
DBHDD: Physical and Nutritional Support Page 2of 8
Georgia Regional Hospital – Atlanta Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
individuals at potential nutritional risk?
physician/APRN will be notified (in person or by phone by the nurse completing the screening) of the need for dietitian consult. Nutrition assessments will occur after consult form is completed by unit MD. The nurse will immediately fax completed consultation and risk screen to the dietitians.
Fax: (404) 243-2167 Notification may also be made by telephone and/or email. Dieticians: (as of 3/8/2010) are Pam Shay, Brenda Garrett and Jeannette McElroy (email: [email protected]; [email protected] or [email protected]). Phone: (404)243-5325
Pg. 12 F.i.a 2. Who will do the notification?
The nurse completing the screening, or the on-coming RN, if the screening occurs near change of shift.
Pg. 12 F.i.a 3. Will notification be done by email, phone, and/or paper referral, and how will receipt of referral be documented?
Notification to dietitians can be e-mail, phone, and fax; once consult is completed the dietitian will indicate in progress note that the consult is completed. In the dietary office there is a log where phoned in consults are recorded (date phoned in, nature of consult, and date completed).
Pg. 12 F.i.a 4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
During typical business hours: Monday – Friday 8am-5pm.
One Registered Dietitian (RD) works Tuesday-Friday 9am - 8pm.
t 5. Would staff be on call in the event that a 24 hour assessment needs to be performed?
No.
Pg. 12 F.i.a 6. How quickly will notification occur? (e.g., if potential risk identified Friday at 10 p.m., when will designee be notified?)
Notification will occur immediately following the completion of the consultation request form.
If potential risk is identified after typical
business hours, the unit nurse will notify the on-call physician by phone. The physician has the option to refer the individual to an acute medical facility for evaluation, treatment, recommendations, etc.
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 3of 8
Georgia Regional Hospital – Atlanta Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
If potential risk is identified after typical business hours notification to dietitians will be by e-mail and/or fax; once consult is completed on the next business day, the dietitian will indicate in progress note that the consult was completed.
Pg. 12 F.i.a 7. How will notification be logged?
Unit based nursing staff maintain a log of referrals of the PNS referrals and recommendations. In the dietary office there is a log where phoned in consults are recorded (date phoned in, nature of consult, and date completed).
Pg. 12 F.i.b 8. If an individual is identified to be at potential nutritional risk, who will be responsible for ordering the initial treatment plan to protect the individual until nutrition assessment?
The physician will be responsible for ordering the initial treatment plan.
C. Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
1. How will clinicians (contract or staff) be notified to do evaluations when clinically indicated for individuals identified to be at high risk for choking and aspiration, fall and/or decubitus ulcer?
The clinician completing the risk assessment will notify the unit or on-call physician of individuals indentified to be at high risk for choking and aspiration, fall and/or decubitus ulcer. If a physician completed the risk assessment, this step will not be necessary.
The physician will notify the PNST
(Physical Nutritional Support Team) of the need for further evaluation via email, fax, and/or telephone (email address- [email protected]). Email notification will allow for the team to receive notification simultaneously, therefore, preventing any delay with notification.
The PNS Team consists of a SLP, PT, OT, RD, MD and RN.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
2. Who will do the notification? The physician writing the referral for evaluation.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
3. Will notification be done by email, phone, and/or paper referral?
Notification will be completed by email and fax. Telephone confirmation can be completed as well.
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 4of 8
Georgia Regional Hospital – Atlanta Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
Contact information:.
Occupational therapy/PNS Coordinator (as of 3/8/2010) is Linda Brownlee: (email: [email protected]. Phone (404)212-4786/(404)212-4780) Fax: (404)212-4785)
If the PNST (Physical and Nutritional Support Team) coordinator is unavailable, nursing staff will call the PNMT therapists and fax the consultation form and indicated documentation to departmental contacts (see below)
Physical Therapy (as of 3/8/2010) is Qua Thomas (email: [email protected]. Phone (404).243-2133/(404) 243-2160 Fax: (404) 243-2288
Speech Pathologist (as of 3/8/2010) is Naarah Brown (email: [email protected]. Phone (404) 243-2133/ (404)243-2160 Fax: (404) 243-2288.
Dietitians: (as of 3/8/2010) are Pam Shay, Brenda Garrett, and Jeanette McElroy (email: [email protected]; [email protected] or [email protected]). Phone (404)243-5325 Fax: (404) 243-2167
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
During typical business hours: Monday – Friday 8am-5pm.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
5. Would staff be on call in the event that an evaluation needs to be performed?
No.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
6. How quickly will notification occur? (e.g., If high risk identified Friday at 10 p.m., when will designee be notified?)
Notification will occur immediately following the completion of the consultation request form.
The PNS Team will receive notification
the next business day if notification occurs after typical business hours.
If potential risk is identified after typical
business hours, the unit nurse will notify the on-call physician by phone.
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 5of 8
Georgia Regional Hospital – Atlanta Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
The physician has the option to refer the individual to an acute medical facility for evaluation, treatment, recommendations, etc.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
7. How will notification be logged?
Unit based nursing staff maintain a log of referrals to the PNST referrals and recommendations. The PNST Coordinator will log all referrals and PNST recommendation in a centralized log book.
D. Pg. 7 C.3 Once an individual is determined to
meet criteria for a 24 hour support plan, how will the person designated to write the initial 24-Hour Support Plan be notified?
The clinician(s) that identified specific needs and completed the evaluation (i.e. physical or nutritional needs) will notify the Treatment Team verbally or by email.
II. Completion of Risk Assessments:
What trained and competent clinicians will be designated to complete the following risk assessments (by discipline, e.g., all physicians and APRNs, by team (a group of identified individuals of various clinical disciplines….)? Pg. 4 a.iii A. Choking and Aspiration Risk
Assessment All physicians and APRNs, RNs, Speech Pathologists, OTs, PTs, & RDs.
Pg. 5 b.iii B. Fall Risk Assessment
All physicians and APRNs, RNs, PTs, & OTs.
Pg. 6 c.iii C. Decubitus Ulcer Risk Assessment
All physicians and APRNs, RNs, PTs, & OTs.
III. 24-Hour Support Plans Documentation:
Pg. 7 C.3 A. Who will be responsible for writing the initial 24-Hour Support Plan? How will responsible person be identified?
Clinician(s) completing the evaluation will write the 24 hour Support plan in collaboration with the Treatment Team. The clinicians that completed the evaluations will work collaboratively as the main authors of the 24 hour Support Plan. All PNS Team clinicians will have write access to the 24 hour Support Plan.
Pg. 7 C.3 Pg. 13 H.2
B. Who will be responsible for updating revisions and changes, and how will these changes be documented?
Clinician(s) determining a change/revision in the plan following reassessment will document revisions/changes based on progress and response to interventions. Revision/ changes will be documented in the applicable section of the 24 Support Plan with revision date.
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 6of 8
Georgia Regional Hospital – Atlanta Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
All PNS Team clinicians will have write access to the 24 hour Support Plan.
Pg. 7 C.4 C. Who will communicate the content of the initial or revised 24 Hour Support Plan to the Treatment Team?
Clinician(s) that wrote the plan will communicate its contents to the Treatment team.
Pg. 9 C.8 D. Where will the original Plan be kept/filed? Where will there be copies (e.g., MAR, dining room, individual’s support book, medical record). Who is responsible for distributing copies and ensuring copies are updated with any change to the Plan?
The plan will be maintained in the Medical Record. Copies of initial/revised plan will be maintained in the Medication Administration Record (MAR), dining room, and individual support plan book (DD units only.) Clinicians writing plan and/or making revisions will be responsible for the distribution of the plan.
IV. Protocol for communication with the TREATMENT TEAM:
A. TREATMENT TEAM approval of the 24-Hour Support Plans (new and revised):
Pg. 7 C.4 1. What is the process by which the Treatment Team approves initial and revised plans?
PNS team members will attend regularly scheduled treatment team meetings (occurs M-F) following completion of the 24 hour Support Plan to present recommended plan to the treatment team for approval.
Pg. 7.C.4 2. Can approval be done by email, verbally, or may it require a special team meeting when clinically appropriate?
The PNS team will report their evaluation findings to the Treatment Team during treatment team meetings the next business day. PNS clinician(s) will notify the Treatment Team via email of evaluation being completed and that evaluation results will be presented at the next Treatment Team meeting (this occurs daily M-F). For initial and revised 24-Hour Support Plans the PNS team members will attend treatment team meetings the next business day following completion of the 24 hour Support Plan to present recommended plan to the treatment team for approval. Minor changes to the 24 Hour Support Plan may be communicated via email to the treatment team. The clinicians on the PNS team making the revision will be responsible for documenting revisions on the Support Plan.
Pg. 4 a.iii. Pg. 4 a.iv
How and when will clinicians doing the PNS Risk Screen, Risk
During Treatment Team meeting either at the next regularly scheduled meeting or called
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 7of 8
Georgia Regional Hospital – Atlanta Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
Pg. 5 b.iii Pg. 5 b.iv Pg. 6 c.iii Pg. 6 c.iv Pg. 12 F.i.c Pg. 14 H.3
Assessments, and/or evaluations report their findings to the other members of the Treatment Team (besides those immediately notified according to PNS procedure)? (e.g., At the next regularly scheduled Treatment Team meeting? At morning unit meetings? Email? etc.)
Treatment Team meetings as indicated based on clinical needs.
V. Who will train family, visitors, and significant others on the 24-Hour Support Plan?
Pg. 9.C.9.a.i A professional staff member (designated trainer) on duty (Nursing staff, Therapists [OT, PT, ST]) will train family, visitors and significant others on 24 hour plans anytime the Plan is initiated or revised. The family member/significant other will be notified by unit staff (Charge Nurse or Social Worker) of required training when plan is initiated or revised. Family member/significant other will schedule time for training.
VI. Dietitian vs. Nurse: Who trends weights and enters/tracks the data?
Pg. 13 F.6 Nursing is responsible for the assessment of’ weights at least monthly (or per physician’s order). Nursing documents this assessment in progress note as well as ordered interventions/assessments/diagnostics. Dietitians will trend the data using a computer program which will indicate 5%, 7.5%, and 10% weight loss or gain at 1, 3, and 6 month intervals, respectively and communicate findings to the physician.
VII. Training protocol: With regard to training direct care and end-user staff on the Plan (new and revised): Pg. 14 H.6 Pg. 14 I.3.a Pg. 14 I.3.b Pg. 14 I.3.c Pg. 15 I.3.g
A. What system will be implemented to ensure all direct care and end-user staff is trained (person specific training) and competent prior to Plan implementation (and if not trained and competent yet are not assigned to care for those individuals)?
Staff (full-time/prn) from each shift will be trained on the 24 hour support plans for individuals they will be assisting. Roster of competent staff will be paired with the 24 hour support plan and placed in central access to scheduling staff. Only staff who have demonstrated person specific competency will be assigned to the care of individuals with 24 hour support plans. The 24 hour Support plan trainer will notify the staff member supervisor if the staff member does not demonstrate competency to ensure that the staff member is not assigned to the care of the individual until competency is achieved.
Pg. 14 I.3.a Pg. 15 I.3.g
B. Who will track this training and % of staff trained and competent until completion?
Nurse Manager, Lead Nurse and/or Service Director will track the % of staff trained and competent on individual’s 24 hour Support Plan.
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 8of 8
Georgia Regional Hospital – Atlanta Details for Implementation of PNS Policy
___________________________________________________________________________________________________________ DBHDD Policy 03-522 Attachment K Version 5-4-2010
Pg. 15 I.3.f Pg. 15 I.3.g
C. If direct care or end-user staff is unable to demonstrate competency during person specific training OR monitoring, who is responsible for developing and tracking a “performance improvement” plan (e.g., repeat didactic training, repeat in vivo competency) through to completion?
Communication between the trainer of the person specific 24 hour support plan and the nursing supervisor of the end-user staff will occur. Assignment to the consumer with the 24 hour support plan will not occur until the training has been successfully completed. The nursing supervisor will ensure the employee is not assigned to the care of the individual for which the (failed) training occurred.
VIII. Process for reassessing the 24-Hour Support Plan:
Pg. 13 H.1 A. Who will do the quarterly and PRN (as clinically indicated) reassessments?
The PNS team (MD, RN, Dietitian, OT, PT and Speech therapists) will be responsible for conducting quarterly and PRN reassessments. The appropriate PNS members will follow up, monitor, and document the status of the individual’s progress until the individual’s problem is determined to be resolved and/or discharged.
Pg. 13 H.1 B. Who will track when they are due and how will it be tracked?
The frequency of PRN reassessment will be determined by the clinicians on the PNS Team based on individualized needs. The PNS Team will track when reassessments are due. Tracking will occur on a centralized database that will store all 24 Support Plans and master calendar for reassessments. Master calendar will be maintained by PNS Team.
Pg. 13 H.1 Pg. 13 H.2
C. What will these reassessments consist of and how will they be documented (e.g., IDN, progress notes) and communicated to the Treatment Team, along with recommendations (i.e., revise Plan or continue with no changes?).
The reassessment will consist of clinical observation, review of the medical record, and the individual’s response to the support plan. Findings will be updated as needed to document any new issues or any that have been resolved. This will be documented on the progress note.
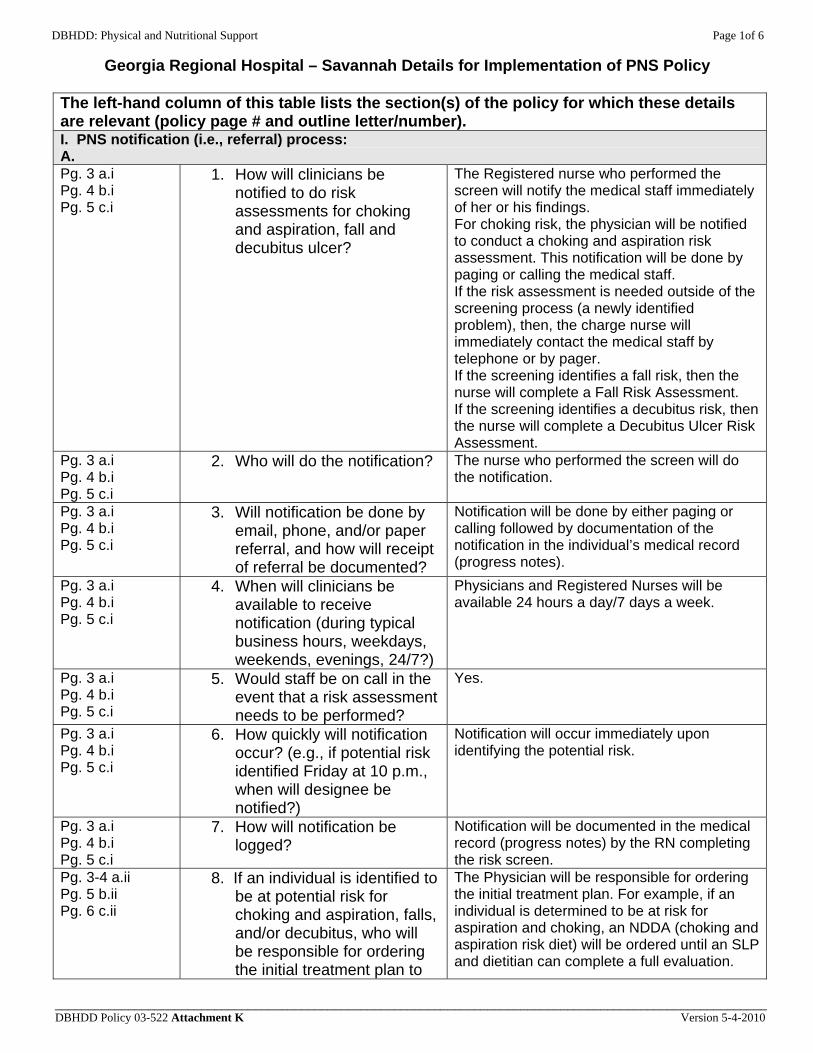
DBHDD: Physical and Nutritional Support Page 1of 6
Georgia Regional Hospital – Savannah Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
The left-hand column of this table lists the section(s) of the policy for which these details are relevant (policy page # and outline letter/number). I. PNS notification (i.e., referral) process: A. Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
1. How will clinicians be notified to do risk assessments for choking and aspiration, fall and decubitus ulcer?
The Registered nurse who performed the screen will notify the medical staff immediately of her or his findings. For choking risk, the physician will be notified to conduct a choking and aspiration risk assessment. This notification will be done by paging or calling the medical staff. If the risk assessment is needed outside of the screening process (a newly identified problem), then, the charge nurse will immediately contact the medical staff by telephone or by pager. If the screening identifies a fall risk, then the nurse will complete a Fall Risk Assessment. If the screening identifies a decubitus risk, then the nurse will complete a Decubitus Ulcer Risk Assessment.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
2. Who will do the notification? The nurse who performed the screen will do the notification.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
3. Will notification be done by email, phone, and/or paper referral, and how will receipt of referral be documented?
Notification will be done by either paging or calling followed by documentation of the notification in the individual’s medical record (progress notes).
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
Physicians and Registered Nurses will be available 24 hours a day/7 days a week.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
5. Would staff be on call in the event that a risk assessment needs to be performed?
Yes.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
6. How quickly will notification occur? (e.g., if potential risk identified Friday at 10 p.m., when will designee be notified?)
Notification will occur immediately upon identifying the potential risk.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
7. How will notification be logged?
Notification will be documented in the medical record (progress notes) by the RN completing the risk screen.
Pg. 3-4 a.ii Pg. 5 b.ii Pg. 6 c.ii
8. If an individual is identified to be at potential risk for choking and aspiration, falls, and/or decubitus, who will be responsible for ordering the initial treatment plan to
The Physician will be responsible for ordering the initial treatment plan. For example, if an individual is determined to be at risk for aspiration and choking, an NDDA (choking and aspiration risk diet) will be ordered until an SLP and dietitian can complete a full evaluation.
DBHDD Policy 03-522 Attachment K Version 5-4-2010
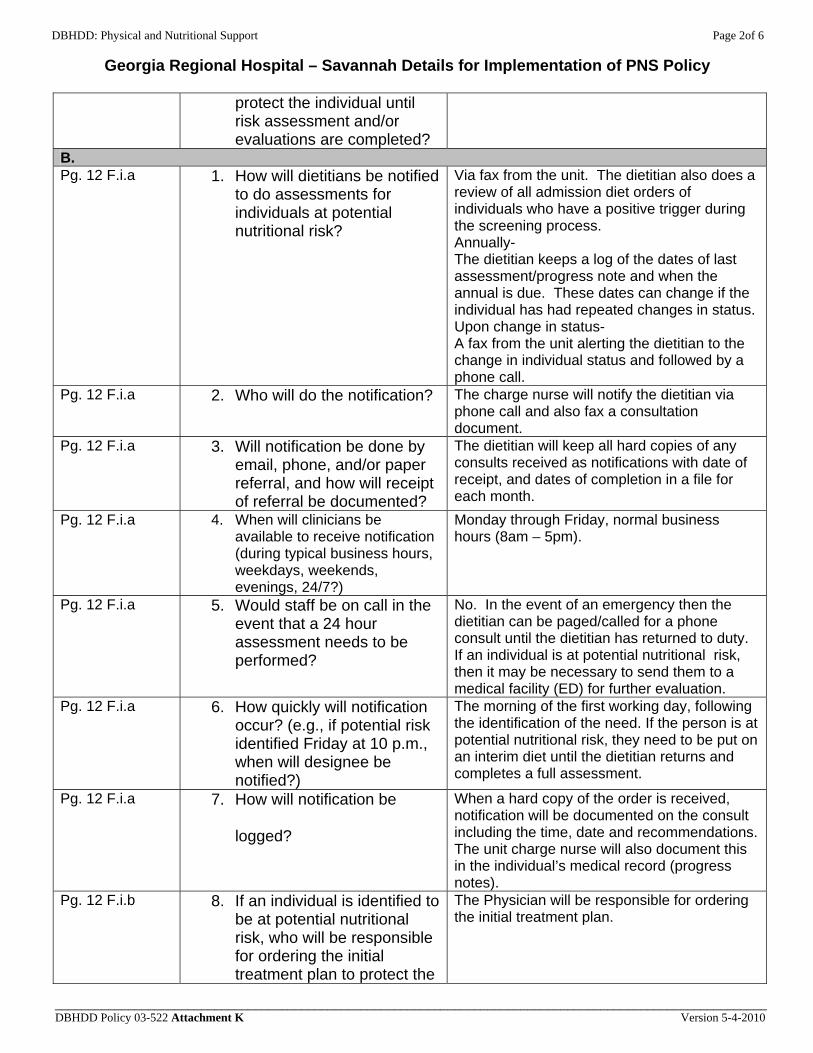
DBHDD: Physical and Nutritional Support Page 2of 6
Georgia Regional Hospital – Savannah Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
protect the individual until risk assessment and/or evaluations are completed?
B. Pg. 12 F.i.a 1. How will dietitians be notified
to do assessments for individuals at potential nutritional risk?
Via fax from the unit. The dietitian also does a review of all admission diet orders of individuals who have a positive trigger during the screening process. Annually- The dietitian keeps a log of the dates of last assessment/progress note and when the annual is due. These dates can change if the individual has had repeated changes in status. Upon change in status- A fax from the unit alerting the dietitian to the change in individual status and followed by a phone call.
Pg. 12 F.i.a 2. Who will do the notification?
The charge nurse will notify the dietitian via phone call and also fax a consultation document.
Pg. 12 F.i.a 3. Will notification be done by email, phone, and/or paper referral, and how will receipt of referral be documented?
The dietitian will keep all hard copies of any consults received as notifications with date of receipt, and dates of completion in a file for each month.
Pg. 12 F.i.a 4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
Monday through Friday, normal business hours (8am – 5pm).
Pg. 12 F.i.a 5. Would staff be on call in the event that a 24 hour assessment needs to be performed?
No. In the event of an emergency then the dietitian can be paged/called for a phone consult until the dietitian has returned to duty. If an individual is at potential nutritional risk, then it may be necessary to send them to a medical facility (ED) for further evaluation.
Pg. 12 F.i.a 6. How quickly will notification occur? (e.g., if potential risk identified Friday at 10 p.m., when will designee be notified?)
The morning of the first working day, following the identification of the need. If the person is at potential nutritional risk, they need to be put on an interim diet until the dietitian returns and completes a full assessment.
Pg. 12 F.i.a 7. How will notification be
logged?
When a hard copy of the order is received, notification will be documented on the consult including the time, date and recommendations. The unit charge nurse will also document this in the individual’s medical record (progress notes).
Pg. 12 F.i.b 8. If an individual is identified to be at potential nutritional risk, who will be responsible for ordering the initial treatment plan to protect the
The Physician will be responsible for ordering the initial treatment plan.
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 3of 6
Georgia Regional Hospital – Savannah Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
individual until nutrition assessment?
C. Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
1. How will clinicians (contract or staff) be notified to do evaluations when clinically indicated for individuals identified to be at high risk for choking and aspiration, fall and/or decubitus ulcer?
If an OT/PT/ SLP evaluation is needed, the consult will be ordered by the physician. If a high risk is identified, the physician can also refer to the ED for evaluation, treatment, recommendations, etc.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
2. Who will do the notification? The physician will order all consults, and the nurse in charge will do the notification and/or scheduling.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
3. Will notification be done by email, phone, and/or paper referral?
Notification will be done by phone call followed by documentation of the notification in the individual’s medical record (progress notes). The physician will write an order and complete consultation/referral form.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
Clinicians (OT/PT/SLP) to be available weekdays, M- F. If a high risk is identified, referral to the ED may be made 24 hours per day/7 days per week.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
5. Would staff be on call in the event that an evaluation needs to be performed?
No.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
6. How quickly will notification occur? (e.g., If high risk identified Friday at 10 p.m., when will designee be notified?)
The morning of the first working day, following the identification of the need. However, the physician has the option to refer the individual to the ED for evaluation, treatment, recommendations, etc.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
7. How will notification be logged?
In the individual’s medical record (progress notes). The OT and PT consults are done by contract with an outside agency. The SLP is a part-time staff member, and a log will be maintained for those referrals by the SLP.
D. Pg. 7 C.3 Once an individual is determined to
meet criteria for a 24 hour support plan, how will the person designated to write the initial 24-Hour Support Plan be notified?
The treatment team nurse will develop the initial 24 hour support plan based upon the assessment findings and the physician orders (e.g., diet). During the interdisciplinary treatment team/plan development meeting the Treatment Team Facilitator (TTF) ensures that a final 24-hour support plan is developed. This person will facilitate a called meeting, when necessary, in order to obtain input from all identified clinicians as well as communicate contents of the plan to the Treatment Team The treatment team nurse will update the plan
DBHDD Policy 03-522 Attachment K Version 5-4-2010
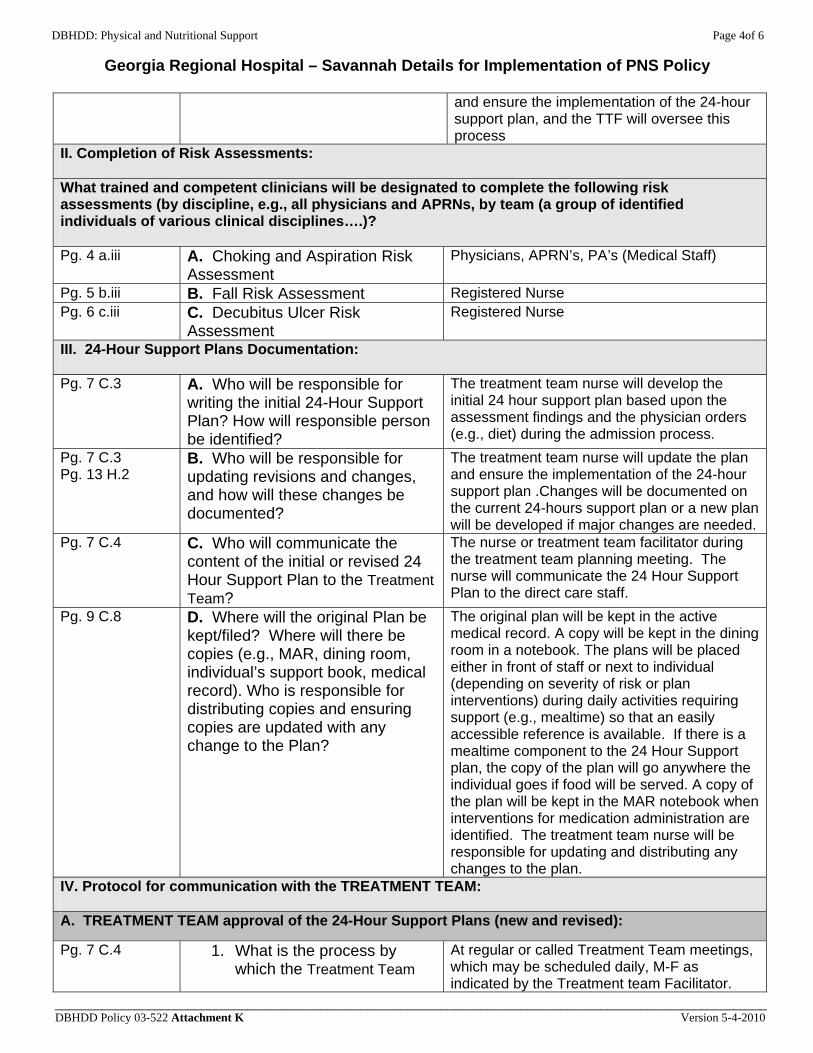
DBHDD: Physical and Nutritional Support Page 4of 6
Georgia Regional Hospital – Savannah Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
and ensure the implementation of the 24-hour support plan, and the TTF will oversee this process
II. Completion of Risk Assessments:
What trained and competent clinicians will be designated to complete the following risk assessments (by discipline, e.g., all physicians and APRNs, by team (a group of identified individuals of various clinical disciplines….)? Pg. 4 a.iii A. Choking and Aspiration Risk
Assessment Physicians, APRN’s, PA’s (Medical Staff)
Pg. 5 b.iii B. Fall Risk Assessment Registered Nurse Pg. 6 c.iii C. Decubitus Ulcer Risk
Assessment Registered Nurse
III. 24-Hour Support Plans Documentation:
Pg. 7 C.3 A. Who will be responsible for writing the initial 24-Hour Support Plan? How will responsible person be identified?
The treatment team nurse will develop the initial 24 hour support plan based upon the assessment findings and the physician orders (e.g., diet) during the admission process.
Pg. 7 C.3 Pg. 13 H.2
B. Who will be responsible for updating revisions and changes, and how will these changes be documented?
The treatment team nurse will update the plan and ensure the implementation of the 24-hour support plan .Changes will be documented on the current 24-hours support plan or a new plan will be developed if major changes are needed.
Pg. 7 C.4 C. Who will communicate the content of the initial or revised 24 Hour Support Plan to the Treatment Team?
The nurse or treatment team facilitator during the treatment team planning meeting. The nurse will communicate the 24 Hour Support Plan to the direct care staff.
Pg. 9 C.8 D. Where will the original Plan be kept/filed? Where will there be copies (e.g., MAR, dining room, individual’s support book, medical record). Who is responsible for distributing copies and ensuring copies are updated with any change to the Plan?
The original plan will be kept in the active medical record. A copy will be kept in the dining room in a notebook. The plans will be placed either in front of staff or next to individual (depending on severity of risk or plan interventions) during daily activities requiring support (e.g., mealtime) so that an easily accessible reference is available. If there is a mealtime component to the 24 Hour Support plan, the copy of the plan will go anywhere the individual goes if food will be served. A copy of the plan will be kept in the MAR notebook when interventions for medication administration are identified. The treatment team nurse will be responsible for updating and distributing any changes to the plan.
IV. Protocol for communication with the TREATMENT TEAM:
A. TREATMENT TEAM approval of the 24-Hour Support Plans (new and revised):
Pg. 7 C.4 1. What is the process by which the Treatment Team
At regular or called Treatment Team meetings, which may be scheduled daily, M-F as indicated by the Treatment team Facilitator.
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 5of 6
Georgia Regional Hospital – Savannah Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
approves initial and revised plans?
This may require a special Treatment Team meeting when clinically indicated.
Pg. 7.C.4 2. Can approval be done by email, verbally, or may it require a special team meeting when clinically appropriate?
Approval is obtained either during the treatment team planning meeting or during a special Treatment Team meeting as indicated for changes. The TTF may call a special Treatment Team meeting.
B. Pg. 4 a.iii. Pg. 4 a.iv Pg. 5 b.iii Pg. 5 b.iv Pg. 6 c.iii Pg. 6 c.iv Pg. 12 F.i.c Pg. 14 H.3
How and when will clinicians doing the PNS Risk Screen, Risk Assessments, and/or evaluations report their findings to the other members of the Treatment Team (besides those immediately notified according to PNS procedure)? (e.g., At the next regularly scheduled Treatment Team meeting? At morning unit meetings? Email? etc.)
During the Treatment Team meeting either at the next regularly scheduled Treatment Team meeting or during a special called meeting.
V. Who will train family, visitors, and significant others on the 24-Hour Support Plan?
Pg. 9.C.9.a.i The Licensed unit Nurse who is familiar with the individual educates these persons if the individual goes off the unit on a trial visit, pass or is discharged. The education is documented on the progress notes. The charge nurse will insure this is done anytime the individual leaves the unit with someone other than a staff member.
VI. Dietitian vs. Nurse: Who trends weights and enters/tracks the data?
Pg. 13 F.6 Nursing staff will enter, track and trend individual’s weights. The nursing staff will advise the dietitian of changes that are either significant or severe.
VII. Training protocol: With regard to training direct care and end-user staff on the Plan (new and revised): Pg. 14 H.6 Pg. 14 I.3.a Pg. 14 I.3.b Pg. 14 I.3.c Pg. 15 I.3.g
A. What system will be implemented to ensure all direct care and end-user staff is trained (person specific training) and competent prior to Plan implementation (and if not trained and competent yet are not assigned to care for those individuals)?
Only trained staff who demonstrate competency will be assigned to assist the individuals. The Nurse Manager or Charge Nurse will utilize rosters on each unit of those direct care staff that are trained in order to ensure that all direct care staff are trained. The dietitian, SLP, and/or nurse will ensure that the direct care staff and end-user staff are trained and competent for individual 24-hour support plans (i.e., will be responsible for conducting the person specific training). Training rosters will be sent to SD&T for entry into the database.
Pg. 14 I.3.a Pg. 15 I.3.g
B. Who will track this training and % of staff trained and competent until completion?
SD&T will track the completion percentage of training. The nurse manager or charge nurse will ensure that all direct care staff on unit are trained on individual 24-hour support plans.
Pg. 15 I.3.f Pg. 15 I.3.g
C. If direct care or end-user staff is unable to demonstrate competency during person specific training OR monitoring,
The Nurse Manager or designee will be responsible for implementing and tracking performance improvement plans (e.g., to re-train staff until competency is satisfied, and
DBHDD Policy 03-522 Attachment K Version 5-4-2010
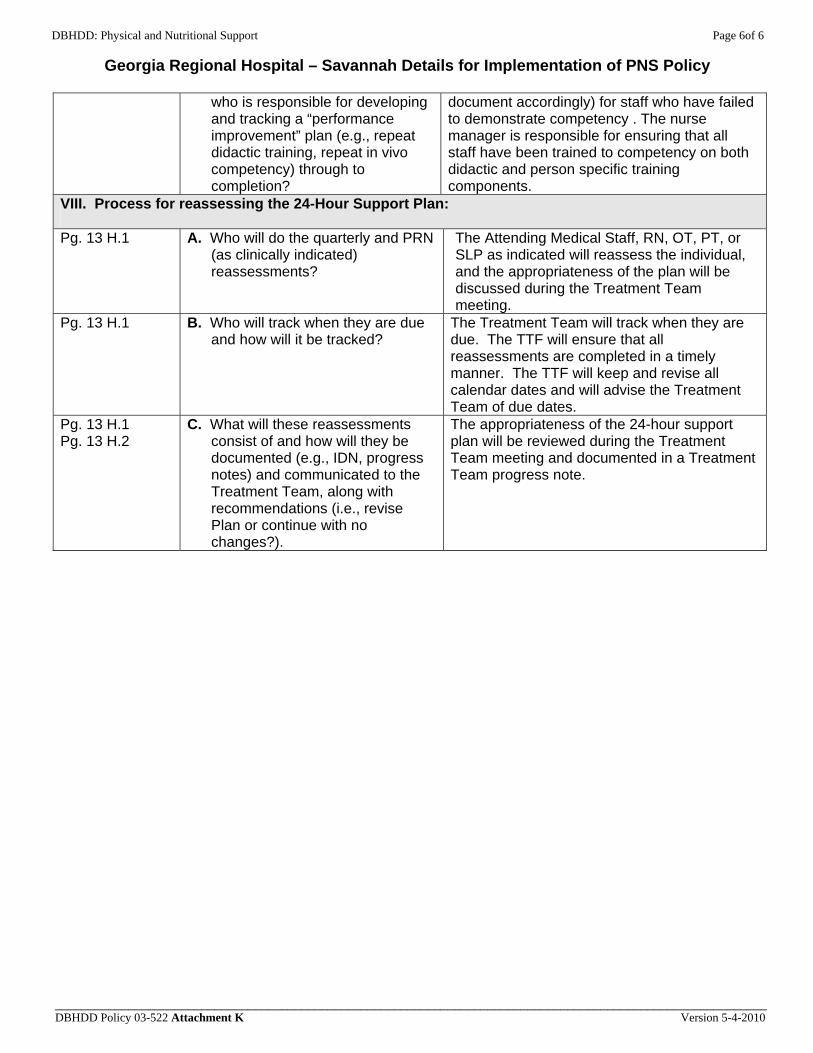
DBHDD: Physical and Nutritional Support Page 6of 6
Georgia Regional Hospital – Savannah Details for Implementation of PNS Policy
___________________________________________________________________________________________________________ DBHDD Policy 03-522 Attachment K Version 5-4-2010
who is responsible for developing and tracking a “performance improvement” plan (e.g., repeat didactic training, repeat in vivo competency) through to completion?
document accordingly) for staff who have failed to demonstrate competency . The nurse manager is responsible for ensuring that all staff have been trained to competency on both didactic and person specific training components.
VIII. Process for reassessing the 24-Hour Support Plan:
Pg. 13 H.1 A. Who will do the quarterly and PRN (as clinically indicated) reassessments?
The Attending Medical Staff, RN, OT, PT, or SLP as indicated will reassess the individual, and the appropriateness of the plan will be discussed during the Treatment Team meeting.
Pg. 13 H.1 B. Who will track when they are due and how will it be tracked?
The Treatment Team will track when they are due. The TTF will ensure that all reassessments are completed in a timely manner. The TTF will keep and revise all calendar dates and will advise the Treatment Team of due dates.
Pg. 13 H.1 Pg. 13 H.2
C. What will these reassessments consist of and how will they be documented (e.g., IDN, progress notes) and communicated to the Treatment Team, along with recommendations (i.e., revise Plan or continue with no changes?).
The appropriateness of the 24-hour support plan will be reviewed during the Treatment Team meeting and documented in a Treatment Team progress note.
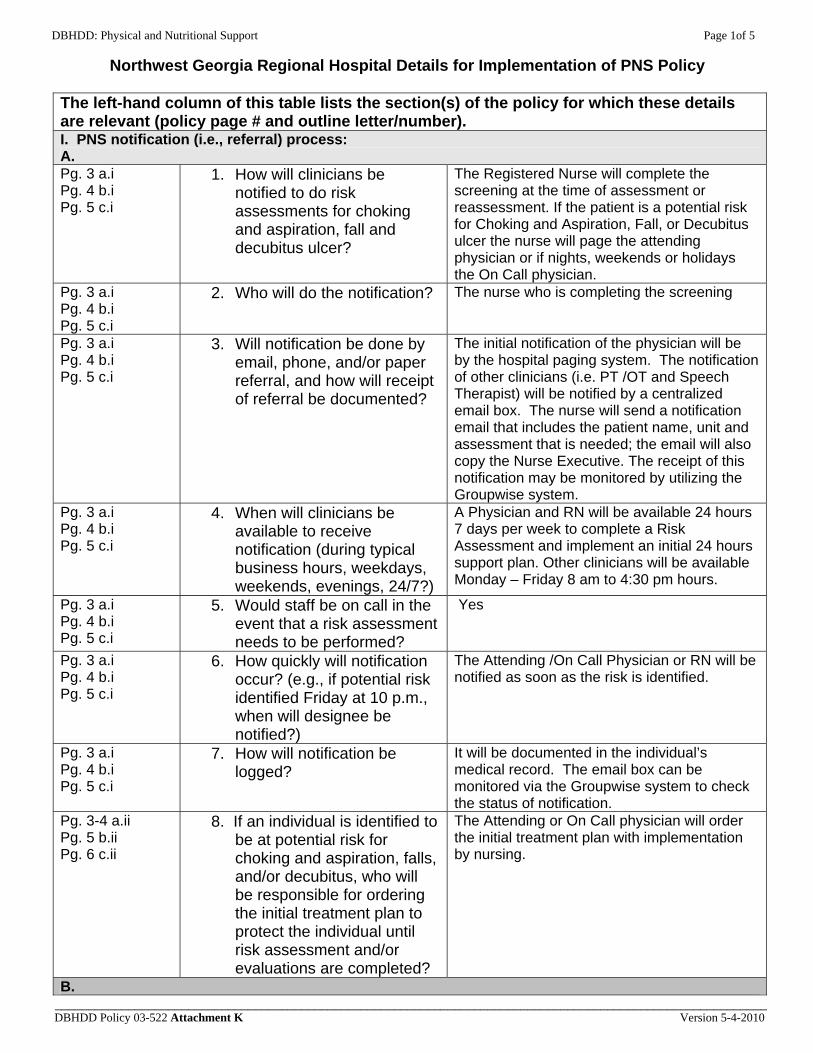
DBHDD: Physical and Nutritional Support Page 1of 5
Northwest Georgia Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
The left-hand column of this table lists the section(s) of the policy for which these details are relevant (policy page # and outline letter/number). I. PNS notification (i.e., referral) process: A. Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
1. How will clinicians be notified to do risk assessments for choking and aspiration, fall and decubitus ulcer?
The Registered Nurse will complete the screening at the time of assessment or reassessment. If the patient is a potential risk for Choking and Aspiration, Fall, or Decubitus ulcer the nurse will page the attending physician or if nights, weekends or holidays the On Call physician.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
2. Who will do the notification? The nurse who is completing the screening
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
3. Will notification be done by email, phone, and/or paper referral, and how will receipt of referral be documented?
The initial notification of the physician will be by the hospital paging system. The notification of other clinicians (i.e. PT /OT and Speech Therapist) will be notified by a centralized email box. The nurse will send a notification email that includes the patient name, unit and assessment that is needed; the email will also copy the Nurse Executive. The receipt of this notification may be monitored by utilizing the Groupwise system.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
A Physician and RN will be available 24 hours 7 days per week to complete a Risk Assessment and implement an initial 24 hours support plan. Other clinicians will be available Monday – Friday 8 am to 4:30 pm hours.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
5. Would staff be on call in the event that a risk assessment needs to be performed?
Yes
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
6. How quickly will notification occur? (e.g., if potential risk identified Friday at 10 p.m., when will designee be notified?)
The Attending /On Call Physician or RN will be notified as soon as the risk is identified.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
7. How will notification be logged?
It will be documented in the individual’s medical record. The email box can be monitored via the Groupwise system to check the status of notification.
Pg. 3-4 a.ii Pg. 5 b.ii Pg. 6 c.ii
8. If an individual is identified to be at potential risk for choking and aspiration, falls, and/or decubitus, who will be responsible for ordering the initial treatment plan to protect the individual until risk assessment and/or evaluations are completed?
The Attending or On Call physician will order the initial treatment plan with implementation by nursing.
B.
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 2of 5
Northwest Georgia Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
Pg. 12 F.i.a 1. How will dietitians be notified to do assessments for individuals at potential nutritional risk?
A copy of the Physical Nutritional Support Risk Screen will be faxed to the dietitian at 706-802-5678
Pg. 12 F.i.a 2. Who will do the notification? The nurse who completed the risk screen. Pg. 12 F.i.a 3. Will notification be done by
email, phone, and/or paper referral, and how will receipt of referral be documented?
Paper referral by fax: The dietitian receives a list of all newly admitted patients every day Monday – Friday and will verify by phone to the patient care unit. The nurse will stamp the original risk screen with the “faxed” date, time and initials and file in the medical record.
Pg. 12 F.i.a 4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
The dietitian will be available Monday – Friday during normal working hours. A dietitian will be available daily 5 am – 7pm to make necessary diet or food allergy changes.
Pg. 12 F.i.a 5. Would staff be on call in the event that a 24 hour assessment needs to be performed?
No.
Pg. 12 F.i.a 6. How quickly will notification occur? (e.g., if potential risk identified Friday at 10 p.m., when will designee be notified?)
The Dietary Department and On Call physician will be notified upon completion of the Nutritional Risk Screen. The dietitian will be notified the morning of the first working day, following the identification of the need.
Pg. 12 F.i.a 7. How will notification be logged?
The Dietitian keeps a log.
Pg. 12 F.i.b 8. If an individual is identified to be at potential nutritional risk, who will be responsible for ordering the initial treatment plan to protect the individual until nutrition assessment?
The On Call Physician will order the initial treatment plan with implementation by nursing.
C. Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
1. How will clinicians (contract or staff) be notified to do evaluations when clinically indicated for individuals identified to be at high risk for choking and aspiration, fall and/or decubitus ulcer?
The initial notification of the physician will be by the hospital paging system. The notification of other clinicians i.e. PT /OT and Speech Therapist will be notified by a centralized email box. The nurse will send a notification email that includes the patient name, unit and evaluation that is needed the email will also copy the Nurse Executive. The receipt of this notification will be monitored by utilizing the Groupwise system.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
2. Who will do the notification? The clinician who completed the assessment.
DBHDD Policy 03-522 Attachment K Version 5-4-2010
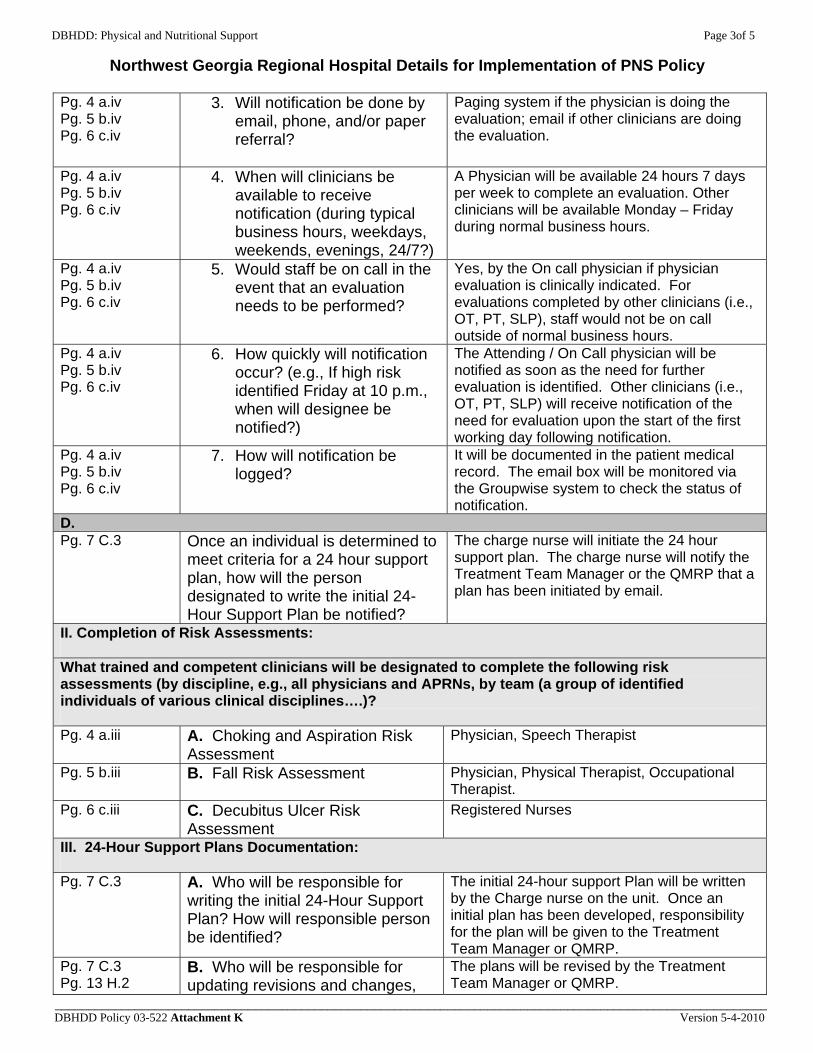
DBHDD: Physical and Nutritional Support Page 3of 5
Northwest Georgia Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
3. Will notification be done by email, phone, and/or paper referral?
Paging system if the physician is doing the evaluation; email if other clinicians are doing the evaluation.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
A Physician will be available 24 hours 7 days per week to complete an evaluation. Other clinicians will be available Monday – Friday during normal business hours.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
5. Would staff be on call in the event that an evaluation needs to be performed?
Yes, by the On call physician if physician evaluation is clinically indicated. For evaluations completed by other clinicians (i.e., OT, PT, SLP), staff would not be on call outside of normal business hours.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
6. How quickly will notification occur? (e.g., If high risk identified Friday at 10 p.m., when will designee be notified?)
The Attending / On Call physician will be notified as soon as the need for further evaluation is identified. Other clinicians (i.e., OT, PT, SLP) will receive notification of the need for evaluation upon the start of the first working day following notification.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
7. How will notification be logged?
It will be documented in the patient medical record. The email box will be monitored via the Groupwise system to check the status of notification.
D. Pg. 7 C.3 Once an individual is determined to
meet criteria for a 24 hour support plan, how will the person designated to write the initial 24-Hour Support Plan be notified?
The charge nurse will initiate the 24 hour support plan. The charge nurse will notify the Treatment Team Manager or the QMRP that a plan has been initiated by email.
II. Completion of Risk Assessments:
What trained and competent clinicians will be designated to complete the following risk assessments (by discipline, e.g., all physicians and APRNs, by team (a group of identified individuals of various clinical disciplines….)? Pg. 4 a.iii A. Choking and Aspiration Risk
Assessment Physician, Speech Therapist
Pg. 5 b.iii B. Fall Risk Assessment
Physician, Physical Therapist, Occupational Therapist.
Pg. 6 c.iii C. Decubitus Ulcer Risk Assessment
Registered Nurses
III. 24-Hour Support Plans Documentation:
Pg. 7 C.3 A. Who will be responsible for writing the initial 24-Hour Support Plan? How will responsible person be identified?
The initial 24-hour support Plan will be written by the Charge nurse on the unit. Once an initial plan has been developed, responsibility for the plan will be given to the Treatment Team Manager or QMRP.
Pg. 7 C.3 Pg. 13 H.2
B. Who will be responsible for updating revisions and changes,
The plans will be revised by the Treatment Team Manager or QMRP.
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 4of 5
Northwest Georgia Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
and how will these changes be documented?
Pg. 7 C.4 C. Who will communicate the content of the initial or revised 24 Hour Support Plan to the Treatment Team?
The charge nurse who attends the Treatment Team will communicate the initial 24 hour support plan to the team. The Treatment Team Manager or QMRP will communicate revisions.
Pg. 9 C.8 D. Where will the original Plan be kept/filed? Where will there be copies (e.g., MAR, dining room, individual’s support book, medical record). Who is responsible for distributing copies and ensuring copies are updated with any change to the Plan?
The original will be kept in the patient medical record, and copies will be kept in the MAR, Dining Room, Treatment Mall or Programming Area. The Treatment Team Managers and QMRP will update the plan. The initial copies will be distributed by the charge nurse and the updated copies will be distributed by the Program Assistants.
IV. Protocol for communication with the TREATMENT TEAM:
A. TREATMENT TEAM approval of the 24-Hour Support Plans (new and revised):
Pg. 7 C.4 1. What is the process by which the Treatment Team approves initial and revised plans?
Mental Health: The charge nurse communicates the initial plan to treatment team for approval. Revisions are communicated by the Treatment Team Manager for approval. Developmental Services: The charge nurse will notify the QMRP of an initial plan, the QMRP will communicate with the Treatment Team for approval.
Pg. 7.C.4 2. Can approval be done by email, verbally, or may it require a special team meeting when clinically appropriate?
Mental Health the approval will take place in Treatment Team which meets daily Monday – Friday. Developmental Services: For minor changes an email will be sent by the QMRP, major changes (hospitalization or significant change in level of care, would require a team meeting.
Pg. 4 a.iii. Pg. 4 a.iv Pg. 5 b.iii Pg. 5 b.iv Pg. 6 c.iii Pg. 6 c.iv Pg. 12 F.i.c Pg. 14 H.3
How and when will clinicians doing the PNS Risk Screen, Risk Assessments, and/or evaluations report their findings to the other members of the Treatment Team (besides those immediately notified according to PNS procedure)? (e.g., At the next regularly scheduled Treatment Team meeting? At morning unit meetings? Email? etc.)
The clinicians will file a report of findings and recommendations in the patient medical record. They will send an email to the Treatment Team stating the assessment has been completed. If the team feels it is clinically indicated they will request that the clinician be present during the Treatment Team.
V. Who will train family, visitors, and significant others on the 24-Hour Support Plan?
Pg. 9.C.9.a.i The Treatment Team Manager, QMRP or the charge nurse will educate the family, visitors and others. They will document in a progress note that this has been done including who was educated, and if family expresses understanding.
VI. Dietitian vs. Nurse: Who trends weights and enters/tracks the data?
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 5of 5
Northwest Georgia Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________ DBHDD Policy 03-522 Attachment K Version 5-4-2010
Pg. 13 F.6 The Nurse will monitor weights: DD monthly, MH weekly. This will be documented in the individual’s medical record. The information will be sent to the program assistant who will enter into a data base so that nursing can track and trend weights and report data to the treatment team with recommendations.
VII. Training protocol: With regard to training direct care and end-user staff on the Plan (new and revised): Pg. 14 H.6 Pg. 14 I.3.a Pg. 14 I.3.b Pg. 14 I.3.c Pg. 15 I.3.g
A. What system will be implemented to ensure all direct care and end-user staff is trained (person specific training) and competent prior to Plan implementation (and if not trained and competent yet are not assigned to care for those individuals)?
All 24 hour support plans will be trained by a qualified trainer during the appropriate setting (e.g., during a meal if mealtime supports are indicated in the 24 hour support plan). A training roster will be maintained by the unit manager on each 24 hour support plan listing all staff that has been trained. The Charge Nurse or Shift supervisor will ensure that staff who have not been trained are not assigned to care for that individual.
Pg. 14 I.3.a Pg. 15 I.3.g
B. Who will track this training and % of staff trained and competent until completion?
The Unit Manager or Supervisor will maintain training rosters on each 24 hour support plan including the names of staff that have been trained.
Pg. 15 I.3.f Pg. 15 I.3.g
C. If direct care or end-user staff is unable to demonstrate competency during person specific training OR monitoring, who is responsible for developing and tracking a “performance improvement” plan (e.g., repeat didactic training, repeat in vivo competency) through to completion?
Any staff that is unable to demonstrate competency will be retrained by the supervisor and asked to return in vivo demonstration. If the staff is unable to show competency by return demonstration after retraining the staff will be removed from care of the individual and receive additional education by the training department. If a staff is removed from care of the individual due to failure to demonstrate competency the Unit Manager and or Team leader will be notified. The Unit Manager and or Team leader will be responsible for tracking performance improvement.
VIII. Process for reassessing the 24-Hour Support Plan:
Pg. 13 H.1 A. Who will do the quarterly and PRN (as clinically indicated) reassessments?
The clinically indicated clinician (e.g., Physician, Nurse, Dietitian, Speech Therapist, PT, OT)
Pg. 13 H.1 B. Who will track when they are due and how will it be tracked?
The QMRP/ Treatment Team Manager will track when due prior to the treatment team review
Pg. 13 H.1 Pg. 13 H.2
C. What will these reassessments consist of and how will they be documented (e.g., IDN, progress notes) and communicated to the Treatment Team, along with recommendations (i.e., revise Plan or continue with no changes?).
The clinician will document the reassessment including the recommendations for revisions to the 24 hour plan in the individual’s medical record under the assessment tab. The QMRP or the Treatment Team Manager will review the assessment and report findings to the Treatment Team.
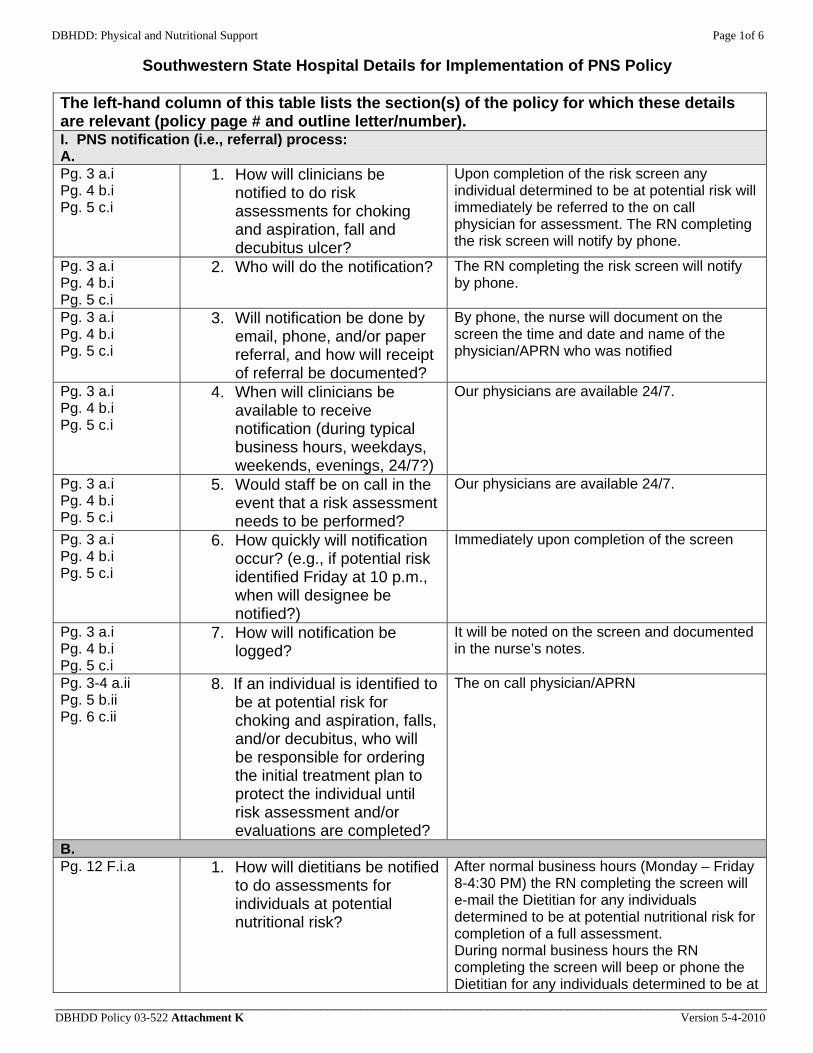
DBHDD: Physical and Nutritional Support Page 1of 6
Southwestern State Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
The left-hand column of this table lists the section(s) of the policy for which these details are relevant (policy page # and outline letter/number). I. PNS notification (i.e., referral) process: A. Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
1. How will clinicians be notified to do risk assessments for choking and aspiration, fall and decubitus ulcer?
Upon completion of the risk screen any individual determined to be at potential risk will immediately be referred to the on call physician for assessment. The RN completing the risk screen will notify by phone.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
2. Who will do the notification? The RN completing the risk screen will notify by phone.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
3. Will notification be done by email, phone, and/or paper referral, and how will receipt of referral be documented?
By phone, the nurse will document on the screen the time and date and name of the physician/APRN who was notified
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
Our physicians are available 24/7.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
5. Would staff be on call in the event that a risk assessment needs to be performed?
Our physicians are available 24/7.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
6. How quickly will notification occur? (e.g., if potential risk identified Friday at 10 p.m., when will designee be notified?)
Immediately upon completion of the screen
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
7. How will notification be logged?
It will be noted on the screen and documented in the nurse’s notes.
Pg. 3-4 a.ii Pg. 5 b.ii Pg. 6 c.ii
8. If an individual is identified to be at potential risk for choking and aspiration, falls, and/or decubitus, who will be responsible for ordering the initial treatment plan to protect the individual until risk assessment and/or evaluations are completed?
The on call physician/APRN
B. Pg. 12 F.i.a 1. How will dietitians be notified
to do assessments for individuals at potential nutritional risk?
After normal business hours (Monday – Friday 8-4:30 PM) the RN completing the screen will e-mail the Dietitian for any individuals determined to be at potential nutritional risk for completion of a full assessment. During normal business hours the RN completing the screen will beep or phone the Dietitian for any individuals determined to be at
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 2of 6
Southwestern State Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
potential nutritional risk for completion of a full assessment.
Pg. 12 F.i.a 2. Who will do the notification?
The RN completing the risk screen. The treatment team nurse will complete the annual screen and the screen for any change in status.
Pg. 12 F.i.a 3. Will notification be done by email, phone, and/or paper referral, and how will receipt of referral be documented?
During normal business hours the notification will be done by phone or beeper. After normal business hours the notification will be done by e-mail. The Dietitian will note the results of the assessment in the progress notes.
Pg. 12 F.i.a 4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
During normal business hours the clinicians will be available via phone and beeper. After normal business hours clinicians will be available via e-mail.
Pg. 12 F.i.a 5. Would staff be on call in the event that a 24 hour assessment needs to be performed?
Our physicians are on campus 24/7 and are available for consultation for any high risk individuals identified. Dietitians will not be on call 24/7.
Pg. 12 F.i.a 6. How quickly will notification occur? (e.g., if potential risk identified Friday at 10 p.m., when will designee be notified?)
Following the completion of the risk screen, the RN will notify the dietitian by phone or beeper. After normal business hours the notification will be done by e-mail. The dietitian will note the results of the assessment in the progress notes.
Pg. 12 F.i.a 7. How will notification be logged?
The dietitian will log receipt of referrals for nutritional assessments.
Pg. 12 F.i.b 8. If an individual is identified to be at potential nutritional risk, who will be responsible for ordering the initial treatment plan to protect the individual until nutrition assessment?
Physician on duty
C. Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
1. How will clinicians (contract or staff) be notified to do evaluations when clinically indicated for individuals identified to be at high risk for choking and aspiration, fall and/or decubitus ulcer?
If further evaluation is required for individuals at high risk for choking and aspiration the physician will order a consult with either OT or SLP. If further evaluation is required for individuals at high risk for falls the physician will order a consult with PT. If further evaluation is required for individuals at high risk for decubitus the physician will consult with the nursing staff for implementation of ordered interventions. If alternate positioning is required or adaptive equipment is indicated the physician will consult with PT.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
2. Who will do the notification? The RN transcribing the order
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 3of 6
Southwestern State Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
3. Will notification be done by email, phone, and/or paper referral?
By phone or email along with a paper referral for tracking purposes.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
During business hours (Monday – Friday 8-4:30) clinicians (OT, PT, SLP) will be available by phone and email for notification of the need for evaluation. For notification made outside of business hours, OT, PT, and SLP clinicians will receive and respond to receipt of notification upon the start of the business day following notification.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
5. Would staff be on call in the event that an evaluation needs to be performed?
No. A physician is on duty 24/7 for initial consultation and development of an initial plan of care until further evaluations can be performed.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
6. How quickly will notification occur? (e.g., If high risk identified Friday at 10 p.m., when will designee be notified?)
Immediately upon completion of the risk assessment indicating a high risk.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
7. How will notification be logged?
All consults are completed using the consultation sheet which is sent to the clinician as ordered by the physician. The receiving clinician will note the date and time of receipt on the consultation form and indicate in their progress note or evaluation.
D. Pg. 7 C.3 Once an individual is determined to
meet criteria for a 24 hour support plan, how will the person designated to write the initial 24-Hour Support Plan be notified?
The Interdisciplinary Treatment Team Leader/Treatment Team Nurse will be notified via e-mail for the need to develop the initial 24-Hour Support Plan. This notification will be done by the charge nurse on duty at the time it is determined an individual meets criteria for a 24 hour support plan.
II. Completion of Risk Assessments:
What trained and competent clinicians will be designated to complete the following risk assessments (by discipline, e.g., all physicians and APRNs, by team (a group of identified individuals of various clinical disciplines….)? Pg. 4 a.iii A. Choking and Aspiration Risk
Assessment Physicians/APRN’s (Input from OT and SLP)
Pg. 5 b.iii B. Fall Risk Assessment Physicians/APRN’s and PT with input from TREATMENT TEAM
Pg. 6 c.iii C. Decubitus Ulcer Risk Assessment
RN will complete the Decubitus Ulcer Risk Assessment
III. 24-Hour Support Plans Documentation:
Pg. 7 C.3 A. Who will be responsible for writing the initial 24-Hour Support Plan? How will responsible person
Team Leader or Treatment Team Nurse with input from the Treatment Team will be responsible for writing the initial 24 hour
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 4of 6
Southwestern State Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
be identified?
support plan and will act as the primary author. Input will be solicited by the primary author from other team members. The lead author will have write access and the treatment team members will have read only access.
Pg. 7 C.3 Pg. 13 H.2
B. Who will be responsible for updating revisions and changes, and how will these changes be documented?
Each discipline will provide input for changes, the team leader or team nurse will be notified by e mail to compile changes and update the original 24 hour support plan. The information will be communicated to the primary author via e-mail. The lead author will have write access and the treatment team members will have read only access.
Pg. 7 C.4 C. Who will communicate the content of the initial or revised 24 Hour Support Plan to the Treatment Team?
The Team Leader or Team Nurse
Pg. 9 C.8 D. Where will the original Plan be kept/filed? Where will there be copies (e.g., MAR, dining room, individual’s support book, medical record). Who is responsible for distributing copies and ensuring copies are updated with any change to the Plan?
The plans will be maintained in the individual’s record, dining area and the Medication Administration Record. The primary author will be responsible for updating changes to the plan and distributing these changes to the Treatment Team. The treatment team nurse/team leader will be responsible for ensuring the old copies of the support plan are replaced once the plan is revised.
IV. Protocol for communication with the TREATMENT TEAM:
A. TREATMENT TEAM approval of the 24-Hour Support Plans (new and revised):
Pg. 7 C.4 1. What is the process by which the Treatment Team approves initial and revised plans?
The Treatment team will review the 24 hour support plan during regularly scheduled/called meetings to approve or make recommendations for changes.
Pg. 7.C.4 2. Can approval be done by email, verbally, or may it require a special team meeting when clinically appropriate?
Approval will require a called Treatment team meeting when clinically indicated. For minor changes approval of the treatment team may be given via email.
Pg. 4 a.iii. Pg. 4 a.iv Pg. 5 b.iii Pg. 5 b.iv Pg. 6 c.iii Pg. 6 c.iv Pg. 12 F.i.c Pg. 14 H.3
How and when will clinicians doing the PNS Risk Screen, Risk Assessments, and/or evaluations report their findings to the other members of the Treatment Team (besides those immediately notified according to PNS procedure)? (e.g., At the next regularly scheduled Treatment Team meeting? At morning unit meetings? Email? etc.)
Email, verbally, or called Treatment Team meetings as indicated based on clinical needs. New information on any individual will be presented to the Treatment Team at the next scheduled meeting unless there is clinical indication of high risk which will necessitate a called meeting prior to the next scheduled meeting.
DBHDD Policy 03-522 Attachment K Version 5-4-2010
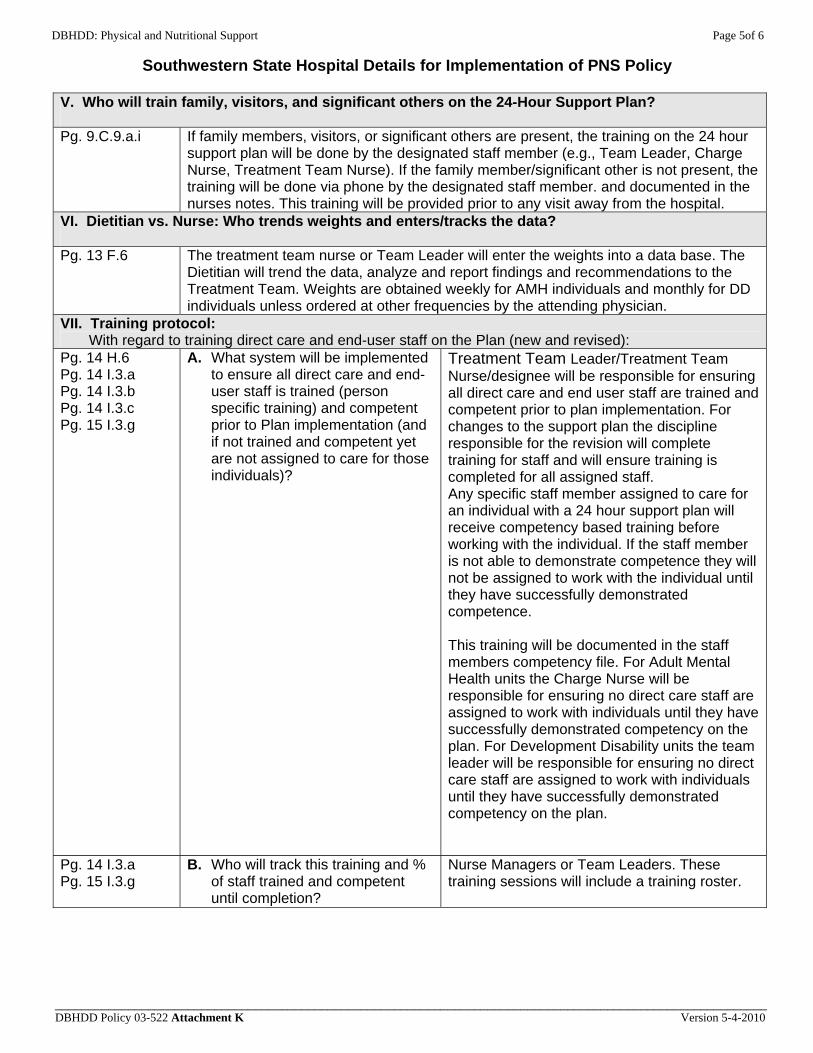
DBHDD: Physical and Nutritional Support Page 5of 6
Southwestern State Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
V. Who will train family, visitors, and significant others on the 24-Hour Support Plan?
Pg. 9.C.9.a.i If family members, visitors, or significant others are present, the training on the 24 hour support plan will be done by the designated staff member (e.g., Team Leader, Charge Nurse, Treatment Team Nurse). If the family member/significant other is not present, the training will be done via phone by the designated staff member. and documented in the nurses notes. This training will be provided prior to any visit away from the hospital.
VI. Dietitian vs. Nurse: Who trends weights and enters/tracks the data?
Pg. 13 F.6 The treatment team nurse or Team Leader will enter the weights into a data base. The Dietitian will trend the data, analyze and report findings and recommendations to the Treatment Team. Weights are obtained weekly for AMH individuals and monthly for DD individuals unless ordered at other frequencies by the attending physician.
VII. Training protocol: With regard to training direct care and end-user staff on the Plan (new and revised): Pg. 14 H.6 Pg. 14 I.3.a Pg. 14 I.3.b Pg. 14 I.3.c Pg. 15 I.3.g
A. What system will be implemented to ensure all direct care and end-user staff is trained (person specific training) and competent prior to Plan implementation (and if not trained and competent yet are not assigned to care for those individuals)?
Treatment Team Leader/Treatment Team Nurse/designee will be responsible for ensuring all direct care and end user staff are trained and competent prior to plan implementation. For changes to the support plan the discipline responsible for the revision will complete training for staff and will ensure training is completed for all assigned staff. Any specific staff member assigned to care for an individual with a 24 hour support plan will receive competency based training before working with the individual. If the staff member is not able to demonstrate competence they will not be assigned to work with the individual until they have successfully demonstrated competence. This training will be documented in the staff members competency file. For Adult Mental Health units the Charge Nurse will be responsible for ensuring no direct care staff are assigned to work with individuals until they have successfully demonstrated competency on the plan. For Development Disability units the team leader will be responsible for ensuring no direct care staff are assigned to work with individuals until they have successfully demonstrated competency on the plan.
Pg. 14 I.3.a Pg. 15 I.3.g
B. Who will track this training and % of staff trained and competent until completion?
Nurse Managers or Team Leaders. These training sessions will include a training roster.
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 6of 6
Southwestern State Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________ DBHDD Policy 03-522 Attachment K Version 5-4-2010
Pg. 15 I.3.f Pg. 15 I.3.g
C. If direct care or end-user staff is unable to demonstrate competency during person specific training OR monitoring, who is responsible for developing and tracking a “performance improvement” plan (e.g., repeat didactic training, repeat in vivo competency) through to completion?
Nurse Managers or Team Leaders will be responsible for developing and tracking a performance improvement plan for any staff not able to initially demonstrate competence.
VIII. Process for reassessing the 24-Hour Support Plan:
Pg. 13 H.1 A. Who will do the quarterly and PRN (as clinically indicated) reassessments?
The Treatment Team to include, OT, PT SLP and Dietitians as clinically indicated.
Pg. 13 H.1 B. Who will track when they are due and how will it be tracked?
Treatment team nurses or Team Leaders will complete or notify clinicians to upcoming due dates for reassessments.
Pg. 13 H.1 Pg. 13 H.2
C. What will these reassessments consist of and how will they be documented (e.g., IDN, progress notes) and communicated to the Treatment Team along with recommendations (i.e., revise Plan or continue with no changes?).
The reassessment will consist of a clinical review of the record, individual’s response to the support plan, a clinical observation of the individual, and review of any instances of choking, falling, skin breakdown, and change in weight. This review will be documented in a progress note by Treatment Team.
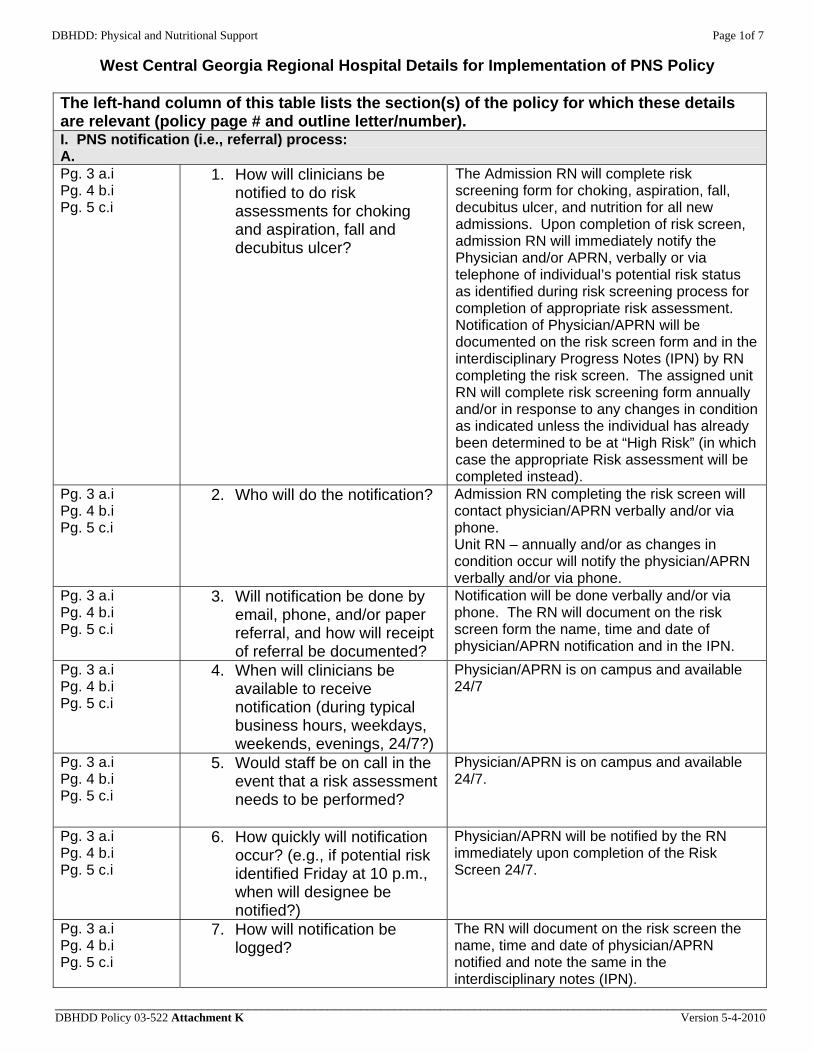
DBHDD: Physical and Nutritional Support Page 1of 7
West Central Georgia Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
The left-hand column of this table lists the section(s) of the policy for which these details are relevant (policy page # and outline letter/number). I. PNS notification (i.e., referral) process: A. Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
1. How will clinicians be notified to do risk assessments for choking and aspiration, fall and decubitus ulcer?
The Admission RN will complete risk screening form for choking, aspiration, fall, decubitus ulcer, and nutrition for all new admissions. Upon completion of risk screen, admission RN will immediately notify the Physician and/or APRN, verbally or via telephone of individual’s potential risk status as identified during risk screening process for completion of appropriate risk assessment. Notification of Physician/APRN will be documented on the risk screen form and in the interdisciplinary Progress Notes (IPN) by RN completing the risk screen. The assigned unit RN will complete risk screening form annually and/or in response to any changes in condition as indicated unless the individual has already been determined to be at “High Risk” (in which case the appropriate Risk assessment will be completed instead).
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
2. Who will do the notification? Admission RN completing the risk screen will contact physician/APRN verbally and/or via phone. Unit RN – annually and/or as changes in condition occur will notify the physician/APRN verbally and/or via phone.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
3. Will notification be done by email, phone, and/or paper referral, and how will receipt of referral be documented?
Notification will be done verbally and/or via phone. The RN will document on the risk screen form the name, time and date of physician/APRN notification and in the IPN.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
Physician/APRN is on campus and available 24/7
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
5. Would staff be on call in the event that a risk assessment needs to be performed?
Physician/APRN is on campus and available 24/7.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
6. How quickly will notification occur? (e.g., if potential risk identified Friday at 10 p.m., when will designee be notified?)
Physician/APRN will be notified by the RN immediately upon completion of the Risk Screen 24/7.
Pg. 3 a.i Pg. 4 b.i Pg. 5 c.i
7. How will notification be logged?
The RN will document on the risk screen the name, time and date of physician/APRN notified and note the same in the interdisciplinary notes (IPN).
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 2of 7
West Central Georgia Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
Pg. 3-4 a.ii Pg. 5 b.ii Pg. 6 c.ii
8. If an individual is identified to be at potential risk for choking and aspiration, falls, and/or decubitus, who will be responsible for ordering the initial treatment plan to protect the individual until risk assessment and/or evaluations are completed?
The physician/APRN will be responsible for ordering the initial treatment plan.
B. Pg. 12 F.i.a 1. How will dietitians be notified
to do assessments for individuals at potential nutritional risk?
During normal business hours, which are Monday – Friday 8:00 a.m.-5:00 p.m., the RN completing the risk screen will notify the Dietitian via email, phone and/or beeper for individuals determined to be at potential nutritional risk for completion of a full nutritional assessment. After normal business hours, the Dietitian will be notified via beeper and/or phone by the RN completing the risk screen.
Pg. 12 F.i.a 2. Who will do the notification?
The RN completing the risk screen will notify the Dietitian and document notification on the screen form and in the IPN.
Pg. 12 F.i.a 3. Will notification be done by email, phone, and/or paper referral, and how will receipt of referral be documented?
During normal business hours, the RN completing the risk screen will notify the Dietitian via email, phone and/or beeper for individuals determined to be at potential nutritional risk for completion of a full nutritional assessment. After normal business hours, the dietitian will be notified via beeper and/or phone by the RN completing the risk screen. The RN will document on the risk screen the name, time and date of notified and note same in the interdisciplinary notes (IPN).
Pg. 12 F.i.a 4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
During normal business hours, which are Monday – Friday 8:00 a.m.-5:00 p.m., the dietitian/designee is available for consultation via e mail, phone and/or beeper. After normal business hours, the Dietitian/designee is available via beeper and/or phone 24/7.
Pg. 12 F.i.a 5. Would staff be on call in the event that a 24 hour assessment needs to be performed?
No.
Pg. 12 F.i.a 6. How quickly will notification occur? (e.g., if potential risk identified Friday at 10 p.m., when will designee be notified?)
Following completion of the risk screen, the RN will notify the dietitian via email, phone and/or beeper. After normal business hours the notification will be done via phone and/or beeper. The Dietitian will document the result of the assessment in the progress notes during
DBHDD Policy 03-522 Attachment K Version 5-4-2010
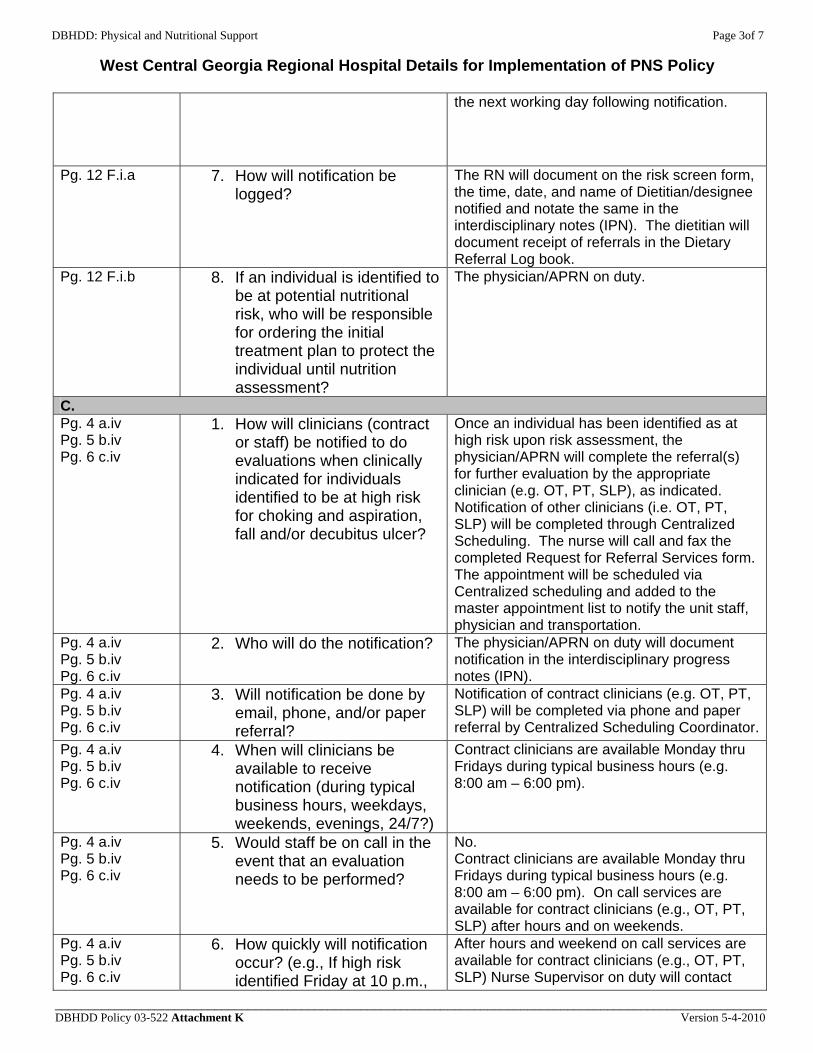
DBHDD: Physical and Nutritional Support Page 3of 7
West Central Georgia Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
the next working day following notification.
Pg. 12 F.i.a 7. How will notification be logged?
The RN will document on the risk screen form, the time, date, and name of Dietitian/designee notified and notate the same in the interdisciplinary notes (IPN). The dietitian will document receipt of referrals in the Dietary Referral Log book.
Pg. 12 F.i.b 8. If an individual is identified to be at potential nutritional risk, who will be responsible for ordering the initial treatment plan to protect the individual until nutrition assessment?
The physician/APRN on duty.
C. Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
1. How will clinicians (contract or staff) be notified to do evaluations when clinically indicated for individuals identified to be at high risk for choking and aspiration, fall and/or decubitus ulcer?
Once an individual has been identified as at high risk upon risk assessment, the physician/APRN will complete the referral(s) for further evaluation by the appropriate clinician (e.g. OT, PT, SLP), as indicated. Notification of other clinicians (i.e. OT, PT, SLP) will be completed through Centralized Scheduling. The nurse will call and fax the completed Request for Referral Services form. The appointment will be scheduled via Centralized scheduling and added to the master appointment list to notify the unit staff, physician and transportation.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
2. Who will do the notification? The physician/APRN on duty will document notification in the interdisciplinary progress notes (IPN).
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
3. Will notification be done by email, phone, and/or paper referral?
Notification of contract clinicians (e.g. OT, PT, SLP) will be completed via phone and paper referral by Centralized Scheduling Coordinator.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
4. When will clinicians be available to receive notification (during typical business hours, weekdays, weekends, evenings, 24/7?)
Contract clinicians are available Monday thru Fridays during typical business hours (e.g. 8:00 am – 6:00 pm).
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
5. Would staff be on call in the event that an evaluation needs to be performed?
No. Contract clinicians are available Monday thru Fridays during typical business hours (e.g. 8:00 am – 6:00 pm). On call services are available for contract clinicians (e.g., OT, PT, SLP) after hours and on weekends.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
6. How quickly will notification occur? (e.g., If high risk identified Friday at 10 p.m.,
After hours and weekend on call services are available for contract clinicians (e.g., OT, PT, SLP) Nurse Supervisor on duty will contact
DBHDD Policy 03-522 Attachment K Version 5-4-2010
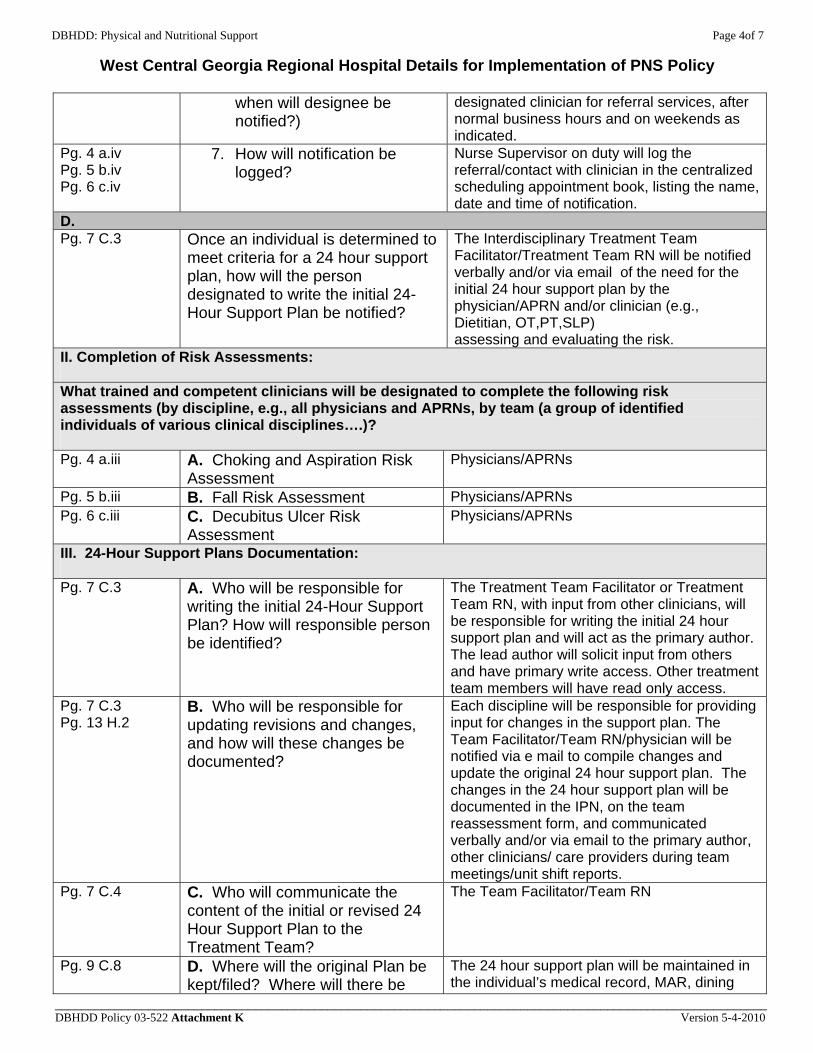
DBHDD: Physical and Nutritional Support Page 4of 7
West Central Georgia Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
when will designee be notified?)
designated clinician for referral services, after normal business hours and on weekends as indicated.
Pg. 4 a.iv Pg. 5 b.iv Pg. 6 c.iv
7. How will notification be logged?
Nurse Supervisor on duty will log the referral/contact with clinician in the centralized scheduling appointment book, listing the name, date and time of notification.
D. Pg. 7 C.3 Once an individual is determined to
meet criteria for a 24 hour support plan, how will the person designated to write the initial 24-Hour Support Plan be notified?
The Interdisciplinary Treatment Team Facilitator/Treatment Team RN will be notified verbally and/or via email of the need for the initial 24 hour support plan by the physician/APRN and/or clinician (e.g., Dietitian, OT,PT,SLP) assessing and evaluating the risk.
II. Completion of Risk Assessments:
What trained and competent clinicians will be designated to complete the following risk assessments (by discipline, e.g., all physicians and APRNs, by team (a group of identified individuals of various clinical disciplines….)? Pg. 4 a.iii A. Choking and Aspiration Risk
Assessment Physicians/APRNs
Pg. 5 b.iii B. Fall Risk Assessment Physicians/APRNs Pg. 6 c.iii C. Decubitus Ulcer Risk
Assessment Physicians/APRNs
III. 24-Hour Support Plans Documentation:
Pg. 7 C.3 A. Who will be responsible for writing the initial 24-Hour Support Plan? How will responsible person be identified?
The Treatment Team Facilitator or Treatment Team RN, with input from other clinicians, will be responsible for writing the initial 24 hour support plan and will act as the primary author. The lead author will solicit input from others and have primary write access. Other treatment team members will have read only access.
Pg. 7 C.3 Pg. 13 H.2
B. Who will be responsible for updating revisions and changes, and how will these changes be documented?
Each discipline will be responsible for providing input for changes in the support plan. The Team Facilitator/Team RN/physician will be notified via e mail to compile changes and update the original 24 hour support plan. The changes in the 24 hour support plan will be documented in the IPN, on the team reassessment form, and communicated verbally and/or via email to the primary author, other clinicians/ care providers during team meetings/unit shift reports.
Pg. 7 C.4 C. Who will communicate the content of the initial or revised 24 Hour Support Plan to the Treatment Team?
The Team Facilitator/Team RN
Pg. 9 C.8 D. Where will the original Plan be kept/filed? Where will there be
The 24 hour support plan will be maintained in the individual’s medical record, MAR, dining
DBHDD Policy 03-522 Attachment K Version 5-4-2010

DBHDD: Physical and Nutritional Support Page 5of 7
West Central Georgia Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
copies (e.g., MAR, dining room, individual’s support book, medical record). Who is responsible for distributing copies and ensuring copies are updated with any change to the Plan?
area and log book. The Team Facilitator/Team RN will be responsible for updating changes to the plan and distributing updated copies to other members of the team, as well as placing updated copies in the MAR, dining area, and log book.
IV. Protocol for communication with the TREATMENT TEAM:
A. TREATMENT TEAM approval of the 24-Hour Support Plans (new and revised):
Pg. 7 C.4 1. What is the process by which the Treatment Team approves initial and revised plans?
The Treatment team will review the 24 hour support plan during regularly scheduled Treatment Team Meetings or called Treatment Team meetings as indicated, to approve, revise or make recommendations for changes to the plan.
Pg. 7.C.4 2. Can approval be done by email, verbally, or may it require a special team meeting when clinically appropriate?
Approval of the initial and revised 24 hour support plan will require a called treatment team meeting when clinically appropriate. However, minor changes (e.g., changes to equipment) to the 24 hour support plan may be done verbally or via email.
Pg. 4 a.iii. Pg. 4 a.iv Pg. 5 b.iii Pg. 5 b.iv Pg. 6 c.iii Pg. 6 c.iv Pg. 12 F.i.c Pg. 14 H.3
How and when will clinicians doing the PNS Risk Screen, Risk Assessments, and/or evaluations report their findings to the other members of the Treatment Team (besides those immediately notified according to PNS procedure)? (e.g., At the next regularly scheduled Treatment Team meeting? At morning unit meetings? Email? etc.)
Notification of risk assessment evaluation/findings are completed via e mail, verbally, during shift reports, regular team meetings and/or called Treatment team meetings as indicated. New information and/or changes in status or treatment for the individual is communicated via e mail, verbally, during shift reports, at morning meetings, scheduled and/or called Treatment Team Meetings.
V. Who will train family, visitors, and significant others on the 24-Hour Support Plan?
Pg. 9.C.9.a.i Training for family, visitors and significant others on the 24-Hour Support Plan will be provided by the Team Facilitator/Team RN or Charge RN when family is present during the treatment team meeting and/or on campus. If family, visitors and/or significant others is not present, training will be completed by the Team Facilitator/Team RN or Charge RN via phone and documented in the IPN notes upon implementation of the initial 24 hour support plan. Retraining will be provided as often as indicated by changes/revisions in the 24 hour support plan and the family, visitors and/or significant others’ ability to verbalize their understanding regarding the 24 hour support plan. Family, visitors and significant others will not be allowed to bring food to individual prior to training on support plan and approval from physician/treatment team.
VI. Dietitian vs. Nurse: Who trends weights and enters/tracks the data?
Pg. 13 F.6 The Team RN/Primary RN will track and enter weights into a data base. The dietitian will trend the data, analyze, report findings and make recommendations to the Treatment Team.
VII. Training protocol:
DBHDD Policy 03-522 Attachment K Version 5-4-2010
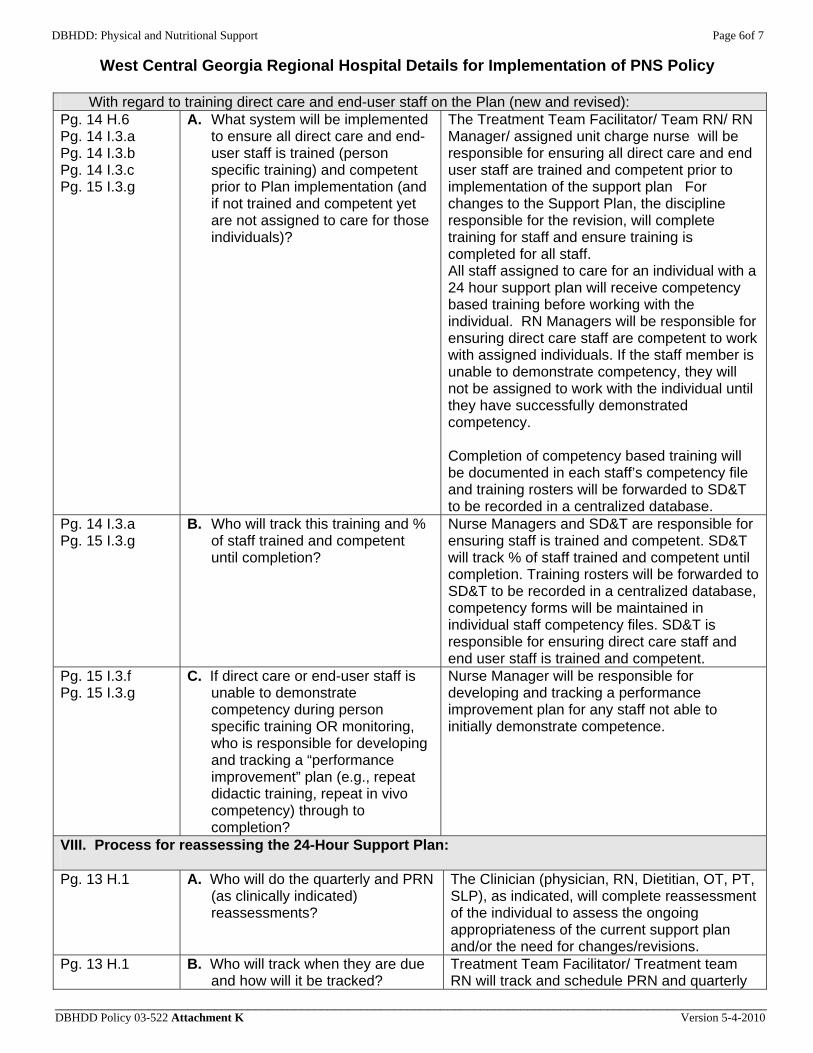
DBHDD: Physical and Nutritional Support Page 6of 7
West Central Georgia Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________
With regard to training direct care and end-user staff on the Plan (new and revised): Pg. 14 H.6 Pg. 14 I.3.a Pg. 14 I.3.b Pg. 14 I.3.c Pg. 15 I.3.g
A. What system will be implemented to ensure all direct care and end-user staff is trained (person specific training) and competent prior to Plan implementation (and if not trained and competent yet are not assigned to care for those individuals)?
The Treatment Team Facilitator/ Team RN/ RN Manager/ assigned unit charge nurse will be responsible for ensuring all direct care and end user staff are trained and competent prior to implementation of the support plan For changes to the Support Plan, the discipline responsible for the revision, will complete training for staff and ensure training is completed for all staff. All staff assigned to care for an individual with a 24 hour support plan will receive competency based training before working with the individual. RN Managers will be responsible for ensuring direct care staff are competent to work with assigned individuals. If the staff member is unable to demonstrate competency, they will not be assigned to work with the individual until they have successfully demonstrated competency. Completion of competency based training will be documented in each staff’s competency file and training rosters will be forwarded to SD&T to be recorded in a centralized database.
Pg. 14 I.3.a Pg. 15 I.3.g
B. Who will track this training and % of staff trained and competent until completion?
Nurse Managers and SD&T are responsible for ensuring staff is trained and competent. SD&T will track % of staff trained and competent until completion. Training rosters will be forwarded to SD&T to be recorded in a centralized database, competency forms will be maintained in individual staff competency files. SD&T is responsible for ensuring direct care staff and end user staff is trained and competent.
Pg. 15 I.3.f Pg. 15 I.3.g
C. If direct care or end-user staff is unable to demonstrate competency during person specific training OR monitoring, who is responsible for developing and tracking a “performance improvement” plan (e.g., repeat didactic training, repeat in vivo competency) through to completion?
Nurse Manager will be responsible for developing and tracking a performance improvement plan for any staff not able to initially demonstrate competence.
VIII. Process for reassessing the 24-Hour Support Plan:
Pg. 13 H.1 A. Who will do the quarterly and PRN (as clinically indicated) reassessments?
The Clinician (physician, RN, Dietitian, OT, PT, SLP), as indicated, will complete reassessment of the individual to assess the ongoing appropriateness of the current support plan and/or the need for changes/revisions.
Pg. 13 H.1 B. Who will track when they are due and how will it be tracked?
Treatment Team Facilitator/ Treatment team RN will track and schedule PRN and quarterly
DBHDD Policy 03-522 Attachment K Version 5-4-2010
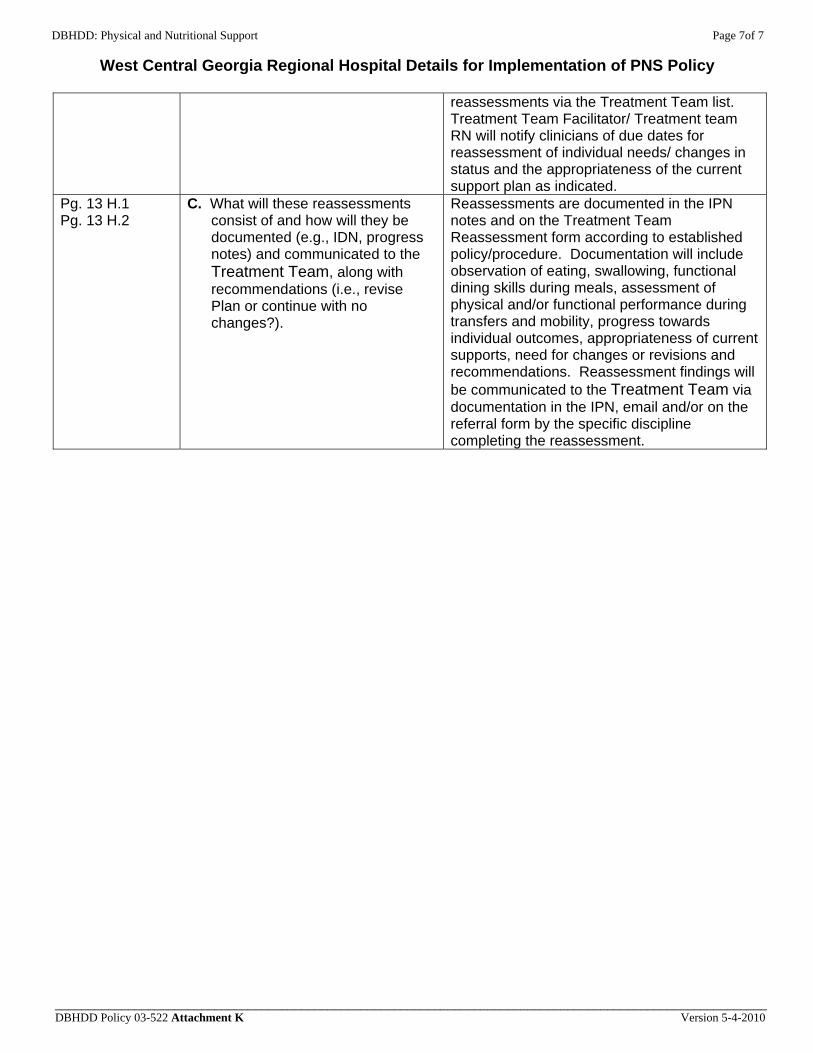
DBHDD: Physical and Nutritional Support Page 7of 7
West Central Georgia Regional Hospital Details for Implementation of PNS Policy
___________________________________________________________________________________________________________ DBHDD Policy 03-522 Attachment K Version 5-4-2010
reassessments via the Treatment Team list. Treatment Team Facilitator/ Treatment team RN will notify clinicians of due dates for reassessment of individual needs/ changes in status and the appropriateness of the current support plan as indicated.
Pg. 13 H.1 Pg. 13 H.2
C. What will these reassessments consist of and how will they be documented (e.g., IDN, progress notes) and communicated to the Treatment Team, along with recommendations (i.e., revise Plan or continue with no changes?).
Reassessments are documented in the IPN notes and on the Treatment Team Reassessment form according to established policy/procedure. Documentation will include observation of eating, swallowing, functional dining skills during meals, assessment of physical and/or functional performance during transfers and mobility, progress towards individual outcomes, appropriateness of current supports, need for changes or revisions and recommendations. Reassessment findings will be communicated to the Treatment Team via documentation in the IPN, email and/or on the referral form by the specific discipline completing the reassessment.