biocompatibles satellite symposium at gest 2011 review of treatment algorithms and procedural...
TRANSCRIPT

Biocompatibles Satellite Symposium at GEST 2011
Review of Treatment Algorithms and
Procedural Standards for DC Bead in HCC
Professor Riccardo Lencioni
Director, Diagnostic Imaging and InterventionDepartment of Hepatology and Liver Transplantation
Pisa University Hospital and School of Medicine, Pisa, Italy

Llovet JM, DiBisceglie A, Lencioni R, et al.
EASL-EORTCClinical Practice Guideline:Hepatocellular Carcinoma
Journal of Hepatology, 2011 - European Journal of Cancer, 2011

Portal pressure/bilirubin
HCC
Ablation Sorafenib
Stage 0PST 0, Child–Pugh A
Very early stage (0) 1 HCC < 2 cm
Carcinoma in situ
Early stage (A)1 HCC or 3 nodules
< 3 cm, PST 0
End stage (D)
Liver transplantation TACEResection Symptomatictreatment (20%)
Survival < 3 monthsCurative treatments (30%)
5-year survival 40–70%Palliative treatments (50%)
Median survival 11–20 months
Associated diseases
YesNo
3 nodules ≤ 3 cm
Increased
Normal
1 HCC
Stage DPST > 2, Child–Pugh C
Intermediate stage (B)Multinodular,
PST 0
Advanced stage (C) Portal invasion, N1, M1, PST 1–2
Stage A–CPST 0–2, Child–Pugh A–B
Treatment of Hepatocellular Carcinoma (HCC):The BCLC Staging System
adapted from Llovet JM, DiBisceglie A, Lencioni R, et al. (in press)

Cancer Treat Rev 2011;37:212-220
Clinical Management of Hepatocellular Carcinoma: Building Multidisciplinary Consensus
• Compared with conventional TACE, drug eluting bead has a standardized methodology, is more reproducible, and offers improved response and a significantly better safety profile.

Drug eluting bead vs conventional TACE: A randomized trial (“PRECISION V”)
Lammer J et al. Cardiovasc Intervent Radiol 2010;33:41-52

p=0.001
0
50
100
150
200
250
300
AS
T U
nit
s/L
DC Bead cTACE
0
50
100
150
200
AL
T U
nit
s/L
p<0.001
p=0.001
Drug-related adverse events Liver toxicity (AST – ALT levels)
DEBDOX: drug-related adverse events and liver toxicity are significantly reduced
Lammer J et al. Cardiovasc Intervent Radiol 2010;33:41-52
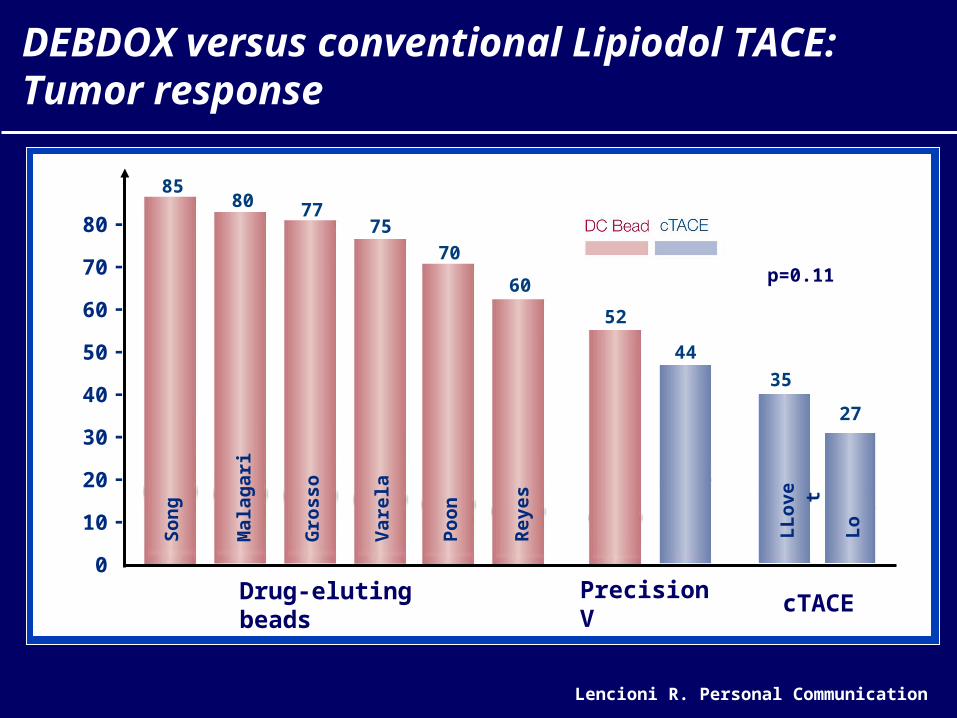
Lencioni R. Personal Communication
80
70
60
50
40
30
20
10
0
-
-
-
-
-
-
-
-
44
52
80
Mal
agar
i
77
Gro
sso
75
Var
ela
70
Po
on
60
Rey
es
85S
on
g
Drug-eluting beads
35
27
LL
ove
t
Lo
cTACE
p=0.11
Precision V
DEBDOX versus conventional Lipiodol TACE: Tumor response
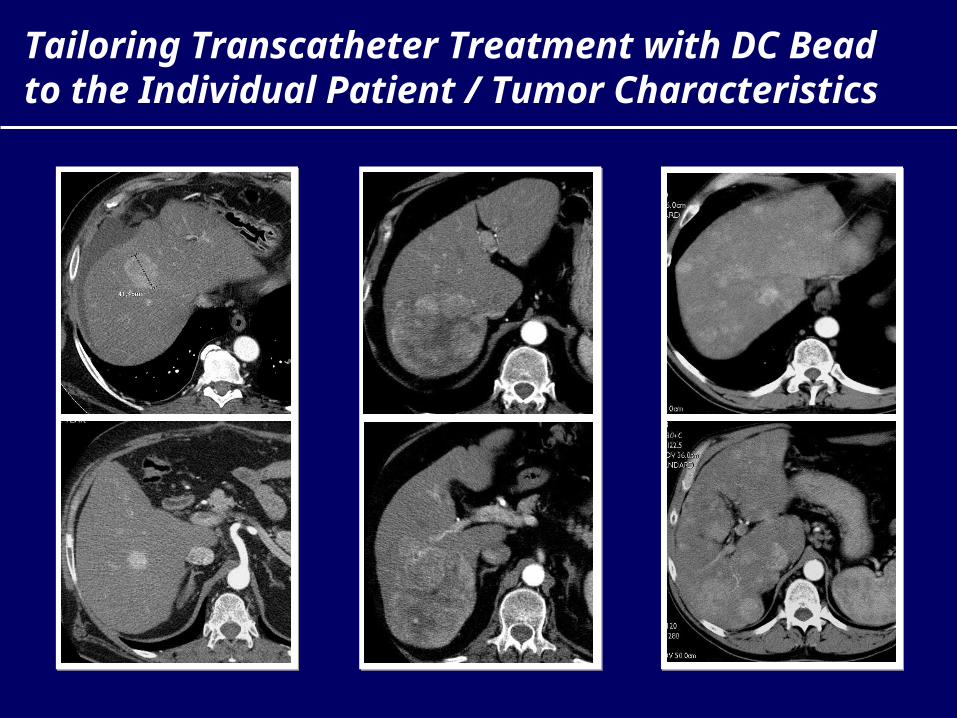
Tailoring Transcatheter Treatment with DC Bead to the Individual Patient / Tumor Characteristics

DC Bead in HCC: Development of Procedural Standards and Technical Recommendations
• The panel: Thierry De Baere / Institut Gustav-Roussy, Paris, France James G. Caridi / University of Florida, USA Jean-Francois H. Geschwind / Johns Hopkins University, USA Riccardo Lencioni / University of Pisa, Italy Katerina Malagari / University of Athens, Greece Robert C. Martin / University of Louisville, USA Elizabeth O’Grady / University Hospital Aintree, UK Thomas J. Vogl / Universty of Frankfurt, Germany
• Consensus Meeting during the ECIO 2010 in Florence
• Independent reviewers: Martha Burrel and Maria Isabel Real, Liver Unit, Barcelona, Spain Johannes Lammer, University of Vienna, Austria Anthony Watkinson, Royan Devon and Exeter University Hospital, UK

Pre-Treatment Imaging
Obtaining a triple-phase CT or MRI of the liver is mandatory to integrate clinical and laboratory data to evaluate the indication to transcatheter treatment of HCC with DC Bead in each individual patient by the local multidisciplinary liver tumor board.
Additional imaging examinations to rule out extrahepatic disease should be performed as appropriate.
DC Bead in HCC: Development of Procedural Standards and Technical Recommendations

Peri-Procedure Medication
Pain medication should be given according to standard hospital protocol.
Antibiotic prophylaxis and gastric protection should be administered at the physician's discretion.
DC Bead in HCC: Development of Procedural Standards and Technical Recommendations
Loading Dose of Doxorubicin
Each vial of DC Bead (2 ml of beads) should be loaded with 50-75 mg doxorubicin (loading dose, 25-37.5 mg doxorubicin / ml of beads).
DC Bead in HCC: Development of Procedural Standards and Technical Recommendations

DC Bead in HCC: Development of Procedural Standards and Technical Recommendations
Planned Dose:
Single / Small HCC
Each treatment:
- 1 vial
- up to 75 mg doxo
Planned Dose:
Large / Multiple HCC
Each treatment:
- 2 vials
- up to 150 mg doxo

Bilobar Tumors
In bilobar tumors, both hepatic lobes should be treated in separate treatment sessions 2-4 weeks apart, in the absence of complications requiring a longer time interval between the two sessions.
Obtaining confirmation that the liver enzymes have returned to baseline before performing the second treatment session is recommended.
DC Bead in HCC: Development of Procedural Standards and Technical Recommendations

Very Large Tumors
In very large tumors, even if unilobar, the same approach including two sessions should be followed.
Indication to treatment with DC Bead in patients with tumor replacing more than 50% of the liver should be carefully evaluated: adequate interventional and clinical expertise is required to manage patients with such advanced disease.
DC Bead in HCC: Development of Procedural Standards and Technical Recommendations
Choice of DC Bead Size
Use of 100-300μm beads is recommended for a standard procedure.
However, individual patient and tumor characteristics, particularly the identification of arterio-venous shunting, should be taken into account when the safety of the treatment and the choice of DC Bead size are determined.
DC Bead in HCC: Development of Procedural Standards and Technical Recommendations

Choice of DC Bead Size
In the case of significant arterio-portal or hepatic venous shunting, embolization of the shunt with gelfoam pledgets is recommended before proceeding with DC Bead treatment.
Confirmation that the shunt is no longer present must be obtained before the DC Bead can be safely administered.
DC Bead in HCC: Development of Procedural Standards and Technical Recommendations

DC Bead Dilution
Mix loaded DC Bead with a non-ionic contrast medium.
At least 5-10 ml of non-ionic contrast should be used per 1 ml of DC Bead (i.e., 10-20 ml are required to dilute one vial of DC Bead) prior to injection).
DC Bead in HCC: Development of Procedural Standards and Technical Recommendations

Catheter Positioning
A superselective (i.e., segmental or subsegmental) approach should be used whenever possible by using a microcatheter.
Use of C-arm rotational angiography with a flat-panel detector system (cone-beam CT) is recommended, if available, to improve the accuracy in identifying tumor-feeding arteries and to confirm adequate targeting and saturation of the tumor(s).
DC Bead in HCC: Development of Procedural Standards and Technical Recommendations

DC Bead in HCC: Development of Procedural Standards and Technical Recommendations
Segmental / Subsegmental approach
Place the microcatheter into the segmental or subsegmental vessel feeding the tumor as distally as possible but avoiding wedging the catheter to avoid reflux along the catheter shaft. Flow within the artery must be preserved.
Lobar approach
Place the catheter as selectively as possible in the right or left hepatic artery. Pay attention to identifying the origin of the cystic artery as well as other arteries supplying flow to extra-hepatic organs. If identified, these vessels must be either embolized using coils or avoided by placing the catheter tip well beyond the origin of these vessels.

Injection of the DC Bead
The injection must be very slow: an injection rate of 1 ml of the contrast agent - DC Bead suspension per minute is recommended.
Care should be taken to avoid sedimentation of the beads in the syringe by rotating the syringes or using a 3-way stopcock to gently suspend the beads in the solution.
DC Bead in HCC: Development of Procedural Standards and Technical Recommendations

Embolization Endpoint
Injection should be continued until “near stasis” is observed in the artery directly feeding the tumor (i.e., the contrast the contrast column should clear within 2-5 heart beats). At that point, injection should be stopped – regardless of the amount of beads that have been actually administered – to avoid reflux of embolic material.
DC Bead in HCC: Development of Procedural Standards and Technical Recommendations

Embolization Endpoint
Once the embolisation endpoint has been achieved, no additional embolic material should be injected.
If the “near stasis” endpoint is not obtained after injection of the scheduled volume of beads, no additional embolization should be performed. This patient is likely to benefit from a second course after imaging follow-up.
DC Bead in HCC: Development of Procedural Standards and Technical Recommendations

Post-Treatment Management
Obtaining a triple-phase CT or MRI of the liver 2-4 weeks after the procedure is recommended to assess the outcome of the first treatment and to plan further action.
Treatment response should be assessed according to modified RECIST (mRECIST) for HCC. *
* Lencioni R, Llovet JM, Semin Liver Dis 2010;30:52-60
DC Bead in HCC: Development of Procedural Standards and Technical Recommendations

Post-Treatment Management
Residual viable tumor (partial response, stable disease, progression): further treatment with DC Bead can be scheduled after 4-8 weeks in the absence of contraindications.
Complete response: imaging follow-up should be scheduled every 2-3 months.
DC Bead in HCC: Development of Procedural Standards and Technical Recommendations

Treatment Discontinuation
Treatment with DC Bead should be discontinued in patients presenting with untreatable progression. *
* Lencioni R et al. ASCO 2010
DC Bead in HCC: Development of Procedural Standards and Technical Recommendations

Untreatable Progression (1)
Failure to achieve objective response in the targeted tumor after at least two DC Bead treatments. The emergence of new intrahepatic tumor foci remote from the treated territory, although clearly represents tumor progression according to modified RECIST for HCC, does not contraindicate further treatment with DC Bead.
DC Bead in HCC: Development of Procedural Standards and Technical Recommendations

Untreatable Progression (2)
Clinical or functional deterioration. Treatment should be discontinued in patients showing clinical progression to ECOG performance status > 2 or evolution to sustained hepatic decompensation (not merely after therapy).
DC Bead in HCC: Development of Procedural Standards and Technical Recommendations

General Statement
The Interventional Radiologists is the only qualified physician to decide how to approach the unique combination of patients and tumor characteristics that he is facing at the time of the procedure.
DC Bead in HCC: Development of Procedural Standards and Technical Recommendations