babies “r” us - seabb.org · babies “r” us october 11, 2007 dr. alexander duncan. lucienne...
TRANSCRIPT

Babies “R” Us
October 11, 2007
Dr. Alexander DuncanLucienne Ide
Ken SuthasinekulScott Robinson
Little Tots need no Clots

“Pregnancy is the only controlled hypercoaguable state we know”

I know it’s your first time, but I promise it won’t hurt!

We came all this way for nothing ?

Anybody got a flashlight?

What do you mean it’s all about fibrinolysis !
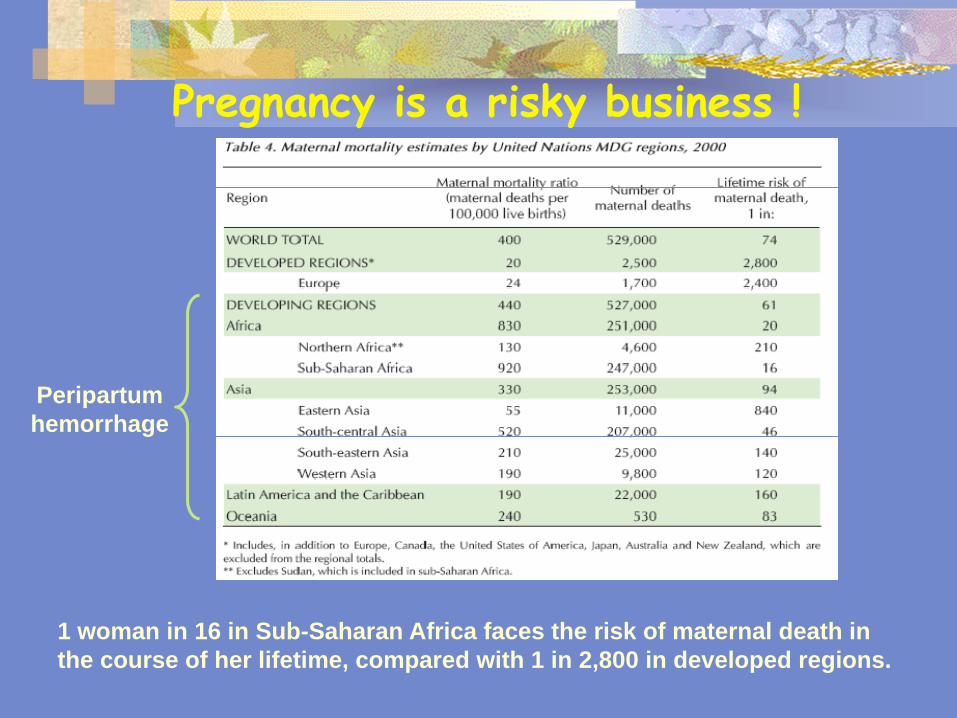
Pregnancy is a risky business !
1 woman in 16 in Sub-Saharan Africa faces the risk of maternal death in the course of her lifetime, compared with 1 in 2,800 in developed regions.
Peripartum hemorrhage

Uterine blood flow increases 50-fold
CO doubles & 40% rise in blood volume
At term, uterine flow rate = 750 mL/min
Gabbe: Obstetrics - Normal and Problem Pregnancies, 4th ed.

What’s wrong with being sticky?

Good/Normal

Bad/Abnormal

“Ugly”

Virchow’s Triad
1. Alterations in blood flow (stasis)
1. Injury to the vascular endothelium
2. Alterations in the blood components (hypercoaguability)

Factor V Leiden
Prothrombin

Normal Coagulation Changes in Pregnancy
Changes start at end of first trimester.
Increases in Fibrinogen, Factors VII &VIII
Increases in PAI-1 & PAI-2
Increased Thrombin generation (MOCHA)
Increased von Willebrands factor
Decreased fibrinolysis
Increased platelet activation
High Lipoprotein (a)

Duncan’s Bad Signs
Any increase in activity in first trimester.
F VII increases faster than F VIII.
Supra normal values in activities.
Rapid increases in MOCHAs
Rapid increases in PAI-1
Early evidence of Pre- eclampsia.
Early IUGR.
Multiple recurrent losses.

MOCHA
What we know about thrombin generation can help us make diagnostic and therapeutic decisions.
Thrombin is locally controlled by various functions including anticoagulants such as antithrombin and the Protein C pathway
Functioning endothelial cells provide the bulk of thrombin downregulation to control in vivo clot extension.
Markers Of Coagulation andHemostasis Activation.
An assessment of thrombin generation and control.
Prothrombin Fragment 1.2
Thrombin: Antithrombin Complexes
Quantitative D-Dimer
Quantitative Fibrin Monomer

Underlying Issues
What about the impact (or not) of underlying thrombophilia ?
Should F V Leiden & PT gene patients be prophylaxed with LMWH if they have had no problems ( NO !!)
What about 1st degree relatives with losses ? ( harder question)
More Issues
What about the patient with 2 losses and no identifiable thrombophilia, desperate to stay pregnant !
What about high Lp(a) ?
What about MTHFR mutations, homozygous/double heterozygotes
Is it true that 70% of first trimester losses are genetic?
Even More Issues
What to do when science and emotion conflict ?
Only 70% of patients with VTE, currently have a diagnostic etiology determined.
What about new analytes !! ( EPCR, TFPI, PZI, TM)
What about safety of therapy!

Gestational Vascular Complications (GVC)
Severe pregnancy complications associated with deficient uteroplacental circulation possibly due to microthrombi of the placental vasculature
• Placental abruption
• Pre-eclampsia
• Intrauterine growth retardation (IUGR)
• Intrauterine fetal death (IUFD)
Serious complications occur in 1-5% of pregnancies
Who is at risk?
Women with primary or secondary thrombophilia.
Five fold increased risk of above complications!
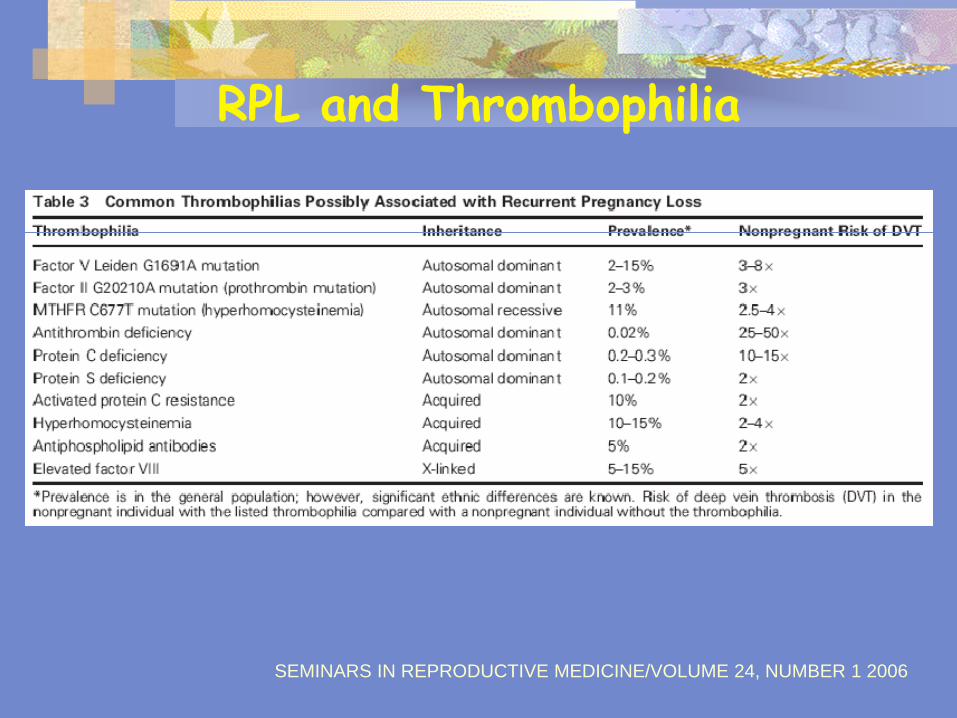
SEMINARS IN REPRODUCTIVE MEDICINE/VOLUME 24, NUMBER 1 2006
RPL and Thrombophilia

Pre-eclampsia10-20% of maternal deathsTreatment is delivery of the fetus and placenta
Placental abruption20% maternal deathsCan lead to hemorrhagic shock & fulminant DICTreatment is delivery of the fetus and placenta
Intrauterine growth retardation (IUGR)Below 10th percentileNutrient and oxygen supply compromised (4x decrease in flow)Treatment is frequently delivery of the fetus
Intrauterine fetal death (IUFD) (>500g, ~20wks)1/4th of cases unexplainedInfections, chromosomal abnormalities, fetal hydrops
Consequences of GVC

IUFD
Also associated with:
• Antithrombin deficiency
• Protein S and C deficiencies
• Other inherited thrombophilias
• Antiphospholipid Syndrome

How to Treat PRL / GVC ?Aspirin
Inhibits cyclooxygenase activityDecrease in TXA2 inhibits platelet aggregation
Low molecular weight heparin (LMWH)Causes conformational change in antithrombin.Increases enzymatic inactivation by 1000-fold (factor Xa>IIa)Stimulates expression of TFPI by endothelial cells
40 mg LMWH v 100mg ASA daily:86% LMWH treated pregnancies vs 29% ASA only treated pregnancies resulted in normal births

LMWH vs UFH
UFH has NO place in prophylaxis anymore.!!!!!
Poor bio-availability, HIT risk, osteoporosis, variable blood levels.
Is good for IV use if monitored properly. Can NOT use the APTT in a term patient to monitor UFH ( high factors, sensitivity)
Shorter half life in pregnancy.

LMWeight Heparins
None approved for use in pregnancy
All have been used with minimal issues.
Minimal to no HIT risk
Almost no osteoporosis ( < 3% average)
More LMWH
FDA state no monitoring of these drugs is needed.
They do need monitoring !!
Many woman are undertreated.
In vivo drug half lives vary by molecular weight. (Fragmin > Lovenox)
Little published on Arixtra, but works well in my experience.

Controversies !!
Some people would argue there is almost NO evidence based medicine to support the use of LMWH in pregnancy.
LOVENOX trial is only major peer reviewed publication
Even less to support it’s use in fertility patients.
More Controversies.
What is the rationale in infertility patients?
Are they hypercoagulable ?
Do they really have hypofibrinolysis ?
What has Lp(a) to do with anything (a lot)
Is it even ethical to treat patients with LMWH just because anecdotal evidence says it works.