bone health...bone metastases •breast cancer has highest incidence of skeletal-related events...
TRANSCRIPT

Bone Health
Michael Collins, BSc Phm, ACPR, PharmD
Clinical Pharmacist – Oncology
Grand River Hospital / Grand River Regional Cancer Centre
CAPhO Fundamentals Day
September 22nd, 2018

Disclosures
• No conflicts of interest

Learning objectives
1. Understand the incidence, epidemiology, pathophysiology and clinical consequences of cancer-induced and cancer-treatment related bone disease;
2. Describe the general management and prevention of metastatic bone disease;
3. Understand the mechanism of action, efficacy and safety of common bone-targeting agents used in cancer patients; and
4. Explain the role of bone-targeted treatment options in the prevention of bone metastasis.

Bone metastases
• Bone metastases is cancer that spread to the bone from another site• Different from primary bone cancer
• Also called “secondary bone cancer” or “metastatic bone disease”
• More common in certain types of cancer• Breast (73%*)
• Prostate (68%*)
• Lung (36%*)
• Kidney (35%*)
• Multiple myeloma (MM) – nearly all patients have bone involvement
*Based on postmortum analysis in Galasko C. The anatomy and pathways of skeletal metastases. In: Weiss L, Gilbert A, editors. Bone metastases. Boston: GK Hall; 1981. p. 49–63.

Bone Metastases
• Breast cancer has highest incidence of skeletal-related events (SREs)• Medial survival with bone metastases was 16 months
• + SRE was only 7 months
• Lung cancer with bone metastases• Median survival was 6-12 months
R. Coleman, et al. Bone health in cancer patients: ESMO Clinical Practice Guidelines, Annals of Oncology, Volume 25, Issue suppl_3, 1 September 2014, Pages iii124–iii137

Bone metastases
• Cancer can metastasize to any bone• Vertebrae, ribs, pelvis, sternum and
skull are most common sites
• May be one or several sites
Image source: https://www.slideshare.net/doctorbobm/bone-metastases
Robert E. Coleman. Clinical Features of Metastatic Bone Disease and Risk of Skeletal Morbidity. Clin Cancer Res October 15 2006 (12) (20) 6243s-6249s

Pathophysiology of bone metastases
• Metastatic cancer can upset the natural process of bone formation and break down• Osteoblastic metastases
• Increase in bone cell formation
• Bone becomes dense and sclerotic
• E.g. prostate cancer
• Osteolytic metastases (more common)• Increase in bone break down
• Weak/brittle bones
• E.g. breast cancer, MM
Molecular Biology of Bone Metastasis - Scientific Figure on ResearchGate. Available from: https://www.researchgate.net/The-vicious-cycle-of-bone-metastases-Factors-such-as-MMPs-chemokine-receptor-4-CXCR4_fig1_5907707 [accessed 18 Aug, 2018]

Clinical consequences of bone metastases
• Skeletal-related events (SREs)• Fractures
• Spinal cord compression
• Surgery to the bone
• Radiation to the bone
• Hypercalcemia
R. Coleman, et al. Bone health in cancer patients: ESMO Clinical Practice Guidelines, Annals of Oncology, Volume 25, Issue suppl_3, 1 September 2014, Pages iii124–iii137
Image source: Agarwal MG, Nayak P. Management of skeletal metastases: An orthopaedic surgeon's guide. Indian J Orthop 2015;49:83-100

Clinical consequences of bone metastases
• Pain• Bone metastases are most common cause of cancer-related pain
• May come and go or constant• Often worse at night
• 3/4 of myeloma patients present with bone pain
• 2/3 of breast cancer osteolytic bone metastases are painless
R. Coleman, et al. Bone health in cancer patients: ESMO Clinical Practice Guidelines, Annals of Oncology, Volume 25, Issue suppl_3, 1 September 2014, Pages iii124–iii137

Cancer treatment-induced fractures
• Chemotherapy
• Aromatase inhibitors
• Luteinizing hormone releasing hormone (gonadotropin releasing hormone)
• Androgen-deprivation therapy
• Corticosteroids
Julie R. Gralow, et al. NCCN Task Force Report: Bone Health in Cancer Care. J Natl Compr Canc Netw 2013;11:S-1-S-50.

Julie R. Gralow, et al. NCCN Task Force Report: Bone Health in Cancer Care. J Natl Compr Canc Netw 2013;11:S-1-S-50.

Case #1
• Miss BC is a 46 year-old premenopausal female with hormone-receptor positive, HER-2 negative breast cancer. She was treated adjuvantly with surgery and dose-dense AC-T (doxorubicin/cyclophosphamide + paclitaxel) chemotherapy.
• Following chemotherapy, she elected to start ovarian suppression with goserelinin combination with tamoxifen.
• After consultation with a gynecologist, she decided to pursue total hysterectomy and oophorectomy. Two weeks later she started letrozole.
• Which of the following therapies is the least likely to increase her risk of treatment-related fractures?
a) Chemotherapy (doxorubicin/cyclophosphamide + paclitaxel)b) Letrozolec) Goserelind) Tamoxifene) I’m not sure

Treatment of Bone Metastases
• Radiation
• Surgery
• Bone-targeting agents
• Hormone therapy
• Pain management
• Life style modification / non-pharmacologic• No smoking, reduced alcohol, calcium, vitamin D, etc.

Bone-modifying agents

Bone-modifying agents in cancer patients
1) Prevention of skeletal-related events• Zoledronic acid, pamidronate, clodronate, ibandronate, denosumab
2) Prevention of treatment-induced bone-loss• Zoledronic acid, pamidronate, ibandronate, alendronate, risedronate,
denosumab
3) Prevention of metastases• Breast – zoledronic acid, clodronate
• Prostate – denosumab
4) Tumour-induced hypercalcemia (not the focus of this talk)• Zoledronic acid, pamidronate, denosumab, etc.
R. Coleman, et al. Bone health in cancer patients: ESMO Clinical Practice Guidelines, Annals of Oncology, Volume 25, Issue suppl_3, 1 September 2014, Pages iii124–iii137

Bisphosphonates
• Mimic pyrophosphate, an endogenous bone resorption inhibitor• Results in reduced osteoclast life span
• Cladronate (IV/PO)
• Ibandronate (IV/PO)
• Pamidronate (IV)
• Zoledronic acid (IV)
• Alendronate (PO)
• Risedronate (PO)
Risks and benefits of long-term bisphosphonate therapy - Scientific Figure on ResearchGate. Available from: https://www.researchgate.net/Proposed-mechanism-of-action-of-bisphosphonates-Reprinted-with-permission-from-Solomon_fig1_44643481 [accessed 19 Aug, 2018]

Bisphosphonates
• Adverse effects• Osteonecrosis of the jaw (ONJ)
• Higher risk in cancer patients vs osteoporosis
• Hypocalcemia• Usually asymptomatic
• Nephrotoxicity• Dose-related, rate of infusion
• Gastrointestinal upset (Orals)• Musculoskeletal pain
• Can be severe
• Acute phase reactions (fever, fatigue, myalgias)• Usually diminish with subsequent doses
• Atypical fractures (rare)
O’Connell M, Borchert JS. Osteoporosis and Osteomalacia. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey L. eds. Pharmacotherapy: A Pathophysiologic Approach, 10e New York, NY: McGraw-Hill; . http://accesspharmacy.mhmedical.com.proxy.lib.uwaterloo.ca/content.aspx?bookid=1861§ionid=146068952. Accessed August 19, 2018.

Osteonecrosis of the jaw
• Osteonecrosis of the jaw (ONJ) • Jaw bone becomes exposed
• Necrosis due to lack of blood supply
• Risk factors:• Steroids, radiation, anti-angiogenic drugs• Invasive dental surgery• Poorly fitting dentures• Smokers
• Onset: months to years• Dental clearance prior to starting
• Avoid invasive dental procedures during treatment
• Report any new jaw pain!• Osteonecrosis of other bones can occur
• Femur, hip, humerus, tibia, ribs, spine, knee etc
Zoledronic acid– Cancer Care Ontario Drug Monograph. https://www.cancercareontario.ca/en/drugformulary/drugs/monograph/43886. Accessed August 19, 2018.
Image source: Heng C, et al. Bisphosphonate-related osteonecrosis of the jaw in patients with osteoporosis. Am Fam Physician. 2012 Jun 15;85(12):1134-41.

Zoledronic acid
• Bone metastases• 4mg IV q3-12weeks
• Over (at least) 15 minutes
• 4mg ≈ $15
• Nephrotoxicity• Doses > 4mg• Infusion over < 15 minutes
• Bloodwork• Serum creatinine, Albumin, Calcium
Starting Dose
Creatinine Clearance (mL/min)
Tumour-inducedhypercalcemia (TIH)
Other cancer patients
> 60 4 mg 4 mg
50 - 60 4 mg 3.5 mg
40 - 49 4 mg 3.3 mg
30 - 39 Consider ↓ 3 mg
<30Or SCr > 265 µmol/L (> 400 µmol/L if TIH)
Do not treat
Adapted from: Zoledronic acid– Cancer Care Ontario Drug Monograph. https://www.cancercareontario.ca/en/drugformulary/drugs/monograph/43886. Accessed August 19, 2018.

Pamidronate
• Bone metastases• 90 mg IV q4weeks over 2 hours
• Or q3weeks to match chemo
• 90mg ≈ $10
• Multiple myeloma• 90 mg IV q4weeks over 4 hours
• Often q5weeks to match chemo
• Bloodwork• Serum creatinine, albumin, calcium
Baseline Renal Function
Level Action
CrCl > 90 mL/min No adjustment needed
CrCl 30-90 mL/min Use 4 hour infusion
CrCl < 30 mL/minorCreatinine> 440 µmol/L (TIH) or> 180 µmol/L (myeloma)
Only use for life-threatening hypercalcemia where the benefit exceeds risk
Note: patients with severe renal impairment (< 30mL/min) have 3xhigher pamidronate exposure than those with normal renal function.
Pamidronate – Cancer Care Ontario Drug Monograph. https://www.cancercareontario.ca/en/drugformulary/drugs/monograph/44011. Accessed August 19, 2018.

Denosumab• Inhibits RANKL binding to RANK
• Blocks activation, development and survival of osteoclasts
• Monoclonal antibody ($$$!)• Fully humanized
• Bone metastases / myeloma• 120mg subcut q28days
• No renal dose adjustment required• ↑life-threatening hypocalcemia
• Higher ONJ risk than bisphosphonates• 1% after 12 months, 4% after 2 years
• Ca, Alb, PO4, Mg, (SCr)
R. Baron, S. Ferrari, R.G. Russell. Denosumab and bisphosphonates: different mechanisms of action and effects. Bone, 48 (2011), pp. 677-692

Case #2
• Mr. LC is a 71 year-old with non-small cell lung cancer and bone metastases. Today he presents to the chemo suite with tumour-induced hypercalcemia (Corrected calcium = 3.15 mmol/L).
• If his creatine clearance is 44 ml/min, which of the following is the most appropriate dose of zoledronic acid?
a) 4mg
b) 3.3mg
c) 3mg
d) Use denosumab instead

Disease-specific evidenceMetastatic prostate, metastatic breast, multiple myeloma

Metastatic breast cancer
• All breast cancer patients with bone metastases should start bone-targeted therapy1
• Pamidronate – 1998 RCT, n = 3821
• Pamidronate 90mg IV q3-4weeks vs placebo x 2 years
• Pamidronate reduced SREs by > 1/3
• Time to first SRE was 13.9 months for pamidronate vs 7.0 for placebo
• No difference in survival
1) Hortobagyi GN, Theriault RL, Lipton A, et al. Long-term prevention of skeletal complications of metastatic breast cancer with pamidronate. Protocol 19 Aredia Breast Cancer Study Group, J Clin Oncol , 1998, vol. 16 (pg. 2038-2044)

Metastatic breast cancer
• Zoledronic acid 4mg vs pamidronate 90mg (2003)1
• 1648 breast cancer and myeloma patients
• Zoledronic acid was non-inferior to pamidronate
• Breast cancer subgroup analysis• Zoledronic acid reduced risk of SRE by additional 20% over pamidonate
• Zoledronic acid also more convenient• 15 minutes vs 2-4 hour infusions
• BUT zoledronic acid was still on patent ($$$) at this time• $400 vs $10 for pamidronate
1) Rosen LS, Gordon D, Kaminski M, et al. Long-term efficacy and safety of zoledronic acid compared with pamidronate disodium in the treatment of skeletal complications in patients with advanced multiple myeloma or breast carcinoma: a randomized, double-blind, multicenter, comparative trial, Cancer , 2003, vol. 98 (pg. 1735-1744)

Metastatic breast cancer
• Q4week vs q12week zoledronic acid• ZOOM trial (2013) – 425 women with bone metastases1
• OPTIMIZE-2 trial (2017) – 416 women with bone metastases2
• Switched to q12weeks after 9-15 months
• Q12weeks as effective as q4weeks• But more cost-effective AND convenient for patient/centre
1) Amadori D, Aglietta M, Alessi B, et al. Efficacy and safety of 12-weekly versus 4-weekly zoledronic acid for prolonged treatment of patients with bone metastases from breast cancer (ZOOM): a phase 3, open-label, randomised, non-inferiority trial. Lancet Oncol. 2013;14(7):663-670.2) Hortobagyi GN, Van Poznak C, Harker WG, et al. Continued Treatment Effect of Zoledronic Acid Dosing Every 12 vs 4 Weeks in Women With Breast Cancer Metastatic to BoneThe OPTIMIZE-2 Randomized Clinical Trial. JAMA Oncol. 2017;3(7):906–912.

Zoledronic acid q4weeks vs q12weeks
• 1822 patients - q4 vs q12weeks x 2 years (2017)1
• Breast (855), prostate (689), multiple myeloma (218)• At least 1 site of bone involvement
• No difference in # of patients with at least 1 SRE • Q4weeks (29.5%) vs q12weeks (28.6%)
• Similar rates for breast, prostate, myeloma
• No statistical difference in adverse events• 2% ONJ in q4weeks
• 1% ONJ in q12weeks
• 1.2% nephrotoxicity for q4weeks
• 0.5% nephrotoxicity for q12weeks
1) Himelstein AL, Foster JC, Khatcheressian JL, et al. Effect of Longer-Interval vs Standard Dosing of Zoledronic Acid on Skeletal Events in Patients With Bone Metastases A Randomized Clinical Trial. JAMA.2017;317(1):48–58.
Zoledronic acid - frequency
• Our approach• Extensive bone metastases and/or +++ symptoms
• Q4weeks…consider switch to q12weeks if stable
• Low burden of bone disease and asymptomatic• Consider q12weeks from the start

Metastatic breast cancer
• Denosumab 120 mg SC vs zoledronic acid 4mg IV q4weeks (2010)1
• 2046 breast cancer patients with bone metastases
• Denosumab superior to zoledronic acid in time to first SRE and number of SREs
• Convenience/cost• SC vs IV
• No renal dosing
• BUT 120 mg = $600!• Zoledronic acid goes generic in 2013
1) Stopeck AT, Lipton A, Body JJ, et al. Denosumab compared with zoledronic acid for the treatment of bone metastases in patients with advanced breast cancer: a randomized, double-blind study, J Clin Oncol , 2010, vol. 28 (pg. 5132-5139)

Metastatic prostate cancer
• All hormone-refractory prostate cancer patients with bone metastases should start zoledronic acid or denosumab1
• Zoledronic acid• 643 hormone-refractory prostate cancer (2004)2
• Zoledronic acid 4mg IV q3weeks vs placebo
• 122 patients completed 24 months• Zoledronic acid reduced risk of SREs by 36%
• Reduced bone pain
• Extended time to first SRE by 4 months
1) R. Coleman, et al. Bone health in cancer patients: ESMO Clinical Practice Guidelines, Annals of Oncology, Volume 25, Issue suppl_3, 1 September 2014, Pages iii124–iii1372) Saad F, Gleason DM, Murray R, et al. Zoledronic Acid Prostate Cancer Study Group. Long-term efficacy of zoledronic acid for the prevention of skeletal complications in patients with metastatic hormone-refractory prostate cancer, J Natl Cancer Inst , 2004, vol. 96 (pg. 879-882)

Metastatic prostate cancer
• Denosumab• 2011 multinational RCT (n=1904)
• Denosumab 120 mg SC q4weeks or zoledronic acid 4mg IV q4weeks
• Denosumab had shorter time to first SRE• 17.1 vs 20.7 months (p=0.008)
• Also less cumulative SREs
1) Fizazi K, Carducci M, Smith M, et al. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: a randomised, double-blind study, Lancet , 2011, vol. 377 (pg. 813-822)

Metastatic prostate cancer
Adverse Event Denosumab (945) Zoledronic acid (943) p-value
Any 916 (97%) 918 (97%) 1.00
Grade 3 or 4 628 (66%) 678 (72%) 0.01
Hypocalcemia 121 (13%) 55 (6%) <0.0001
ONJ 22 (2%) 12 (1%) 0.09
Adapted from: Fizazi K, Carducci M, Smith M, et al. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: a randomised, double-blind study, Lancet , 2011, vol. 377 (pg. 813-822)

Metastatic prostate cancer
• Other agents• Enzalutamide – androgen receptor inhibitor
• Improved overall survival, progression-free survival and time to first SRE1
• Abiraterone – androgen synthesis inhibitor• Improved overall survival and time to first SRE2
• Radium-223 – alpha particle-emitting agent (radiopharmaceutical)• Improved overall survival versus placebo3
• Reduced time to first SRE3
1) Scher HI et al. Increased survival with enzalutamide in prostate cancer after chemotherapy. N Engl J Med. 2012;367(13):1187–97.2) Logothetis CJ et al. Effect of abiraterone acetate and prednisone compared with placebo and prednisone on pain control and skeletal-related events in patients with
metastatic castration-resistant prostate cancer: exploratory analysis of data from the COU-AA-301 randomised trial. Lancet Oncol. 2012;13D12]:1210–7.3) Parker C et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N Engl J Med. 2013;369D3]:213–23.

Multiple Myeloma
• Pamidronate 90mg IV q4weeks vs placebo x 21 cycles (1998)1
• 392 MM patients with at least one lytic bone lesion
• Pamidronate: lower SREs, lower pains scores, improved quality of life
• And a survival advantage!• First evidence of bisphosphonate anti-myeloma effects
• Zoledronic acid 4mg IV q4weeks showed similar results in MM2
1) Berenson JR, Lichtenstein A, Porter L, et al. Long-term pamidronate treatment of advanced multiple myeloma patients reduces skeletal events. Myeloma Aredia Study Group. J Clin Oncol 1998;16:593–602.
2) Rosen LS, Gordon D, Kaminski M, et al. Long-term efficacy and safety of zoledronic acid compared with pamidronate disodium in the treatment of skeletal complications in patients with advanced multiple myeloma or breast carcinoma. Cancer 2003;98(8):1735–1744.
Multiple Myeloma
• Meta-analysis (2017) of 24 RCTs and 7293 patients1
• Bisphosphonates vs placebo or no treatment
• Moderate-qualify evidence to support overall survival benefit
• Moderate-qualify evidence for reduction in vertebral fractures and SREs
• Low-quality of evidence for reduction in pain
• No evidence for superiority of one bisphosphonate over another• (Except zoledronic acid over etidronate)
• 1/1000 will experience ONJ• No difference between bisphosphonates
1) Mhaskar R, Kumar A, Miladinovic B, Djulbegovic B. Bisphosphonates in multiple myeloma: an updated network meta‐analysis. Cochrane Database of Systematic Reviews 2017, Issue 12. Art. No.: CD003188.

Multiple Myeloma (MM)
• Denosumab vs zoledronic acid (2011)1
• 1776 patient with advanced cancer• MM = 180 (10%)
• Non-inferior for time to first SRE• 20.6 vs 16.3 months
• Overall survival (OS) and progression-free survival were similar
• BUT….• Post-hoc analysis showed OS benefit for
zoledronic acid (HR = 2.26)2
• Limits use of denosumab in MM
1) Henry DH, Costa L, Goldwasser F, et al. Randomized, Double-Blind Study of Denosumab versus Zoledronic Acid in the Treatment of Bone Metastases in Patients with Advanced Cancer (Excluding Breast and Prostate Cancer) or Multiple Myeloma. J Clin Oncol 2011;29:1125–1132.
2) N Raje, S Vadhan-Raj, W Willenbacher, et al. Evaluating results from the multiple myeloma patient subset treated with denosumab or zoledronic acid in a randomized phase 3 trial. Blood Cancer J, 6 (2016), p. e378

Multiple Myeloma (MM)• Denosumab vs zoledronic acid (March 2018)1
• Randomized, double-blind, double-dummy, active-controlled, phase III study in 259 centres and 29 countries (n = 1718)
• 1718 newly diagnosed MM patients with at least one lytic bone lesion
• Denosumab was non-inferior to zoledronic acid in prevention of SREs
• No difference in overall survival!
1) N Raje, E Terpos, W Willenbacher, et al.Denosumab versus zoledronic acid in bone disease treatment of newly diagnosed multiple myeloma: an international, double-blind, double-dummy, randomised, controlled, phase 3 study. Lancet Oncol (2018) Epub 2018 Feb 9.
Adverse effect Denosumab Zoledronic acid
Nephrotoxicity 85 (10%) 146 (17%)
Hypocalcemia 144 (17%) 106 (12%)
ONJ 35 (4%) 24 (3%)
Cost $600/dose $10/dose

Multiple myeloma - clinical controversies
• Length of therapy?• Most trials evaluated 2 years of therapy
• Most MM patients survive longer than this!
• Bone-targeted agents have a real risk of ONJ
• Switch to q3months after 2 years?
• Safety• Some clinicians prefer pamidronate over zoledronic acid
• Observational evidence for increased ONJ, renal toxicity
• No head-to-head evidence
• Denosumab: less renal toxicity…but more ONJ, hypocalcemia?• Evidence is not clear

Prevention of metastasesBreast and prostate
Breast – prevention of bone metastases
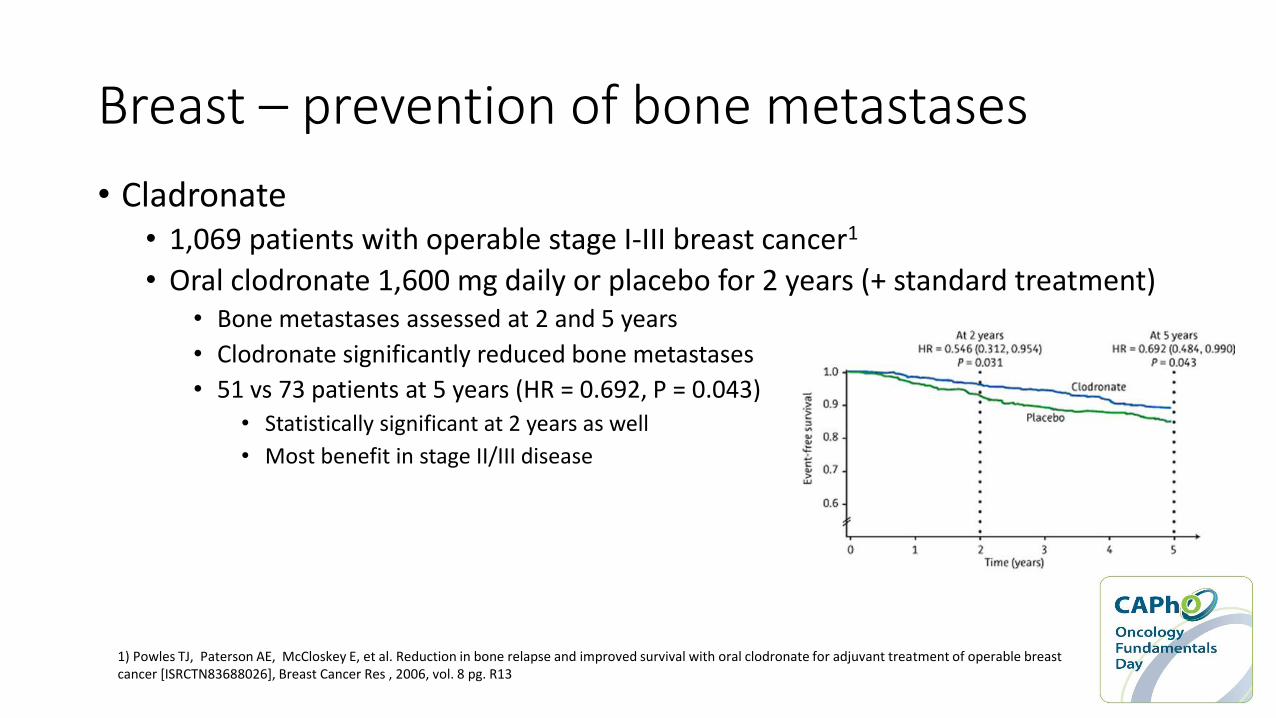
• Cladronate• 1,069 patients with operable stage I-III breast cancer1
• Oral clodronate 1,600 mg daily or placebo for 2 years (+ standard treatment)• Bone metastases assessed at 2 and 5 years
• Clodronate significantly reduced bone metastases
• 51 vs 73 patients at 5 years (HR = 0.692, P = 0.043)• Statistically significant at 2 years as well
• Most benefit in stage II/III disease
1) Powles TJ, Paterson AE, McCloskey E, et al. Reduction in bone relapse and improved survival with oral clodronate for adjuvant treatment of operable breast cancer [ISRCTN83688026], Breast Cancer Res , 2006, vol. 8 pg. R13

Breast – prevention of bone metastases
• Zoledronic acid• AZURE trial - Open-label phase 3 RCT (2011; n = 3360)1
• Standard therapy ± zoledronic acid q3-4weeks x 6 doses, then q3-6months x 5 years
• No significant difference in disease-free survival (DFS) at 59 months
• AZURE trial at 84 months2
• Again, DFS, OS and distant recurrences did not differ with addition of zoledronic acid• Not affected by estrogen-receptor status
• Zoledronic acid did improve invasive DFS in women >5 years since menopause• 71% vs 78% (HR = 0.75, CI 0.59-0.96, p = 0.02).
• 26 (1.7%) confirmed cases of ONJ in zoledronic acid group
1) Coleman RE, Marshall H, Cameron D, et al. Breast cancer adjuvant therapy with zoledronic acid, N Engl J Med , 2011, vol. 365 (pg. 1396-1405)

Breast – prevention of bone metastases
• Meta-analysis of adjuvant bisphosphonates in early breast cancer (2015)1
• Data from 18,766 women (18,206 [97%] in trials of 2-5 years of bisphosphonate)
• Premenopausal women: no effect on any outcome
• Postmenopausal women• Significant reductions in recurrence, distant recurrence, bone recurrence and breast-cancer mortality
• Conclusion: • “Adjuvant bisphosphonates reduce the rate of breast cancer recurrence in the bone and
improve breast cancer survival, but there is definite benefit only in women who were postmenopausal when treatment began.”
1) Early Breast Cancer Trialists' Collaborative GroupAdjuvant bisphosphonate treatment in early breast cancer: meta-analyses of individual patient data from randomised trials. Lancet (2015) Oct 3;386(10001):1353-1361.

Breast – prevention of bone metastases
• 1803 premenopausal women receiving goserelin ovarian suppression1
• With tamoxifen or anastrozole ± zoledronic acid 4mg IV q6months x 3 years
• Zoledronic acid increased DFS (Figure A)• HR = 0.68 (0.51-0.91); p=0.009
• Did not significantly reduce risk of death • 30 vs 43 deaths; HR 0.67 (0.41-1.07); p=0.09
1) Gnant M, Mlineritsch B, Stoeger H, et al. Adjuvant endocrine therapy plus zoledronic acid in premenopausal women with early-stage breast cancer: 62-month follow-up from the ABCSG-12 randomised trial, Lancet Oncol , 2011, vol. 12 (pg. 631-641)

Prostate – prevention of bone metastases
• Denosumab vs placebo (2012)1
• 1432 patients from 30 countries with non-metastatic hormone-resistant prostate cancer at high risk of bone metastases• Denosumab significantly increased bone-metastasis-free survival by 4.2 months
• Denosumab significantly delayed time to first bone metastasis by 3.7 months
• No difference in overall survival
• ONJ: 5% for denosumab vs 0% for placebo
• Clinical significance?
• Does delaying bone metastases reduce SREs?
1) Smith MR, Saad F, Coleman R, et al. Denosumab and bone-metastasis-free survival in men with castration-resistant prostate cancer: results of a phase 3, randomised, placebo-controlled trial, Lancet , 2012, vol. 379 (pg. 39-46)

Prostate – prevention of bone metastases
• Zoledronic acid?• ZEUS trial (2014)1
• 1393 patients with high-risk non-metastatic prostate cancer• Zoledronic acid 4mg IV q3months x 4 years
• Ineffective in preventing bone metastases
• RADAR trial (2014)2
• 18 months of ADT + radiation ± zoledronic acid vs 6 months of ADT + radiotherapy ±zoledronic acid (4 treatment arms 1:1:1:1)• Did not meet primary endpoints (prostate cancer specific mortality)
• 18 months ADT + radiation + zoledronic acid was more effective if Gleason score 8-10• Secondary end-point, post hoc analysis
1) Wirth M, Tammela T, Cicalese V, Gomez Veiga F, Delaere K, Miller K, et al. Prevention of bone metastases in patients with high-risk nonmetastatic prostate cancer treated with zoledronic acid: efficacy and safety results of the Zometa European Study (ZEUS). Eur Urol. 2015;67:482–91.
2) Denham, James W et al. Short-term androgen suppression and radiotherapy versus intermediate-term androgen suppression and radiotherapy, with or without zoledronic acid, in men with locally advanced prostate cancer (TROG 03.04 RADAR): an open-label, randomised, phase 3 factorial trial. The Lancet Oncology , Volume 15 , Issue 10 , 1076 – 1089.

Prevention of treatment-induced bone lossBreast and prostate

R. Coleman, et al. Bone health in cancer patients: ESMO Clinical Practice Guidelines, Annals of Oncology, Volume 25, Issue suppl_3, 1 September 2014, Pages iii124–iii137

Prevention of treatment-induced bone loss
• Breast cancer on AI or ovarian suppression• Zoledronic acid 4 mg IV q6months
• Alendronate 70 mg po qweekly
• Risedronate 35 mg po qweekly
• Denosumab 60 mg SC q6months
• Prostate cancer on adrogen-deprivation therapy• Denosumab 60 mg SCq6months
• Pamidronate 60 mg IV q3months
R. Coleman, et al. Bone health in cancer patients: ESMO Clinical Practice Guidelines, Annals of Oncology, Volume 25, Issue suppl_3, 1 September 2014, Pages iii124–iii137

Case #3
• Mr. PC is a 67 year-old male with non-metastatic hormone-resistant prostate cancer and a high-risk of bone metastases (i.e. PSA ≥8.0 μg/L).
• Which agent has the best evidence for the prevention of bone metastases in his case?
a) Pamidronate
b) Zoledronic acid
c) Denosumab
d) Cladronate

Summary
1) Bone metastases have significant clinical consequences• Pain, fractures, spinal cord compression, hypercalcemia, surgery etc.
2) Some cancers have a particular affinity for bone• Breast, prostate and multiple myeloma
3) Several bisphosphonates and denosumab have shown good evidence to reduce skeletal-related events in metastatic bone disease
4) Some cancer therapies may induce bone loss and increase facture risk• Bisphosphonates and denosumab can prevent bone loss associated with the use of ovarian suppression
and AIs in early breast cancer and ADT in prostate cancer
5) Bisphosphonates can reduce the frequency of bone metastases and improve survival in postmenopausal women• Do not improve outcomes in premenopausal women
6) Denosumab can delay bone metastases in hormone-resistant prostate cancer

Selected references
1. Julie R. Gralow, J. Sybil Biermann, Azeez Farooki, Monica N. Fornier, Robert F. Gagel, Rashmi Kumar, Georgia Litsas, Rana McKay, Donald A. Podoloff, Sandy Srinivas, and Catherine H. Van Poznak. NCCN Task Force Report: Bone Health in Cancer Care. J Natl Compr Canc Netw2013;11:S-1-S-50.
2. R. Coleman, on behalf of the ESMO Guidelines Working Group, J. J. Body, on behalf of the ESMO Guidelines Working Group, M. Aapro, on behalf of the ESMO Guidelines Working Group, P. Hadji, on behalf of the ESMO Guidelines Working Group, J. Herrstedt, on behalf of the ESMO Guidelines Working Group; Bone health in cancer patients: ESMO Clinical Practice Guidelines, Annals of Oncology, Volume 25, Issue suppl_3, 1 September 2014, Pages iii124–iii137.
3. Robert E. Coleman. Clinical Features of Metastatic Bone Disease and Risk of Skeletal Morbidity. Clin Cancer Res October 15 2006 (12) (20) 6243s-6249s
4. O’Connell M, Borchert JS. Osteoporosis and Osteomalacia. In: DiPiro JT, Talbert RL, Yee GC, Matzke GR, Wells BG, Posey L. eds. Pharmacotherapy: A Pathophysiologic Approach, 10e New York, NY: McGraw-Hill; http://accesspharmacy.mhmedical.com.proxy.lib.uwaterloo.ca/content.aspx?bookid=1861§ionid=146068952. Accessed August 19, 2018.
5. R. Baron, S. Ferrari, R.G. Russell. Denosumab and bisphosphonates: different mechanisms of action and effects. Bone, 48 (2011), pp. 677-692