before the pregnancy - tarrant county infant health...
TRANSCRIPT
BEFORE THE PREGNANCY – H OW M AT E R N A L FAC TO R S I N F LU E N C E P R E G N A N C Y O U TC O M E
Tracy Papa, D.O., FACOOG Fort Worth Perinatal Associates DrTracyPapa.com Twitter: @DrTracyPapa
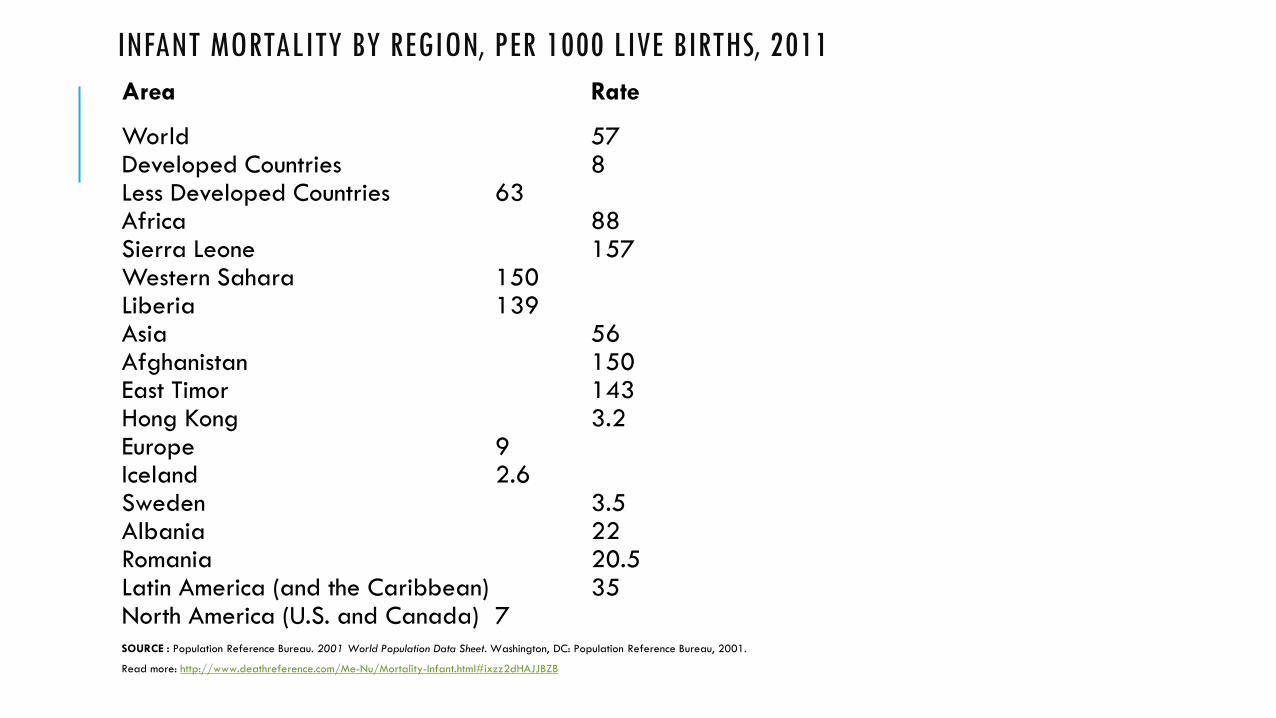
INFANT MORTALITY BY REGION, PER 1000 LIVE BIRTHS, 2011 Area Rate World 57 Developed Countries 8 Less Developed Countries 63 Africa 88 Sierra Leone 157 Western Sahara 150 Liberia 139 Asia 56 Afghanistan 150 East Timor 143 Hong Kong 3.2 Europe 9 Iceland 2.6 Sweden 3.5 Albania 22 Romania 20.5 Latin America (and the Caribbean) 35 North America (U.S. and Canada) 7 SOURCE : Population Reference Bureau. 2001 World Population Data Sheet. Washington, DC: Population Reference Bureau, 2001.
Read more: http://www.deathreference.com/Me-Nu/Mortality-Infant.html#ixzz2dHAJJBZB
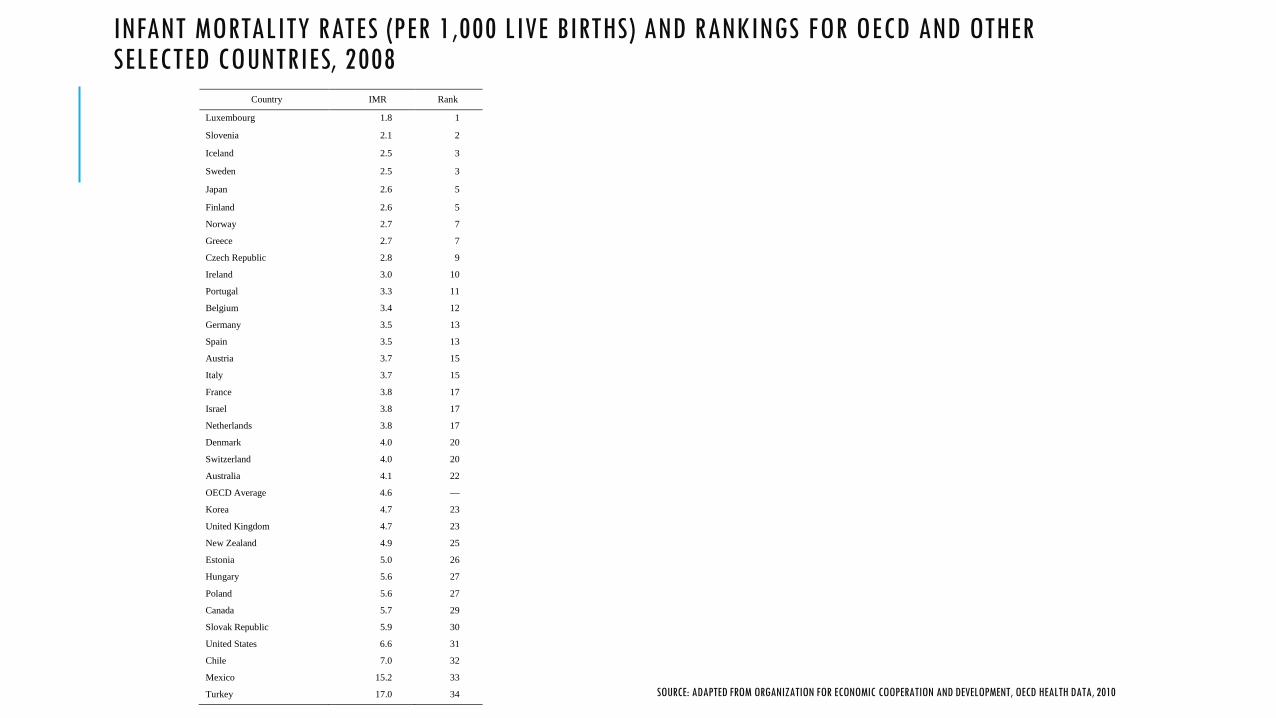
INFANT MORTALITY RATES (PER 1,000 LIVE BIRTHS) AND RANKINGS FOR OECD AND OTHER SELECTED COUNTRIES, 2008 Country IMR Rank
Luxembourg 1.8 1
Slovenia 2.1 2
Iceland 2.5 3
Sweden 2.5 3
Japan 2.6 5
Finland 2.6 5
Norway 2.7 7
Greece 2.7 7
Czech Republic 2.8 9
Ireland 3.0 10
Portugal 3.3 11
Belgium 3.4 12
Germany 3.5 13
Spain 3.5 13
Austria 3.7 15
Italy 3.7 15
France 3.8 17
Israel 3.8 17
Netherlands 3.8 17
Denmark 4.0 20
Switzerland 4.0 20
Australia 4.1 22
OECD Average 4.6 —
Korea 4.7 23
United Kingdom 4.7 23
New Zealand 4.9 25
Estonia 5.0 26
Hungary 5.6 27
Poland 5.6 27
Canada 5.7 29
Slovak Republic 5.9 30
United States 6.6 31
Chile 7.0 32
Mexico 15.2 33
Turkey 17.0 34
SOURCE: ADAPTED FROM ORGANIZATION FOR ECONOMIC COOPERATION AND DEVELOPMENT, OECD HEALTH DATA, 2010
FACTORS THAT MAY CONTRIBUTE TO RELATIVELY HIGH U.S. IMR
Inconsistent recording of live births
Different rates of low birth weight and preterm births
Racial and ethnic IMR disparities
SOURCE: ADAPTED FROM ORGANIZATION FOR ECONOMIC COOPERATION AND DEVELOPMENT, OECD HEALTH DATA, 2010
PREMATURITY AND LOW BIRTH WEIGHT IN U.S.
Preterm birth much more common in U.S. than in Europe Double that of Scandinavian countries
If U.S. had same rate of preterm birth as Sweden, CDC estimates that our IMR would be 3.9
Reducing preterm birth/low birth weight in U.S. would lower IMR
OECD suggests that the increasing rate of preterm/LBW infants may explain stagnation in U.S. IMR
BEHIND INTERNATIONAL RANKINGS OF INFANT MORTALITY: HOW THE UNITED STATES COMPARES WITH EUROPE, U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES: CENTERS FOR DISEASE CONTROL AND PREVENTION: NATIONAL CENTER FOR HEALTH STATISTICS, NCHS DATA BRIEF NO.23, HYATTSVILLE, MD, NOVEMBER 2009
EFFECT OF RACIAL DISPARITIES ON U.S. IMR
IMR for infants of black mothers - 12.7
IMR for infants of white mothers - 5.5
Black mothers have 16% of infants in U.S., but 30% of infant deaths
Eliminating racial disparity differences would lower IMR, but we would still be higher than the OECD average of 4.6
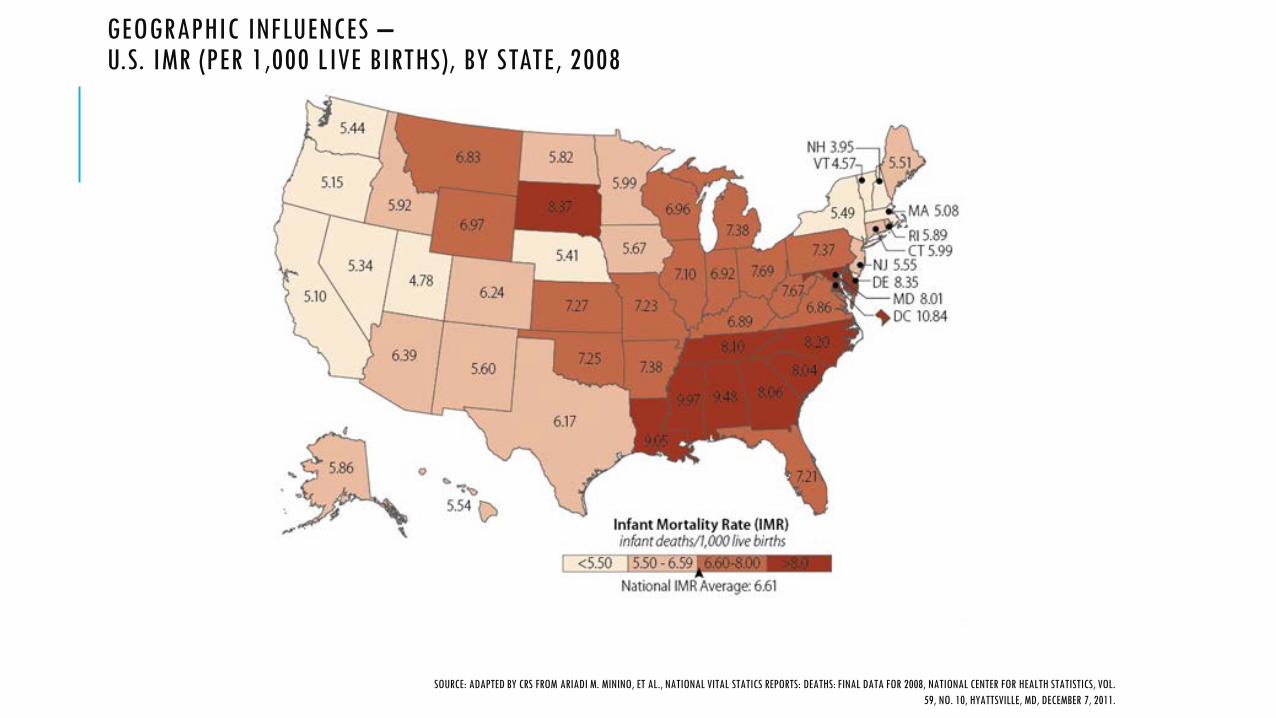
GEOGRAPHIC INFLUENCES – U.S. IMR (PER 1,000 LIVE BIRTHS), BY STATE, 2008
SOURCE: ADAPTED BY CRS FROM ARIADI M. MININO, ET AL., NATIONAL VITAL STATICS REPORTS: DEATHS: FINAL DATA FOR 2008, NATIONAL CENTER FOR HEALTH STATISTICS, VOL. 59, NO. 10, HYATTSVILLE, MD, DECEMBER 7, 2011.
TEXAS 2008
2478 infant deaths – 6 per 1000 live births Black 10 per 1000 White 6 per 1000 Hispanic 5.4 per 1000
U.S. rate 6.8 per 1000
FROM TEXAS DEPARTMENT OF STATE HEALTH SERVICES, 2011
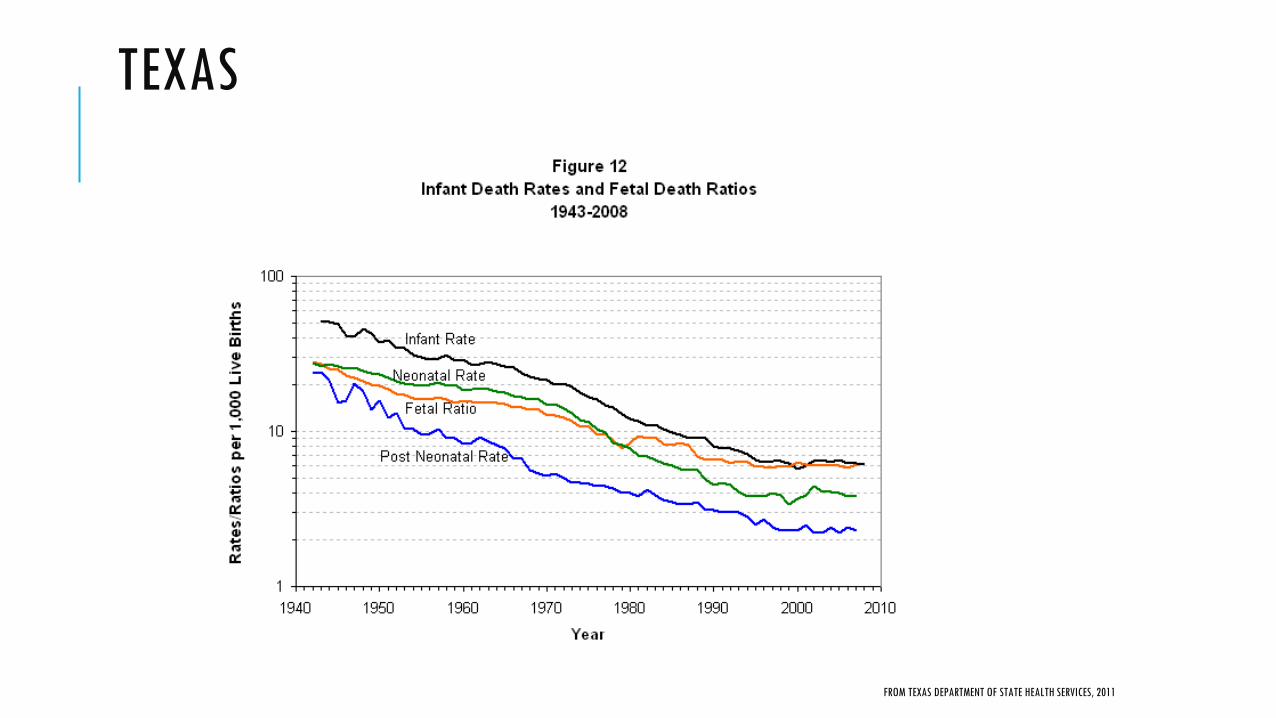
TEXAS
FROM TEXAS DEPARTMENT OF STATE HEALTH SERVICES, 2011
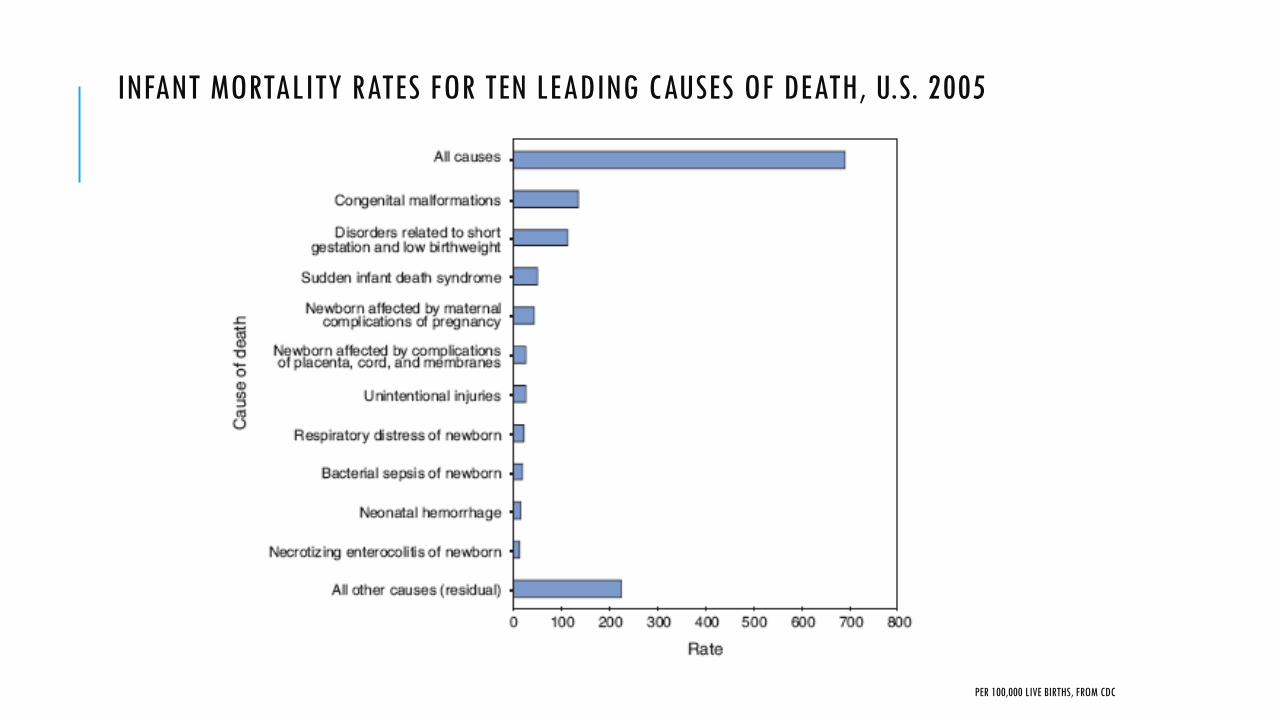
INFANT MORTALITY RATES FOR TEN LEADING CAUSES OF DEATH, U.S. 2005
PER 100,000 LIVE BIRTHS, FROM CDC
FACTORS INFLUENCING PERINATAL OUTCOME
Income
Race
Ethnicity
Age
Preconception health
SOURCE: CDC
Age Preconception health Maternal obesity Maternal diabetes
TEEN PREGNANCY
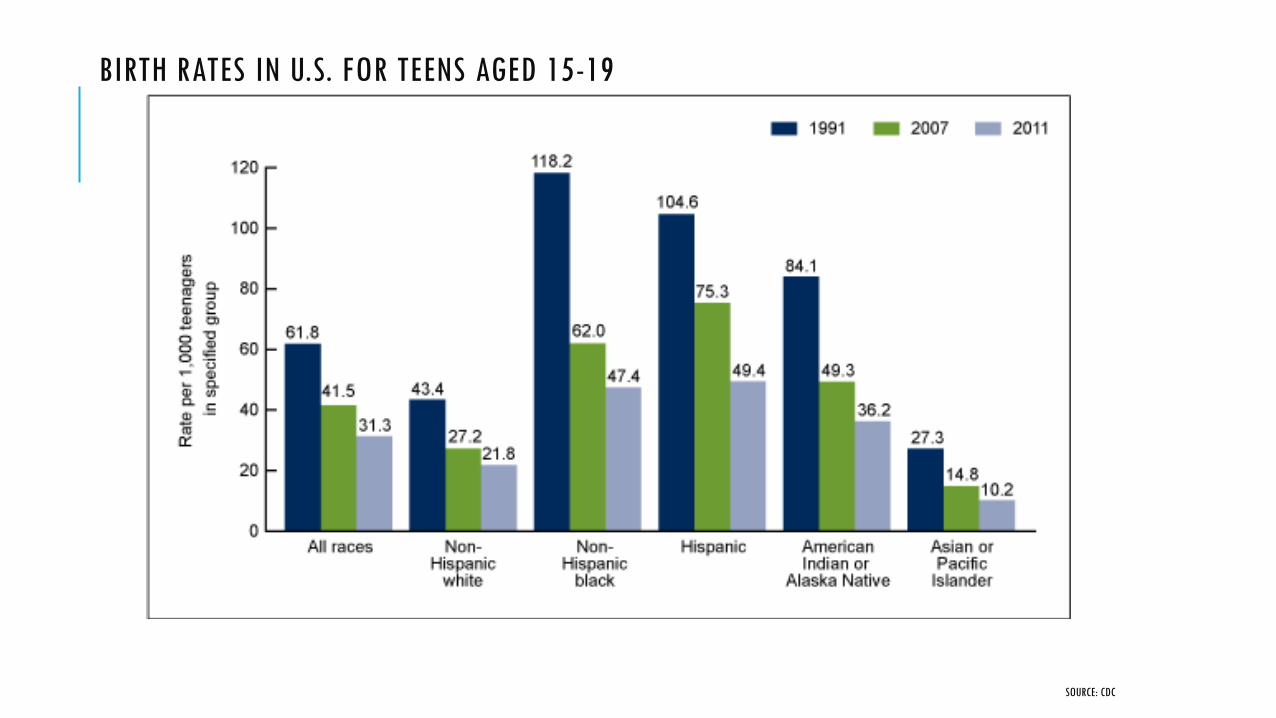
BIRTH RATES IN U.S. FOR TEENS AGED 15-19
SOURCE: CDC
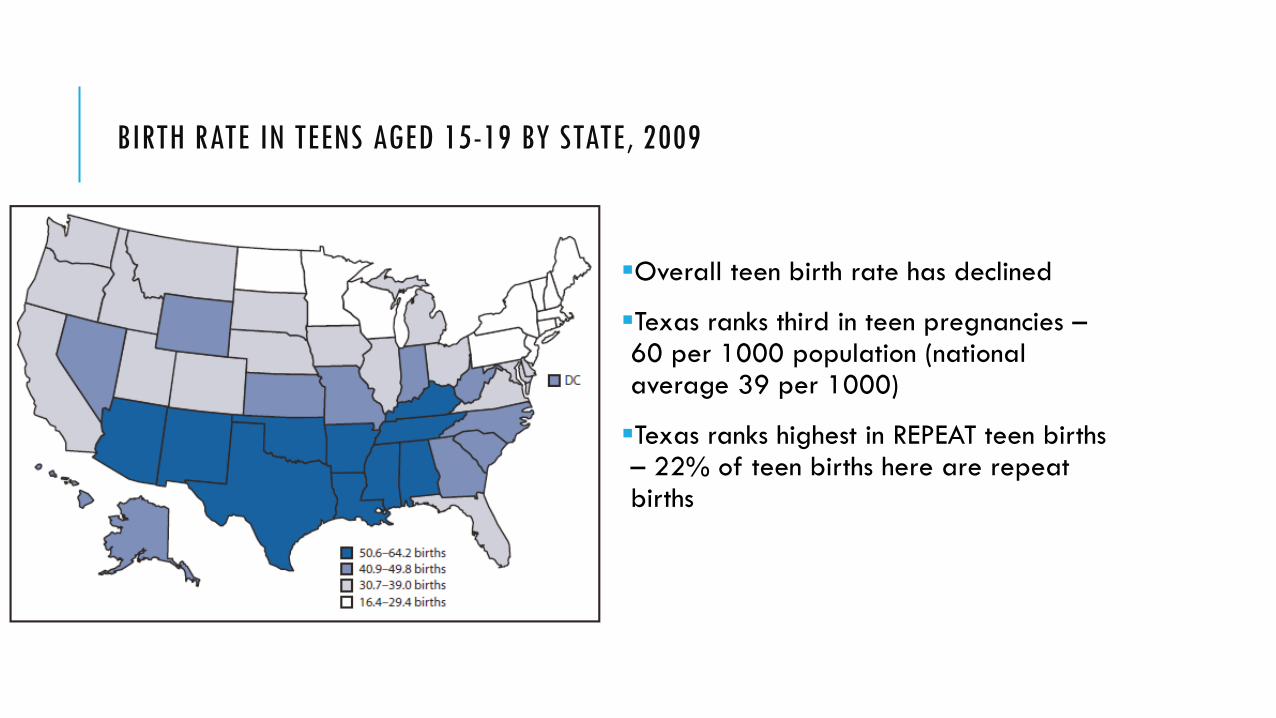
BIRTH RATE IN TEENS AGED 15-19 BY STATE, 2009
Overall teen birth rate has declined
Texas ranks third in teen pregnancies – 60 per 1000 population (national average 39 per 1000)
Texas ranks highest in REPEAT teen births – 22% of teen births here are repeat births


MATERNAL OBESITY
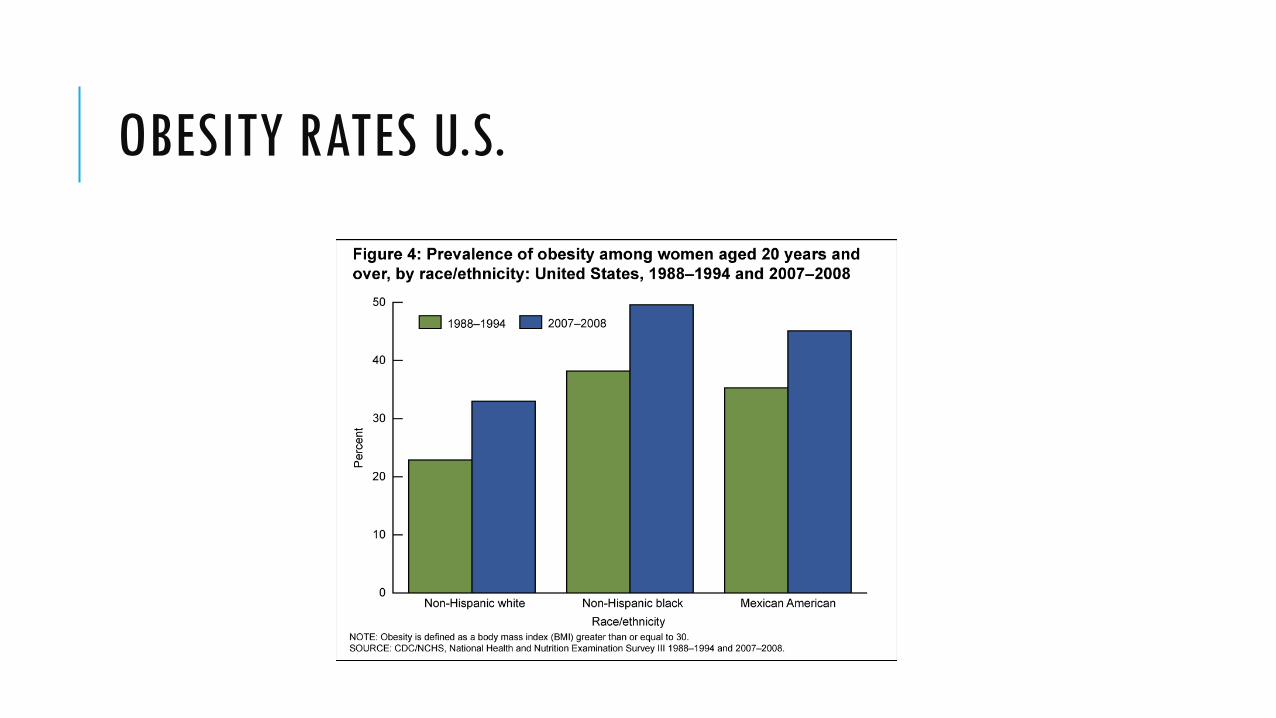
OBESITY RATES U.S.
• Normal weight – BMI 18.5 – 24.9 • Overweight – BMI 25 – 29.9 • Obese – BMI ≥ 30
• Class I – BMI 30 – 34.9 • Class II – BMI 35 – 39.9 • Class III (extreme) – BMI ≥ 40
NIH/WHO DEFINITIONS BMI = KG/M²
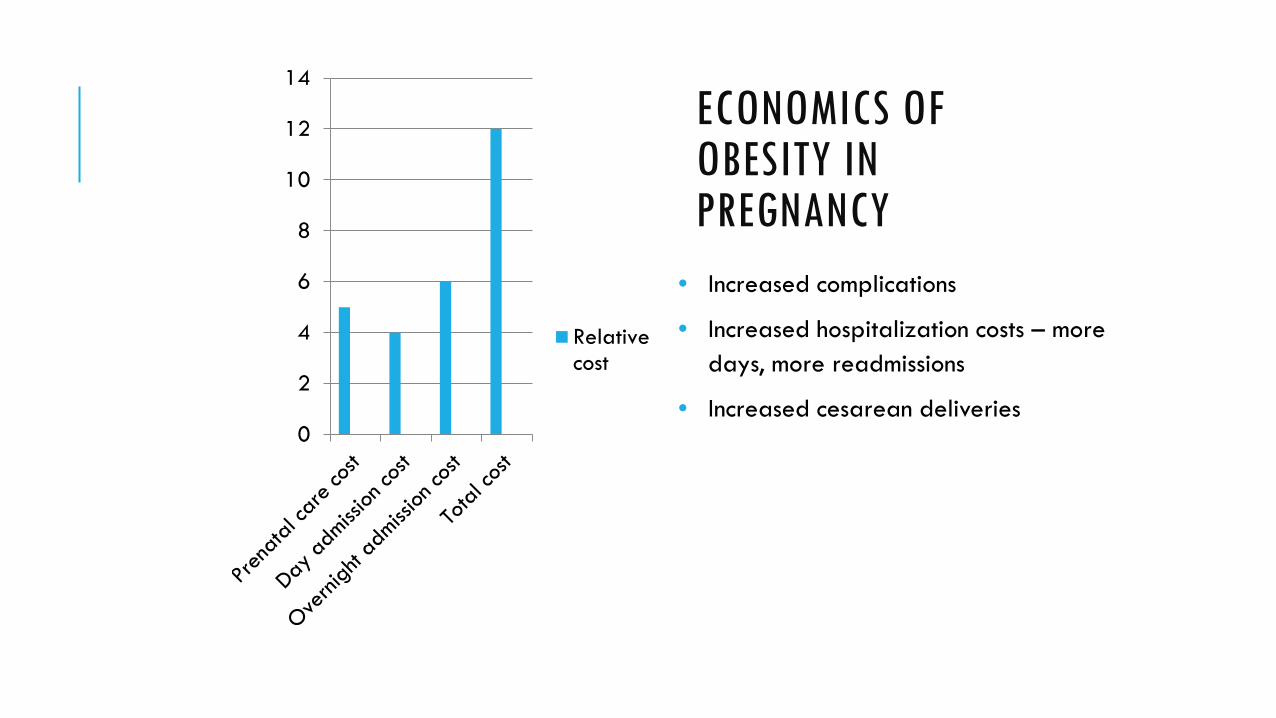
ECONOMICS OF OBESITY IN PREGNANCY
0
2
4
6
8
10
12
14
Relativecost
• Increased complications
• Increased hospitalization costs – more days, more readmissions
• Increased cesarean deliveries
Gestational diabetes
Preeclampsia
Cesarean delivery Increased surgical and anesthesia risks Increased operative time and blood loss
Babies have increased risk of: Neural tube defects Stillbirth Prematurity Macrosomia
COMPLICATIONS OF OBESITY
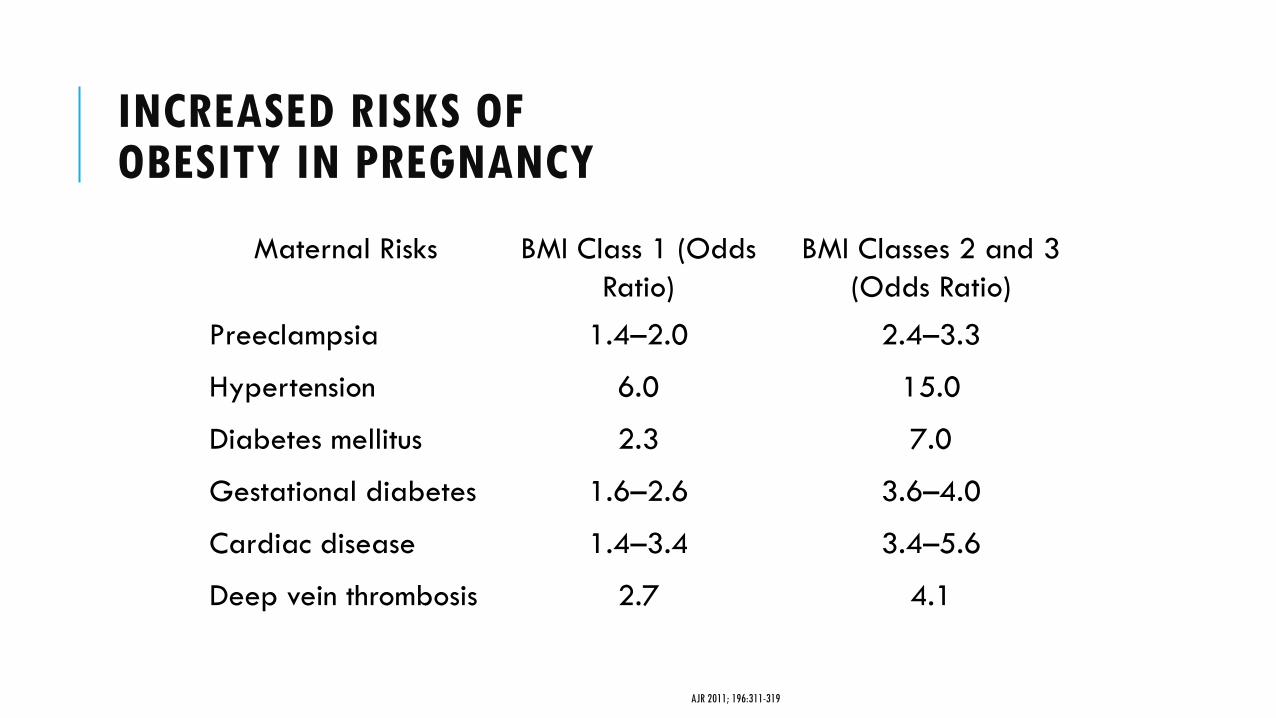
Maternal Risks BMI Class 1 (Odds Ratio)
BMI Classes 2 and 3 (Odds Ratio)
Preeclampsia 1.4–2.0 2.4–3.3
Hypertension 6.0 15.0
Diabetes mellitus 2.3 7.0
Gestational diabetes 1.6–2.6 3.6–4.0
Cardiac disease 1.4–3.4 3.4–5.6
Deep vein thrombosis 2.7 4.1
INCREASED RISKS OF OBESITY IN PREGNANCY
AJR 2011; 196:311-319
Information Review risks and outcomes for obesity
Intervention Weight loss/exercise counseling Bariatric surgery Folate supplementation
Screening for comorbid conditions Hypertension Diabetes Thyroid disease
PRECONCEPTION COUNSELING IN OBESITY

Reduce BMI prior to pregnancy, avoid weight loss attempts during pregnancy
Ideally, women should have BMI <25-30 prior to pregnancy
Minimal weight gain improves pregnancy outcome
Initial goal – reduce total weight by 5-10% over 6 months
Exercise 30 minutes/day, increase tolerance to 60 minutes daily
PRECONCEPTION GOALS
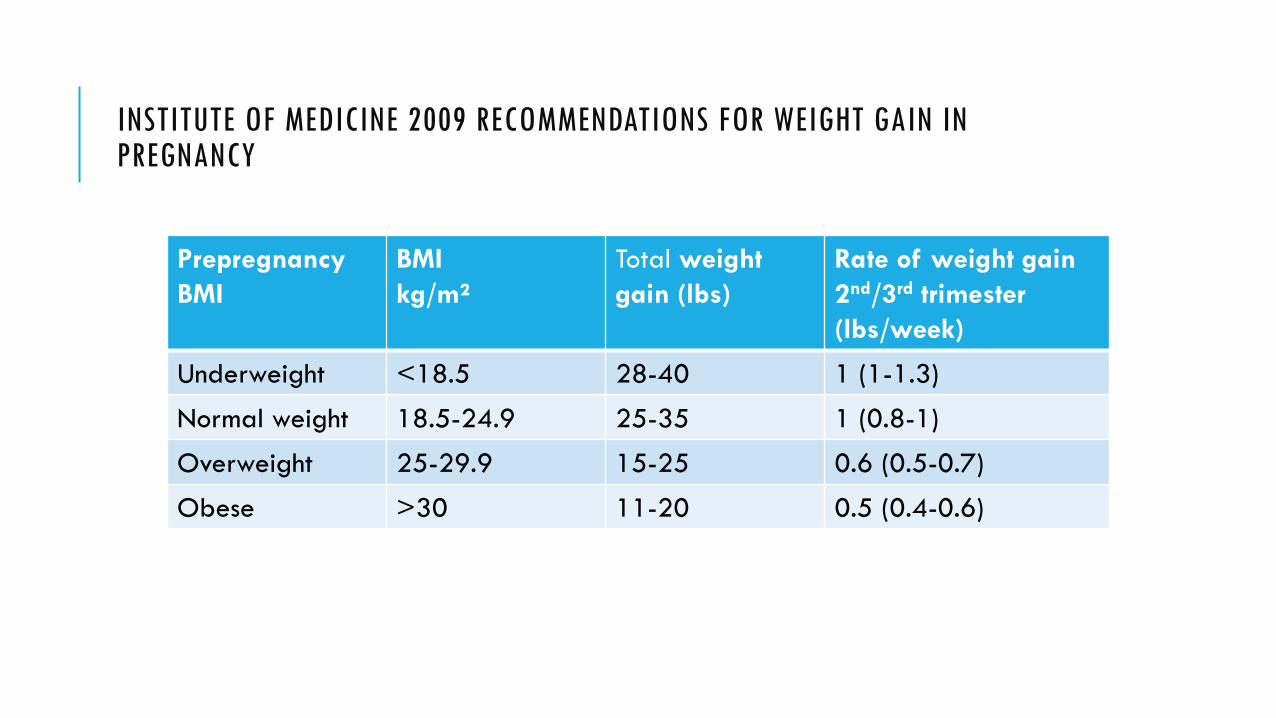
Prepregnancy BMI
BMI kg/m²
Total weight gain (lbs)
Rate of weight gain 2nd/3rd trimester (lbs/week)
Underweight <18.5 28-40 1 (1-1.3)
Normal weight 18.5-24.9 25-35 1 (0.8-1)
Overweight 25-29.9 15-25 0.6 (0.5-0.7)
Obese >30 11-20 0.5 (0.4-0.6)
INSTITUTE OF MEDICINE 2009 RECOMMENDATIONS FOR WEIGHT GAIN IN PREGNANCY
First and second trimester serum screens affected by maternal obesity
Screens depend on serum analytes to determine risk of aneuploidy
Plasma markers adjusted upward for obesity (increased plasma volume)
MSAFP adjusted up to maternal weight of 200 lbs. Higher weights have lower MoM and increased risk of positive Down syndrome screen
EFFECT OF OBESITY ON PRENATAL SCREENING
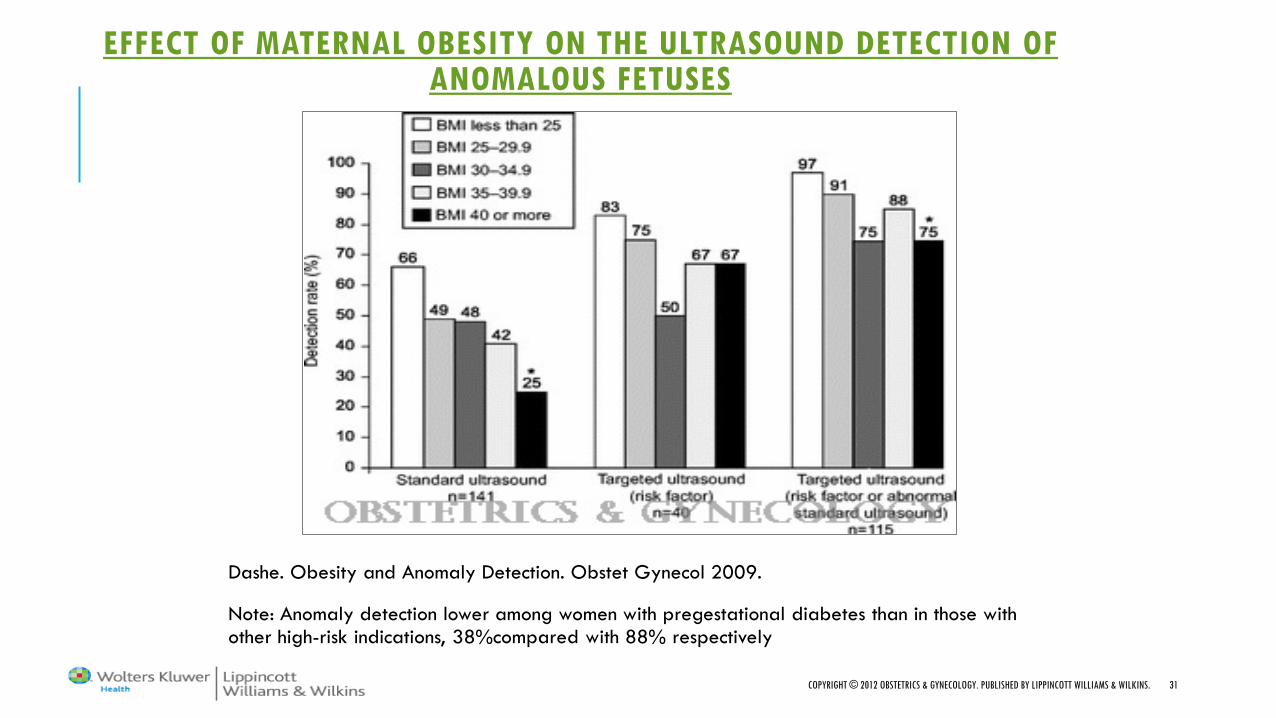
EFFECT OF MATERNAL OBESITY ON THE ULTRASOUND DETECTION OF ANOMALOUS FETUSES
Dashe. Obesity and Anomaly Detection. Obstet Gynecol 2009.
Note: Anomaly detection lower among women with pregestational diabetes than in those with other high-risk indications, 38%compared with 88% respectively
COPYRIGHT © 2012 OBSTETRICS & GYNECOLOGY. PUBLISHED BY LIPPINCOTT WILLIAMS & WILKINS. 31

COPYRIGHT © 2012 OBSTETRICS & GYNECOLOGY. PUBLISHED BY LIPPINCOTT WILLIAMS & WILKINS. 32
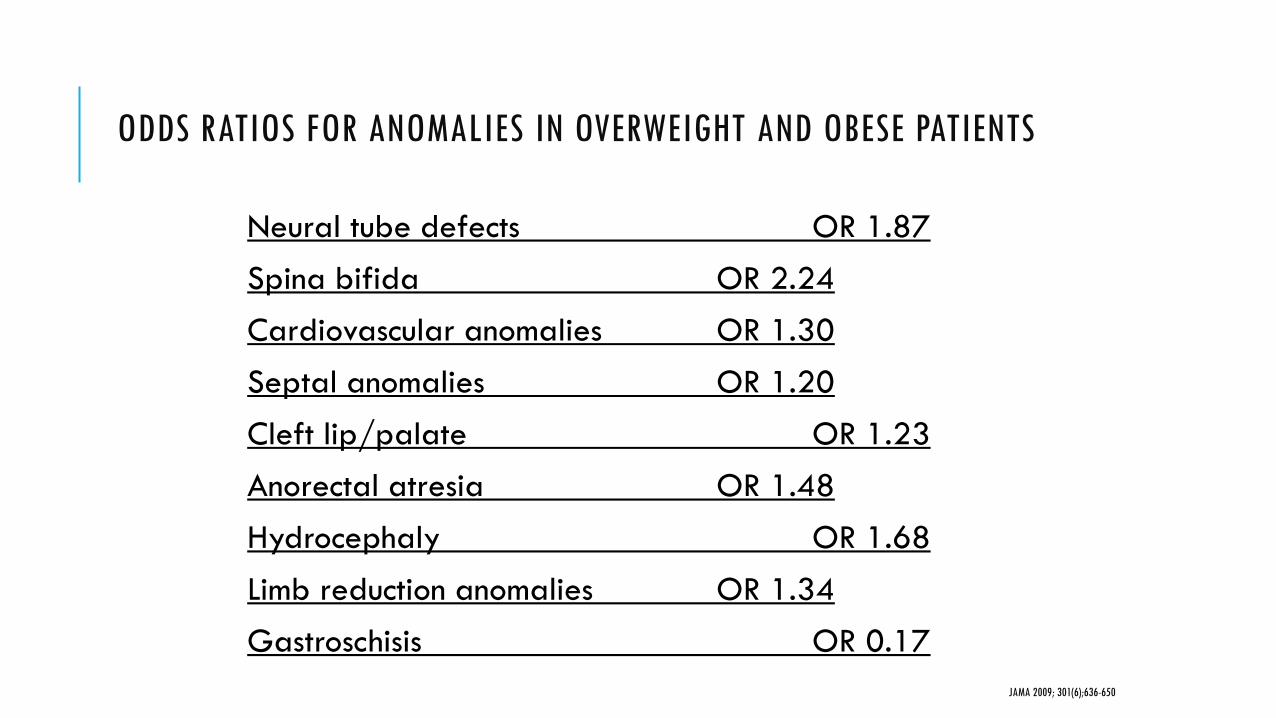
Neural tube defects OR 1.87
Spina bifida OR 2.24 Cardiovascular anomalies OR 1.30
Septal anomalies OR 1.20
Cleft lip/palate OR 1.23 Anorectal atresia OR 1.48
Hydrocephaly OR 1.68
Limb reduction anomalies OR 1.34 Gastroschisis OR 0.17
ODDS RATIOS FOR ANOMALIES IN OVERWEIGHT AND OBESE PATIENTS
JAMA 2009; 301(6);636-650
Increased rate of stillbirth BMI 25-29.9 kg/m2 – OR 1.9-2.7 (12-15/1000) BMI > 30 kg/m2 – OR 2.1-2.8 (13-18/1000) Present even after correction for smoking, diabetes, preeclampsia
Risk appears to be greatest at later gestational ages.
Hazard ratio for stillbirth: 2.0 at 30 weeks to 4.0 at term
No ACOG recommendations regarding antepartum testing
Obstet Gynecol 2009; 113:748–61.
Am J Obstet Gynecol 2005; 193:1923-35.
Obstet Gynecol 2005;106:250–9
ANTEPARTUM SURVEILLANCE IN OBESITY
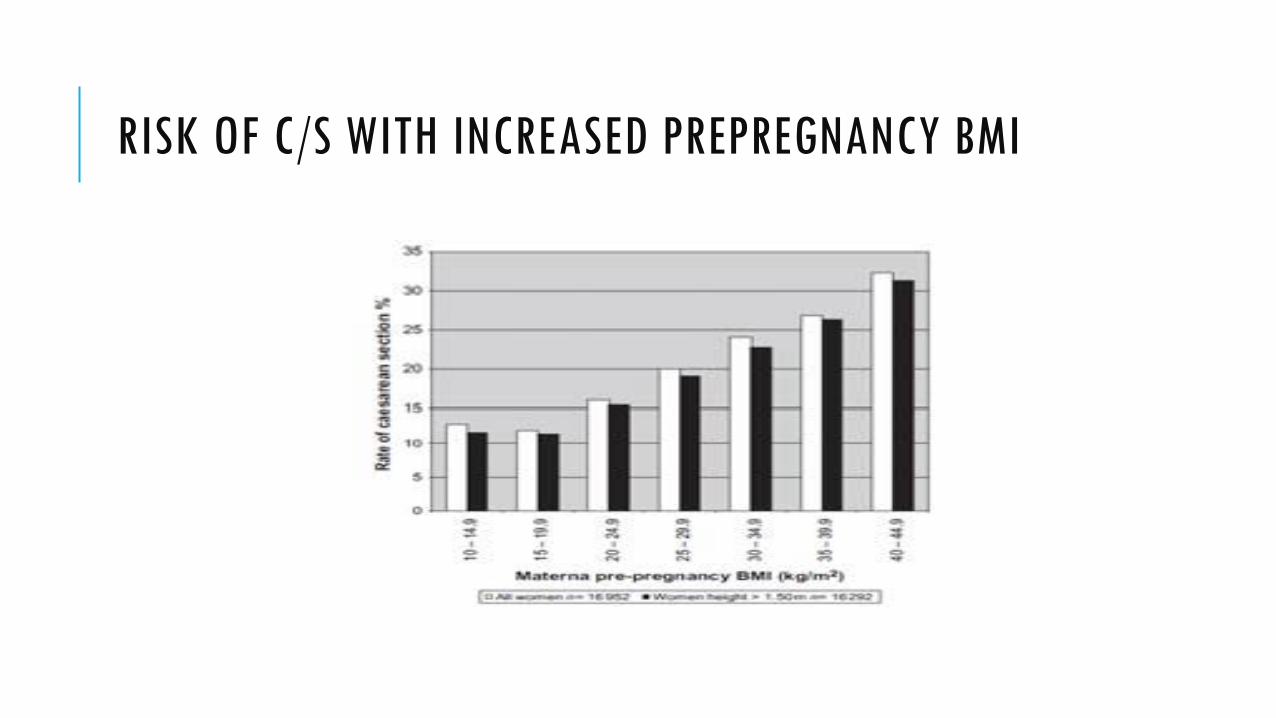
RISK OF C/S WITH INCREASED PREPREGNANCY BMI
External fetal monitoring relies on ultrasound signal
Increased rate of internal monitoring with obesity
Small studies are evaluating fetal ECG as alternative to external ultrasound monitoring
Consider anesthesia consult to evaluate anesthetic risk
Obese pregnancy increases risk of VTE Consider thromboprophylaxis based on comorbidities
INTRAPARTUM FETAL MONITORING

HOVERMATT
Relative to normal BMI women undergoing VBAC: 5 X increase in uterine rupture/dehiscence 2 X risk maternal morbidity 5 X risk in neonatal injury (fracture, brachial plexus injury, laceration) 3 X increase in 5-minute APGAR < 7
VBAC RISKS IN OBESITY
OBSTET GYNECOL 2006; 108:125-133
At Duke University, most hospital readmissions are due to wound infections related to morbid obesity.
Cost up to $60,000 per patient to treat
Centers for Medicare and Medicaid Services (CMS) have adopted payment rules that will deny reimbursement for some complications
HOSPITAL READMISSION
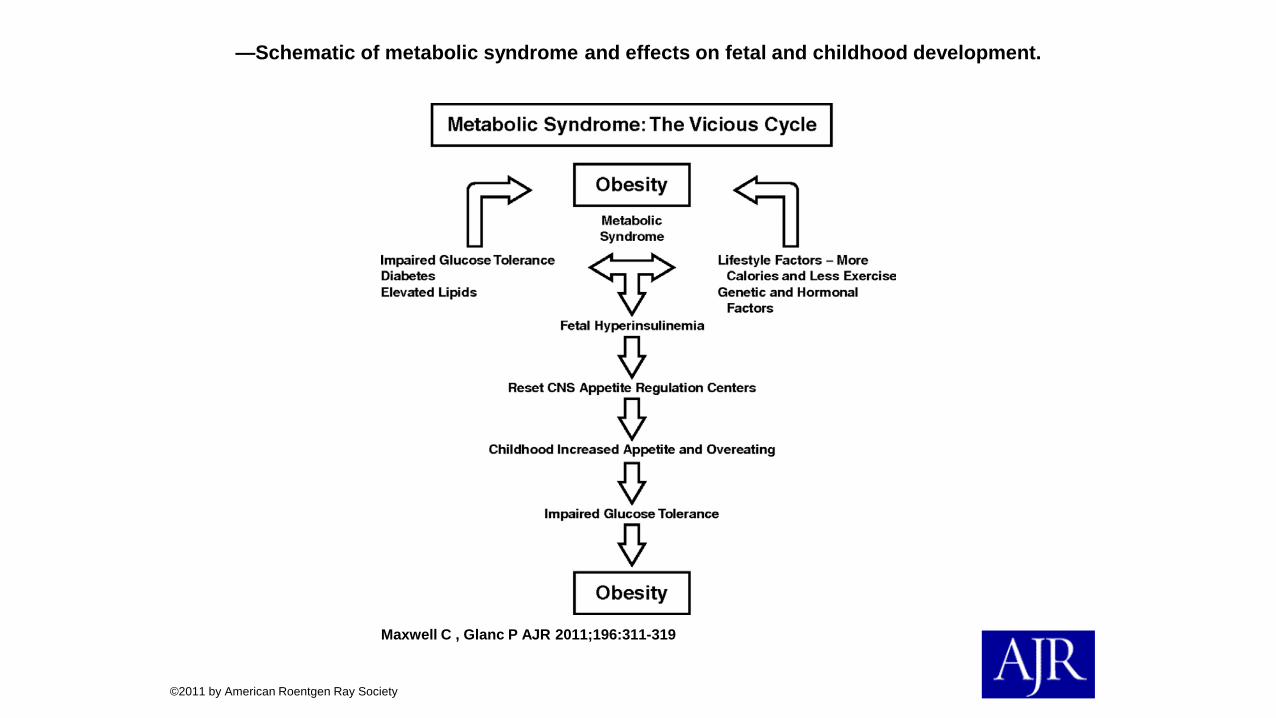
—Schematic of metabolic syndrome and effects on fetal and childhood development.
Maxwell C , Glanc P AJR 2011;196:311-319
©2011 by American Roentgen Ray Society
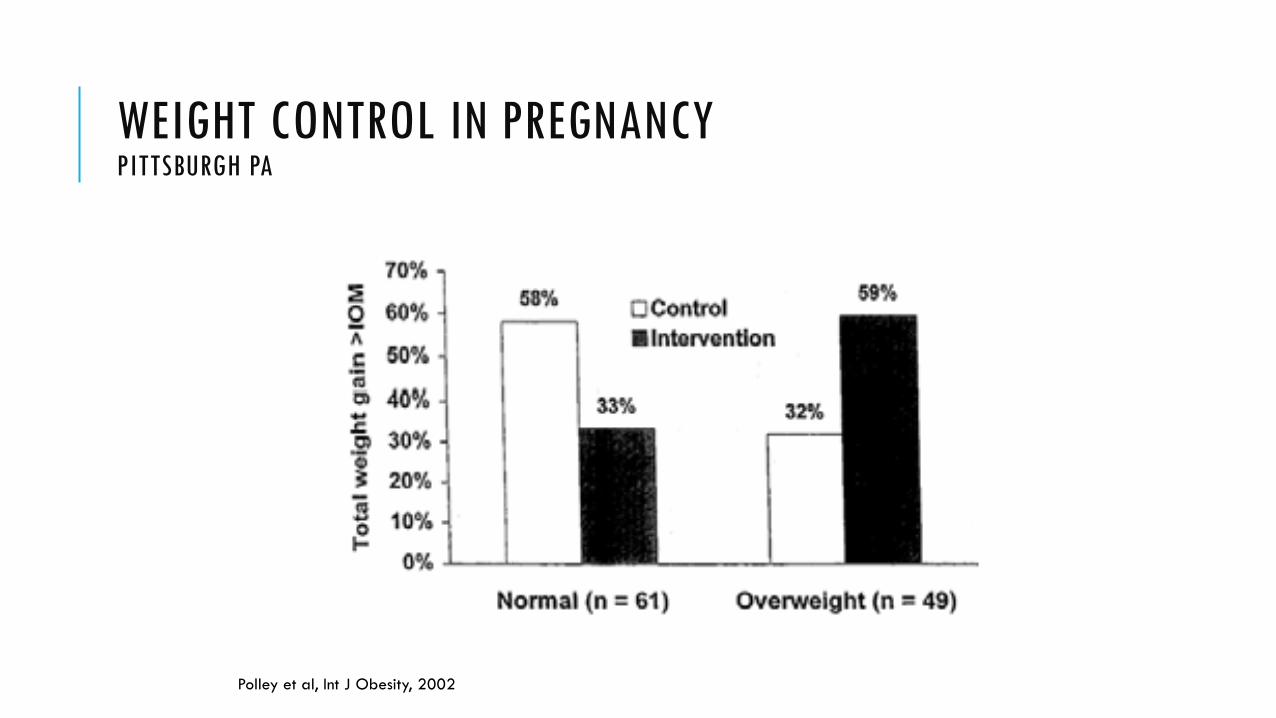
110 patients followed to delivery 57 intervention (30 nl weight, 27 overweight) 53 controls (31 nl weight, 22 overweight)
Intervention group received education about weight gain, healthy eating, and exercise and individual graphs of their weight gain. Those exceeding weight gain goals were given more intensive intervention.
Overall, no difference between groups in wt gain
Significant reduction in fat intake by most patients, not related to intervention
Intervention was associated with more activity
No effect of treatment group on PP wt loss
Polley et al, Int J Obesity, 2002
WEIGHT CONTROL IN PREGNANCY PITTSBURGH PA
Polley et al, Int J Obesity, 2002
WEIGHT CONTROL IN PREGNANCY PITTSBURGH PA
DIETARY RESOURCES FOR OBESE PREGNANCIES CHOOSEMYPLATE.GOV
Traditionally, 35 kcal/kg/day recommended Example: 250 lb woman = 3,977 calories/day
Counseling should be individualized
Patients may be unaware that concept of “eating for two” is outdated
Allowances for level of activity
Portion Control Learn serving sizes for different foods Limits even on “good” foods—fruits and vegetables, dairy Use 24 hour recall diaries
DIETARY COUNSELING
NIH criteria for surgery: BMI > 40 BMI > 35 + comorbid illness
Restrictive surgery – restricts total intake, limiting calories obtained Roux-en-Y gastric bypass Laparoscopic adjustable banding
Malabsorptive – limits absorption of calories Roux-en-Y Biliopancreatic diversion/duodenal switch
BARIATRIC SURGERY
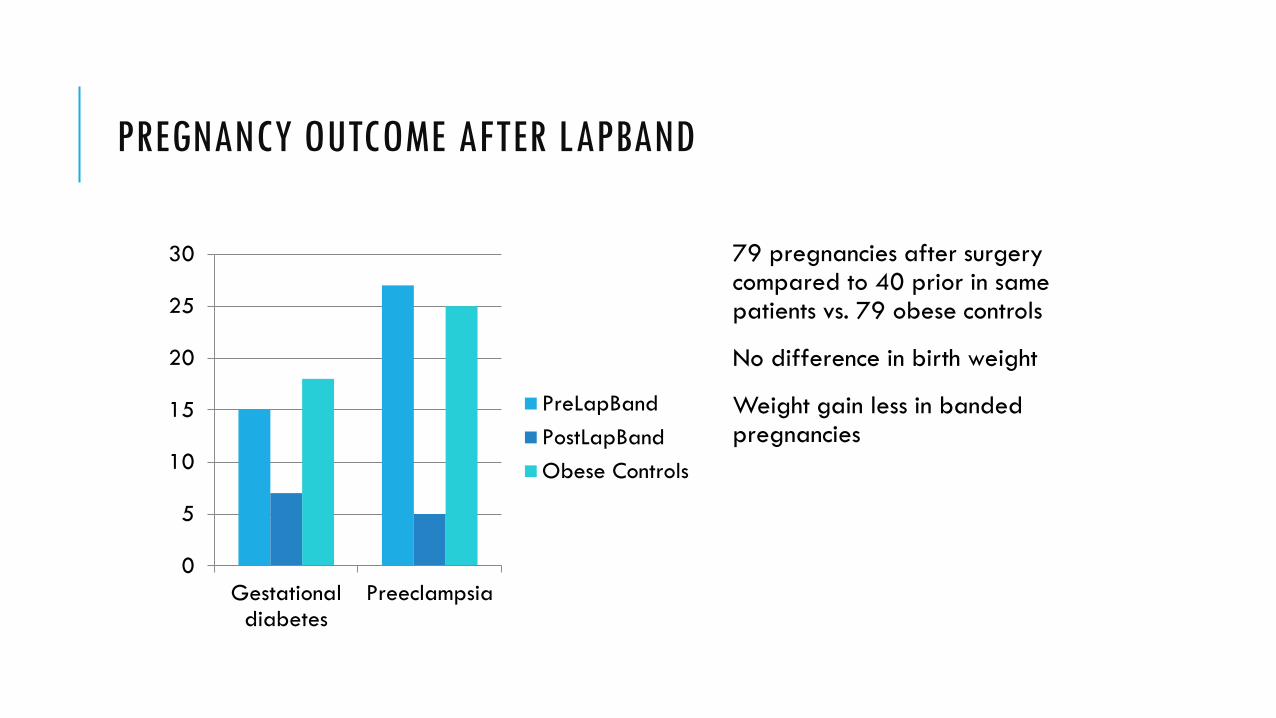
PREGNANCY OUTCOME AFTER LAPBAND
0
5
10
15
20
25
30
Gestationaldiabetes
Preeclampsia
PreLapBandPostLapBandObese Controls
79 pregnancies after surgery compared to 40 prior in same patients vs. 79 obese controls
No difference in birth weight
Weight gain less in banded pregnancies
Rapid weight loss phase 6-24 months
Ideally, delay pregnancy 2 years, or 1 year after stable weight – yeah, right…
Possible nutritional deficiencies following bariatric surgery, especially in 1st year B12 B6 Folate Iron Vitamin K
DIETARY COUNSELING POST BARIATRIC SURGERY
B12 Common after 1 year post-surgery Up to 70% of patients affected Decreased gastric acid prevents binding
Folate 20% of patients deficient after 1 year post-surgery
Iron Absorbed in proximal intestine 50-60% deficient after 1 year post-surgery Replace with IV/IM iron – limited absorption orally
VITAMIN DEFICIENCIES
All patients should have some level of nutritional counseling, ideally before pregnancy
All pregnant women should know recommendations for total weight gain
For obese patients, caloric goal based on ideal body weight
Screen obese patients for comorbid conditions
Screen post-bariatric surgery patients for vitamin deficiencies and supplement as needed
SUMMARY

DIABETES IN PREGNANCY
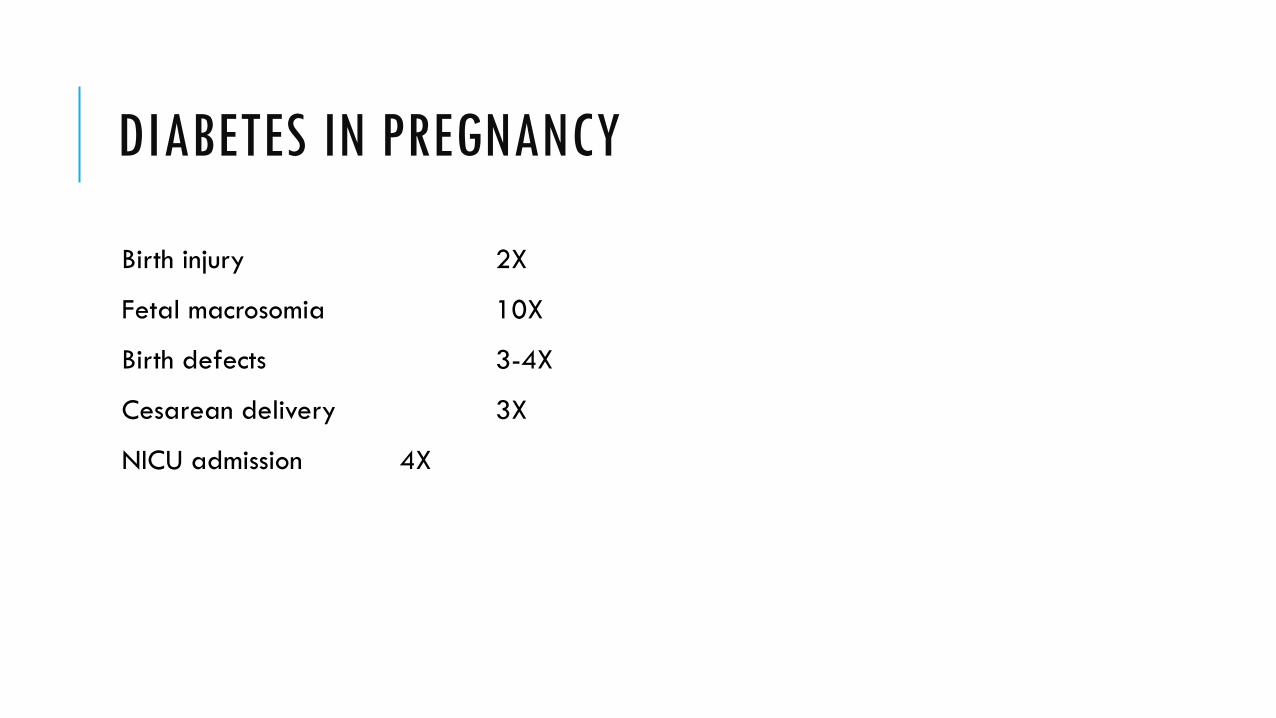
DIABETES IN PREGNANCY
Birth injury 2X
Fetal macrosomia 10X
Birth defects 3-4X
Cesarean delivery 3X
NICU admission 4X
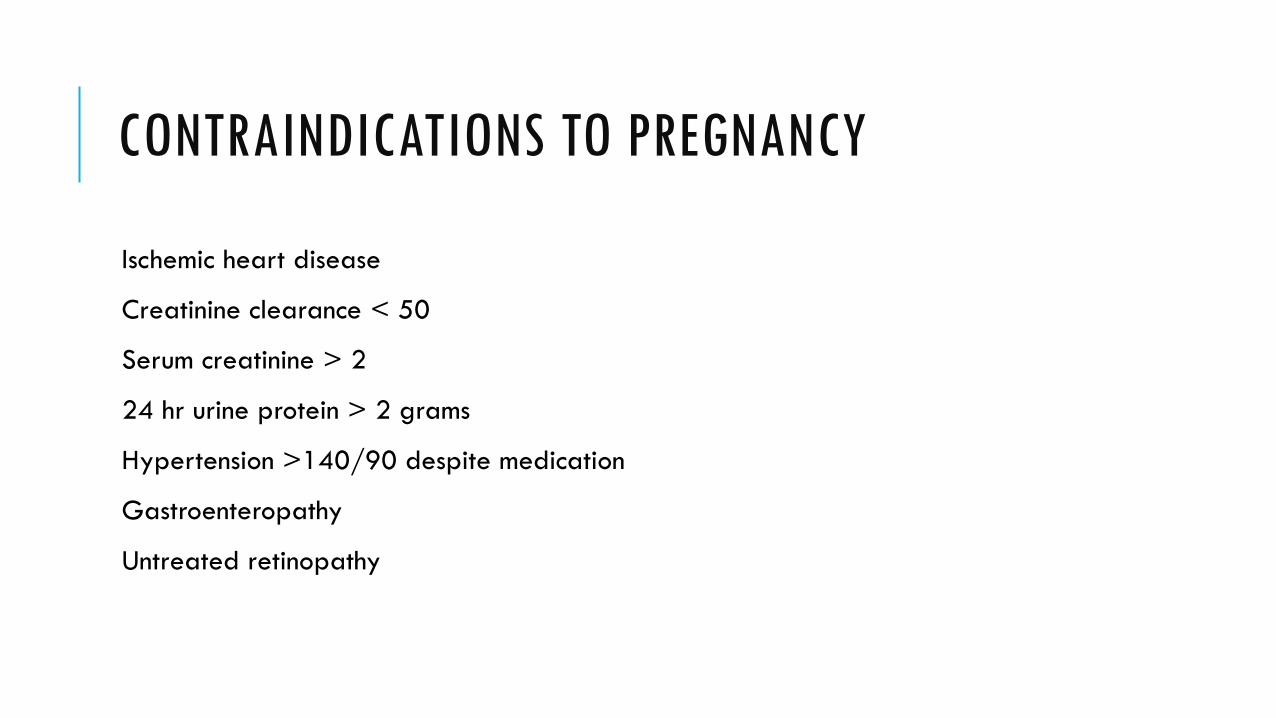
CONTRAINDICATIONS TO PREGNANCY
Ischemic heart disease
Creatinine clearance < 50
Serum creatinine > 2
24 hr urine protein > 2 grams
Hypertension >140/90 despite medication
Gastroenteropathy
Untreated retinopathy
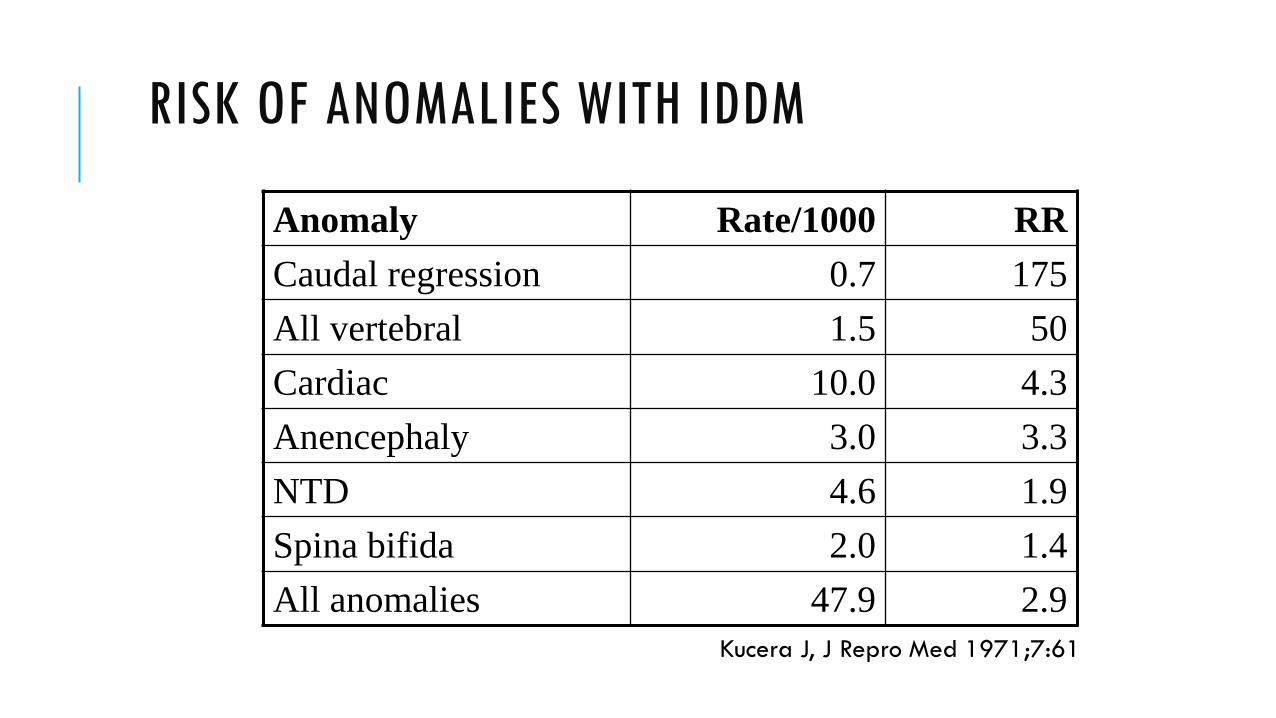
RISK OF ANOMALIES WITH IDDM
Anomaly Rate/1000 RR Caudal regression 0.7 175 All vertebral 1.5 50 Cardiac 10.0 4.3 Anencephaly 3.0 3.3 NTD 4.6 1.9 Spina bifida 2.0 1.4 All anomalies 47.9 2.9
Kucera J, J Repro Med 1971;7:61
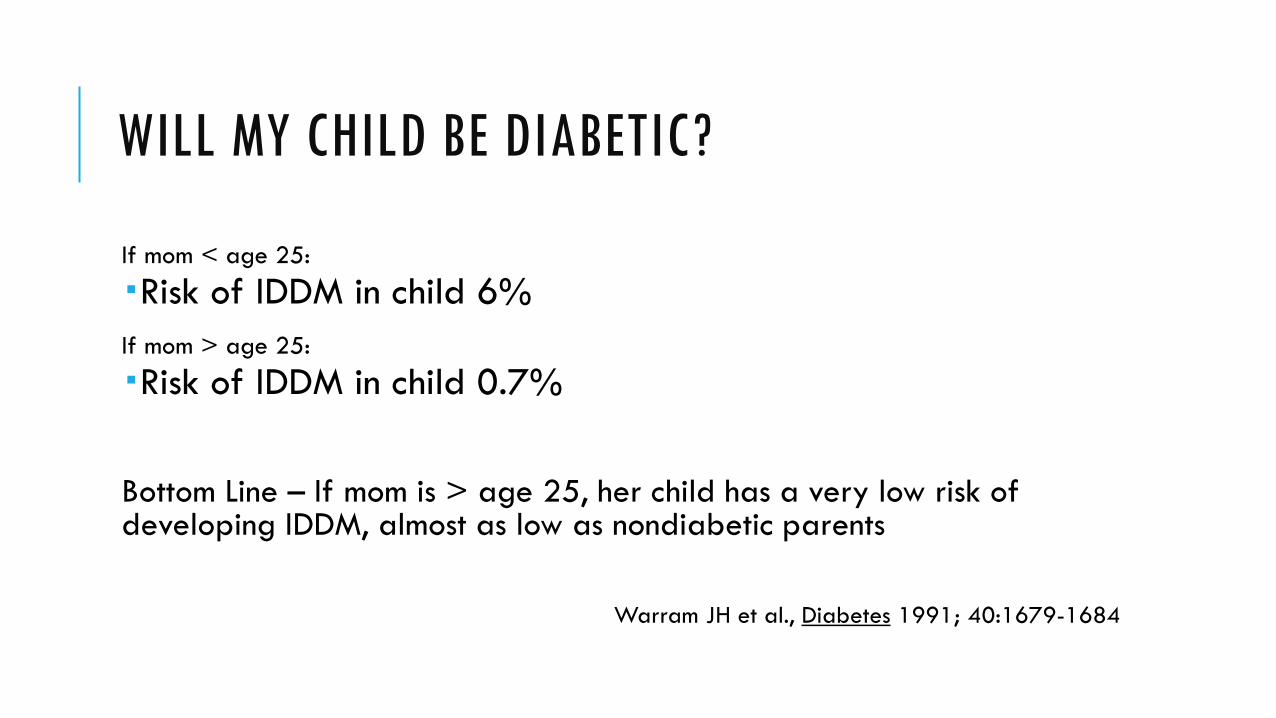
WILL MY CHILD BE DIABETIC?
If mom < age 25:
Risk of IDDM in child 6% If mom > age 25:
Risk of IDDM in child 0.7%
Bottom Line – If mom is > age 25, her child has a very low risk of developing IDDM, almost as low as nondiabetic parents
Warram JH et al., Diabetes 1991; 40:1679-1684
RE-EDUCATING DIABETIC PATIENTS
Glucoses checked at least QID
Insulin regimen may need to be updated
Follow up with endocrinologist or MFM
Dietary consult
GLUCOSE METABOLISM IN PREGNANCY
Lower fasting glucoses
Placental steroid hormones rise
Insulin less effective in pregnancy – more insulin required
Fetal glucose about 80% of maternal glucose
RISK FACTORS FOR GDM
Previous infant >4000 grams
Previous stillbirth
Maternal obesity or weight gain
Multiple gestation
Previous gestational diabetes
GLUCOSE SCREENING IN PREGNANCY
Screen at 24-28 weeks
If risk factors - screen on entry
50 gram 1 hour GTT
Positive screen > 140 mg/dl
If screen positive - 3 hour GTT
2 or more abnormal values = GDM
METFORMIN IN PREGNANCY
Metformin given increasingly to women with PCOS-related infertility
Reduces incidence of first trimester pregnancy loss in women with PCOS
Decreases development of gestational diabetes in women with PCOS 3% with metformin 31% without metformin
ORAL HYPOGLYCEMICS
In Oct 2000 NEJM, Langer compared glyburide and insulin in gestational diabetics
No difference in macrosomia, lung complications, NICU admissions, or fetal anomalies
Cord insulin levels similar
No glyburide detected in cord blood
PRE-PREGNANCY COUNSELING - WHY?
Establishes working relationship with your doctor
Obtain optimal glucose and weight control before conception
Begin folic acid supplementation
Address smoking, obesity, alcohol use