benefits at a glance handbook - secure.icbdr.com · the benefits at a glance handbook is designed...
TRANSCRIPT

BENEFITS at a GLANCE
Handbook
Benefit Year: December 1, 2014 – November 30, 2015

This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
TOPIC PAGE #
Tobacco Free Information 2
Legal Notices 3
Enrollment Information 4
Miscellaneous Information 5
Medical Plans 6-11
Dental Plan 12-13
Vision Plan 14
Life Insurance 15
Short-term Disability 16
Long-term Disability 17
Flexible Spending Account 18-19
Direct Deposit 19
Retirement Plan 20
Paid Time Off 21
Voluntary Products Portfolio 22-23
Employee Assistance Program 24
Key Contacts 25
Privacy Notice 26-27
IMPORTANT NOTE
The Benefits At A Glance Handbook is designed to provide select information on Employee Benefit plans and programs available
during the 2014-2015 Plan Year. It does not detail all of the provisions, restrictions and exclusions of the various benefit programs
described herein. This booklet does not constitute a Summary Plan Description (SPD) or Plan Document as defined by the Employee
Retirement Income Security Act. The Summary Plan Description or Plan Document is available from your Benefits Administrator.
If you are newly eligible and/or electing group life, voluntary life and/or disability coverage for the first time, you are required to be
‘Actively at Work’ on the day that the coverage commences. ‘Actively at Work’ is defined as, you are working for your Employer
for earnings that are paid regularly and that you are performing the material and substantial duties of your regular occupation. Please
note that Medical, Dental and Vision coverage is not subject to the ‘Actively at Work’ Provision.
Prepared By:
Table of
Contents

2 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
TOBACCO USE SURCHARGE
If you used tobacco products in the preceding 6 months (smoke, chew or any other manner) and are enrolled in Aspire
Health Partners’ medical plan, you will be assessed a tobacco-use surcharge.
Not only are we trying to reduce our escalating insurance costs, but we are also striving for a healthier work force. There is
a proven link between smoking and the rising cost of healthcare because smokers / tobacco-users have a higher risk of can-
cer, stroke, heart disease and chronic obstructive pulmonary disease (COPD) than non-tobacco users. You will be required
to complete a Tobacco-Use certification as part of your benefits enrollment.
Aspire Health Partners offers a reasonable opportunity for employees to avoid the smoking premium surcharge upon completion
of an approved tobacco cessation program. This applies to covered employees, for whom it is unreasonably difficult because of a
medical condition, or for whom it is medically inadvisable to be tobacco-free under our standard. Aspire Health Partners has
chosen the standards that the tobacco cessation program must meet such as the timeframe, and the manner in which employees
must certify their completion of the program. An approved tobacco cessation program may be a certified online program, class-
room-based course, or telephonic counseling/support program.
Smoking Premium Surcharge Reasonable Alternative Information
The following information describes Aspire Health Partners “reasonable opportunity” for you to avoid the smoking premi-
um surcharge. It is each employee’s responsibility to pay for the cost of tobacco cessation.
Step 1: Choose an approved online, classroom-based or telephonic tobacco cessation program. Some resources available
to help you locate approved tobacco cessation programs include:
Telephonic Courses: More than 30 states now run tobacco guidelines that are confidential, staffed by trained spe-
cialists and free to residents. Some of these helplines provide over-the-counter support products, such as gum or
patches, at reduced prices or as part of the program. Courses must consist of at least four telephonic counseling /
support sessions to be acceptable. You will have to obtain verification that you completed at least four sessions.
Online Course: Take the online American Lung Association’s Freedom From Smoking Program (make sure to
elect the Premium membership for a nominal fee so you can present a completion certificate.) Go to:
www.ffsonline.org A completion certificate will be required as proof of your online course.
Classroom-Based Courses: Approved classroom-based courses are those offered through a hospital, community
organizations (such as the American Cancer Society) or your state’s Department of Health courses. Courses must
consist of at least four classroom-based meetings to be acceptable. You will have to obtain verification that you
completed at least four sessions.
The Tobacco Free Florida Website is a great place to start www.tobaccofreeflorida.com
If you do not have access to a computer, you may call 877-822-6669 for your options.
Step 2: Enroll in and complete one of the approved tobacco cessation programs listed above.
Step 3: Obtain a completion certificate from your program and submit to your Human Resources Department
Tobacco Free
Discount

3 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
MEDICAID AND THE CHILDREN’S HEALTH IN-
SURANCE PROGRAM (CHIP) If you are eligible for health coverage but are unable to
afford the premiums, some States have premium assistance
programs that can help pay for coverage. These States use
funds from their Medicaid or CHIP programs to help people
who are eligible for employer-sponsored health coverage,
but need assistance in paying their health premiums. If you
or your dependents are NOT currently enrolled in Medicaid
or CHIP, and you think you or any of your dependents
might be eligible for either of these programs, you can con-
tact your State Medicaid or CHIP office or dial 1-877-
KIDSNOW or go to www.insurekidsnow.gov to find out
how to apply. If you qualify, you can ask the State if it has
a program that might help you pay the premiums for an
employer-sponsored plan. Once the State determines that
you or your dependents are eligible for premium assistance
under Medicaid or CHIP, your employer’s health plan is
required to permit you and your dependents to enroll in the
plan – as long as you and your dependents are eligible, but
not already enrolled. This is called a “special enrollment”
opportunity, and you must request coverage within 60 days
of being determined eligible for premium assistance.
PATIENT PROTECTION AND AFFORDABLE CARE
ACT
The Patient Protection and Affordable Care Act (PPACA)
requires most US Citizens to obtain health insurance begin-
ning January 1, 2014. Individuals who do not obtain health
insurance will be subject to a penalty of $95 or 1% of your
gross household income (whichever is greater) for each
uninsured adult for 2014. The penalty for each uninsured
child is equal to half of the adult penalty, not to exceed
three times the adult penalty for the calendar year. Penal-
ties will increase in 2015 to $325 or 2% of gross household
income (whichever is greater), in 2016 to $695 or 2.5% of
gross household income (whichever is greater), and for
each year thereafter, it will be increased by the cost-of-
living adjustment. The annual penalty will not exceed the
national average premium for Bronze coverage in an Ex-
change. If you choose not to enroll you can go to
www.healthcare.gov to review and/or obtain coverage
through the federal Marketplace exchange.
Notices
NOTICE REGARDING THE WOMEN’S HEALTH AND
CANCER RIGHTS ACT OF ‘98
Under federal law, group plans providing benefits for a mas-
tectomy must also provide, in connection with the mastecto-
my for which the participant or beneficiary is receiving bene-
fits, coverage for:
Reconstruction of the breast on which the mastectomy
has been performed;
Surgery and reconstruction of the other breast to produce
a symmetrical appearance; and
Prosthesis and physical complications of mastectomy,
including lymph edemas, in a manner determined in con-
sultation between the attending physician and the patient.
PORTABILITY OF COVERAGE
The Health Insurance Portability and Accountability Act
(HIPAA) of 1997 entitles you to a complete transfer of bene-
fits (no pre-existing condition exclusions) if you change jobs
or change health insurance carrier(s). In order to qualify for
this transfer of benefits, your previous coverage must not
have lapsed for more than 63 days prior to your new date of
hire. In order to guarantee the portability of your benefits, you
must provide proof of prior coverage to your new employer at
the time of application or a certificate of coverage can be sent
directly to United Healthcare.
THE NEWBORNS AND MOTHERS’ HEALTH PRO-
TECTION ACT OF 1996 (NMHPA) Under Federal law, you and your newborn child are covered
for a hospital stay following childbirth. The law applies both
to persons enrolled in group health plans and to persons who
have individual health care coverage. In general, plans and
health insurance issuers that are subject to NMHPA may NOT
restrict benefits for a hospital stay in connection with child-
birth to less than 48 hours following a vaginal delivery or 96
hours following a delivery by cesarean section.
UNIFORMED SERVICES EMPLOYMENT AND
REEMPLOYMENT RIGHTS ACT
The Uniformed Services Employment and Reemployment
Rights Act (USERRA) prohibits discrimination against any-
one for serving in the armed forces or for taking military
leave from a civilian job. This includes discrimination in hir-
ing, promotion, reemployment, or any other benefit of em-
ployment. USERRA also prohibits retaliation against anyone
who seeks to enforce their rights under USERRA or assists
another in enforcing those rights.

4 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
The guide is to help you make the benefit choices that are
right for you. Think carefully about which options best suit
your individual needs and budget. The choices that you
make cannot be changed until December 1, 2015, unless you
experience a qualifying life event that is consistent with the
changes you wish to make.
ELIGIBILITY
You are eligible to participate in the benefits program if you are
a full time employee and normally work 30 hours per week.
Your benefits begin on the first day of the month following 60
days of continuous employment.
If you begin work as a part-time employee and become full time
you may participate in the benefits program on the first of the
month following 60 days from the date you became full time. If
your job status changes from full time to part-time (less than 30
hours per week), your benefits will end. You will be offered an
opportunity to continue your medical, vision, FSA and dental
benefits at your own expense per Federal COBRA regulations.
If an employee returns to their full time status within 90 days of
termination, all benefits will be reinstated effective on the full
time rehire date.
Dependents are eligible for coverage under the health plans if
they are the employee’s spouse or domestic partner, or the em-
ployee’s children including adopted, foster, step-children, or
children for whom legal guardianship has been court appointed.
Coverage for the dependent children on the medical, dental and
vision plans continues until end of the month in which they turn
age 26. Please refer to your certificate of coverage for each ben-
efit’s dependent qualification.
A dependent child may also remain covered on the medical plan
after their 26th birthday provided the child is incapable of self-
sustaining employment by reason of mental or physical handi-
cap. Special approval must be obtained from the insurance car-
riers.
DOMESTIC PARTNERS
Domestic partners are eligible to be enrolled for benefits. To
become covered, you must meet the following qualifications:
• Each party is at least 18 years old and competent to con-
tract
• Neither party is married, nor a partner to another domestic
partnership relationship
• Each party is the sole domestic partner of the other person
• Each party is not related to the other by blood
• Both parties consent to the domestic partnership relation-
ship without force, duress or fraud
• Both parties agree to be jointly responsible for each others
basic food, shelter, common necessities of life and welfare
• Neither party has been a member of another domestic part-
nership for the past year
• Each party shares his or her primary residence with the
other
• Each party considers himself/herself to be a member of the
immediate family of the other partner
Please take note that IRS Section 152 states that employees
adding a domestic partner or the child of a domestic –partner
who do not meet the IRS Section 152 definition of qualified
dependents will have additional taxable income, which needs to
be taxed and reported. When an employer provides health in-
surance coverage for the domestic partner or the dependents of
the domestic partner of an employee, federal tax law considers
the fair market value of that coverage, including the employee's
pre-tax contributions, as "imputed income" to the employee.
Additionally, employees cannot use pre-tax dollars to pay for a
domestic partner's coverage, precluding them from the full ben-
efits of a Flexible Spending Account, Health Reimbursement
Account or Health Savings Account.
Enrollment
Information

5 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
CHANGING YOUR BENEFIT CHOICES
Your benefit choices will stay in effect for a full plan year.
If you have a qualified change in family status, you may be able
to change benefit elections. Qualified family status changes
include, but are not limited to:
• Marriage or Divorce
• Birth, Adoption or Legal Custody of an eligible dependent
• Death of your spouse or dependent
• A covered Dependent becomes ineligible
• Change from full time to part-time status, or vice versa, by
you or your spouse
• Unpaid leave of absence by you or your spouse
• Significant change in your spouse's coverage attributable to
employment
• Termination or commencement of spouse's employment
If you experience a qualified family status change and wish to
make changes, you must notify Human Resources within 31
days of the change. If you do not notify Human Resources
within 31 days of the qualifying event, you must wait until the
next annual enrollment period to make any desired changes.
Please keep in mind that documentation may be required.
BENEFIT TERMINATION & THE COBRA
CONTINUATION OPTION
Your benefits will term at the end of the month in which you
either elect not to participate in the plan, or you cease to be a
full-time employee.
The Federal Consolidated Omnibus Budget Reconciliation Act
(COBRA) provides insured employees and their qualified
beneficiaries the opportunity to continue health, dental, vision,
and flexible spending account coverage when a “qualifying
event” would normally result in the loss of coverage eligibility.
Common qualifying events include resignation or termination
from employment, the death of an employee, a reduction in
employee’s hours, an employee’s divorce, and dependent child
no longer meeting eligibility requirements. Under COBRA, the
employee or dependent pays the full cost of coverage at the
current group rates plus an administrative fee of 2%.
PAYING FOR BENEFITS WHILE ON AN APPROVED
FAMILY MEDICAL LEAVE OR A MEDICAL LEAVE
RELATED TO A WORKCOMP INJURY
Employees on an approved leave are still responsible for paying
the same portion of premiums paid prior to the leave. You may
pay your portion of premiums due before starting your leave, or
you may pay monthly during your leave. Payment is due on or
before the first of the month. Failure to make payments in a
timely manner will result in termination of coverage, retroactive
to the day your FMLA began. You should contact your Human
Resources to make payment arrangements prior to your leave.
Employees on an approved leave can stop health coverage alto-
gether and restart it when returning to work.
PRE-TAX OR AFTER-TAX?
For some benefits, you use pre-tax dollars from your pay. For
others, you must use after-tax dollars. When you pay for bene-
fits with pre-tax dollars, money is deducted from your pay be-
fore taxes are taken out. In this way, you avoid paying Federal
Income and Social Security taxes on what you spend on bene-
fits. With after-tax contributions, just the opposite is true. Pre-
miums are deducted from your pay after Federal and Social
Security taxes are calculated and deducted from your gross pay.
A NOTE ABOUT SOCIAL SECURITY
Pre-tax deductions taken from your paycheck lower your taxa-
ble income, your Social Security taxes (and, therefore, your
future Social Security benefits) may be lower. How you are
affected depends on your pay and the amount of pre-tax contri-
butions you make.
The reduction in Social Security benefits, if any, for most em-
ployees will be minimal - a few dollars a month. Younger em-
ployees who use large amounts of tax-free dollars to pay for
benefits over a long period (20 to 30 years) may experience a
greater reduction in benefits when they retire. However, for
most people, the benefit reduction has been more than offset by
the tax savings. For more information, please contact your local
Social Security Administration office.
MEDICARE PART D ELIGIBLE INDIVIDUALS
If you and/or your dependents have Medicare or will become
eligible for Medicare in the next 12 months, a Federal law gives
you more choices about your prescription drug coverage. This
booklet does not constitute disclosure of creditability status.
Please contact Human Resources for your personalized disclo-
sure notice regarding the credibility status of your plan.
Miscellaneous
Information

6 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
DIRECT ACCESS BENEFITS
Referrals are not usually needed for specialist visits, including
routine eye exams and gynecological/obstetrical care. However,
certain laboratory procedures and X-Ray service care must be
pre-certified by your physician prior to the visit
EMERGENCY CARE
Emergency services are covered anytime, anywhere in an out of
network. If you need emergency care, here are some basic
guidelines:
Go to the nearest emergency room or call 911. If a delay
would not be detrimental to your health, call your doctor
first.
To avoid a long wait in the emergency room, you can visit
any participating urgent care facility in your area.
If you’re admitted to the hospital, you or a family member
should notify your doctor or United Healthcare.
UNITED BEHAVIORAL HEALTH
United Behavioral Health offers confidential, comprehensive
services and a wide array of treatment options from acute inpa-
tient care to individual outpatient counseling. When you call
United Behavioral Health for assistance, you will speak directly
to a mental health professional who can answer questions relat-
ed to the mental health and substance abuse benefits. United
Behavioral Health program specializes in depression, stress &
anxiety, child/adolescent issues, phobias, personality disorders,
anorexia & bulimia, post traumatic syndrome, alcohol and
chemical dependency.
CARE COORDINATION
United Healthcare, is able to identify, quantify and address the
fragmentation of care that comprises health outcomes. Their
Care Coordinationsm approach goes beyond traditional medical
coverage and preventive services and fill gaps in care. Care
Coordination focuses on offering education, accelerating access
to care and providing early identification and monitoring of
chronic conditions. They are:
Health education and reminder programs
Admission counseling
Inpatient care advocacy
Welcome Home!sm (readmission prevention)
IMPACTsm (complex illness support)
PROVIDER DIRECTORIES
To find a participating providers prior to the effective date of
your coverage, go to www.uhc.com. Once you are enrolled you
can access this information at www.myuhc.com.
MYUHC.COM
MyUHC.com gives you access to tools and information so
you may:
View benefit and claim information
Find a physician
Print a temporary ID card
Request a replacement ID card
View preferred drug lists and prescription history
Order prescription and over the counter products through
home delivery service
Set up email reminders for prescription refills
MEMBER SERVICES
Member Service representatives are trained to answer your
questions concerning your health plan benefits. Call the toll-
free number on your ID card to:
Ask about your benefits
Request another ID card
RX HOME DELIVERY
Home delivery saves time and money. Through a partnership
with Optum you can have prescriptions medications and other
health and beauty products sent right to your home. There is
NO added shipping or handling fees for prescriptions.
The following information is provided under your pharmaceu-
tical needs at www.myuhc.com:
View personal benefit coverage information and prescrip-
tion history
Search the Preferred Drug List online
Order Prescription and over the counter drugs for home
delivery
myNurseLineSM
Reliable health information from registered nurses available
24 hours / 7 days a week by calling 800-846-4678. Receive
immediate answers from nurses backed by medical profes-
sionals who can help you:
Understand you current symptoms
Decide if you should see a doctor or go to the ER
Find a network doctor or hospital
Explore treatment options
Learn more about a diagnosis
Understand you medications
Medical

7 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
GOLD Coverage Choice In-Network Only In-Network Out-of-Network
Lifetime Maximum Unlimited
Calendar Year Deductible (CYD) $575 Individual
$1,150 Family No Coverage
Out of Pocket Maximums (Includes deductible, coinsurance, co-pays; excludes Rx)
$2,000 Individual
$4,000 Family No Coverage
Co-Insurance 80% / 20% No Coverage
Well Child Care /Immunizations
100% No Coverage
Routine Adult Physicals 100% No Coverage
Primary Physician Office Visit $25 Copay No Coverage
Specialty Care Physician Office Visit $40 Copay No Coverage
Emergency Room (Facility) $200 Copay $200 Copay
Urgent Care $50 Copay No Coverage
In-Patient Hospitalization CYD then 20% No Coverage
Out-Patient Hospitalization CYD then 20% No Coverage
Laboratory and Radiology Services Covered at 100% No Coverage
Advanced Radiological Imaging (CT Scans, PET Scans, MRI, MRA & Nuclear Medicine) CYD then 20% No Coverage
Chiropractic Care
$40 Copay
No Coverage
In-Patient Mental Health and Substance Abuse (MH/SA) Treatment CYD then 20% No Coverage
Office visit Mental Health and Substance Abuse (MH/SA) Treatment $25 Copay (varies depending on treatment type)
No Coverage
*Prescription Drug Co-Payments
(30 day supply) Tier 1
Tier 2
Tier 3
Mail Order Prescription Drug
(31-90 day supply)
$15 Copay
$25 Copay
$60 Copay
$30/$50/$120 Copay
No Coverage
Medical
Payroll Deductions (26 pay periods)
Coverage Option GOLD - Non-Tobacco GOLD - Tobacco
Employee
Employee & 1
Employee & 2+
$62.40
$210.00
$240.00
$65.90
$213.50
$243.50 GOLD

8 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
SILVER Coverage Choice In-Network Only In-Network Out-of-Network
Lifetime Maximum Unlimited No Coverage
Calendar Year Deductible (CYD) $1,000 Individual
$3,000 Family No Coverage
Out of Pocket Maximums (Includes deductible, coinsurance, co-pays; excludes Rx)
$3,500 Individual
$7,000 Family No Coverage
Co-Insurance 80% / 20% No Coverage
Well Child Care Exams/ Immunization 100% No Coverage
Routine Adult Physical Exams 100% No Coverage
Primary Physician Office Visit $25 Copay No Coverage
Specialty Physician Office Visit $50 Copay No Coverage
Emergency Room Co-Payment (Facility) $200 Copay $200 Copay
Urgent Care $75 Copay No Coverage
In-Patient Hospitalization CYD then 20% No Coverage
Out-Patient Hospitalization CYD then 20% No Coverage
Laboratory and Radiology Services Co-Payment
Covered at 100% No Coverage
Advanced Radiological Imaging Co-Payment (CT Scans, PET Scans, MRI, MRA & Nuclear Medicine)
CYD then 20% No Coverage
Chiropractic Care Co-Payment $50 Copay No Coverage
In-Patient Mental Health and Substance Abuse (MH/SA) Treatment
CYD then 20% No Coverage
Office visit Mental Health and Substance Abuse (MH/SA) Treatment $25 Copay (varies depending on treatment type)
No Coverage
*Prescription Drug Co-Payments
(30 day supply) Tier 1
Tier 2
Tier 3
Mail Order Prescription Drug
(31-90 day supply)
$30 Copay
$50 Copay
$100 Copay
$60/$100/$200 Copay
No Coverage
Medical
Payroll Deductions (26 pay periods)
Coverage Option SILVER - Non-Tobacco SILVER - Tobacco
Employee
Employee & 1
Employee & 2+
$41.63
$175.00
$210.00
$45.13
$178.50
$213.50 SILVER
9 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
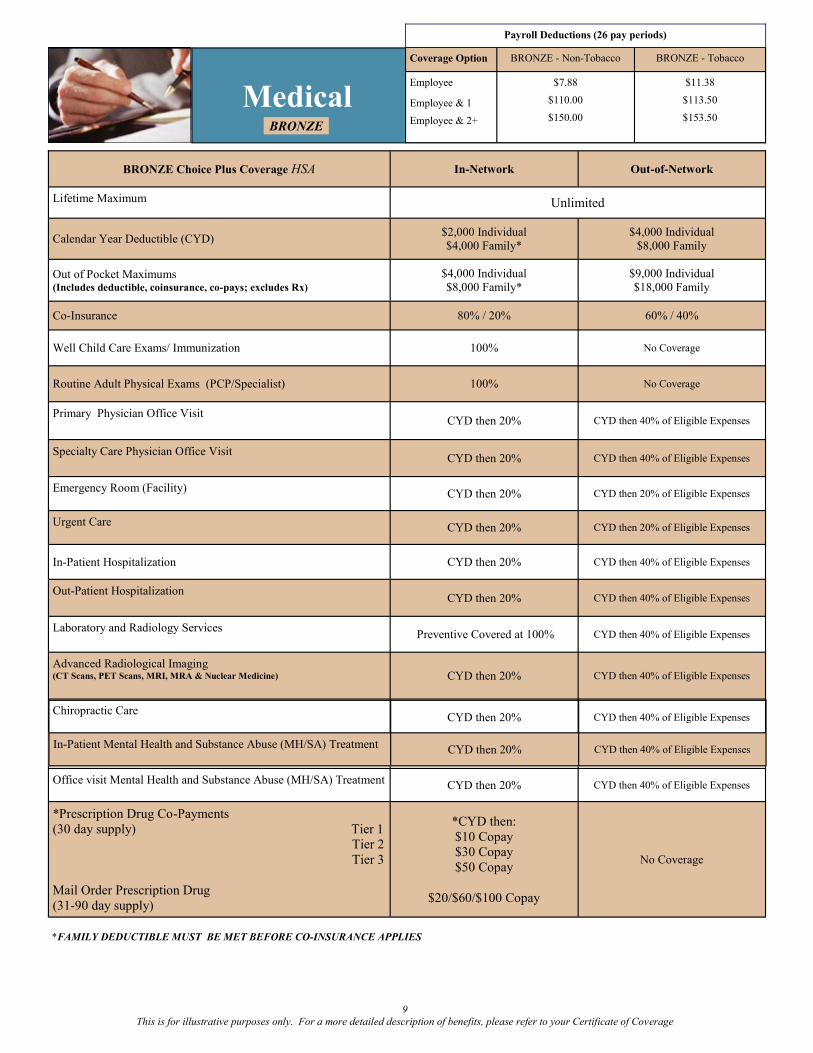
BRONZE Choice Plus Coverage HSA In-Network Out-of-Network
Lifetime Maximum Unlimited
Calendar Year Deductible (CYD) $2,000 Individual
$4,000 Family*
$4,000 Individual
$8,000 Family
Out of Pocket Maximums (Includes deductible, coinsurance, co-pays; excludes Rx)
$4,000 Individual
$8,000 Family*
$9,000 Individual
$18,000 Family
Co-Insurance 80% / 20% 60% / 40%
Well Child Care Exams/ Immunization 100% No Coverage
Routine Adult Physical Exams (PCP/Specialist) 100% No Coverage
Primary Physician Office Visit CYD then 20% CYD then 40% of Eligible Expenses
Specialty Care Physician Office Visit CYD then 20% CYD then 40% of Eligible Expenses
Emergency Room (Facility) CYD then 20% CYD then 20% of Eligible Expenses
Urgent Care CYD then 20% CYD then 20% of Eligible Expenses
In-Patient Hospitalization CYD then 20% CYD then 40% of Eligible Expenses
Out-Patient Hospitalization CYD then 20% CYD then 40% of Eligible Expenses
Laboratory and Radiology Services
Preventive Covered at 100% CYD then 40% of Eligible Expenses
Advanced Radiological Imaging (CT Scans, PET Scans, MRI, MRA & Nuclear Medicine) CYD then 20% CYD then 40% of Eligible Expenses
Chiropractic Care
CYD then 20% CYD then 40% of Eligible Expenses
Office visit Mental Health and Substance Abuse (MH/SA) Treatment CYD then 20% CYD then 40% of Eligible Expenses
*Prescription Drug Co-Payments
(30 day supply) Tier 1
Tier 2
Tier 3
Mail Order Prescription Drug
(31-90 day supply)
*CYD then:
$10 Copay
$30 Copay
$50 Copay
$20/$60/$100 Copay
No Coverage
Medical
*FAMILY DEDUCTIBLE MUST BE MET BEFORE CO-INSURANCE APPLIES
Payroll Deductions (26 pay periods)
Coverage Option BRONZE - Non-Tobacco BRONZE - Tobacco
Employee
Employee & 1
Employee & 2+
$7.88
$110.00
$150.00
$11.38
$113.50
$153.50 BRONZE
In-Patient Mental Health and Substance Abuse (MH/SA) Treatment
CYD then 20% CYD then 40% of Eligible Expenses

10 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
Health Savings
Account (HSA)
A Health Savings Account (HSA) is a tax-preferred account that may be opened by individuals covered by a Qualified High Deduct-
ible Health Plan (HDHP). If you are enrolled in Bronze plan, and are otherwise qualified, you have the option of opening an HSA.
HOW AN HSA WORKS
Part 1:
Qualifying High
Deductible Health
Insurance Plan
2015
Employee Only Coverage $ 3,350
Family Coverage $ 6,550
Catch Up Contributions $ 1,000
WHY OPEN A HEALTH SAVINGS ACCOUNT
An HSA can be used to accumulate funds on a tax-free basis
to pay for qualified health care expenses, as defined by the
Internal Revenue Service (IRS). The account acts like a regu-
lar bank account with a debit card and/or checkbook, and ac-
crues interest. Depositing funds in your HSA through pay-
roll deductions can help you be prepared for expenses that
you incur before your deductible is met. The account is
owned by you and funds can accumulate over time. The ac-
count is portable among employers.
WHO CAN OPEN A HEALTH SAVINGS ACCOUNT
The IRS has established guidelines on individuals qualified to
open an HSA. You must be:
Covered by a Qualified High Deductible Health Plan, and
Not covered by any other plan that is not a Qualified
High Deductible Health Plan
Not enrolled in Medicare or Medicaid
Not eligible to be claimed as a dependent on another’s
tax return
Not covered under an unlimited FSA or HRA
PERMISSIBLE INSURANCE WITH A HSA
Coverage under certain types of insurance policies will not
affect your ability to open an HSA. Permissible insurances
include:
Workers Compensation
Disability insurance
Dental insurance
Vision insurance
Specific Disease policies (Accident, Cancer, etc.)
Long Term Care insurance
MAXIMUM CONTRIBUTION LIMITS
The maximum amount that can be deposited, from all sources,
into the HSA each calendar year is established by the IRS and
whether you have employee only coverage or family cover-
age. HSA contributions are separate from, and in addition to,
the premium you pay for your Qualified High Deductible
Health Plan. HSA contributions may be made through pay-
roll deductions on a pre-tax basis, or you can make contribu-
tions directly to your HSA. You may contribute any amount
up to the maximums shown below. Individuals age 55 and
older can make “Catch-Up Contributions” in addition to the
maximum annual contribution limits.
Pays for out-of-pocket
expenses incurred before
the deductible is met.
Part 2:
Health Savings
Account
(HSA)
1. Employee enrolls in a Qualified High Deductible
Health Plan (HDHP).
2. Employee opens an HSA (encouraged, but not re-
quired) and provides account information to Human
Resources.
3. Employee makes deposits to their HSA account
through pre-tax payroll deductions (encouraged, but not
required).
4. Employee or covered Dependent seeks medical
services.
5. Medical services are covered by the HDHP, subject
to a deductible and coinsurance.
6. Employee may use their HSA account to pay for
qualified medical expenses, including those applied to
their deductible and coinsurance.
The Deductible is waived for Preventive care. Refer
to the Benefit Summary for additional information.
Employees may also make deposits directly to their
HSA account without going through payroll.
Intended to cover serious
illness or injury after the
deductible has been met.

11 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
HSA FREQUENTLY ASKED QUESTIONS
What is a qualified High Deductible Health Plan?
The IRS has established guidelines on the minimum in-
network deductibles and out-of-pocket maximums for quali-
fied plans. The plan must also require that the deductible
apply to all services, including prescriptions. The only excep-
tion is that the plan may pay for preventive care without hav-
ing to meet the deductible. The United Healthcare plans are
qualified High Deductible Health Plans.
What happens to the money in my HSA at the end of the
year?
The funds remain in your account, continue to earn interest,
and are available to pay for qualified expenses tax free in the
future.
What happens if I go over the maximum contribution?
If your deposits (including contributions from all sources)
exceed the maximum contribution limit you will be required
to pay income tax and penalty tax on the excess amount. This
is also the case if you do not remain covered for the entire
testing period and your contributions exceed the pro-rated
contribution limit. Excess contributions can be withdrawn
without tax penalties if the withdraw is completed prior to
your tax filing deadline. Contact your HSA trustee and/or
your tax advisor for assistance.
What happens to the money in my HSA if I decide next
year to go back to a non-qualified plan?
The money is yours to keep. You can no longer deposit addi-
tional money into the account if you are not HSA eligible, but
you can continue to use the funds tax-free to pay for qualified
expenses or you can let the funds stay there and accumulate
interest.
What happens to the money in my HSA if I leave my cur-
rent employer?
The money in the HSA is yours to keep. If you remain HSA
eligible, you can continue to make contributions directly to
your HSA. If you do not remain HSA eligible, you can no
longer deposit additional money into the account, but you can
continue to use the funds tax-free to pay for qualified expens-
es or you can let the funds stay there and accumulate interest.
Can my spouse have an HSA?
Yes, provided he/she is covered under a qualified High De-
ductible Health Plan. If both spouses have HSA’s, the maxi-
mum family contribution as defined by the IRS each year is
divided equally between them unless both spouses agree on a
different division. If both spouses are 55 or over, they can
both make “Catch-Up Contributions” in addition to the fami-
ly maximum.
Can I use my HSA to pay for my family’s qualified ex-
penses if they are not covered under my health plan?
Yes, as long as the expense is not reimbursed by another
health plan, you may use your HSA to pay for qualified ex-
penses incurred by you, your spouse, and your dependent
children., even if they are not covered on the qualified health
plan.
What happens if I don’t have enough money in my HSA to
cover the charge?
You will need to pay the provider from another source. You
can later reimburse yourself when the funds are available in
your HSA, if you choose to do so. Remember to keep all
receipts to show that the funds were withdrawn for a qualified
expense.
If I use all the money in my HSA early in the year can I
put more in?
You can not exceed the maximum contribution limits for the
calendar year, even if some of that money was taken out to
pay for qualified expenses. You will be able to deposit addi-
tional funds in the next calendar year, if you remain HSA
eligible.
Can I use my HSA to pay for my dental and expenses?
Yes, as long as the expense was not reimbursed by another
plan. However, dental expenses will not help you meet the
deductible on your health plan.
Why should I choose an HSA?
1. Cost Savings
Reduction in medical plan premium (payroll deduction)
Tax benefits
HSA contributions are excluded from federal income
tax
Withdrawals for eligible expenses are exempt from
federal income tax
Unused money is held in an interest-bearing account
2. Long-term financial benefits
Save for future medical expenses
Unused funds roll over year to year
This is your account, you take it with you
3. Choice
You control and manage your health care expenses.
You choose whether to use your HSA dollars to pay
your health care expenses or to save them for future use.

12 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
Dental
PPO DMO
(Co-Payment Schedules)
Benefit Description In-Network Out-of Network In-Network Only
YOU PAY YOU PAY YOU PAY
Preventive Services
Cleanings, oral exams
0%
Deductible Waived
0%
Deductible Waived
See schedule of benefits
(see next page)
Basic Services
Oral Surgery-Simple extractions, fillings
Periodontics
Deductible then 20% Deductible then 20%
of eligible expenses
See schedule of benefits
(see next page)
Major Services Crowns, Dentures, Bridges
Deductible then 50% Deductible then 50%
of eligible expenses
See schedule of benefits
(see next page)
Orthodontic Services
50%
Child to Age 19 Only
$1,000 Lifetime Maximum 50%
See schedule of benefits,
Adult and Child Ortho is covered
Calendar Year Maximum $1,500 Per Person No Annual Maximum
Calendar Year Deductible
Per Person
Per Family
$50
$150
$50
$150
No Deductible
Payroll Deduction (26 pay periods)
Coverage Option Dental PPO Plan DMO Plan
Employee
Employee & 1
Employee & 2+
$13.72
$26.85
$45.37
$6.93
$12.15
$18.02
PRE-DETERMINATION REVIEW
When the expected cost of a proposed course of treatment is
$200 or more, United Healthcare will review the treatment plan
and let your dentist know what benefits could be payable. Simp-
ly ask your dentist to fax your treatment plan to United
Healthcare and request a Pre-Determination Review prior to re-
ceiving care.
SPECIAL LIMITATION
Teeth lost or missing before a covered person becomes insured
by this plan. The plan won’t pay for a prosthetic device which
replaces such teeth unless the device also replaces one or more
natural teeth lost or extracted after the covered person became
insured by this plan.
WWW.MYUHCDENTAL.COM
You can access your dental plan 24 hours a day, 7 days a
week at www.myuhcdental.com. Once registered you can
search for a participating dentist, review your claims, view
your remaining Calendar Year Benefit, and much more!
LATE ENTRANT PENALTIES
If you decline this coverage now, and choose to enroll later,
you may be subject to late entrant penalties. Late Entrant
penalties may be waived during Open Enrollment.

13 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
Dental (DMO Sample Fee Schedule)

14 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
Eye Examination In-Network Out-of-Network
Co-Payment $10 No Coverage
Frequency Every 12 months No Coverage
Frames In-Network Out-of-Network
Coverage $25 Co-Payment
$130 retail allowance $61 retail allowance
Frequency Every 24 months Every 24 months
Lenses In-Network Out-of-Network
Coverage $25 Co-Payment then Covered in Full –
plastic or glass lenses
Allowance
$40 Single Lens
$60 Bifocal Lens
$80 Trifocal Lens
$80 Lenticular Lens
Frequency Every 12 months Every 12 months
Contacts In-Network Out-of-Network
Coverage
$25 Co-Payment
$125 retail allowance if Elective
Covered in Full if Therapeutic
$125 retail allowance if Elective
$210 retail allowance if Therapeutic
Frequency Every 12 Months in lieu of glasses Every 12 Months in lieu of glasses
Vision
SUMMARY OF BENEFITS
Vision Coverage is available through United Healthcare. Please register at myuhcvision.com to print your Vision ID card.
Payroll Deduction (26 pay periods)
Coverage Option
Employee
Employee & 1
Employee & 2+
$2.63
$4.79
$8.30

15 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
BASIC LIFE COVERAGE
Aspire Health Partners provides all full time employees (at no
cost to you) with basic life insurance coverage equal to one
times your annual salary up to $300,000. Lincoln Financial is
the carrier for your basic life benefit.
VOLUNTARY LIFE
Full time employees may purchase additional voluntary life
insurance for themselves and their dependents.
AGE REDUCTION
(Applies to Basic & Voluntary Life) At age 70, the benefit amount will be reduced by 40% and at
age 75 the benefit amount will be reduced by an additional
10%. Benefits will terminate upon retirement.
CONVERSION POLICY
(Applies to Basic & Voluntary Life)
Allows a covered person whose life insurance coverage ends to
obtain an individual policy at his/her expense, without provid-
ing evidence of insurability. A covered person may convert all
or part of the coverage. The premiums will be based on the
amount of coverage and the covered person’s age and class of
risk at the time of conversion (Subject to state requirements).
PORTABILITY COVERAGE
(Applies to Voluntary Life ONLY)
This feature allows a covered employee, whose optional life
coverage ceases, the right to continue all or a portion of his/her
optional life benefit. A covered employee may make a written
request to continue his or her benefits during the Request Peri-
od, which is 31 days after coverage ceases.
GUARANTEE ISSUE
If you are enrolling during your initial eligibility period Medical
Underwriting is required for amounts over the guarantee issue.
• Employee: $250,000 under age 70
• Spouse: $30,000 for your spouse.
• Children: $10,000 from 6 months to age 19
• Dependent children up to age 25 if unmarried and
a full time student
Life Insurance
You must complete an Evidence of Insurability form for
submission to be approved in the following circumstances:
A) If you are electing coverage for yourself or your spouse
over the guarantee issue amounts.
PLEASE NOTE THAT YOU MUST BE APPROVED FOR COV-
ERAGE BEFORE YOUR PAYROLL DEDUCTIONS WILL
BEGIN. You can obtain an Evidence of Insurability Form by con-
tacting Human Resources.
COVERAGE CHOICES
Age Spouse Rate is determined by using
Employee’s Age
Payroll Deduction Rates Per
$1,000
of Coverage
Under 30 0.028
30-34 0.028
35-39 0.042
40-44 0.069
45-49 0.106
50-54 0.203
55-59 0.318
60-64 0.346
65-69 0.637
70+ 1.306
All Children (over 6 months of age
to age 19 or 25 if full time student)
0.92/ $10,000
Employee Spouse Child (ren)
Increments 1, 2, 3, 4, 5x Salary $1,000 $10,000
Minimum Amount $10,000 $5,000 $10,000
Maximum Amount
5x annual salary
(rounded to the nearest
$1,000) or $500,000,
whichever is lower
50% of Employee
amount (rounded
down to the nearest
$1,000) or $100,000,
whichever is lower
$10,000
Guarantee Issue
Amount
$250,000 under age 70 $30,000 under age 60 $10,000
To Calculate Payroll Deduction: 1) Determine if you want to elect 1, 2, 3, 4 or 5 x your salary
2) Round up to the next $1,000
3) Divide the amount you elect by 1,000 4) Multiply the amount in # 2 times the corresponding rate in the table
Example: John is 42, his salary is $40,000. He elects the amount of
$80,000:
1) $80,000
2) $80,000 / 1,000 = 80
3) 80 x 0.069 = $5.52 = payroll deduction

16 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
Disability coverage is designed to replace a portion of your
income should you become unable to work due to a non-work
related accident or illness. Please refer to your summaries for
additional details, including limitations and exclusions.
ELIMINATION PERIOD:
Benefits begin on the 8th day after a non work related injury
or illness.
INCOME BENEFIT:
66.67% of your income to a maximum of $1,000 per week if
you are unable to work due to an injury or illness.
DURATION:
You may receive benefits for up to 13 week if you continue to
be disabled and are unable to work.
PRE-EXISTING CONDITIONS:
If you have been treated for a condition in the 3 months prior
to the effective date, that condition will not be covered for
the first 6 months of coverage.
EVIDENCE OF GOOD HEALTH
If you are enrolling during an annual open enrollment period
and previously waived this coverage you must first complete
an Evidence of Insurability Form prior to benefits being ap-
proved. Coverage and/or Payroll Deductions will not begin
until this approval process is complete.
HOW TO CALCULATE YOUR PAYROLL
DEDUCTION
The cost for the voluntary short term disability plan is based
upon your weekly benefit. If you would like to calculate your
payroll deduction, please follow the formula outlined below.
The amount is based on your weekly rate excluding overtime
compensation.
Short-Term
Disability
APPROXIMATE BIWEEKLY PAYROLL DEDUCTION
COSTS FOR VOLUNTARY SHORT TERM DISABILITY
(Use this chart to determine the approximate
payroll deductions )
HOW TO CALCULATE VOLUNTARY STD PAYROLL DEDUCTIONS
Base Annual Income Weekly Income STD Weekly Benefit Per $10 Increment Multiply by Rate Payroll Deduction
$24,000
(÷) Divide by 52
$461.54
(x) Multiply by 0.6667
$307.71
(÷) Divide by $10
$30.77
(x) Multiply by 0.83
$25.54
(x) Multiply by 12 and divide by 26
$11.79
Weekly Earnings STD Weekly Benefit
Rate $0.83
$200 $133 $5.11
$250 $167 $6.38
$300 $200 $7.66
$350 $233 $8.94
$400 $267 $10.22
$450 $300 $11.49
$500 $333 $12.77
$550 $367 $14.05
$600 $400 $15.32
$650 $433 $16.60
$700 $467 $17.88
$750 $500 $19.15
$800 $533 $20.43
$850 $567 $21.71
$900 $600 $22.99
$950 $633 $24.26
$1,000 $667 $25.54
$1,050 $700 $26.82
$1,100 $733 $28.09
$1,200 $800 $30.65
$1,250 $833 $31.92
$1,300 $867 $33.20
$1,350 $900 $34.48
$1,400 $933 $35.76

17 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
Disability coverage is designed to replace a portion of your in-
come should you become unable to work due to a non-work re-
lated accident or illness. Please refer to your summaries for addi-
tional details, including limitations and exclusions.
ELIMINATION PERIOD:
Benefits begin on the 91st day after a non work related injury or
illness.
INCOME BENEFIT:
60% of your income to a maximum of $6,000 per month if you
are unable to work due to injury or illness.
DURATION:
Benefits are payable to your normal social security retirement
age if you continue to be disabled and unable to work.
PRE-EXISTING CONDITIONS:
If you have been treated for a condition in the 3 months prior to
the effective date, that condition will not be covered for the first
6 months of coverage.
EVIDENCE OF GOOD HEALTH
If you are enrolling during an annual open enrollment period and
previously waived this coverage you must first complete an Evi-
dence of Insurability Form prior to benefits being approved. Cov-
erage and/or Payroll Deductions will not begin until this approval
process is complete.
EVIDENCE OF GOOD HEALTH
If you are enrolling for the first time and still within your ini-
tial eligibility period, you will not be required to complete an
Evidence of Insurability Form. If you are enrolling during an
annual open enrollment period and previously waived this
coverage you must first complete an Evidence of Insurability
Form prior to benefits being approved. Coverage and/or Pay-
roll Deductions will not begin until this approval process is
complete.
Please note that you do not have to enroll in both Short Term
Disability and Long Term Disability. You may choose both
plans or just one of the plans.
Long-Term
Disability
HOW TO CALCULATE LTD PAYROLL DEDUCTIONS
(determine the approximate payroll deductions )
Annual
Income
Monthly Income Per $100 Increment Multiply by Rate 0.93 Convert monthly deduction to 26 Pay Periods
$24,000
(÷) Divide by 12
$2,000
(÷) Divide by $100
$20.00
(x) Multiply by 0.93
$18.60
(x) Multiply by 12 months and (÷) divide by the 26 pay periods
$8.58

18 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
FLEX SPENDING ACCOUNTS
JANUARY 1, 2015 TO DECEMBER 31, 2015
Employees have a choice of two FSA plans, which create an
opportunity to save on taxes. Money is deducted from you
pay and contributed to the accounts on a pre-tax basis so that
taxes aren't paid on eligible expenses.
HEALTHCARE ACCOUNT
Allows you to reimburse yourself with pre-tax dollars, from a
minimum of $300 up to $2,500 in eligible expenses not reim-
bursed under any healthcare plan.
HOW IT WORKS
During the enrollment period, you decide how much
you want to contribute to each account.
Each pay period, the appropriate amount is deducted
(before taxes) and contributed to your account.
When incurring an eligible expense you may either pay
for the services at that time and then submit the expense
for reimbursement or use the debit MasterCard.
If you do not use your debit card, you must submit a claim
form to in order to be reimbursed. You must attach either a
copy of your Explanation of Benefits or a paid receipt.
You have three months after the end of the plan year to submit
claims incurred during the previous year. Claims incurred during
one plan year cannot be submitted for reimbursement from con-
tributions made to your account during any other plan year.
CARRYOVER PROVISION
Amounts allocated to the Health FSA that are unused at the
end of the Plan Year (determined as of the last day of the Run
-Out Period for that Plan Year) up to a maximum of $500
may be used to reimburse Eligible Medical Expenses incurred
in the current Plan Year.
ELIGIBLE HEALTHCARE EXPENSES
The general rule is that any medical expense that is deductible
on your federal income tax return may be reimbursed through
the healthcare flex spending account.
Flexible Spending
Account
HOW THE FLEX ACCOUNT WORKS WITH THE HSA
ACCOUNT (Limited Flex Account)
You may continue to use your debit MasterCard to pay for un-
reimbursed expenses on anything other than medical expenses.
You must use the funds in your HSA account to cover any out of
pocket expenses you incur as a result of obtaining medical care.
Out of pocket expenses for things like dental work and eyeglass-
es would still be covered under the debt MasterCard.
You are responsible to provide receipts, if request-
ed for all transactions processed by the Debit Card.
EXAMPLES OF ELIGIBLE EXPENSES
Alcoholism treat-
ment
Artificial limbs
Car control for the
handicapped
Chiropractor fees
Christian Science
practitioner fees
Contact Lenses
Crutches
Dental fees
Doctor fees
Eyeglasses
Guide Dog
Hearing Aids
Hospital Services
In vitro fertilization
Lab fees
Learning disability
tuition, if referred by
a physician
Nursing services
Optometrist fees
Orthopedics shoes
Oxygen
Orthodontics
Psychoanalysis
Special school for
the handicapped
Sterilization
Surgery
Telephones for
the deaf
Therapy
(medical)
Transplants of
organs
Transportation for
medical care
Wheelchairs
X-rays
EXAMPLES OF INELIGIBLE
HEALTHCARE EXPENSES
Health Clubs, spas,
and non prescribed
weight loss pro-
gram
Expenses covered
by another plan
Smoking cessation
education materi-
als and programs
Hair transplants
Over the counter
medications
Electrolysis
Teeth Whiten-
ing
Cosmetic Sur-
gery unless
medically nec-
essary

19 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
FSA (cont.) &
Direct Deposit
DEPENDENT CARE ACCOUNT
Allows you to reimburse yourself with pre-tax dollars for day-
care expenses for your children under age 13 and other quali-
fied dependents. You may contribute from a minimum of
$300 up to $5,000 a year.
MONEY LEFT IN THE ACCOUNT AFTER
TERMINATION OF EMPLOYMENT
If you have unused money in your account and you terminate
your employment, you must elect to continue the plan through
the COBRA program in order to have access to the unused
healthcare account funds.
EASY BALANCE ACCESS
An automated voice response system designed to provide parti
cipants of the Flexible Spending Account (FSA) and Depend-
ent Care Assistance (DCAP) easy access to their account bal-
ance. You may call Medcom’s regular number 800-523-7542
and continue to “press 1” until you enter the Easy Balance
System which is available around the clock 24/7. Participants
only need to enter their MasterCard debit number, type of
plan (FSA or DCAP), and zip code for primary card holder.
Eligible Day Care Expenses
Childcare/Adult Care by a licensed childcare facility for children
under age 13 who qualify as dependents on your federal income
tax return
Childcare/Adult Care for children or adult of any age who are
physically or mentally unable to care for themselves and who
qualify as dependents.
Ineligible Day Care Expenses
Child support payments
Food, clothing and entertain-
ment
Educational supplies and
activity fees
Cleaning and cooking services
not provided by the day care
provider
Overnight camp
DIRECT DEPOST & PAY CARDS
Aspire requires direct deposit, which means the electronic
deposit of your paycheck to a bank account or other account.
For employees with or without existing bank accounts, a
paycard is an alternative to using a bank account. Aspire has
teamed with two banks to offer a safe and convenient alterna-
tive to paper payroll checks.
FAQs
How does the Paycard VISA work?
Your net pay is automatically deposited to your paycard every
payday. You no longer have to come in person to Human Re-
sources to pick up a paper check. The paycard is a Visa pre-
paid card that will allow you to withdraw your money from
the bank, or use it for purchases at grocery stores, restaurants,
online, and other places you find the Visa logo.
When you pick up your first paycard, you will also get in-
structions for using the card and a schedule of fees. You will
need to call and activate your card before using it for the first
time. You will be asked to confirm personal information to
ensure you are truly the cardholder. If you do not activate the
card, you will not be able to use it.
How does the paycard benefit me?
Having a paycard means no check-cashing fees, no more wor-
ry about how you will pick up your paycheck in the rain or if
you are on vacation, and you have instant access to your mon-
ey on payday instead of waiting for a paper check to be depos-
ited to your account! All of your pay stub information can be
viewed on the employee portal.
How much does it cost? Your paycard is free for most transactions. There are no
monthly charges and you are only charged a fee if you exceed
the free transaction limits. The schedule of fees will be pro-
vided when you receive your paycard.
More information on Direct Deposit and Paycards can be ob-
tained from your HR or PR office.

20 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
Retirement Plan
403(b) RETIREMENT PLAN
Providing a retirement plan that lets you save for the future is
important to us. To better serve all of our Aspire employees
and offer the best possible services and benefits we have
teamed up with Transamerica Retirement Solutions.
WHAT YOU NEED TO DO:
Step 1: Review the highlights of the Aspire Health Partners
Retirement Plan. You can find them along with other
valuable information in the enrollment book located under the
plan information tab at aspire2retire.trsretire.com.
Step 2: Join the plan by visiting aspire2retire.trsretire.com and
selecting "New user? Get started now." Establish a customer
ID and password.
Step 3: You may choose to make pretax contributions up to
the maximum allowed by law. Transamerica Retirement Solu-
tion's free auto-increase service allows you to raise your plan
contribution rate once a year by an amount you choose. You
can sign up for the auto-increase service online at aspire2re-
tire.trsretire.com.
You may designate your contributions as traditional pretax
contributions, after-tax Roth contributions, or a combination
of both.
You should evaluate your ability to continue the auto-increase
service in the event of a prolonged market decline, unexpected
expenses, or an unforeseeable emergency.
Step 4: Contribute enough to take full advantage of your em-
ployer's total contribution.
Aspire Health Partners provides a plan contribution of 2% of
compensation. You will receive the 2% plan contribution re-
gardless of whether you elect to defer into the plan or not.
You will begin receiving this contribution once you have
completed one year and 1,000 hours of service.
After one year and 1,000 hours of service, you are also eligible
to take advantage of your employer's matching contribution
which is based on your level of contribution:
• 4% Employee Contribution (payroll deduction)
2% (50% match on Employee's 4%)
+ 2% Employer Contribution
4% total Employer Contribution
8% Employee Contribution (payroll deduction)
4% (50% match on Employee's 8%)
+ 2% Employer Contribution
6% total Employer Contribution
Employer contributions will begin on either January 1 or July 1
-whichever date occurs first after you meet eligibility. You will
be 100% vested (all employer contributions belong to you)
once you have completed three years of service with any As-
pire Health Partners affiliate.
Matching contributions are subject to plan vesting require-
ments.
Step 5: Decide how your contributions will be invested among
the available investment options.
Designating a beneficiary: Designate at least one beneficiary
for your retirement account, so that your assets can be distrib-
uted according to your wishes upon your death. You can find
the Beneficiary Designation form under the plan information
tab at aspire2retire.trsretire.com.
.

21 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
WHAT IS PAID TIME OFF?
To reward employees for loyal and continuous service, Aspire
Health Partners provides a pre-determined number of paid days
off to observe such occasions as vacations, illness, medical
appointments, personal business or leave of absence.
The Paid Time Off (PTO) program gives you flexibility in
taking paid time off from work. Time away from work will
make you more productive when you are working. Under the
PTO program, you decide, with your supervisor’s approval at
least two weeks in advance, when and how you will use your
PTO hours.
HERE’S HOW IT WORKS
Time off for vacation, personal business, or personal and family
illness is taken utilizing PTO hours. You need to schedule your
time off at least two weeks in advance to allow more efficient
staffing throughout Aspire Health Partners.
ELIGIBILITY
If you are classified as a Full-Time (30+ hours) employee you
are eligible to accrue PTO based upon length of service to the
organization. A staff member is not eligible to use PTO hours
for the first 90 days of employment. You may schedule time off
based on your available hours. Under no circumstances will you
be able to borrow against PTO hours to be earned in the future,
or paid in advance of the regular payday for PTO hours.
PAYMENT METHOD
PTO hours are paid at your base hourly rate of pay in effect at
the time you use the hours.
PERIOD OF ACCRUAL
You accrue hours each pay period to a maximum amount of
320. When your accrued hours fall below 320, you will start
accruing again. The CSD (normally your date of hire) will
change if your status changes from a regular to a non-benefit
eligible position or vice versa.
ACCRUAL AMOUNTS
The chart at the bottom of the page details the maximum
number of hours you accrue in the PTO plan. The maximums
are based on a 80 hours per pay period.
SCHEDULED TIME OFF
Earned PTO hours will be used for personal business any time
during the year, provided such time off has management’s
approval. Jury duty and bereavement times are covered under
separate policies and do not come from the PTO bank.
Requests for PTO hours must be submitted on the appropriate
form with management authorization obtained in advance.
Approvals are made by the employee’s manager based on
periods convenient to the operations of the department.
Preferences for PTO hours will be granted whenever possible.
The approval of request for PTO hours is based on departmental
needs.
OBSERVED HOLIDAYS
Aspire Health Partners observes the following seven holidays:
New Year’s Day, Memorial Day, Independence Day (July 4th),
Labor Day, Thanksgiving Day, Christmas Day and “Floating
Holiday”.
PTO HARDSHIP CASH-OUT PROVISIONS
A PTO hardship is defined as an unexpected expense which
would cause an interruption in the course of everyday living
such as a foreclosure or repossession of property, major repair
for living quarters or transportation. In order to be eligible to
cash out PTO hours due to a hardship case, the employee must
complete a PTO Hardship Request Form and have it approved
by Human Resources. The employee needs to have been
employed for over one year and leave a minimum balance of 80
hours after the cash out of PTO for hardship. Details explaining
the hardship will be required when completing the PTO
Hardship Request Form. Please note a PTO hardship is paid at
75% of the gross amount. A Hardship is not defined as:
Needing to lower the balance of PTO to prevent stoppage
of accrual
Payments for recurring expenses
Purchase of personal merchandise such as a car or furniture
Paid
Time Off
Years of Service Hours per pay period ANNUAL
Hour Days Weeks
0-1.99 3.85 100 12.50 2.5
2-4.99 6.15 160 20.00 4.0
5-8.99 7.08 184 23.00 4.6
9-13.99 8.00 208 26.00 5.2
14+ 9.24 240 30.00 6

22 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
Critical Illness AFLAC
Voluntary Products
Benefits With Cancer Benefit
Heart Attack 100% Percentage of Principal Sum
Stroke 100% Percentage of Principal Sum
Major Organ Transplant 100% Percentage of Principal Sum
End-Stage Kidney Failure 100% Percentage of Principal Sum
Coronary Artery Bypass Graft Surgery 25% Percentage of Principal Sum
Diagnosis of Cancer - Invasive 100% Percentage of Principal Sum
Diagnosis of Cancer In Situ 25% Percentage of Principal Sum
Subsequent Diagnosis of Different Illness Original Percentage of face amount
Time separation for recurrence 90 Days between different illnesses
Available Coverage
Employee 20,000
Spouse 10,000
Child $5,000 at no charge
Guarantee Issue
Employee $20,000
Spouse $10,000
Child (to age 26) None
Health Assessment Benefit (Wellness) $50 subject to 30 day waiting period
Pre-Existng Conditional Limitations 6/12
Benefit Reduction None
Limit on Number / Amount of Claims Each claim category will be paid once
Waiting Period 30 Days
CRITICAL ILLNESS
A critical illness plan helps prepare you for the added costs of battling a specific critical illness. The good news is that many peo-
ple with a specified critical illness survive these life-threatening battles. Unfortunately, as the recovery process begins, people
become aware of the unexpected bills that have piled up. Your recovery doesn’t have to be spoiled by unexpected bills. With this
plan, our goal is to help you and your family cope with and recover from the financial stress of surviving a specified critical ill-
ness. Listed below is a brief summary of the benefits.
AFLAC Critical Illness Bi-Weekly Payroll Deductions
EMPLOYEE $20,000 SPOUSE $10,000
ISSUE AGE BI WEEKLY ISSUE AGE BI WEEKLY
18-29 10.67 18-29 5.60
30-39 10.67 30-39 5.60
40-49 20.83 40-49 10.67
50-54 31.94 50-54 16.34
55-59 43.11 55-59 21.92
60-64 69.42 60-64 35.08
65-69 75.60 65-69 38.17

23 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
Emergency Care
Ambulance $450
Emergency Room $300
Treatment Care
Hospital Admission $1,000
Hospital Confinement Daily Benefit $300 / Day up to 365 Days
Intensive Care Unit Daily Benefit $500 / Day up to 30 Days
Specific Injuries or Treatments
Blood $250
Joint Dislocation $400-$4,500 Closed / $600-$6,750
Spouse & Children paid at 50% of Employee Amount
Dental Crown $250
Laceration $50 - $400
Ruptured Disc $100 - $400
Fractures (Per Fracture)
Leg (knee to ankle) $3,600 / $5,400
Ankle, arm, bones of face, collarbone, elbow, foot,
hand, jaw, kneecap, shoulder blade, wrist $1,800-$3,000 / $2,700-$4,500
Accidental Death & Dismemberment
Accidental Death of Employee $75,000
Accidental Death of Spouse $37,500
Accidental Death of Child $10,000
Loss of or loss of use of one: hand, foot , arm, leg or
eye $18,750 EE / $9,375 SP / $2,500 CH
Catastrophic loss $37,500 EE / $18,750 SP / $10,000
Health Assessment Benefit (Wellness) $60 Subject to 12 month wait period
Pre-Existing Condition Limitations 6/12
Limit on Number / Amount of Claims Limited to 150% for multiple fractures or dislocations
Off Job Coverage
Payroll Deductions
Employee Only $5.84
Employee & Spouse $7.61
One Parent Family $10.75
Employee & Family (children to age 26) $12.52
Accident AFLAC
Voluntary Products
ACCIDENT
An accident insurance plan provides benefits to help cover the costs associated with unexpected bills. You don’t budget for accidents
if you’re like most people. When a Covered Accident occurs, the last thing on your mind is the charges that may be accumulating
while you’re at the emergency room. These costs add up—fast. You hope they never happen, but at some point you may take a trip to
your local emergency room. If that time comes, wouldn’t it be nice to have an insurance plan that pays benefits regardless of any
other insurance you have? This group accident plan does just that. Listed below is a brief summary of the Accident Policy.

24 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
Employee
Assistance Plan
EmployeeConnect Services There are times when we all need a little help. No matter
what the issue, EAP Plus counseling services are availa-
ble 24 hours a day, seven days a week with confidential
support, guidance, and resources.
Assistance for you or an immediate household
family member.
Six in-person counseling sessions per person
per issue per year.
24 x 7 x 365 telephone and Web access.
Unlimited phone access to legal counsel.
25% discount for in-person legal services.
Work/life services for assistance with:
Parenting and Childcare
Eldercare
Relationships
Work and career
Financial
To learn more about the Lincoln Financial EmployeeConect
program visit:
www.Lincoln4Benefits.com or
www.GuidanceResources.com
(User name=LFGsupport; password=LFGsupport1)
or talk with a specialist at 1-888-628-4824.
LifeKeys Services When you choose life insurance, you’re planning for your
family’s future assuring their comfort and securing their
plans. With Lincoln Term Life Insurance, you can also access
services that make a real difference now as well as in the fu-
ture. LifeKeys services, included at no additional cost with all
Lincoln Term Life and Accidental Death and Dismemberment
Insurance policies, provide assistance to you, your family and
your beneficiaries.
EstateGuidance® Will Preparation
GuidanceResources® Online
Identity Theft
Legal Support
Other support services
To utilize LifeKeys services, please contact 1-855-891-3684
or visit GuidanceResources.com or
www.lincoln4benefits.com (WebID= LifeKeys)
TravelConnect Traveling just got easier.
An employee benefit that includes travel, medical, and safety
related services while traveling. Lincoln Financial has part-
nered with MEDEX Assistance Corporation, a worldwide
leader in travel assistance, to make this valuable benefit avail-
able to you and your immediate family members.
Business or leisure travel – it’s covered.
The TravelConnect benefit is provided at no cost to you and
includes a wealth of services when traveling just 100 miles or
more from home. These services are provided regardless if
you’re traveling for business or leisure. Whether you simply
want the weather forecast for your travel destination or you
need emergency medical assistance halfway around the
world, MEDEX has the professional staff and resources to
provide support, 24 hours a day, seven days a week.
Comprehensive coverage.
Just a sampling of the services includes:
Destination info – weather, currency, etc.
Emergency travel arrangements and funds transfer.
Lost or stolen travel documents assistance.
Language translation services.
Emergency medical evacuation and transportation.
Dependent child transportation if left unattended.
Medical and dental referrals.
Assistance with corrective lenses or medical device re-
placement.
Treatment monitoring of a medical situation.
Arrange delivery of medications, vaccines, or blood.
Updates to family, employer, and/or home physician.
Repatriation of a deceased traveler.
Security and political evacuation assistance.
Travel assistance services are subject to specific terms, condi-
tions and limitations. A program description is available at
www.lincoln4benefits.com. To use TravelConnect services,
call MEDEX at (800) 527-0218 or (410) 453-6330.

25 This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
Key
Contacts COMPANY CONTACT INFORMATION WEBSITE/ EMAIL
UNITED HEALTHCARE
Customer Service
866-844-4864 Gold and Silver
866-734-7970 Bronze
Claims: PO Box 740835
Atlanta, GA 30374
www.myuhc.com.
United Behavioral Mental Health:
800-582-8220 or 800-557-5745
UNITED HEALTHCARE
Dental 800-445-9090 www.myuhcdental.com
Vision 800-638-3120 www.myuhcvision.com
OPTUM BANK
Health Savings Account 866-234-8913 www.optumbank.com
LINCOLN FINANCIAL
Life Claims & Customer Service
Short-Term & Long-Term Disability 800-423-2765 www.lfg.com
LINCOLN FINANCIAL
Employee Assistance Program
EmployeeConnect Services 877-757-7587
LifeKeys Services 855-891-3684
TravelConnect 800-527-0218
www.lincoln4benefits.com
FLEXIBLE SPENDING ACCOUNT
Medcom
Customer Service
800-523-7542
Email claims to:
Check your debit card:
www.mywealthcareonline.com/medcom
LASSITER-WARE INSURANCE
Employee Customer Service
800-845-8437 ext. 605
Fax 888-883-8680 [email protected]
AFLAC VOLUNTARY PRODUCTS PORTFOLIO
AFLAC 800-443-3036
WebSite: www.aflac.com
Email: [email protected]
TRANSAMERICA RETIREMENT SOLUTIONS
Transamerica 800 755-5801 aspire2retire.trsretire.com
ASPIRE HEALTH PARTNERS
Human Resources Department
Jannette Mulero
407-875-3700 x6025
Linda Lovett
407-875-3700 x3222
This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
This Notice is provided as required by the Federal Health Insurance Portability and Accountability Act of 1996, as amended (“HIPAA”) and its regulations issued at 45 CFR Parts 160 through 164 (the “Privacy Regulations”). It is for partici-pants and beneficiaries in the (referred to as the “Plan”).
You are entitled to receive a notice of our procedures for protecting the privacy of your health information. “Protected Health Information” is information that identifies you and is related to your medical history for health care you receive or the payment for that care. We must follow the terms of the notice currently in effect. This notice describes how we may use or disclose your Protected Health Information and your rights regarding the use and disclosure of that information.
You may also receive privacy notices from others, such as other health care plans, insurers (including HMOs) and providers about their use and disclosure of your health information.
HOW THE PLAN MAY USE AND DISCLOSE YOUR PROTECTED HEALTH
INFORMATION
The Plan may use and disclose your Protected Health Information for different purposes. The examples below illustrate the types of uses and disclosures we may make without your authorization for treatment, payment and health care operations.
Treatment. The Plan may disclose your Protected Health Information to assist your health care providers (doctors, pharmacies, hospitals and others) in your diagnosis and treatment. For example, The Plan may disclose to one treating physician the name of another treating physician so that he or she can obtain records or other information needed for diag-nosis or treatment.
Payment. The Plan may use and disclose your Protected Health Infor-mation in order to pay for your covered health expenses. For example, we may use your Protected Health Information to enroll you for coverage or to determine if a claim for benefits is covered under the Plan (e.g., if treat-
ment is medically necessary).
Health Care Operations. The Plan may use and disclose your Protected Health Information in order to perform Plan activities, such as quality as-sessment and improvement activities, reviewing competence or qualifica-tions of health care providers, underwriting, premium rating and other insurance activities relating to creating or renewing insurance contracts. Other activities include disease management, case management, conduct-ing or arranging for medical review, legal services and auditing functions, including fraud and abuse compliance programs, business planning and development, business management and general administrative activities. For example, The Plan may use information about your claims to refer you to a disease management program.
Plan Sponsor. The Plan discloses your medical information to , which sponsors the Plan, for Plan administration purposes that are described in the document that governs the specific Plan. The Plan Sponsor will be required to certify to us that it will use your medical information in accord-ance with the Privacy Regulations.
Enrolled Dependents and Family Members. The Plan will mail explana-tion of benefits forms and other mailings containing Protected Health Infor-mation to the address we have on record for the employee who is enrolled in the health plan.
OTHER PERMITTED OR REQUIRED DISCLOSURES
To Your Family Member, Other Relative or Close Personal Friend. The Plan may disclose Protected Health Information to a family member, other relative or close personal friend provided that information is directly relevant to that person’s involvement in your health care or to notify them of your location, general condition or death. The Plan will not make any such disclosure unless you are given a reasonable opportunity under the circumstances to object and did, in fact, object.
As Required by Law. The Plan must disclose Protected Health Infor-
mation about you when we are required to do so by law.
Public Health Activities. The Plan may disclose Protected Health Information
to public health agencies for reasons such as preventing or controlling disease, injury or disability. This includes disclosures necessary to report product de-fects, to permit product recalls and to conduct post-marketing surveillance. Protected Health Information may also be used or disclosed if you have been exposed to a communicable disease or are at risk of spreading a disease or condition, if authorized by law.
Victims of Abuse, Neglect or Domestic Violence. The Plan may disclose Protected Health Information to government agencies about abuse, neglect or domestic violence if there is a reasonable belief that you may be a victim of abuse, neglect to domestic violence. In that case, The Plan will promptly in-form you that a disclosure has been or will be made unless that notice would cause a risk of serious harm. For purposes of reporting child abuse or neglect, it is not necessary to inform the minor that such disclosure has been or will be made. Disclosure may generally be made to the minor’s parents or other rep-resentatives although there may be circumstances under federal or state law when the parents or other representatives may not be given access to the minor’s Protected Health Information.
Health Oversight Activities. The Plan may disclose Protected Health Infor-mation to government oversight agencies (e.g., U.S. Department of Labor) for oversight activities authorized by law. This includes uses or disclosures in civil, administrative or criminal investigations; inspections licensure or disciplinary actions (for example, to investigate complaints against providers); and other activities necessary for appropriate oversight of government benefit programs.
Judicial and Administrative Proceedings. The Plan may disclose Protected
Health Information in response to a court or administrative order. The Plan may also disclose Protected Health Information about you in certain cases in response to a subpoena, discovery request or other lawful process. In such case, The Plan will require satisfactory assurances that the requesting party has made a good faith attempt to provide written notice to you, and the notice provided sufficient information about the proceeding to permit you to raise an objection and no objections were raised, or if any were raised, that they were
resolved in favor of disclosure by the court or tribunal.
Law Enforcement. The Plan may disclose Protected Health Information under limited circumstances to a law enforcement official in response to a warrant or similar process; to identify or locate a suspect or witness; or to provide infor-mation about the victim of a crime. Such disclosures include disclosing infor-mation about an individual who is or is suspected to be a victim of a crime, but only if the individual agrees to the disclosure, or the Plan is unable to obtain the individual’s agreement because of emergency circumstances. The law en-forcement official must represent that the information is not intended to be used against the individual, the immediate law enforcement activity would be materi-ally and adversely affected by waiting to obtain the individual’s agreement, and disclosure is in the best interest of the individual as determined by us in our sole discretion.
Coroners, Funeral Directors, Organ Donation. The Plan may release Pro-tected Health Information to coroners or funeral directors as necessary to allow them to carry out their duties. The Plan may also disclose Protected Health Information in connection with organ or tissue donation.
Plan Information and Programs. The Plan may contact you to provide infor-mation about alternative treatment programs or other health-related benefits and services that may be of interest to you.
Research. Under certain circumstances, the Plan may disclose Protected Health Information about you for research purposes, provided certain measures have been taken to protect your privacy.
To Business Associates. We may disclose Protected Health Information to a “business associate”, provided that person or entity enters into an agreement as described in the Privacy Regulations. A “business associate” is a vendor that provides certain services (typically Plan administration services) to or on behalf of the Plan.
To Limited Data Recipients. The Plan may disclose Protected Health Infor-mation to a “limited data recipient”, provided that person or entity enters into an agreement as described in the Privacy Regulations. A “limited date recipient” is a person or entity that receives Protected Health Information that is partially de-identified in accordance with the Privacy Regulations and used for purposes
of research, public health or health care operations.
NOTICE OF PRIVACY
RIGHTS
THIS NOTICE DESCRIBES HOW PROTECTED HEALTH INFORMATION ABOUT YOU
MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
PLEASE REVIEW IT CAREFULLY.

This is for illustrative purposes only. For a more detailed description of benefits, please refer to your Certificate of Coverage
NOTICE OF PRIVACY
RIGHTS
THIS NOTICE DESCRIBES HOW PROTECTED HEALTH INFORMATION ABOUT YOU
MAY BE USED AND DISCLOSED AND HOW YOU CAN GET ACCESS TO THIS INFORMATION.
PLEASE REVIEW IT CAREFULLY.
NOTICE OF PRIVACY RIGHTS continued…..
Marketing. The Plan may use Protected Health Information for purposes of marketing where it is face-to-face and involves a matter of nominal value.
To Avert a Serious Threat to Health or Safety. The Plan may disclose your Protected Health Information, with some limitations, when necessary to prevent a serious threat to your health and safety or the health and safety of the public or another person.
Special Government Functions. The Plan may disclose information as required by military authorities or to authorized federal officials for national security and intelligence activities.
Workers’ Compensation. The Plan may disclose Protected Health Infor-
mation to the extent necessary to comply with state law for workers’ com-pensation programs or similar programs established by law.
Incidental to Another Permitted Use. The Plan may disclose Protected Health Information as permitted by the Privacy Regulations to be incidental to another permitted use.
YOUR RIGHTS REGARDING YOUR PROTECTED HEALTH INFORMATION
You have certain rights regarding Protected Health Information that the Plan maintains about you.
Right To Access Your Protected Health Information. You have the right to review or obtain copies of your Protected Health Information from a “designated record set” with some limited exceptions. A designated record set includes the medical and billing records about you that a covered health care provider maintains. It includes enrollment, billing, claims pay-ment and case or medical management records maintained by us or for the Plan. Your request to review and/or obtain a copy of Protected Health Information in your designated record set must be made in writing. The Plan may charge a fee for the costs of producing, copying and mailing your requested information, but the Plan will tell you the cost in advance.
If access is denied, you will be provided with a written denial explaining the basis for the denial, a description of how you may exercise those review rights and a description of how you may complain to the Secretary of the U.S. Department of Health and Human Services.
Right To Amend Your Protected Health Information. If you believe that Protected Health Information about you in a designated record set (maintained by the Plan) is incorrect or incomplete, you may request that the Plan amend the information. Your request must be made in writing and must include the reason you are requesting a change. Your request may be denied, for example, you ask the Plan to amend information that was not created by the Plan or that is already accurate and complete. If the request is denied, you must be provided with a written denial that explains the basis for the denial. You may then submit a written statement of disa-
greement.
Right to an Accounting of Disclosures by the Plan. You have the right to
request a list of certain disclosures the Plan has made of your Protected Health Information. The request must be in writing. If you request an ac-counting for the same time period more than once within a 12-month period, the Plan may charge a reasonable fee.
Right To Request Restrictions on the Use and Disclosure of Your Pro-tected Health Information. You have the right to request that the Plan restrict the way it uses or discloses your Protected Health Information for treatment, payment or health care operations. The Plan may not agree to your request. Your request for a restriction must be made in writing. In your request you must tell the Plan (1) what information you want to limit; (2) whether you want to limit how the Plan uses or discloses your infor-mation, or both; and (3) to whom you want the restrictions to apply.
Right To Receive Confidential Communications. You have the right to
request that the Plan use a certain method to communicate with you or that information be sent to a certain location. Your request to receive confiden-tial communications must be made in writing. Your request must clearly state that all or part of the communication from the Plan could endanger you. The Plan will accommodate all reasonable requests.
Right to a Paper Copy of This Notice. You have a right at any time to request a paper copy of this Notice, even if you had previously agreed to receive an electronic copy. To request a paper copy of this Notice, you must contact the Privacy and Complaint Officer identified at the end of this Notice.
Contact Information for Exercising Your Rights. You may exercise any of the rights described above by contacting your companies Privacy and Complaint Officer.
PERSONAL REPRESENTATIVES
Your personal representative may exercise your rights. The representative must produce evidence of his/her authority to act on your behalf before that person will be given access to your Protected Health Information. Proof of such authority may be in one of the following forms:
a power of attorney for health care purposes,
notarized by a notary public;
a court order of appointment of the person as the conservator or guardian of the individual; or
the parent of a minor child.
The Plan may deny access to your Protected Health Information to a personal representative in order to protect certain individuals who depend on others to exercise their rights under the Privacy Regulations and who may be subject to abuse or neglect, including minors.