bayesian probability prospective - homepage |...
TRANSCRIPT
DIAGNOSTIC METHODSPROBABILLIfY ANALYSIS
Bayesian probability analysis: a prospectivedemonstration of its clinical utility in
diagnosing coronary diseaseROBERT DETRANO, M.D., PH.D., JOHN YIANNIKAS, M.D., ERNESTO E. SALCEDO, M.D.,GuSTAVo RINCON, M.D., RAYMUNDO T. Go, M.D., GEORGE WILLIAMS, PH.D.,AND JUDY LEATHERMAN, B.S.
ABSTRACT One hundred fifty-four patients referred for coronary arteriography were prospectivelystudied with stress electrocardiography, stress thallium scintigraphy, cine fluoroscopy (for coronary
calcifications), and coronary angiography. Pretest probabilities of coronary disease were determinedbased on age, sex, and type of chest pain. These and pooled literature values for the conditionalprobabilities of test results based on disease state were used in Bayes' theorem to calculate posttestprobabilities of disease. The results of the three noninvasive tests were compared for statisticalindependence, a necessary condition for their simultaneous use in Bayes' theorem. The test resultswere found to demonstrate pairwise independence in patients with and those without disease. Somedependencies that were observed between the test results and the clinical variables of age and sex were
not sufficient to invalidate application of the theorem. Sixty-eight of the study patients had at least onemajor coronary artery obstruction of greater than 50%. When these patients were divided into low-,intermediate-, and high-probability subgroups according to their pretest probabilities, noninvasive testresults analyzed by Bayesian probability analysis appropriately advanced 17 of them by at least one
probability subgroup while only seven were moved backward. Of the 76 patients without disease, 34were appropriately moved into a lower probability subgroup while 10 were incorrectly moved up. Weconclude that posttest probabilities calculated from Bayes' theorem more accurately classified patientswith and without disease than did pretest probabilities, thus demonstrating the utility of the theorem inthis application.Circulation 69, No. 3, 541-547, 1984.
BAYES' THEOREM' can be used to calculate theprobability of coronary artery disease based on clinicaldata and multiple noninvasive test results.2 3 Pretestprobabilities of disease are assigned based on clinicaldata and the equation is used to calculate posttest prob-abilities after multiple sequential tests.The validity of application of the theorem to multi-
ple clinical and test variables depends on the mutualstatistical independence of these variables in popula-tions of patients with and without disease.4 The resultsof this investigation provide evidence that indepen-dence does in fact exist for the results of the followingnoninvasive tests: stress electrocardiography, thal-lium-201 stress scintigraphy, and cardiac cine fluoros-copy (for coronary calcifications). With some excep-tions there is also evidence for the independence of
From the Departments of Cardiology, Nuclear Medicine, and Biosta-tistics, Cleveland Clinic Foundation, Cleveland.
Address for correspondence: Ernesto E. Salcedo, M.D., ClevelandClinic Foundation, 9500 Euclid Ave., Cleveland, OH 44106.
Received Aug. 18, 1983; revision accepted Nov. 23, 1983.
Vol. 69, No. 3, March 1984
these three test variables and the clinical variables ofage, sex, and type of chest pain.
Diagnostic testing is useful if patients with diseasewho are initially judged to have a low probability ofdisease are finally judged to have a high probabilitybecause of the test results. Similarly, test utility isdemonstrated if patients without disease are appropri-ately moved from a subgroup of high probability to oneof low probability. Although previous reports2 3 havedemonstrated that posttest probabilities are fairlyclosely associated with disease prevalence, there hasbeen no prospective demonstration that they appropri-ately move patients from lower to higher probabilitygroups or vice versa. This study demonstrates how a
Bayesian analysis of clinical data and noninvasive test
results can be useful in classifying patients with andwithout coronary disease.
MethodsStudy sample. Between May 1981 and October 1982, 226
patients without histories or electrocardiographic evidence of
541
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from

DETRANO et al.
myocardial infarction were referred to a group of six participat-ing cardiologists at our institution for the angiographic evalua-tion of suspected coronary disease. Sixty-seven of these wereexcluded from this study because they refused to undergo test-ing, had known or suspected valvular or cardiomyopathic dis-ease, unstable angina, serious arrhythmia, left bundle branchblock, extreme obesity, or orthopedic or neurologic conditionsprecluding performance of a sympton-limited treadmill exercisetest. All 159 remaining subjects were informed and they andtheir angiographers agreed that test results would influence onlypostcatheterization medical or surgical management and not thedecision of whether or not to perform an angiographic examina-tion. Despite this, a breach in the research protocol resulted infive subjects not undergoing cardiac catheterization becausethey were considered to have a very low probability of signifi-cant coronary disease based on their exercise test results. Sincethe study subjects did not receive the full potential benefit ofpreangiography exercise testing, the cost of stress electrocardio-graphy was absorbed by the institution. Of the 154 subjectsundergoing angiography, there were 111 men and 43 women.Their mean age was 54 years.
Clinical data. Clinical histories were reviewed by an investi-gator unaware of any test or angiographic results. Patients weregrouped according to age, sex, and type of chest pain. The latterwas divided into the following four categories:
(1) Typical angina pectoris. Pain that occurs in the anteriorthorax, neck, shoulders, jaw, or arms is precipitated byexertion and relieved within 20 min by rest.
(2) Atypical angina. Pain in one of the above locations andeither not precipitated by exertion or not relieved by restwithin 20 min.
(3) Nonanginal pain. Pain not located in any of the abovelocations, or if so located not related to exertion, andlasting less than 10 sec or longer than 30 min.
(4) No pain.Test protocolExercise tests. All subjects underwent treadmill exercise ac-
cording to the Bruce protocol. Exercise was terminated becauseof fatigue, dyspnea, progressive angina, ST depression greaterthan 2.5 mm, or when the subject reached his age-adjustedtarget heart rate. Modified 12-lead electrocardiograms were re-corded in subjects at rest and at peak exercise. One minutebefore the completion of exercise, 2 mCi of thallium-201 wereinjected directly into an arm vein. Nuclear imaging was begunabout 5 min after injection in the 45 degree and 70 degree leftanterior oblique and anterior projections. All images were re-corded for 10 min for each projection on a portable gammacamera with 1/4 inch crystal and a high-sensitivity low-energycollimator. All three projections were repeated approximately 4hr after thallium injection to obtain redistribution images. Ac-quired data were stored in the VIP-550 microprocessor systemfor subsequent analysis.
Coronary arteriography and cine fluoroscopy. On the dayafter treadmill exercise all patients underwent selective coro-nary arteriographic examination by the Sones technique andmultiple projections of each vessel were obtained. During thisprocedure cine fluoroscopic examination without contrast wasdone in the left and right anterior oblique projections. The x-rayexposure factors used for both cine angiography and cine fluo-roscopy were 300 mA, 75 to 95 kV, and a 5 msec pulse width.
Test analysis. ST segment depressions at peak exercise wereanalyzed by an observer blinded to the clinical data, the nonin-vasive test results, and the results of angiographic examination.The vertical distance between the middle point of the PR seg-ment and the ST segment 80 msec after the J point was measuredto the nearest 0.2 mm for several complexes in leads I, II, V2,V4, and V5. The resulting ST segment shifts were averaged for
each lead and the corresponding resting ST shifts were subtract-ed. The five resulting ST segment depressions relative to restwere searched for a maximum and this number was assigned tothe appropriate category from the following: ST < 0.5, 0.5 z
ST < 1.0, 1.0 -,C ST < 1.5, 1.5 -,: ST < 2.0, 2.0 -,- ST < 2.5,2.5S ST. The appropriate category became the test result foreach subject's stress electrocardiogram.
Computer-stored scintigraphic data were analyzed by an in-vestigator unaware of the other test and angiographic results.Myocardial segments were evaluated by quantification of thedecreased radioactivity in the poorly perfused area and compari-son with the maximum pixel count in normal myocardium.5Three results were possible: (1) normal, (2) fixed abnormality(defects observed during exercise that persisted at redistribu-tion), and (3) reversible abnormality (defects present duringexercise and significantly corrected during redistribution).Fluoroscopic films without contrast were reviewed by two in-vestigators without knowledge of the clinical, exercise, or an-
giographic results. A result of one, two, three, or no calcifiedvessels was assigned to each subject. Coronary arteriogramswere interpreted by an experienced angiographer not directlyinvolved in the study. A stenosis of greater than 50% of theintraluminal diameter of one of the four main coronary arterieswas considered sufficient to classify a subject as having coro-
nary artery disease.Probability analysis. Let the symbol D denote the event that
a patient has coronary artery disease and let ND denote thealternative event that he does not have disease. P(D) will be thepretest probability of disease and will be, in fact, the prevalenceof disease in a population of patients of a given sex and age
(decade of life) and with one of the four possible types of chestdiscomfort, as defined above.
Let ST, Th, and Ca denote variables that can take on valuesdetermined by the results of the three noninvasive tests. Forexample, the stress electrocardiographic change, ST, can havethe value "[1.5 - ST < 2.0]" and the thallium scintigraphyreading Th can have the value "reversible perfusion defect."The number of calcified arteries. Ca, might take the value "2."P(STJD), P(ThID), and P(CaID) are the conditional probabil-ities of a particular test result given that an individual has coro-
nary disease. If our tests had only two possible outcomes (posi-tive or negative), these probabilities would be the testsensitivities. Similarly, P(STIND), P(ThIND), and P(Ca|ND)are the conditional probabilities of the same test results giventhat a subject does not have disease. For tests with two out-comes, these would be the false-positive rates (1 - specificity).Bayes' theorem states that if the variables ST, Th, and Ca are
statistically independent in both the diseased and nondiseasedpopulations, then the probability of coronary disease given thetest results ST, Th, and Ca is defined by the equation
P(D|ST, Th. Ca) =
P(D) P (ST|D)P(ThID)P(Ca]D)P(D) P(STID)P(ThJD)P(CaID) + [1 - P(D)] P(STIND)P(ThtND)P(CaIND)
The left side of the equation, P(D|ST, Th, Ca), will be referredto as the posttest probability. The pretest probabilities used inthis research, P(D), and the conditional probabilities P(ST|D),P(STIND), P(ThfD), P(ThIND), P(CaID), and P(Ca|ND) were
calculated by Diamond and Forrester2 by pooling estimates ofthese quantities from the literature on the prevalence of coronarydisease and the sensitivities and specificities of the noninvasivetests. The reference group that provided the data base for thepretest probabilities based on age, sex, and chest pain consistedof 4952 symptomatic individuals studied with coronary arteri-ography and 23,996 asymptomatic persons who died of diseaseother than cardiac disease and were not known to have coronary
disease previous to their postmortem examinations. The condi-tional probabilities applied to our study group for the stress-
542 CIRCULATION
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from
DIAGNOSTIC METHODS-PROBABILITY ANALYSIS
induced ST segment depression, thallium perfusion defects, andcoronary calcifications were based on results in 4838, 1132, and507 patients, respectively, studied with the respective noninva-sive test and coronary arteriography.2 Three of our subjects'stress electrocardiograms revealed rate dependent left bundlebranch block. Since the conditional probabilities of this testresult are unknown, we ignored their stress electrocardiogramsin the probability calculations.
For each patient in the study a pretest probability was chosenfrom the pooled literature values2 based on age, sex, and type ofchest pain. Conditional probabilities of the various noninvasivetest results for subjects with and without disease were alsoassigned according to their performances on the tests. Thesequantities were then substituted into Bayes' theorem to calculateposttest probability.
Both the pretest and posttest probabilities were divided intoprobability subgroups as follows: low (0 < p < .2), intermedi-ate (.2 S p S .8), and high (.8 < p S 1.0). A pretest andposttest subgroup was thus assigned to each subject and thenumber of subjects for whom probability either advanced orretreated by at least one subgroup as a result of testing wasdetermined for subjects with and those without disease. Theboundaries of these subgroups were chosen to obtain significantnumbers of patients in each one and to retain symmetry betweenthe first and third subgroup, and because we judged them to beclinically relevant to the decision of whether or not to performangiography.
Independence. The validity of Bayes' theorem depends onthe mutual statistical independence of the test variables ST, Th,and Ca for subjects with and those without disease. It alsodepends on the statistical independence of these test variablesand the clinical variables of age, sex, and type of chest pain,since the Bayes' equation cannot be validly used if the condi-tional probabilities of certain test results in the patients with andwithout disease depend on the pretest probability determined byage, sex, and type of pain. There are thus three test variables forwhich mutual independence is required and independence be-tween these and the three clinical variables should also be pres-ent. Because the number of patients with particular values foreach clinical and test variable was small, it was necessary todichotomize the variables as follows: age <55, age >55; male,female; angina pectoris, other symptoms; ST depression < 1.0,ST depression 1.0; thallium normal, thallium abnormal; nocalcified vessels, at least one calcified vessel. These six varia-bles were then paired and tested for pairwise dependence with achi-squared test and a 5% significance level without controlover the type I error rate for multiple comparisons. True mutualindependence was not tested because of the inadequate samplesize.
ResultsClinical data. The numbers of men and women with
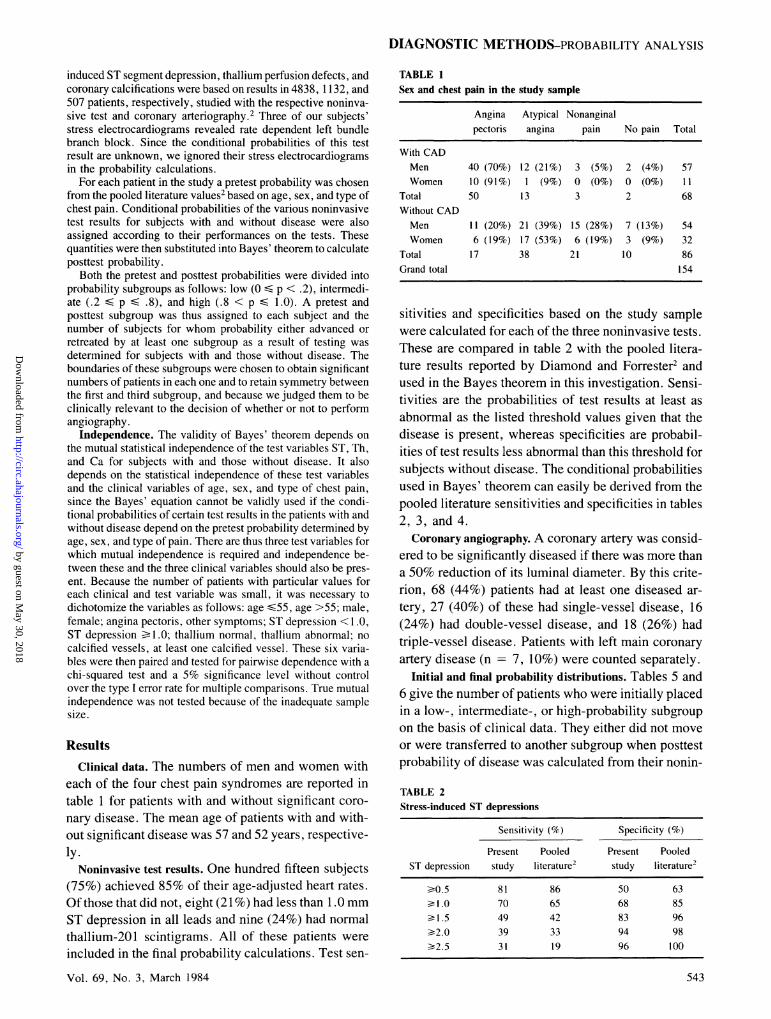
each of the four chest pain syndromes are reported intable 1 for patients with and without significant coro-nary disease. The mean age of patients with and with-out significant disease was 57 and 52 years, respective-ly.
Noninvasive test results. One hundred fifteen subjects(75%) achieved 85% of their age-adjusted heart rates.Of those that did not, eight (21 %) had less than 1.0 mmST depression in all leads and nine (24%) had normalthallium-201 scintigrams. All of these patients wereincluded in the final probability calculations. Test sen-
TABLE 1Sex and chest pain in the study sample
Angina Atypical Nonanginalpectoris angina pain No pain Total
With CADMen 40 (70%) 12 (21%) 3 (5%) 2 (4%) 57Women 10 (91%) 1 (9%) 0 (0%) 0 (0%) 11
Total 50 13 3 2 68Without CADMen 11 (20%) 21 (39%) 15 (28%) 7 (13%) 54Women 6 (19%) 17 (53%) 6 (19%) 3 (9%) 32
Total 17 38 21 10 86Grand total 154
sitivities and specificities based on the study samplewere calculated for each of the three noninvasive tests.These are compared in table 2 with the pooled litera-ture results reported by Diamond and Forrester2 andused in the Bayes theorem in this investigation. Sensi-tivities are the probabilities of test results at least asabnormal as the listed threshold values given that thedisease is present, whereas specificities are probabil-ities of test results less abnormal than this threshold forsubjects without disease. The conditional probabilitiesused in Bayes' theorem can easily be derived from thepooled literature sensitivities and specificities in tables2, 3, and 4.Coronary angiography. A coronary artery was consid-
ered to be significantly diseased if there was more thana 50% reduction of its luminal diameter. By this crite-rion, 68 (44%) patients had at least one diseased ar-tery, 27 (40%) of these had single-vessel disease, 16(24%) had double-vessel disease, and 18 (26%) hadtriple-vessel disease. Patients with left main coronaryartery disease (n = 7, 10%) were counted separately.
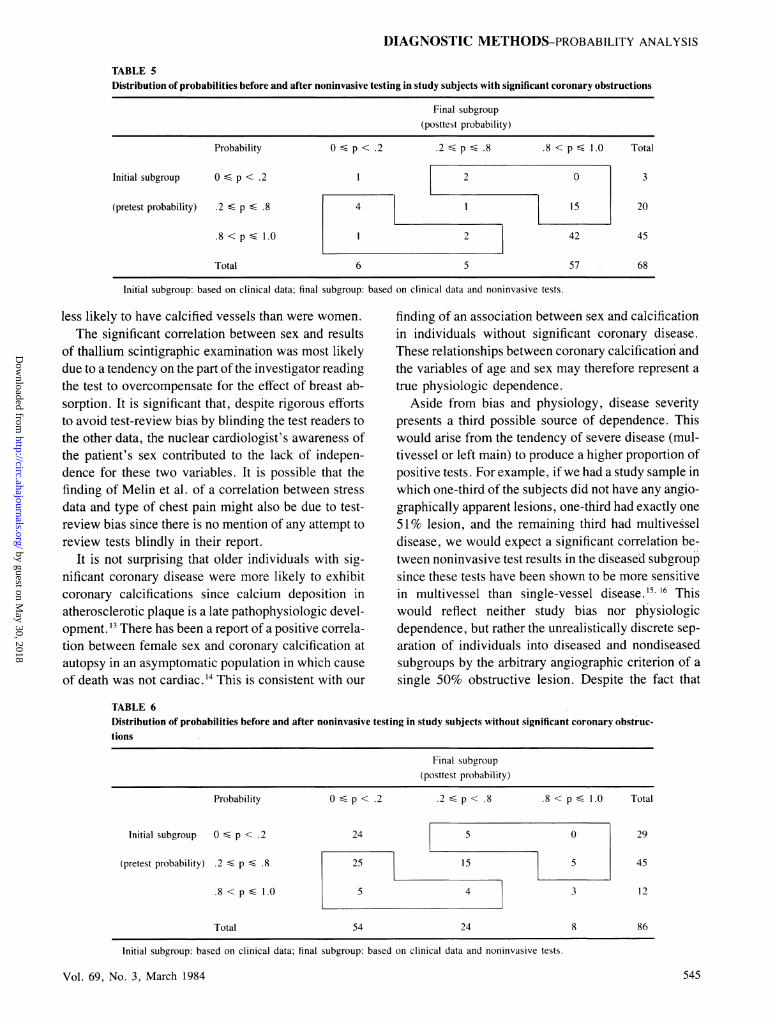
Initial and final probability distributions. Tables 5 and6 give the number of patients who were initially placedin a low-, intermediate-, or high-probability subgroupon the basis of clinical data. They either did not moveor were transferred to another subgroup when posttestprobability of disease was calculated from their nonin-
TABLE 2Stress-induced ST depressions
Sensitivity (%) Specificity (%)
Present Pooled Present PooledST depression study literature2 study literature2
>0.5 81 86 50 631.0 70 65 68 85
> .5 49 42 83 96¢2.0 39 33 94 98>2.5 31 19 96 100
Vol. 69, No. 3, March 1984 543
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from

DETRANO et al.
TABLE 3Thallium scintigraphic results
Sensitivity (%) Specificity (%)
Present Pooled Present PooledAbnormality study literature2 study literature2
Fixed or reversible defect 82 85 81 84Reversible defect 78 71 86 94
vasive test results. Only data from patients with sig-nificant coronary disease are included in table 5, whiletable 6 contains those from subjects without disease.When the numbers in the boxes in table 5 are added, itis apparent that noninvasive testing appropriately ad-vanced 17 diseased patients by at least one probabilitysubgroup, while seven patients with disease were in-correctly moved backward. A similar analysis of table6 reveals that 34 subjects without disease were appro-priately moved into a lower subgroup after testing,while 10 were incorrectly moved up.
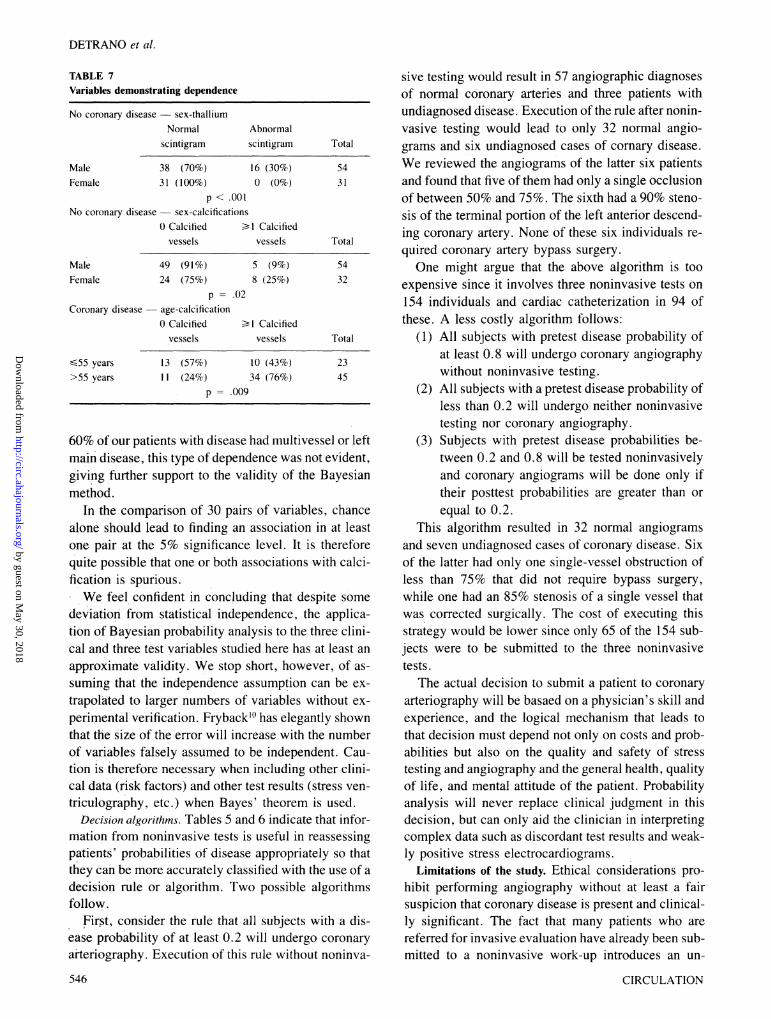
Independence. Only the two variable pairs sex-thal-lium scintigraphy and sex-coronary calcificationsshowed significant pairwise associations in the sub-jects without disease (p < .001; p = .02, respective-ly). Among the subjects with disease only age andcalcification were related (p = .009). Table 7 illus-trates these relationships. Care must be taken in inter-preting these associations since by chance alone somecorrelations would be expected when making compari-sons between a large number of variable pairs andwhen a significance level of .05 is used.
DiscussionThe utility of diagnostic testing depends on its abili-
ty to refine the clinician's capacity to distinguish indi-viduals with disease from those without. Since anysingle noninvasive test can add only a limited amountof information for the clinical assessment of patientswith suspected coronary artery disease, there havebeen attempts to combine tests in order to better predictthe presence or absence of disease.S9
Bayes' theorem allows probabilistic revision of di-agnostic assessments by incorporating new informa-tion made available by multiple noninvasive tests. Thetheorem has been applied in this way, but before thisstudy its utility in improving clinical predictions ofcoronary disease had not been demonstrated. Diamondet al. .3using a method very similar to our own, at-tempted to document the applicability of the theorembut failed to verify that posttest probabilities were sig-nificantly better in correctly classifying patients thanthose based on clinical data. In their work angiograph-544
ic assessment of coronary disease was accomplished inonly 15% of an original group of 1097 patients whounderwent clinical and noninvasive evaluations. Sincethe decision to defer angiography in the other 85% wasbased on data from the noninvasive work-up, a biaswas introduced that overemphasized falsely high andunderemphasized falsely low posttest probabilities.Since our protocol did not allow the exercise test re-sults to be used in the decision of whether or not toperform angiography, relatively few subjects (3%)dropped out because of negative test results. This factundoubtedly increased the ability of our posttest prob-abilities to correctly classify patients.
Independence. One theoretical objection to the use ofBayesian probability analysis in the general case,"' andin the particular case of coronary artery disease, hasbeen the lack of experimental verification of the statis-tical independence of test results and clinical data,independence meaning that the conditional probabil-ities on the right side of Bayes' theorem depend onneither the clinical variables used to estimate the pre-test probabilities nor on the other noninvasive test re-sults. Such independence is a necessary condition forthe valid use of the theorem in this form. Some evi-dence of independence of these variables has beenshown in a small group of 43 subjects, 1" but the routineuse of as many as 20 variables'2 has not been experi-mentally justified. In fact, the finding of Melin et al.6that the sensitivities of stress electrocardiography andstress thallium scintigraphy depend on type of chestpain seems at first glance to negate the hypothesis ofindependence.Our results differ from those of Melin et al. in that
significant pairwise association was found for onlythree of 30 possible pairings of the six variables andthere was no pairwise association between test varia-bles. We specifically found an inordinate number ofwomen without disease with negative stress thalliumscintigrams and we found that older individuals withcoronary disease were more likely to have fluoroscopicevidence of coronary calcifications than younger sub-jects. We also found that men without disease were
TABLE 4Cine fluoroscopically detected coronary calcifications
No. of Sensitivity (%) Specificity (%)calcified Present Pooled Present Pooledvessels study literature2 study literature2
¢1 65 58 85 96¢2 29 34 97 983 12 14 99 100
CIRCULATION
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from
DIAGNOSTIC METHODS-PROBABILITY ANALYSIS
TABLE 5Distribution of probabilities before and after noninvasive testing in study subjects with significant coronary obstructions
Final subgroup(posttest probability)
Probability 0 ' p < .2 .2 , p .8 .8 < p 1.0 Total
Initial subgroup 0 S p < .2 1 2 0 3
(pretest probability) .2 S p S .8 4 I 15 20
.8<pS l.0 1 2 42 45
Total 6 5 57 68
Initial subgroup: based on clinical data; final subgroup: based on clinical data and noninvasive tests.
less likely to have calcified vessels than were women.The significant correlation between sex and results
of thallium scintigraphic examination was most likelydue to a tendency on the part of the investigator readingthe test to overcompensate for the effect of breast ab-sorption. It is significant that, despite rigorous effortsto avoid test-review bias by blinding the test readers tothe other data, the nuclear cardiologist's awareness ofthe patient's sex contributed to the lack of indepen-dence for these two variables. It is possible that thefinding of Melin et al. of a correlation between stressdata and type of chest pain might also be due to test-review bias since there is no mention of any attempt toreview tests blindly in their report.
It is not surprising that older individuals with sig-nificant coronary disease were more likely to exhibitcoronary calcifications since calcium deposition inatherosclerotic plaque is a late pathophysiologic devel-opment. 13 There has been a report of a positive correla-tion between female sex and coronary calcification atautopsy in an asymptomatic population in which causeof death was not cardiac.'4 This is consistent with our
finding of an association between sex and calcificationin individuals without significant coronary disease.These relationships between coronary calcification andthe variables of age and sex may therefore represent atrue physiologic dependence.
Aside from bias and physiology, disease severitypresents a third possible source of dependence. Thiswould arise from the tendency of severe disease (mul-tivessel or left main) to produce a higher proportion ofpositive tests. For example, if we had a study sample inwhich one-third of the subjects did not have any angio-graphically apparent lesions, one-third had exactly one51% lesion, and the remaining third had multivesseldisease, we would expect a significant correlation be-tween noninvasive test results in the diseased subgroupsince these tests have been shown to be more sensitivein multivessel than single-vessel disease. 5. 16 Thiswould reflect neither study bias nor physiologicdependence, but rather the unrealistically discrete sep-aration of individuals into diseased and nondiseasedsubgroups by the arbitrary angiographic criterion of asingle 50% obstructive lesion. Despite the fact that
TABLE 6Distribution of probabilities before and after noninvasive testing in study subjects without significant coronary obstruc-tions
Final subgroup(posttest probability)
Probability 0 p < .2 .2 p < .8 .8 < p .0 Total
Initial subgroup 0 S p < .2 24 5 0 29
(pretest probability) .2 < p U .8 25 15 5 45
.8<ps l.0 5 4 3 12
Total 54 24 8 86
Initial subgroup: based on clinical data; final subgroup: based on clinical data and noninvasive tests.
Vol. 69, No. 3. March 1984 545
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from
DETRANO et al.
TABLE 7Variables demonstrating dependence
No coronary disease -sex-thalliumNormal
scintigram
MaleFemale
38 (70%)31 (100%)
Abnormalscintigram
16 (30%)0 (0%)
p < .001No coronary disease sex-calcifications
0 Calcified >1 Calcifiedvessels vessels
MaleFemale
Coronary disease
sf55 years>55 years
49 (91%)24 (75%)
p = .(age-calcification0 Calcified
vessels
5 (9%)8 (25%)
[)2
BI Calcifiedvessels
13 (57%) 10 (43%)11 (24%) 34 (76%)
p = .009
Total
5431
Total
5432
Total
2345
60% of our patients with disease had multivessel or leftmain disease, this type of dependence was not evident,giving further support to the validity of the Bayesianmethod.
In the comparison of 30 pairs of variables, chancealone should lead to finding an association in at leastone pair at the 5% significance level. It is thereforequite possible that one or both associations with calci-fication is spurious.We feel confident in concluding that despite some
deviation from statistical independence, the applica-tion of Bayesian probability analysis to the three clini-cal and three test variables studied here has at least anapproximate validity. We stop short, however, of as-suming that the independence assumption can be ex-trapolated to larger numbers of variables without ex-perimental verification. Frybacklt has elegantly shownthat the size of the error will increase with the numberof variables falsely assumed to be independent. Cau-tion is therefore necessary when including other clini-cal data (risk factors) and other test results (stress ven-triculography, etc.) when Bayes' theorem is used.
Decision algorithms. Tables 5 and 6 indicate that infor-mation from noninvasive tests is useful in reassessingpatients' probabilities of disease appropriately so thatthey can be more accurately classified with the use of adecision rule or algorithm. Two possible algorithmsfollow.
First, consider the rule that all subjects with a dis-ease probability of at least 0.2 will undergo coronaryarteriography. Execution of this rule without noninva-
546
sive testing would result in 57 angiographic diagnosesof normal coronary arteries and three patients withundiagnosed disease. Execution of the rule after nonin-vasive testing would lead to only 32 normal angio-grams and six undiagnosed cases of comary disease.We reviewed the angiograms of the latter six patientsand found that five of them had only a single occlusionof between 50% and 75%. The sixth had a 90% steno-sis of the terminal portion of the left anterior descend-ing coronary artery. None of these six individuals re-quired coronary artery bypass surgery.One might argue that the above algorithm is too
expensive since it involves three noninvasive tests on154 individuals and cardiac catheterization in 94 ofthese. A less costly algorithm follows:
(1) All subjects with pretest disease probability ofat least 0.8 will undergo coronary angiographywithout noninvasive testing.
(2) All subjects with a pretest disease probability ofless than 0.2 will undergo neither noninvasivetesting nor coronary angiography.
(3) Subjects with pretest disease probabilities be-tween 0.2 and 0.8 will be tested noninvasivelyand coronary angiograms will be done only iftheir posttest probabilities are greater than orequal to 0.2.
This algorithm resulted in 32 normal angiogramsand seven undiagnosed cases of coronary disease. Sixof the latter had only one single-vessel obstruction ofless than 75% that did not require bypass surgery,while one had an 85% stenosis of a single vessel thatwas corrected surgically. The cost of executing thisstrategy would be lower since only 65 of the 154 sub-jects were to be submitted to the three noninvasivetests.
The actual decision to submit a patient to coronaryarteriography will be basaed on a physician's skill andexperience, and the logical mechanism that leads tothat decision must depend not only on costs and prob-abilities but also on the quality and safety of stresstesting and angiography and the general health, qualityof life, and mental attitude of the patient. Probabilityanalysis will never replace clinical judgment in thisdecision, but can only aid the clinician in interpretingcomplex data such as discordant test results and weak-ly positive stress electrocardiograms.
Limitations of the study. Ethical considerations pro-hibit performing angiography without at least a fairsuspicion that coronary disease is present and clinical-ly significant. The fact that many patients who arereferred for invasive evaluation have already been sub-mitted to a noninvasive work-up introduces an un-
CIRCULATION
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from

DIAGNOSTIC METHODS-PROBABILITY ANALYSIS
avoidable selection bias. The degree of this bias will bereflected in the number of abnormal angiograms. Sinceonly 44% of our study sample had significantly abnor-mal coronary arteries by angiography, we are confi-dent that we have decreased this bias.We conclude from our results that pairwise if not
mutual statistical independence, although imperfect, isat least an approximately valid assumption. The limit-ed size of our study sample may hide subtle associ-ations that could only be revealed by studying a largergroup of patients.
The conditional probabilities on the right side ofBayes' theorem were calculated by Diamond and For-rester2 as weighted averages of several results from theliterature for the corresponding noninvasive tests. Theelectrocardiographic stress test literature in particularis notorious for the wide range of values for the sensi-tivity and specificity of ST segment depressions. Phil-brick et al.17 reviewed this subject and concluded thatthis variability was as much due to methodologic biasas it was to inconsistencies in the criteria for abnormaltests and difference in leads and stress protocol. Ourown review of the publications selected by Diamondand Forrester revealed similar biases, inconsistencies,and differences.
Although the sensitivities and specificities of exer-cise thallium imaging and fluoroscopy for diagnosingcoronary calcifications are less variable than those ofstress electrocardiography, inconsistencies in themethods of performance and analysis that were presentin the reports of the studies reviewed by Diamond andForrester and differences between these and our ownmethods of performance and analysis also limit thevalidity of our application of the pooled values of con-ditional probabilities to our study group's test results.Not surprisingly, the test sensitivities and specific-
ities derived from our study sample for various thresh-old test criteria were different from those of the pooledliterature that we used in Bayes' theorem (tables 2through 4). Despite these differences, Bayes' theoremperformed remarkably well in separating subjects withdisease from those without it.We conclude that, despite some limitations, this
application of Bayes' theorem has approximate valid-ity and is clinically useful in the noninvasive diagnosisof coronary artery disease.
The help of Helga Lombardo in screening patients for thisstudy was invaluable. The abstracting assistance of Rona Baker
and Marcie Kaiser, and the secretarial assistance of Paula La-Manna are deeply appreciated.
References1. Ingelfinger JA, Mosteller F, Thibodeau LA, Wane JH: Biostatis-
tics in clinical medicine. New York, 1983, McMillan, pp 1-242. Diamond GA, Forrester JS: Analysis of probability as an aid in the
clinical diagnosis of coronary artery disease. N Engl J Med 300:1350, 1979
3. Diamond GA, Staniloff HM, Forrestser JS, Pollock BH, SwanHJC; Computer-assisted diagnosis in the non-invasive evaluationof patients with suspected coronary artery disease. J Am Col Car-diol 1: 444, 1983
4. Feinstein AR: The haze of Bayes. The aerial palaces of decisionanalysis and the computerized Ouija board. Clin Pharmacol Ther21: 482, 1977
5. Maclntyre WJ, Go RT, Cook SA: Comparison of stress and redis-tribution thallium planar imaging with a single proton transaxialtomographic technique. In Raymond C, editor: Nuclear medicineand biology. Paris, 1982, Pergamon Press
6. Melin JA, Piret LJ, Vanbutsele RJ, Rousseau MI, Cosyns J, Bras-seur LA, Beckers C, Detry JR: Diagnostic value of exercise elec-trocardiography and Thallium myocardial scintigraphy in patientswithout previous myocardial infarction: a Bayesian approach. Cir-culation 63: 1019, 1981
7. Patterson RE, Horowitz SF, Eng C, Rudin A, Meller J, HalgashDA, Pichard AD, Goldsmith SJ, Herman MV, Gorlin R: Canexercise electrocardiography and Thallium-201 myocardial imag-ing exclude the diagnosis of coronary artery disease? Am J Cardiol49: 1127, 1982
8. McCarthy DM, Sciacca RR, Bloud DK, Cannon PJ: Discriminantfunction analysis using Thallium-201 scintiscans and exercisestress test variables to predict the presence and extent of coronaryartery disease. Am J Cardiol 49: 1917, 1982
9. Aldrich RF, Brensike JF, Battaglini JW, Richardson JM, Loh IK,Stone NJ, Passamani ER, Ackerstein H, Seningea R, Borer JS,Levy RI, Epstein SE: Coronary calcifications in the detection ofcoronary artery disease and comparison with electrocardiographicexercise testing. Circulation 59: 1113, 1979
10. Fryback DG: Bayes theorem and conditional nonindependence ofdata in medical diagnosis. Computers Biomed Res 11: 423, 1978
11. Charuzi Y, Diamond GA, Pichler M, Waxman A, Vas R, Silver-berg RA, Berman DS, Forrester JS: Analysis of multiple non-invasive test procedures for the diagnosis of coronary artery dis-ease. Clin Cardiol 4: 67, 1981
12. Pollock BH, Slaniloff HM, Diamond GA: Computer assisted inter-pretation of non-invasive tests for the diagnosis of coronary arterydisease. Cardiovasc Review Rep 4: 367, 1983
13. Warburton RK, Tampas JP, Soule AB, Taylor HC: Coronary arterycalcification. Its relationship to coronary artery stenosis and myo-cardial infarction. Radiology 91: 109, 1968
14. Eggen DA, Strong JP, McGill HC: Coronary calcification: relationto clinically significant coronary lesions and race, sex and topo-graphic distribution. Circulation 32: 948, 1965
15. Dash H, Massie BM, Botvinick EH, Brundage BH: The non-invasive identification of left main and three vessel coronary arterydisease by myocardial stress perfusion scintigraphy and treadmillexercise electrocardiography. Circulation 60: 276, 1979
16. Nahormek PA, Chahene RA, Raizner AE, Thomly JI, Ishimori T,Montero A, Lochi RJ: The magnitude of exercise produced STsegment depression and the predictive value of exercise testing.Clin Cardiol 2: 286, 1979
17. Philbrick JT, Horwitz RI, Feinstein AR: Methodologic problems ofexercise testing for coronary artery disease: groups, analysis andbias. Am J Cardiol 46: 807, 1980
Vol. 69, No. 3, March 1984 547
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from

R Detrano, J Yiannikas, E E Salcedo, G Rincon, R T Go, G Williams and J Leathermandiagnosing coronary disease.
Bayesian probability analysis: a prospective demonstration of its clinical utility in
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright © 1984 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation doi: 10.1161/01.CIR.69.3.541
1984;69:541-547Circulation.
http://circ.ahajournals.org/content/69/3/541the World Wide Web at:
The online version of this article, along with updated information and services, is located on
http://circ.ahajournals.org//subscriptions/
is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer information about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. FurtherEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculationpublished in Requests for permissions to reproduce figures, tables, or portions of articles originallyPermissions:
by guest on May 30, 2018
http://circ.ahajournals.org/D
ownloaded from