autism spectrum disorder and toddlers regional autism spectrum team cork & kerry september 2013
TRANSCRIPT
Autism Spectrum Disorder and Toddlers
Regional Autism Spectrum Team
Cork & Kerry
September 2013

Aims of this session
To increase your knowledge of:
1. Current best practise guidelines re Assessment of toddlers with possible ASD
2. Typical toddler development in the areas of social interaction, play and communication
3. Signs of an ASD in a toddler.

Autism Diagnostic Assessments and Toddlers
• Parents generally identify concerns regarding their’s child’s development between 12-18 months. (Zwaigenbaum et al,2009)
• Clinical guidelines on the early identification, screening, and diagnosis of ASD recommend that 18- and 24-month-olds be screened for an ASD. (NICE guidelines,
1. Best Practise Guidelines on screening
and assessment with Toddlers. • The following information is mainly based on:
– NICE Clinical guidelines: Autism diagnosis in children and young people. Recognition, referral and diagnosis of children and young people on the autism spectrum. (2011)
– Scottish Intercollegiate Guidelines Network (SIGN). (2007) Assessment, diagnosis and clinical interventions for children and young people with autism spectrum disorders. A national clinical guideline.
– Also consulted the Canadian best practise, Californian Best practise and the Vermont Best practise guidelines.

• Be aware that in some children and young people there may be uncertainty• about the diagnosis of autism, particularly in:• children younger than 24 months• children or young people with a developmental age of less than 18 months• children or young people for whom there is a lack of available information
about• their early life (for example some looked-after or adopted children)• older teenagers• children or young people with a complex coexisting mental health disorder
(for• example ADHD, conduct disorder, a possible attachment disorder), sensory• impairment (for example severe hearing or visual impairment), or a motor
disorder• such as cerebral palsy.

• The assessment of children and young people with developmental delay, emotional and
• behavioural problems, or genetic syndromes should include surveillance for ASD as part
• of routine practice.• Healthcare professionals should consider informing
families that there is a substantial• increased risk of ASD in siblings of affected children.• C The use of an appropriate structured instrument
may be a useful supplement to the• clinical process to identify children and young
people at high risk of ASD
• The evidence regarding the minimum age at which ASD can be reliably diagnosed is not clear.
• Findings suggest that:• the diagnosis of autism is always more reliable and
stable than the diagnosis of other autism• spectrum disorders, regardless of age, and can be
reliably diagnosed between the ages of• 2-3 years by experienced healthcare professionals.39,
40• in children later identified as having ASD, features
reported when they were under two• years may have been non-specific.41

• Early identification is essential for early therapeutic intervention and leads
• to a higher quality of life for the child and family
• Social-communication, notably a lack of/atypicalities in• Eye gaze and shared/joint attention• Affect and its regulation (eg, less positive and more negative affect)• Social/reciprocal smiling• Social interest and shared enjoyment (in absence of physical contact such• as tickling)• Orienting to name called• Development of gestures (eg, pointing)• Coordination of different modes of communication (eg, eye gaze, facial• expression, gesture, vocalization)• Play, notably• Reduced imitation of actions with objects• Excessive manipulation/visual exploration of toys and other objects• Repetitive actions with toys and other objects• Language and cognition, notably a lack of/delays or atypicalities in• Cognitive development• Babbling, particularly back-and-forth social babbling• Language comprehension and production (eg, odd first words or• unusually repetitive)• Unusual prosody/tone of voice• Regression/loss of early words and/or social-emotional• engagement/connectedness• Visual/other sensory and motor, notably• Atypical visual tracking, visual fixation (eg, on lights) and unusual• inspection of objects• Underreactive and/or overreactive to sounds or other forms of sensory• stimulation• Decreased activity levels and delayed fine and gross motor skills• Repetitive motor behaviors and atypical posturing/motor mannerisms• Atypicalities in regulatory functions related to sleep, eating, and attention

• First, some children with ASDs, particularly those• with more intact language and intellectual development,• may have more subtle symptoms at an early age.44,50• Speech delays are often the concern that parents first• report, so for children without marked delays, early• symptoms may be less apparent. As well, a proportion of• children with ASD symptoms may show “plateauing,”• deceleration, or frank losses in cognitive and social development• or functioning in the second year.44,48,50 Thus,• mild symptoms and even an absence of symptoms at 18• months do not “rule out” a later diagnosis of ASDs.• Ongoing surveillance and follow-up are essential, particularly• for children who are referred because of early• concerns but do not initially receive an ASD diagnosis
• Second, it may be difficult to distinguish between• ASDs and other atypical patterns of development at an• early age. This may be especially true among infant• siblings of children with ASDs, who are at risk not only• for ASDs but also for a broader spectrum of delays including• but not limited to the areas of emotion expression• and referential communication.20,53,94–98 Similarly,• early diagnosis of ASDs may be difficult in toddlers with• severe developmental delays, or impairments in vision• and/or hearing, for whom standardized diagnostic instruments• have shown limited specificity.80,99

• Often, a misdiagnosis that
• results in a child failing to receive necessary services is the greatest concern. On the other
• hand, over-diagnosis has negative consequences for individual children, public health
• strategies and research.

• Toddlers diagnosed with an ASD according to the DSM-5 were found to represent a more impaired population compared to those who qualified for a diagnosis of an ASD based on the DSM-IV-TR, but not the DSM-5. The group diagnosed according to the DSM-IV-TR represented a population of toddlers who were more impaired than atypically developing peers.
• Conclusions: The proposed changes to the DSM will likely result in those diagnosed with an ASD according to the new criteria representing a more functionally impaired group

• Population screening for ASD is not recommended. False positive or false negative results from
• inappropriate use of screening tests may delay correct diagnosis. The decision about the need
• for referral and further assessment should be made on clinical grounds. As part of the core programme of child health surveillance, healthcare professionals
• can contribute to the early identification of children requiring further assessment for
• ASD, and other developmental disorders:• clinical assessment should incorporate a high level of vigilance for features• suggestive of ASD, in the domains of social interaction and play, speech and
language• development and behaviour• CHAT or M-CHAT can be used in young children to identify clinical features• indicative of an increased risk of ASD but should not be used to rule out ASD.

Autism in Infancy and Early Childhood
• During the first 6-8 months babies who later received a diagnosis show diminished visual attention to people,
• They tend to seek others less frequently and are less likely to engage in early social communicative exchanges (i.e. smiling at others, vocalising).
• No different from typical children exploring and showing interest in objects.

• delay or absence of spoken language• looks through people; not aware of others• not responsive to other people’s facial expression/feelings• lack of pretend play; little or no imagination• does not show typical interest in or play near peers purposefully• lack of turn-taking• unable to share pleasure• qualitative impairment in non-verbal communication• does not point at an object to direct another person to look at it• lack of gaze monitoring• lack of initiation of activity or social play• unusual or repetitive hand and finger mannerisms• unusual reactions, or lack of reaction, to sensory stimuli

abnormalities in language development including mutenessodd or inappropriate prosodypersistent echolaliareference to self as ‘you’, ‘she’ or ‘he’ beyond three yearsunusual vocabulary for child’s age/social grouplimited use of language for communication and/or tendency to talk freely only aboutspecific topicsSocial impairmentsinability to join in play of other children or inappropriate attempts at joint play (maymanifest as aggressive or disruptive behaviour)lack of awareness of classroom ‘norms’ (criticising teachers, overt unwillingness to cooperatein classroom activities, inability to appreciate or follow current trends)easily overwhelmed by social and other stimulationfailure to relate normally to adults (too intense/no relationship)showing extreme reactions to invasion of personal space and resistance to being hurriedImpairments of interests, activities and/or behaviourslack of flexible cooperative imaginative play/creativitydifficulty in organising self in relation to unstructured space (eg hugging the perimeter ofplaygrounds, halls)inability to cope with change or unstructured situations, even ones that other childrenenjoy (school trips, teachers being away etc)Other factorsunusual profile of skills/deficitsany other evidence of odd behaviours including unusual responses to sensory stimuli

Infants and toddlers with Autism vs. typical toddlers
Excessive mouthing
Aversive to social touch
Poor response to name,
Infrequent looking at objects held by others
Limited ability to anticipate being picked up,
Low frequency of looking at people,
Little interest in interactive games,
Little affection toward familiar people
Content to be alone
1st
year
Stereotypical Behaviours
CommunicationSocial Interaction

Early Communicate intentTypical developing child Child with an ASD
By 12 months: Recognise mothers voice
Synchronising their patterns of eye gaze, movements, facial expressions of affectVocal turn taking
Requesting objects, rejecting offered actions, calling attention to objects and events and commenting on their appearance using gestures such as reaching, pointing, pushing away, shaking head. (gradually accompanied or replaced by sounds and words)
Beginning to understand words- esp .in games/routines: show me your nose!, lets play pat a cake
Less responsive to people speaking, their mothers voice or to their name.
Limited in the variety of communicative behaviours
Expressive language skills developing at a slower rate
Frequency of initiation joint attention and imitation are strong predictors for language acquisition in children with an ASD
Vocalisations less likely to be paired with non-verbals
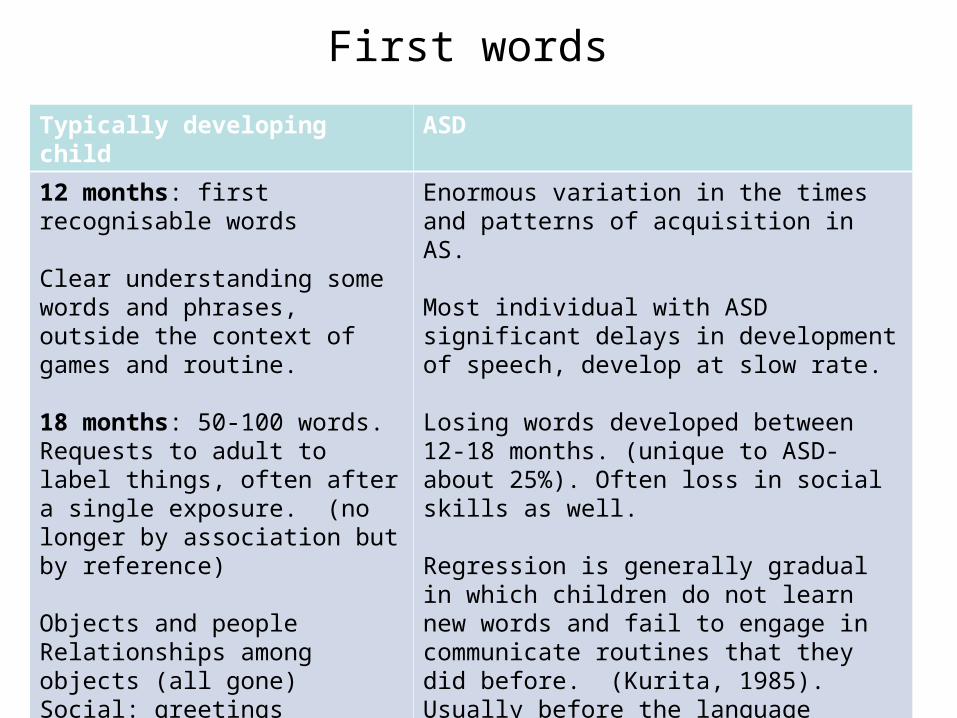
First words
Typically developing child ASD
12 months: first recognisable words
Clear understanding some words and phrases, outside the context of games and routine.
18 months: 50-100 words. Requests to adult to label things, often after a single exposure. (no longer by association but by reference)
Objects and peopleRelationships among objects (all gone)Social: greetingsIdeas: uh-oh, more
Enormous variation in the times and patterns of acquisition in AS.
Most individual with ASD significant delays in development of speech, develop at slow rate.
Losing words developed between 12-18 months. (unique to ASD- about 25%). Often loss in social skills as well.
Regression is generally gradual in which children do not learn new words and fail to engage in communicate routines that they did before. (Kurita, 1985). Usually before the language explosion.
Only a minimal relationship between language regression and later outcome- usually slightly lower verbal IQ scores compared with those with no language loss.
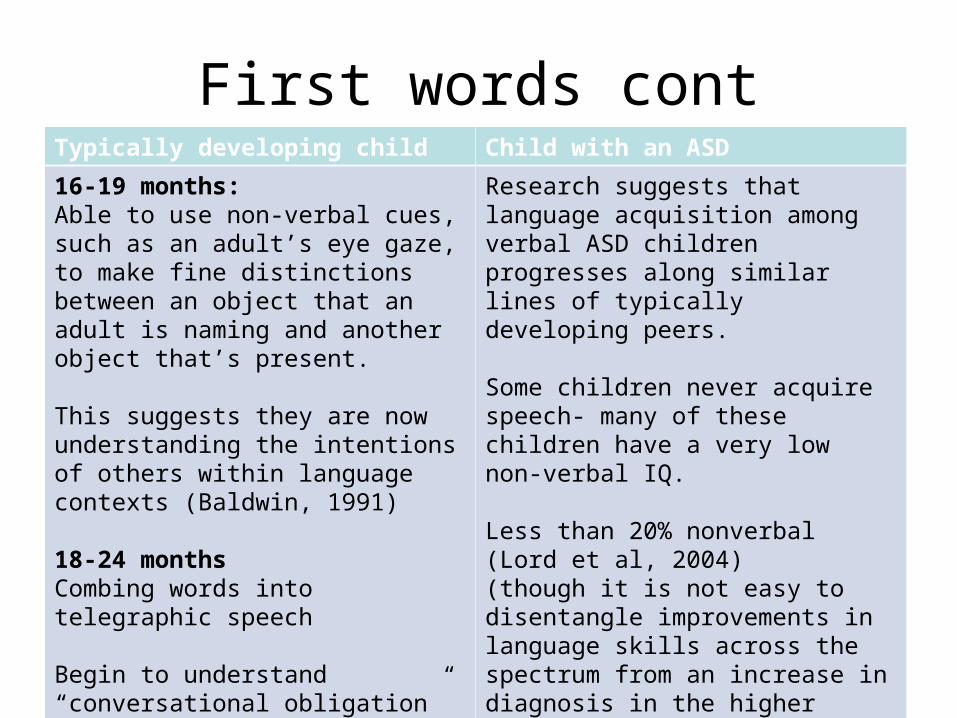
First words contTypically developing child Child with an ASD
16-19 months: Able to use non-verbal cues, such as an adult’s eye gaze, to make fine distinctions between an object that an adult is naming and another object that’s present.
This suggests they are now understanding the intentions of others within language contexts (Baldwin, 1991)
18-24 monthsCombing words into telegraphic speech
Begin to understand “conversational obligation” to answer speech with speech. They ask AND answer questions, taking part in back and forth conversations.
Research suggests that language acquisition among verbal ASD children progresses along similar lines of typically developing peers.
Some children never acquire speech- many of these children have a very low non-verbal IQ.
Less than 20% nonverbal (Lord et al, 2004)(though it is not easy to disentangle improvements in language skills across the spectrum from an increase in diagnosis in the higher functioning population).
Articulation often normal.

Linguistic StructuresTypical developing child Child with an ASD
2-5 years: fully grammatical forms. Approximately more and more to language spoken at home.
Content expands to allow reference to events remote in time and space.
Children begin to use their language in more diverse way to include imaginative, nonliteral, interpretative and logical functions
Maintain and add new information to a conversational topic, clarify and request clarification of misunderstood utterances, make request and comments using polite or indirect forms, choose appropriate speech style on the basis of the speakers role and the listeners status.
Different types of discourse: storytelling, recounting events, personal narratives, all of which follow cultural conventions for these diverse genres of linguistic reporting.
Often slower in development but same path.
Confusion of personal pronouns- however can occur in children with SLI and blind children: but MOST common in ASD. Pronoun confusion is seen as a reflection of difficulties in notions of self and other and in shifting roles between the speaker and listener. (perspective taking).

Echolalia
One of the most Salient features of an ASD but NOT unique to ASD. Most common in ASD though.
Immediate or delayed and functional or non-functional.
Echolalia- also occurs in: • blind children, • children with language impairments, • older people with dementia • TYPICALLY DEVELOPING CHILDREN!For all children will decline over the course of
development.