benefits of - who.int · benefits and risks of art ... pre-preg cart during preg azt >4 wk...
TRANSCRIPT

Benefits and Risks of ART
Dr Paula Munderi
WHO Training Course for Introducing Pharmacovigilance of HIV Medicines
23 ‐ 28 November 2009, Dar Es Salaam

Summary
Progress in ART coverage ‐ WHO Progress Report
Benefits of ART
Survival
Decreased Morbidity
Decreased Transmission
Vertical & Horizontal
Principles of ART
Measurement of efficacy
Risks of ART linked to AEs and Toxicities
Adherence : determinant of ART efficacy
Special Populations : Women & Children
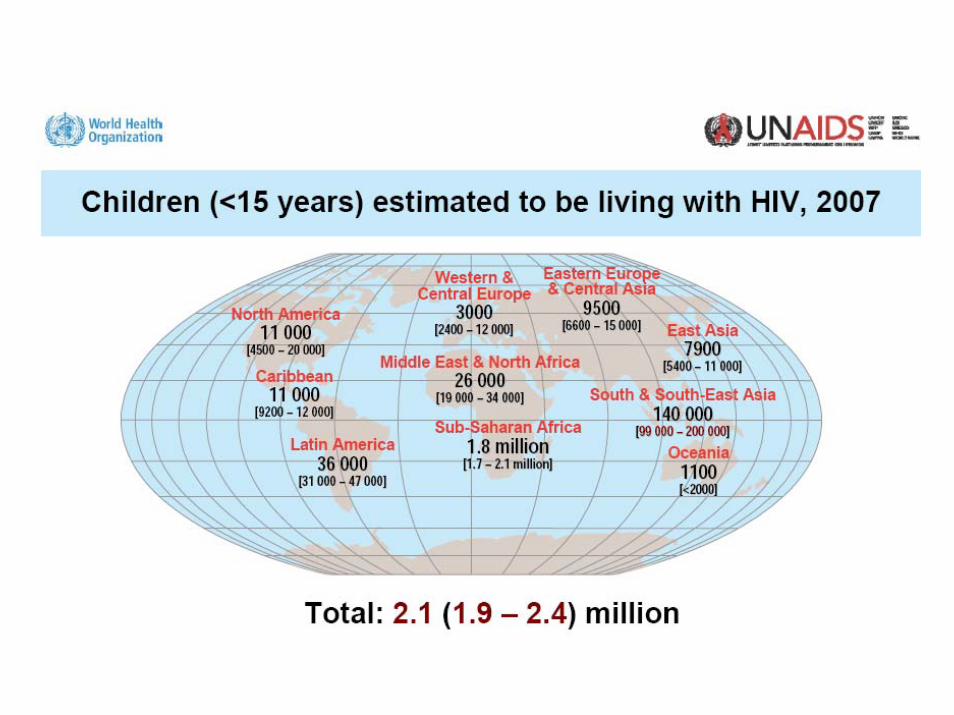
Epidemiology of Paediatric HIV
Pregnancy and ART
Co‐morbidities of specific concern : TB, HepB, Hep C, (Malaria)
Programme implications
Selection of ARVs in the PH approach
ART principles & recommendations
Current ART practice in LMIC
What this means for countries

AcknowledgementsSources of Slide Material
Published data
WHO progress report on access 2009
Jens Lundgren
Lynne Moffenson
WHO HQ ‐ HIV Dept (ATC team)
DART study group

IBenefits of ART
•Improved Survival
•Reduced morbidity
•Reduced vertical transmission of HIV
•Possibly – reduced horizontal transmission of HIV

Number of people receiving antiretroviral therapy in low‐ and middle‐income countries, by region, 2002–2008
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
End 2002 End 2003 End 2004 End 2005 End 2006 End 2007 End 2008
Mill
ions
North Africa and the Middle East
Europe and Central Asia
East, South and South-East Asia
Latin America and the Caribbean
Sub-Saharan Africa

Reduced Death rates over time
on ART
Rate per 100 person years
0‐1 years 17.9 [14.5 – 22.1]
1‐2 years 2.3[14.5 – 22.1]
2‐3 years 1.2 [0.5‐3.3]
Castelnuovo B, Manabe YC, Kiragga A et al CID 2009; 49:965–72

DART Study Group. IAS July 2009
Survival impact of ART
0.90
0.87
0.08
0.92
0.90
0.18
0.95
0.94
0.55
0 1 2 3 4 5
0.0
0.2
0.4
0.6
0.8
1.0
Prop
ortio
n alive
Years from enrolment into cohort
Entebbe Cohort(same community)
NO ART available1996‐2000
median CD4 75 at enrolment
57.7/100 PY
LCM: 2.2/100 PY
CDM: 2.9/100 PY
median CD4 86 at enrolment
DART cohortART: 2003 ‐ 2008
‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐

DART Study Group: XVI INTERNATIONAL AIDS CONFERENCE 2006
Impact of ART on causes of death Pre-ART cohort: ECn = 516 PYO = 658
Oct 95 - Dec 00
Post-ART cohort: DARTn = 1015 PYO = 1819
Feb 03 - Jan 06
Deaths (rate/100PY) Deaths (rate/100PY)
Specific HIV-related causes 118 (17.9) 27 (1.5)
Cryptococcus 64 (9.7) 4 (0.2)
Cryptosporidium 18 (2.7) 2 (0.1)
Tuberculosis 16 (2.4) 10 (0.5)
HIV-related malignancy 11 (1.7) 6 (0.3)
Bacteraemia 3 (0.5) 5 (0.3)
CMV 4 (0.6) 0 (0)
Severe anaemia 2 (0.3) 0 (0)
Syndrome likely HIV related 176 (26.7) 18 (1.0)
Wasting (+/- diarrhoea) 111 (16.9) 1 (0.1)
Febrile event 48 (7.3) 12 (0.7)
Neurological event 17 (2.6) 5 (0.3)
Cause not HIV-related 4 (0.6) 6 (0.3)
Unknown cause 82 (12.6) 11 (0.6)
Total deaths 380 (57.7) 62 (0.3)

Malaria – DART cohort

1%6%
11%
21%
32%
0
10
20
30
40
% T
rans
mis
sion
<400 400-3000
3000-40000
40000-100000
>100000
Delivery Plasma HIV RNA
Vertical Transmission – Maternal Viral Load in absence of ART
Blattner W. XIII AIDS Conf, July 2000, Durban S Africa (LBOr4) WITS study, 1990-1999

PregnancyPre-natal
15 %
5% 10%
Breast-feedingPost-natal
Timing of vertical transmission for 30%
DE LIVERY
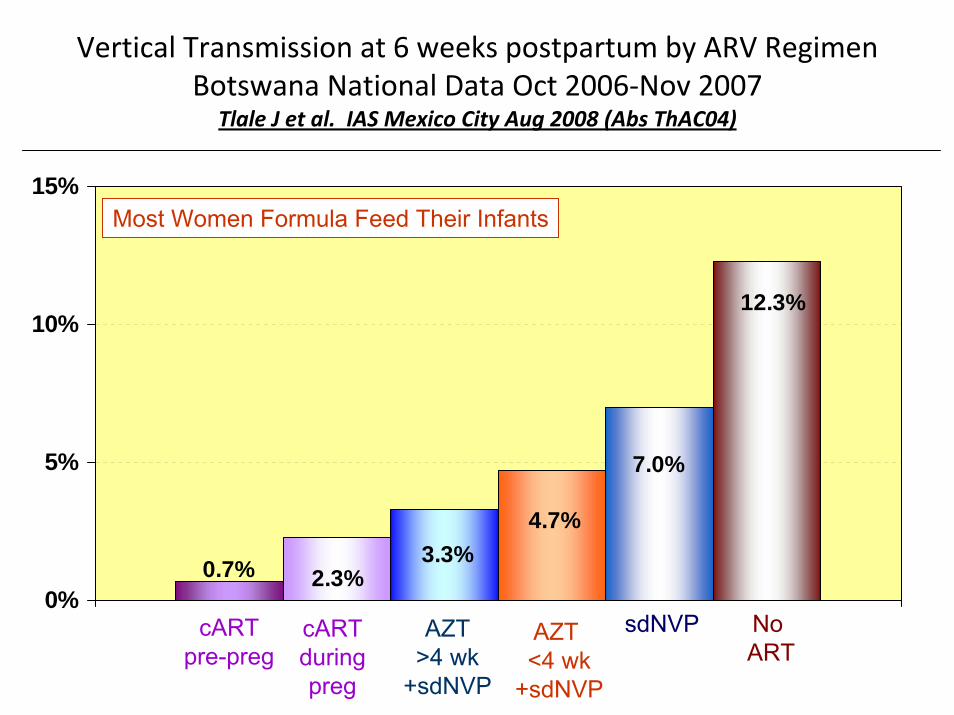
Vertical Transmission at 6 weeks postpartum by ARV Regimen Botswana National Data Oct 2006‐Nov 2007
Tlale J et al. IAS Mexico City Aug 2008 (Abs ThAC04)
0.7% 2.3%3.3%
4.7%
7.0%
12.3%
0%
5%
10%
15%
cARTpre-preg
cARTduringpreg
AZT>4 wk
+sdNVP
AZT <4 wk
+sdNVP
sdNVP No ART
Most Women Formula Feed Their Infants

Vertical transmission of HIV
15-35%
<1% Antenatal screenMaternal ARTNeonatal ARTC. sectionNo breastfeeding

« Les personnes séropositives ne souffrant d’aucune autre MST et suivant un traitement antirétroviral efficace ne transmettent pas le VIH par voie sexuelle »
Commission fédérale pour les problèmes liés au sida (CFS), Commission d’experts clinique et thérapie VIH et sida de l’Office fédéral de la santé publique (OFSP)
P Vernazza, B Hirschel, E Bernasconi, M Flepp. Bulletin des médecins suisses 2008;89: 5
Scientific basis: Effective ART → undetectable HIV ‐ RNA
Epidemiologic basis :
vertical transmission
is related to plasma HIV‐RNA
• e.g PMTCT

Longitudinal studies in HIV sero‐discordant couples
393 couples followed for 14 years
no transmission from person on cART
8.6 % transmission with no cART 1
‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐
93 couples; in 41 +ve partner on cART
6 infections – all in non treated 2
‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐
62 couples; Males +ve
pregnancy desired
no infection in female partner3
Rwanda & Zambia
• 2, 993 couples
• followed from 2002 – 2008
• HIV testing every 3 months
• 5’609 person years
• 4 HIV infections from partners on cART
• 171 infections partners not on cART
Incidence density of HIV transmission 4
0.7% on cART vs 3.4% off cART
[RR = 0.21, CI: 0.08, 0.59]
NB: HIV persists in semen and cervicovaginal fluid during effective cART

ARVs for Prevention
• PEP & PMTCT
• Universal Test & Treat– combination ART
• Pre‐ Exposure prophylaxis (PrEP)– Tenofovir
• ARVs as “ vaginal microbicides”– Tenofovir
– Maraviroc
IIPrinciples of ART
•Combination therapy
•Avoidance of resistance•Importance of adherence

For sustained efficacy of ART ...
• synergistic combinations of ≥ 3 active drugs usually from 2 different classes – single or dual drug therapy only in PMTCT; low risk PEP
• the large number of possible combinations is only apparent – cross resistance develops within classes – Cross resistance may occur between NRTIs and NNRTIs
• preserving future treatment options is critical– choice of initial regimen – rational sequencing of combinations thereafter

Measurement of efficacy of ART
When is treatment working?
• Absence of clinical disease– WHO clinical staging
• Immune restoration– Rise in CD4 count
• Viral suppression– Undetectable VL
When has treatment failed
• Recurrence of clinical illness– WHO stage II/III/IV
• Fall in CD4 count– to below 100 cells/mm3
• Detectable VL– to >5000 copies/ml

Resistant virus
Wild-type virus
10-2
0%

Drug pressure
Resistant virus
Wild-type virus
10-2
0%

Adherence – Efficacy
Nachega et al, Ann Intern Med, 2007Nachega et al, Ann Intern Med, 2007

IIIRisks of ART
Mainly related to toxicities

NB: Most ART Toxicities are ...
‐ Predictable
‐ Clinically detectable
‐ Can be managed
The key is patient and provider education !

Main reasons of discontinuationof first cART regimen within1st year: ICONA cohort
I C ON A
ItalianCohort
NaiveAntiretroviral
Monforte et al. AIDS 1999
ToxicityFailureNon-adherenceOtherContinued

Reasons for change of a first combination ART regimen
N 107 87 133 161 138 Median CD4 300 326 382 363 418 p=0.0013Median VL 3.26 2.81 2.60 2.46 2.60 p=0.0022
Reason N CD4 VL
Unknown 49 312 2.26
Other 112 391 2.60
Choice 189 364 2.60
Toxicities 190 386 2.28
Failure 86 328 3.78
p=0.27 p<0.0001
EuroSIDA: Mocroft et al, AIDS Research Hum Retro, 2005

Castelnuovo B, Manabe YC, Kiragga A et al CID 2009; 49:965–72
ART Toxicity related deaths:1st year ‐ 1 Hepatotoxicity, 2 Lactic acidosis2nd year ‐ 1 Hepatotoxicity; 2 lactic acidosis; 1 pancreatitis

NB: Most ART Toxicities are ...
‐ Predictable
‐ Clinically detectable
‐ Can be managed
The key is patient and provider education !

IV
Women & Children
•Pregnancy• In utero & Perinatal exposure to ARVs• cART in children

Incidence of Seroconversion in Pregnancy: Prevention of HIV in Pregnant Women is Critical
Country Reference Incidence per 100 Pt‐YrsPregnancy
Uganda Gray R et al. Lancet 2005;366:1182
2.3
Botswana Lu L et al. 2009 CROI Abs.94LB 1.3 (0.5‐3.1)
Zimbabwe, Uganda
Morrison CS et al. AIDS 2007;21:1027
1.6
South Africa Rehle T et al. S Afr Med J 2007;97:194
5.2 (0‐12.9)
South Africa Moodley D et al. AIDS 2009;23:1255
10.7 (8.2‐13.1)

43% of New Infant Infections in Botswana May be Due to Maternal Seroconversion in Pregnancy/PP
Lu L et al . 16th CROI, Montreal, Canada Feb 2009 Abs 94LB
HIV diagnosed before or
during ANC
New maternal infection late pregnancy
New maternal infection 1 yr postpartum
# HIV+ women
13,952 378 (incidence 1.3%)
450(incidence 1.8%)
Estimated MTCT rate
4.7%(with PMTCT ARV)
73% 36%
# infected infants
620 276 186
Of the estimated 1,082 infant HIV infections inBotswana in 2007, 462 (43%) were due to
incident cases of maternal HIV in pregnancy/PP

Unintended Pregnancy Among HIV‐Infected Women
• 51% unintended pregnancies among women with HIV in Cote d’Ivoire.
• 74% unintended pregnancies among women in HIV care in Rwanda.
• 84% unintended pregnancies among PMTCT clients in South Africa.
• 93% unintended pregnancies among women in HIV-ART care in Uganda. Desgrees‐du‐Lou A et al. Int J STD AIDS 2002
Bangendanye, 3rd Ped CLS 2007Rochet T et al. JAMA 2006Homsy J et al. PLosOne 2009
Prevention of HIV in Women,
(Especially Young
Women)
Prevention of
Unintended Pregnancies
in HIV-Infected
Women
Prevention of
Transmission from an
HIV-Infected Woman
to Her Infant
Support for HIV-Infected Mother and
Family

<1 year 1‐2 years 2‐3 years 3‐4 years >4 years
Time since enrolment in DART
Incide
nce rate per
100 wom
an years
0
2
4
6
8
10
12
14
16
18
Age at enrolment
18‐29 yrs30‐34 yrs35‐39 yrs40‐44 yrsAll women <45
Incident pregnancy on ART – DART cohort

Physiologic Changes During Pregnancy Can Affect Therapeutic Drug Administration
• Increased plasma volume
– dilution effect
• Decreased in serum albumin
– increase in free fraction of drug
• Increased GFR 20‐60% starting 1st trimester
– change in drug clearance
• Changes in hepatic enzyme activity
– increase CYP34A, 2D6 = change in drug metabolism
• Decreased gastric acid secretion, prolonged gastric emptying andintestinal transit time
– decreased oral drug absorption

Pregnancy & Antiretroviral PharmacokineticsNRTIs
Abacavir No ∆Didanosine No ∆Emtricitabine No ∆Lamivudine No ∆Stavudine No ∆Zidovudine No ∆
NUCLEOTIDESTenofovir AUC↓
NNRTIsEfavirenz No dataEtravirine No dataNevirapine No ∆
PIsAtazanavir AUC ↓Darunavir No dataFosamprenavir AUC ↓?Indinavir AUC ↓Lopinavir/rit AUC ↓Nelfinavir AUC ↓Ritonavir AUC ↓Saquinavir AUC ↓Tipranavir No data
FUSION INHIBITORSEnfuvirtide No data
CCR5 CO-RECEPTOR ANTAGONISTSMaraviroc No data INTEGRASE INHIBITORS
Raltegravir No data
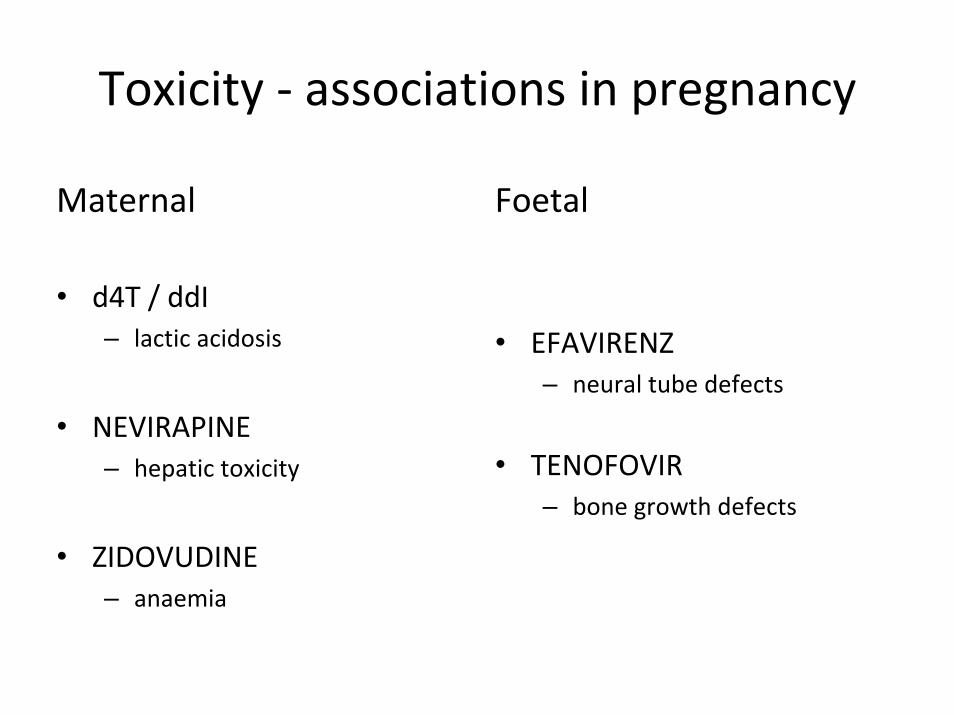
Toxicity ‐ associations in pregnancy
Maternal
• d4T / ddI– lactic acidosis
• NEVIRAPINE– hepatic toxicity
• ZIDOVUDINE– anaemia
Foetal
• EFAVIRENZ– neural tube defects
• TENOFOVIR– bone growth defects

Antiretroviral Pregnancy Registry1/89‐ 1/09 Prospective Cases (http://www.APRegistry.com)
% Birth Defect
Atazanavir sulfate-containing (7/292) ABC-containing (18/608)AZT-containing (95/3108)3TC-containing (93/3226)d4T-containing (19/754) Indinavir-containing (6/276)Nelfinavir-containing (37/1074) Nevirapine-containing (18/817)Ritonavir-containing (20/883) Lopinavir-containing (8/470)Tenofovir-containing (16/678)ddI-containing (16/365)
2.4% (1.0 - 4.9%)3.0% (1.8 – 4.6%)3.1% (2.5 - 3.7%)2.9% (2.3 - 3.5%)2.5% (1.5 – 3.9%)2.2% (0.8 - 4.7%)3.4% (2.4 – 4.7%)2.2% (1.3 – 3.5%)2.3% (1.4 – 3.5%)1.7% (0.7 – 3.3%)2.4% (1.4 – 3.8%)4.4% (2.5 – 7.0%)
CDC general birth defect surveillance 2.7% (2.7-2.8%)
1st trimester any ARV exposure 2.9% (2.4 - 3.4%)

HIV negative but exposed childrenfollowing in utero exposure to ARVs
Clinically symptomatic mitochondrial dysfunction – rare 0.3% ‐ 3 per 1,000– very rarely (0.07% ‐ 7 per 10,000) can be fatal
Mild, clinically asymptomatic, but persistent hematologic abnormalities – anaemia, neutropenia
Transient elevations in lactic acid – common with in utero exposure – usually asymptomatic– resolve within months

ARV toxicities in treated childrensimilar spectrum to adults
Of particular importance in children:
Metabolic abnormalities– hyperlipidaemia
– glucose intolerance
Fat redistribution
Bone density & growth