babies and due dates dispatchers ditch shovels … delivery babies and due dates don't always...
TRANSCRIPT

Home Delivery Babies and due dates don't always agreeThe National Academies of Emergency Dispatch
Snow falls fast & furiousDispatchers ditch shovels to assist the snowbound
VIVA LANAVIGATOR Dispatch rocks Vegas
Dispatch Research Public expects PAIs during an emergency
TheJournal Journal May/June 2011
Of EmErgEncy DispatchOf EmErgEncy Dispatch
emergencydispatch.org

2 THE JOURNAL | emergencydispatch.org
Fire Priority Dispatch System™ v.5The most advanced Fire Dispatching System. Unleashed.
Highlights of v.5 ProQA® & cardsets:
• Incorporates the National Academies of Emergency Dispatch’s™ newest fi re protocols • Faster dispatch points • New Pre-Arrival Instructions • New protocols • More than 40 new determinant descriptors
800-811-2248www.dispatchfaster.com
UPDATED
VERSION
Ask the right questions. Get the right answers. Send the right information.

THE JOURNAL | May/June 2011 3
g columns4 | Contributors5 | Dear Reader6 | President’s Message7 | Ask Doc8 | Leadership Insights 9 | Centered Study10 | Attitude Adjustment50 | Retro Space
g industry insider11 | Latest news updates
g departmentsBestPractices
15 | FAQ Does breathing and unconscious patient with respirator need CPR?
OnTrack
30 | Police CDE Maintaining safety is priority
33 | Universal CDE Callers expect PAIs when protocol long established
YourSpace
42 | Stork Stories
features16 | Viva La Navigator
Navigator 2011 held at the Paris Hotel in Las Vegas featured a record number of classes, special events, exhibits, and people eager to learn lots and win big.
26 | Swept By SnowHale and hearty dispatchers traded snow shovels for phones and radios to assist people stranded in their homes and on the roads due to nearly record-breaking snowfall affecting most of the country.
The following U.S. patents may apply to portions of the MPDS or software depicted in this periodical: 5,857,966; 5,989,187; 6,004,266; 6,010,451; 6,053,864; 6,076,065; 6,078,894; 6,106,459; 6,607,481; 7,106,835; 7,428,301; 7,645,234. The PPDS is protected by U.S. patent 7,436,937. FPDS patents are pending. Other U.S. and foreign patents pending. Protocol-related terminology in this text is additionally copyrighted within each of the NAED’s discipline-specific protocols. Original MPDS, FPDS, and PPDS copyrights established in September 1979, August 2000, and August 2001, respectively. Subsequent editions and supporting material copyrighted as issued. Portions of this periodical come from material previously copyrighted beginning in 1979 through the present.
INSIDE theJournalM A y · J U N E 2 011 | V o L . 1 3 N o . 3
Fire Priority Dispatch System™ v.5The most advanced Fire Dispatching System. Unleashed.
Highlights of v.5 ProQA® & cardsets:
• Incorporates the National Academies of Emergency Dispatch’s™ newest fi re protocols • Faster dispatch points • New Pre-Arrival Instructions • New protocols • More than 40 new determinant descriptors
800-811-2248www.dispatchfaster.com
UPDATED
VERSION
Ask the right questions. Get the right answers. Send the right information.
4 THE JOURNAL | emergencydispatch.org
CON
TrIBuTO
rS
Leann HoLLinsHead
Leann Hollinshead is the director of the Pennington Area Emergency Services Communications Center in Rapid City, S.D., which is a NAED Accredited Center of Excellence (ACE) answering about 250,000 calls each year. Before becoming the communications director, she served 20 years in crisis communications for the U.S. Air Force in various emergency operations centers around the country.
Your Space | paGe 36
JaCi FoX
Jaci Fox is the co-chair of the Police Council of Standards for the IAED. She is also an EPD and EPD-Q instructor. Jaci is a certified quality assurance specialist on the Quality Assurance Team at the Medicine Hat Regional 911 Communications Centre in Medicine Hat, Alberta, Canada. Medicine Hat Regional 911 is one of three tri-Accredited Centers of Excellence. Jaci also spent 14 years as a calltaker and dispatcher.
attitude adjuStment | paGe 10
Lora reed, PH.d.
Lora Reed holds a bachelor’s degree in American Studies from Eckerd College, a master’s in Applied Sociology from Norwich University, and a Ph.D. in Organization and Management and Certificate in Training and Development from Capella University. Her dissertation examined the Big Five personality traits and servant leadership characteristics as factors in retention of 9-1-1 telecommunicators. She is a professor at Eckerd College in St. Petersburg, Fla.
centered StudY | paGe 9
JoHn BroPHy
John R. Brophy is director of the communications center at Community EMS in Southfield, Mich. He previously served as manager of the Jersey City Medical Center EMS Communications Center, New Jersey’s first and only Accredited Center of Excellence. Additionally, John has 28 years in the fire service, having held the rank of captain, and 10 years of service as a U.S. Navy corpsman.
LeaderSHip inSiGHtS | paGe 8
Brett a. Patterson
Brett A. Patterson is an Academics & Standards associate and Research Council chair for the NAED. His role involves training, curriculum, protocol standards, quality improvement, and research. He is a member of the NAED College of Fellows, Standards Council, and Rules Committee. Brett began a career in EMS communications in 1987. Prior to accepting a position with the NAED, he spent 10 years working in Pinellas County, Fla.
faq | paGe 15

THE JOURNAL | May/June 2011 5
ConnectionsNavigator’s all about the people
Audrey Fraizer, Managing Editor
g dearreader
Networking” implies—at least to me—schmoozing to further business or social
connections. It’s not a “bad” word suggesting phony intentions but it’s also not a word I would use to define a friendship, although a business acquaintance can turn into someone you communicate with through more than an occa-sional e-mail or telephone call. And I mean that in the friendly sense.
So when I go to Navigator, “networking” is not how I would describe The Journal's work. The event is a chance to meet people, and listening to their stories
With that said, I did make a point of talking to Margaret Moran, a long-time employee of EnRoute, a CAD/CAM software company that sponsors both the Dispatcher of the year and Dr. Jeff Clawson Leadership awards. As part of the latter award, EnRoute provides a $500 honorarium to the recipient who then chooses the charitable organization to receive the money. This year, the $500 went to the Red Cross in Japan to help relief efforts following the earthquake and tsunami.
I suppose Margaret could be considered a business contact, except that we didn’t talk business. EnRoute has been a Navigator mainstay for longer than I’ve been attending and it was about time for me to make introductions.
I’m glad it happened.Margaret is a former EMT,
switching to dispatch in Pompano, Fla., where she worked for six years, from 1983 to 1989. That was back in the pre-CAD days of dispatch. Margaret and the other dispatch-ers would write the address of the
caller’s emergency on an index card and position the card into a geographically-slotted conveyer belt. The card was time stamped once the ambulance went out.
The first computers in Pom-pano were serially connected stand alones (no networking capability). Eventually, operating systems that could support multiple simultane-ous users replaced the stand alones. A UNIX operating system ran the ProQA graphical user interface.
ProQA grabbed Margaret’s attention. She saw consistency and became an advocate for a process that gave dispatchers “a solid rock to stand by.” She eventually trans-ferred over to IT in Pompano and ran the CAD system.
Margaret joined EnRoute 19 years ago. She directs sales and, as part of her job, she is a fixture at the EnRoute booth for tradeshows and conferences, including the annual Navigator conference.
yes, her job requires business “networking.” But she also favors relationships that go beyond elbow rubbing.
“Dispatch is about establishing relationships,” she said. “And for people in an emergency, it might be the most important relationship they ever have.” g
Setting the record Straight
In the March/April 2011 article “EMD-Q Scoring Standards Up For New Release,” on page 9, we misstated the Protocol numbers. The article should have referred to Protocols 6 and 10. We thank our readers for their dili-gence in bringing this to our attention. A corrected version is available from our web site at www.emergencydis-patch.org/Journal.
naeD Journal STaffCOMMUNiCATiONS | CrEATivE DirECTOrKris Christensen Berg
MANAgiNg EDiTOrAudrey Fraizer
TEChNiCAl EDiTOrBrett A. Patterson
ASSiSTANT EDiTOrSheather Darata Cynthia Murray
ArT DirECTOrlee Workman
SENiOr DESigNErChris Carr
PrODUCTiON MANAgErJess Cook
WEB | MUlTiMEDiA MANAgErErwin Bernales
WEB DESigNErJason Faga
acaDemy STaffPrESiDENTScott Freitag
ASSOCiATE DirECTOr | USACarlynn Page
ASSOCiATE DirECTOr | U.K.Beverley logan
ASSOCiATE DirECTOr | AUSTrAlASiAPeter hamilton
ACADEMiCS & STANDArDS ASSOCiATEBrett A. Patterson
ADMiNiSTrATOr OF iNSTrUCTOr SErviCESCindy grigg
COMMUNiCATiONS DirECTOrKris Christensen Berg
DirECTOr OF CUrriCUlUM DESigNlarry E. latimer, M. Ed.
DirECTOr OF EUrOPEAN OPErATiONSTudy Benson
iNTErNATiONAl liAiSONAmelia Clawson
MEMBErShiP SErviCES MANAgErArabella vanBeuge
The National Journal of Emergency Dispatch is the official bimonthly publication of the National Academies of Emer-gency Dispatch (NAED), a non-profit, standard-setting organization promoting safe and effective emergency dispatch services worldwide. Comprised of three allied academies for medical, fire, and police dispatching, the NAED supports first-responder-related research, unified protocol application, legislation for emergency call-center regulation, and strengthen-ing the emergency dispatch community through education, certification, and accreditation.
general NAED membership, which includes a Journal subscription, is available for $19 annually, $35 for two years, or $49 for three years. Non-member subscriptions are available for $25 annually. By meeting certain requirements, certi-fied membership is provided for qualified individual applicants. Accredited Center of Excellence status is also available to dispatch agencies that comply with Academy standards. © 2011 NAED. All rights reserved.
TheJournalOf EmErgEncy Dispatch
naTional acaDemieS of emergency DiSpaTch139 East South Temple, Suite 200 Salt lake City, UT 84111 USA USA/Canada toll-free (800) 960-6236 int’l/local: (801) 359-6916 Fax: (801) 359-0996 www.emergencydispatch.org [email protected]
inTernaTional acaDemieS of emergency DiSpaTchAUSTrAlASiAN OFFiCE011-61-3-9806-1772
CANADiAN OFFiCE1-514-910-1301
EUrOPEAN OFFiCE011-43-5337-66248
iTAliAN OFFiCE011-39-011-513-2588
MAlAySiAN OFFiCE011-603-2168-4798
U.K. OFFiCE011-44-0-117-934-9732
BoarDS & councilSACCrEDiTATiON BOArD ChAirBrian Dale
AlliANCE BOArD ChAirKeith griffiths
CErTiFiCATiON BOArD ChAirPamela Stewart
CUrriCUlUM COUNCil ChAirSvictoria Maguire (Medical/EMD Board) Mike Thompson (Fire/EFD Board) Jaci Fox (Police/EPD Board) Susi Marsan (ETC)
rESEArCh COUNCil ChAirBrett A. Patterson
STANDArDS COUNCil ChAirSMarie leroux (Medical/EMD) gary galasso (Fire/EFD) Tamra Wiggins (Police/EPD)
college of fellowSChAirMarc gay (Emeritus)
AUSTrAlASiA | SOUTh AMEriCAFrank Archer, MD (Australia) Andrew K. Bacon, MD (Australia) Peter lockie (New Zealand) Peter Pilon (Australia)
CANADADrew Burgwin (Br. Columbia) Claude Desrosiers (Québec) Douglas Eyolfson, MD (Manitoba) Martin Friedberg, MD (Ontario) Marie leroux, rN (Québec) (Emeritus) Mark gay, (Québec) (Emeritus) Paul Morck (Alberta) Wayne Smith, MD (Québec)
EUrOPEAndre Baumann (germany) gianluca ghiselli, MD (italy) Jean-marc labourey, MD (France) Jan de Nooij, MD (Netherlands) gwyn Pritchard (Cyprus) (Emeritus) Bernhard Segall, MD (Austria) gernot vergeiner (Austria) Christine Wägli (Switzerland)
UNiTED KiNgDOM | irElANDTrevor Baldwin (England) Michael Delaney (ireland) Conrad Fivaz, MD (England) louise ganley (England) James gummett (England) Chris hartley-Sharpe (England) Andy heward (England) Stuart ide (England) Peter Keating (ireland) ray lunt (England) Andy Newton (England) (Emeritus) John D. Scott, MD (England) Janette K. Turner (England)
UNiTED STATESBill Auchterlonie (KS) robert Bass, MD (MD) Christopher W. Bradford (Fl) Thera Bradshaw (CA) (Emeritus) geoff Cady (CA)
Steven M. Carlo (Ny) Jeff Clawson, MD (UT) Phil Coco (CT) Brian Dale (UT) Chip Darius, MA (CT) Kate Dernocoeur (Mi) Norm Dinerman, MD (ME) Patricia J. Dukes, MiCT (hi) James v. Dunford, MD (CA) Marc Eckstein, MD (CA) John Flores (CA) Scott Freitag (UT) gary galasso (CA) Keith griffiths (CA) Jeffrey r. grunow, MSN (UT) Darren Judd (UT) Alexander Kuehl, MD, MPh (Ny) (Emeritus) James lake (SC) James lanier (Fl) Bill leonard (AZ) Stephen l’heureux (Nh) victoria A. Maguire (Mi) Sheila Malone (iN) Susi Marsan (gA) robert l. Martin (DC) Dave Massengale (CA) Jim Meeks, PA-C (UT) Shawna Mistretta (CO) gene Moffitt (UT) Jerry l. Overton (CA) Eric Parry, ENP (TX) rick W. Patrick (PA) Brett A. Patterson (Fl) Paul E. Pepe, MD, MPh (TX) ross rutschman (Or) (Emeritus) Joe ryan, MD (Nv) Doug Smith-lee (WA) Tom Somers (CA) Paul Stiegler, MD (Wi) Michael Thompson (SD) Carl C. van Cott (NC) Sheila Q. Wheeler, MSN (CA) Craig Whittington (NC) Arthur h. yancey, ii, MD, MPh (gA) Tina young (CO)
“

6 THE JOURNAL | emergencydispatch.org
Last Man DownDispatchers spellbound by stories from 9/11
Scott Freitag, NAED President
g President’sMessage
The elevator ride to my room at the Paris in Las Vegas took me well above the slowly moving walls of people already
crowding the cobblestone streets in a simu-lated Parisian neighborhood. I had been up early that day—probably before 6 a.m.—eager to attend Navigator’s opening Session.
I wasn’t alone in my anticipation. The prospect of meeting Keynote Speaker Rich-ard Picciotto and hearing his experiences from 9/11 filled every chair in the spacious conference hall. Several hours later, his talk ended, the piercing mixture of voices and slot machines during those few steps to the hotel lobby and up to my room to drop off an autographed copy of Picciotto’s book Last Man Down stood in stark contrast to the hundreds of dispatchers captivated by his 60-minute presentation.
I don’t remember the last time a sip from a cup of coffee by the person behind me could be heard above the accustomed noise from a room full of dispatchers. This was the cautious tranquility of a symphony. No one wanted to interrupt the reverence we held for a member of our EMS family describing a day most of us watched horrified from many, many miles away.
Picciotto is a retired New york Fire Department (FDNy) chief and the highest-ranking firefighter to survive the Sept. 11, 2001, terrorist attacks on the World Trade Center. He and members of his depart-ment’s Battalion 11 were descending a stair-well between the sixth and seventh floors of the North Tower when—at 10:28 a.m. Eastern time—the tower collapsed. Picciotto remembers seeing his life flash before him during the eight seconds of floor slamming upon floor to the ground below.
“What can you do?” asked Picciotto, a 28-year veteran of the FDNy. “I thought about my family and said a compilation of every prayer I knew. I did not want to suffer. I said ‘Please God make this quick.’”
The st a ircase dis integrated, t hey tumbled through pitch-black, landing in
isolated piles of debris and dust; Picciotto and his firefighters spent the next four hours sending Mayday signals, finally making it out of the hole when they climbed toward a shred of light tunneling through the debris from four stories above.
Thirteen people, including Picciotto, had survived. They climbed out to utter devastation.
“We didn’t see a single rescue person,” Picciotto said. “They were blocks away climb-ing through debris. We eventually mean-dered our way out west of the south tower.”
The smell, the ruin, and the horror Pic-ciotto experienced will stay with him. No one above the 91st floor in the North Tower is believed to have survived the attack; no one will ever know how many people jumped through shattered windows to escape toxic gas. The first firefighter died when a jumper landed on top of him.
Images of the good people did that day are the bright pieces he carries. Strangers flee-ing down stairs carrying injured strangers on
their backs. Forty people in a room on the 12th floor orchestrating the evacuation of 40 others who couldn’t walk independently down the stairs. office workers going down-stairs offering final words of encouragement to firefighters running up the stairs.
Dispatchers, he said, did a tremendous job answering hundreds of calls, and many from people making their last call ever. Audiotapes of calls they received include the voices of firefighters and emergency medical technicians who were among the 343 fire department personnel killed in the attack. Nine hours of partial recordings released by New york City in 2006 show desperate attempts to calm callers’ fears and, in many instances, dispatchers assuring callers on the upper floors that help was on its way.
New york Fire Commissioner com-mended dispatchers as the “unsung heroes on the darkest days in our city’s history,” according to an Associated Press story pub-lished on the day the tapes were released to the public. Some dispatchers never came back to work after that day. Some retired early. In 2004, the Sept. 11 commission concluded that the operators did not have enough information to allow more people to escape.
What did Chief Picciotto take away from the experience?
He underscores the importance of family and friends, and acknowledges the support of people as the lifeline in crisis and tragedy. He regrets the loss of closeness nationally that 9/11 brought to the country. He real-izes all prayers are not answered and, for him on that day, it was for the better.
Written transcripts of telephone con-versations between 9-1-1 dispatchers of the New york City Fire Department and people calling 9-1-1 are available in PDF format online. As required by the decision of the New york Court of Appeals, the conversa-tions and identifying information have been redacted to protect the privacy of those who called 9-1-1. g

THE JOURNAL | May/June 2011 7
Aspirin AdministrationDoes coating decrease the benefit?
Jeff Clawson, M.D.
g asKdOC
dr. Clawson:Is there any risk, or decreased benefit, of
chewing a coated aspirin (i.e., Ecotrin), in the presence of chest pain as recommended by the American Heart Association (AHA), as compared to a non-coated aspirin?
Bardona J. Woods, ENPDirector of CommunicationsWashington Co. Emergency CommunicationsHagerstown, Md.
Bardona:Thanks for your question on this subject.
Enteric-coated aspirin administered at dis-patch needs to be chewed. This question was anticipated before the Aspirin Dx Tool release in August 2007 and this is the official answer
that appears in Principles of Emergency Medical Dispatch, 4th edition, starting on page 6.16. The following text is the answer to your spe-cific question, which is found on page 6.21.
We asked two pharmacists in person and e-mailed a question to Rite Aid’s “Ask a Phar-macist” program. Both local pharmacists said there were no problems chewing a coated aspirin and the effect should be the same. Here is the Rite Aid response:
“Thank you for using Rite Aid Clinical Services. In reviewing our drug information resources, we have found chewing aspirin hastens its anti-platelet effects. Chewing an aspirin is a very important emergency mea-sure for the prevention of a suspected heart attack or stroke to prevent damage due to
blood clotting. Although uncoated aspirin is preferred in this emergency situation, we found no information to suggest that chew-ing a coated aspirin was any less beneficial.”
Finally, we even went so far as to test chewing a 325 mg Ecotrin (looks like a big M&M), and it didn’t break any teeth in our test monkey here.
If someone has problems chewing, crush it between two spoons, and then down it. We also checked a few studies on the absorp-tion rates of chewed coated aspirins, which I can find if necessary. They were supportive of chewing them. Also, if 8 mg tablets are used, they need to chew four of them.
Hope this answers your question.onward through the salicylate fog… Doc g

8 THE JOURNAL | emergencydispatch.org
Make The ConnectionMentoring benefits the individual and the organization
John R. Brophy
g LeadersHiPinsigHts
Developing and sustaining successful organizations requires mentoring. As leaders we must develop our talent
pool to fill and succeed at their present roles and grow into the jobs they might assume in the future. Much like parents, we are their guardians; the people we train, lead, and men-tor will both shape and carry out our legacy.
Mentoring the succession process, how-ever, goes beyond training someone how to perform current duties. The leader must serve as more than just a boss by creating an environment that encourages advancement and empowers people. Developing such an environment takes recognizing the strengths and weaknesses of staff members and build-ing on their strengths using positive rein-forcement and positive criticism.
But beware.Praising an individual’s performance is
easy; people appreciate the attention. Posi-tive reinforcement is critical to job satisfac-tion and continued motivation.
Critical analysis, however, is tough and if mishandled, damaging to the aspiring pro-tégé. The leader must plan carefully before providing constructive criticism, making sure the key points come across and allow-ing room for discussion. The leader should emphasize the value the individual brings to the company and highlight positive strides. The individual should find the experience meaningful and leave understanding the problem with a clear path for resolving it. Follow up should always be part of the pro-cess, also. Even if it’s a quick pat on the back for a job well done, the leader must acknowl-edge the individual when goals are met and progress has been made.
situational leadership“Situational leadership,” as championed
by Paul Hersey and Ken Blanchard, is task-oriented leadership adapted to influence the targeted individual or group. The men-tor/leader must take into account education and experience and the willingness to take
on responsibility. High and realistic expec-tations generally lead to high performance (and vice versa). By explaining the “why,” “how,” and “when” of task performance, the situational leader invests in the future of the people and organization. When adeptly
employed, supervisory mentoring builds self-confidence and the commitment of the individual involved.
Situational mentoring requires more of a coaching approach and it’s an ongoing process that continues well past the first formal meeting. Similar to sports, the coach guides the talented player in selecting the right “play” for the relevant conditions. The leader asks questions, listens to the protégé’s perspective, and truly hears the concerns. Collaboration between the leader and pro-tégé leads to a reasonable path of success. Situational mentoring opportunities are “teachable moments” in which the protégé can learn and grow under the guidance of a leader acting as mentor and coach.
Formal mentoring programs Formal mentoring programs often have a
defined period of time, six months to a year for example, and regularly scheduled follow up. In some cases, protégés select a mentor, in others they are assigned to one. The decision varies with the company and the overall goal.
In general, an orientation session is a good starting point in the program: the leader should explain the mentoring process and how it can benefit the protégé, mentor, and the organization. The leader should discuss the goals mentoring is meant to accomplish. After orientation, participants can be given time to reflect and identify strengths and weaknesses and consider a good mentor fit.
The protégé should consider an individual he or she respects and believes would help solidify strengths while addressing weak-nesses. often times a protégé simply selects his or her immediate supervisor, a close friend, or family member. While choosing mentoring through an established relation-ship has merit, the protégé should consider someone who could give a new perspective; perhaps someone less familiar but equally capable of providing the necessary guidance.
once the selection is made, the mentor and protégé should establish parameters. They should discuss details such as when, where, and how often they will meet and what each would like to accomplish through the mentoring experience. From there, they can review the strengths and weaknesses identified by the protégé and determine the best way to proceed.
everyone benefitsFinally, the protégé is not the only person
benefiting from the mentoring relationship. The mentor also has the opportunity to gain new perspectives and approaches to interper-sonal communications and to develop and practice a more personal situational style of management. Both the protégé and mentor are enhancing the effectiveness of their organization.
organizations that embrace mentor-ing and staff development understand the atmosphere of trust that supports both per-sonal and professional growth that, in turn, increases job satisfaction. The value placed in mentoring translates into improved perfor-mance, minimized burnout, and an overall positive environment. g

THE JOURNAL | May/June 2011 9
Culture ShockStudy is an organizational eye-opener
Lora L. Reed, Ph.D.
g CenteredstUdY
Editor’s Note: In the summer of 2010 a national study was conducted to explore perceptions of leadership, followership, and organizational culture in Public Safety Answering Points (PSAPs). Lora L. Reed, Ph.D., conducted the research, made possible through support of the Greenleaf Center for Servant Leadership, with cooperation from the National Academies of Emergency Dispatch® (NAED™), 911Lifeline, and other public safety organizations.
An online questionnaire delivered through e-mail blasts saturated more than 46,000 potential participants,
creating a snowball sample of almost 900 PSAP employees at all levels of responsibil-ity. After cleaning up the data, eliminat-ing all questionnaires with more than 5% missing responses or unreadable items, 673 responses remained from 45 states, Canada, and Australia. The data from this study should culminate in at least one peer-reviewed publication, but it can also ben-efit PSAP decision makers in practical every day applications. This article is the first in a series targeted to the day-to-day perspective of managing a PSAP.
In January and March 2011, six webi-nars with consistent content focusing on data from the study were delivered in col-laboration with 911Lifeline. The Web-based introductions explained the rationale for the study, preliminary results as related to contemporary management and leadership literature, and the meaning of the study's findings specific to PSAPs. The webinars were an expression of gratitude for the par-ticipants and to further signify my interest in continuing an ongoing conversation and conducting qualitative research specific to PSAP organizations.
This column recaps the preliminary findings from the webinars. We continue to mine the data and will share pertinent infor-mation in future columns in The Journal. We hope to assist PSAP decision makers in organizational and employee development at
a time when budgets are tight and demands are high; we look forward to continuing this conversation.
study rationaleAlthough emergency dispatcher and
related occupations are only about 40 years old, they are of increasing importance to society. Rapid technological advances, pop-ulation growth, and shifting demographics are among drivers of growth in the industry, but employee retention has remained prob-lematic since inception of these occupations.
According to a recent study (APCo 2009), the average turnover rate for dis-patchers is about 17%, higher than teachers or nurses (about 15%). In the past decade environmental stressors and high-tech employment opportunities luring employees to other jobs have further exacerbated reten-tion. According to APCo (2009), the recent economic downturn may have increased the number of candidates who apply for posi-tions, but it has not necessarily brought more of the right dispatchers into the occupation.
dispatcher competenciesAt their best, dispatchers possess a
unique set of competencies:
• Aptitudefortechnologyisessentialtoperformance of tasks and is expected to increase due to rapid technological advances such as texting and multime-dia applications
• Emotional intelligencepertains tounderstanding self and others, includ-ing peers, other first responders, and emergent callers
• Leadershipisimportantatallorganiza-tional levels. Dispatchers and calltak-ers briefly lead all persons with whom they come into contact either by tele-phone or other electronic devices. Shift supervisors lead teams; directors lead agencies.
• OrganizationalCitizenshipBehaviors(oCBs) occur on both individual and group levels. They can be related to indi-vidual and organizational well-being, employee commitment, and social influ-ence on others.
In future columns we will explore how many of these competencies relate to our study, and we will examine passive and proactive followership in PSAP organiza-tional culture.
Why study PsaP leadership?PSAP leadership is important at all
organizational levels and employees per-ceive it as essential to successful task com-pletion. But the study results show many dispatchers do not perceive themselves as recognized leaders and perceptions are important to job satisfaction, retention, and organizational performance.
Further, the study examined self-report employee perceptions of executive servant leadership in PSAPs, along with percep-tions of dispatchers as passive or proactive followers. Four employee groups—dispatch-ers, shift supervisors, directors, and support staff/IT—had very different perceptions of agency leadership (agencies ranged from less than 5 to more than 100 employees). More closely aligning the groups’ perceptions of leadership may result in improved effective-ness and employee retention. The same four groups ranked themselves and each other low on passive followership (response to authoritarian leadership in a bureaucratic environment) and high on proactive followership. The ranking indicates the propensity toward shared leadership in an empowered environment.
In future columns these and other findings will be explored as pertinent to single and multi-agency function and organizational culture. g
for more information visit www.drloraconsulting.com or 911Lifeline.org. you can also contact Dr. Lora reed at [email protected]

10 THE JOURNAL | emergencydispatch.org
Whom do you serve? our jobs revolve around others
Jaci Fox
g attitUdeadjUstMent
I come from a mid-sized center in Alberta, Canada, and believe that I have been taught who we truly serve. I am not sure
I knew that when I started the job. I have also had the good fortune of traveling to many call centers all over North America and the U.K. and have observed the same values in success-ful call centers: Successful centers value what they practice—and practice what they value—and they truly know who they serve.
I bet when each of us contemplated this line of work, we believed that we were sign-ing up for genuine reasons. We thought we would be changing the world and changing lives—in our communities and on a global level. We saw ourselves accomplishing major feats while managing hysterical people. This was the dream job. Unfortunately, the job posting failed to list several qualities nec-essary for success. Trust, patience, under-standing, empathy, knowledge, confidence, determination, and humility should have been there in BoLD letters.
Trusting the processes is the key to suc-cess. We trust that someone has done the learning for us. We trust the past experiences of others for obtaining vital information such as addresses. We trust that our training along with our technical tools will lead to success.
When obtaining information from stressed callers, we must trust the process and exercise patience. Patience is essential at all times. People do call 9-1-1 to report a barking dog, and they do request ambulances for hangovers, sprained toes, and non-allergic reactions to bee stings. A non-emergency to us might still be an emergency to the caller, and we must treat it as such.
Did anyone tell us that the job would require typing faster than people talk or to understand sometimes incoherent speak-ing? I didn’t sign up for that. I signed up to save lives, change lives, and fight crime and evil. No one told me about the patience and understanding required.
Somewhere in the midst of training, came knowledge. Somehow, after about 100
shifts dealing with many of the same types of calls, it seemed the answers just came to me. If I trusted the process, it would lead me to the answers. occasionally, I heard a coworker answering “that call.” What happens if I pick up the line on “that call,” and don’t have the
answers? The fear (or feeling of terror) tells us more training may be in order.
During training and practicing what we were taught, confidence developed. The caller trusts us to have the answers and does
not like to hear any apprehension in our voices. once a calltaker/dispatcher has con-fidence, the job goes so much easier.
At this point, we might see something else happen. We’ve been at the job a long time and instead of developing the good qualities, other traits bubble to the surface. We might lose the empathy, patience, and understanding critical to caring for the caller. Confidence and knowledge meld into a sense of superiority and entitlement. Calltakers and dispatchers become impatient; annoy-ance creeps into their tone of voice. “your emergency is not an emergency—period.”
How did this happen? How do we become like that? We were going to change people’s lives and save lives!
When was the last time you asked: “Whom do I serve in the call center?” Some-how, the job has evolved into serving me: serving my knowledge, entitlement, and success. What has become of my priorities?
In the call center, our priorities must revolve around the agency and its stakehold-ers: police, fire, EMS, and our communities. We serve everyone but ourselves. our job is always about someone else. The rule applies to someone in cardiac arrest the same way it does to the person calling about a barking dog.
Understanding our relation to public service brings us back full circle to deter-mination and humility. We must remem-ber that the person on the other end of the phone or radio has needs greater than our own. We must be kind and sincere. People deserve that much.
We must ask the questions and give life-saving instructions exactly as written because we are determined to get the best information possible for our emergency responders. We must provide the highest standard of care and practice possible for callers during their emer-gencies and we must do so with humility.
We must never forget whom we serve. our work is not about us but rather the peo-ple coming into our world every day through every call we answer. g
We saw ourselves accomplishing major feats while managing hysterical people. This was the dream job.

THE JOURNAL | May/June 2011 11
Phantom calls haunt dispatch centers
The stories show a similar pattern. A call comes in and a dispatcher picks up the line to hear no one on the other end. Thirty seconds later, it happens again but this time another dispatcher fields the call. The pat-tern repeats sometimes hour after hour, vis-iting itself upon any number of dispatchers working the shift.
But is it the usual suspect, “pocket” wire-less cell phone calls, or something else caus-ing the annoyance?
For the Palo Alto (Calif.) Police Depart-ment, the phantom was a misfiring auto-matic alarm system placed inside a vehicle to alert 9-1-1 centers when an accident occurs. over a five-hour period in January, the cul-
prit triggered 566 calls, according to a story in the Palo Alto Daily News.
Unlike the services provided by onStar, which has real people answering calls com-ing from vehicles when an accident occurs, automatic dialing services connect directly to dispatch centers. No one moderates from the middle, fueling disruption of the 9-1-1 system and aggravation among those hired to coordinate response when it’s a false alarm.
Automatic gadgets behaving badly, how-ever, aren’t the only phantoms plaguing the system. others jockeying for position include wireless phones preprogrammed to dial 9-1-1 and the accidental resend of a 9-1-1 call from a wireless phone or landline. In some com-munities phantom wireless calls account for between 25% and 70% of all 9-1-1 calls, according to statistics from the National Emergency Number Association (NENA).
To combat the phantom calls, the Cen-ter for Problem-oriented Policing has made the following recommendations (Misuse and Abuse of 911, Guide No. 19):
• Require manufacturers to redesign wireless phones. on June 9, 1999, the Federal Communications Commission (FCC), which regulates the wireless industry, requested that manufactur-ers redesign their wireless phones to address the phantom call problem.
• Recall preprogrammed wireless phones. While an FCC order would address all future wireless manufacturing, a recall would resolve the issue of the millions of phones that currently cause phantom calls.
• Distribute phone button guards. Button guards reduce the accidental pressing of the 9 or 1 key, which causes certain phones to speed dial 9-1-1, and protect the redial key if 9-1-1 was the last number dialed.
• Prohibit automatic 9-1-1 dialing. Sev-eral states and parts of Canada prohibit automatic 9-1-1 dialing systems. Use of an automatic device that connects to the Palo Alto dispatch center is a mis-demeanor and in February, Palo Alto Police asked the FCC to investigate the mobile device that triggered hundreds of calls received in January.
IndustryInsider
About 1,430 Journal readers answered a seven-question survey evaluating the Nov/Dec 2010 issue for a chance to win one of two iPod touch devices up for grabs.
or, maybe, they took 10 minutes out of their day just to give us their opinion about a magazine devoted to the 9-1-1 dispatch community?
Whatever their reason, the winners were glad they did.
Tracey Erickson, supervisor, Penobscot Regional Communications Center (Bangor, Maine), said word of an iPod in the mail made her day, but it wasn’t the only delivery she looks forward to.
“I usually read it [The Journal] from cover to cover,” she said. “This is one of the better magazines for dispatch.”
Erickson, in charge of training and qual-ity assurance at her center, concentrates her time on The Journal searching for stories related to training and stories that might benefit the center’s entire staff. Articles about stress and wellness, she said, score high among the dispatchers.
Shane Sweno, telecommunicator II at Williamson County Department of Emer-gency (Georgetown, Texas), said the win turned his luck around.
“This is absolutely incredible,” he said. “I never win anything.”
Sweno prefers the Journal’s Continuing Dispatch Education (CDE) articles to main-
tain his tri-certification (EPD, EMD, and EFD). He also enjoys reading articles about the technological applications in centers around the world.
“It’s very interesting to me,” he said. “Not everyone does the exact same thing but everybody has a common goal.”
The Journal received survey results from readers in the United States, Canada, Eng-land, Australia, New Zealand, Ireland, and Wales. Watch for future survey contests to be announced. Who knows? your turn to win might be next. g
Contest Winners
Journal readers reap rewards

12 THE JOURNAL | emergencydispatch.org
Hialeah is new home to tri-accredited ACE
The City of Hialeah (Fla.) Public Safety Communications Division is now home to a tri-accredited emergency dispatch center.
The announcement, made April 21 at Navigator 2011 in Las Vegas, underscore the center’s high standards and excellence in three disciplines of emergency dispatch: law enforcement, fire, and EMS. It is only one of three 9-1-1 centers in the world to achieve triple Accredited Center of Excellence (ACE) status through the National Acad-emies of Emergency Dispatch® (NAED™).
Hialeah Director of Communications Chief Lazaro Guerra credited hardwork-ing staff for reaching the goal that not only accomplishes prioritized emergency response and technical capabilities but, also, the cus-tomer service provided at a center receiving 345,500 calls annually. Hialeah is the fifth largest city in Florida.
“Tri-ACE was the direct result of shared staff training, hard work, and tenacity,” he said. “We are now able to verify and validate our performance for everyone to see.”
The recognition followed within two years of the center’s consolidation. In octo-ber 2009, the dispatchers and calltakers from two centers merged into a new 3,000 square-foot facility located in the fire admin-istration building.
Waste management crews trash crime
Local police and emergency services have moved into the sanitation line.
Well, sort of.A program initiated by Waste Manage-
ment (WM) Inc., a national company based in Houston, Texas, provides a community
watch program for sanitation drivers through partnerships with local police and emergency services agencies. Drivers who are taught what to look for in relation to suspicious people or surroundings don’t intervene if they notice something amiss. Rather, they are trained to report the situation to their WM dispatcher who in turn conveys the informa-tion to the proper authorities.
According to information on WM’s web-site: “The right information at the right time can halt or even prevent crime, reduce the extent of personal injuries or property dam-age, or keep a minor mishap from turning into a major catastrophe.”
And who better to notice than waste management crews routinely traveling neighborhood routes? The frequency in which crews travel the same routes makes them the ideal eyes for catching something out of character like warehouse doors open after closing time, an overturned car on a deserted road, or a stack of unopened news-papers in a driveway.
The National Sheriffs’ Association rec-ognized the Waste Watch program in 2008 with its Excellence in Neighborhood Watch award, four years after the program started.
Proposed legislation could persuade calls to 9-1-1 in case of overdose
The Palm Beach County (Fla.) Sheriff’s office (PBSo) is working with Florida Rep. Mackenson “Mack” Bernard to create a Good Samaritan law in hopes of preventing more deaths from accidental drug overdoses.
The legislation would provide limited immunity from drug-possession charges being filed against a drug overdose victim or a witness seeking medical assistance for the victim, according to a Sun Sentinel article. In turn, hopes are that more people will seek the medical attention without worrying about potential consequences to themselves.
“Fear of law enforcement is the main rea-son people don’t call 9-1-1,” PBSo Detective Gary Martin said in the article. “What we’re hoping to do is organize a public-awareness campaign. In an overdose situation, don’t concern yourself about getting arrested.”
Bernard planned to introduce the legisla-tion when Florida’s legislature was back in session in March.
New Mexico was the first state to adopt a 911 Good Samaritan law in 2007.
According to the Centers for Disease
Control and Prevention, more than 20,000 people die each year in the United States from drug overdose. Drug overdose deaths were second only to motor vehicle crash deaths among leading causes of uninten-tional injury death in 2007. According to the Sun Sentinel article, the number of acciden-tal-overdose deaths in Palm Beach County in 2009 was 286 and in 62% of them, at least one other person was with the victim.
There’s an app for that
Smartphone applications have discovered public services.
The free iPhone fire department app, publicly released in January, connects a per-son trained in cardiopulmonary resuscitation (CPR) to someone needing the help. Accord-
ing to a TechCrunch article, the iPhone user registers when launching the CPR app. A 9-1-1 dispatcher receiving a call about a sus-pected cardiac arrest can activate the app; the app uses the iPhone’s geo tracking service to locate a person close to the incident and will-ing and registered to give CPR. It’s up to that individual to reach the scene. The app also includes the locations of automated external defibrillators (AEDs).
The San Ramon Valley Fire Protection District in connection with students at the Center for Applied Infomatics at Northern Ken-tucky University developed the app.
other apps focus on the law enforce-ment side of public safety. According to an article in Government Technology, the not-yet released SafetyNet Mobile Insight app will give police officers the ability to point an iPhone camera at a location, use the phone’s GPS to bring up the address in question, and check law enforcement history or officer safety hazard information for that specific location.
The app has several applications, accord-ing to its developer. For example, the app could come in handy for police scanning addresses for registered sex offenders in a neighborhood where a child has been
more information about the app can be found at firedepartment.mobi/

THE JOURNAL | May/June 2011 13
reported missing. The app can also be used for video chats and to track police units in relation to a crime scene. The phone doesn’t store the data and the messages are encrypted through a virtual private network. If a phone is lost, data can be remotely wiped.
Another app, this one not yet released, gives University of Maryland dispatchers direct access to the scene. According to an Emergency Management article, the V911 app streams audio and video from a 9-1-1 caller to the university’s dispatch center. With the touch of a button the app can be enabled, forming a connection between dispatcher and caller.
A four to six week pilot was scheduled to start at the end of March and there are plans, if all goes well, to have V911 available when fall semester begins in August. Researchers are negotiating with wireless carriers to cover the cost.
National consortium monitors emerging health trends
An emergency communications system operated by the Centers for Disease Con-trol and Prevention (CDC) and comprised of 176 medical organizations provides cli-nicians with up-to-date information about emerging health trends. And the National
Academies of Emergency Dispatch® (NAED™) is one of the providers.
The extended network under the CDC’s Clinician outreach Communication Activ-ity (CoCA) distributes information about trends, such as pandemics, natural disasters, and terrorism, in order to:
• helpcliniciansprovidethebestpos-sible care to patients by supplying them with the most current and reliable information
• disseminateevidence-basedhealthinformation and public health emer-gency messages to clinicians
• provide and promote emergencypreparedness and response training opportunities
• obtainfeedbackfromhealthcarepro-vider audiences to help improve emer-gency communications to clinicians
• identifyclinicalissuesduringemergen-cies to help direct communication strat-egy and outreach to clinicians
Clinicians signed up for the service are eligible to receive information via several sources, including e-mail news releases from the CDC, training and conference announce-ments, and direct e-mail access ([email protected]) for questions and feedback. Influenza preparedness and clinician involvement in the cholera epidemic in Haiti were among the topics discussed during recent confer-ence calls CoCA has sponsored.
Old scam packaged with new twist
A new twist on the wel l - traveled “advance fee” scam pulls police officers into the game with one catch—the officers are as phony as the claims.
you’ve heard of the scam: the potential victim must send $19.95 for priority ser-vice to receive $15,000 won in a contest. The winner doesn’t remember entering a sweepstakes or in the case of a lottery, buy-ing a ticket, and that’s where the new twist comes in.
A scammer claiming to be a local police officer later contacts the potential dupe, say-ing he or she has caught wind of the contest (and presumably a list of its winners) and has
How would your communications center celebrate the arrival of a new computer software system? High fives? Applause? or maybe nothing at all?
Well, the Carrollton (Texas) Public Safety team decorated their halls using brightly-colored signs and helium-filled balloons and
served frosted cupcakes adorned with syringes delivered by a dis-patcher wearing a lab coat to celebrate the arrival of the medical ver-sion of ProQA®.
A columnist in the center’s newsletter, The Telecommunicator, rejoiced at the efficiency and ease the software would provide in comparison to the manual EMD cards they have been using since version 10.0: “Here’s the cool part—based on answers you provide in Case Entry and Key Questions (which is a series of clicking for the most part), the program will calculate your Determinant Code and take you straight to the only Post-Dispatch and Pre-Arrival Instruc-tions you are supposed to read! And, for example, instead of memo-rizing the card and panel number for a ruptured cord (F Card, Panel 10a), there is [a tab] you can click on that will take you directly to that series of instructions to read verbatim to the caller. If you come across an instance where an agonal check is appropriate, there is an icon you can push and the program will even display a clock for you to time with.”
The columnist goes on to acknowledge the Carrollton Fire Department for an equipment request to the City Council making the software purchase possible. g
CeLeBration
ProQA is something to get excited about
ProQA® Paramount, © 2004-2011 PDC.

14 THE JOURNAL | emergencydispatch.org
a call into the FBI to verify the legitimacy. you guessed it. The phony officer follows
up, claims the contest legit, and instructs the “winner” to send the money ASAP before further delay results in losing to a second name selected.
The Salem (Mass.) and Eugene (ore.) Police Departments recently reported two such cases—and similar to other scams—pri-marily targeting the elderly population.
The onerous attempts to rob the elderly of retirement savings have lawmakers in states across the country bent on prosecuting the scammers. For example, Virginia legisla-tors are proposing felony counts against con artists found guilty of scamming people over the age of 60 or those with certain disabili-ties. The law would increase penalties and jail time. The legislation is modeled after similar legislation in states known for larger than average elderly populations, including Arizona, Florida, and Nevada.
The first step, however, is catching the con artist and virtually all municipalities rec-ommend calling 9-1-1 as the first step when a scam is suspected.
Calling 9-1-1 is free and easy for the right crowd
Law enforcement and agencies benefit-ing seniors offer free emergency 9-1-1 cell phone programs based on two conditions: you can’t use the phone for anything else and, in most cases, you must be over the age of 65 to qualify. The service generally waives the activation fee and monthly charges. The fol-lowing list provides a few of the free services we found.
The Burlington County (N.J.) Sheriff’s Department Senior Services Unit accepts donations of used cell phones and power charging cables from the public. An out-source agency tests each phone and deletes personal information.
The Clallam County (Wash.) Sheriff’s office received 86 used cell phones ear-lier this year from the public to reprogram through the national 911 Cell Phone Bank before distributing them free to vulnerable populations without immediate 9-1-1 access, including senior citizens, people who live
alone, people with disabilities, and victims of violent crimes.
The national 911 Cell Phone Bank, cre-ated in May 2004, collects used cell phones that are distributed to law enforcement and affiliated victim services agencies. The organization encourages community dona-tions through local events and sending the phones to the phone bank in prepaid boxes it provides. The community sending in the donated cell phones receives funds for the value of the phones collected.
The Des Plaines (Ill.) Cell Phones for Seniors Program provides a free 9-1-1 emer-gency digital cellular telephone to county res-idents over the age of 65 who Do NoT have a cellular phone. Any brand, make, or model of cellular phones is accepted for donation, whether it is in working order or not.
The Black Hawk County (Iowa) Sheriff's office Senior Safe cell phone program has given more than 6,000 cellular phones to senior citizens living in the county. Recipi-ents are encouraged to use the phone to dial 9-1-1 to report accidents or to summon help if witnessing a crime in progress or someone else in need.
But what good is a cell phone if the senior doesn’t know how to use it?
Those are the questions that motivated the Brookfield (N.y.) High School Key Club to make a trip to the city’s senior center. The students, members of the high school arm of the volunteer-based Kiwanis Club, regu-larly stop by to teach senior cell phone users to make the most of the device, including texting, checking voicemail, and maybe even downloading the latest apps.
Campaign urges women to call 9-1-1 at heart attack warning signs
The U.S. Department of Health and Human Services (HHS) office on Women's Health (oWH) introduced a national initia-tive to increase awareness and recognition of the seven most common heart attack symp-toms among women and to encourage calling 9-1-1 when these symptoms occur.
The Make the Call, Don't Miss A Beat campaign aims to educate, engage, and empower women and their families to rec-ognize the seven symptoms of a heart attack that most commonly present themselves in women. only half of women who partici-pated in an American Heart Association (AHA) survey recognized chest pain and
pain in the arm, neck, and shoulders as typi-cal symptoms of a heart attack. Even fewer women could identify other common heart attack symptoms, including shortness of breath (29%), chest tightness (17%), nausea (15%), and fatigue (7%).
The ef for t i s consistent wit h t he Healthy People 2020 goal to increase the proportion of adults aged 20 years and older who are aware of the early warning symptoms and signs of a heart attack and the importance of accessing rapid emer-gency care by calling 9-1-1 or another emergency number. The office on Wom-en's Health, which is sponsoring a national public health education campaign, urges women to make the call to 9-1-1 immedi-ately if they experience one or more of the following symptoms:
• Chestpain,discomfort,pressure,orsqueezing
• Shortnessofbreath
• Nausea
• Light-headednessorsuddendizziness
• Unusualupperbodypain,ordiscom-fort in one or both arms, back, shoulder, neck, jaw, or upper part of the stomach
• Unusualfatigue
• Breakingoutinacoldsweat(differsfrommenopause hot flashes because there is no “hot” period during a cold sweat)
The new Make the Call initiative will include a pub-lic service advertising cam-paign including: TV, radio, print, and outdoor materials; a campaign website, a strong social and news media effort; and partner- and commu-nity-based outreach. g
more information can be found at www.womenshealth.gov/heartattack

THE JOURNAL | May/June 2011 15
g FaQ
BestPractices
Brett:I would like the Academy’s perspective on
a rather unusual call I answered. The daugh-ter of an 82-year-old male called and said her father was unconscious and breathing with the aid of a respirator. The daughter said he sounded as if he was gurgling (perhaps ago-nal breathing) and she attempted to suction his mouth but nothing came out. She also said that her father had a pulse. What is the Academy’s perspective on this type of situa-tion? Is the protocol still followed using CPR instructions or is this null and void because of the respirator?
Thank you,Melissa BrownEmergency Communications of Southern oregon
Melissa:Excellent question.CPR supports circulation and breath-
ing manually and externally. There are also medical devices designed to support circu-lation and breathing on an ongoing basis. Devices that help failing hearts pump blood are most commonly called Left Ventricular
Assist Devices (LVADs). These are less com-mon and less well known to the public than the familiar respirators many patients use to assist breathing but, basically, both types of devices support a vital function.
Fortunately, caregivers who are famil-iar with the devices are mainly the ones making emergency calls for these patients. They are aware of factors that might prohibit a certain procedure because of the likelihood of unwanted results. For instance, doing chest compressions on patients with some types of LVADs is inadvisable because the force of the com-pressions can tear the catheters out of the heart, while CPR is okay with other medi-cal devices. Additionally, we don't always know what the underlying problem is, i.e., did the machine fail, or the patient?
Where does all of this leave the EMD? A call involving a patient using a respirator is a bit more straightforward since the rise and fall of the chest confirms breathing. If breath-ing is already being supported artificially, there is no need to do mouth to mouth. However, since unconsciousness with absent or questionable breathing calls for compres-sions, and we know the breathing we see is artificial, we can assume compressions are appropriate to advise when the respirator
patient is unconscious, unless the caregiver advises the situation otherwise.
In your case, however, the caregiver said a pulse was present. While the Academy does not advise pulse checks by laypersons because of the proven false-positive rate, there are pro-visions in the protocol for mouth-to-mouth only when a caregiver or health professional insists the patient has a pulse (Panel C-14). But because your patient already has the res-pirations covered, and a pulse was apparently present, it seems that following the protocol pathway for the unconscious but breathing patient is most appropriate. This leads us from the Protocol 31: Unconscious/Fainting (Near) DLS link to Protocol C, ending up on Panel 16 to monitor the patient until EMS arrival.
Since I brought up the LVAD issue, a related Axiom and Rule in MPDS® v.13.0 is designed to educate EMDs about these devices and encourage mouth-to-mouth only instructions or to follow the advise of the caregiver.
While various presentations and situ-ations make absolutes impossible, it helps to know something about the purpose and function of artificial support systems in order to make reasonable decisions in cooperation with the often-educated caller. In short, if we can assume the artificial sys-tem is working, which it most often is, we can leave that issue alone and focus on the problem. Remember, the caller has called for help and providing that help is not harmful to the already dead or dying patient. It is far better to provide compressions to someone who may not need the compressions than not provide compressions to someone who does.
I’m sorry I couldn't give you a short and more definitive answer, but this subject is not always black and white. Let me know if this helps.
Brett A. PattersonIAED Academics & Standards AssociateResearch Council Chair g
Does use of respirator void CPr for unconscious but breathing patient?
By Brett Patterson
16 THE JOURNAL | emergencydispatch.org

THE JOURNAL | May/June 2011 17
Guide to the Stars Navigator celebrates emergency dispatch
Navigator 2011 opened and closed with-out a dry eye in the place.
Well, at least that’s how it happened for many of those attending Navigator at the Paris Hotel in Las Vegas from April 20 to April 22.
Wednesday’s opening Keynote Speaker Richard Picciotto brought tears during a 60-minute presentation that ended in a stand-ing ovation. Picciotto, a 28-year-veteran of the New york Fire Department, was among 13 survivors tunneling out of the North Tower on Sept. 11, 2001, hours after the building col-lapsed, trapping them in debris between what used to be the sixth and seventh floors of the World Trade Center building.
Jack Hamilton, a dispatcher from Branch-burg, N.J., is like many Americans when it comes to remembering the events of that day.
“Ten years in September (2011) and it’s just like yesterday,” said Hamilton, a former New york (Kenilworth) firefighter. “I have friends who died in the tower. Two of the men were Port Authority police officers. It was very hard.”
The two speakers highlighting Thursday’s opening Session and the “Au Revoir” Luncheon may have lacked the poignancy of 9/11 but cer-tainly not the personal charisma to bring—in contrast—tears of laughter to their audiences.
But that wasn’t because of their delivery. They had the subject matter to punctuate talks with some light-hearted humor.
Kevin Willett, a favorite speaker among the Navigator crowd, played segments from
songs found on his playlist including “Ain’t No Mountain High Enough,” “Proud,” “one Chance At A Life,” and “Circle of Life” to describe the soundtrack of a dispatcher’s life.
“We’re not going to be killed in the line of duty and maybe the biggest danger we face is the steam from opening a bag of popcorn fresh from the microwave, but that doesn’t diminish our job,” he said. “Chang-ing the world is a big deal and that’s what we do every day.”
Ed Racht, M.D., took a few punches to the funny bone during Jerry overton’s intro-duction of the AMR chief medical officer. After that, it was 45 minutes Racht spent itemizing a dispatcher’s toolbox in relation to skill set.
“you have to prepare for things most of us can’t imagine,” he said. “you need tools that look slightly different from the rest of the EMS world.”
The tools dispatchers require make up the heart of Navigator. Educational ses-sions, networking, exhibits, off-site visits to the local communications center, and even those few minutes in conversation prior to an opening presentation give dispatchers the opportunity to share their experiences among community partners.
“This is an exciting place to be,” said Donita Scott, a dispatcher for the Kear-neysville Communications Center in West Virginia. “Protocol means a lot to us. It’s life saving. We feel good about helping people in their time of crisis.” g

18 THE JOURNAL | emergencydispatch.org
ACE
rebecca FullerWest Metro FireLakewood, Colo.
Dispatcher Rebecca Fuller attended her first Navigator in the 19 years since accept-ing the job with plans to take in all she could about Quality Assurance, continuing educa-tion, and the Fire Priority Dispatch System™ (FPDS™). The agency Fuller works for as an EMD-Q is new to the Medical Priority Dispatch System™ (MPDS®), but she isn’t, having used it while working emergency communications in upstate New york. “It was a relief for me to go back to it (EMD),” she said. “I like the fact that we can modify our responses and that the determinants are researched and proven.” West Metro Fire is gearing up to implement ProQA® as part of the package and Fuller attended the Data Mining pre-conference classes to collect information for future use when the soft-
ware is up and running. “I just want to learn as much as I can and take it back to my center to help the program succeed,” Fuller said.
Jennifer swisherWashington County emergency Communications CenterWilliamsport, Md.
With Navigator’s growing list of ses-sions, the opportunity to network, and the conference’s rejuvenation powers, Jennifer Swisher looks forward to the conference she has attended five years running. “It’s a great way to expand your knowledge,” said Swisher, an EMD-Q, EFD-Q, EPD-Q, and ETC-I. “There are so many years of experience here. It’s amazing what you can actually resolve.” Pre-conference class From ostrich to Eagle gave Swisher tips on motivating personnel and preventing stag-nation. Whether motivating someone with-out blaming a group or working with people
who aren’t compliant, Swisher collected information that could benefit anyone from a line dispatcher to administration. Swisher maps out her list of must-attend sessions ahead of time and this year included those offered on the quality assurance and man-agement tracks plus the police session Psy-chology of an Active Assailant.
By The Numbers Navigator conference keeps on growing
1,200attendees
14countries represented
97speakers
91sessions
“I am passionate about EMD, and, where else am I going to find so many other people in one place that are just as enthusiastic?” —Vicki Mitchell
1 tri-aCe 12 new aCe's 33 re-aCe's
Representatives from new Accredited Centers of Excellence met Accreditation Chair Brian Dale and NAED Associate Director Carlynn Page on stage.

THE JOURNAL | May/June 2011 19
delsie LewisMuskogee County eMsMuskogee, okla.
Dispatch Supervisor Delsie Lewis works for a consolidated center serving both Musk-ogee City and County, so it was only natu-
ral to gather as much information possible about others in similar situations. Not only does the transition from four separate agen-cies to one provide a steep learning curve, but so does the addition of novice dispatchers plus the police and fire protocols. That’s why she finds Navigator’s leadership track and networking opportunities important. “It’s got to be the interaction with everybody,” Lewis said. “It’s getting to know how other people do things. The advice you get.”
Matt Formby and Chris MarshallHumboldt CountyWinnemucca, nev.
Communications Training officer Chris Marshall and dispatcher Matt Formby traveled to Las Vegas to attend the National Center for Exploited and Missing Children (NCMEC) ses-sion Time to Act: The 9-1-1 Center and Miss-ing Kids comm. course to gather tools useful in their communications center. Marshall said
Humboldt County receives calls about several chronic runaways in the community; sexual assault cases are coming in more often, too. “I’d like to see everybody in our center take the class,” Marshall said. Marshall also attended the From ostrich to Eagle class and classes included in the police, leadership, medical, and stress management tracks. Formby focused on the fire and police tracks.
28,696square feet of meeting rooms
16,343square foot space used for opening sessions
35,383square foot exhibit hall
15 sponsors generously contributed to the awards presented, including long-time sponsor EnRoute Emergency Systems that brings the Dispatcher of the year and Dr. Jeff Clawson Leadership Award to the stage each year.
305 sings and banners created by the graphics department adorned the conference halls.

20 THE JOURNAL | emergencydispatch.org
Navigator is quickly becoming the inter-national hotspot for emergency dispatch.
This year at every event and in every classroom, people from around the world took advantage of spending three to six days at the Paris Hotel in Las Vegas to participate in what Navigator facilitates best: learning, certifying, and networking, although not necessarily in that order.
Paulius Dobuzinskas, project director for the Medical Priority Dispatch System™ (MPDS®) implementation in Kaunas, Lithu-
ania, and five coworkers from the same coun-try spent three days in the pre-conference EMD certification course taught by Dave Brinton, an instructor from Salt Lake City.
“Protocol fits our vision to bring emer-gency care to a higher standard,” Dobuzin-skas said. “Dispatch will no longer be the weakest link in the chain of EMS.”
Dobuzinskas traveled thousands of miles as part of a team representing the Crisis Research Center and its affiliated emergency response facility. The emergency dispatch
center will be the first to introduce protocol to the Lithuanian govern-ment and the country’s 3.5 million citizens.
“ We k n o w h o w good the system is,” Dobuzinskas said. “It’s the safe way to dis-patch and covers all situations.”
São Paulo Serviço de Atendimento Móvel de Urgência (SAMU 192, with 192 being the number called in an emergency) is the
largest center in South America to adopt the MPDS and the first center in the world to put a Portuguese ProQA® version of MPDS into practice since going live Feb. 24, 2011.
Walquíria Regia Vilaça Mordjikian, executive coordinator of central operations, believes their support of protocol will stimu-late “a great revolution” in her country’s dis-patch system.
“This is a huge event in São Paulo [Brazil] and a tremendous benefit for our people,” she said.
The Global Scene Protocol and Navigator attract international crowd
Lysa Kimbrough9-1-1 association of Central oklahoma Governments (aCoG)oklahoma City, okla.
Lysa Kimbrough, ACoG training coordi-nator and public educator, approached her first time at Navigator like a child in a candy store. As someone who trains dispatchers
staffing the 20 Public Safety Answering Points (PSAPs) in the central oklahoma area, Kimbrough honed in on tracks provid-ing dispatch education ideas. With nearly all of the 20 ACoG PSAPs answering police and fire with some also handling medical calls, she concentrated on several tracks includ-ing the Psychology of the Active Assailant. Kimbrough was also keen on networking with other attendees. “I’m trying to meet new people,” she said. “It’s big to have that experience from all over the U.S.”
terry Bavousettamarillo emergency Communications Centeramarillo, texas
Terry Bavousett, assistant manager, arrived at his first Navigator with the impres-sions of center personnel who had attended Navigator 2010. “People were blown away,” he said. And by the time the pre-conference Executive Workshop was over, he had a pile
of notes that could help work out the kinks following consolidation of area communica-tions centers. With the center using all three protocols (MPDS, FPDS, and PPDS™) in

THE JOURNAL | May/June 2011 21
The transition to a standardized protocol system was a major undertaking. Pre-ProQA days, calltakers relayed calls to doctors on the dispatch floor. The doctors talked to each caller and decided case by case the response necessary. The process sometimes resulted in up to 100 callers stalled in a queue, waiting for response.
Fernando Luis Schmiegelow, director of marketing for Latin America’s software distributor SISGRAPH, said the protocol is making great headway.
“The patterned response helps SAMU 192 meet goals to rescue victims of the most grievous cases like heart attacks and acci-dents with firearms,” he said.
Mordjikian looks forward to claiming the first Accredited Center of Excellence (ACE) distinction in South America.
“That’s our next job,” she said.Paul Engelen, who co-managed a private
ambulance service in the Hollands-Midden region of the Netherlands, wanted a medical protocol featuring standardized questions to use in the affiliated dispatch center.
So, he did what anyone else might do: he went online and googled the words “emer-gency dispatch protocols.”
“MPDS was the first to come up,” he said. “I went to the site and watched the demon-stration. That started the ball rolling.”
The ball rolled along slowly and took sev-eral sharp turns during the three years it took Engelen to convince the Dutch Ambulance Institute of protocol’s benefit to EMS. The
26 EMS regions in the Netherlands are self-dispatching and every call coming into the centers are nurse-triaged. Ambulance pro-viders in the Netherlands are under contract with the Dutch Ambulance Center, which requires specific standards for each stage of emergency service patient care.
“It was a hard sell," Engelen said. "I had to convince them by showing what was wrong with the way we were doing dispatch. Calltakers were making mistakes without even knowing it. This wasn’t their fault but the fault of the system.”
Engelen contacted Jan de Nooij, the EMS medical manager at the Regional Ambulance Service and Emergency Medical Dispatch Center in Hollands-Midden. He liked the concept and protocol demonstration. Enge-len rallied co-workers. MPDS went live May 19, 2011, at the center in Leiden. Engelen anticipates five centers will follow.
Engelen modestly attributes at least this initial success to the 25 years he has dedi-cated to EMS. He is a known and accom-plished perfectionist.
“People trust me,” he said. “They listen to what I say.”
Rene van Kleef, ICT/Functional control room manager, Medical Hollands Midden, believes their ambulance service communi-cations center will ignite a dispatch revolu-tion in the Netherlands.
“We are proud of this,” he said. “This will prove a landslide in the Netherlands. People see how protocol works and the light bulbs will go off.”
Three communication specialists from the Jiangsu Province in China flew 15 hours to reach Navigator in time for the pre-confer-ence EMD certification course, with another three days to spend at the conference and tour the city that never sleeps.
“At Navigator we can meet others who use the protocol and learn from them,” said Suzhou Emergency Center Manager Luo Meng yue. “We’re also interested in becom-ing an ACE.”
The emergency dispatch center in Suzhou, Jiangsu Province of China went live with protocol on Jan. 1, 2011, approximately 10 years into the life of the center. The cen-tral facility and its 18 substations send medi-cal and police emergency response and serve 3 million people.
During the first four months of using MPDS, Pre-Arrival Instructions includ-ing those for CPR, pregnancy/child-birth, and choking have already helped save lives, according to Center Director Zhang Hong.
“We are the pioneers,” Hong said. “We are the first in China to implement the protocols and we want to be at the top for dispatch in our country.”
NAED President Scott Freitag called the international growth “exciting.”
“Just about everywhere we go calltakers are answering calls the way they should,” Fre-itag said. “other aspects of operations may vary from country to country but protocol is a common thread.” g
ProQA the transition was particularly tough for fire and police employees new to protocol. Bavousett had a hard time choosing which sessions to attend, finally deciding on the leadership and police tracks, knowing four
other people from his center were branching out to cover other tracks with plans to share information compiled during the conference.
Colette thibodeau and Myra LanthierPalmer Police departmentPalmer, alaska
Colette Thibodeau and Myra Lanthier made the trip from Palmer, Ala., to attend their first Navigator conference. The pre-conference class Complacency, Cannibalism, and Critical Thinking: How to Avoid a Toxic Workplace hit close to home as Lanthier reflected on a toxic supervisor she’d had in the past. She also attended leadership courses and the Wilder and Crazier Police Calls ses-sion to diversify her experience. Thibodeau attended the pre-conference offering From ostrich to Eagle, which reminded her that it’s oK to make waves. She also focused on attending classes about stress management and those offered by NCMEC that involved calls about missing and exploited children.
edward Washingtonoffice of Unified CommunicationsWashington, d.C.
The plan to go for ACE made Edward Washington's, assistant operations manager, simplified course selection. He attended ACE track classes including Bullets and Water: The Nuts and Bolts of Becoming an ACE for Police and Fire. He also attended police and quality assurance classes to round

22 THE JOURNAL | emergencydispatch.org
out his experience. But it isn’t just the ses-sions that Washington enjoys. “Navigator is great because it helps everyone come together and it’s a great learning experience,” he said.
Leanne stewartambulance tasmaniaHobart, tasmania, australia
For Communications officer Leanne Stewart, coming to Navigator in Las Vegas
was meant to be. The name she put in the hat was the one chosen by Paramedics Aus-tralasia to receive a $1,500 scholarship to attend. As the only one in attendance from Tasmania, Stewart attended medical courses including What’s New in v13 and Choking Case & 2010 Resuscitation Guidelines. Psy-chology of a 9-1-1 Call, Wilder and Crazier Police Calls, and stress management classes filled out her list. As an agency that services the 50,000 people in the state of Tasma-nia with its share of remote areas, Stewart enjoyed meeting people using the protocol throughout the world. “I love it (Navigator) and I’m planning on coming again in two years,” she said. “It’s certainly worthwhile.”
Keith Cameronamerican Medical responseJackson, Miss.
Stress management courses were a big draw for Communications Supervisor
Keith Cameron on the heels of traumatic calls/situations that have affected the cen-ter as well as fire and medical responders on scene. He also attended police track offer-
ings for a better perspective on the types of calls his center doesn’t handle. “I wanted to get a feel of the other side and what they
Dispatcher of the Year They meet again on Navigator’s stage
Denise and Tom (TJ) Cogswell enjoy the quieter side of life. They are active in their
Wolfeboro, N.H., community but never anticipated an event that would introduce
them to an audience of peo-ple from around the world.
That was until Thanks-giving Day 2010, the day Denise received an unex-pected and not at all wel-coming invitation to join the sudden cardiac death survivors’ club.
“I’ve gained a whole differ-ent view of living and dying,” Denise said. “It has enhanced my ability to enjoy all that is in my life, to live it the best way I can, one day at a time.”
Denise was at Navigator, along with her son Derek Brockney, and husband TJ to watch New Hampshire Bureau of Emergency Com-munication PSAP Supervi-sor Stephen Harris, EMD, accept the Dispatcher of the year Award.
Harris was at work on the midnight shift when he answered TJ’s call at 2:30 a.m. The nightmare TJ
thought was causing Denise’s wild thrashing had turned into something much more serious.
THE JOURNAL | May/June 2011 23
have to go through,” Cameron said. While it was Cameron’s third time attending Naviga-tor, it was the first time the three-day MPDS Mentor course had been offered and he was
among the first in line to register for that. Cameron highly recommends Navigator for its educational side and networking oppor-tunities including the opportunity to meet the various exhibitors.
Kecia Beverly-Leroyeast Bay regional Parks PoliceCastro Valley, Calif.
Kecia Beverly-Leroy couldn’t say enough good about Navigator after attending the conference for the first time. Dispatch-related offerings reinforced her skills and reenergized her motivation, giving her the desire to help others kick start their motiva-tion. Even though she works as a dispatcher for an agency that doesn’t use Academy pro-tocols, she got a lot out of the conference, finding little time to play while in the city that never sleeps. “I enjoyed it,” Beverly-Leroy said. “I didn’t play at all. I enjoyed the sessions and the keynote speakers.”
Marco Parigiregola Cadtorino, italy
First-time Navigator attendee Marco Parigi enjoyed the medical sessions because they added to his knowledge of fieldwork as a volunteer firefighter and volunteer Italian Red Cross worker. Since it was only his sec-ond time in the United States, Parigi partici-
“She wasn’t waking up,” TJ said. “I grabbed the phone and called 9-1-1.”
TJ expected his call would bring help to the scene. That was it. He did not antici-pate the Medical Priority Dispatch System™
(MPDS®) CPR Pre-Arrival Instructions (PAIs) Harris recited from the ProQA® screen. Derek, home from college, took over the phone, repeating the instructions, while his stepfather provided compressions.
“I did not know Steve would walk us through CPR,” TJ said. “We now know it was his great training to assist in CPR that saved Denise’s life.”
Harris stayed on the line with Derek until the ambulance arrived. Paramedics took over chest compressions and applied two shocks from a defibrillator prior to transport. From the local hospital, Denise was sent to Dartmouth-Hitchcock Medical Center in Lebanon, N.H., where she spent one week in ICU.
Dartmouth cardiac specialists diagnosed aborted sudden cardiac death caused by ven-tricular fibulation. She had suffered from heart arrest; the heart had stopped pumping blood. According to statistics, she had a two percent chance of survival.
Denise acknowledged Harris, her son, TJ, and MPDS for beating the odds.
“There were a lot of heroes that day,” Denise said. “And, I’d like to thank all of you.
I am alive because of what you do.”Their appearance at Navigator was
not their f irst face-to-face introduc-tion. Almost one month to the day after the emergency, Denise, TJ, Derek, and his 24-year-old brother Jason Brockney, stopped by the communications center to
personally thank Harris.Harris was pleased to meet the recipient
of his actions, although he downplayed the heroism involved.
“I followed the protocol and everything worked out as it’s supposed to,” said Harris, a firefighter prior to transferring to dispatch three years ago. “I am in awe [of the award], but that’s not the reason I do this. It feels great to know we can help save lives.”
Denise doesn’t recall the medical aspects of her arrest. As soon as her brain healed from the temporary loss of oxygen, she was able to gain long-term memory and make a full recovery. She does, however, recall a spiri-tual event from the emergency scene.
“I could see my husband and my son over me and I could hear my son’s call, but I
was unable to communicate back,” she said. “I believe that God did not think it was my time and gifted back to me my life as I know it now.”
In a round about way, that partially explains the reason Denise, TJ, and Derek agreed to join Harris on stage. Telling others
about their experience can influ-ence decision makers.
“We speak out on our emer-gency event to help bring attention to the need for CPR, AED's, train-ing for emergency staff, and fund-ing to keep these programs in tact,” Denise said. “We are proof that the people and programs can and do save lives.”
The following is an excerpt from that 9-1-1 call:
Dispatcher: "New Hampshire 911. What is your emergency?"
TJ: "My wife is unresponsive. I just woke up in the middle of the night.”
(Note: Harris immediately asked the Key Questions to gather more information about the situation. When TJ responded no to whether she was conscious and breathing and that she had no pulse, Harris immedi-ately instructed TJ to begin giving CPR— Denise had gone into cardiac arrest.)
Son: “you can do this, Mom! We love you mom, come on.”
Son: “She’s alive! She’s alive!”Dispatcher: “What is she doing?”Son: “Her mouth is kind of moving. Her
airway is open.” g
“I’ d like to thank all of you. I am alive because of what you do.” —Denise Cogswell

24 THE JOURNAL | emergencydispatch.org
road Trip Las Vegas Fire & Rescue opens doors to Navigator
Marco Parigi, a volunteer firefighter and volunteer Italian Red Cross worker, took the bus ride to a backstage tour of Las Vegas Fire & Rescue (LVFR) to compare notes.
“It was interesting to see how in the U.S. the rescue operators work because in Italy we have a different methodology,” he said.
The center in Las Vegas dispatches both medical and fire calls for a variety of agen-cies including three fire departments, two air force bases, and McCarran International Airport’s fire station, while centers in Italy, are divided by province with each province dispatching from three separate centers (medical, fire, and police) to handle emer-gency calls.
But it wasn’t just Parigi who took the tour, offered Wednesday and Thursday dur-ing the Navigator conference, for more than just an afternoon joy ride.
Montye Jolliff, 9-1-1 dispatcher for Fulton County (Ill.) Sheriff’s Department, noted the organization’s preparedness, cama-raderie, and proactive attitude. The feature capturing his attention, however, was their ability to dispatch responders from any agency served by the Fire Alarm office. For example, North Las Vegas firefighters might be dispatched to an incident in Clark County
pated in the field trip to the Las Vegas Fire & Rescue communications center. His suitcase was filled with the information he was taking home to co-workers. Parigi enjoyed his Navi-gator experience and hopes to attend next year’s conference in Baltimore.
dr. James KuthyBiddle Consulting GroupFolsom, Calif.
A decade into his attendance at Navigator and industrial and organizational psycholo-gist Dr. James Kuthy never tires of network-ing and the opportunity to learn more about the profession. While at the Paris, he gave the session Performance Appraisals and Ter-minations: Researched-Based Best Practices, which he described as a hot-button issue revolving around performance appraisals, documentation, best practices suggested by the courts, and minimizing legal exposure. He also sat in on sessions about personnel-related issues and certification.
Corey Howardshelby County Fire departmentMemphis, tenn.
For CAD Manager/Communications Supervisor Corey Howard, his second Navi-gator was the chance to divide his time learn-ing more about the roles he has assumed at the Shelby County Fire Department. Since
Next Generation technology is part of his job, Howard attended the Introduction to Converging 9-1-1 Technologies. other classes he chose included Data Mining 201 and selections from the technology and opera-tions tracks. Howard also spent time gath-ering information to use in his supervisory role including conflict resolution and stress management. “There’s a lot of valuable infor-mation that’s given here,” Howard said. g

THE JOURNAL | May/June 2011 25
Navigator was just the right setting for artist Jason Bullard’s series No Greater Love.
“We just knew that we wanted to get those in the hands of as many people as pos-sible,” said Mike Singleton, co-owner of Sage-brush Fine Art, publisher of the series. “It’s such a wonderful piece.”
No Greater Love features figures from public safety. The firefighter with blazing wings—distributed at the conference—is the second in the series, following a piece honor-ing the military. Separate pieces of an EMT and, also, a dispatcher are next in line once he completes his current work showcasing police.
Five years as a police offi-cer spurred his No Greater Love series, Bullard said.
“I have such a high respect a n d r e g a r d for what they do,” he said. “The greatest
love of all is when some-one lays down their life for another.”
Bullard hopes that his images convey respect for the people dedicated to protecting the public. The feedback he’s received has been positive.
“People really seemed to like them,” Singleton said. “We like to do prints of those who help save lives throughout com-munities.” g
No Greater LoveArtist honors dedication to public good
Overlooking the Crowd Perspective depends on your view
Standing 50 stories high at the top of the Eiffel Tower at the Paris Hotel in Las Vegas gave a new perspective to Navigator’s theme: you Can Change the World.
“If you’re going to change the world you have to be able to look at other perspectives,” said first-year Navigator presenter Jennifer Kirkland, Vail (Colo.) Public Safety Commu-nications training supervisor, who included a tour to the top of the Eiffel Tower as part of her objective: Perspective presentation. “It’s always good to take another look at what someone’s trying to tell you.”
For instance, a new hire’s view on the com-munications center differs from a trainer’s or manager’s perspective. Look at it this way: a truck might hit a person running across the street between casinos while a plane is more likely to take out a person standing on the top of the simulated Eiffel Tower.
A different perspective also changes our view, both literally and figuratively.
Linda Gorko with PSC Calgary in Cal-gary, Alberta, Canada, said she could no longer saw the gum stuck to the sidewalks below, but she did notice the empty pool on the roof of Caesars Palace.
“you get so focused into the detail that you don’t step back and see the big picture,” she said.
Rosanna Wisener, San Marcos (Texas) Police Department records/communications manager, compared her distance above the crowd to the dispatch environment.
“The calltaker is removed from the scene, making it easier to calm a distraught caller,” she said. “Down there is the hustle and bustle and from up here it’s orderly.” g
while Clark County firefighters are respond-ing to a call on the Strip.
If a disaster strikes the Fire Alarm office, dispatchers can continue sending response from the Mobile Command Unit attendees had a chance to step inside.
Upstairs from headquarters is home to 47 dispatchers/calltakers that, according to Supervisor Mike Tomko, rotate positions with shifts staggered to begin every two hours. Walls covered with Life Saver awards and Special (baby) Delivery Reports high-light the great service they provide.
Fire dispatcher Christy Canada has worked in dispatch for 14 years, spending the last seven at LVFR helping to answer the more than 300,000 calls that come in each year.
“I enjoy the adrenaline and I enjoy help-ing,” she said.
Canada credits technology and protocol for making her job more efficient. The auto-mated dispatching system that takes over once a call is assigned broadcasts tones and voice announcements to responding units. GPS tracking allows dispatchers to identify responders closest to the scene. All depart-ments have signed an automatic-aid agree-ment to send the closest unit to the call regardless of jurisdiction.
But dispatch wasn’t the only stop during the two-hour tour.
In Fire Station No. 1 Fire-PIo Tim Szy-manski gave attendees a look at a fire engine’s tool cache and the inside of an ambulance. Their equipment for cardiac arrest patients includes the Zoll AutoPulse (provides 100% efficient CPR) and cold saline to start hypo-thermia treatment through a cold intrave-nous infusion. Szymanski said 48% of cardiac arrest victims they treat go home.
“The results have just been astounding,” he said. “We’re really, really proud.”
Ambulance Tasmania Communications officer Leanne Stewart was pulled in by the equipment LVFR uses to help patients suf-fering from cardiac arrest.
“That’s fascinating,” she said. “They are going to the next stage of assistance to achieve the better outcome.”
LVFR started small as a volunteer fire department more than a century ago. The city has provided funding since 1942 and today LVFR services 1.5 million people resid-ing in Las Vegas Valley (435 square miles). LVFR employs more than 600 people—including 47 calltakers/dispatchers using the Medical Priority Dispatch System™ (MPDS®)—staffing 18 fire stations and 39 paramedic rescue (ambulance) units. g
for more information about Jason Bullard, visit www.bullardpublishing.com/?page_id=11.his prints can also be found on www.sagebrushfineart.com/results.php?artist=34&category=&size=&keyword=KEYWORD&code=CODE&s=1&x=129&y=26
26 THE JOURNAL | emergencydispatch.org
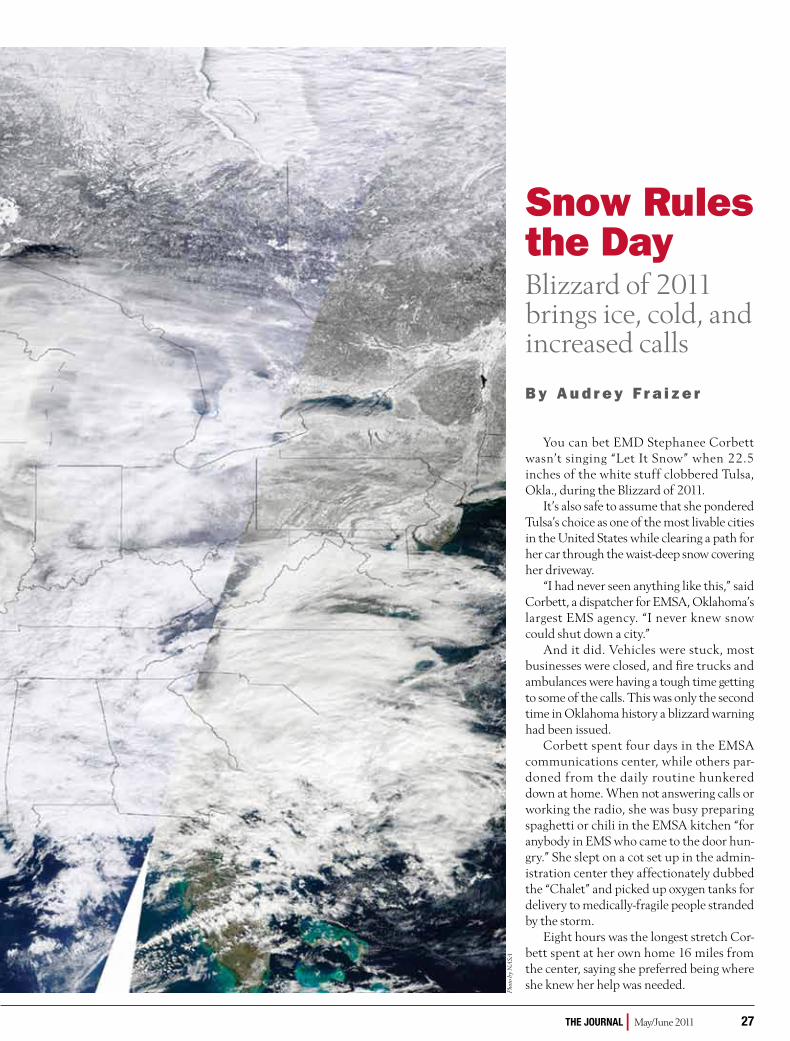
THE JOURNAL | May/June 2011 27
Snow rules the Day Blizzard of 2011 brings ice, cold, and increased calls
B y A u d r e y F r a i z e r
you can bet EMD Stephanee Corbett wasn’t singing “Let It Snow” when 22.5 inches of the white stuff clobbered Tulsa, okla., during the Blizzard of 2011.
It’s also safe to assume that she pondered Tulsa’s choice as one of the most livable cities in the United States while clearing a path for her car through the waist-deep snow covering her driveway.
“I had never seen anything like this,” said Corbett, a dispatcher for EMSA, oklahoma’s largest EMS agency. “I never knew snow could shut down a city.”
And it did. Vehicles were stuck, most businesses were closed, and fire trucks and ambulances were having a tough time getting to some of the calls. This was only the second time in oklahoma history a blizzard warning had been issued.
Corbett spent four days in the EMSA communications center, while others par-doned from the daily routine hunkered down at home. When not answering calls or working the radio, she was busy preparing spaghetti or chili in the EMSA kitchen “for anybody in EMS who came to the door hun-gry.” She slept on a cot set up in the admin-istration center they affectionately dubbed the “Chalet” and picked up oxygen tanks for delivery to medically-fragile people stranded by the storm.
Eight hours was the longest stretch Cor-bett spent at her own home 16 miles from the center, saying she preferred being where she knew her help was needed.
Phot
o by
NA
SA

28 THE JOURNAL | emergencydispatch.org
But call it a bad experience?“Not at all,” she said.The 26.1 inches of snow that pulverized
Tulsa during three significant storms in late January and early February broke the record of 25.6 inches set in 1923-1924 and, oddly enough, drew people together both inside and outside the communications center.
The Tulsa Area Chapter of the Ameri-can Red Cross opened warming stations for stranded travelers and placed volun-teers on alert. The Tulsa County Sheriff’s Department and EMSA deployed 4-wheel drive emergency vehicles. Residents put plows on pick up trucks to clear streets, checked on senior citizens and people with disabilities, and pushed stalled cars up highway ramps.
EMSA dispatcher Stephanie Jones, who also spent four consecutive days working the phones and radio, said it was the adrenaline rush that kept them going.
“The hardest part was making sure we were all fed,” she said.
the Blizzard of 2011The 2011 North American winter storm
brought frigid air, heavy snowfall, and pow-erhouse winds in its path from New Mexico and northern Texas to New England and Eastern Canada.
In Chicago, the Blizzard of 2011—the third worst in the city’s history—will be remembered for its winds topping 60 miles per hour, 21.2 inches of snow, thunder snow, wind chill, white-out conditions slashing visi-bility under a quarter of a mile, and dramatic increases in the number of 9-1-1 calls.
“Stuck” is the word Rhonda Lea used to describe conditions in Aurora, Ill., a suburb in Kane County southwest of Chicago.
“People were stuck in cars and their homes,” said Lea, supervisor of Communi-cations for the Aurora Police Department. “The snow didn’t paralyze us like it did in other parts of the country but, still, 18 inches of snow at one time was pretty amazing.”
Snow ordinances prohibiting parking during a snowfall might have been the bigger headache for
drivers abandoning their cars en route or unable to move them from city streets and alleyways. Between Feb. 1 and Feb. 6, Aurora police reported that 101 vehicles were towed to make way for the snowplows. In nearby Lake County, cars stuck in unincorporated areas were towed at the request of local fire departments, the Illinois Department of Transportation, and other agencies.
Unlike in Chicago where snow-idled cars were towed without cost, however, some Lake County motorists paid hefty towing fees to retrieve their cars. That’s because City of Chicago tow tr uck s removed the cars on Lake Shore Drive. In Lake County, private companies did the towing. The hardest part in Chicago was finding your car among the dozens of holding lots.
But not everyone made it out of their snow-stuck cars. Dispatchers in Green County, Wis., kept company with motorists stranded for up to 11 hours overnight along roads east of New Glarus before emergency workers could reach their vehicles.
1. Bring out the Plows Trucks pushed piles of snow off roads giving access to local traffic while holding parked cars captive, unless towed.
2. Clearing a Path Snowblowers were the tools of necessity for people given little choice but to cut paths through snow clogged sidewalks and driveways.
3. easier to Walk Drivers plowed their cars through snow stacked streets in metropolitan Chicago following one of the worst blizzards on record.
1 2
3

THE JOURNAL | May/June 2011 29
“They did a good job of keeping in touch with the motorists via cell phone,” said Tanna McKeon, emergency management coordinator for Green County. “We wanted to make sure they were oK.”
At one point, a Green County Division of Wildlife Resources warden drove his snowmobile to deliver a gallon of gas to a stranded mother with a toddler in the car; it was too cold to bring them out on the snow machine, though, they now had enough gas to stay warm until emergency crews could reach them.
snow shifts response policiesFending until help arrived was the order
of the day in many areas trounced by snow, drifting, and subzero temperatures making travel impossible.
In Tulsa, dispatchers had to do the impossible. Callers were told EMS could not respond immediately to situations coded oMEGA, BRAVo, or ALPHA. Emergency response w a s l i m i t e d t o E C H o - , DELTA-, and CHARLIE-level Determinant Codes.
“I’ve never been in a position where we can’t send an ambulance immediately,” Jones said. “That was stressful until realizing no one was suffering.”
The decision by EMSA Medical Director Jeffrey Goodloe, M.D., with approval from the independent Medical Control Board, is not an option often implemented, said Jim Winham, EMSA director of Clinical Services.
“The snow was unprecedented,” Win-ham said. “We get an inch of snow and it shuts down the airport. We don’t have snowsuits. We don’t buy snowblowers for our driveways.”
Response was sent to higher-level calls and to patients with exceptional medical needs. For example, a multiple agency dialy-sis task force was created to coordinate the transportation of dialysis patients to treat-ment centers. EMSA dispatchers relayed the information between centers and crews and took meals to patients unable to return home from the dialysis center because of the snow.
Low-level calls were put on active standby and tracked. once the calltaker knew the call was a BRAVo or below, the call’s prior-ity was manually changed to stand-by status. The change in response required a standard dispatch statement, which Quality Improve-ment Supervisor Bryon Schultz quickly crafted: “Sir/Ma’am, due to the extreme
weather and impassable road conditions, we will not be able to respond to you at this time. We will be calling you back within 6 hours to check on you (the patient). If your (his/her) condition worsens in any way, call us back on 911.”
“This kept the call from being dispatched and allowed us to keep track with a running time for follow-up,” Schultz said.
A dispatcher dedicated to follow-up returned calls within six hours of initial con-tact. A change in patient status would deter-mine response; if no one answered the phone in a follow-up call, a field supervisor was sent to the home. BRAVo calls that did require a response—such as a fall outside causing hip pain—would override the standby-status and signal response.
Corbett answered a call from a woman who had fallen inside her home.
“She needed someone to help her up,” Corbett said. “She wasn’t hurt and said to send help when we had the time. She had her dog and the electricity was on. We got help there and she was oK.”
The public took the situation in stride, Center Supervisor Cathy Smith said.
“People were very good, very understand-ing,” she said. “We had few complaints. They knew what was going on outside. Roads were impassable. Emergency vehicles couldn’t get through to the neighborhoods. They under-stood if we couldn’t make it.”
MedStar in Fort Worth, Texas, experi-enced an unprecedented increase of 13% in call volume over the same time one year ago, according to MedStar Public Information Specialist Suzy Miller.
“It was unprecedented,” she said. “The severe weather of Super Storm 2011 and the influx of visitors to the area for Super Bowl 2011 combined made February super busy.”
MedStar, which typically responds to 320 calls each day, responded to more than 400 calls during several days in February. Call vol-ume jumped in every category and in some, much more than others. Fall-related calls were more than triple the average volume and pregnancy-related calls went up 145%. Breathing problems skyrocketed by 96% at
the height of the storm. Traffic accidents increased about 41%.
MedStar suspended lights-and-sirens response and did not transport patients outside the organization’s service area dur-ing four days of snow, icy roads, and frigid temperatures. Dispatchers unable to make it home stayed in local hotels.
MedStar Communications Supervisor Melissa Allen spent most of her time in the center when the weather was at its worst.
“We knew the storm was coming and it was as bad as they said it was going to be,” she said. “It slammed us all at once.”
no place like homeonondaga County in New york is
known for heavy, wet snowfall resulting from both the lake effect from Lake ontario and storms, called nor’easters, forming along the East Coast. Syracuse, the county seat and only city in onondaga County, averages 121.2 inches of snow per year and the metro area receives more snow on aver-age than any other large city in
the United States.Winter 2011 dumped about 52 inches
above average snowfall, which is nearly 20 inches below the record set in 1992–1993.
“We’re used to the snow,” said Chuck Combs, supervisor—Training Division for the onondaga County 9-1-1 Center in Syracuse. “During a major storm, our calls generally increase, but they’re usually relevant to the day and time. We do get a lot of calls concern-ing quality of life and reduced utilities.”
When forecasts call for a particularly nasty storm, extra food is brought in to cover increased staffing requirements. Back-up operations are activated and dispatchers are briefed on affected areas or services and directed to ask additional questions to assist in prioritizing response due to restricted travel. on the rare occasion staff can’t make it home, space available in the communica-tions center and nearby fire stations offer additional shelter. Five hospitals in the Syra-cuse area are short trips even on bad days.
The potential of annual snowfalls exceed-ing the height of a 10-story building is exactly the reason Allen lives in the southern United States.
“We’re from Texas,” she said. “We don’t do the sled thing. The White Christmas in 2010 is memorable, but not the ice and freezing cold that lasted much longer than we expected.” g
“We’re from Texas. We don't do the sled thing.” —Melissa Allen

30 THE JOURNAL | emergencydispatch.org
g PoLiCe Cde g UniVersaL Cde
OnTrack
An emergency ser vices dispatcher must consider many factors when mak-ing decisions regarding the most appropri-ate response, and when the call involves imminent danger to life or property the highest level of public safety services must come into play.
But what happens when the person calling is in a dangerous situation? Maybe gunshots have been fired, or the caller is reporting that the suspect is in the area where a bank robbery just occurred. Perhaps, there is a burglary in progress and the caller is hiding. Take, for example, the following call
that came into the Hialeah, Fla., communica-tions center.
Just after 1 p.m. on Monday, Feb. 21, 2011, Cynthia Valdez grabbed a phone and hid in a closet to call 9-1-1 when she heard two men breaking into the family home.
“There's somebody, there's a guy—I'm home alone. Please, send me somebody here quick," she told the operator.
As officers rushed to the scene, Val-dez stayed in the closet. Before the rob-bers could get to her, officers arrived and arrested both men.
Valdez was nervous when making the call, and understandably so. A caller’s ability to give information in the face of approach-ing danger is as varied as the circumstances.
For example, the caller may be unable to respond because of proximity, or the caller might be in a state of panic and may not even be sure of his or her location. The caller may be too overwhelmed to relay accurate infor-mation and too frightened to move from a perceived place of safety.
The calltaker, however, needs the caller’s help; the key to an appropriate response is accurate information from the caller. Police officers need as much information as pos-sible prior to arriving on scene in order to take necessary resources and other precau-tions. once they arrive, it will be their job to assess the potential danger to themselves and the public and cordon off the area to prevent people from leaving the scene. While
Caller In Danger Dispatcher in unique position to help
g POLiCeCde
By Jaci Fox
THE JOURNAL | May/June 2011 31
responders are en route, however, preserving the caller’s safety is also of great importance.
The incident can become a three-ring circus.So, what can a calltaker do to protect the
caller and bystanders while, also, securing the scene for the arrival of law enforcement?
That’s where the Police Priority Dispatch System™ (PPDS™) comes in. The protocol is an essential element in an emergency com-munications center, providing the tools essential to proper interrogation and, con-sequently, scene safety. Asking the right questions at the right time protects the responders while also safeguarding the caller.
Protocol C: Caller in dangerThe CID Protocol is a pathway of ques-
tions and instructions designed to lead the caller to safety while asking “yes” or “No” questions the caller may be able to answer inconspicuously. The caller’s responses provide responders the necessary details to formulate an appropriate response without putting the caller in further jeopardy. These instructions and questions are specifically designed to address the needs of the caller and must be read in the order presented and exactly as written.
Twenty of the PPDS Chief Complaint Protocols SHUNT directly to Protocol C: Caller in Danger when the caller answers “yes” to the Key Question, “Are you in imme-diate danger?” The CID Protocol may also be used at any time during Key Questions, as the caller moves in or out of the “danger zone.” The instructions are designed to be used similarly to any Pre-Arrival Instruction (PAI). Because of the volatile and unpredict-able nature of crime scenes, the calltaker might provide CID instructions to the caller several times over the course of interrogation.
Above all else, ensuring and maintain-ing safety is the primary concern in police call processing.
immediate dangerAs the Caller in Danger Rules on Case
Entry explain, the CID Protocol is used after dispatch has been initiated or when circumstances or caller statements indicate that the caller is in immediate danger unless the caller is reporting:
• Protocol108:BombFound/Suspi-cious Package (Letter, Item)
• Protocol109:Bomb/CBRNThreat• Protocol 121: Mental Disorder
(Behavioral Problems)—suspect caller • Protocol 127: Suicidal Person/
Attempted Suicide – suspect caller
Callers reporting those situations are never considered to be safe and out of dan-ger and shunting to another protocol could delay call processing. Caller safety for these incidents is best addressed on the appropri-ate Chief Complaint Protocol.
If the caller does not know if the situa-tion presents immediate danger, the calltaker should begin Caller in Danger instructions/questions to preserve scene safety where any doubt exists. This simple precaution can be done easily since the calltaker can move quickly and seamlessly in and out of the CID Protocol during the interrogation process. Case Entry Rule 7 allows for this slight detour in the protocol pathway, as the calltaker will suspend questioning in order to give necessary instructions for patient/vic-tim safety or care, returning to the question sequence when possible.
Getting to safetyIn almost all cases, it is necessary to dis-
patch law enforcement prior to giving CID instructions on Protocol C. The CID path-way is designed to lead the caller to safety or to provide safety at the caller’s current location since the conditions on scene may prohibit movement. From the information provided in this protocol, the caller may be directed to any among these alternatives:
Go to a safe locationIf the caller is unable to take the phone
in the escape (e.g., calls from a landline), he or she will be instructed to call back from a safe location (if possible); if he or she is not able to call back from that location, Panel 3 instructs to “Make yourself known to the police officers when they arrive.”
stay on the line with the calltaker (caller in safe place)
After determining that the caller is in a safe place and can speak freely with the calltaker (the pathway of Panels 1, 2, and 3), the calltaker will return to the Key Question sequence at the point where the interroga-tion started.
stay on the line with the calltaker (caller cannot speak freely)
The calltaker may determine (through Panels 1, 2, and 4) that the caller is unable to speak freely and, subsequently, may only answer the calltaker’s questions with either single-word responses such as “yes” or “No” or, if the caller is restrained not to speak, the calltaker might ask the caller to tap a
response on the phone—e.g., tapping one time for “yes” and two times for “No” as sug-gested in Panel 6.
If a simple verbal response or tapping is possible, the calltaker resumes the Key Ques-tion sequence to gather the required informa-tion for responding crews.
In some cases, the caller may also be asked to make the call sound like a casual conversa-tion between two friends to quell suspicions when the suspect is within earshot.
If any type of response is impossible, the calltaker remains on the line with the caller and provides instructions to “Stay on the line with me as long as you can. If you need to leave, don’t hang up, just put the phone down.”
Post-dispatch instructionsAfter completing the Key Questions, the
calltaker will provide Post-Dispatch Instruc-tions (PDIs). The calltaker must give the PDIs from the specific Chief Complaint Protocol and may also give the caller any of nine CID Post-Dispatch Instructions when possible and appropriate:
a) If you think you can leave safely, get away and call us from somewhere safe.
b) If the person is nearby and you are unable to leave safely, keep very quiet and stay out of sight.
c) Do not put yourself in any (more) danger.
d) Try to avoid any contact with her/him.
e) Lock your doors and windows.f) If the person returns, do not let her/
him in and tell me immediately.g) If the person leaves the scene, tell me
immediately.h) If you need to talk to her/him, speak
softly and calmly. Do not upset her/him.
i) If it is safe to do so, observe her/him continuously.
Lastly, while waiting for the police to arrive, the calltaker may use the Case Exit Stay on the Line instructions, assuring the caller: “An officer will be dispatched as soon as possible.” The calltaker may be in a posi-tion to tell the caller when officers have arrived, rather than the caller telling the calltaker when this happens. In either case, it is acceptable for the calltaker to alter the wording in Case Exit to accommodate the particular situation, if needed. g

32 THE JOURNAL | emergencydispatch.org
CDE Quiz Mail-In Answer SheetAnswer the test questions on this form. (A photocopied answer sheet is acceptable, but your answers must be original. We Will not process altered sizes.)
A CDE acknowledgement will be sent to you. (You must answer 8 of the 10 questions correctly to receive credit.)
clip and mail your completed answer sheet along with the $5 non-reFUndaBle processing fee to:
The National Academies of Emergency Dispatch139 East South Temple, Suite 200Salt Lake City, UT 84111 USA (800) 960-6236 US; (801) 359-6916 Intl. Attn: CDE Processing
Please retain your CDE acknowledgement for future reference.
Name _________________________________
Organization ____________________________
Address _______________________________
City________________St./Prov. ____________
Country__________________ZIP ___________
Academy Cert. # ________________________
Daytime Phone ( ) ___________________
E-mail: _________________________________
primary FUnction
Public Safety Dispatcher (check all that apply)
_____Medical _____Fire _____Police
Paramedic/EMT/Firefighter
Comm. Center Supervisor/Manager
Training/QI Coordinator
Instructor
Comm. Center Director/Chief
Medical Director
Commercial Vendor/Consultant
Other
ANSWER SHEET ? POLICEMay/June Journal 2011 vOl. 13 NO. 3 (Caller in Danger ) Please mark your answers in the appropriate box below.
1. o A o B
2. o A o B o C o D
3. o A o B o C o D
4. o A o B o C o D
5. o A o B o C o D
6. o A o B
7. o A o B o C o D
8. o A o B o C o D
9. o A o B
10. o A o B
CDE-Quiz Police Answers to the CDE quiz are found in the article “Caller in Danger,” which starts on page 30. Take this quiz for 1.0 CDE unit.
1. The Caller in Danger Protocol provides a series of “yes” and “No” questions without any instructions for the caller.
a. trueb. false
2. The questions and instructions on Protocol C: Caller in Danger:
a. are specifically designed to address the needs of the caller. b. must be read in the order they are presented.c. must be read as written.d. all of the above
3. The Caller in Danger Protocol is:
a. designed to be used similarly to any other PAi.b. different from any other PAi.c. can be used more than once in the duration of a single call.d. a and c
4. What is the primary concern in police call processing?
a. getting the best informationb. ensuring and maintaining safetyc. sending the right units at the right timed. navigating correctly through the protocol
5. Certain Chief Complaint Protocols do not link to the CiD Protocol because their potential safety issues are best addressed on the original protocol. Which is NOT an example of this?
a. Protocol 127: Suicidal Person/Attempted Suicideb. Protocol 121: Mental Disorder (Behavioral Problems)c. Protocol 109: Bomb/CBrN Threatd. Protocol 101: Abduction (Kidnapping)/Custodial Abduction/hostage Situation
6. if a caller does not know if the situation presents immediate danger, the calltaker does not need to go to the Caller in Danger Protocol.
a. true b. false
7. Which rule instructs the calltaker to suspend interrogation in order to give instructions pertaining to patient/victim safety or care?
a. rule 1 on Protocol 113b. Case Entry rule 7 c. Case Entry rule 2d. Caller in Danger rules
8. Which of the following statements is NOT found in the CiD Post-Dispatch instructions?
a. if the person is nearby and you are unable to leave safely, keep very quiet and stay out of sight.b. if it is safe to do so, observe her/him continuously.c. Don’t disturb anything at the scene, including weapons, tools, or objects found nearby.d. Do not put yourself in any (more) danger.
9. The calltaker may use the Case Exit Stay on the line instructions.
a. trueb. false
10. in Case Exit, it is acceptable to alter the wording to accommodate the situation, if needed.
a. true b. false
$
Expires 06/30/12
YOU MUST BE POLICE CERTIFIED TO TAKE THIS QUIZ.
To be considered for CDE credit, this answer sheet must be received no later than 06/30/12. A passing score is worth 1.0 CDE unit toward fulfillment of the Academy’s CDE requirements. Please mark your responses on the answer sheet located at right and mail it in with your processing fee to receive credit. Please retain your CDE letter for future reference.

THE JOURNAL | May/June 2011 33
The purpose of this CDE article is to provide the reader with a better under-st anding of some of the key st atisti -cal terminologies used in the scientific manuscript entitled “Public Expecta-tions of Receiving Telephone Pre-Arrival Instructions from Emergency Medical Dispatchers at 3 Decades Post origination at First Scripted Site” (see page 34-39). The authors of the manuscript have put together simple but precise definitions to terms relevant to this study.
Understanding scientific studies comes from continuing to read a lot of studies. Scientific studies are valuable educational resources for everyone and as this study hopefully shows, anyone can understand and enjoy them.
research terminology 101Hypothesis
The hypothesis is the assumption to be proven in a study. For example, in an experi-ment to test the effect of a (new) drug, a hypothesis would be that the new drug has the predicted effect.
VariableA variable is anything that we measure in
an experiment or study. It is any parameter that is likely to change —meaning it can take on different values at different points during the time of a study. Weather, blood pressure, patient weight, and protocol compliance are examples of common variables.Mean
Mean is basically the average of a set of data. For example, the mean or average age of students in a class would be the sum of all the ages of the students in the class divided by the total number of students in the class.
Median Median is the middle value in a set of
data. For example, if we arrange the ages of students in a class from the youngest to the oldest and pick the age of the student in the middle, we have a median value.
p-value The p-value indicates how likely the
result obtained in a statistical test is due to chance rather than a true difference between
two study groups. In this study, the p-value is used to show whether or not a statistically significant difference exists between two study groups. A p-value ranges from 0 to 1. The lower the p-value, the less chance has to do with it. In this study, the p-value equal to or less than (≤) 0.05 indicates that the results are valid (a statistically significant difference exists). When the p-value is greater than (>) 0.05, the results are probably due to chance (no significant statistical difference).
odds ratioThe odds ratio is a way of comparing
whether the probability of a certain event is the same for two groups. More specifically, the odds ratio is a ratio of two probabilities and it describes the strength of a relationship between the two variables. The "odds" of an event is the ratio of the chance of the event occurring, to the chance of it not occur-ring. For example, in healthcare, the odds ratio could be used as a statistical measure of the likelihood of developing bird flu if exposed to a sick bird. Therefore, the odds ratio is the odds of developing bird flu in the group exposed to a sick bird divided by the odds of developing bird flu in the unexposed group. An odds ratio of 1 demonstrates that it is equally likely for both groups to develop bird flu. on the other hand, an odds ratio greater than one (>1) implies that develop-ing bird flu is more likely to occur in the group exposed to a sick bird, than in the unexposed group. An odds ratio less than one (<1) implies that developing bird flu is more likely to occur in the unexposed group.
95% Confidence intervalThe 95% Confidence Interval (CI) implies
that there is 95% chance or probability that the calculated range of values will contain the true value. Therefore, the CI is not a probabil-ity—it’s a range of numbers. The less variation between the limits of the range in the CI, the more accurate the estimated value is. For example, we independently draw two sample groups of 50 people each from all the NAED staff to estimate the overall mean (average) age of all NAED staff. Suppose the first sample of 50 staff members gives us a mean age of 35.2 years, 95% CI: 33 -36, and the second sample also gives a mean age of 35.2, 95% CI: 28 -40. These results imply that the mean age obtained using the first sample is more accurate than the one found using the second sample. This is because the 95% CI is narrower in the first sample (33-36) than the second sample (28-40). g
The CDE Article: Understanding Research Studies
Scientific studies are valuable educational resources for everyone.
g UniVersaLCde

34 THE JOURNAL | emergencydispatch.org
Public Expectations of receiving Telephone Pre-Arrival Instructions from Emergency Medical Dispatchers at 3 Decades Post Origination at First Scripted Site Amelia Clawson1, Pamela Stewart1, Christopher Olola PhD1, Scott Freitag2, Jeff Clawson MD1
1International Academies of Emergency Dispatch, Salt Lake City, Utah, USA29-1-1 Communication Center, Salt Lake City Fire Department, Salt Lake City, Utah, USA
abstractIntroduction: Dispatcher-provided tele-
phone pre-arrival instructions (PAIs) date back over 3 decades in the United States of America. In 1979, the Salt Lake City Fire Department began providing Medical Pri-ority Dispatch System™ (MPDS®) protocol-driven PAIs for every MPDS chief complaint – including airway management, cardio-pulmonary resuscitation (CPR), Heimlich maneuver, and childbirth situations. There-fore, with 3 decades of experience with scripted PAIs, Salt Lake City is a prime site for studying public expectations of receiving PAIs when calling 9-1-1. The authors hypoth-esized that the North American public has strong expectations of receiving telephone CPR and Heimlich maneuver PAIs and are likely to accept transfer to phone-advice pro-fessionals when dispatchers determine that their medical problem is non-emergent.
Objective: To assess public expectations of receiving telephone PAIs from 9-1-1 Emergency Medical Dispatchers (EMDs), 3 decades after introduction.
Methods: The survey involved a ran-dom selection of Salt Lake City residents in September 2007. The questionnaires and response cards (in English language) were mailed to a convenience sample of 2,000 respondents to complete. The survey responses were presented and the expecta-tions of receiving PAIs assessed. Evaluation of the association between demographics and PAI expectations was performed, adjusting for PAI type. The difference between CPR and Heimlich maneuver PAI expectations was also assessed, along with willingness of caller transfer to a phone-advice professional when a medical problem is non-emergent.
Results: Two hundred and seventy (270) survey questionnaires were com-pleted and returned (10.4%) showing ove ra l l , t h a t 8 8 . 7 % ( 9 5 % C I : 8 3 . 3 % ,
92.8%) of citizen respondents expect PAIs from EMDs. The expectation of receiving PAIs was significantly associ-ated with female callers (oR (95%CI): 3.05 (1.21, 7.65), p = 0.022). Citizens age 15 to 45 years were significantly less likely to accept transfer to a phone-advice nurse than other age groups combined (p = 0.033). Though not statistically sig-nificant, citizens age 60 to 75 years were 4 times more likely to expect to receive CPR PAIs from EMDs, twice more likely to expect to receive Heimlich maneuver PAIs or accept transfer to a phone advice nurse. Household income was not signifi-cantly associated with PAI expectations or transfer to a phone-advice nurse.
Conclusions: The public has high expec-tations of receiving life-saving PAIs from EMDs. Females have higher expectations of receiving CPR or Heimlich maneuver advice. In the future, with well constructed, scripted telephone instructions in EMD protocols, we expect similar public acceptance of a wider range of enhanced telephone-directed patient evaluations, advice, and care.
Keywords: Pre-Arrival Instructions Expectation, Emergency Medical Dispatch Protocol, Medical Priority Dispatch System, Emergency Medical Service, Emergency Medical Dispatcher, Cardiopulmonary Resuscitation, Heimlich Maneuver, Nurse Advice Transfer, Telephone Advice.
introductionThe history of dispatcher-provided tele-
phone pre-arrival instruction (PAIs) dates back over 3 decades in the United States. The first known recorded resuscitation-type phone instructions occurred in Phoenix, where an injured paramedic, assigned to the dispatch center, began providing occasional ad lib instructions for 9-1-1 calls in 1974.1 In 1979, the Salt Lake City Fire/Emergency
Medical Services Alarm office began pro-viding Medical Priority Dispatch System (MPDS) protocol-driven instructions for every one of the MPDS chief complaints – including airway management, CPR, Heim-lich maneuver, and childbirth situations.2
Cardiac ar rest (CA) is one of the leading causes of mor tality in Nor th America and the overall survival rate for out-of-hospital CA falls below 5%.3 Increased survival has been associated with bystander cardiopulmonary resusci-tation (CPR).4 Several community train-ing methods have been used in the past to improve bystander CPR.5-25 Lately, lack of community interest and motivation pose a great challenge, although dispatch-assisted CPR PAIs have been shown to enhance bystander CPR rates.26 For many years, Emergency medical dispatchers (EMDs) have also assisted 9-1-1 callers through telephone PAIs to effectively per-form the Heimlich maneuver procedure. This procedure, which involves abdomi-nal thrusts was introduced in 1974 to save lives of choking victims.27
Public awareness and expectation of receiving telephone-directed help, virtually non-existent in the 1970s, began to grow in the 1980s, and got sporadic regional aware-ness whenever a dramatic “emergency dis-patcher saves a life” story was covered in the news, radio, or television media.
In 1989, the Columbia Broadcasting System (CBS) primetime television show “RESCUE 911”28 was broadcast to millions of Americans and Canadians, as well as to citizens of 45 other countries, highlighting the importance of the dispatch role of 9-1-1 service in every case portrayed in the 7-year series. It remained in re-runs until 2005.
By 1990, it is estimated that hundreds of centers in North America had some type of protocol and/or training to provide such

THE JOURNAL | May/June 2011 35
telephone help. Whether they actually did or not, and to what extent, remains unknown. The extent of the public’s expectations of receiving PAIs has only been the subject of one study to date, in the Rochester, New york area in 2000. Billittier et al.29 reported in their study that knowing how to “dial 9-1-1 or 9-11” numbers significantly predicted the lay public’s expectation of receiving PAIs and that the public expected to receive PAIs when they make such calls. They recorded an average expectation rate of receiving advice of 76% (95% CI: 73%, 80%) for all of the four following medical conditions: 88% (95% CI: 85%, 90%) for choking, 87% (95% CI: 84%, 90%) for not breathing, 89% (95% CI: 86%, 91%) for bleeding, and 88% (95% CI: 86%, 91%) for childbirth.
In several states in Australia, country-wide in the UK, and in a few Emergency Medical Systems (EMS) in North America, EMDs utilize special protocols to transfer the caller to EMS-approved healthcare entities, once it has been determined that a patient’s
medical problem is not urgent and non-life threatening. This transfer is based on medi-cally approved pre-set, low acuity codes. The call may be transferred to a phone-advice nurse or other professional non-emergency care source, such as Rape Crisis Centers or Mental Health Help Lines for further evalu-ation and care or, in some cases, return to the 9-1-1/EMS system for a mobile response. This method significantly optimizes the uti-lization of dispatch resources.30-32
The authors hypothesized that the North American public today has strong expectations of receiving telephone CPR and Heimlich maneuver pre-arrival instructions when they call 9-1-1 and are also likely to accept transfer to phone-advice professionals when EMDs determine that their problem is not a medical emergency.
MethodsSalt Lake City, the birthplace of scripted
PAIs, is a prime example for studying pub-lic expectations of receiving PAIs. The study was based on a mail-in survey conducted in
September 2007. In collaboration with the Salt Lake City Fire Department, a citizen survey questionnaire, instruction sheet, and a postage-paid return response card (Figure 1) were constructed and printed in English. Using the 2007 Salt Lake City phone book, a participant selection was accomplished by selecting every 5th name on each 5th page of the book. These addresses were vetted against a zip code map from the phone book while comparing each with a digital internet source33 to identify actual resident areas within the city limits. All non-Salt Lake City addresses were excluded from the study sample. Survey questionnaires were then sent out via first class US mail in September 2007, to a convenience sample of 2,000 residents in Salt Lake City. There was no formal consenting process, but consent was assumed with the return of a completed survey response card. The respondents were requested to anonymously complete and mail back their responses in the pre-paid survey response envelopes.
Figure 1: National Academy of Emergency Dispatch/Salt Lake City Fire Department 9-1-1 questionnaire and answer card – 2007.

36 THE JOURNAL | emergencydispatch.org
Data AnalysisA web interface with a report gen-
eration component was created for data entry. Initial descriptive (frequencies and averages) statistics were generated upon the completion of data entry. Intercooled STATA for Windows® software (STATA Statistical Software: Release 9 ©2007, StataCorp, College Station, TX, USA) was used for detailed data analysis.
odds ratio (oR) with 95% confidence intervals (CIs) and p-values were used to assess associations between study groups, at 0.05 significance level. The study responses were analyzed, while categoriz-ing by the citizen’s gender, age, and type of PAI. The next analyses evaluated asso-ciation between the citizen’s expectations of receiving PAIs and their age, and gen-der. The association between gender, age, household income, and PAIs expectation was also evaluated, while adjusting for the type of PAI. Finally, the difference between the level of the public’s PAIs expectation to receive CPR and Heimlich maneuver instructions was assessed, as well as the level of acceptance of transfer to a nurse when their problem was non-emergent.
resultsTwo-hundred and seven (10.4%) citi-
zens participated in the survey. Based on this sample, Salt Lake City citizens expect to receive PAIs from EMDs to help them in the life-threatening emergencies of cardiac
arrest and choking (Table 1), confirmed by an average expectation rate of 88.7% (95%CI: 83.3%, 92.8%). They were also willing to accept transfer to phone-advice professionals when EMDs determined that their medical problem was non-emergent (88.5% (95%CI: 82.8%, 92.8%)).
The level of public expectation of receiving PAIs from EMDs was significantly associated with female callers (Table 2). However, age was not significantly associated with the likelihood of expecting to receive PAIs from EMDs.
Citizens age 15 to 45 years were the only group that was significantly less likely than all the other age groups com-bined to accept to be transferred to a
phone-advice professional (p = 0.033) (Table 3). Though not statistically signifi-cant, citizens age 60 to 75 years were four times more likely to expect to receive PAIs from EMDs to help them perform CPR, and twice as likely to expect to receive PAIs from EMDs to either help them do the Heimlich maneuver or to accept trans-fer to phone-advice professionals for non-emergent situations. In addition, female citizens were three times more likely than males to expect to receive PAIs from EMDs to help them do CPR or the Heim-lich maneuver, but were less likely (odds reduced by about 46%) to accept transfer to phone-advice professionals. All the dif-ferences found, however, were not statisti-cally significant.
There was no significant difference in PAI expectation for CPR between citizens living in households with incomes higher than the overall median income ($41,864) than for those who earned less. However, citizens who had higher incomes than the overall median income had slightly higher odds of expecting PAIs for CPR. A similar pattern was observed in the citizens who accepted transfers to phone-advice profes-sionals. on the other hand, although not a statistically significant difference, those living in households with income less than the overall income had a high expectation of receiving PAIs from EMDs to help them do the Heimlich maneuver.
There was no significant difference in the expectation of receiving CPR and Heimlich maneuver PAIs (91.2% each) (Table 4).
Table 4: Comparison of public expecta-tions of receiving CPR or Heimlich Maneu-ver PAIs from EMDs.
Survey Questions Responses Measure n (%)
Gender Male 91 (44.2)
Female 115 (5 5.8)
Age (years) 15- 45 59 (28.9)
45- 60 56 (27.4)
60- 75 45 (22.1)
>75 44 (21.6)
Yes 166 (81.4 )
No 16 (7.8)
Don’t know 22 (10.8)
Yes 175 (86.2)
No 17 (8.4)
Don’t know 11 (5.4)
Yes 154 (75.5)
No 20 (9.8)
Don’t know 30 (14.7)
If someone you know collapsed in front of you and their heart had stopped, would you expect the 9-1-1 dispatcher to tell you how to do CPR to help them?
If someone you know was choking to death in front of you, would you expect the 9-1-1 dispatcher to tell you how to do the Heimlich maneuver to help them?
If the 9-1-1 dispatcher determined that your medical problem was not an emergency, and recommended transfer-ring you to a phone advice nurse for further evaluation and care, would that be okay with you?
CPR = Cardiopulmonary resuscitation
table 1: Profile of citizen responses categorized by gender, age, and type of PAI.
Measure n Pre-Arrival Instructions (PAIs)
p* Yes: n (%) No: n (%)
Age (years) Continuous 192 170 (57.1±18.2)† 22 (56.6±18.3)
† 0.901‡
15- 45 56 50 (89.3) 6 (10.7)
0.335§
45- 60 55 47 (85.5) 8 (14.5) 60- 75 43 41 (95.3) 2 (4.7) >75 38 32 (84.2) 6 (15.8)
Gender Female 108 101 (93.5) 7 (6.5) Male 86 71 (82.6) 15 (17.4) 0.022
*Two-sided Fisher’s Exact test p-value, unless otherwise stated. †n(mean ± standard deviation). ‡Two-sided Student t-test p-value for testing the difference in the mean age (with unequal variance) between the two levels of the citizen’s expectation to receive PAIs from EMDs. The PAIs exclude transfers to advice nurse for non-emergent cases. §Trend analysis p-value (Fisher’s Exact). Female citizens were three times more likely to expect to receive PAIs from EMDs than males (oR (95%CI): 3.05 (1.21, 7.65), p = 0.022).
table 2: Association between public expectation of receiving PAIs from EMDs by age and gender.

THE JOURNAL | May/June 2011 37
discussionAfter 3 decades of PAI availability locally
and exposure nationally, over 91% of Salt Lake City citizens responding to this survey expect to receive this elevated level of tele-phone help. A significant public expectation obviously exists, therefore a public safety standard of care and practice is no longer disputable here.
This study has further examined sev-eral variations within the social parameters affecting a citizens’ degree of expectation of receiving PAIs from EMDs. Such expec-tations differ significantly by gender, and slightly by age and median household income. Females had a significantly higher expectation of receiving CPR or Heimlich maneuver PAIs from EMDs, than their male counterparts. However, males with problems not deemed by the EMD to be an emergency were more likely to accept non-emergency transfer to phone-advice professionals than females. The responding citizens under 45 years of age and those over 60 had the highest expectation of receiving PAIs.
Nearly 90% of all citizens reported that, if their problem was determined not to be urgent, they were “okay” with being trans-ferred to phone-advice professionals for fur-ther advice. Within this group, citizens age 15 to 45 years were significantly less likely (odds reduced by 66%) to accept a transfer to phone-advice professionals when the 9-1-1 EMD determined that their medical prob-lem was not an emergency. Although not
statistically significant, citizens age 60 to 75 years were four times more likely to expect to receive CPR instructions and twice as likely to expect Heimlich maneuver choking relief instructions. Similarly, they were nearly twice as likely to accept transfer to phone-advice professionals.
Households with an income higher than Salt Lake City’s median level had high expectations of receiving CPR instructions and were likely to accept transfer to phone-advice professionals. on the other hand, the higher income households were less likely to expect Heimlich maneuver instructions (odds reduced by 24%). The differences in both these instances, however, were not sta-tistically significant, but certainly of interest. overall, there was no significant difference between the expectation of receiving CPR and Heimlich maneuver instructions, although both were quite high (91.2%).
The clinical effects of these levels of public expectation regarding PAIs are sev-eral and potentially wide reaching. A new standard of public safety telephone care and practice now clearly exists where it did not (and could not) 3 decades ago. These public expectations now likely include other aspects of 9-1-1 intervention in areas related to advice and direction by EMDs. Such aspects include the acceptance of improved interro-gation (questioning); the addition of more intricate instructions, such as the recent advent of phone instructions for high-risk childbirth situations (including breech birth,
shoulder dystocia, and cord presentation); as well as new phone procedures for stroke identification and agonal breathing detec-tion.34, 35 We believe that public acceptance of new and more complicated instructions can now be reasonably predicted.
In our opinion, the most unexpected result of the study was the high acceptance of being transferred to phone-advice profes-sionals when the problem was determined by the EMD as not being an emergency. That this expectation was reported by about 90% of respondents was most surprising, however, in today’s healthcare climate, it is not totally unexpected.
These findings support and build upon the earlier findings of Billittier et al.,29
reported 10 years ago, in a geographic area with significantly less history of receiving 9-1-1 telephone instructions.
other concerns that could potentially affect public expectations (for better or for worse) include publicized governmen-tal requirements, dispatcher liability, and PAI-related lawsuits. However, the public is likely not aware of the existence of stat-utes or EMS/EMD rules and regulations that establish a governmental standard of care for EMD training and protocol use, including PAI provision, in their area. The first process of this kind, started in Utah in 1982, resulted in State EMS regulations that required 9-1-1 centers to have an EMD protocol in place, including private ambulance companies or any ser-vice receiving emergency calls from the public. The mandating of an EMD pro-cess, as opposed to EMS and paramedic laws, rules, and regulations, has only very slowly spread within the US. Accord-ing to the International Academies of Emergency Dispatch® (IAEDTM) statis-tics, only 21 states have any statewide table 4: Profile of citizen responses categorized by gender, age, and type of PAI.
Measure
Cardiopulmonary Resuscitation (CPR) Heimlich Maneuver Phone Advice Nurse
n* PAIs: n (%)
OR (95%CI)† p‡ n* PAIs: n (%)
OR (95%CI)† p‡ n* Transfer: n (%)
OR (95%CI)† p‡
Male 80 69(86.3) 85 74 (87.1) 74 68 (91.9)
Female 102 97 (95.1) 3.09 (1.07, 8.91) 0.062 107 101 (94.4) 2.50 (0.91, 6.82) 0.123 100 86 (86.0) 0.54 (0.20, 1.44) 0.336
Age (years) 15-45 56 52 (92.9 1.38 (0.45, 4.25) 0.779 55 50 (90.9) 0.98 (0.34, 2.79) 1.000 49 39 (79.6) 0.34 (0.14, 0.86) 0.033
45-60 54 48 (88.9) 0.68 (0.24, 1.91) 0.568 55 48 (87.3) 0.55 (0.20, 1.48) 0.268 50 46 (92.0) 1.72 (0.57, 5.15) 0.439
60-75 38 37 (97.4) 4.34 (0.70, § ) 0.199 43 41 (95.4) 2.33 (0.57, §) 0.369 38 35 (92.1) 1.68 (0.49, 5.66) 0.571
>75 33 28 (84.9) 0.45 (0.15, 1.34) 0.176 37 34 (91.9) 1.14 (0.33, 3.90) 1.000 36 33 (91.7) 1.56 (0.46, 5.25) 0.770
Income# High 35 32 (91.4) 1.04 (0.30, 3.60) 1.000 37 33 (89.2) 0.76 (0.24, 2.35) 0.747 35 32 (91.4) 1.50 (0.44, 5.06) 0.768
Low 146 133 (91.1) 154 141 (91.6) 138 121 (87.7)
PAIs = Pre-Arrival Instructions from EMDs. *Excludes all the “I don’t know/not sure” responses (CPR: n=22, Heimlich maneuver: n=11, Phone advice nurse: n=30). †odds ratio and 95% confidence interval. ‡Two-sided Fisher’s Exact test p-value. §The upper limit of 95%CI was undeterminable. #Median household income (median; minimum-maximum: $41,864; $31,868 – $73,322); Low: household income is less than or equal to the overall median, High: household income is greater than the overall median). Source: 2005-2007 USA Census Bureau (http://factfinder.census.gov/home/saff/main.html?_lang=en).
table 3: Association between public expectation of receiving PAIs from EMDs for gender, age, and household income.
Citizen’s medical problem n* PAIs: n (%) OR (95%CI)† p‡
Cardiopulmonary resuscitation(CPR) 182 166 (91.21) 1.01 (0.50, 2.04) 1.000
Heimlich maneuver 192 175 (91.15)
PAIs = Pre-Arrival Instructions from EMDs. *Excludes all the “I don’t know/not sure” responses (CPR: n = 22 and Heimlich maneuver: n = 11). †odds ratio and 95% confidence interval. ‡Two-sided Fisher’s Exact test p-value.

38 THE JOURNAL | emergencydispatch.org
mandated EMD requirements. 36 Even this does not insure that PAIs are “always given when possible and appropriate” or given correctly.37 The fact that the pub-lic has such a high expectation of receiv-ing PAIs, establishes, in-and-of-itself, a clear standard of care. We also know that about 3,100 centers in the U.S. have, at one point, adopted these PAIs using some version of the MPDS.38 Model EMD Leg-islation and Model EMD Regulations and Standards documents36 have been pub-lished by the IAED, and have been used in several states and jurisdictions to set governmentally required standards of EMD care and practice.
Contrary to what is often assumed, there has never, to our knowledge, been an issue of legal liability in any interac-tion with the public during a 9-1-1 call in terms of the public’s acceptance of fol-lowing dispatcher-given PAIs. Historically, this assumption often came from within the reluctant-to-change public safety community itself, at times supported by ill-informed city or county attorneys. Rather it is the failure to provide PAIs, and not the public’s willingness to follow dispatcher-given PAIs that becomes a legal liability. Generally, when the lay public or elected officials are told that their com-munity is not providing PAIs, they com-ment, amazed, “ you mean we are not doing this already?” Frequently, the public is exposed to cases of failure to provide PAIs – for which the unofficial legal term is “dispatcher abandonment.” Public out-rage can be significant in communities bearing the brunt of high profile cases where failure to provide PAIs seems so blatant.39 Indeed, one mother started an organization called Parents Against Neg-ligent Dispatch Agencies (P.A.N.D.A.), after losing a twin daughter in a backyard drowning incident (the dispatch center provided no PAIs having been told by local authorities not to give telephone instructions for fear of liability).40 The issue of receiving PAIs becomes little more than common sense once the pub-lic is exposed to the idea. To date, there has never been a successful lawsuit that we are aware of, regarding the worldwide provision of medically approved PAIs. on the contrary, each legal case in this arena is related to the failure to advise. Such absence of any reported, publicly known error or legal case regarding the provision of telephone instructions by EMDs could
be assumed to be a contributing factor to the public’s acceptance and the public safety community’s support and expan-sion of telephone-provided care. Future investigation should concentrate on other areas of scripted telephone-provided care and advice, as well as how to best provide these verbal services in the proper format, context, and linguistic presentation. As a recent chief of the Salt Lake City Fire Department stated in a written order, “Failure to provide pre-arrival instruc-tions is not an option at City Fire.”
Study limitationsAlthough this survey was conducted in
Salt Lake City, which has used MPDS for over 3 decades, there is no guarantee that the same results could be applied to other communities. In addition, the sample size may have been too small to make valid con-clusions. However, Salt Lake City should pro-vide results consistent with other cities that have had PAIs consistently given by EMDs for a period of time significant enough to create similar expectations. Future studies in other locations are recommended to validate these findings. Lastly, a small but important number of citizens were still unsure of their expectations of receiving PAIs from 9-1-1 EMDs (CPR: 10.8%; Heimlich maneuver: 5.4%; and transfer to phone-advice profes-sionals: 14.7%). While we believe citizens’ expectations of receiving PAIs from EMDs reflect widespread current reality, interpre-tations of these results should be done with some caution.
ConclusionThe public in Salt Lake City clearly
expects to receive PAIs from EMDs when they call 9-1-1 and the level of expectations is significantly associated with female gen-der, but not with age. Females have higher expectation than males of receiving CPR or Heimlich instructions. Males are slightly more likely to accept transfer to phone-advice professionals when EMDs determined their medical problem to be “not an emergency”. Citizens in households with higher median income have a moderate level (i.e., odds ratio slightly more than 1.0) of expectation of receiving CPR PAIs, along with accept-ing transfer to phone-advice professionals for non-emergent medical conditions. In the future, with well constructed, scripted telephone instructions in EMD protocols, we can expect public acceptance of wider ranging and more comprehensive forms
of telephone-directed patient evaluations, advice, and care.
acknowledgmentsWe would like to acknowledge the deter-
mination and help of Lindsay Palmer, Natalie Baird, Jillian Cowley, and Joel Hales at the Cli-ent Services Division and Internal Software Applications Development Department of Priority Dispatch Corp. (PDC), for address-ing, mailing, receiving, sorting, and perform-ing data entry of all the survey responses. We thank Holly Mills at the Research & Standards Division of PDC for her input on the graphics for the figures presented in this manuscript. We also gratefully acknowledge the Salt Lake City Fire Department EMS Division and its dually (Medical and Fire) Accredited Center of Excellence Communications Center for their 30 years of support and effective dispatching, relevant advice, and help with this study.
Source of support: No specific funding was provided outside of the employment rela-tionships noted in the competing interests section below.
Contributors: AC, PS, JC and SF con-ceived the study design. All the authors sub-stantially participated in the implementation of the study and the acquisition of the data. Co validated the data and performed data analysis and interpretation. All the authors drafted and critically revised the article for important intellectual content, and finally approved of this version of the manuscript for submission to The Journal.
Conflict of Interest: JC is CEo and Medical Director of the Research and Standards Divi-sion of Priority Dispatch Corp. and member of the Council of Standards, and Board of Trustees of the International Academies of Emergency Dispatch. He is the inventor of the Medical Priority Dispatch Protocol and Quality Assurance System studied herein.
Ethical approval: The study was approved by the International Academy of Emergency Dispatch (IAED)’s Institutional Review Board (United State Department of Health and Human Services registration number: IRB00006450). g
references
1. Toon B. Life-impacting via telephone instructions. In: Jeff J. Clawson, Kate B. Dernocoeur, Benjamin Rose, eds. Principles of Emergency Medical Dispatch: 30 years of protocols (1979-2009). 4th ed. Salt Lake City, Utah: National Academy of Emer-gency Medical Dispatch; 2008; 1.10-1.11.
THE JOURNAL | May/June 2011 39
2. Clawson J. Dispatch priority training – Strengthening the weak link. JEMS. 1981; 6:23-36.
3. Rea TD, Eisenberg MS, Sinibaldi G, White RD. Incidence of EMS treated out-of-hospital cardiac arrest in the United States. Resuscitation. 2004;63:17-24.
4. Woollard M, Jones G. Post-dispatch and pre-arrival instructions – Wales’ experience. In: Jeff J. Clawson, Kate B. Dernocoeur, Benjamin Rose, eds. Prin-ciples of Emergency Medical Dispatch: 30 years of protocols (1979-2009. 4th ed. Salt Lake City, UT: National Acad-emy of Emergency Medical Dispatch; 2008: 8.8-8.9.
5. Larkin GL, Marco CA. Who knows CPR?: a national survey. Acad Emerg Med. 2001;8:434-5.
6. Fong yT, Anantharaman V, Lim SH, Leong KF, Pokkan G. Mass cardio-pulmonary resuscitation 99–survey results of a multi-organisational effort in public education in cardiopul-monary resuscitation. Resuscitation. 2001;49:201-5.
7. Pane GA , Salness KA. A sur vey o f p a r t i c i p a n t s i n a m a s s C P R training course. Ann Emerg Med. 1987;16:1112-6.
8. Pearn J, Dawson B, Leditschke F, Petrie G, Nixon J. Who accepts first aid training? Aust Fam Physician. 1980;9:602-5.
9. Eisenberg M, Damon S, Mandel L, Tewodros A, Meischke H, Beaupied E, Bennett J, Guildner C, Ewell C, Gor-don M. CPR instruction by videotape: results of a community project. Ann Emerg Med. 1995;25:198-202.
10. Alderman C. Emergency bystander life support training. Emerg Nurse. 1997;5:10-1.
11. Eisenberg MS, Bergner L, Hallstrom A. Cardiac resuscitation in the com-munity. Importance of rapid provi-sion and implications for program planning. JAMA. 1979;241:1905-7.
12. Standards and guidelines for Car-diopulmonary Resuscitation (CPR) and Emergency Cardiac Care (ECC). National Academy of Sciences — National Research Council. JAMA. 1986;255:2905-89.
13. Axelsson A, Thorén A, Holmberg S, Herlitz J. Attitudes of trained Swed-ish lay rescuers toward CPR perfor-mance in an emergency. A survey of
1012 recently trained CPR rescuers. Resuscitation. 2000;44:27-36.
14. Bahr J. CPR education in the commu-nity. Eur J Emerg Med. 1994;1:190-2.
15. Baskett PJ. Teaching the public car-diopulmonary resuscitation. Br J Hosp Med. 1992;48:447, 451.
16. Jackson RE, Swor RA. Who gets bystander cardiopulmonary resuscita-tion in a witnessed arrest? Acad Emerg Med. 1997;4:540-4.
17. Lie KG, Richardson M. Attitudes of health professionals toward cardio-pulmonary resuscitation training for family members of cardiac patients. Coron Health Care. 1999;3(2):91-8.
18. Chu KH, May CR, Clark MJ, Breeze KM. CPR training in households of patients with chest pain. Resuscitation. 2003;57:257-68.
20. Eisenburger P, Safar P. Life supporting first aid training of the public–review and recommendations. Resuscitation. 1999;41:3-18.
21. Mancini ME, Kaye W. Resuscitation training: a time for reassessment. J Cardiovasc Nurs. 1996;10:71-84.
22. American Academy of Pediatrics Com-mittee on School Health. Basic life support training school. Pediatrics. 1993;91:158-9.
23. DeMuth WE Jr, Saunders EF. Public education in emergency medical ser-vices. Pa Med. 1975;78:49-52.
24. Lyttle J. Mandatory CPR training for students may improve cardiac-arrest survival rate, MDs say. CMAJ. 1996;155:1172-4.
25. Laf fer ty C, Larsen PD, Gallet ly D . R e s u s c i t a t i o n t e a c h i n g i n New Zealand schools. N Z Med J. 2003;116:U582.
26. Vaillancourt C, Stiell IG, Wells GA. Understanding and improving low bystander CPR rates: a systematic review of the literature. CJEM. 2008 Jan;10(1):51-65.
27. Heimlich HJ, Patrick EA. The Heim-lich maneuver. Best technique for sav-ing any choking victim's life. Postgrad Med. 1990 May 1;87(6):38-48, 53.
28. Wikimedia Foundation, Inc. Res-cue 911. Wikipedia®. 2009. http://en.wikipedia.org/wiki/Rescue_911. Accessed on January 4, 2011.
29. Billittier AJ 4th, Lerner EB, Tucker W, Lee J. The lay public's expectations of prear-rival instructions when dialing 9-1-1. Pre-hosp Emerg Care. 2000 Jul-Sep;4(3):234-7.
30. Dale J, Williams S, Foster T, Higgins J, Snooks H, Crouch R, Hartley-Sharpe C, Glucksman E, George S. Safety of telephone consultation for "non-seri-ous" emergency ambulance service patients. Qual Saf Health Care. 2004 oct;13(5):363-73.
31. Dale J, Higgins J, Williams S, Foster T, Snooks H, Crouch R, Hartley-Sharpe C, Glucksman E, Hooper R, George S. Computer assisted assess-ment and advice for "non-serious" 999 ambulance service callers: the potentia l impact on ambulance d e s p a t c h . E m e r g M e d J . 2 0 0 3 Mar;20(2):178-83.
32. Casciato D. Richmond offers more than a ride to the hospital. Best Prac-tices. 2007 July; 10(7):73, 84.
33. John Coryat Systems. Zip Code Map Version 3.0. U.S Naviguide Co.© 1997-2009. http://maps.huge.info/zip.htm. Accessed on January 4, 2011.
34. Clawson J, olola C, Scott G, Heward A, Patterson B. Effect of a Medical Priority Dispatch System key ques-tion addition in the seizure/con-vulsion/fitting protocol to improve recognit ion of inef fect ive (ago-nal) breathing. Resuscitation. 2008 Nov;79(2):257-64.
35. Patterson B. Childbirth and delivery complications: Understanding ver-sions 11.2 PAIs. National Academies of Emergency Dispatch. 2005;7(2):9-16.
36. National Academies of Emergency Dispatch (NAED™). EMD Model Leg-islation and Model Rules and Regula-tions. 2008. National Academies of Emergency Dispatch © http://emer-gencydispatch.org/res_legislation.php. Accessed on January 4, 2011.
37. National Institutes of Health. Emer-gency Medical Dispatching: Rapid Identification and Treatment of Acute Myocardial Infarction. NIH Publica-tions. 1994; No.94.
38. The National Academy of Emergency Dispatch (NAED). The Medical Prior-ity Dispatch System™.
39. Hurtado F. EMD Risky Business? The risks associated with the failure to cor-rectly implement a formal emergency medical dispatch program. 9-1-1 Maga-zine. 2001 Sep/oct: pp 1-4.
40. Harrawood D, Shepler P, Gunder-son MR. Risky business. Why EMS needs risk management. JEMS. 1995 Jul;20(7):30-4.

40 THE JOURNAL | emergencydispatch.org
CDE Quiz Mail-In Answer SheetAnswer the test questions on this form. (A photocopied answer sheet is acceptable, but your answers must be original. We Will not process altered sizes.)
A CDE acknowledgement will be sent to you. (You must answer 8 of the 10 questions correctly to receive credit.)
clip and mail your completed answer sheet along with the $5 non-reFUndaBle processing fee to:
The National Academies of Emergency Dispatch139 East South Temple, Suite 200Salt Lake City, UT 84111 USA (800) 960-6236 US; (801) 359-6916 Intl. Attn: CDE Processing
Please retain your CDE acknowledgement for future reference.
Name _________________________________
Organization ____________________________
Address _______________________________
City________________St./Prov. ____________
Country__________________ZIP ___________
Academy Cert. # ________________________
Daytime Phone ( ) ___________________
E-mail: _________________________________
primary FUnction
Public Safety Dispatcher (check all that apply)
_____Medical _____Fire _____Police
Paramedic/EMT/Firefighter
Comm. Center Supervisor/Manager
Training/QI Coordinator
Instructor
Comm. Center Director/Chief
Medical Director
Commercial Vendor/Consultant
Other
ANSWER SHEETMay/June Journal 2011 vOl. 13 NO. 3 (research Studies) Please mark your answers in the appropriate box below.
1. o A o B
2. o A o B o C o D
3. o A o B
4. o A o B o C
5. o A o B o C o D
6. o A o B
7. o A o B
8. o A o B o C
9. o A o B
10. o A o B
CDE-Quiz Answers to the CDE quiz are found in the article “Understanding research Studies” which starts on page 33. Take this quiz for 1.0 CDE unit.
1. The study used a mail-in survey questionnaire and response card to collect research data?
a) trueb) false
2. What was the hypothesis of the study?
a) to determine whether CPr PAis or heimlich PAis are more important to the publicb) cardiac arrest is one of the leading causes of mortality in North Americac) the North American public has strong expectations of receiving telephone CPr and heimlich maneuver PAis when they call 9-1-1 and are also likely to accept transfer to phone-advice profes- sionals for non-emergent problemsd) citizens in Salt lake City have more expectations of receiving PAis because Salt lake City is the birthplace of PAis
3. if the odds ratio is greater than (>)1, is it more likely that the group exposed to a sick bird will develop bird flu compared to the unexposed group.
a) trueb) false
4. What percent of All citizens who responded in this study were “okay” with being transferred to a phone-advice professional if their problem was determined not to be urgent?
a) less than 25%b) about 76%c) nearly 90%
5. Out of the 2,000 surveys mailed out, how many were completed and returned?
a) 10.4%b) 18.6%c) 32.7%d) 51.0%
6. One of the main findings in the study was that the public in Salt lake City clearly expects to receive PAis from EMDs when they call 911.
a) trueb) false
7. The authors predict that the results of this study can effectively be applied to other communities other than Salt lake City.
a) trueb) false
8. What would be the median age of 5 brothers ages 8, 19, 12, 21, and 15?
a) 75b) 15c) 21
9. A p-value greater than (>) 0.05 shows compelling evidence that the results are valid and not by chance.
a) trueb) false
10. Protocol compliance is an example of a variable.
a) trueb) false
$
Expires 06/30/12
YOU MUST BE CERTIFIED TO TAKE THIS QUIZ.
To be considered for CDE credit, this answer sheet must be received no later than 06/30/12. A passing score is worth 1.0 CDE unit toward fulfillment of the Academy’s CDE requirements. Please mark your responses on the answer sheet located at right and mail it in with your processing fee to receive credit. Please retain your CDE letter for future reference.

THE JOURNAL | May/June 2011 41

42 THE JOURNAL | emergencydispatch.org
g storK stories
YourSpace
For better or worse, the social net-work Facebook is credited for rekindling friendships.
And in the case of the Padilla/Sando-val family in Watsonville, N.M., Facebook proved a winner. The reconnect came through a birth announcement Santa Cruz Regional Dispatcher Abby Hernandez posted the day after Mirtha Padilla literally wel-comed her second child into their home.
Hernandez didn’t include the baby’s name but wanted to let others know about the awesome experience.
“I was on Cloud 9,” Hernandez said. “It was such an emotional moment when I heard the baby cry. Tears came down my face. This was so different than the bad things we usually hear.”
The brief announcement caught the attention of Mirtha’s brother omar Padilla; he is one of Hernandez’s Facebook friends. Mirtha and Hernandez’s sister Judy were best friends in grade school and high school. omar knew that his sister had delivered a baby at the same time on the same day with the aid of a 9-1-1 dispatcher.
omar responded. Was this irony or coin-cidence? They corresponded. The baby was his nephew.
“What’s the chance of that happening?” Hernandez said. “Judy hadn’t talked to Mirtha since high school.”
Hernandez sent a congratulatory teddy bear to the hospital. She and Mirtha talked
on the phone. Three weeks later, Diego vis-ited the communications center, along with his parents and sister Azucena, who slept through her brother’s delivery.
Mirtha said the first visit would not be their last.
“We definitely plan to stay in touch,” she said.Hernandez said she was happy to be
there on the phone, giving instructions and encouragement.
“This was an honor,” she said. “His birth was a big deal for all of us; it was the highlight of every dispatcher’s day. We do make a dif-ference for people.”
Diego Angel was born a little after 11 p.m. on March 8 when contractions com-ing every five minutes indicated a delivery earlier than the March 14 due date. Mirtha wanted a quick shower, figuring there would be ample wiggle room to freshen up before leaving on the 25-minute drive to Sutter Hospital in Santa Cruz.
That wasn’t going to happen. Her water broke.“I had an urge to push,” Padilla said.Sandoval called 9-1-1, but hung up before
anyone answered. Hernandez called back. She convinced the couple now was not the time to leave the house. Although her first baby deliv-ery in nine years at dispatch, she was confident that the Medical Priority Dispatch System™ (MPDS®) Pre-Arrival Instructions for child-birth and delivery would work in their favor.
Padilla agreed to put delivery in the hands of Sandoval.
Hernandez initiated instructions. Diego arrived moments before the ambulance, but just in time for Police officer Corey Johnston to arrive and rub the baby’s chest to stimu-late breathing. Sandoval used dental floss—the only string he could find—to tie off the umbilical cord.
“The nurses got a kick out of that,” Hernan-dez said. “They had never seen that before.” g
Long days of summer turning to long nights of winter means it’s time once again to run the delightful deluge of baby stories coming to us from our dispatcher centers.
After months of patient waiting for baby to be born, delivery for these families took an unexpected course inside vehicles, in the bathrooms and bedrooms of homes, and even a rest stop along a busy highway. The event was particularly startling for those unaware of a baby’s growing presence over the past nine months or, perhaps, the baby’s momentary persistence defying the doctor’s due dates.
Fortunately, an EMD was just a three-digit call away.
Deliveries that didn’t begin on the best note, ended in harmony for our featured guests. Babies are healthy; families are relieved; and dispatchers are proud to have participated in the sudden joyous—albeit stressful—event. Protocol’s Pre-Arrival Instructions made the sailing go more smoothly.
So sit back, if you can, and take a few min-utes to read about the good news you bring into the world every day, day in and day out. g
Facebook Connects Baby announcement refreshes friendship
SurprisePackages Delivery comes without benefit of fair warning
g stOrKstOries

THE JOURNAL | May/June 2011 43
Priceless Quality training returns far and above initial investment
Ever wonder about the effectiveness of one of the dispatch center programs? What about training, continuing dispatcher edu-cation, or quality assurance improvement? When budgets get tight, the quality and training programs are typically the first casu-alties. When does the return on investment become more important?
For the Pennington County (S.D.) Emer-gency Services Communications Center, training is conducted in a “stair step” approach. A skill set is taught, hands-on trained, certified, and used by the employee before learning another one. New employees spend five weeks in the local classroom, two weeks at the state academy, and six weeks of hands-on basic calltaker certification. Six weeks of hands-on radio back-up train-ing follows.
After six months on the job utilizing the calltaker and back-up skill sets, the telecom-
municator begins law enforcement radio training, spending three weeks hands on. About six months later, the dispatcher will cross-train to the second law enforcement radio. A dispatcher typically has three years of experience in the 9-1-1 center before start-ing fire/medical training. This training, two in-class sessions followed by hands-on con-sole training, will typically last about three months. All the while, monthly continuing dispatcher education (CDE) is reinforcing these skills for each discipline and qual-ity assessment feedback reinforces desired behaviors and discourages less than desirable performance before it becomes a bad habit.
For some people, this may seem like an extraordinary amount of time to spend on a single dispatcher. Is the return on the invest-ment worth it?
Just ask this couple. I’m sure they would answer “yes.”
Taking a seemingly mundane road trip, a U.S. Navy veteran and his young wife were moving 900 miles from home to find steady
employment. Who could possibly know the life-changing event that would unfold on their journey?
It was a routine evening at dispatch when a 9-1-1 medical call came in. Corey Noble, a young dispatcher certified as an EMD in April, answered the call. Thankfully, the call was from a pay phone at a rest stop on a main highway because the caller, not familiar at all with the area, could not identify where he was other than on the highway at a rest area with the map showing him “an inch to the left of” the nearest town. The couple was 15 miles from the nearest small town and more than 100 miles from a hospital.
A woman could be heard screaming from the restroom 20 yards from the phone; the caller just wanted help sent for what he described as abdominal pain, likely from the ovarian cysts that occasionally caused his wife’s pain.
Corey immediately convinced the caller to stay on the phone (despite the wife’s loud protests) so that together they could provide information to responders and assistance to the wife. Within a few moments, the caller said his wife was screaming it was a baby—and they hadn’t known she was pregnant. Corey asked the appropriate questions, and the husband let the phone dangle while he ran into the restroom to observe what was asked of him. It was quickly apparent that the baby was breech, the entire body and limbs had delivered, but not the head.
only 3% of pregnancies present breech; of those the mortality rate is 12%, and that is under professional medical care in a hospital (Fischer, 2009). This young couple was more than 100 miles from a hospital. They had a cell phone, but there was no coverage; they had to rely on the pay phone past a wall and 20 yards from where the patient was.
Corey’s five coworkers that night were all women, most mothers. Between dispatching the nearest sheriff’s deputy, ambulance ser-vice, and life flight helicopter, as well as the routine calls for service and radio traffic, they listened as much as they could as the event unfolded.
Following established protocol (the Medi-cal Priority Dispatch System™) while using calming and reassuring techniques, Corey
one For the road Baby's surprise birth at rest stop emphasizes importance of protocols, training, and pay phones.
By Leann Hollishead

44 THE JOURNAL | emergencydispatch.org
facilitated the birth with the help of the hus-band and a passerby who had also stopped at the rest area. While Corey gathered infor-mation and gave instructions, the two men alternated between the woman and the phone, reporting what was happening and getting further instructions, one staying with the woman at all times. The baby delivered, they got it breathing, delivered the placenta, and tied the umbilical cord during the next 29 minutes. Corey disconnected when first responders arrived on scene.
With teary eyes and a happy cheer, every-one was thrilled when they learned the mom and baby boy were both doing just fine.
For most dispatch calls, the “rest of the story” is rarely ever known. But the next day, Corey got to meet the mom, dad, and baby! The new par-ents had been trying to get pregnant for quite awhile but the mom was told that because of her medical issues, she would likely never be able to have children; that was why they didn’t know she was pregnant. The other gentleman at the rest area, who willingly helped, had delivered his third and fifth children at home. Best guess was the baby was between 32–36 weeks gestation, much better odds for surviving vaginal delivery for breech presentation.
And they had a dedicated EMD on the other end of the phone, calmly walking them through the Pre-Arrival Instructions (PAIs). What a miracle this couple experienced!
A lot of time and effort as well as tight budget funds go into acquiring, imple-menting, and utilizing protocols, as well as developing the training program and administering the quality program. It’s times like this that prove it’s worth every dollar invested.
Cost of hiring . . . . . . . . . . . . . . . . . . . . . $2,000
Cost of dispatcher training . . . . . . . . $15,000
Cost of EMD certification /card set/QI/CDE . . . . . . . . . . . . . . . . $1,700
For the EMD—knowing you helped bring a live baby into the world = priceless
For the parents—the assistance and guid-ance of a well-trained EMD during the mirac-ulous birth of a baby the doctors said you’d never have = priceless. g
Editor’s Note: Dispatcher Corey Noble and parents Chris and Stasi Thornton were featured in a video presentation shown at Navigator 2011.
reference: Richard Fischer, M.D., Division Head, Maternal-Fetal
Medicine, Professor, Department of obstetrics and Gynecology, Section of Maternal-Fetal Medicine, Cooper University Hospital, “Breech Presentation.” July, 2009.
I Can’t Drive 55Despite dad’s fast driving, baby arrives en route to hospital
Dana Bongle doesn’t remember the speed he was driving, and neither does he recall seeing or hearing the emergency vehicles in hot pursuit of the white van he was piloting south on the interstate toward the hospital.
He just knew he had to get there and fast. His wife Rachel was close to delivering their child from the backseat of their van with the assistance of a family friend who was consol-ing Rachel and calling 9-1-1.
“It was crazy,” said Manitowoc County (Wis.) Division of Emergency Services Dis-patcher Ann Sheahan. “We had responders chasing them down the highway. He was sure they could make it to the hospital before the baby was born.”
Dana’s timing was slightly off. An ambu-lance responding down the road in the oppo-site direction of the van caught his attention. He stopped the van at the side of the highway just after exiting the interstate.
Baby Audrey had arrived. She was already taking her first breaths in her mom’s arms when paramedics opened the van’s back door. The Bongles’ friend had tied the cord with white lacing from Dana’s size 14 shoe. How the lace got from the shoe to the cord is anyone’s guess.
For Sheahan, the healthy 6 pound, 13 ounce baby born within three minutes of the call to 9-1-1 was nothing short of remark-able. Audrey’s birth was a first for Sheahan, a dispatcher since 1993, and also a first for the
Manitowoc County Joint Dispatch Center. Sheahan was their first dispatcher to make it through the entire delivery.
“This was an awesome experience, one I will never forget,” said Sheahan, who had turned to the MPDS Pre-Arrival Instructions (PAIs) for childbirth/delivery. “After hearing the baby take her first breath, my co-worker [Katie Brull, who dispatched the ambulance] and I cried. We were so relieved.”
The story of Audrey’s interstate birth made the next day’s news. Sheahan penned a congratulatory note and sent it to the hos-pital, hoping the Bongles might extend an invitation to meet the dispatcher assisting in the 12:56 a.m. birth of Audrey.
The Bongles did just that. Sheahan stopped by their house for a brief introduc-tion soon after they brought Audrey home and a year later—in April 2009—the Bongles, with their daughter in tow, celebrated the one-year reunion at the center. Sheahan gave Audrey a pink blanket embossed with the 9-1-1 logo. They plan to jointly commemo-rate the reunion date in the years to come.
Sheahan said Audrey’s birth culminated a perfect week. The center gave her a stork pin in recognition of the event that coinci-dentally happened less than one hour after the annual National Public Safety Telecom-municator Week ended.
“It was great to have the call come in right at the same time,” she said. g
Mustang audrey Little Audrey had her dad running all over town and the highway in his rush to get to the hospital in time.

THE JOURNAL | May/June 2011 45
Getting To Know You Visit to communications center completesthe circle for dispatcher and family
Since pictures don't lie, it's obvious that little Vincent Van Sloten had a rough day meeting and greeting his fans at the Sioux Falls Metro Communications Center.
But did the tuckered out toddler even remotely consider the heightened level of anxiety he caused the day the center aided his delivery into the world?
Probably not.Vincent made his debut with mom and
dad—Tracy and Paul Van Sloten—in tow six months after he arrived rather unexpectedly at his home in South Dakota.
Metro Communications Shift Supervisor Janet Sternhagen, EMD, was ecstatic about their visit in october 2010, citing the rare opportunity of meeting a caller face-to-face coupled with the good fortune of holding the reason for the 9-1-1 connection.
“Vincent was healthy, happy, and very well-behaved,” said Sternhagen, who had the chance to hold baby Vincent on her lap six months after she helped in his over-the-phone delivery. “I was very happy to meet him and his parents.”
on April 10, 2010, Tracy was at work, with two weeks until the due date of her second child, when she realized something
wasn’t right. She drove home, called the doc-tor, and because of the discomfort she felt she was told to call 9-1-1. The timing was too close for her to get to the hospital on her own.
Tracy wasn’t hysterical, Sternhagen said, but definitely excited and in need of assistance. once Sternhagen knew exactly what was happening, she instructed Tracy, who was home alone, to first make sure the door was unlocked for access by paramed-ics already on their way. Approximately five minutes and 30 seconds into the call, the 8 lb Vincent was born.
But not without complications, Sternha-gen said. The head had delivered, but not his body, and his coloring was closer to purple than pink. Tracy could not detect any breath-ing. Sternhagen instructed her to continue to push to deliver the baby and then to briskly rub the baby’s back with a towel, accord-ing to Medical Priority Dispatch System™ (MPDS®) Pre-Arrival Instructions (PAIs).
“He took a breath and I heard his first cry,” Sternhagen said. “It was a wonderful sound to hear. I was sure glad to hear that and know that instructions for CPR were not needed.”
The caller disconnected once para-
medics arrived and although Sternhagen wanted to meet the family, she did not contact them, preferring to respect their privacy. This was her second baby delivery in 32 years of emergency communications (24 of those years at Metro) and the first time she had a mother home alone without anyone to assist.
Six months down the road, the Van Slo-tens scheduled a visit and Sternhagen intro-duced Vincent to the world of emergency dispatch or, at least, his parents to the won-derful world of Pre-Arrival Instructions.
obviously, Sternhagen was more than happy to provide the introductions.
“Janet did an outstanding job,” said Aimee Chase, Metro Communications qual-ity assurance coordinator. “We posted an Exemplary Performance Report with details of the call for everyone in the center to read.”
Metro Communications is a consoli-dated public safety communications center responsible for the dispatch of all emergency services within the city and county. This includes three law enforcement agencies, four ambulance services, 15 fire depart-ments, Emergency Management, and the City of Sioux Falls Animal Control. g
too Pooped to Party Vincent Van Sloten catches a quick couple of Z's in his dad's arms during a visit to meet EMD Janet Sternhagen.

46 THE JOURNAL | emergencydispatch.org
To The rescue Panicked dad hands phone to 10-year-old daughter
Never underestimate the courage and focus of a 10-year-old.
At least, that might be the message EMD Gina Reed will emphasize the next time someone complains about the "talk to my hand" generation.
The 10-year-old in Reed’s life was given the serious task of assisting her mother in delivering a baby on the family’s bathroom floor. Apparently the emergency was too much for dad, who had originally placed the call and, then, hastily handed the phone over
to his daughter once hearing there would be delivery instructions to follow.
“Although the husband had initiated, when we got to what he should do next, that was enough for him,” said Reed, a dispatcher for American Medical Response (AMR) com-munications center LIFECoM in Modesto, Calif. “The next thing I knew I was talking to a little girl.”
The mother’s contractions were only seconds apart when the call came in during the early hours of Dec. 8, 2010. Dad was pan-icked from the start, Reed said, in answering the Key Questions and providing a primary and secondary assessment of the mother in a voice noticeably shaken.
Not so for his daughter, however.“She was unbelievably good,” Reed said.
“A sweetheart.”The “sweetheart” was obviously eager to
take over from dad. She gave Reed control of the situation, complying with each step in the Pre-Arrival Instructions (PAIs). While mom screamed in the background, dad gathered whatever his daughter was told she needed and even opened the door for the paramedic unit arriving eight minutes into the call.
Strangers Come TogetherGood Samaritan aids dispatcher in delivering baby
When york County (Pa.) 911 Commu-nications dispatcher Mike Knaper signed in on Dec. 6, 2010, the last thing he expected
was the first call he answered to be his first baby delivery—particularly a delivery in which he’d need the help of a Good Samaritan.
Shirley Snyder and her pregnant granddaughter Keri Lavetan were on their way to the hospital when Snyder called 9-1-1. With Lavetan’s contrac-tions three to five minutes apart, Snyder wasn’t sure deliv-ery would wait the 10 miles to the hospital.
Knaper asked Snyder to pull off the road and she pulled into a conve-nience store parking lot. Knaper moved through the Medical Priority Dispatch
System™ (MPDS®) to give Snyder delivery instructions, but Synder didn’t want her great-grandchild coming any sooner than inside a maternity ward.
“She was stressed out,” Knaper said. “She didn’t really want to deliver the baby.”
Fortunately, their predicament caught a stranger’s eye. According to a Daily Record article, Joe Lesoken approached their car and saw Lavetan stretched out across the front seats. once Lesoken was told Lavetan was giving birth, he offered to take over; Snyder gladly opened the car door and handed him the phone. Lesoken gave Lavetan a pep talk, telling her she would do just fine giving birth where she was.
In seconds the delivery went from Leso-ken telling Knaper that he couldn’t see any
When Push Comes to shove With dispatcher's help, 10-year-old takes over delivery from dad.
not a second too soon Commotion in car brings stranger to the rescue of grandmother overwhelmed by granddaughter's chance delivery.

THE JOURNAL | May/June 2011 47
Beat The Clock Baby Haley makes a fast dashfor home delivery
An impatient baby made the early hours of oct. 16, 2010, a day to always remember for EMD Sharie Eastridge and the baby’s mother April Cox.
Cox anticipated this delivery to be no dif-ferent from previous deliveries, which to her meant a relatively uneventful delivery with her doctor on hand. She was sent home from the hospital when contractions that brought her there were dismissed as premature labor, but told to return once the pregnancy pro-gressed further.
Baby Haley apparently disagreed, out-smarting the doctor’s timetable and, in the process, leaving only her parents and grand-mother to deliver her—with the help of East-ridge, a Pittsylvania County (Va.) dispatcher.
Cox and her boyfriend Justin Thornton hadn’t been home long from the hospital when an intense abdominal pressure had Cox rushing to the bathroom to relieve what she thought to be a very full bladder. Her mother, Pamela Riggins, called 9-1-1 and Eastridge, who answered their call, was soon giving the Post-Dispatch Instructions (PDIs) for Protocol 24: Pregnancy/Childbirth/Miscarriage.
But the instructions were cut short. “The baby’s coming. The baby’s coming,” Riggins
shouted into the phone. And in less time than it takes change a diaper, Riggins told her Thornton had just delivered a healthy, baby Haley.
“It went really fast,” Eastridge said. Eastridge skipped to Card F: Childbirth-
Delivery Panel 7—Check Baby and gave instructions to clean the baby’s face and wrap her up, reaching the part about tying the umbilical cord as first responders pulled up. Two days later, Eastridge visited the hos-pital to meet Cox, Thornton, and baby Haley Ranae Thornton.
“The baby was perfect,” said Eastridge, who marks Haley as her first childbirth delivery in the four years she’s been a dis-patcher. “They (Cox and Thornton) were very thankful that we had the instructions to give them.”
It’s a good thing Haley picked the date she did. Pittsylvania County went live with the Medical Priority Dispatch System™ (MPDS®) on oct. 11, less than a week before her birth, making Haley and Eastridge the inaugural party for childbirth-delivery Pre-Arrival Instructions (PAIs).
“I couldn’t have asked for anything better than the way it played out,” Eastridge said. “It was definitely a great experience for me.” g
no time Like the Present Baby Haley arrives at home contrary to the doctor's and family's timetable.
The girl was short of breath by the time baby arrived and most likely elated about the sibling she helped bring into the world. Mother and baby and big sister were report-edly doing well when paramedics arrived for the ride to the hospital.
No telling, however, the spin on the story dad will take in the days and years to come.
“He was lucky his daughter was there,” Reed said. “She never left the phone once.”
AMR presented Reed with a letter of rec-ognition, honoring her “competent and early intervention,” and a stork pin commemorat-ing her entry into a rather exclusive club.
“This was a fantastic week for Gina,” said LIFECoM CQI Supervisor Teri Griffin, who spent considerable time on the incident (as well as others), tracking down the respond-ing crew and following with ED staff. “She received a save pin for a DLS save 10 days ago and a stork pin about a week apart.”
The baby delivery in December was Reed’s second delivery in two months. In october, Reed provided PAIs to a new dad assisted by several neighbor ladies apparently on the alert in case of imminent delivery.
These are the reasons Reed likes the job.“I wanted a change from the office work
I had done for a long time,” she said. “This is great. I found something that’s never the same day to day.”
AMR communications center LIFECoM in Modesto, Calif., is a NAED Accredited Center of Excellence (ACE). g
part of the baby to seeing the baby’s head and reaching out his hands to catch Evan Robert Lavetan. They dried off Evan and wrapped him in blankets to keep out the winter’s chill. Police pulled in, followed by the ambulance.
“I consider him my guardian angel,” Lavetan was quoted as saying in the article. “Had he not been there, I don’t know what would’ve happened.”
Knaper isn’t sure how it would have turned out either.
“He (Lesoken) was basically my sav-ior because he was willing to listen to my instructions,” Knaper said. “He just stepped in there and took control of the situation and delivered a baby. I don’t know what we would have done if the grandmother was the only one there to assist.”
Knaper, a york County dispatcher for three years, wasn’t the only dispatcher at the center to assist in delivering a bundle of joy that cold December day—two fellow dis-patchers also received stork pins. g
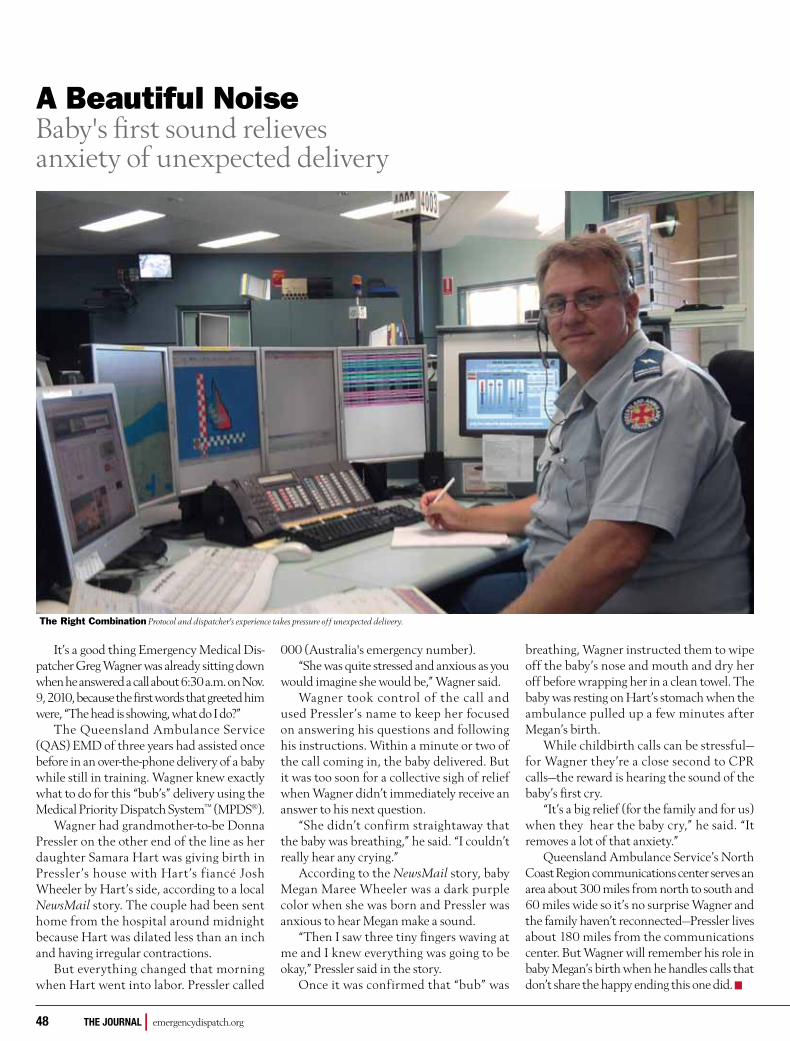
48 THE JOURNAL | emergencydispatch.org
A Beautiful Noise Baby's first sound relievesanxiety of unexpected delivery
It’s a good thing Emergency Medical Dis-patcher Greg Wagner was already sitting down when he answered a call about 6:30 a.m. on Nov. 9, 2010, because the first words that greeted him were, “The head is showing, what do I do?”
The Queensland Ambulance Service (QAS) EMD of three years had assisted once before in an over-the-phone delivery of a baby while still in training. Wagner knew exactly what to do for this “bub’s” delivery using the Medical Priority Dispatch System™ (MPDS®).
Wagner had grandmother-to-be Donna Pressler on the other end of the line as her daughter Samara Hart was giving birth in Pressler’s house with Hart’s fiancé Josh Wheeler by Hart’s side, according to a local NewsMail story. The couple had been sent home from the hospital around midnight because Hart was dilated less than an inch and having irregular contractions.
But everything changed that morning when Hart went into labor. Pressler called
000 (Australia's emergency number).“She was quite stressed and anxious as you
would imagine she would be,” Wagner said. Wagner took control of the call and
used Pressler’s name to keep her focused on answering his questions and following his instructions. Within a minute or two of the call coming in, the baby delivered. But it was too soon for a collective sigh of relief when Wagner didn’t immediately receive an answer to his next question.
“She didn’t confirm straightaway that the baby was breathing,” he said. “I couldn’t really hear any crying.”
According to the NewsMail story, baby Megan Maree Wheeler was a dark purple color when she was born and Pressler was anxious to hear Megan make a sound.
“Then I saw three tiny fingers waving at me and I knew everything was going to be okay,” Pressler said in the story.
once it was confirmed that “bub” was
breathing, Wagner instructed them to wipe off the baby’s nose and mouth and dry her off before wrapping her in a clean towel. The baby was resting on Hart’s stomach when the ambulance pulled up a few minutes after Megan’s birth.
While childbirth calls can be stressful—for Wagner they’re a close second to CPR calls—the reward is hearing the sound of the baby’s first cry.
“It’s a big relief (for the family and for us) when they hear the baby cry,” he said. “It removes a lot of that anxiety.”
Queensland Ambulance Service’s North Coast Region communications center serves an area about 300 miles from north to south and 60 miles wide so it’s no surprise Wagner and the family haven’t reconnected—Pressler lives about 180 miles from the communications center. But Wagner will remember his role in baby Megan’s birth when he handles calls that don’t share the happy ending this one did. g
the right Combination Protocol and dispatcher's experience takes pressure off unexpected delivery.

THE JOURNAL | May/June 2011 49
register online and get up-to-date conference information at QUESTIONS 011 801 359 [email protected]
50 THE JOURNAL | emergencydispatch.org
Let It SnowBlizzards bring dispatch mixed blessings
Audrey Fraizer
g retrOsPaCe

THE JOURNAL | May/June 2011 51
A fierce three-day storm crippling Cen-tral New york March 13 and 14, 1993, dumped more than three feet of snow
against a backdrop of thunder, lightning, and variable winds whipping circles at 23 mph. Paramedics and rescue crews used toboggans to transport patients from homes to ambulances and volunteer firefighters in onondaga Hill rode snowmobiles to reach people.
Four floors above in the Syracuse (New york) emergency command center, Syracuse Fire Department Deputy Chief John Falge was on the phone to the 9-1-1 communica-tions center giving dispatchers instructions on priority calls. During the next 24 hours, they answered a record 6,500 calls. Dispatch-ers in onondaga County took 4,203 calls that weekend, blowing the former record of 2,772 calls out of the water. People calling in for road conditions were promptly cut short.1
But not everyone was dialing 9-1-1.Roads closed, businesses shut down, and
people stayed home finding more to do than just throw snowballs. Nine months later, hospitals reported a 30 percent average increase in births.
“It sure beats shoveling,” said Jeff Gage, proud father of Kelsey Lynn Gage who was born on the date estimated by doctors for babies conceived during one of the days a cumulative 42.9 inches of snow fell on Central New york.2
And while experts don’t always agree on the baby-boom blizzard hypothesis, which suggests a direct correlation between increased births and bad weather, these stories seem to at least moderately tip the demographer’s apple cart.
Nora Kathleen Beatty checked in Nov. 3, 1978, just a few days shy of exactly nine months from the day the Great Blizzard of 1978 ravaged New England, isolating thou-sands of families from everyone but each other. But Kate was not alone. After deliv-ery, mom spent the next five hours in a cor-ridor until space opened up in the crowded maternity ward at South Shore Hospital in Weymouth, Mass.3
Babies arrived in record numbers during two months in the fall following blizzards marooning residents in their Alton, Ill., homes for prolonged periods of time during January and February 1984. Alton Memorial Hospital Nurse Ruth Standefer had noted a “baby boom from bad weather” on her calendar and sure enough, the maternity ward hosted 49 babies during three days in November coinciding with the nine-month lapse since the big snow.4
So, what does this all mean to weather warrior emergency dispatchers?
Emergency dispatchers join snowplow drivers and weather forecasters as the most beleaguered bunch during a blizzard. They’re probably not home throwing snowballs or mak-ing babies. They’re answering tens of thousands of calls during these same storms, struggling to sort the true life-and-death emergencies from the more minor problems associated with heavy snow. These are just a few of the examples:
• CommunicationscentersintheMid-west received hundreds of calls during the blizzard of 1993 from emergency workers requesting four-wheel drive assistance for ambulance services, par-ticularly in the windblown remote sec-tions of the states.
• Duringtheblizzardsof1997,aSouthDakota woman called 9-1-1 on her cell phone when she became stranded in a blizzard. She hung on and was found several hours later because of emergency officials—including 9-1-1 dispatchers—who wouldn’t give up at determining her exact location.
• TheBlizzardof2010haddispatchersin New york answering thousands of calls and working multiple shifts, cov-ering for coworkers who were stranded because of the public transit standstill.
And don’t forget the prank callers who find a winter crisis the opportune time to call 9-1-1. Hundreds of requests for everything from a Saturday newspaper to help with a
flat snowblower tire plagued Manitoba’s (Canada) 9-1-1 emergency centers during a weekend blizzard in November 1986. one woman phoned police in a panic because she couldn’t leave the house to buy hotdog buns. Another called 9-1-1 four times in a row to complain that her house was shaking from the snowplows working outside.
“For some reason, we’re usually the first place people call,” said Manitoba Police Inspec-tor Bryan Kramble. “And it seems when the situation gets tense, instead of reacting in a sensible way, they react in a frustrated way.”5
Crime is one of the few activities giving emergency police dispatchers a break during inclement weather. oklahoma City (okla.) police dispatchers received 1,200 fewer calls during the February 2011 storm (4,644 calls over a 48-hour period compared to the usual 6,000 calls). Following the blizzard of 1996, police from Boston to Washington reported drops in almost all categories of crimes. Phil-adelphia lasted 60 hours without a murder and New yorkers had almost three full days without any reported homicides.
“We’re thankful for any help we can get from God or man in our fight to reduce crime,” Philadelphia Police Commissioner Richard Neal told reporters. “And who knows? Maybe nature can teach people the senselessness of pitting man against man.”6
And the sense of bringing them together. g
Sources1 Brian Carr, We’re Snow King, Syracuse Herald Journal,
March 3, 1993; retrieved March 1, 2011
2 Brian Carr and Amber Smith, Area hospitals report a flurry
of blizzard babies, Syracuse Herald Journal, Dec. 27, 1993;
retrieved March 1, 2011
3 UPI- Boston, The blizzard babies arrive, Salina Journal, Nov.
19, 1978; retrieved March 1, 2011
4 Mary Ann Mazenko, Baby boom from winter storm proves
nurse’s prediction, Alton Telegraph, Dec. 4, 1982; retrieved
March 1, 2011
5 Don Lett, Frivolous calls tax 911 system, Winnipeg Free
Press, Nov. 2, 1986; retrieved March 1, 2011
6 AP Crime takes a cold holiday, The News, Frederick, M.D.,
Friday, Jan. 12, 1996; retrieved March 1, 2011

52 THE JOURNAL | emergencydispatch.org