autonomic neuroscience from bench to bedside
DESCRIPTION
Autonomic Neuroscience from Bench to Bedside. Ann Arbor May 14, 2004. Mentoring Advice. Become a skilled clinician Use the best methodology Know everything about something Work hard John B. Youmans, John A. Oates and Victor A. McKusick. How Dysautonomias Teach Us. Amplification of Signal. - PowerPoint PPT PresentationTRANSCRIPT
Autonomic Neuroscience from Bench to Bedside
Ann Arbor
May 14, 2004
Mentoring Advice
• Become a skilled clinician
• Use the best methodology
• Know everything about something
• Work hard
– John B. Youmans, John A. Oates and Victor A. McKusick
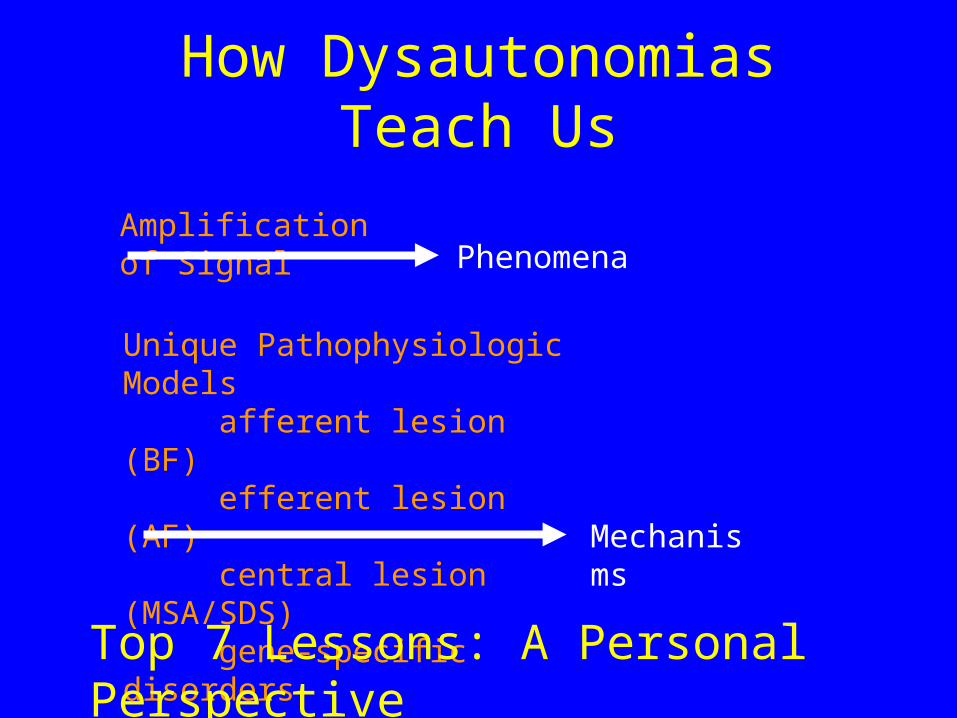
How Dysautonomias Teach Us
Amplification of Signal
Unique Pathophysiologic Modelsafferent lesion (BF)efferent lesion (AF)central lesion (MSA/SDS)gene-specific disorders
Phenomena
Mechanisms
Top 7 Lessons: A Personal Perspective
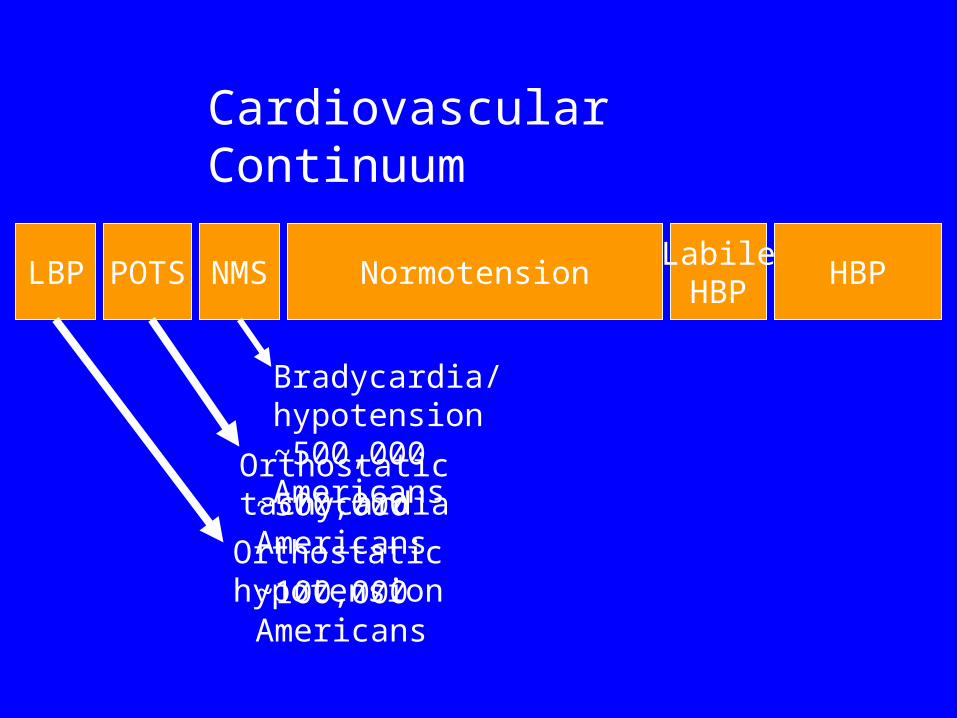
LBP POTS NormotensionLabileHBP
HBP
Cardiovascular Continuum
Orthostatic tachycardia
Orthostatic hypotension
~500,000 Americans
~100,000 Americans
NMS
Bradycardia/hypotension~500,000 Americans
Top 7 Lessons From Dysautonomias
• You can live without norepinephrine (NE)
• Dopamine can be important in BP control
• Baroreflex failure (BF) can present as Pheo
• BF can present as malignant vagotonia
• Food and water powerfully affect BP
• Orthostatic tachycardia (POTS) is common
• Too much NE can be bad for you
DBH Deficiency
• Severe orthostatic hypotension• Ptosis of the eyelids• Complicated perinatal course
– Shock– Hypoglycemia– Hypothermia
• Nasal stuffiness• Retrograde ejaculation
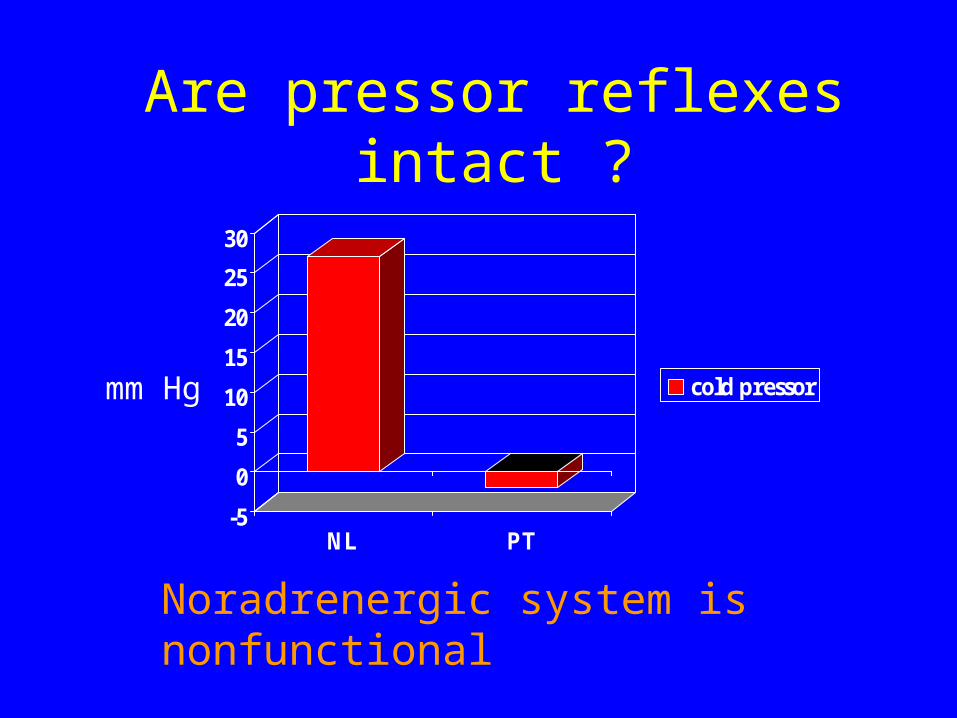
Are pressor reflexes intact ?
-5
0
5
10
15
20
25
30
NL PT
cold pressormm Hg
Noradrenergic system is nonfunctional
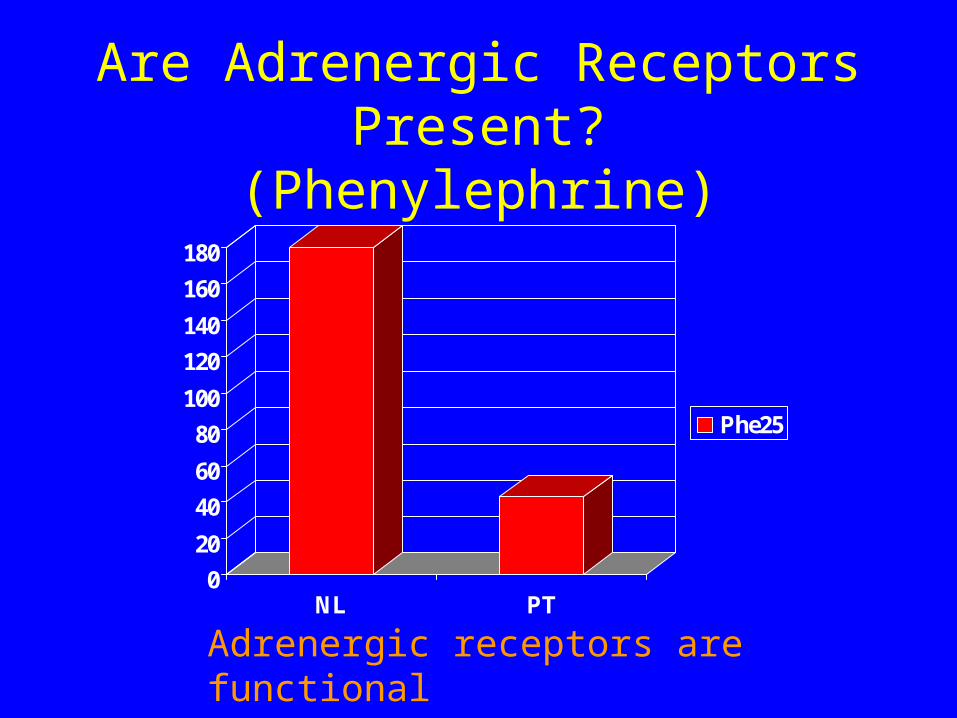
Are Adrenergic Receptors Present?(Phenylephrine)
0
20
40
60
80
100
120
140
160
180
NL PT
Phe25
Adrenergic receptors are functional
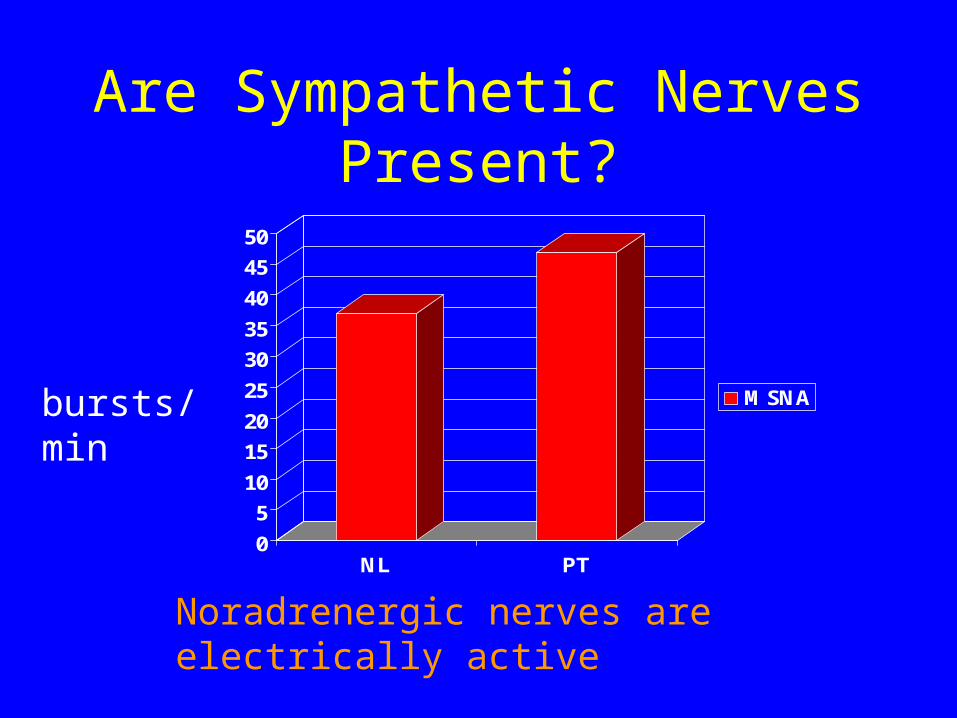
Are Sympathetic Nerves Present?
0
5
10
15
20
25
30
35
40
45
50
NL PT
MSNAbursts/min
Noradrenergic nerves are electrically active
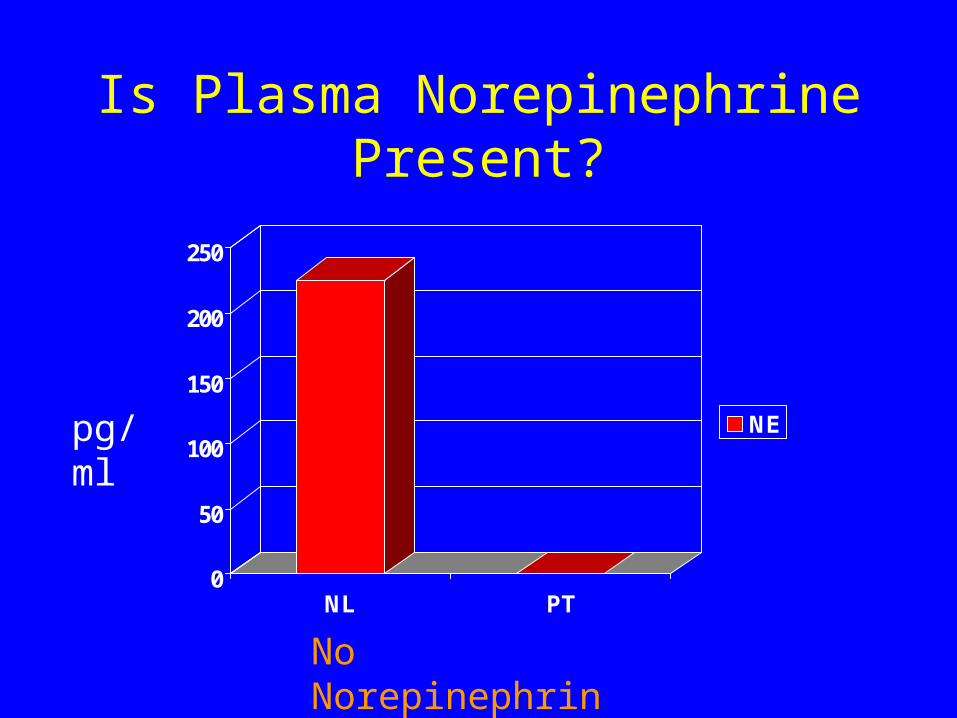
Is Plasma Norepinephrine Present?
0
50
100
150
200
250
NL PT
NEpg/ml
No Norepinephrine

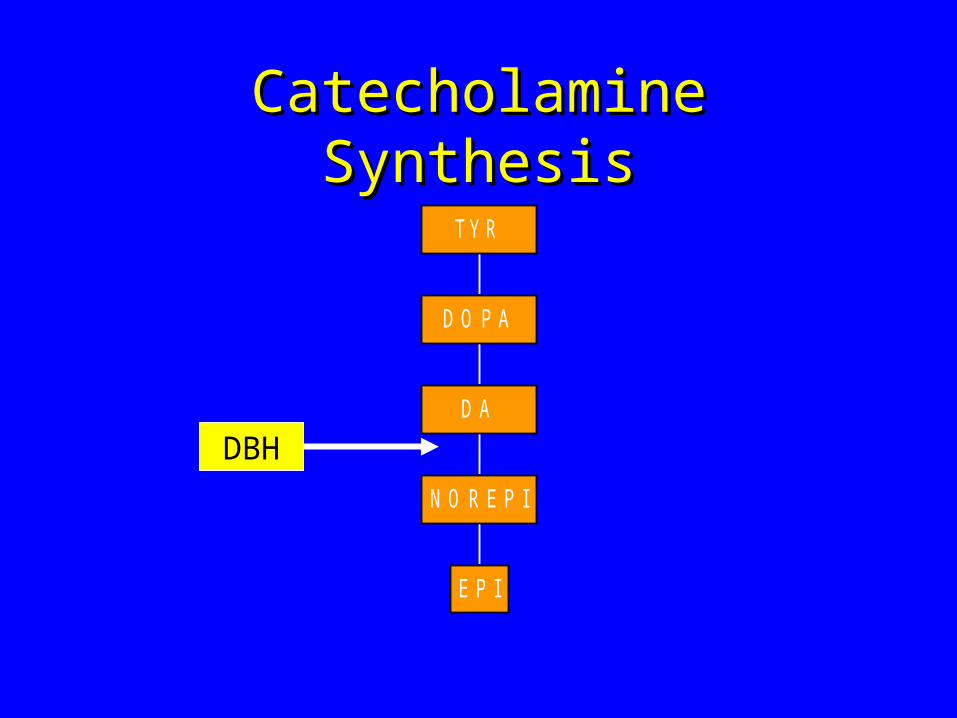
Catecholamine SynthesisCatecholamine Synthesis
E P I
N O R E P I
D A
D O P A
TY R
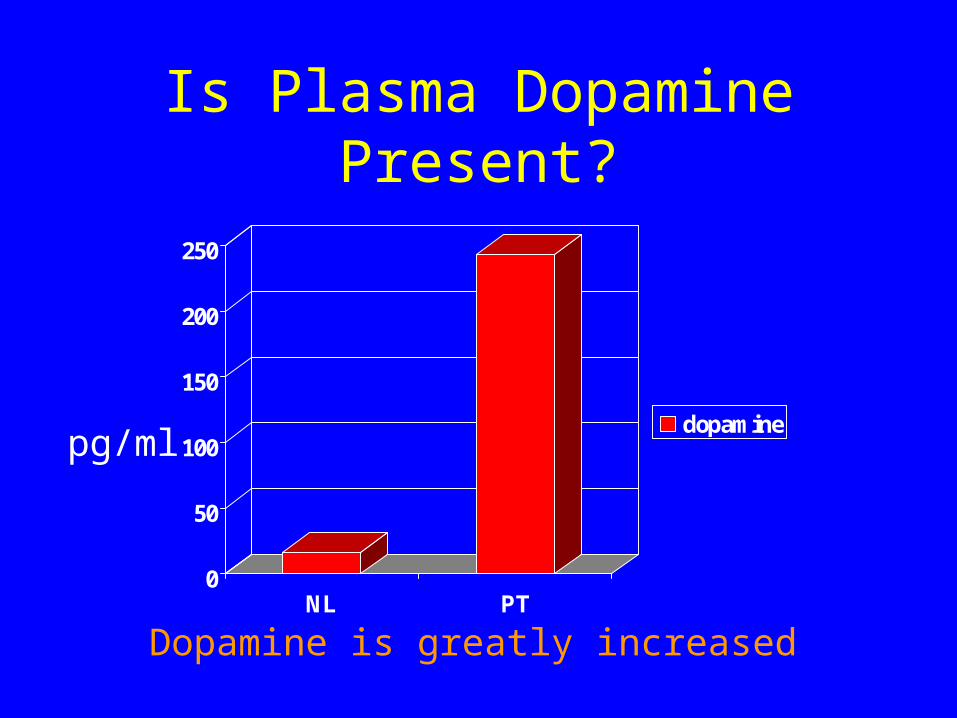
Is Plasma Dopamine Present?
0
50
100
150
200
250
NL PT
dopamine
Dopamine is greatly increased
pg/ml

Plasma DA >> NE
0
50
100
150
200
250
NL PT
DANEpg/ml
DA replacing NE ?
Catecholamine SynthesisCatecholamine Synthesis
E P I
N O R E P I
D A
D O P A
TY R
DBH
DBH Deficiency Genetics
• IVS1+2T>C is causative in both patients.
• Missense mutation in exon 2.
• Missense mutations in exons 1 and 6.
Kim K-S, Am J Hum Gen 2002; 108: 140
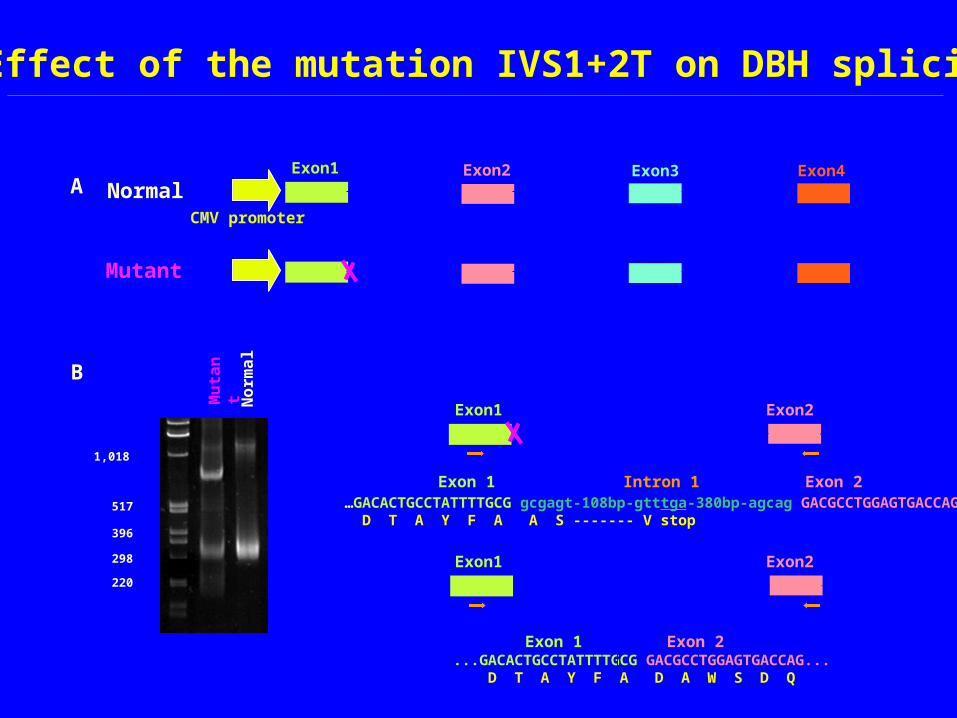
...GACACTGCCTATTTTGCG GACGCCTGGAGTGACCAG... D T A Y F A D A W S D Q
Exon1 Exon2
Exon 1 Exon 2
…GACACTGCCTATTTTGCG gcgagt-108bp-gtttga-380bp-agcag GACGCCTGGAGTGACCAG D T A Y F A A S ------- V stop
Exon 1 Intron 1
1,018
517
396
298
220
Exon 2
Exon1 Exon2
B
Effect of the mutation IVS1+2T on DBH splicing
No
rma
l
Mu
tan
t
AExon1 Exon2 Exon3 Exon4
CMV promoter
Normal
Mutant
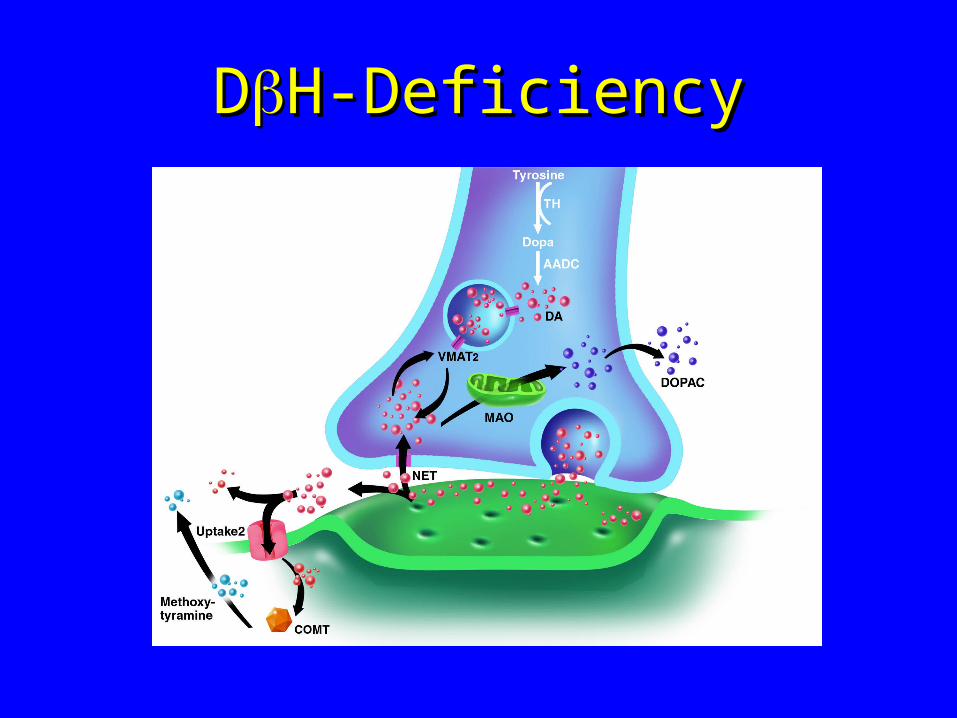
DDH-DeficiencyH-Deficiency

DOPS TherapyDOPS Therapy
DOPSDOPSDOPS
NE
NE

DOPS* Restores NE to Normal
0
100
200
300
400
500
600
Placebo DOPS
DANEStand Time
pg/ml orseconds
*Norepinephrine-COOH
Catechols in DBH Deficiency
• ‘Normal’ cognitive and psychiatric faculties• Completely absent in blood, CSF, urine:
– Norepinephrine– Epinephrine– Normetanephrine– Metanephrine– DHPG– VMA
Top 7 Lessons From Dysautonomias
• You can live without norepinephrine (NE)
• Dopamine can be important in BP control
• Baroreflex failure (BF) can present as Pheo
• BF can present as malignant vagotonia
• Food and water powerfully affect BP
• Orthostatic tachycardia (POTS) is common
• Too much NE can be bad for you
• “Why is BP low in DBH Deficiency ? – because NE is absent ?– or because DA is raised ?”
…..Otto Kuchel, Montreal
Metyrosine blocks tyrosine hydroxylase causing hypotension by lowering NE
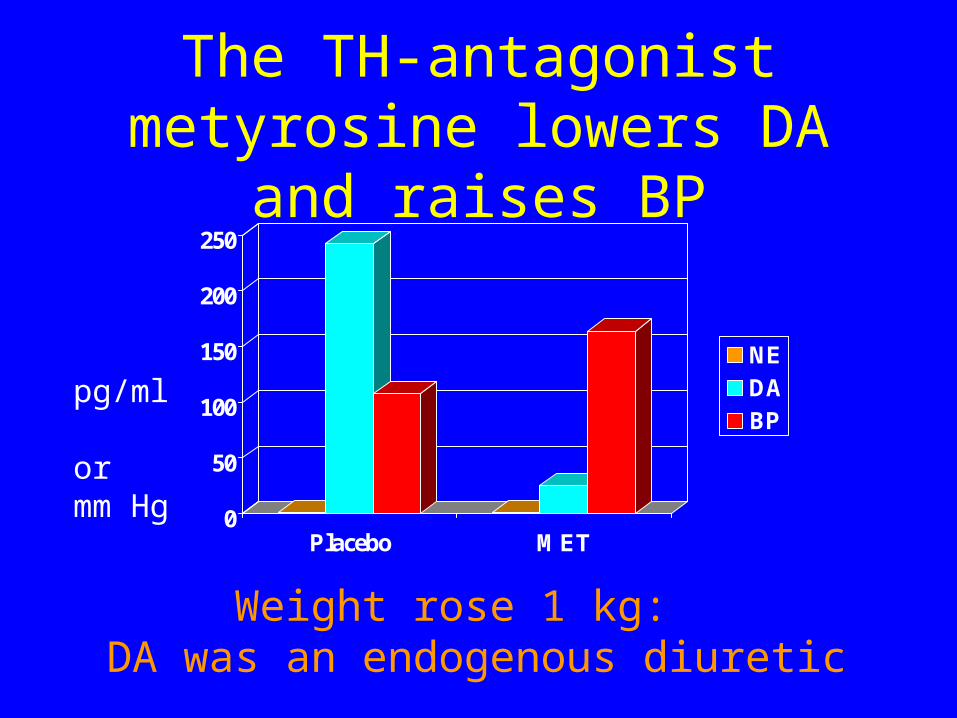
The TH-antagonist metyrosine lowers DA and raises BP
0
50
100
150
200
250
Placebo MET
NEDABP
pg/ml ormm Hg
Weight rose 1 kg: DA was an endogenous diuretic
Top 7 Lessons From Dysautonomias
• You can live without norepinephrine (NE)
• Dopamine can be important in BP control
• Baroreflex failure (BF) can present as Pheo
• BF can present as malignant vagotonia
• Food and water powerfully affect BP
• Orthostatic tachycardia (POTS) is common
• Too much NE can be bad for you
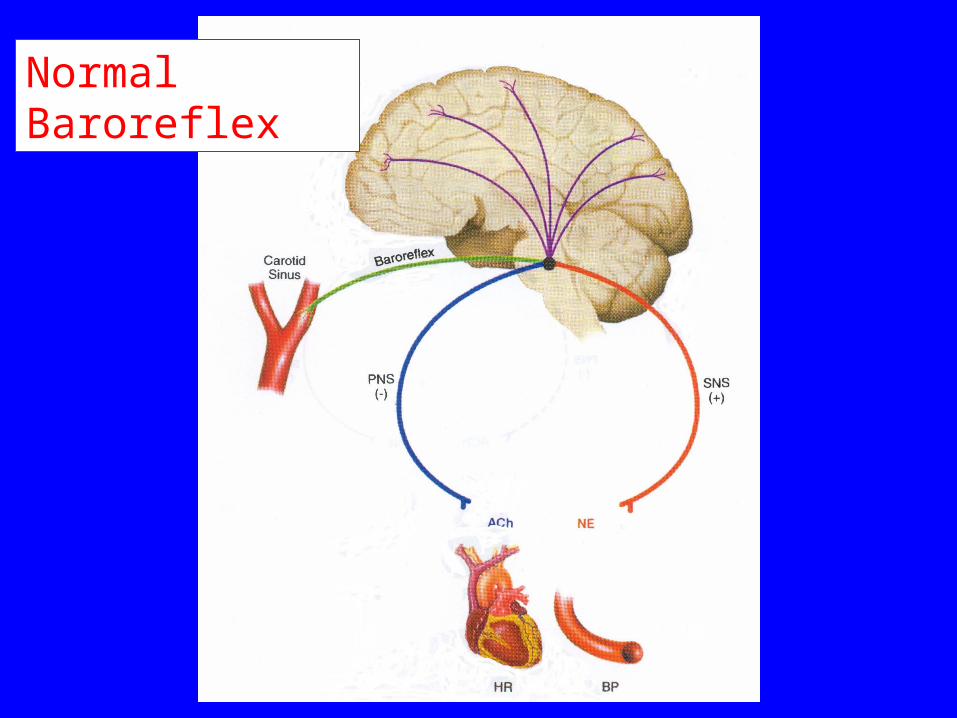
Normal Baroreflex
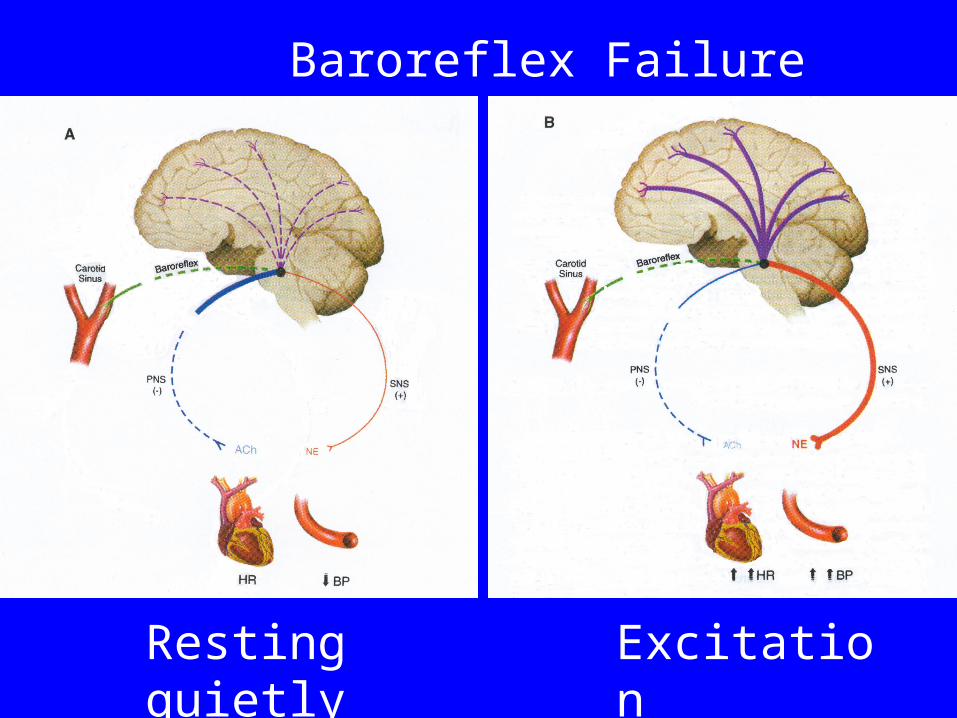
Baroreflex Failure
Resting quietly Excitation
Top 7 Lessons From Dysautonomias
• You can live without norepinephrine (NE)
• Dopamine can be important in BP control
• Baroreflex failure (BF) can present as Pheo
• BF can present as malignant vagotonia
• Food and water powerfully affect BP
• Orthostatic tachycardia (POTS) is common
• Too much NE can be bad for you
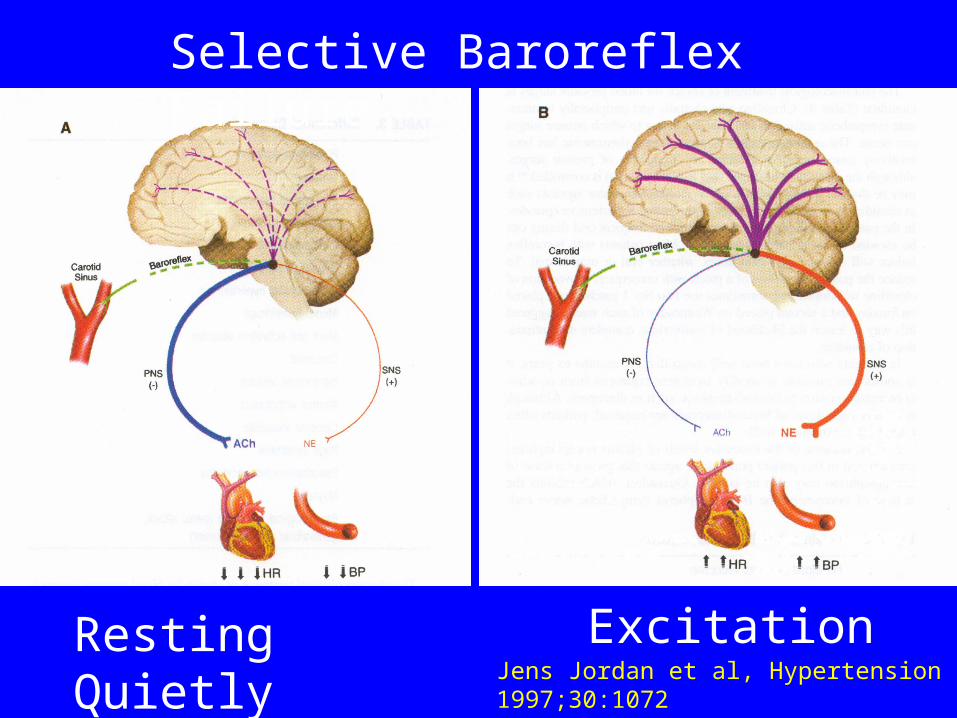
Selective Baroreflex Failure
Resting Quietly ExcitationJens Jordan et al, Hypertension 1997;30:1072
Top 7 Lessons From Dysautonomias
• You can live without norepinephrine (NE)
• Dopamine can be important in BP control
• Baroreflex failure (BF) can present as Pheo
• BF can present as malignant vagotonia
• Food and water powerfully affect BP
• Orthostatic tachycardia (POTS) is common
• Too much NE can be bad for you
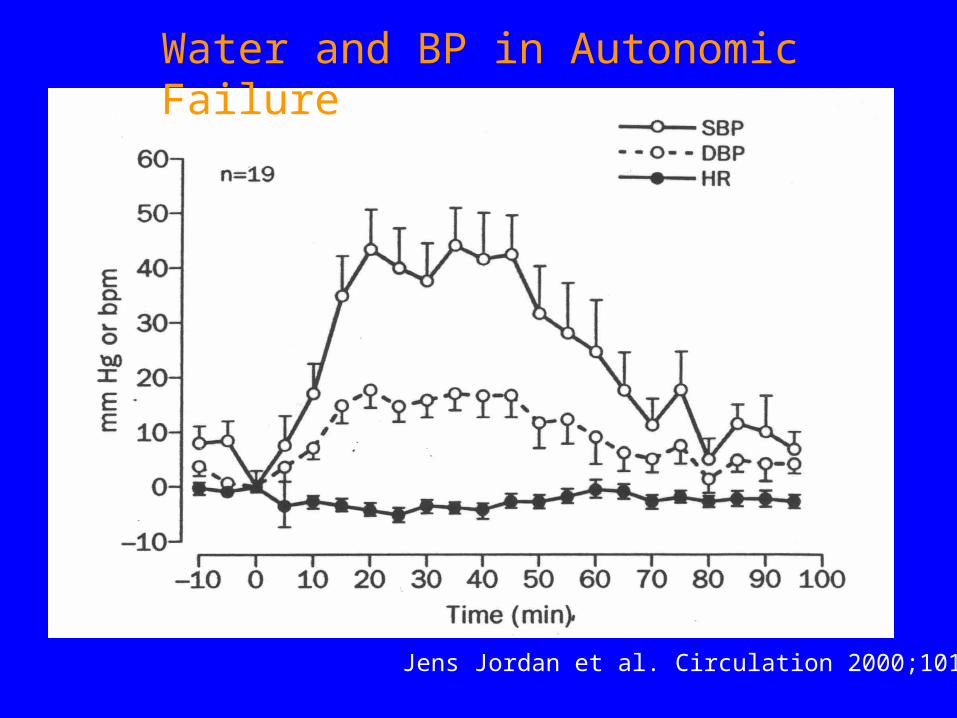
Water and BP in Autonomic Failure
Jens Jordan et al. Circulation 2000;101:504
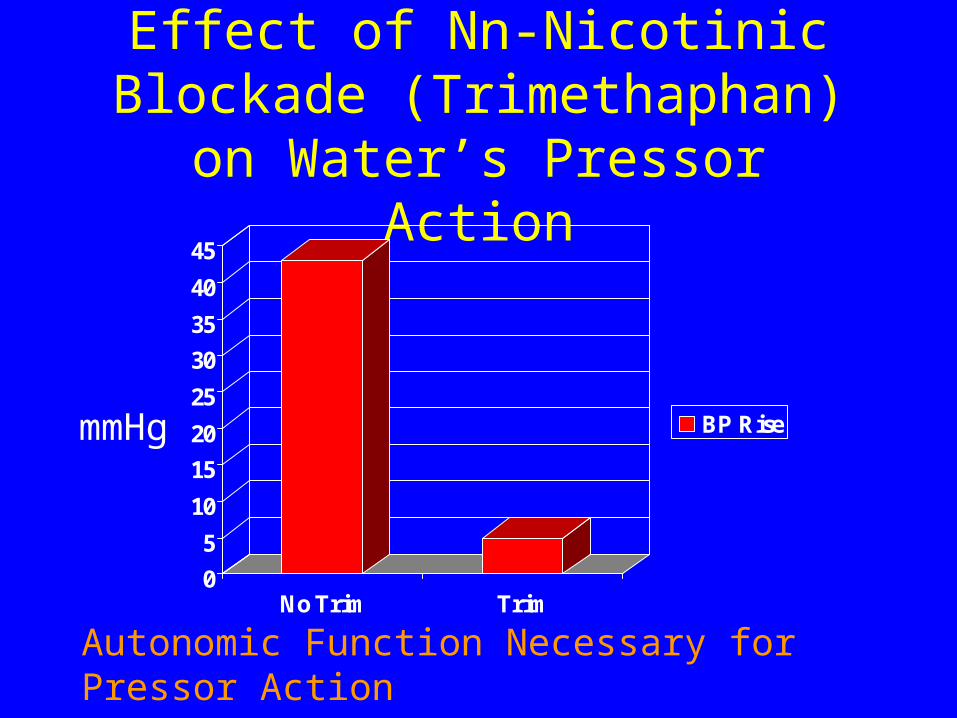
Effect of Nn-Nicotinic Blockade (Trimethaphan) on Water’s Pressor
Action
0
5
10
15
20
25
30
35
40
45
No Trim Trim
BP RisemmHg
Autonomic Function Necessary for Pressor Action
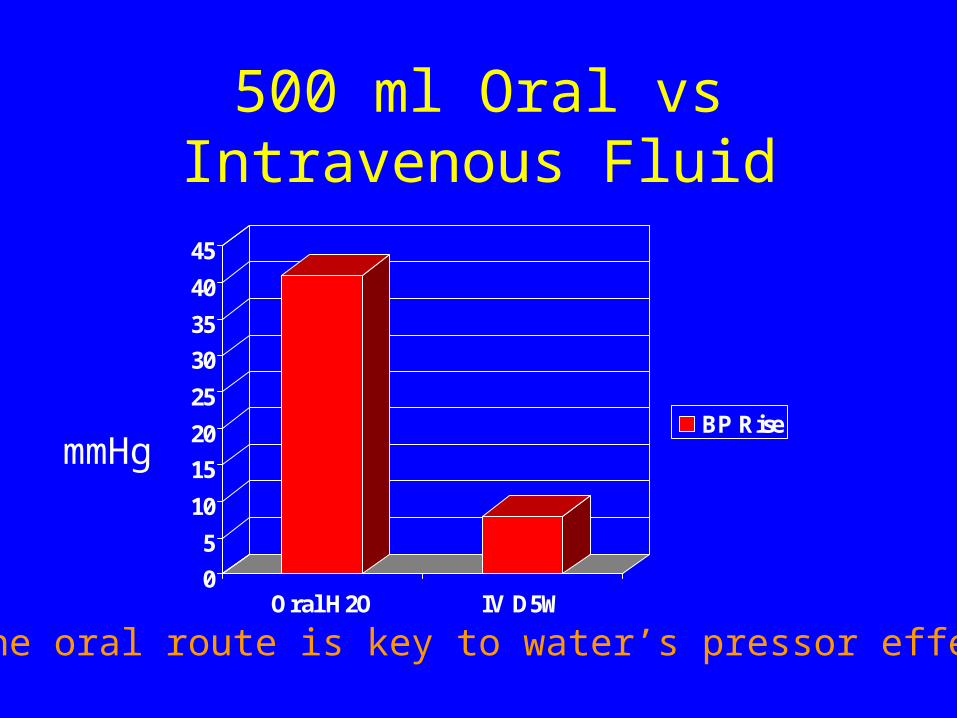
500 ml Oral vs Intravenous Fluid
0
5
10
15
20
25
30
35
40
45
Oral H2O IV D5W
BP Rise
The oral route is key to water’s pressor effect
mmHg
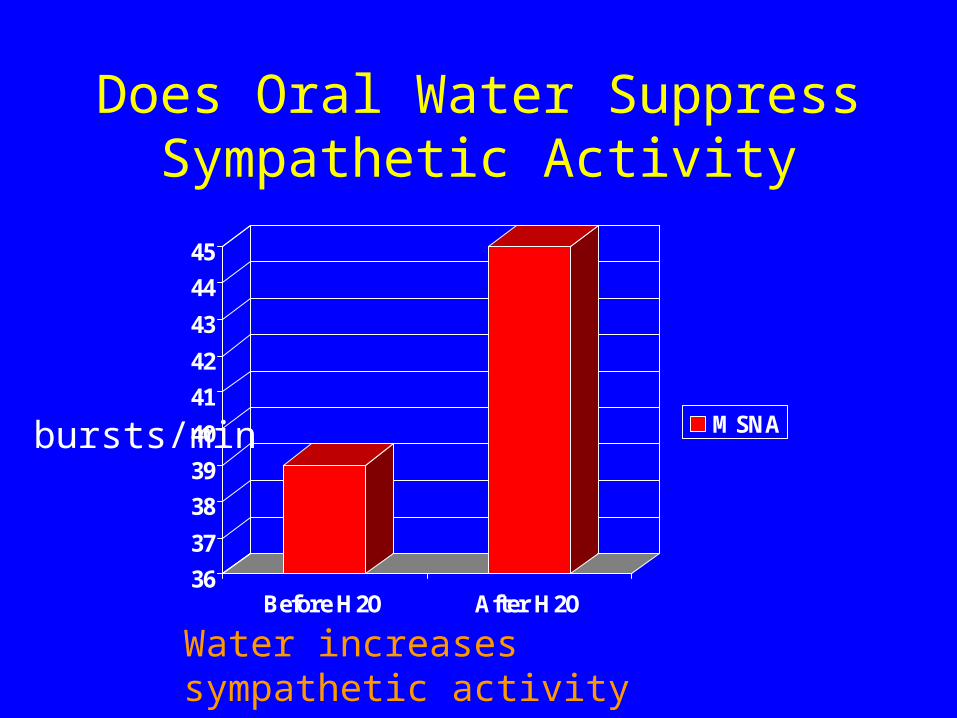
Does Oral Water Suppress Sympathetic Activity
36
37
38
39
40
41
42
43
44
45
Before H2O After H2O
MSNAbursts/min
Water increases sympathetic activity
Water and BP: Many questions
• Pressor when baroreflex fails
• Must be oral for effect
• Causes increased sympathetic activity
Water in normal subjects
• Water raises BP ~11 mmHg in older normal subjects
Is water ingestion a source of noise in clinic BP determinations?
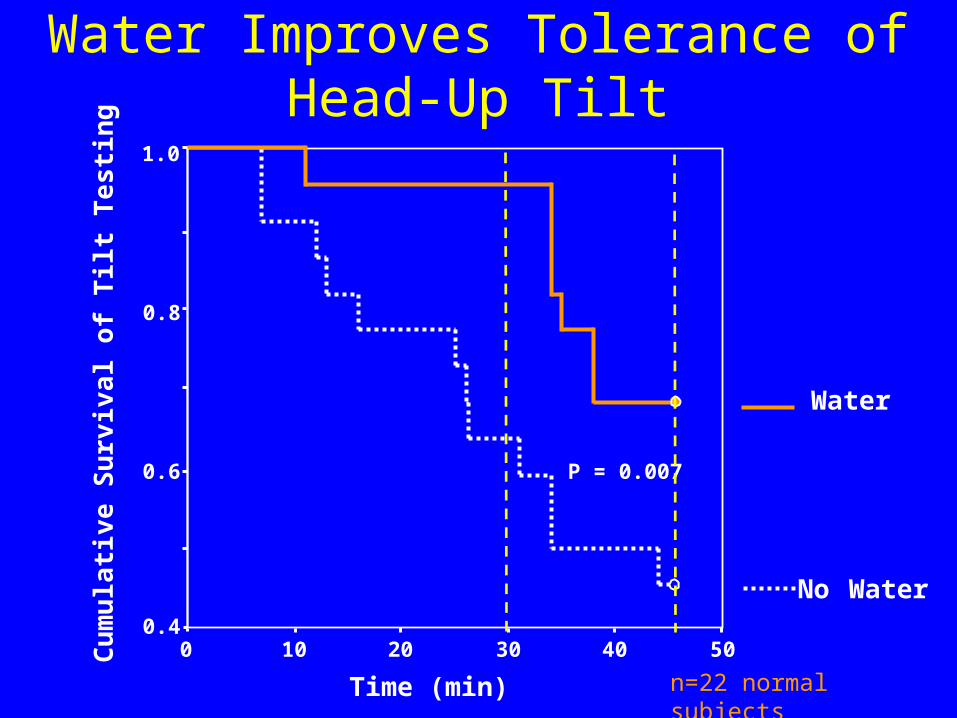
Water
No Water
Water Improves Tolerance of Head-Up Tilt
Time (min)
50403020100
Cu
mu
lati
ve S
urv
ival
of
Tilt
Te
sti
ng
1.0
0.8
0.6
0.4
P = 0.007
n=22 normal subjects
Top 7 Lessons From Dysautonomias
• You can live without norepinephrine (NE)
• Dopamine can be important in BP control
• Baroreflex failure (BF) can present as Pheo
• BF can present as malignant vagotonia
• Food and water powerfully affect BP
• Orthostatic tachycardia (POTS) is common
• Too much NE can be bad for you
Postural Tachycardia Syndrome(POTS)
• Symptoms of sympathetic activation x 6 mo
• Orthostatic tachycardia > 30 bpm
• No orthostatic hypotension (BP > 20/10)
• Plasma NE > 600 pg/ml

Postural Tachycardia Syndrome:Many Names
Orthostatic Intolerance (OI)Effort SyndromeHyperdynamic ß-Adrenergic StateIdiopathic HypovolemiaIrritable HeartMitral Valve Prolapse SyndromeNeurocirculatory AstheniaOrthostatic Tachycardia SyndromeSoldier’s HeartVasoregulatory Asthenia
Postural Tachycardia (POTS)
Not a disease !
A syndrome
Like “anemia” or “fever”
Top 7 Lessons From Dysautonomias
• You can live without norepinephrine (NE)
• Dopamine can be important in BP control
• Baroreflex failure (BF) can present as Pheo
• BF can present as malignant vagotonia
• Food and water powerfully affect BP
• Orthostatic tachycardia (POTS) is common
• Too much NE can be bad for you
Proband with POTSProband with POTS
• Palpitations
• Dizziness or lightheadedness
• Slowed thinking on standing
• Reduced exercise capacity
• Fatigue
• Near-fainting often and rarely fainting
John R. Shannon NEJM 2000;342:541

Plasma NE and Sympathetic Plasma NE and Sympathetic Activity (SA)Activity (SA)
050
100150200250300350400450
SA NE SA NE
Normal Patient
supineupright
% ofsupine value
An electrical/chemical dissociation ?
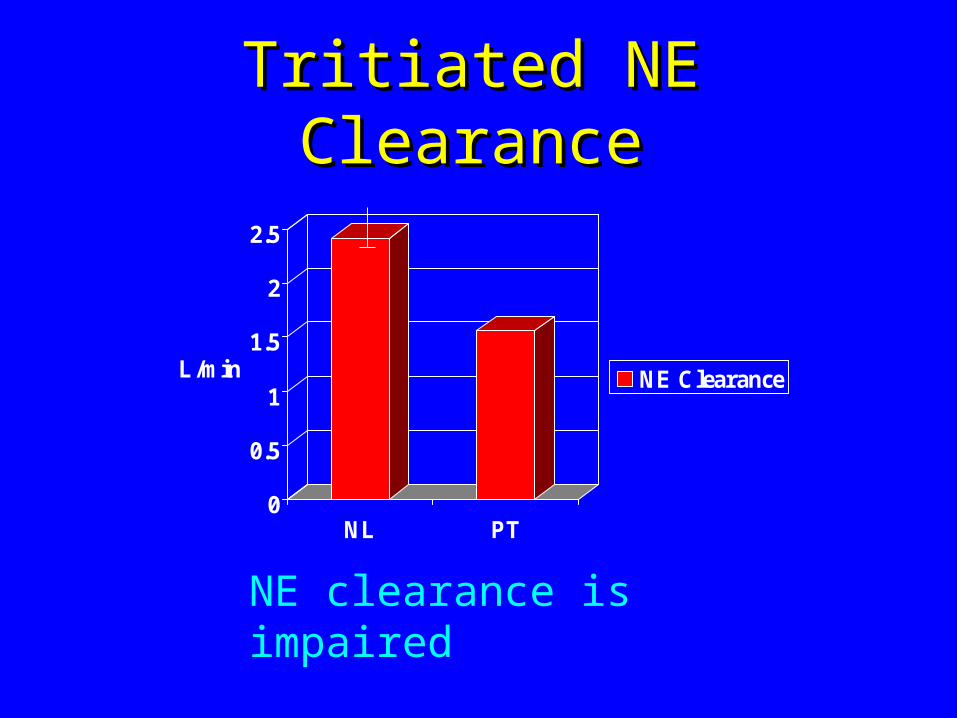
Tritiated NE ClearanceTritiated NE Clearance
0
0.5
1
1.5
2
2.5
L/min
NL PT
NE Clearance
NE clearance is impaired
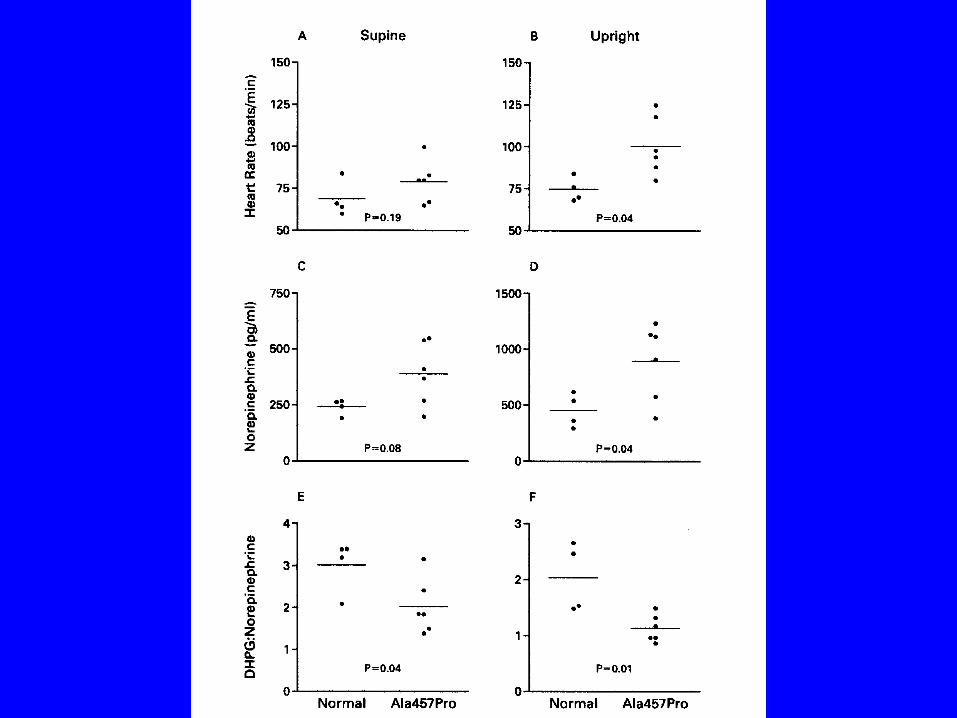
Evidence of NET DeficiencyEvidence of NET Deficiency
• NE/MSA Dissociation
• Impaired NE Clearance
• Tyramine Insensitivity
• Yohimbine Hypersensitivity
• Low DHPG/NE Ratio
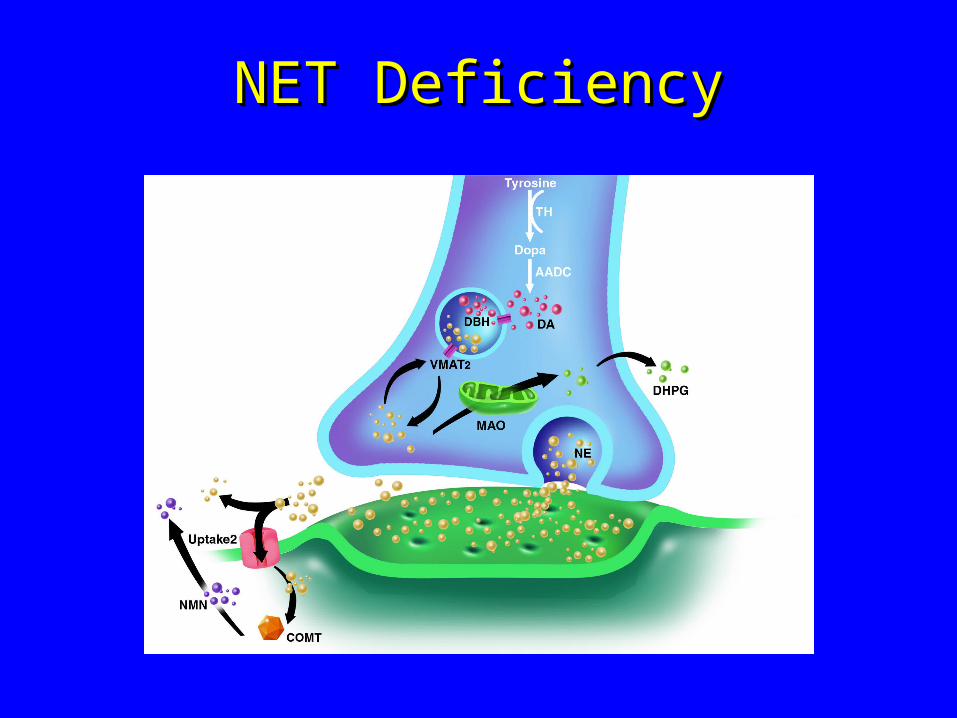
NET DeficiencyNET Deficiency

.
P
P P P
P
S-S
P
V69I
T99I
V245I
V449I
G478SA457P
N292T
V356L
A369P N375S
K463R
F528C
Y548H
Identified Coding Variants in the Human Norepinephrine Transporter
[3H
]NE
Up
take
(p
erce
nt
hN
ET
wt)
0.00
20.00
40.00
60.00
80.00
100.00
120.00
CHO LLC-PK1 HEK-293 COS-7
A457P
wt
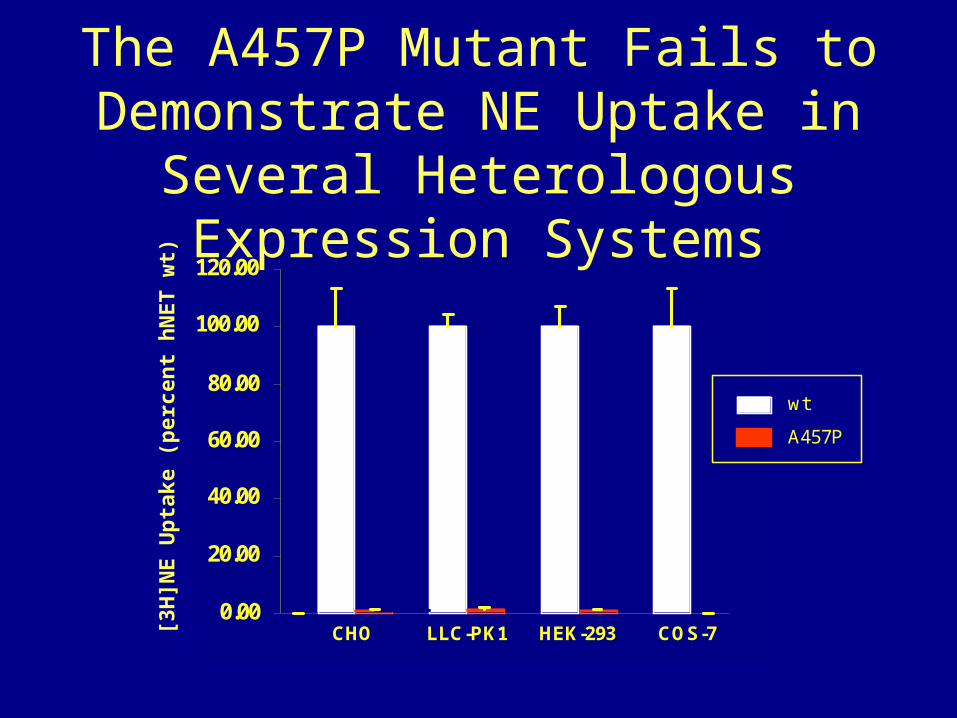
The A457P Mutant Fails to Demonstrate NE Uptake in Several Heterologous
Expression Systems

How dysfunctional is A457P ?
• A457P has virtually no NE transport function.
• Little A457P actually gets into the cell surface.
• A457P interferes with WT NET getting to surface.
Conclusions
• Autonomic disorders lead us to discovery of both phenomena and mechanisms.
• Autonomic disorders like POTS are heterogeneous and will lead to discovery of many new genetic and acquired pathophysiologies.
• These discoveries will be enabled by bedside interventions and imaging capabilities which allow us to visualize physiology in real time.

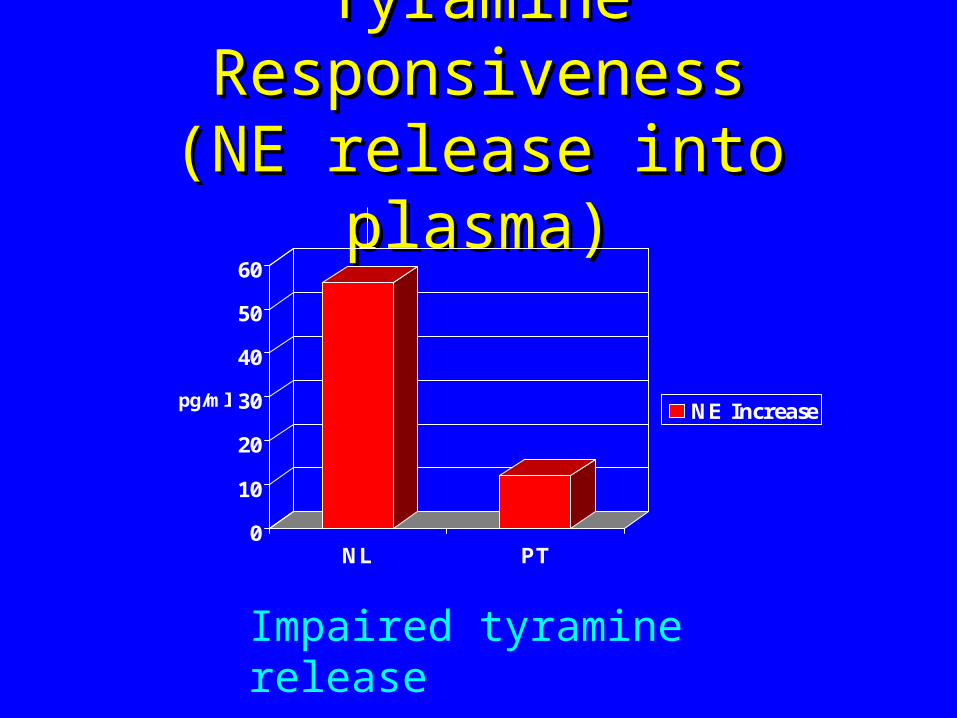
Tyramine ResponsivenessTyramine Responsiveness(NE release into plasma)(NE release into plasma)
0
10
20
30
40
50
60
pg/ml
NL PT
NE Increase
Impaired tyramine release
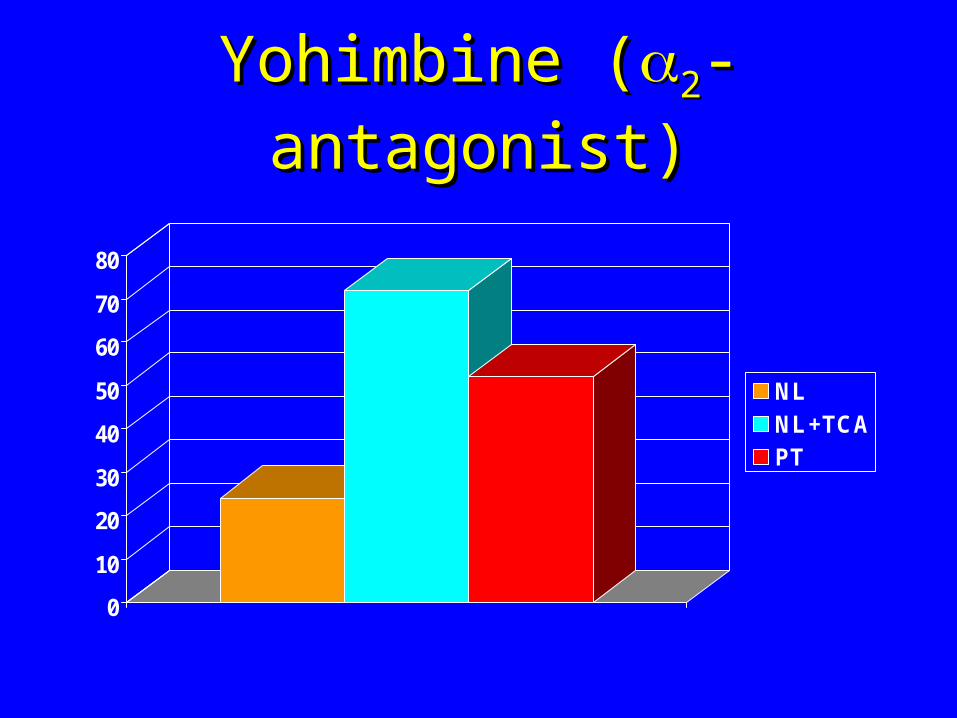
Yohimbine (Yohimbine (22-antagonist)-antagonist)
0
10
20
30
40
50
60
70
80
NLNL+TCAPT
Therapy of Severe Dysautonomias
FIRST LINE:1. Water (+40 mmHg!)2. Food (-30mmHg!)
SECOND LINE:1. Physical Maneuvers2. Exercise (in water)
THIRD LINE:1. Fludrocortisone + Salt2. Pressor Drugs (midodrine)
Audience Question
I wondered if you’d comment on the other major pressor system, “rigination” intensive system, either in the DBH defiency or during the water “logging”?

Audience Question
There’s another system that involves anti-diuretic hormone… is there some sort of paradoxical DBH response to water in these individuals?
Audience Question
I was kind of puzzled about the fact that the absence of norepinephrine has little effects on brain function and also knowing that norepinephrine plays a significant role on appetite regulation because some of the anorexgenic drugs actually cause an increase in norepinephrine or norepinephrine “???” inhibitors. Was there any subtle effects that you could see whether these people tested by cognitive function or some other way?
Audience Question
So other neurotransmitters must be compensated for the absence of norepinephrine?
Audience Question
There has been a lot of interest in the pain field very recently in the COMT enzyme and that polymorphisms might be responsible for differences in pain sensitivity. But I am not aware of works that been done looking at the consequences on classic text of autonomic function. Are any of those polymorphisms associated with differences in autonomic function as we know it?
Audience Question
It’s always striking to me that patience with the “??????????” dysfunction are not orthostatic at all as compared to the “puromotic” failure. Do you have good explanations for the clinical evidence for the no orthostatis whatsoever in these patience?