brazilian issn 0103-5355...
TRANSCRIPT

BrazilianNeurosurgery Arquivos Brasileiros de Neurocirurgia
EditorEberval Gadelha Figueiredo
ISSN 0103-5355
Number 3 • Volume 36 • Pages 143–202 • September 2017

Brazilian Neurosurgery Arquivos Brasileiros de Neurocirurgia
ISSN 0103-5355
Editor-in-Chief | Editor-Chefe
Eberval Gadelha Figueiredo
Emeritus Editors | Editores Eméritos
Milton ShibataGilberto Machado de Almeida†
Editorial Board | Conselho EditorialChairman | Presidente
José Marcus RottaManoel Jacobsen Teixeira
National Board | Conselho Nacional
Albedi BastosBelém, PA
Arnaldo ArrudaFortaleza, CE
Benedicto Oscar ColliRibeirão Preto, SP
Carlos TellesRio de Janeiro, RJ
Carlos Umberto PereiraAracaju, SE
Eduardo VellutiniSão Paulo, SP
Ernesto CarvalhoPorto, Portugal
Evandro de OliveiraSão Paulo, SP
Fernando Menezes BragaSão Paulo, SP
Francisco Carlos de AndradeSorocaba, SP
Hélio Rubens MachadoRibeirão Preto, SP
Hildo AzevedoRecife, PE
João Cândido AraújoCuritiba, PR
João Paulo FariasLisboa, Portugal
Jorge Luiz KraemerPorto Alegre, RS
José Alberto Gonçalves†
João Pessoa, PBJosé Alberto Landeiro
Rio de Janeiro, RJJosé Carlos Esteves Veiga
São Paulo, SPJosé Carlos Lynch Araújo
Rio de Janeiro, RJJosé Marcus Rotta
São Paulo, SPJosé Perez Rial
São Paulo, SPJose Weber V. de Faria
Uberlândia, MGLuis Alencar Biurrum Borba
Curitiba, PRManoel Jacobsen Teixeira
São Paulo, SPMarco Antonio Zanini
Botucatu, SPMarcos Barbosa
Coimbra, PortugalMarcos Masini
Brasília, DFMário Gilberto Siqueira
São Paulo, SPNelson Pires Ferreira
Porto Alegre, RSÓscar Luis Alves
Porto, PortugalPedro Garcia Lopes
Londrina, PRRicardo Vieira Botelho
São Paulo, SPRoberto Gabarra
Botucatu, SPSebastião Gusmão
Belo Horizonte, MGSérgio Cavalheiro
São Paulo, SPSergio Pinheiro Ottoni
Vitória, ESWaldemar Marques
Lisboa, Portugal
International Board | Conselho Internacional
Albert Sufi anovRussia
André G. MachadoUSA
Antonio de SallesUSA
Beatriz LopesUSA
Clement HamaniUSA
Daniel PrevedelloUSA
Felipe AlbuquerqueUSA
Jorge MuraChile
Kumar KakarlaUSA
Michael LawtonUSA
Nobuo HashimotoJapan
Oliver BozinovSwitzerland
Pablo RubinoArgentina
Paolo CappabiancaItaly
Peter BlackUSA
Peter NakajiUSA
Ricardo HanelUSA
Robert F. SpetzlerUSA
Rungsak SiwanuwatnThailand
Volker SonntagUSA
Yasunori FujimotoJapan

Brazilian Neurosurgery Arquivos Brasileiros de Neurocirurgia
ISSN 0103-5355
S ociety Board | Diretoria (2017–2018)
Chairman | PresidenteRonald de Lucena Farias
Vice-Chairman | Vice-PresidenteValdir Delmiro Neves
General Secretary | Secretário-GeralItalo Capraro Suriano
Treasurer | TesoureiraMarise Augusto Fernandes Audi
First Secretary | Primeiro SecretárioMarco Antonio Herculano
Former Chairman | Presidente AnteriorModesto Cerioni Junior
Next Chairman 2019–2020 | Presidente Eleito 2019–2020Luis Alencar Biurrum Borba
Congress Chairman 2018 | Presidente do Congresso 2018Marcelo Paglioli Ferreira
Congress Chairman 2020 | Presidente do Congresso 2020Stenio Abrantes Sarmento
Equity and Controllership | Patrimônio e ControladoriaFrancisco de Assis Ulisses Sampaio Júnior
Educational & Scientifi c | Educacional e Científi co
Neurosurgery Formation | Formação NeurocirúrgicaSérgio Cavalheiro
Continued Education | Educação ContinuadaAlexandre Novicki Francisco
Guidelines and New Technologies | Diretrizes e Novas TecnologiasRicardo Vieira Botelho
Research | PesquisaEberval Gadelha Figueiredo
Public Relationship & Communication | Comunicação e Relacionamento Social
Communication & Marketing | Comunicação e MarketingFernando Campos Gomes Pinto
Social Responsibility | Responsabilidade SocialCarlos Roberto Sampaio de Assis Drummond
Ombudsman | OuvidoriaJair Leopoldo Raso
Professional Protection of Associated Activities | Defesa Profi ssional de Atividades Associativas
Professional Protection | Defesa Profi ssionalAlbert Vincent Berthier Brasil
National Integration | Integração Nacional Mauro Takao Marques Suzuki
Departments | Departamentos Ruy Castro Monteiro da Silva Filho
Technical - SUS | Câmara Técnica - SUSBruno Silva Costa
Statute | Codifi cação Wuilker Knoner Campos
Institutional Relations | Relações Institucionais Aluízio Augusto Arantes Junior
International Relations | Relações InternacionaisJosé Marcus Rotta
Policies | PolíticasModesto Cerioni Junior
Parliament | ParlamentoSandoval Inácio Carneiro
Think First Project | Projeto Pense BemFrancisco Ricardo Borges Ribeiro
Advisory Board | Conselho Deliberativo
Chairman | PresidenteLuiz Carlos de Alencastro
Secretary | SecretárioMarcos Masini
Directors | ConselheirosAluízio Augusto Arantes JuniorBenjamim Pessoa ValeGeraldo de Sá Carneiro FilhoJair Leopoldo RasoJânio NogueiraJorge Luiz KraemerJosé Carlos SalemeJosé Fernando Guedes CorreaJosé Marcus RottaLuis Renato Garcez de Oliveira MelloOrival AlvesOsmar José Santos de MoraesRicardo Vieira Botelho

Brazilian Neurosurgery Arquivos Brasileiros de Neurocirurgia
Volume 36, Number 3/2017
online www.thieme-connect.com/products
Editorial143 Editorial - Patient with Recurrent Glioblastoma Responding Favorably to Ketogenic Diet
Combined with Intranasal Delivery of Perillyl Alcohol Editorial - Paciente com glioblastoma recorrente respondendo positivamente a dieta cetogênica
combinada a álcool perílico intranasalHelder Picarelli, MD, PhD
Original Article | Artigo Original145 Surgical Strategy for Dermoid and Epidermoid Tumors of the Posterior Fossa - Experience
with 21 Patients Melhor estratégia cirúrgica para tumores dermoides e epidermoides da fossa posterior - experiência
em 21 pacientesJosé Carlos Lynch, Leonardo C. Welling, Antonio Aversa, Celestino Esteves, Jânio Nogueira, Mariângela Gonçalves, Hélio Lopes
Review Articles | Artigos de Revisão
153 The Natural History of Brain Arteriovenous Malformations História natural das malformações arteriovenosas encefálicas
Carlos Michel Albuquerque Peres, Vitor Nagai Yamaki, Eberval Gadelha Figueiredo
160 Endoscopic and Microsurgical Approaches to the Cavernous Sinus – Anatomical Review Abordagem endoscópica e microcirúrgica do seio cavernoso – revisão da anatomia
Flavio Ramalho Romero, Daphyne Ramires, Luigi Carrara Cristiano, Marcos Paulo Silva, Rodolfo Brum Vieira
167 Paraspinal Lumbar Spine Approach -Wiltse Access Abordagem paravertebral da coluna lombar - acesso de Wiltse
Nícollas Nunes Rabelo, Bruno Nascimento Bettencourt da Silva, Luciano José Silveira Filho, George Santos dos Passos, Vitor Hugo Honorato Pereira, Luiz Antônio Araujo Dias Junior, Luiz Antônio Araujo Dias, Koji Tanaka
172 Intraoperative Neurophysiological Monitoring for Spinal Fusion Monitorização neurofi siológica intraoperatória para fusão espinhal
Marco de Agassiz Almeida Vasques, Eliana de Barros Marques Fonseca
178 Trochlear Nerve Schwannoma: Case Report and Literature Review Schwannoma do nervo troclear: revisão da literatura e relato de caso
Marcelo Lemos Viera da Cunha, Mario Henrique Furlanetto Miranda, Giulia Luiza Cecconello
Case Reports | Relatos de Caso185 Neurosarcoidosis Associated with Psychiatric Symptoms: Case Report Neurossarcoidose associada com sintomas psiquiátricos: relato de caso
Maick Wilen Fernandes Neves, Paulo Henrique Pires de Aguiar, Telmo Augusto Barba Belsuzarri, Wolnei Marques Zeviani, João Flavio de Araújo Mattos, Juliano Nery Navarro, Renata de Melo Braga Marques, Letícia Marissol de Souza Francisco
Thieme Revinter Publicações Ltda

190 Anconeus Epitrochlearis Muscle as a Cause of Ulnar Nerve Compression at the Elbow Músculo anconeu epitroclear como causa de compressão do nervo ulnar no cotovelo
Luiz Fernando Cannoni, Luciano Haddad
194 Patient with Recurrent Glioblastoma Responding Favorably to Ketogenic Diet Combined with Intranasal Delivery of Perillyl Alcohol: A Case Report and Literature Review
Paciente com glioblastoma recorrente respondendo positivamente a dieta cetogênica combinada a álcool perílico intranasal: relato de caso e revisão da literaturaJuliana Guimarães Santos, Wanise Maria Souza Da Cruz, Axel H. Schönthal, Marcela D'alincourt Salazar, Cristina Asvolinsque Pantaleão Fontes, Thereza Quirico-Santos, Clovis Orlando da Fonseca
200 C1-C4 Dorsal Column Stimulation for Refractory Occipital Neuralgia Treatment. Case Report Estimulação da coluna dorsal emC1-C4 para tratamento de neuralgia occipital refratária. Relato de caso
José Augusto Malheiros, Sergio Augusto Vieira Cancado, Célia Maria de Oliveira, Wancler Albert Gomes dos Santos
Brazilian Neurosurgery | Arquivos Brasileiros de Neurocirurgia Volume 36, Number 3/2017
Some of the product names, patents, and registered designs referred to in this publication are in fact registered trade marks or proprietary names even though specifi c reference to this fact is not always made in the text. Therefore, the appearance of a name without designation as proprietary is not to be construed as a representation by the Publisher that it is in the public domain.
All rights, including the rights of publication, distribution, and sales, as well as the right to translation, are reserved. No part of this work covered by the copyrights hereon may be reproduced or copied in any form or by any means—graphic, electronic, or mechanical, including photocopying, recording, taping, or information and retrieval systems—without written permission of the Publisher.
Important Note: Medical knowledge is ever-changing. As new research and clinical experience broaden our knowledge, changes in treatment and drug therapy may be required. The authors and editors of the material here-in have consulted sources believed to be reliable in their efforts to provide information that is complete and in accord with the standards accepted at the time of publication. However, in view of the possibility of human er-ror by the authors, editors, or publisher of the work herein, or changes in
medical knowledge, neither the authors, editors, or publisher, nor any other party who has been involved in the preparation of this work, warrants that the information contained here in is in every respect accurate or complete, and they are not responsible for any errors or omissions or for the results obtained from use of such information. Because of rapid advances in the medical sciences, independent verification of diagnoses and drug dosages should be made. Readers are encouraged to confirm the information con-tained herein with other sources. For example, readers are advised to check the product information sheet included in the package of each drug they plan to administer to be certain that the information contained in this publi-cation is accurate and that changes have not been made in the recommended dose or in the contraindications for administration. This recommendation is of particular importance in connection with new or infrequently used drugs.
Although all advertising material is expected to conform to ethical (medical) standards, inclusion in this journal does not constitute a guar-antee or endorsement of the quality or value of such product or of claims made by its manufacturer.
Copyright © 2017 by Thieme Revinter Publicações Ltda, Rio de Janeiro, Brazil. Arquivos Brasileiros de Neurocirurgia is published four times a year in March, June, September, and December by Thieme-Revinter Publicações Ltda, Rua do Matoso, 170, Rio de Janeiro, 20270-135, Brazil.
Editorial comments should be sent to [email protected]. Articles may be submitted to this journal on an open-access basis. For further informa-tion, please send an e-mail to [email protected]. The content of this journal is available online at www.thieme-connect.com/products. Visit our Web site at www.thieme.com and the direct link to this journal at www.thieme.com/bns.
Arquivos Brasileiros de Neurocirurgia is an official publication of the Brazilian Neurosurgery Society (Sociedade Brasileira de Neurocirurgia) and the Portuguese Language Neurosurgery Societies. It is listed in LILACS and LILACS-Express (Latin-American and Caribbean Center on Health Sciencies Information), and Latindex (Regional Cooperative Online Information System for Scholarly Journals from Latin America, the Caribbean, Spain and Portugal). Thieme Medical Publishers is a member of the CrossRef initiative.
ISSN 0103-5355
The colored content of this issue is available online at www.thieme.com/bns.


Sem título-1 1 05/09/17 16:10

Editorial
Editorial - Patient with Recurrent Glioblastoma RespondingFavorably to Ketogenic Diet Combined with Intranasal Deliveryof Perillyl Alcohol
Editorial - Paciente com glioblastoma recorrente respondendopositivamente a dieta cetogênica combinada a álcool perílico intranasal
Helder Picarelli, MD, PhD1
1Division of Neurosurgery, Instituto do Câncer do Estado de São PauloOctavio Frias de Oliveira (Icesp), São Paulo, SP, Brazil
Arq Bras Neurocir 2017;36:143–144.
Glioblastoma (GBM) is by far themost frequent andmalignanttype of primary brain tumor in the adult population. Despiteconsiderable efforts and extensive researches, it still has one ofthe poorest prognoses in cancerdiseases. According to the new(2016)WorldHealthOrganization (WHO) classification, GBMsare categorized by their histologic findings and diagnosticbiomarkers as: a) isocitrate dehydrogenase (IDH) mutant; b)IDH wild type; and c) NOS GBM (IDH1/2 not tested or incon-clusive). Themajority of GBMs is IDHwild type (90%), and theyoccur preferentially in elderly people without a pre-existinglower-grade glioma precursor. Currently, it is believed that theknowledge of the genetic, epigenetic and chromosomal aber-rations on GBMs can predict the therapy response and theoutcomes. Normally, IDHmutantGBMhas IDH1/2, TP53, ATRXmutation, and they are glioma-CpG island methylator pheno-type (G-CIMP). On the other hand, IDH wild-type GBM hasTERT, PTEN, TP53, PIK3CA, PIK3R1, NF1, H3F3A mutation;EGFR, PDGRA,MET,CDK4, CDK6,MDM2,MDM4amplification;EGFRvIII deletion mutation, and they have MGMT promotermethylation. Regardless of the significant changes and refine-ment of the WHO classification, the treatments and outcomesare still dismal and disappointing, because the patients have ashort survival rate and severe disabilities. In order to changethis picture, novel treatment strategies are needed.
The extent of the resection is still considered one of themost important positive prognostic factors, but the advan-ces in surgery (such as neuronavigation, monitoring, brainmapping and dyes) appear to have nearly reached theirlimits in achieving the maximal safe resection. Similarly, therole and the way of performing radiotherapy already seemto be well established. Despite this, they are performed
focally (saving critical and functional areas), making italmost impossible to eradicate all cancerous cells, sinceGBMs are diffuse or multifocal. Eventually, the disease willprogress, leading to serious disabilities and low quality oflife, unless another effective therapy is performed simulta-neously. Although the current adjuvant chemotherapy isonly minimally effective in the treatment of GBMs, theaddition of temozolomide (an alkylating agent) prolongsthe progression-free survival time, especially in the MGMTpromoter methylation phenotype tumor. Another concernis that GBM is a very heterogeneous disease, and its cells canpromptly acquire new mutations and convert into a thera-py-resistant malignancy. In spite of that, many weak keypoints involved in the growth and apoptosis of cancerous-cells (immunomodulatory, metabolic or genetic pathways)could be attacked.
Even though the treatment for GBM recurrence has manyethical and financial implications, the rescue surgery andbevacizumab (humanized monoclonal antibody targetingVEGF) administration seem to be reasonable for patientswith good functional status. Recently, many pre-clinical stud-ies and phase II/III clinical trials have been conducted to assessnew options. Tumor-treating fields (TTFs) and re-irradiationhave been mentioned as promising approaches, but currentdata also indicates that an effective strategy needs to be acombinatorial and individual therapy according to the tumor’sgenetic signature. In fact, the target therapymustbe the future,and the main approaches in focus are: a) targeting immuno-suppressive checkpoints, such as ipilimumab and nivolumab;b)active immunotherapy, suchascancer vaccinesand immunestimulatory gene therapy; c) passive immunotherapies using
Address for correspondenceHelder Picarelli, MD, PhD, Divisãode Neurocirurgia, Instituto doCâncer do Estado de São PauloOctavio Frias de Oliveira (Icesp),São Paulo, SP, Brazil(e-mail: [email protected];[email protected]).
DOI https://doi.org/10.1055/s-0037-1606299.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Editorial 143

antibodies; and d) adoptive strategies, such as the ones usingchimeric antigen receptor (CAR) T cells.
In this issue, Brazilian Neurosurgery publishes a casereport of a recurrent GBM patient who was successfullytreated combining daily intranasal delivery of monoterpene
perillyl alcohol (a Ras/MAPK pathway inhibitor) and aketogenic diet. The therapeutic potential of this natural,apparently safe and low-cost target therapy for recurrenceshould not be neglected despite the need for furtherstudies.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Editorial144

Surgical Strategy for Dermoid and EpidermoidTumors of the Posterior Fossa - Experience with21 Patients
Melhor estratégia cirúrgica para tumores dermoides eepidermoides da fossa posterior - experiência em21 pacientes
José Carlos Lynch1 Leonardo C. Welling2 Antonio Aversa3 Celestino Esteves1 Jânio Nogueira3
Mariângela Gonçalves1 Hélio Lopes1
1Neurocirurgia, Hospital Federal Servidores do Estado do Rio deJaneiro, Rio de Janeiro, RJ, Brazil
2Neurocirurgia, Universidade Estadual de Ponta Grossa,Ponta Grossa, PR, Brazil
3Neurocirurgia, Instituto Nacional do Câncer/INCA, Rio de Janeiro,RJ, Brazil
Arq Bras Neurocir 2017;36:145–152.
Address for correspondence Leonardo C. Welling, MD, PhD,Universidade Estadual de Ponta Grossa, Ponta Grossa, Paraná, Brazil(e-mail: [email protected]).
Keywords
► dermoid tumor► epidermoid tumor► intracranial tumor► microsurgery► posterior fossa
Abstract Objective The aim of this paper is to describe our surgical strategy and technique andto identify the best management for posterior fossa dermoid and epidermoid tumors(PFDETs).Methods We retrospectively identified 21 consecutive patients (11 males and 10females), with a mean age of 33.2 years, a mean follow-up of 6.1 years, andpathologically confirmed PFDETs. Total 17 patients were submitted to the extendedretrosigmoid approach. This approach incorporates transverse sigmoid sinus exposureand a generous mastoidectomy.Results Gross total tumor removal was achieved in 16 (76.1%) cases, with no surgicalmortality and a recurrence rate of 9.5%.Conclusions The surgical strategies used in this group of patients enabled the totalremoval of most tumors without surgical mortality and with minimal morbidity andrecurrence rates. The extended retrosigmoid approach used is an alternative pathregarding cranial base approaches. This approach is quick, simple and safe, anddecreases the retraction of the cerebellum.
Resumo Objetivos O objetivo deste estudo é descrever a técnica operatória para a melhorabordagem dos tumores dermoides e epidermoides da fossa posterior.Métodos Foram analisados retrospectivamente 21 pacientes (11 masculinos e 10femininos), com idade média de 33,2 anos e acompanhamento de 6,1 anos, comdiagnóstico histopatológico de tumor dermoide ou epidermoide de fossa posterior.
receivedMay 19, 2017acceptedAugust 1, 2017published onlineAugust 23, 2017
DOI https://doi.org/10.1055/s-0037-1606292.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Original Article | Artigo Original 145

Introduction
Intracranial dermoid and epidermoid tumors (IDETs) arecongenital, slow-growing tumors that develop between the3rd and 5th weeks of gestation from ectodermal remnantsduring neural tube formation in embryogenesis. Epidermoidtumors are lined by a delicate capsule of stratified squamousepithelium,while dermoid tumors include, in addition to skin,many hair follicles, as well as sebaceous and sweat glands.1–3
These tumors are rare, comprising around 1% to 2% of allintracranial tumors.1–14 The cerebellopontine angle (CPA)constitutes the place of 7% to 9% of all tumors.5,7,9,10,15–21
Despite the development of microsurgery and cranial basetechniques, the surgical management of posterior fossadermoid and epidermoid tumors (PFDETs) continues to be aformidable technical challenge to neurosurgeons, becausethese tumors grow in close contact with neural and vascularstructures that cannot be sacrificed or retracted.A controversial debate has continued for several years, whichhas not been completely settled to date. Should the neuro-surgeon promote gross total removal (GTR) of the tumor,which can result in unwarranted cranial nerve (CN) deficitand/or arterial injury, or should GTR be avoided, and a safer,subtotal removal (STR) of the tumor be performed instead?Traditionally, CPA lesions are treated through a retrosigmoidapproach. While these operative corridors are sufficient inmost cases, they still only provide a limited angle of view.Compared with the classical retrosigmoid approach, the
extended retrosigmoid approach allows for greater visualiza-tion and operative space within the posterior fossa.22–25
The objectives of the current paper are to report on ouroperative strategy and surgical technique, and to identify thebest operative management for PFDETs.
Methods
Data CollectionThis study included 21 consecutive patients with PFDETs whounderwent surgerybetween January1986and January2014attheDepartmentofNeurosurgeryof three different institutionsin Rio de Janeiro, Brazil. The main authors (JCL and AA)performed the majority of the surgeries. The medical charts,pre- and postoperative imaging, and pathological reports ofthe patients were retrospectively reviewed to ascertain thediagnosis of PFDETs, thereby creating a database from whichinformation pertinent to the present study was collected. Theintraoperative videos and/or photos of 14 patients were ana-lyzed for nuances of the microsurgical technique. Informedconsent was waived due to the retrospective character of thestudy. Computed tomography (CT) and magnetic resonanceimaging (MRI) scans were reviewed with the RadiologyDepartment (►Figs. 1–3 [1A, 2A and 3]). Control postoperativeimaging studies were performed within the first 48–72 hoursafter surgery to document the extent of the resection andpostoperative changes (►Fig. 1E and 2D). The first clinic visitoccurred � 15 days after hospital discharge, with subsequent
Nesse grupo, 17 pacientes foram submetidos a abordagem retrossigmoide estendida.Esta abordagem inclui exposição do seio transverso e sigmoide, além de amplamastoidectomia.Resultados Remoção cirúrgica total foi alcançada em 16 (76,1%) casos sem morta-lidade e com recidiva em 9,5% dos casos.Conclusões As abordagens cirúrgicas utilizadas nesta série permitiram a ressecçãototal na maioria dos pacientes, sem mortalidade cirúrgica e com morbidade erecorrência mínima. A craniotomia retrossigmoide estendida utilizada é uma boaalternativa para abordagens da base do crânio. É uma abordagem simples, rápida,segura, e que minimiza a retração do cerebelo.
Palavras-chave
► tumor dermoide► tumor epidermoide► tumor intracraniano► microcirurgia► fossa posterior
Fig. 1 (A) Coronal T1-weighted MRI image revealing CPA hypointense lesion with brainstem compression and contralateral shift. (B) Operativeview showing a wide mastectomy and complete skeletonization of the SS. (C) The dura mater is opened with the base toward the midline, staysutures elevated the SS and father further increase the access to the CPA. (D) Microphotograph after the extended retrosigmoid approachdemonstrates that the tumor filled the CPA and engulfed most of the neurovascular structures. (E) Immediate postoperative CT: observe theextension of the mastectomy creating a flat corridor to the CPA (arrow).
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Surgical Strategy for Dermoid and Epidermoid Tumors of the Posterior Fossa Lynch et al.146

visitsat2and6months.After that, thepatientswerescheduledfor revision at one-year intervals. They were contacted forimaging studies and clinic visits, or interviewed by telephone.In thisseries, three recently introduced innovationswereused:neurophysiological monitoring, endoscopy, and neuronaviga-tion. The Glasgow Outcome Scale (GOS) defined the outcome.
Neurosurgical Approaches and MicrosurgeryTechnique for Lesions Situated in the cerebellopontineangleWe used a tailored surgical approach tomanage each case: a)CPA tumors were removed via a suboccipital retrosigmoid oran extended approach, depending on the size and extensionof the tumor; b) vermian and fourth-ventricular lesionswereoperated through a midline suboccipital craniotomy. Con-sidering that IDETs situated in the CPA are the most chal-lenging to remove, we describe in details our surgicaltechnique to manage 15 (71.4%) IDETs located in the CPA.
Patient PositioningUnder endotracheal general anesthesia, most patients wereplaced in a semi-sitting position, with the head flexedforward and secured in the Mayfield three-point fixationdevice (Integra LifeSciences Holding Corporation, Plains-boro, NJ, US). The semi-sitting position enables naturalcerebellar relaxation via gravity without the need for lum-
bar drainage. Some patients, however, were placed in dorsaldecubitus with contralateral head rotation and ipsilateralshoulder elevation (surgeon’s preference). An arterial lineand a central venous catheter were placed in all patients.The patients were secured with a large tape in the operatingtable to allow table rotation to the right or to the left, andelevation or tilt of the head. These simple maneuvers,associated with multiple microscope angulations, enhancethe exposure, expanding the operative field. The involvedregion was shaved, prepped, and draped in a sterile fashion.Routine antibiotics, dexamethasone, and mannitol wereused. The procedure was initiated with the utilization ofa 2.5x surgical loupe and co-axial lighting for soft tissueincision and bone work.
Skin Incision and Muscle DissectionA10-cmvertical linear incisionwasmade 2–3 cmmedially tothe mastoid and centered � 2 cm above the mastoid tip. Theincision went down through the galea and periosteum overthe suboccipital bone and the posterior border of the ster-nocleidomastoid and trapezius muscles, proceeding to thelevel of C2. Emissary veins that opened during the subper-iosteal dissection were controlled using bipolar coagulationand waxed immediately, with repeated waxing at the end ofthe surgery. The spinous process of the 2nd cervical vertebrawas the palpatory bony landmark guide to the position of the
Fig. 2 (A) Coronal T1-weighted MRI showing a large mass lesion in the left CPA that extends to the hiatus incisura. (B) Operative photograph of apatient in semi-sitting position showing the extended retrosigmoid craniectomy with skeletonization of the SS (asterisk). (C) After elevation ofthe left cerebellar hemisphere, the large epidermoid tumor came clearly into view in the operative corridor. (D) A postoperative CT scan revealsGTR and the generous mastectomy, and a flat corridor to the CPA (arrow).
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Surgical Strategy for Dermoid and Epidermoid Tumors of the Posterior Fossa Lynch et al. 147

foramen magnum, and enabled a safe subperiosteal dissec-tion of the suboccipital region to be performed along theposterior C1 arch. The paravertebral muscles were detachedfrom the occipital bone squama and progressively sectionedwith a scalpel. A self-retaining retractor was graduallyinserted into the wound, thus exposing the suboccipitaltriangle and maintaining the paravertebral muscles in theappropriate position. At that point, the posterior arch of C1was identified.
CraniectomyThe retrosigmoid craniectomy is performed unilaterallyusing a high-speed drill with a cutting burr. The overlyingbone is reduced to the thickness of an eggshell, then a burrhole is drilled just inferior to the junction of the transversesinus (TS) and sigmoid sinus (SS). The craniectomy extended
medially� 5 cm. A regular Leksell rongeur is used to enlargethe craniectomy from the posterior edge of the occipitalcondyle to the inferior edge of the TS, exposing the lateraledge of the SS. In the case of large, giant or multicompart-ment tumors, we perform the extended retrosigmoidapproach: the dura mater is dissected bluntly from the innersurface of the sub-occipital squama; at that moment, therongeuring crosses the SS and comes to within almost acentimeter of the jugular bulb. After the SS has been thor-oughly exposed (skeletonizing), the mastoid process is ron-geured generously away, permitting a far lateral exposure. Ifthe meningioma extends to the foramen magnum (FM), theFM and the posterior arch of C1 are removed. The pieceremoved from thebone thinnedbya drill is the safestmethodof exposure of the SS. The access achieved provides a direct,parallel and unobstructed view of the petrous ridge,
Fig. 3 MRI and CT scan in cases of PFDETs found in this series.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Surgical Strategy for Dermoid and Epidermoid Tumors of the Posterior Fossa Lynch et al.148

providing sufficient midline and lateral exposure of thetumor. Emissary veins can produce brisk bleeding; thehemostasis is obtained with the help of bipolar coagulationor with hemostatic sponges. The operating microscope isbrought to the surgical field and the operation proceeds withmagnification, which ranges from 10X to 20X.
Opening the DuraThe dura mater is opened by a horseshoe-shaped incisionwith its base toward the midline. Two relaxing incisions aremade laterally, one to the TS and the other to the SS. The duraledges are tented up and rotate anteriorly with the SS out ofthe bone margins and down over the cut surface of themastoid. The arachnoid of the cisterna magna is incised,and the cerebrospinal fluid (CSF) is allowed to drain sponta-neously. The combination of bone removal, dural opening,and CSF drainage provides excellent visualization of theentire CPA, with minimal cerebellar retraction.
Exposing the LesionThe tumor was then visualized under the arachnoid as abright whitemass. The exposure was improved after a gentleelevation of the cerebellum, which was maintained in posi-tion with fixed retractors. The arachnoid attachments alongthe cerebellum in the cerebellopontine cistern were opened,and the arachnoid membrane enveloping the tumor wasincised in the posterior aspect of the exposed area usingmicro scissors. Then, the arachnoid membrane was gentlydissected away from the tumor surface to the sides usingmicrosurgery instruments. The arachnoid membrane wasleft intact to protect the brainstem from surgical dissection.At that point, the high magnification provided by the oper-ating microscope proved particularly beneficial. AlthoughIDETs are soft and usually poorly vascularized lesions, thor-ough hemostasis was obtained throughout the procedureusing bipolar forceps to keep the field bloodless.
Debulking the TumorAfter low-current bipolar coagulation under saline irrigationof a few fine vessels travelling on the tumor surface, thelesion was incised, penetrated, and progressively debulkedfrom within, mobilized, and removed in piecemeal fashion.Careful attention is paid to identifying and preserving thearachnoid plane at the tumor-brainstem interface, whichfacilitated complete tumor resection and minimized smallvessel, CN and brainstem injuries.
Dissecting the TumorAs the surgery proceeded within the space provided by theprogressive tumor debulking, the DET was dissected andmobilizedaway fromthefacial, acousticand trigeminalnerves,the brainstem, and blood vessels by gentle, meticulous micro-surgical techniques.We used, at that point, finemicro scissorsand several types of angled dissectors in addition to multiplemicroscope angulations at varying magnifications. As tumordebulking proceeded, thebrainstemprogressively relaxed andprovided additional working space for dissection. When deal-ingwith large lesions that compress anddeformthebrainstem,
these tumors should be dissected from, and not against, thebrainstem and CNs. The lesion was mobilized and, once rid ofadhesions, removed from the surgical field with cuppedforceps; small fragments were sucked away with the aid ofirrigation. The surgeons should be aware that CNs and vesselsare usually engulfed by the tumor; these delicate structuresshould be carefully dissected and spared. The aspiration isperformed in a soft suction mode during the microsurgicaldissection to avoid injuries to those fragile structures. Grosstotal tumor removal is always attempted, but whenever thedissection of the tumor from thebasilar and vertebral arteries,their perforating branches, the brainstem, or CNs could entailrisk of damage, we left a thin rim of tumor tissue attached tothosestructures. In caseof supratentorial tumorextension, thelesion would be resected through the ipsilateral corridor asmuch as possible, and the remnant would be followed for anysymptomatic or radiological growth. With recent advances inneuroendoscopic techniques, reports of endoscopic-assistedand purely endoscopic removal of CPA epidermoid tumorshave emerged. The endoscope is a useful adjunct to themicroscope in facilitating additional inspection and furtherresection of PFDETs. In this series, the endoscopic-assistedtechniques were only employed on two occasions. Duringthe operation, copious irrigation is provided, and cottonpads are placed around the exposed area to reduce the spillageof irritating cyst content into the subarachnoid space. Inspec-tion of the tumor bed with the operating microscope is thenperformed for verification of the extent of tumor resection.Before closure, the patient’s blood pressure is brought to anormotensive level for at least 10–15 minutes and monitoredfor risk of oozing. The dura is closed primarily or with a freepericranial graft. The craniectomy defect is covered with apaste made of bone dust and a few drops of blood and normalsaline. All open mastoid cells are sealed with bone wax toprevent CSF leaks. The superficial planes are closed in threelayers using interrupted nylon sutures. Postoperatively, allpatients are cared for at an intensive care unit before returningto the ward.
Illustrative CaseA 68-year-old woman developed progressive gait ataxia, dip-lopia, left-ear deafness, and a left facial paresis that lasted fortwoyears. AnMRI scan showed a tumor located in the left-sideCPA with brainstem distortion and contralateral shift(►Fig. 1A). The patient was placed in a semi-sitting, positionand the extended retrosigmoid approach was achieved(►Fig. 1B and C). The tumor occupied the entirely left CPAand engulfed most of the neurovascular structures. After STR,the 7th and 8th CNs were preserved, and the brainstem,decompressed (►Fig. 1D). A postoperative CT scan showedthe extent of themastoidectomy (►Fig. 1E). The recovery wasslow, but the patient eventually achieved a GOS score of 3.
Results
Patient Demographics and Clinical CharacteristicsSince this is a retrospective study, it has inherent biases anddrawbacks that only a multicenter, prospective study could
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Surgical Strategy for Dermoid and Epidermoid Tumors of the Posterior Fossa Lynch et al. 149

overcome.Twenty-onepatientswithPFDETswere identified.Atthe time of diagnosis, the patients’ average age was 32.4 years,ranging between 1 and 78 years. In our study, 11 (52.3%)patientsweremale, and 10 (47.6%)were female. The neurolog-ical symptoms and signs vary according to tumor location andextension of the lesion. The demographics, neurological pre-sentation, and results are summarized in ►Table 1.
NeuroimagingAll patientsunderwent aCT and/or anMRI scan. Ingeneral, thetumors appeared as low-density lesions on plain CT. The MRIrevealed that, in the majority of the cases, the lesion washypointense on T1-weighted and hyperintense on T2-weight-ed images, similarly to theMRI appearance of arachnoid cysts.When available, the differential diagnosis was solved oninspection of the diffusion-weighted images (DWIs), whichshowed the epidermoid tumors to be distinctly bright com-pared with arachnoid cysts and other tumors. The DWI is thebest MRI sequence to diagnose and follow-up these lesions.
One tumor appeared as a high-intensity signal on T1, andas amixed-intensity signal onT2. Five (22.7%) lesions showed
irregular enhancement after contrast injection. Two (9.5%) ofthem revealed calcifications. (►Fig. 1A and 1B)
Mortality, Morbidity, Extension of Resection, andRecurrenceWe used a tailored surgical approach to manage each case: a)from total 17 CPA tumors, for 11 patients, due to the large sizeor extension of the lesions, we chose the extended retrosig-moid approach. In other 6 individuals with smaller tumors, aconventional retrosigmoid approach was performed; b)vermian and fourth ventricular lesions were operated uponthrough a midline suboccipital craniectomy. There was nooperative mortality until 30 days after surgery, but 2 elderlypatients with CPA lesions died from pulmonary complicationsat the90thand210thpostoperativedays. Thefollow-upperiodranged from 1 to 21.5 years (mean: 7.2 years). Two patientswere lost to follow-up. The dissection of the adherent capsulefrom the 6th, 7th, and 8th CNs led to transient abducens andfacial nerve palsies, as well as permanent hearing loss, in7 patients. Eight patients had hearing deficits before surgery;none of them improved after surgery.Most facial nerve palsiesrecovered after a few months. Two pediatric patients withfourth ventricle tumors developed transient difficulty inswallowing. Temporary postoperative complications, includ-ing wound infection, CSF fistulas that needed reoperation,deep venous thrombosis, and pulmonary complicationsoccurred in 5 (22.7%) patients.
We achieved GTR in 16 (76.1%) patients, and STR in 5(23.8%), and surgeon impression and/or postoperative imag-ing confirmed all. Fourteen (66.6%) patients achieved GOSscores of 4 or 5.
Discussion
Mortality and MorbidityMany studies7–11,14,15,19,21,26–28 have reported that the clin-ical symptoms vary among patients depending on tumorlocation, ranging from slight CN deficits to severe ataxia, CNdysfunction, and brainstem compression, as we observed inthis series (►Table 1). Since the advent of microsurgicaltechniques, several series have shown that PFDETs can besurgically resected with a good outcome.4,12,17,20,28,29 Samiiet al12 revealed that operative morbidity and mortality fromPFDET removal had declined remarkably in the past 20 years.Before the advent of the operating microscope, the operativemortality ranged from 20% to 57%. Contemporary series havereported zero or low operative mortality4,12,15,19,20,28,30
(►Table 2). Notwithstanding, complications have been de-scribed.4,12,15,16,20,21 Aseptic meningitis is reported to be acommon cause of postoperative morbidity. Two patientsdeveloped a postoperative CSF leakage that needed reopera-tion to close the fistula. In this current series, there was nosurgical mortality.
Extension of Resection Dilemma and RecurrenceYasargil et al,4 Samii et al,12 and other authors7,15,27,30,31
advocate that the ideal management of PFDETs is GTR.However, GTR could be dangerous for some patients and
Table 1 Characteristics of 21 patients treated for PFDETs
n %
Age at treatment
1–78 years (mean: 32.4 years)
Gender
Male 11 52.3%
Female 10 47.6%
Location
CPA 17 80.9%
Cerebellar 4 19.0%
Neurological Presentation
Elevated ICP 9 42.8%
CN deficits 9 42.8%
Gait disturbance 8 38.0%
Visual deficit 4 19.0%
Trigeminal neuralgia 3 14.2%
Pathology
Epidermoid 17 80.9%
Dermoid 4 19.0%
Gross total removal 16 76.1%
Follow-up
1–23 years (mean: 6.1 years)
Surgical mortality 0 0%
Recurrence 3 14.2%
GOS 4 or 5 14 66.6%
Abbreviations: CN, cranial nerve; CPA cerebellopontine angle; GOS,Glasgow Outcome Sclae; ICP, intracranial hypertension; PFDETs,posterior fossa dermoid and epidermoid tumors.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Surgical Strategy for Dermoid and Epidermoid Tumors of the Posterior Fossa Lynch et al.150

difficult to achieve because these tumors can be criticallylocated, and there may be adherence or even encasement ofvital structures by the tumor.5,7,8,10,15–17,20,21 BecausePFDETs “flow” into any available subarachnoid space, slowlyincrease their volume and conform to the shape of thecavities they enter, CNs and arteries can be engulfed ordisplaced by the tumor. On diagnosis, many PFDETs arealready large or giant, and frequently have extended intomultiple anatomic compartments. For these reasons, manyauthors recommend that GTR should be avoided to decreasemortality and morbidity.15–17,19–21,28,29 In our series, threeCPA tumors spread along the cisterns of the posterior fossaand became partially trapped between the pons and theanteriorly displaced vertebrobasilar arteries, enveloping theperforating branches, and densely adhering to the brainstem.We performed a careful dissection at higher magnification toprevent injury of the fragile perforating vessels that wereengulfed by the tumor. However, even a delicate dissectioncould entail the risk of damaging these perforating vessels,which could provoke profound and permanent neurologicaldisabilities. We cautiously left a rim of tumor attached tothose structures (STR). In case those tumors had extendedinto multiple anatomic compartments, the lesion would beresected through the ipsilateral corridor as much as possible,and the contralateral or supratentorial remnant would befollowed for any symptomatic or radiological growth.
To preserve the function of the 7th and 8th nerves, wetook several careful steps during the surgery:
1. The preservation of the auditory artery branch is requisiteif the hearing is to be maintained.
2. Sharp dissection with micro scissors is used for thedissection of the tumor from the nerves, the use of bipolarcoagulation is kept to a minimal necessary, and whenused, the coagulation is done in small segments betweenthe forceps tips under a stream of normal saline, with alow current, to prevent heating damage.
3. The aspiration is regulated in the soft module, and asuction tip can be used without fear of damaging a nerveor vascular structures.
4. The dissection of the meningioma from the 7th and 8th
nerves should be performed frommedial to lateral, avoid-ing traction under the fragile cochlear nerve in themeatus.
5. After the removal of the lesion, if there is slight ooze underthe facial nerve, a hemostatic agent should be usedinstead of the bipolar coagulation.
6. Drilling the posterior wall of the IAC to remove intra-canalicular fragments is performed with a 2.5-mm burrunder continuous irrigation,without damaging the neuralstructures.
The best surgical strategy for PFDETs has been debated for along time. The controversy is underlined by one major ques-tion: how far can we go with the intent of achieving GTR? Onthe one hand, if the surgeon persists with any attempt toremove every last residual lesion to achieve the cure of thepatient, it could result in an unwarranted CNor arterial injury,thus increasing mortality and morbidity. On the other hand,experience emphasizes that when tumors are removed in-completely, they tend to regrow after varying periods of time.As Sekhar andWright30 point out, the next surgeon operatingon the patient will be confronted with severe adhesions ofblood vessels and CNs to the brain, and with the inability toremove the lesion entirely or nearly entirely. Because PFDETsare indolent, the risk of potential complications of GTR shouldbewellweighed against the benefits. Consequently, GTR is notalways a reasonable goal to achieve, especially in elderlypatients.7,8,10,12,16,17,20,21,25,28,29
Published papers on PFDETs have reported GTR rates rang-ing from 0% to 95.4%.4,7,8,10–12,14–16,20,21,29 In the currentseries, we achieved GTR in 72.7% of the patients (►Table 1).Our surgical objective was always to prioritize the patient’squality of life; therefore, STR could represent a very acceptablegoal in tumors encasing the basilar and vertebral arteries, orperforating vessels, or those adhering to CNs. Previous studieswith long-term follow-up have reported an overall estimatedrecurrence rate ranging from 0% to 26%.8,10,11,13,15,19,29,31 Inthe present series, the recurrence rate was of 9% (3 cases).
The extended retrosigmoid approach, first described byMalis L23,24 and subsequently by other authors,25 is anexcellent alternative approach to the classical retrosigmoidapproach. In this approach, the SS is fully skeletonized, movelateral and superior by a dural tend suture, expanding theoperative field to the CPA and deep vascular structures.A generous drilling of the mastoid air cells and skeletonizingthe SSmarkedly increase the anterior exposure and decreasethe amount of cerebellum retraction. It is particularly usefulin cases of giant tumors that extend into the incisural notchor to the contralateral side. This approach is quick, simple,safe, and diminishes the amount of bone removal in compar-ison with the more radical, time-consuming skull baseapproaches.23–25 There is a worry that the SS can besqueezed against the occipital bone and produce venouscongestion and cerebral edema. If this happens, it will be
Table 2 Contemporary surgical series on posterior fossa dermoidand epidermoid tumors
Authors/Year Numberof cases
MORT(%)
GTR(%)
REC(%)
F/U(years)
Berguer et al17/1985 13 0 0 7.6 4.6
De Souza et al19/1989 30 3.7 18 14.8 9
Yasargil et al4/1989 43 0 95.4 0 5.2
Lunardi et al8/1990 17 12 35 17.6 9
Vinchon et al21/1995 9 22.2 0 N/A 3
Samii et al12/1996 40 2.5 75 7.5 5.7
Mohanty et al20/1997 25 8 48 0 3.5
Talacchi et al15/1998 28 3.5 57 30 8.6
Kobata et al28/2002 30 0 56.7 6.6 11.4
Lynch et al/2017(present study)
21 0 76 9 7.2
Abbreviations: F/U, follow-up; GTR, gross total removal; MORT, mor-tality; N/A, not avaible; REC, recurrence.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Surgical Strategy for Dermoid and Epidermoid Tumors of the Posterior Fossa Lynch et al. 151

necessary to relieve the traction on the SS. This complicationwas not observed in this series. We used the extendedretrosigmoid approach in 11 patients with large, giant ormulticompartment lesions. In 3 out of our 4 patientswho hada supratentorial extension, the lesions could be entirelyremoved using this approach.
Conclusion
The neurosurgical management of PFDETs remains controver-sial, but our results allow us to conclude that the best surgicalstrategy is GTR. In cases of giant ormulticompartment lesions,the extended retrosigmoid approach, which offers directvision to the APC, reducing retraction to the cerebellum, is agood alternative. We achieved GTR in the majority of ourpatients without surgical mortality, and with low morbidity.However, GTR can be difficult to achieve because PFDETs canbe critically located, with adherence to and involvement ofvital structures. Our surgical objectivewas always to prioritizethe patient’s quality of life. Subtotal removal could represent avery acceptable goal in tumors encasing the basilar artery andperforating vessels or adhering to CNs. If the functional risk ofGTRoutweighs itspotential benefits, anSTRstrategy shouldbeadopted. Recurrence is rare after GTR, although a longerfollow-up is required.
References1 Zülch KJ. Brain tumors their biology and pathology. New York:
Springer; 1965:240–2452 Rubinstein LJ. Tumors of the nervous System. Washington. DC:
Armed Forces Institute of Pathology; 1972:288–2923 Russell DS, Rubinstein LJ. Pathology of Tumors of the Nervous
System, ed 4. Baltimore: Williams & Wilkins; 1977:29–324 Yaşargil MG, Abernathey CD, Sarioglu AÇ. Microneurosurgical
treatment of intracranial dermoid and epidermoid tumors. Neu-rosurgery 1989;24(04):561–567
5 Grant FC, Austin GM. Epidermoids; clinical evaluation and surgi-cal results. J Neurosurg 1950;7(03):190–198
6 Guidetti B, Gagliardi FM. Epidermoid and dermoid cysts. Clinicalevaluation and late surgical results. JNeurosurg1977;47(01):12–18
7 Schroeder HW, Oertel J, Gaab MR. Endoscope-assisted microsur-gical resection of epidermoid tumors of the cerebellopontineangle. J Neurosurg 2004;101(02):227–232
8 Lunardi P, Missori P, Innocenzi G, Gagliardi FM, Fortuna A. Long-term results of surgical treatment of cerebello-pontine angleepidermoids. Acta Neurochir (Wien) 1990;103(3-4):105–108
9 Obrador S, Lopez-Zafra JJ. Clinical features of the epidermoids ofthe basal cisterns of the brain. J Neurol Neurosurg Psychiatry1969;32(05):450–454
10 Rubin G, Scienza R, Pasqualin A, Rosta L, Da Pian R. Craniocerebralepidermoids and dermoids. A review of 44 cases. Acta Neurochir(Wien) 1989;97(1-2):1–16
11 Salazar J, Vaquero J, Saucedo G, Bravo G. Posterior fossa epider-moid cysts. Acta Neurochir (Wien) 1987;85(1-2):34–39
12 Samii M, Tatagiba M, Piquer J, Carvalho GA. Surgical treatment ofepidermoid cysts of the cerebellopontine angle. J Neurosurg1996;84(01):14–19
13 Ulrich J. Intracranial epidermoids. A study on their distributionand spread. J Neurosurg 1964;21:1051–1058
14 Yamakawa K, Shitara N, Genka S, Manaka S, Takakura K. Clinicalcourse and surgical prognosis of 33 cases of intracranial epider-moid tumors. Neurosurgery 1989;24(04):568–573
15 Talacchi A, Sala F, Alessandrini F, Turazzi S, Bricolo A. Assessmentand surgical management of posterior fossa epidermoid tumors:report of 28 cases. Neurosurgery 1998;42(02):242–251, discus-sion 251–252
16 Ahmed I, Auguste KI, Vachhrajani S, Dirks PB, Drake JM, Rutka JT.Neurosurgical management of intracranial epidermoid tumors inchildren. Clinical article. J Neurosurg Pediatr 2009;4(02):91–96
17 Berger MS, Wilson CB. Epidermoid cysts of the posterior fossa.J Neurosurg 1985;62(02):214–219
18 Cobbs CS, Pitts LH, Wilson CB. Epidermoid and dermoid cysts ofthe posterior fossa. Clin Neurosurg 1997;44:511–528
19 deSouza CE, deSouza R, da Costa S, et al. Cerebellopontine angleepidermoid cysts: a report on 30 cases. J Neurol NeurosurgPsychiatry 1989;52(08):986–990
20 Mohanty A, Venkatrama SK, Rao BR, Chandramouli BA, JayakumarPN, Das BS. Experience with cerebellopontine angle epidermoids.Neurosurgery 1997;40(01):24–29, discussion 29–30
21 VinchonM, Pertuzon B, Lejeune JP, Assaker R, Pruvo JP, ChristiaensJL. Intradural epidermoid cysts of the cerebellopontine angle:diagnosis and surgery. Neurosurgery 1995;36(01):52–56, discus-sion 56–57
22 Sanai N, McDermott MW. A modified far-lateral approach forlarge or giant meningiomas of the posterior fossa. J Neurosurg2010;112(05):907–912
23 Malis LI. Nuances in acoustic neuroma surgery. Neurosurgery2001;49(02):337–341
24 Malis LI. Acoustic neuroma Surgery. Randolf: Codman; 1987:1–2025 Quiñones-Hinojosa A, Chang EF, Lawton MT. The extended retro-
sigmoid approach: an alternative to radical cranial base approachesfor posterior fossa lesions. Neurosurgery 2006;58(04, Suppl 2):ONS-208–ONS-214, discussion ONS-214
26 Gagliardi FM, Vagnozzi R, Caruso R, Delfini R. Epidermoids of thecerebellopontine angle (cpa): usefulness of CT scan. Acta Neuro-chir (Wien) 1980;54(3-4):271–281
27 Altschuler EM, Jungreis CA, Sekhar LN, Jannetta PJ, Sheptak PE.Operative treatment of intracranial epidermoid cysts and cho-lesterol granulomas: report of 21 cases. Neurosurgery 1990;26(04):606–613, discussion 614
28 Kobata H, Kondo A, Iwasaki K. Cerebellopontine angle epider-moids presenting with cranial nerve hyperactive dysfunction:pathogenesis and long-term surgical results in 30 patients. Neu-rosurgery 2002;50(02):276–285, discussion 285–286
29 Gormley WB, Tomecek FJ, Qureshi N, Malik GM. Craniocerebralepidermoid and dermoid tumours: a review of 32 cases. ActaNeurochir (Wien) 1994;128(1-4):115–121
30 Talacchi A, Sala F, Alessandrini F, Turazzi S, Bricolo A. Assessmentand surgical management of posterior fossa epidermoid tumors:report of 28 cases. Neurosurgery 1998;42(02):242–251, discus-sion 251–252 (Comments)
31 Sabin HI, Bordi LT, Symon L. Epidermoid cysts and cholesterolgranulomas centered on the posterior fossa: twenty years ofdiagnosis andmanagement. Neurosurgery 1987;21(06):798–805
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Surgical Strategy for Dermoid and Epidermoid Tumors of the Posterior Fossa Lynch et al.152

The Natural History of Brain ArteriovenousMalformations
História natural das malformações arteriovenosasencefálicas
Carlos Michel Albuquerque Peres1 Vitor Nagai Yamaki2 Eberval Gadelha Figueiredo2
1Department of Neurosurgery, Hospital Santa Julia, Manaus,AM, Brazil
2Division of Neurosurgery, School of Medicine, Universidade de SãoPaulo, São Paulo, SP, Brazil
Arq Bras Neurocir 2017;36:153–159.
Address for correspondence Carlos Michel Albuquerque Peres, MD,Department of Neurosurgery, Hospital Santa Julia, Av. Jorn. UmbertoCalderaro Filho, 455 / 1204, Manaus, AM 69057-015, Brazil(e-mail: [email protected]).
Keywords
► intracranialarteriovenousmalformations
► arteriovenous fistula► cerebral hemorrhage► natural history of
diseases
Abstract Brain arteriovenous malformations (AVMs) are relatively rare lesions with irreversibleconsequences in the context of hemorrhage. They are characterized by directconnections between arteries and veins without an intervening capillary network.The natural history of brain AVMs is controversial in the literature, with low evidencelevel gathered in the papers published, and with large divergence of results amongthem. A detailed understanding of the natural history is critical for treatment decision.The risk of development of deleterious outcomes such as hemorrhage or braininfarction should always be considered when submitting a patient to the risks oftreatment. Several factors related to the patient and to the AVMs are determinants inthe natural history of this disease. The topography, size, morphology and angioarch-itecture of AVMs determine the risk of rupture. Large AVMs, those located in theposterior fossa and with deep venous drainage, have higher risk of rupture. Due todivergence in the literature regarding the natural history of AVMs, the choice oftreatment should also consider experiences acquired over the years from referencecenters with a high number of AVMs treated per year. We determined 7 variables thatshould be considered during the decision to treat an AVM: 1) previous hemorrhage; 2)aneurysm associated to the AVM; 3) direct arteriovenous fistula; 4) factors related tothe nidus; 5) age and habits (smoking, sedentary lifestyle, diet quality); 6) thefunctional performance of the patient; 7) psychological factors.
Resumo Malformações arteriovenosas (MAVs) são lesões caracterizadas por conexões diretasentre artérias e veias sem rede capilar. São relativamente raras e com consequênciasmuitas vezes irreversíveis no contexto de hemorragia. A história natural das MAVs écontroversa na literatura, com pouca evidência extraída dos artigos publicados, alémde alta divergência entre resultados. Um entendimento detalhado da história naturalda doença é determinante para a decisão do tratamento. O risco de desenvolver
receivedMay 18, 2017acceptedJune 5, 2017published onlineJuly 19, 2017
DOI https://doi.org/10.1055/s-0037-1604344.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Review Article | Artigo de Revisão 153

Introduction
Brain arteriovenousmalformations (AVMs) are characterizedby a nidus of abnormal vessels that forms a direct connectionbetween arteries and veins, without an intervening capillarybed, resulting in one or several arteriovenous fistulas in thesame lesion.1,2 Arteriovenous malformations have specificcharacteristics according to their topography, size, morphol-ogy, and angioarchitecture. Therefore, the choice of treat-ment should be individualized for each patient. Despite therelatively low prevalence (16 cases per 100,000 habitants),3
they are the most frequent etiology of non-traumatic intra-cranial hemorrhage in the young population (< 40 yearsold).4,5
Although several papers have been published recently,there are no evidence-based guidelines for the treatment ofAVMs.6 Most studies addressing the natural history of thisdisease were conducted with an observational design withlow statistical power for consistent conclusions; in addition,there is a large disagreement among the results presented inthe literature. Thus, the risk factors should be carefully takeninto consideration before the decision to treat these lesions.7
The Natural History of AVM
There is a large spectrum of AVMs presenting symptom, suchas:
– Cerebral hemorrhage (50%): the neurological deficit isrelated to the topography of the lesion inside the paren-chyma, or to its extension to the subarachnoid or ventric-ular compartments.
– Seizure (30%): the seizure semiology might be related tospecific locations in the brain, especially for focal seizures.
– Headache (14%).– Other symptoms: neurological deficit (related to inade-
quate blood influx caused by the AVM shunt); and pulsa-tile tinnitus.
The frequency of these symptoms varies according to thegeographical differences of the population studied: hemor-rhage represented 71% of AVM presenting symptoms in
Nordic countries, while in the United States and Europethe rates were 42% and 52% respectively.8,9
The most common hemorrhage caused by AVM rupture isintraparenchymal bleeding; but, in 24% of the cases, sub-arachnoid or ventricular hemorrhagemay be associated.10,11
Arteriovenous malformations are usually isolated lesions,except when they are included in the manifestations ofgenetic diseases, such as hemorrhagic hereditary telangiec-tasia (Rendu-Osler-Weber disease).12
Thefirst question to be answered is related to the decisionof whether to treat AVMs: is the risk of hemorrhage higherthan the riskof the treatment? Unfortunately, such details onthe natural history of AVMs remain unknown. The firststudies that came out addressing this issue were surgicalcase series with only frequency variables analyzed retro-spectively.13,14 Nowadays, the multivariate analysis in largeprospective series predicts the annual risk of rupture relatedto a specific risk factor. This study design is certainly addingmore evidence to the literature over time.15
Intracranial hemorrhagewas the most frequent symptom(65% of cases) at admission in a population study conductedby the Mayo Clinic in the state of Minnesota, USA. Theincidence rate of the first hemorrhage was of 0.82 per100.000 people/year; 75% of the bleeding events happenedin patients under 50 years old, and the mortality rate in30 days was of 17.5%.16
Ondra et al,11 in a prospective study of 166 symptomaticAVM patients with 24 years of follow-up, found an annualrate of rupture of 4% per year, and a mortality rate of 1% peryear. At the end of this study, 23% of the patients had died ofhemorrhage. This study was a landmark for the naturalhistory of AVMs. However, the data included ruptured andunruptured AVMs in the same analysis; moreover, mostpatients had their hemorrhages detected clinically or bylumbar puncture, since the computerized tomography (CT)scan only became available after 1973, while the study wasaccomplished in 1975.17
Considering the annual risk of rupture between 2–4% forunruptured AVMs, a formula to estimate the risk of hemor-rhage has been suggested.8,18,19
RISK OF HEMORRHAGE (%) ¼ 105–AGE
consequências deletérias como hemorragia ou isquemia deve ser sempre conside-rado antes de submeter pacientes ao tratamento. Vários fatores relacionados aopaciente e às MAVs são determinantes na história natural da doença. A localização,tamanho, morfologia e angioarquitetura das MAVs estimam o risco de ruptura. AsMAVs grandes, de fossa posterior, com drenagem venosa profunda, têm maior riscode ruptura. A decisão de tratar deve também levar em conta a experiência do serviço,adquirida após anos de tratamento de MAVs. Nós determinamos 7 fatores quedevem ser avaliados diante da decisão de tratamento das MAVs: 1) hemorragiaprévia; 2) aneurismas associados à MAV; 3) fístula arteriovenosa; 4) fatores relacio-nados ao nidus; 5) idade e hábitos de vida; 6) performance funcional do paciente; 7)fatores psicológicos.
Palavras-chave
► malformaçõesarteriovenosasintracranianas
► fístulaarteriovenosa
► hemorragiacerebral
► história natural dasdoenças
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Natural History of Brain AVMs Peres et al.154

This formula was created based on a homogeneous popu-lation, and does not consider additional risk factors thatmight increase the chances of hemorrhage, such as: associ-ated aneurysms, venous drainage stenosis, and AVMtopography.
In 2008, a Finnish study included 238 patients withuntreated AVMs from admission to the beginning of treat-ment or hemorrhage or death. The study lasted from 1942until 2005, with amedian follow-up of 13.5 years. The annualrate of hemorrhage was of 2.4%, and the risk factors identi-fied were: younger population, previous rupture, deep loca-tion, infratentorial lesions and those with exclusive deepvenous drainage.20 Then, a Canadian study21 with 678 pa-tients (211 previously submitted to partial embolization),using the same statistic tests, found an annual risk ofhemorrhage of 4.6%. Even though both studies were per-formed under same conditions and methodological require-ments, the Canadian population presented a risk ofhemorrhage � 2 times higher.
The study “Columbia and the New York Island” (ColumbiaAVMDatabaseprojectandtheNewYork IslandsAVMstudy)22,23
performed a prospective analysis of over 600 patients. Themainfindings of this study were:
– Annual incidence of hemorrhage of 34.4% for patientswith 3 simultaneous risk factors: previous hemorrhage,deep location and deep venous drainage.
– Annual incidence of hemorrhage determined at 4.5% forpatients with only previous hemorrhage.
– For patients without previous hemorrhage, the annualrate of hemorrhagewas 3.1% for deep location AVMs; 2.4%for AVMs with deep venous drainage; and 0.9% for pa-tients without any risk factor.17
The study called “A Randomized Trial of Unruptured BrainArteriovenous Malformations” (ARUBA) gathered resultsfrom different institutions worldwide, and found that theconservative treatment had better outcomes than interven-tion (surgery, radiosurgery, embolization). However, thisstudy recruited only 226 out of the initially planned sample
of 400 patients due to a National Institution of Health (NIH)safety board intervention, since the preliminary resultsshowed symptomatic stroke or death in 10% of the patientsfor the clinical treatment group, and in 31% of those submit-ted to any intervention (p < 0.0001) during a mean follow-up of 33 months.24
The external validity of the ARUBA trial was questionedsince AVMs with different grades were analyzed together, aswell as different interventions (surgery, coiling, radiosur-gery). There was a considerable selection bias in the recruit-ment of the patients. Several centers in the United States didnot contribute with the research due to lack of clinicalequipoise, since there was not enough doubt to justify therandomization instead of treating patients with high riskfactor unruptured AVMs.25 ►Table 1 summarizes the mainshortcomings of the ARUBA trial.
In a meta-analysis published by the American Associationof Neurological Surgeons,13 Gross and Du gathered informa-tion from 9 natural history studies with 3.923 patients and18.423 patient-years of follow-up. The annual rate of hem-orrhage was of 2.2% (95% confidence interval [95%CI]: 1.7–2.7%) for unruptured AVMs; and of 4.5% (95%CI: 3.7–5.5%) forruptured AVMs. These resultsmight be influenced by the riskfactors that will be described in the next section.
Risk Factors for AVM hemorrhage
Arteriovenous malformations belong to a heterogeneousgroup of cerebrovascular diseases in which several riskfactors influence the risk of rupture. A well-designed multi-variate analysis can differentiate the independent risk fac-tors from those that are just associated with a positivepredictive value.9 For example, it was postulated thatAVMs with a small nidus have higher risk of rupture. How-ever, a prospective Finnish study proved that a larger nidus isa good predictor of future hemorrhagic events.26,27 Anotherrelationship previously accepted was that younger patientswere more prone to AVM rupture; however, the oppositerelation showed statistical significance in the most current
Table 1 ARUBA trial shortcomings
Topic Limitations
Study design Absence of therapeutic plan: selection bias (the European centers randomizedmore for endovasculartherapy, while the American centers randomized more AVMs for the surgery group).
The study did not analyze the outcomes with different interventions separately. Thus, the studysuggested the superiority of the clinical treatment for all kinds of unruptured AVMs, but failed todetermine whether this is true for one specific treatment modality.
The study did not evaluate the associated conditions that would increase the risk of AVM rupture,such as: the angioarchitecture and topography of the lesions, and the presence of aneurysms.Therefore, the study failed to conclude if the clinical treatment is superior for all types of AVMs.
The requirement for participation in the study was 10 AVMs treated per year. This may suggest thatcenters unexperienced in AVMs collaborated with the treatment outcomes.
Study conduction Short follow-up (3 years); intervention group still under analysis.
Cohort shorter than planned (interrupted for ethical and safety issues).
Abbreviations: ARUBA, A Randomized Trial of Unruptured Brain Arteriovenous Malformations; AVMs, arteriovenous malformations.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Natural History of Brain AVMs Peres et al. 155
large series.28 It is noteworthy that the most updated knowl-edge about AVMs is based on non-randomized observationalstudies with some degree of methodological bias.7
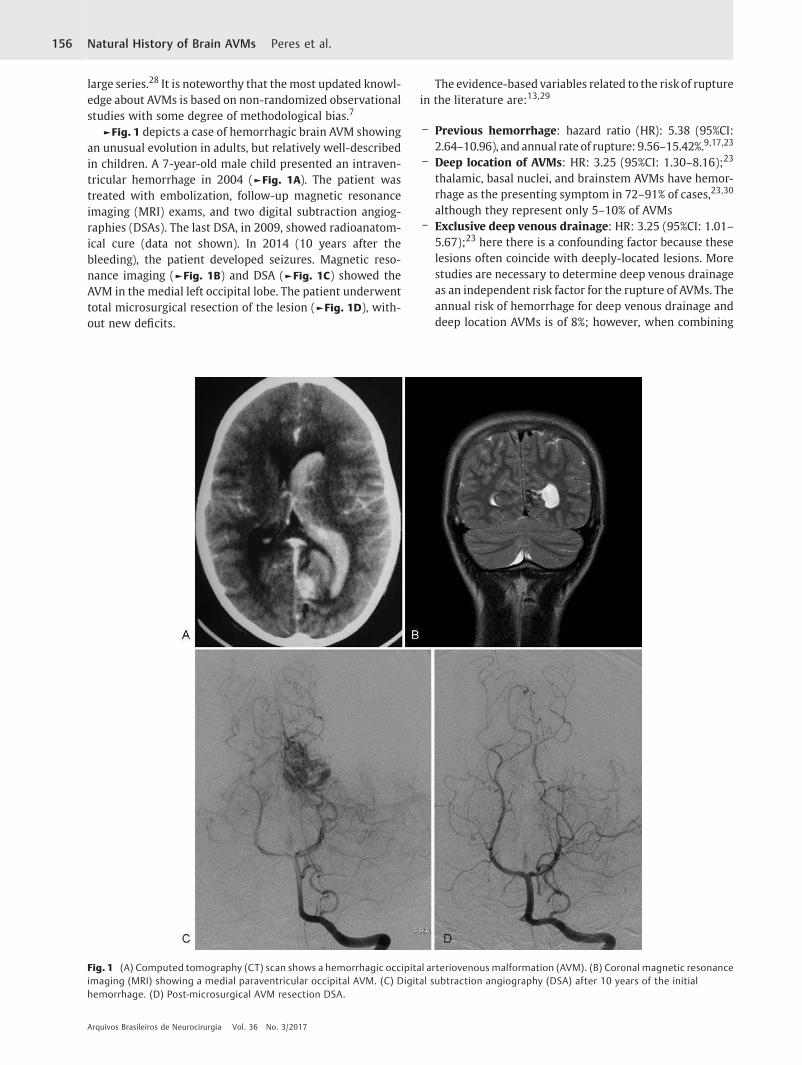
►Fig. 1 depicts a case of hemorrhagic brain AVM showingan unusual evolution in adults, but relatively well-describedin children. A 7-year-old male child presented an intraven-tricular hemorrhage in 2004 (►Fig. 1A). The patient wastreated with embolization, follow-up magnetic resonanceimaging (MRI) exams, and two digital subtraction angiog-raphies (DSAs). The last DSA, in 2009, showed radioanatom-ical cure (data not shown). In 2014 (10 years after thebleeding), the patient developed seizures. Magnetic reso-nance imaging (►Fig. 1B) and DSA (►Fig. 1C) showed theAVM in the medial left occipital lobe. The patient underwenttotal microsurgical resection of the lesion (►Fig. 1D), with-out new deficits.
The evidence-based variables related to the riskof rupturein the literature are:13,29
– Previous hemorrhage: hazard ratio (HR): 5.38 (95%CI:2.64–10.96), and annual rate of rupture: 9.56–15.42%.9,17,23
– Deep location of AVMs: HR: 3.25 (95%CI: 1.30–8.16);23
thalamic, basal nuclei, and brainstem AVMs have hemor-rhage as the presenting symptom in 72–91% of cases,23,30
although they represent only 5–10% of AVMs– Exclusive deep venous drainage: HR: 3.25 (95%CI: 1.01–
5.67);23 here there is a confounding factor because theselesions often coincide with deeply-located lesions. Morestudies are necessary to determine deep venous drainageas an independent risk factor for the rupture of AVMs. Theannual risk of hemorrhage for deep venous drainage anddeep location AVMs is of 8%; however, when combining
Fig. 1 (A) Computed tomography (CT) scan shows a hemorrhagic occipital arteriovenous malformation (AVM). (B) Coronal magnetic resonanceimaging (MRI) showing a medial paraventricular occipital AVM. (C) Digital subtraction angiography (DSA) after 10 years of the initialhemorrhage. (D) Post-microsurgical AVM resection DSA.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Natural History of Brain AVMs Peres et al.156

deep venous drainage with previous bleeding, the risk isof 11.4% per year.9,27
– Arteriovenous fistula: it is characterized by direct con-nections between arteries and veins without a nidalnetwork interposed. Those fistulas might be within theAVM31 nidus, whichmay be identified only through superselective DSA with microcathethers.31
– Venous ectasias: they are characteristic of reduced ve-nous drainage, which is considered a risk factor forrupture. The hemorrhage happens by rupture of the nidalvessels, often the vein of drainage, for increased pressureor thrombosis.32
– AVM-related aneurysms: aneurysms are present in 2.3%to 16.7% of brain AVMs.33 They represent a risk factor forhemorrhage, with an odds ratio of 1.8 (95%CI: 1.6–2.0).13
Aneurysms on the distal arterial branches (closer to thenidus) or intranidal aneurysms aremore prone to rupture.It is a hard task to identify intranidal aneurysms, for theiridentification depends on a good-quality microcathethe-rization.34 Some authors consider those aneurysms origi-nating from the venous system, since, histologically, thenidus is more related to the venous structure.34,35 Proxi-mal aneurysms (Willis polygon arteries), related or not tothe arterial influx of the nidus, do not increase the risk ofAVM hemorrhage. Some authors advocate that theyshould be treated as saccular aneurysms, according tothe findings of the International Study of UnrupturedIntracranial Aneurysms (ISUIA).34,36,37 Proximal aneur-ysms aremore easily diagnosed by DSA, and have a higherincidence in the elderly and posterior circulation.38
Treatment indications for ArteriovenousMalformation
The decision of whether to treat an AVMor not is not a simpletask, especially for the unruptured lesions. A strict clinical
pre-operative evaluation is mandatory, including age, de-tailed neurological examination, use of anti-epileptic drugs,perspectives about the disease, degree of disability, and itsinfluence in daily life activities. The modified Rankin scale isthe most relevant scale to stratify these patients. ►Fig. 2
shows the case of a valid option for conservative treatment.A 42 year-old woman, a Portuguese language college profes-sor, with a single episode of seizure, which was well-con-trolled with anticonvulsant monotherapy. Conservativetreatment was chosen. This is the 4th year MRI (►Fig. 2A)and second digital subtraction angiography (►Fig. 2B),unchanged related to the first one (data not shown).
In addition, a detailed neuroimaging evaluation should beperformed, including an MRI with susceptibility weightedimaging, and good-quality DSA with at least 4 framesper second. Three-dimensional imaging reconstructionsand microcatheterization techniques will provide additionalinformation on the therapeutic plan, as well as enhance thepossibility of detecting small intranidal aneurysms.
The classification of AVMs as ruptured and unruptured isbased on clinical presentation and imaging findings (CT orMRI). They can also be differentiated according to histologicalcharacteristics after microsurgical resection. The unrupturedAVMs, inmore than30%of cases, showmicrohemorrhages dueto the presence of hemosiderin and macrophages.38
Magnetic resonance imaging sequencing with increasediron sensibility, such as T2� gradient echo and susceptibility-weighted images,might detectmicrohemorrhages in asymp-tomatic AVM patients. The micro hemorrhage found in thosepatients can be compared with sentinel hemorrhage in theaneurismal subarachnoid hemorrhage.39,40
Before making the decision to treat or not an AVM, it isalways important to consider:
1. Previous hemorrhage.2. Aneurysm associated to the AVM.
Fig. 2 (A) MRI showing a left frontal unruptured AVM. (B) DSA showing a left frontal unruptured AVM.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Natural History of Brain AVMs Peres et al. 157

3. Direct arteriovenous fistula.4. Factors related to the nidus.5. Age and habits (smoking, sedentary lifestyle, diet quality).6. The functional performance of the patient.7. Psychological factors.
The aforementioned topics do not represent a consensusin the literature. However, there is no guideline with level 1or 2 of evidence addressing the treatment decisions in AVMs.Therefore, the decisions should be taken based on theevidences that fit better according to the clinical practiceexperience; moreover, a multidisciplinary discussion (withneuroradiologists, neurologists, neurosurgeons, and radio-therapists) ismandatory in order to achieve better outcomes.Since it is a relatively rare disease, favorable outcomes mightbe easily reached through specialized AVM centers withenough cases and acquired experience over time. ►Table 2
summarizes the annual rate of AVM rupture according totopographic and vascular variables.
References1 McCormick WF. The pathology of vascular (“arteriovenous”)
malformations. J Neurosurg 1966;24(04):807–8162 Atkinson RP, Awad IA, Batjer HH, et al; Joint Writing Group of the
Technology Assessment Committee American Society of Inter-ventional and Therapeutic Neuroradiology; Joint Section onCerebrovascular Neurosurgery a Section of the American Asso-ciation of Neurological Surgeons and Congress of NeurologicalSurgeons; Section of Stroke and the Section of InterventionalNeurology of the American Academy of Neurology. Reportingterminology for brain arteriovenous malformation clinical andradiographic features for use in clinical trials. Stroke 2001;32(06):1430–1442
3 Al-Shahi R, Fang JS, Lewis SC,WarlowCP. Prevalence of adultswithbrain arteriovenous malformations: a community based study inScotland using capture-recapture analysis. J Neurol NeurosurgPsychiatry 2002;73(05):547–551
4 Fleetwood IG, Steinberg GK. Arteriovenousmalformations. Lancet2002;359(9309):863–873
5 Ruíz-Sandoval JL, Cantú C, Barinagarrementeria F. Intracerebralhemorrhage in young people: analysis of risk factors, location,causes, and prognosis. Stroke 1999;30(03):537–541
6 Pollock BE. The alchemy of brain arteriovenous malformationmanagement. World Neurosurg 2015;83(03):337–338
7 Raymond J, Naggara O, Guilbert F, AltmanDG. Assessing prognosisfrom nonrandomized studies: an example from brain arteriove-nous malformations. AJNR Am J Neuroradiol 2011;32(05):809–812
8 Ogilvy CS, Stieg PE, Awad I, et al; Stroke Council, AmericanStroke Association. Recommendations for the management ofintracranial arteriovenous malformations: a statement forhealthcare professionals from a special writing group of theStroke Council, American Stroke Association. Circulation 2001;103(21):2644–2657
9 Abecassis IJ, Xu DS, Batjer HH, Bendok BR. Natural history of brainarteriovenous malformations: a systematic review. NeurosurgFocus 2014;37(03):E7
10 Graf CJ, Perret GE, Torner JC. Bleeding from cerebral arteriovenousmalformations as part of their natural history. J Neurosurg 1983;58(03):331–337
11 Ondra SL, Troupp H, George ED, Schwab K. The natural history ofsymptomatic arteriovenousmalformations of thebrain: a 24-yearfollow-up assessment. J Neurosurg 1990;73(03):387–391
12 Brown RD Jr, Flemming KD, Meyer FB, Cloft HJ, Pollock BE, LinkML. Natural history, evaluation, and management of intracranialvascular malformations. Mayo Clin Proc 2005;80(02):269–281
13 Gross BA, Du R. Natural history of cerebral arteriovenous mal-formations: a meta-analysis. J Neurosurg 2013;118(02):437–443
14 Forster DM, Steiner L, Håkanson S. Arteriovenous malformationsof the brain. A long-term clinical study. J Neurosurg 1972;37(05):562–570
15 Stefani MA, Porter PJ, terBrugge KG, Montanera W, Willinsky RA,Wallace MC. Angioarchitectural factors present in brain arterio-venous malformations associated with hemorrhagic presenta-tion. Stroke 2002;33(04):920–924
16 Brown RD Jr, Wiebers DO, Torner JC, O’Fallon WM. Frequency ofintracranial hemorrhage as a presenting symptom and subtypeanalysis: a population-based study of intracranial vascular mal-formations in Olmsted Country, Minnesota. J Neurosurg 1996;85(01):29–32
17 Stapf C, Mohr JP, Choi JH, Hartmann A, Mast H. Invasive treatmentof unruptured brain arteriovenous malformations is experimen-tal therapy. Curr Opin Neurol 2006;19(01):63–68
18 Kondziolka D, McLaughlin MR, Kestle JR. Simple risk predictionsfor arteriovenous malformation hemorrhage. Neurosurgery1995;37(05):851–855
19 Brown RD Jr. Simple risk predictions for arteriovenous malforma-tion hemorrhage. Neurosurgery 2000;46(04):1024
20 Hernesniemi JA, Dashti R, Juvela S, Väärt K, Niemelä M, Laakso A.Natural history of brain arteriovenous malformations: a long-term follow-up study of risk of hemorrhage in 238 patients.Neurosurgery 2008;63(05):823–829, discussion 829–831
21 da Costa L, Wallace MC, Ter Brugge KG, O’Kelly C, Willinsky RA,Tymianski M. The natural history and predictive features ofhemorrhage from brain arteriovenous malformations. Stroke2009;40(01):100–105
22 Stapf C, Mast H, Sciacca RR, et al; New York Islands AVM StudyCollaborators. The New York Islands AVM Study: design, studyprogress, and initial results. Stroke 2003;34(05):e29–e33
23 Stapf C, Mast H, Sciacca RR, et al. Predictors of hemorrhage inpatients with untreated brain arteriovenous malformation. Neu-rology 2006;66(09):1350–1355
Table 2 AVM annual bleeding rate according to previous hemorrhage, venous drainage pattern and nidus topography9,17
Previous hemorrhage Superficial venous drainage Deep venous drainage Nidus topography
Unruptured AVM 0.9% 2.4% Superficial nidus
3.1% 8.0% Deep nidus
Ruptured AVM 14.8% 34.4%
4.5% 11.4% Superficial nidus
Abbreviation: AVM, arteriovenous malformation.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Natural History of Brain AVMs Peres et al.158

24 Mohr JP, Parides MK, Stapf C, et al; international ARUBA investi-gators. Medical management with or without interventionaltherapy for unruptured brain arteriovenous malformations (AR-UBA): a multicentre, non-blinded, randomised trial. Lancet 2014;383(9917):614–621
25 Amin-Hanjani S. ARUBA results are not applicable to all patientswith arteriovenous malformation. Stroke 2014;45(05):1539–1540
26 Spetzler RF, Hargraves RW, McCormick PW, Zabramski JM, FlomRA, Zimmerman RS. Relationship of perfusion pressure and size torisk of hemorrhage from arteriovenous malformations. J Neuro-surg 1992;76(06):918–923
27 Laakso A, Hernesniemi J. Arteriovenous malformations: epide-miology and clinical presentation. Neurosurg Clin N Am 2012;23(01):1–6
28 FullertonHJ,AchrolAS, JohnstonSC,et al;UCSFBAVMStudyProject.Long-term hemorrhage risk in children versus adults with brainarteriovenous malformations. Stroke 2005;36(10):2099–2104
29 Pollock BE, Flickinger JC, Lunsford LD, Bissonette DJ, Kondziolka D.Factors that predict the bleeding risk of cerebral arteriovenousmalformations. Stroke 1996;27(01):1–6
30 Cheng C-H, Crowley RW, Yen C-P, Schlesinger D, Shaffrey ME,Sheehan JP. Gamma Knife surgery for basal ganglia and thalamicarteriovenous malformations. J Neurosurg 2012;116(04):899–908
31 Yuki I, Kim RH, Duckwiler G, et al. Treatment of brain arteriove-nous malformations with high-flow arteriovenous fistulas: riskand complications associated with endovascular embolization inmultimodality treatment. Clinical article. J Neurosurg 2010;113(04):715–722
32 Valavanis A, Pangalu A, Tanaka M. Endovascular treatment ofcerebral arteriovenous malformations with emphasis on thecurative role of embolisation. Interv Neuroradiol 2005;11(01,Suppl 1):37–43
33 Miyasaka K, Wolpert SM, Prager RJ. The association of cerebralaneurysms, infundibula, and intracranial arteriovenous malfor-mations. Stroke 1982;13(02):196–203
34 D’Aliberti G, Talamonti G, Cenzato M, et al. Arterial and venousaneurysms associated with arteriovenous malformations. WorldNeurosurg 2015;83(02):188–196
35 Cagnazzo F, Brinjikji W, Lanzino G. Arterial aneurysms associatedwith arteriovenous malformations of the brain: classification,incidence, risk of hemorrhage, and treatment-a systematic re-view. Acta Neurochir (Wien) 2016;158(11):2095–2104
36 Wiebers DO,Whisnant JP, Huston J III, et al; International Study ofUnruptured Intracranial Aneurysms Investigators. Unrupturedintracranial aneurysms: natural history, clinical outcome, andrisks of surgical and endovascular treatment. Lancet 2003;362(9378):103–110
37 Mansmann U, Meisel J, Brock M, Rodesch G, Alvarez H, LasjauniasP. Factors associated with intracranial hemorrhage in cases ofcerebral arteriovenous malformation. Neurosurgery 2000;46(02):272–279, discussion 279–281
38 Morgan MK, Alsahli K, Wiedmann M, Assaad NN, Heller GZ.Factors Associated With Proximal Intracranial Aneurysms toBrain Arteriovenous Malformations: A Prospective Cohort Study.Neurosurgery 2016;78(06):787–792
39 Abla AA, Nelson J, Kim H, Hess CP, Tihan T, Lawton MT. Silentarteriovenous malformation hemorrhage and the recognition of“unruptured” arteriovenous malformation patients who benefitfrom surgical intervention. Neurosurgery 2015;76(05):592–600,discussion 600 discussion
40 LawtonMT, Abla AA. In Reply: Silent ArteriovenousMalformationHemorrhage and the Recognition of “Unruptured”ArteriovenousMalformation Patients Who Benefit From Surgical Intervention.Neurosurgery 2015;77(05):E843–E844
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Natural History of Brain AVMs Peres et al. 159

Endoscopic and Microsurgical Approaches tothe Cavernous Sinus – Anatomical Review
Abordagem endoscópica e microcirúrgica do seiocavernoso – revisão da anatomia
Flavio Ramalho Romero1 Daphyne Ramires1 Luigi Carrara Cristiano1 Marcos Paulo Silva1
Rodolfo Brum Vieira1
1Faculdade de Medicina, Universidade Estadual Paulista Julio deMesquita Filho, Botucatu, São Paulo, Brazil
Arq Bras Neurocir 2017;36:160–166.
Address for correspondence Flavio Ramalho Romero, MD, MSc, PhD,Universidade Estadual Paulista Julio de Mesquita Filho, Faculdade deMedicina, Botucatu, São Paulo, Brazil (e-mail: [email protected]).
Introduction
Cavernous sinus surgery has always represented a surgicalchallenge due to the great importance of the surrounding
anatomical structures and to the high morbidity associated toit.1,2 The pathological findings of the cavernous sinus regionare diverse and include intrinsic and extrinsic lesions, such asvascular and neoplastic lesions, and inflammatory diseases,
Keywords
► cavernous sinus► endoscopic
endonasal approach► transsphenoidal
surgery► transpterygoid
approach► microsurgical
cavernous sinus
Abstract Cavernous sinus surgery has always represented a surgical challenge due to the greatimportance of the surrounding anatomical structures and to the high morbidityassociated to it. Although the anatomy of this region has been extensively described,controversy remains related to the best treatment and approaches for different kinds oflesions. In this article, a literature review was performed on the surgical anatomy andapproaches to the cavernous sinus.
Palavras-chave
► seio cavernoso► acesso endoscópico
endonasal► cirurgia
transesfenoidal► acesso
transesfenoidal► microcirurgia do seio
cavernoso
Resumo A cirurgia da região do seio cavernoso sempre representou um desafio devido à grandeimportância das estruturas anatômicas e às altas taxas de morbidade associadas.Embora a anatomia da região tenha sido extensivamente descrita, permanece contro-verso o melhor tratamento e o acesso para diferentes tipos de lesão que acometem aregião. Neste artigo foi realizada uma revisão de literatura focando a anatomia cirúrgicae os acessos à região do seio cavernoso.
receivedMarch 27, 2017acceptedMay 31, 2017published onlineJuly 12, 2017
DOI https://doi.org/10.1055/s-0037-1604166.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Review Article | Artigo de Revisão160

with several different approaches described to deal withlesions in and around this region.1,2 The aims of the surgeryare to confirm cavernous sinus invasion, to reach a histologicaldiagnosis, and to remove the tumor as radically as possible.3,4
Although the anatomy of this region has been extensivelydescribed, the best approach to cavernous sinus lesions iscontroversial. In this article, a literature review was per-formed using the main databases available (Embase,PubMed/MEDLINE, and Scielo) on surgical anatomy of thecavernous sinus focusing on the advantages and disadvan-tages of the endoscopic and microsurgical techniques. Someexamples of cases are also presented.
Anatomical Review of the Cavernous Sinus
The cavernous sinus is a venous structure in themiddle cranialbase resting on the intracranial surface of the sphenoid andtemporal bones, surrounded by dural walls, which containsneurovascular structures and face the sella turcica, with thepituitary gland on one side, and the temporal lobe on the otherside. Defined as a dural envelope, it contains the third, fourth,fifth and sixth cranial nerves and the cavernous carotid ar-tery1,2, but it is also the site of venous confluence that receivesthe terminal end of multiple veins from the orbit, the sylvianfissure, and theanterior andmiddlefossae. Thecavernoussinushas free communicationwith the basilar, superior and inferiorpetrosal sinuses, and with the intercavernous sinuses.1–7
The cavernous sinus is located on the intracranial surfaceof the sphenoid and temporal bones (►Fig. 1). The anterioredge of the cavernous sinus extends downward from thelower surface of the anterior clinoid process along theanterior edge of the carotid sulcus and the posterior edgeof the optic strut and superior orbital fissure. The posterioredge extends from the posterior clinoid process above to thejunction of the petrous apex with the body of the sphenoidbone below. After defining the anterior and posterior limits,the upper and lower limits of the cavernous sinus are definedby lines extending from the upper and lower ends of theanterior and posterior edges. The inferior limit extendsbackward from just below the inferior edge of the superiororbital fissure and lower edge of the carotid sulcus, passesalong the lateral edge of the intracranial end of the carotidcanal, and ends at the superior end of the petroclival fissure.The superior limit extends from the lower surface of the baseof the anterior clinoid process along the lateral margin of thesella to the posterior clinoid process.1–7
The posterior part of the lower edge of the sinus is locatedabove the junction of the petrous apex and the body of thesphenoid bone at the upper end of the petroclival fissure, andthe posterior edge of the medial wall rests against the lateraledge of the dorsum sellae.1–4 The cavernous sinus extendsdownward and laterally from the lateral margin of the sella,across the sphenoid body to the junction of the body andgreater sphenoid wing of the sphenoid, but does not extendlaterally to include the margins of the foramina ovale,rotundum, or spinosum, although venous channels coursingthrough and around these foramina empty into the sinus andare part of the pericavernous venous plexus.1–6
The cavernous sinus has four walls: lateral and medialwalls, a roof, and posterior walls. The roof faces the basalcisterns; the lateral wall faces the temporal lobe; the medialwall faces the sella turcica, pituitary gland, and sphenoidbone; and the posterior wall faces the posterior cranial fossa.The medial and lateral walls join inferiorly at the level of thesuperior margin of the second division of the trigeminalnerve (maxillary nerve), and the narrow anterior edgeborders the superior orbital fissure.1–7
The nerves related to the cavernous sinus are the oculo-motor, trochlear, ophthalmic, and abducens nerves, and thesympathetic plexus around the intracavernous carotid artery(►Fig. 2). The nerves in the sinus wall or sinus are, fromsuperior to inferior, the third cranial nerve followed by thetrochlear, ophthalmic, and abducens nerves. The oculomotor,trochlear, and ophthalmic nerves course along the inner partof the lateral sinus wall. The abducens nerve and the sympa-thetic plexus around the intracavernous carotid artery are theonly nerves that have a purely intracavernous course.1–10
The oculomotor nerve courses along the lower edge of theanterior clinoid process to enter the superior orbital fissure.The trochlear nerve enters the roof of the sinus posterolateralto the third nerve and courses below the oculomotor nerve inthe posterior part of the lateral wall. The ophthalmic nerve(the first and smallest trigeminal division) is embeddedwithin the inner layer of the lateral wall of the cavernoussinus together with the oculomotor and trochlear nerves.
Fig. 1 (A and B) Osseous relationship in the central base of the skull;(C and D) dural and cranial nerve relationships in the base of the skull.The blue circle shows the position of the cavernous sinus, and the bluearrow indicates the Grubber ligament. Abbreviations: ACP, anteriorclinoid process; AN, abducens nerve; C, clivus; CA, carotid artery; CI,carotid impression; DS, dorsum sellae; IAC, internal acoustic channel;IAM, internal acustic meatus; JF, jugular foramen; OC, optic channel;OcN, oculomotor nerve; ON, optic nerve; OS, optic strut; PS, planumsphenoidale; S, sella; SOF, superior orbital fissure; TN, trochlear nerve;TS, tuberculum sphenoidale.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Endoscopic and Microsurgical Approaches to the Cavernous Sinus – Anatomical Review Romero et al. 161

Themaxillary nerve (the second trigeminal division) coursesbelowand does not belong to the lateralwall of the cavernoussinus. The cavernous sinus ends just above the superiormargin of the maxillary nerve.1–3,7–10 The abducens nerveand the sympathetic plexus around the intracavernous car-otid artery are the only nerves that have a purely intraca-vernous course (►Fig. 2).7–10
The intracavernous carotid artery has five parts and twomain branches. The five divisions are the posterior verticalsegment, the posterior bend, the horizontal segment, theanterior bend, and the anterior vertical segment. The firstbranch, the meningohypophyseal trunk, arises from the pos-terior bend originating from the posterior bend of the intra-cavernous carotid artery and has three divisions: the dorsalmeningeal artery, the inferior hypophyseal artery and thetentorial artery (artery of Bernasconi-Cassinari). The secondbranch, the inferolateral trunk, also called the artery of theinferior cavernous sinus, arises from the horizontal segmentand nearly always passes above the abducens nerve and thendownward between the abducens and ophthalmic nerves tosupply the dura of the inferolateralwall of the cavernous sinusand adjacent area around the foramen rotundumand ovale.1–4
Microsurgical Approaches to the CavernousSinus
Parkinson, Dolenc and other neurosurgeons have describedapproaches to the cavernous sinus in published papers withfew patients because of the risks and difficulty.8,11 This lack of
information was largely a result of the inability in the pre-microsurgical era to effectively address the extreme risks ofsignificant hemorrhage and damage to the cranial nerves in theregion. The modern era of microscopic neurosurgery has en-abled expanded capabilities in surgical technique and hasfostered the work of several neurosurgeons who have madegreat strides in effectively approaching this regionwith reducedmorbidity.8–11 Moreover, new forms of therapy such as radio-surgery have been used, despite the controversial results.12
The indications for the surgical treatment of neoplasticlesions arising in or involving the cavernous sinus are con-troversial.8,11,12 The presence of a mass in the cavernoussinus, of course, does not itself constitute an absolute in-dication for a direct operation. Many variables must be takeninto account, including the age and medical condition of thepatient, the imaging characteristics, the adjacent structuresinvolved, the time course of the process, and the functionalseverity of the symptoms.12–14
Very important to the surgeon’s understanding of therelevant surgical anatomy of the cavernous sinus is a thor-ough working knowledge of the multiple triangular entrycorridors into the region. Surgical facility with cavernoussinus lesions requires intimate knowledge of the entryspaces into the cavernous sinus to minimize morbidity.Some middle fossae triangles were described as possibleentry corridors to the cavernous sinus (►Fig. 3).1,2,11,12,14,15
The anterior triangle is exposed by removing the anteriorclinoid process, either intradurally or extradurally. Thebound-aries of the triangle are the extradural optic nerve, the fibrous
Fig. 2 Cavernous sinus structures after dural removal, in posteroanterior view (A); lateral view (B); oblique view (C); and anterior view (D).Abbreviations: ICA, internal carotid artery; OcN, oculomotor nerve; ON, optic nerve; PS, planum sphenoidale; TN, trochlear nerve; V1,ophthalmic portion of the trigeminal nerve; V2, mandibular portion of the trigeminal nerve.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Endoscopic and Microsurgical Approaches to the Cavernous Sinus – Anatomical Review Romero et al.162

dural ring, and the medial wall of the superior orbital fissure.The intradural carotid artery, the posterior clinoid process, theporus oculomotorius, and the siphon angle of the carotidartery delimit the medial triangle. This space is also criticalin terms of exposure for most intracavernous tumors. Thesuperior triangle is bounded by the oculomotor and trochlearnerves medially and laterally, and by the dura along thepetrous ridge posteriorly. This triangle is the entry corridorused to locate the meningohypophyseal trunk.16–19
The lateral triangle is a very narrow space that is delimitedby the trochlear nerve medially and by the ophthalmicdivision of the trigeminal nerve laterally, and the dura ofthe petrous ridge forms the posterior margin.16,17 The pos-terolateral triangle, first described by Glasscock in 1968,describes the location of the horizontal intrapetrous carotidartery, and is defined by the foramen ovale, the foramenspinosum, the posterior border of the mandibular division ofthe trigeminal nerve, and the cochlear apex. The poster-omedial triangle, first described by Kawase, allows awindowinto the petrous apex to the posterior fossa.16–19 The poster-oinferior triangle is defined by the porus trigeminus, theposterior clinoid, and the entrance to the Dorello canal. Anincision in this area exposes the petrosphenoidal ligament(Gruber ligament), which forms the roof of the Dorello canal.The anterolateral triangle is defined by the area between thefirst and second divisions of the trigeminal nerve in their exitin the middle cranial fossa.16–18
The cavernous sinus can be divided into four separatequadrants. Lesions involving the anteromedial region areapproached via the anteromedial and anterolateral triangles.Because these two triangles are exposed extradurally, inselected cases (such as neurinoma of themandibular portion
of the trigeminal nerve [V2], for example), opening the duramater might not be necessary in the resection of such alesion. This concept similarly applies to lesions located in theanterolateral quadrant, approached via the lateral loop andposterolateral triangles.12–21
More posterior lesions, involving the posteromedial andposterolateral regions of the cavernous sinus, usually requireexposure through the medial, superior, and lateral triangles.These triangles, although possible to open through an extra-dural route, are typically entered intradurally. Posteromediallesions without extension lateral to the cavernous carotidartery may also be considered for an endonasal endoscopicapproach.17–19 Masses confined mainly to the posterolateralquadrant of the region are best approached laterally throughthe middle fossa in our opinion. Lesions involving more thanone of these four areas, such as a mass with extensiveposterior cavernous involvement with extension into theposterior fossa, for example, may require a combined ap-proach for adequate exposure.17–19
Case 1
A 56 year-old male was admitted with history of headacheand diplopia. A neurological examination showed left
Fig. 3 Microsurgical cavernous sinus view and its relationships. Abbre-viations: CS, cavernous sinus; dr, dural ring; FR, foramen rotundum; FO,foramen ovale; ICA, internal carotid artery; ON, optic nerve; SOF, superiororbital fissure; SS, sphenoidal sinus; V, trigeminal nerve; V1, ophthalmicportion of the trigeminal nerve; V2, mandibular portion of the trigeminalnerve; V3;.III, oculomotor nerve; IV, troclear nerve, VI, abducens nerve.Notes: �optic strut; blue – anterior triangle; red – medial triangle; green –lateral triangle; purple – posteroinferior triangle; yellow – anterolateraltriangle; black – far lateral triangle.
Fig. 4 Example of a case of cavernous sinus meningioma treated bymicrosurgical extra- and intradural approaches. (A) Preoperativemagnetic resonance imaging (MRI) showing a left cavernous sinusextra-axial lesion extending to the medial fossa; (B) extradural ap-proach drilling the anterior clinoid process; (C) intradural dissection ofthe temporal lobe (TL) and tumor capsule (Tu); (D) dissection of thetumor from the lateral wall of the cavernous sinus; (E) after tumorresection, showing the preservation of the neural and vascularstructures; (F) postoperative MRI.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Endoscopic and Microsurgical Approaches to the Cavernous Sinus – Anatomical Review Romero et al. 163

oculomotor and trochlear palsies. A computed tomography(CT) scan and magnetic resonance imaging (MRI) (►Fig. 4)were performed with left cavernous homogeneous lesionwith middle fossae extension and intracavernous carotidartery stenosis. He was submitted to left fronto-temporalcraniotomy and middle fossae peeling with subtotal tumorresection through the lateral, antero-lateral and far-lateraltriangles. He was discharged ten days after surgery withworse ocular palsy anatomopathologicaly compatible withmeningotelial meningioma (World Health Organization[WHO] grade 1). Therefore, adjuvant radiation therapy wasindicated. After nine months, he had an improvement in theocular palsy, and an MRI showed no tumor growing rates.
Endoscopic Approaches to the CavernousSinus
Medial lesions may be considered for the endonasal endo-scopic approach and lateral lesions bymiddle fossa.14,19,21–24
The introduction of the endoscope in pituitary surgeryenabled a wide peripheral vision through a limited surgicalchannel and an adequate lateral control of the cavernoussinus region. The results attained in the treatment of pitui-tary adenomas, fistula correction and the development ofspecific technology to improve hemostasis pushed us toapply endoscopic endonasal surgery to the treatment ofcavernous sinus tumors.22,23
Multiple endoscopic endonasal surgical corridors to thecavernous sinus have been described, giving access to themedial and lateral compartments (relative to the position ofthe intracavernous internal carotid artery).24–26 The choiceof approach is based on the grade, type and location of thelesions in the cavernous sinus. Lesions confined to themedialand postero-superior compartments are treated by a trans-sphenoidal transselar transcavernous (TTT) endoscopicapproach. When the lesion is located in the lateral orantero-inferior compartments, an endoscopic ethmoid-pter-ygoid-sphenoidal (EPS) approach is required.22,23
The TTT endoscopic approach is initiated using a 0° rodlens endoscope. The lateralization of the inferior turbinatesincreases the space for the insertion andmanipulation of theinstruments. First, a nasoseptal flap is prepared for recon-struction of the skull base defect at the end of the procedure.A posterior nasal septectomy in addition to wide bilateralsphenoidotomies and posterior ethmoidectomies completethe nasal corridor. The anterior wall of the sella is drilled out,exposing the superior and inferior intercavernous sinuses
Fig. 5 Endoscopic view of the transsphenoidal and transpterygoidapproaches. (A) transsphenoidal approach in a cadaveric specimen;(B) transsphenoidal approach; (C) transpterygoid approach; (D)transpterygoid approach showing the left cavernous sinus after tumorresection. Abbreviations: ACP, anterior clinoid process; CC, cavernouscarotid artery; DDR, distal dural ring; OS, optic sheet; PDR, proximaldural ring; PG, pituitary gland impression; TS, tuberculum sellae.Note: the yellow circle shows the position of the cavernous sinus.
Fig. 6 (A) Axial preoperative T1-enhanced MRI of a pituitary tumorwith extension to the left cavernous sinus; (B) coronal preoperative ofa T2 MRI; (C) axial T2 MRI; (D) coronal preoperative T2 MRI; (E) axial 6moths postoperative MRI; (F) axial 6 months postoperative MRI.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Endoscopic and Microsurgical Approaches to the Cavernous Sinus – Anatomical Review Romero et al.164

and the cavernous sinus bilaterally. This relatively wideexposure, coupled with an incision of the dura, enables anunencumbered intrasellar dissection. The most commonindications for this approach are pituitary tumors extendingto the medial compartment of the cavernous sinus(►Fig. 5).22–30
The EPS approach enables the frontal view of the caver-nous sinus with direct control of the medial and lateralcompartments. The procedure starts with an ethmoidect-omy with partial resection of the middle and superiorturbinates. Then, opening the posterior ethmoidal cellsenables the exposure of the anterior wall of sphenoid sinus,the orbital apex and the base of the pterygoid. The anteriorwall of the sphenoid sinus is removed, and the sphenopala-tine artery is cauterized using a bipolar forceps. At this point,the posterior wall of the maxillary sinus is exposed by amedial maxillectomy in the area of the middle and posteriorthirds of the inferior turbinate, opening the pterygomaxil-lary fossae. After the removal of the posterior wall of themaxillary sinus, the contents of pterygomaxillary and infra-temporal fossae are visible. Then, the vidian artery is cauter-ized, and the base of the pterygoid process and thesphenoidal sinus floor are drilled out. Thismaneuver enablesthe visualization of the cavernous sinus and middle cranialfossae. In cases in which lateral inspection is needed, a totalmaxillectomy may be performed with this approach. More-over, the procedure comprises a wide contralateral trans-sphenoidal approach. With the exception of the tumorexclusively located in the lateral portion of the cavernoussinus, dural opening is made in the sellar region, and isprogressively enlarged following the lesion from the medialto the lateral portions (►Fig. 5).22–30
Closure is performed with fat, fascia lata, nasoseptal flapand dura mater sealants. The external lumbar drain is notused unless an intraoperative high-flow leakof cerebrospinalfluid (CSF) is observed.
Case 2
A 31 year-old female was admitted at the emergency roomwith headache, visual disturbances characterized by lefttemporal hemianopsia, diplopia and strabismus. She had aprevious transsphenoidal surgery for the treatment of apituitary tumor in 2011. Upon neurological examination,she had complete left third nerve palsy and incompletedeficits in the fourth and sixth nerves. An MRI showed aresidual pituitary tumor with an extension to the left of thecavernous sinus (►Fig. 6). Hormonal screening showed pan-hypopituitarism. She was submitted to an extended endo-scopic endonasal transsphenoidal transpterygoid approachto the tumor (►Fig. 7). After five days, she was discharged ingood health condition, with complete recovery of the fourthand sixth nerve palsies and improvement of third nervedeficit and left temporal hemianopsia. At six months fol-low-up, she had a complete recovery of the visual distur-bances, but an MRI showed a small residual tumor (►Fig. 6E
and 6F). Conservative treatment was indicated with a newMRI in three months.
Conclusion
Cavernous sinus lesions are challenging, with high surgicalrisks. Extensive microsurgical anatomical knowledge andendoscopic skills are required to choose the best treatmentand surgical approach. The microsurgical and endoscopicapproaches have specific indications based on the position ofthe lesion and the skills of the surgeon.
References1 Yasuda A, Campero A, Martins C, Rhoton AL Jr, de Oliveira E, Ribas
GC. Microsurgical anatomy and approaches to the cavernoussinus. Neurosurgery 2005;56(1, Suppl)4–27, discussion 4–27
2 Rhoton AL Jr. The supratentorial cranial space: Microsurgical anat-omy and surgical approaches. Neurosurgery 2002;51(Suppl 1):375–410
Fig. 7 Endoscopic approach to the tumor in the sellar regionextending to left cavernous sinus. (A) Endoscopic transsphenoidalview of the anatomy of the base of the skull; (B) endoscopictranspterygoid view of the lateral left cavernous region and itsrelationships; (C) view of the sellae after intrasellar tumor resection;(D) opening the dura anteriorly to the cavernous sinus; (E) View intocavernous sinus during tumor resection; (F) view after tumor resec-tion. Abbreviations: CA, carotid artery; DS, diaphragm sella; PG,pituitary gland.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Endoscopic and Microsurgical Approaches to the Cavernous Sinus – Anatomical Review Romero et al. 165

3 Sekhar LN, Burgess J, Akin O. Anatomical study of the cavernoussinus emphasizing operative approaches and related vascular andneural reconstruction. Neurosurgery 1987;21(06):806–816
4 Parkinson D. The cavernous sinus, in Dolenc VV (ed): The Caver-nous Sinus. New York: Springer-Verlag; 1987, pp 3–29
5 Harris FS, Rhoton AL Jr. Anatomy of the cavernous sinus. A micro-surgical study. J Neurosurg 1976;45(02):169–180
6 Glasscock ME III. Exposure of intrapetrous portion of the internalcarotid artery, inHamburgerCA,Wersall J (eds):Disorders of theSkullBase Region: Proceedings of the Tenth Nobel Symposium, Stockholm,1968. Stockholm, Almquist and Wiksel, 1969, pp 135–143.
7 Romero FR, Ramos JG, Chaddad-Neto F, Bethencourt JM, deOliveira E. Microsurgical anatomy and injuries of the abducensnerve. Arq Neuropsiquiatr 2009;67(01):96–101
8 Tedeschi H, de Oliveira EP, Wen HT, Rhoton AL Jr. Perspectives onthe approaches to lesions in and around the cavernous sinus. OperTech Neurosurg 2001;4:82–107
9 Umansky F, Valarezo A, Elidan J. The superior wall of the caver-nous sinus: a microanatomical study. J Neurosurg 1994;81(06):914–920
10 Yasuda A, Campero A, Martins C, Rhoton AL Jr, Ribas GC. Themedial wall of the cavernous sinus: microsurgical anatomy.Neurosurgery 2004;55(01):179–189, discussion 189–190
11 Sekhar LN,Møller AR. Operativemanagement of tumors involvingthe cavernous sinus. J Neurosurg 1986;64(06):879–889
12 Alfieri A, Jho HD. Endoscopic endonasal cavernous sinus surgery:an anatomic study. Neurosurgery 2001;48(04):827–836, discus-sion 836–837
13 Cusimano MD, Sekhar LN, Sen CN, et al. The results of surgery forbenign tumors of the cavernous sinus. Neurosurgery 1995;37(01):1–9, discussion 9–10
14 Arbolay OL, González JG, González RH, Gálvez YH. Extendedendoscopic endonasal approach to the skull base. Minim InvasiveNeurosurg 2009;52(03):114–118
15 Cavallo LM, Cappabianca P, Galzio R, Iaconetta G, de Divitiis E,Tschabitscher M. Endoscopic transnasal approach to the caver-nous sinus versus transcranial route: anatomic study. Neurosur-gery 2005;56(2, Suppl)379–389, discussion 379–389
16 DeMonte F, SmithHK, al-MeftyO.Outcomeofaggressive removal ofcavernous sinus meningiomas. J Neurosurg 1994;81(02):245–251
17 Isolan GR, Krayenbühl N, de Oliveira E, Al-Mefty O. MicrosurgicalAnatomy of the Cavernous Sinus: Measurements of the Trianglesin and around It. Skull Base 2007;17(06):357–367
18 Isolan G, de Oliveira E, Mattos JP. Microsurgical anatomy of thearterial compartment of the cavernous sinus: analysis of 24cavernous sinus. Arq Neuropsiquiatr 2005;63(2A):259–264
19 Jho HD, Ha HG. Endoscopic endonasal skull base surgery: Part 2–The cavernous sinus. Minim Invasive Neurosurg 2004;47(01):9–15
20 Eisenberg MB, Al-Mefty O, DeMonte F, Burson GT. Benign non-meningeal tumors of the cavernous sinus. Neurosurgery 1999;44(05):949–954, discussion 954–955
21 Frank G, Pasquini E. Endoscopic endonasal cavernous sinus sur-gery, with special reference to pituitary adenomas. Front HormRes 2006;34:64–82
22 Kassam AB, Gardner P, Snyderman C, Mintz A, Carrau R. Expandedendonasal approach: fully endoscopic, completely transnasalapproach to the middle third of the clivus, petrous bone, middlecranial fossa, and infratemporal fossa. Neurosurg Focus 2005;19(01):E6
23 Kassam AB, Prevedello DM, Carrau RL, et al. The front door tomeckel’s cave: an anteromedial corridor via expanded endo-scopic endonasal approach- technical considerations and clin-ical series. Neurosurgery 2009;64(3, Suppl)ons71–ons82,discussion ons82–ons83
24 Zhao B, Wei YK, Li GL, et al. Extended transsphenoidalapproach for pituitary adenomas invading the anterior cranialbase, cavernous sinus, and clivus: a single-center experiencewith 126 consecutive cases. J Neurosurg 2010;112(01):108–117
25 Woodworth GF, Patel KS, Shin B, et al. Surgical outcomes using amedial-to-lateral endonasal endoscopic approach to pituitaryadenomas invading the cavernous sinus. J Neurosurg 2014;120(05):1086–1094
26 Nishioka H, Fukuhara N, Horiguchi K, Yamada S. Aggressivetranssphenoidal resection of tumors invading the cavernous sinusin patients with acromegaly: predictive factors, strategies, andoutcomes. J Neurosurg 2014;121(03):505–510
27 Ceylan S, Koc K, Anik I. Endoscopic endonasal transsphenoidalapproach for pituitary adenomas invading the cavernous sinus.J Neurosurg 2010;112(01):99–107
28 Cappabianca P, Cavallo LM, Esposito F, De Divitiis O, Messina A, DeDivitiis E. Extended endoscopic endonasal approach to the mid-line skull base: the evolving role of transsphenoidal surgery. AdvTech Stand Neurosurg 2008;33:151–199
29 Inoue T, Rhoton AL Jr, Theele D, Barry ME. Surgical approaches tothe cavernous sinus: a microsurgical study. Neurosurgery 1990;26(06):903–932
30 de Divitiis O, Conti A, Angileri FF, Cardali S, La Torre D, Tscha-bitscher M. Endoscopic transoral-transclival approach to thebrainstem and surrounding cisternal space: anatomic study.Neurosurgery 2004;54(01):125–130, discussion 130
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Endoscopic and Microsurgical Approaches to the Cavernous Sinus – Anatomical Review Romero et al.166

Paraspinal Lumbar Spine Approach - Wiltse Access
Abordagem paravertebral da coluna lombar - acesso deWiltse
Nícollas Nunes Rabelo1 Bruno Nascimento Bettencourt da Silva1 Luciano José Silveira Filho1
George Santos dos Passos1 Vitor Hugo Honorato Pereira1 Luiz Antônio Araujo Dias Junior1
Luiz Antônio Araujo Dias1 Koji Tanaka1
1Department of Neurosurgery, Hospital da Santa Casa de RibeirãoPreto, Ribeirão Preto, SP, Brazil
Arq Bras Neurocir 2017;36:167–171.
Address for correspondence Nícollas Nunes Rabelo, MD, Av. AntonioDiederichsen, n. 190, apt. 193, Jardim América, CEP: 14020-250,Ribeirão Preto, SP, Brazil (e-mail: [email protected]).
Keywords
► Wiltse access► lumbar spine► paraspinal approach► spine surgery
Abstract Introduction Technical developments in spinal surgery have reduced the number ofsurgical incisions and of the length of time for the procedure.Objective Describe topographical landmarks, anatomy and characteristics of theWiltse access, a paraspinal approach to the lumbar spine.Methods A review of the literature was performed using as databases: PubMed,Embase, Science Direct, the Cochran Database and Google Scholar. Total 22 papersmetthe inclusion criteria, and they were all published between 1959 and 2016.Discussion The Wiltse approach is performed by median skin incision with lateralmuscle dissection between the multifidus and the longissimus muscles, in a naturalpathway. This approach allows access to the pedicles and to the lateral recess, enablingthe performance of posterior spinal fusion and decompression and minimally invasivediscectomy techniques. This access is less traumatic than the median approach, and itis ideal for lower levels, like L4–5 and L5-S1.Conclusion The authors strongly encourage this approach because they believe that,when well-indicated, the benefits outweigh the disadvantages and complications dueto the fact that it is a less invasive procedure.
Resumo Introdução Os desenvolvimentos técnicos na cirurgia da coluna vertebral têmproporcionado a redução das incisões cirúrgicas e da duração do procedimento.Objetivo Descrever marcos topográficos, anatômicos e características do acesso deWiltse, uma abordagem da coluna vertebral lombar.Métodos A revisão bibliográfica foi realizada utilizando como banco de dados:PubMed, Embase, Science Direct, banco de dados Cochran e Google Scholar. Foramencontrados 22 trabalhos que atenderam aos critérios de inclusão, todos publicadosentre 1959 e 2016.Discussão A abordagem de Wiltse é realizada pela incisão cutânea mediana comdissecção muscular lateral entre o músculo multifidus e o músculo longissimus, na via
receivedFebruary 5, 2017acceptedMay 9, 2017published onlineJuly 12, 2017
DOI https://doi.org/10.1055/s-0037-1604267.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Review Article | Artigo de Revisão 167

Introduction
Different approach methods to spinal surgery have beendeveloped to reduce the aggressiveness of the current surgi-cal approach.
Authors like Mathieu and Dermirleau, in 1936, describedone technique in which the spine access to the sacrospinousmuscle was lateral. In their approach, a hole was drilledthrough the ilium, and an iliac graft was driven through thishole to engage the transverse process of L5. Watkins, in 1953,first described an approach that was lateral to the sacrospi-nalis. In this approach, he took a thinflake of bone off the iliumwith the entire sacrospinalis group of muscles attached. Thus,the iliocostalis, the longissimus, and part of the multifiduscould be retracted upward and medially, out of way. Ray4
describeda far lateral approach tothespine,whichhecalls “theparalateral approach”., LikeWatkins’approach, itwas lateral toall three muscles of the sacrospinalis group between theiliocostalis and the quadratus lumborum. In this approach,the muscles are split, differing from Watkins’ approach, inwhich a flake of bone is left attached at its medical end, and isturned cranially andmedially. If, at the L5 level, the crest of theilium is in theway, Ray recommends the removal of bone fromthe posterior iliac spine as necessary.1–4
The paravertebral approach, initially described by LeonWiltse in California in 1968 as two paramedian skin incisionsand then, posteriorly, a single median incision, is a surgicalapproach that results in less tissue injury, and that hasprovided a postoperative outcome with less pain, less bleed-ing and less damage to the muscles. These lower morbiditycharacteristics of theWiltse approach stand as an alternativeto the large incisions used in the past, allowing better resultsin surgery of the lumbar spine.4
The purpose of this review is to describe the topographicallandmarks, anatomy and characteristics of theWiltse access,a paraspinal approach to the lumbar spine.
Material and Methods
Weperformeda reviewof theliteratureusingPubMed, ScienceDirect, Embase, Clinical Trials, Ebsco, and Scielo databases.Weselected articles from the period between 1959 and 2016.There were total 22 papers that met the inclusion criteria.These were studies that described the original technique oflateral access to the posterior spine, by Wiltse, and comparedthe midline and paraspinal posterior approaches.
Technique
This spine posterolateral approachwithmidline skin incisioncreates a wall along the sacrospinalis muscle. This anatomi-cal avascular space lies between the multifidus (medial) andthe longissimus (lateral) muscles.5,6
The procedurewas initially describedwith two cutaneousincisions located at 30 mm from the spinous processes toallow direct access to the osseous structures. But, in 1988,Wiltse extended the indications of this approach, and rec-ommended that a single median incision be performed.7
The surgery should be performed with the patient inprone position, with cushions under the pelvis and thorax,and with the table flexed, but this is a matter of individualpreference, as long as preservation of physiological lumbarlordosis is maintained during the procedure.8
The correct level is localized by fluoroscopy prior toincision. A median longitudinal skin incision is performedin the midline, followed by two longitudinal incisions in themuscular aponeurosis, in general 1.5–2 cm from themidline.One central skin incision is more cosmetically desirable thantwo lateral incisions or even a transverse incision. A finger-breadth dissection is made between the multifidus and thelongissimusmuscles laterally on either side. A retractor, suchas a gelpi, and suture on the bilateral multifidus can be usedto facilitate the visualization (►Fig. 1).9
There is a natural cleavage plane between the multifidusand the longissimusmuscles, anaturalpathway.Afingercanbeinserted between these muscles at any point at or above thespecific level.At thesacral level, themultifidusswings laterally,but it is amuchbloodierapproach,andthere ismuscular strain.The thoracic levels are already very thin10 (►Fig. 2).
Little blood loss may occur. For bestter exposure, the gelpiretractors need to be repositioned frequently. Extra softtissue in the bottom of the wound is removed. The laminaeof the vertebrae to be fused are exposed well up onto thesloping basis of the adjacent spinous process. The lumbartransverse processes should also be denuded of soft tissue allthe way up to their tips and well around their superior andinferior borders, for the visualization of anatomical land-marks like the pedicle and facet joint.11
We never place bone in front of the transverse processes.The spinal nerves are just in front of the transverse processes,and may be injured if the exposure is continued aroundanteriorly. Injury to these nerves is a lot more likely if bone ispacked in this area. There seems to be little danger of
natural. Esta abordagem permite o acesso aos pedículos e ao recesso lateral, e arealização de fusão posterior e descompressão de fratura da coluna vertebral e técnicasde discectomia minimamente invasivas. Este acesso é menos traumático do que aabordagem mediana, e é ideal para níveis mais baixos, como L4–5 e L5-S1.Conclusão Os autores recomendam esta abordagem, pois acreditam que os bene-fícios desta técnica, quando bem indicada, superam as desvantagens e complicaçõespor ser esta menos invasiva.
Palavras-chaves
► acesso de Wiltse► coluna lombar► abordagem
paraespinhal► cirurgia da coluna
vertebral
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Paraspinal Lumbar Spine Approach - Wiltse Access Rabelo et al.168

damaging the spinal nerves if the dissection is kept posteriorto the transverse processes, preserving the medial branch ofthe dorsal nerve. The lumbar arteries and veins pass justabove the basis of the transverse processes and also at theangle of the medial point of the sacral spine. These oftenbleed profusely, and the bleeding can be difficult to stopwithcautery. These bleeding areas can be plugged with a wad ofsurgicel (Ethicon, Sommerville, NJ, US). The vessels comingout of the superior sacral foramen may also bleed profusely,and the bleeding can also be stopped with surgicel.11
The surgicel can be removed before closing; however, noharm is done if a small wad of surgicel is left inadvertently. Ifone is to use cautery at this point, it should be thebipolar type,as unipolar cautery may damage the adjacent spinal nerve.Particular care should be taken not to remove the capsule ordamage theadjacent jointat this level, andtopreserve thefacetjoint; neither should thesurgeonexposeanypartof the laminaof the vertebra immediately above the area to be fused. Withthese precautions taken, any tendency of the fusion to extendupward will be avoided since there will be no instability.Incidentally, we also believe that damage to these facets mayaccount for some of the cases of spondylolisthesis and otherproblemsseenasyearsgobyat theupperends of thefusions.12
Often times, there are not more than a few centimeters ofarea available for fusion, but every bit of that area should beused. Not only the lateral surfaces of the superior articularprocess, but the dorsal and lateral areas of the pars interarti-cularis should also be denuded. The laminae, as farmedially asthebases of the spinousprocesses themselves are not exposed,thereby preserving their ligamentous attachments and someof their blood supply. Preservation of thesemidline structuresand maintenance of adequate circulation and innervation arethe main advantages of this approach.12
Fig. 2 (A) The finger can be plunged between multifidus and thelongissimus muscle creating one natural wall. Sacroespinalis is thename of the complex of longissimus, iliocostalis and sacroespinales.(B) Two retractors can be used to expose facet joint and pedicule. 1- M.(muscle) Longissimus, 2- M. Iliocostalis, 3- M. Sacroespinalis, 4- M.Psoas Major, 5 - Multifidus, * - Pedicle, Black arrow - Facet joint.
Fig. 1 (A) Patient in prone position, with support on the face, chest, abdomen and lower limbs. (B) Posterolateral approach with midlinelongitudinal skin incision, followed by 2 longitudinal incisions in muscular aponeurosis, in general, 1.5–2 cm from the midline.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Paraspinal Lumbar Spine Approach - Wiltse Access Rabelo et al. 169

The intervertebral joints within the fusion area areexposed carefully. If the surgeon wishes, the posteriortwo-thirds of the joint cartilage can be removed. In thecase of spondylolisthesis loose element, this cartilagejoint should not be removed because this further destabil-izes an already unstable area. In spondylolisthesis, alwaysfuse the loose element to S1, since this loose element mayrock about with the muscle contractions. Thus, it shouldbe prepared with a rongeur. Never use a hammer and gouge,as they have been known to damage the underlyingnerves.11
Before closure, any small tags of muscle are snipped off.The muscle itself is closed extremely loosely with smallsutures. The fascia is closed securely.11,12
It is important to suture the skin edges to the underlyingdeep fascia, or blood and serumwill collect under the portionof skin that has been undermined, and the area will balloonout. If this occurs, the blood and serum may need to beaspirated.11
The far lateral zone is defined as that area lateral to thepedicles. This is difficult to approach from the midline, buteasily reached through a paraspinal approach. The laminaedo not need to be exposed if the rupture is lateral to thepedicles. Themedial half or two-thirds of the intertransversemuscle and ligament are removed.7,8,13
Discussion
TheWiltse approach allows further instrumented fusion anddecompressionwithminimal trauma, accurate identificationof the natural cleavage plane between the multifidus andlongissimus muscles, and reduced postoperative morbidity(►Fig. 1). When using the Wiltse approach, we recommendperforming: a preoperative magnetic resonance imaging(MRI) to plan the distance in skin incisions from the midlineto each vertebral level; a computed tomography (CT) of thespine to evaluate bone viability; and dynamic bending andlateral radiographs to assess the mobility of the spaces to bemanipulated during surgery.11
Benefits14–17
(1) Reduced chronic low back pain after surgery, with lessmuscle manipulation.
(2) Reduces intraoperative damage due to the developmentof access roads and minimally invasive and less trau-matic discectomy techniques.
(3) Multifidus muscle preservation, vascularization andtissue innervation; optimal exposure of the pedicledoes not require specific instruments.
(4) Reduced length of surgical time.(5) It enables the removal of bone graft in the same incision,
needs little traction, and causes less muscle ischemiawhile also providing accessibility to extraforaminal andlateral recess disc herniations.
(6) The supra and interspinous ligaments are left intact,with less postoperative pain, no dead space, and lowincidence of infection;
(7) This approach is used for the classical herniated discextraforaminal and lateral recess channel;
(8) This approach is extremely useful for putting in pedi-cle screws since it makes aiming the screws mediallyvery easy;
(9) Through this approach the surgeon has freer access tolaterally placed structures, and hence can decompressthe nerves more easily than he can through the midlineapproach;
(10) Vigorous retraction is not necessary, and hence there isless muscle ischemia;
(11) Preservation of the nerve of the medial dorsal branchand its transverse spinal and interspinal branches, withsuperior and inferior anastomosis.
(12) Useful for interbody fusion surgeries, like posteriorlumbar interbody fusion (PLIF) and transforaminal lum-bar interbody fusion (TLIF)
(13) It can be useful for the correction of small deformities,but in more serious cases, it is sometimes necessary toutilize techniques like osteotomy, which can introducemore difficulties to the surgeon.
Disadvantages14
(1) Familiarity with the surgical approach is required;(2) Poor visibility;(3) Difficulty to enucleate the intervertebral disc and risk of
root injury;(4) Tendency to lateralization at the point of entry;(5) Necessity to complement with another access if dural
access is required.(6) It can be performed at thoracic levels, but more experi-
ence and familiarity with the anatomy are required. Themultifidus muscle becomes thinner with each upwardsegment, giving the surgeon a greater chance of differen-tiating his laterality, but this represents a slightly greatertechnical difficulty. We recommend levels below T7/T8,despite the fact that the multifidus extends from thesacrum to the axis. In fact, low lumbar levels can be verythick and hamper the approach.
Complications17,18
Some of the complications related to this surgical techniquecan be: infection, hematoma, loosening or breakage theimplants, kyphosis and facet dislocation, and pain disability.However, these complications are common to all surgeries.
Postoperative RecommendationsThe patients submitted to this access are instructed toremain supine for 24 hours, after which they are allowedto sit on the bed. The mean time of the hospital stay is threedays. Prophylactic antibiotics and analgesia are commonlyused. After three days, kinesiotherapy is started, and thepatient can resume his/her daily activities. Rehabilitationstarts in the second postoperative month, with exercisescontrolled by the physiotherapist. After the third month, thepatient is referred to aerobics to start a supervised muscularrecovery program.19,20
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Paraspinal Lumbar Spine Approach - Wiltse Access Rabelo et al.170

Comparison between the Midline and theMuscle-splitting Approaches
Street and colleagues established, in 2016, with a retrospec-tive study, that patients who underwent surgery performedwith the paraspinal approach of Wiltse had decreased riskof wound breakdown and infection, reduced blood loss,and fewer reoperations than the patients submitted tothe midline approach. The risk of adjacent segment failurein short posterior constructs is also lower with the Wiltseapproach.20,21
Mukai and colleagues, in 2013, made a randomized studythat was designed to elucidate the time course of theperioperative development of intramuscular multifidusmuscle pressure after interfusion body surgery with midlinedissectionWiltse approach resultant in low-back pain; how-ever, pain did not differ between the 2 groups.22
Buttermann and colleagues, in 2015, mentioned that themidline and paraspinal approaches result in similar out-comes in two-level spinal fusions. They were unable todemonstrate that a paraspinal muscle-splitting approachto two-level fusions was superior to the muscle-strippingmidline approach, or that the Wiltse approach was superiorto the midline approach. However, the study had low statis-tical power.22
Conclusion
The paraspinal approach to the lumbar spine was described40 years ago bymedian skin incisionwith lateralmuscle dissec-tion between themultifidus and longissimus muscles, in natu-ral pathway. A low rate of surgical complications such asinfections,bleedingandpostoperativepainhavebeenobserved,as well as good anatomy dissection to access the pedicle/facetjoint, with less tissue damage and less tissue ischemia.
Even though some papers have controversies regardingthe indications, the authors strongly encourage this ap-proach, as they believe that, when well-indicated, the bene-fits outweigh the disadvantages and complications because itis a less invasive procedure.
References1 Watkins MB. Posterolateral bonegrafting for fusion of the lumbar
and lumbosacral spine. J Bone Joint Surg Am 1959;41-A(03):388–396
2 Mathieu P, Demirleau J. Surgical Therapy in painful spondylolisth-esis. Rev Chir Orthop Repar Appar Mot 1936;23:352
3 Watkins MB. Posterolateral fusion in pseudarthrosis and poster-ior element defects of the lumbosacral spine. Clin Orthop RelatRes 1964;35(35):80–85
4 Ray CD. The paralateral approach to decompression for lateralstenosis and far lateral lesions of the lumbar spine. Chapter 29.Lumbar Discectomy and Laminectomy. Edited by Watkins.Collins, Aspen Publishers; 1987:217–227
5 Wiltse LL, Hutchinson RH. Surgical treatment of spondylolisth-esis. Clin Orthop Relat Res 1964;35(35):116–135
6 Wiltse LL. The paraspinal sacrospinalis-splitting approach to thelumbar spine. Clin Orthop Relat Res 1973;(91):48–57
7 Wiltse LL, Spencer CW. New uses and refinements of the para-spinal approach to the lumbar spine. Spine 1988;13(06):696–706
8 Wiltse LL, Bateman JG, Hutchinson RH, NelsonWE. The paraspinalsacrospinalis-splitting approach to the lumbar spine. J Bone JointSurg Am 1968;50(05):919–926
9 Wiltse LL, Guyer RD, Spencer CW, Glenn WV, Porter IS. Alartransverse process impingement of the L5 spinal nerve: the far-out syndrome. Spine 1984;9(01):31–41
10 Katz JN. Lumbar disc disorders and low-back pain: socioeco-nomic factors and consequences. J Bone Joint Surg Am 2006;88(Suppl 2):21–24
11 Lin PM, Cautilli RA, Joyce MF. Posterior lumbar interbody fusion.Clin Orthop Relat Res 1983;(180):154–168
12 Wetzel FT, LaRocca H. The failed posterior lumbar interbodyfusion. Spine 1991;16(07):839–845
13 Zindrick M, Wiltse LL, Assan S, Benson M. Symptomatic discherniation lateral to the intervertebral foramen. (ScientificExhibit). American Academy of Orthopaedic Surgeons, NewOrleans, Louisiana, February 10–15, 1986
14 Rodríguez-Vela J, Lobo-Escolar A, Joven-Aliaga E, et al. Periopera-tive and short-term advantages ofmini-open approach for lumbarspinal fusion. Eur Spine J 2009;18(08):1194–1201
15 Strempel AV, Moosmann D, Stoss C. Stabilization of the degener-ated lumbar spine in the nonfusion techniquewith cosmic poster-ior dynamic system. WSJ 2006;1:40–47
16 Wrugler-Hauri CC, Kalbarczyk A, Wiesli M, Landolt H, Fandino J.Dynamic neutralization of the lumbar spine after microsurgicaldecompression in acquired lumbar spinal stenosis and segmentalinstability. Spine 2008;33(09):1050
17 Freudiger S, Dubois G, Lorrain M. Dynamic neutralisation of thelumbar spine confirmed on a new lumbar spine simulator in vitro.Arch Orthop Trauma Surg 1999;119(3-4):127–132
18 Schmoelz W, Onder U, Martin A, von Strempel A. Non-fusion in-strumentation of the lumbar spine with a hinged pedicle screw rodsystem: an in vitro experiment. Eur Spine J 2009;18(10):1478–1485
19 Street JT, Andrew Glennie R, Dea N, et al. A comparison of theWiltse versus midline approaches in degenerative conditions ofthe lumbar spine. J Neurosurg Spine 2016;25(03):332–338
20 Tsutsumimoto T, Shimogata M, Ohta H, Misawa H. Mini-openversus conventional open posterior lumbar interbody fusion forthe treatment of lumbar degenerative spondylolisthesis: com-parison of paraspinal muscle damage and slip reduction. Spine2009;34(18):1923–1928
21 Mukai Y, Takenaka S, Hosono N, Miwa T, Fuji T. Intramuscularpressure of themultifidusmuscle and low-back pain after poster-ior lumbar interbody fusion: comparison of mini-open and con-ventional approaches. J Neurosurg Spine 2013;19(06):651–657
22 Buttermann GR, Mullin WJ. Two-Level Circumferential LumbarFusion Comparing Midline and Paraspinal Posterior Approach:5-Year Interim Outcomes of a Randomized, Blinded, ProspectiveStudy. J Spinal Disord Tech 2015;28(09):E534–E543
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Paraspinal Lumbar Spine Approach - Wiltse Access Rabelo et al. 171

Intraoperative Neurophysiological Monitoringfor Spinal Fusion
Monitorização neurofisiológica intraoperatória parafusão espinhal
Marco de Agassiz Almeida Vasques1 Eliana de Barros Marques Fonseca1
1Hospital das Forças Armadas, Brasília, DF, Brazil
Arq Bras Neurocir 2017;36:172–177.
Address for correspondence Marco de Agassiz Almeida Vasques, MD,PhD, Neurosurgeon, Hospital das Forças Armadas, Brasília, DF, Brazil(e-mail: [email protected]).
Introduction
Spinal decompressions and fusions are among the most fre-quently performed surgeries,1 carrying a real chance of neuralinjury2–5 with possibly disastrous consequences for the pa-tients’ quality of life and elevated health care costs.6 Over thelast decade, the use of intraoperative neurophysiologicalmonitoring has becomeessential in neurosurgical procedures,because it brings safety to the patients,7–10 as it can detectimpending neurologic compromise, modifying the actions ofthe operating team to avoid injuries, and it might be consid-ered as a minimal acceptable standard of care for all spinalprocedures.11,12 The decision of using intraoperative neuro-physiologicalmonitoring is stillmademostly by thesurgeon.13
Theeffectiveness of intraoperativeneurophysiologicalmon-itoring has been challenged by some studies based on theassumptionofa lowriskofpostoperativedeficitsandadditionalcosts with small differences in clinical outcomes.14–17
In the surgical treatment of spinal pathologies, there arethree main goals to achieve: decompression of the neuralstructures, spinal stability, and preservation of the patient’sfunction. In order to achieve these goals, spine surgeonsmusthave adequate training on the specific surgery and utilize allthe tools available to assure the appropriate positioning ofthe materials and to avoid neural injury.2–5,18 Nevertheless,some health insurance companies still insist on denying thecoverage for intraoperative neurophysiological monitoring.Themain reason for those denials is thefinancial cost.16,19–21
Keywords
► intraoperativeneurophysiologicalmonitoring
► spinal fusion► review
Abstract The surgical techniques of spinal fusion are frequently used in the treatment of manyspine conditions. Apart from having anatomical knowledge, in order to perform thoseprocedures safely, it is essential to utilize all the tools available to assure the appropriatepositioning of the materials and avoid neural injury. The goal of this article is to reviewthe literature on the use of intraoperative neurophysiological monitoring for spinalfusion procedures and to discuss the controversies regarding this issue.
Palavras-chave
► monitorizaçãoneurofisiológicaintraoperatória
► fusão espinhal► revisão
Resumo As técnicas cirúrgicas de fusão espinhal são frequentemente utilizadas no tratamentode muitas condições da coluna vertebral. Além do conhecimento anatômico, pararealizar esses procedimentos com segurança é essencial utilizar todas as ferramentasdisponíveis para assegurar o posicionamento adequado dos materiais e evitar lesõesneurais. O objetivo deste artigo é revisar a literatura sobre o uso de monitorizaçãoneurofisiológica intraoperatória para procedimentos de fusão espinhal e discutir ascontrovérsias relacionadas a essa questão.
receivedMarch 20, 2017acceptedMay 31, 2017published onlineJuly 3, 2017
DOI https://doi.org/10.1055/s-0037-1604135.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Review Article | Artigo de Revisão172

Unfortunately, the economic power of those companiesfrequently prevails over themedical indications, many timeswith losses to the patients. A scientific approach, withknowledge of the benefits of the technique, should be usedmore frequently. In this article, the authors review theliterature on the use of intraoperative neurophysiologicalmonitoring for spinal fusion procedures.
Methods
The Medline/Pubmed database was utilized for the crossedsearch of articles on the subject with the use of the narrowterms intraoperative neurophysiological monitoring and spinalfusion, with no filters. The LILACS database was also searched,with the use of the narrow term intraoperative neurophysio-logical monitoring. The resulting articles were analyzed, andtheir contents were summarized and discussed.
Results and Discussion
In the literature, there are many publications on the use ofintraoperativeneurophysiologicalmonitoring (on thePubMeddatabase alone, we found 660 articles with a narrow termresearch). With more restricted terms, the crossed searchusing intraoperative neurophysiologicalmonitoringAND spinalfusion resulted in 31 articles. Studying those articles, we foundinteresting results. From the31 articles, by applying the articletypefiltering, therewere9 case reports,22–305 reviews,28,31–34
and 2 clinical trials.11,35 Twenty five articles (80.64%) werepublished in theperiodbetween2013and2017.On theLILACSdatabase, with the use of the narrow term intraoperativeneurophysiological monitoring, we found 13 articles, but only9 were related to spinal surgery.36–44
Anterior FusionLegatt et al22 reported a case of anterior cervical discectomyand fusion surgery in which findings on somatosensory-evoked potential monitoring led to the correction of carotidartery compression in a patient with a vascularly isolatedhemisphere (no significant collateral blood vessels to thecarotid artery territory), and the patient suffered no neuro-logical morbidity. During anterior cervical spine surgery,carotid artery compression by the surgical retractor cancause hemispheric ischemia and infarction in patients withinadequate collateral circulation. Changes in the corticalsomatosensory-evoked potentials and no changes in thecervicomedullary somatosensory-evoked potentials warnto the possibility of hemispheric ischemia.
Nair et al30 reported a case in which vascular injury wasdetected by multimodality neurophysiological monitoringduring an L3-S1 anterior lumbar interbody fusion, demon-strating the need for multimodality monitoring and the com-bined use of somatosensory-evoked potentials and motor-evoked potentials.
Posterior FusionThe importance of intraoperative electromyography moni-toring for lumbar fusionwas already prospectively evaluated
by Welch et al,7 once this method early warned the surgeonthat redirection of the pedicle probe or screw was necessaryto avoid nerve root irritation or injury. Those authors saidthat stimulus-evoked electromyography proved to be reli-able and effective, especially when used in combinationwithspontaneous electromyography. Once neuroanatomicalstructures near the bony pedicles of the lumbar spine allowlittle room for technical error or compromise of the boneduring pedicle screw insertion, in these procedures thissafety item could be deemed essential.
Kulik et al11 performed a computed tomography-basedstudy investigating the relationshipbetween thepedicle screwplacement and the stimulation threshold of the compoundmuscle action potentials measured by intraoperative neuro-physiological monitoring. They studied 68 thoracic and136 lumbar screws placed under electromyography controlin30patients, and foundamorefrequent truepredictionof thecorrect position of the screw for lumbar than for thoracicscrews. They also concluded that a screw stimulation thresh-old > 10 mA does not necessarily indicate correct pediclescrew placement, as there were some false negative cases inwhich a screw stimulation > 10 mAwithoutmuscle responsewas associated with misplacement of the screws; a gradualdecrease in thescrewstimulation thresholdswasnotobservedas the screwplacement approached thenerve root; otherwise,a threshold of 2 mA with muscle response indicates directcontact with nervous tissue. In spite of those limitations,the authors state that “[…]neurophysiological monitoringremains useful andmight be regarded as aminimal acceptablestandard of care for all spinal procedures except perhapssimple lumbar disc surgery.”
Agarwal et al45 performed a retrospective review of 784patients undergoing posterior spinal fusion with intra-operative neurophysiological monitoring without any base-line deficits. Those authors found somatosensory-evokedpotential and motor-evoked potential changes in 3.3% ofthe patients undergoing posterior spinal fusion, with thehighest incidence at the cervicothoracic level. Eighty-eightpercent of the patients with intraoperative neurophysiologi-cal monitoring changes had improvements in intraoperativeneurophysiological monitoring signals following interven-tions during surgery. Fifteen percent of the patients hadneurological deficits despite surgeon intervention followingneurophysiological monitoring alerts.
In scoliosis correctionsurgeries, as there is ahighnumberoflevels, there is a real risk of occurrence of poor positioning ofthepedicle screws inserted, evenwith theaidof intraoperativeelectromyographic stimulation.36 Kobayashi et al23 studiedthe characteristics of cases with intraoperative transcranialmotor-evoked potential waveform deterioration (defined as adecrease in intraoperative amplitude � 70% of the controlwaveform) during posterior corrective fusion for adolescentidiopathic scoliosis. Waveform deterioration commonlyoccurred during rotation maneuvers and more frequently inpatientswitha largerpreoperativeCobbangle. Theyalso foundsignificant relationships between theestimatedblood loss andthe number of levels fused with waveform deterioration.Rumalla et al,46 in a study of trends in spinal fusion surgery
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Intraoperative Neurophysiological Monitoring for Spinal Fusion Vasques et al. 173

for pediatric neuromuscular scoliosis, found an increase inintraoperative neurophysiological monitoring from 2009 to2011. Additionally, in the univariate analysis, they found thatthe use of intraoperative neurophysiological monitoring wasassociated with decreased complications and length of stay.Those authors concluded that increasing the use of intra-operative neurophysiological monitoring and posterior-onlyapproaches may combat the high complication rates in neu-romuscular scoliosis.
Thirumala et al,31 in a review, researched the diagnosticaccuracy of somatosensory-evoked potential monitoringduring adolescent idiopathic scoliosis fusion. This meta-analysis covering 4,763 operations on idiopathic scoliosispatients showed that the somatosensory-evoked potential isa highly sensitive and specific test, and that iatrogenic spinalcord injury resulting in new neurological deficits was 340times more likely to present changes in the somatosensory-evoked potential compared with those injuries without anynew deficits. Somatosensory-evoked potential monitoringduring scoliosis correction surgeries in children remains ahighly reliable method for reducing iatrogenic neurologicdeficits with high sensitivity and specificity.47
Chung et al,24 in a technical report, informed that thegrowing rod technique for spinopelvic dissociation underintraoperative neurophysiological monitoring could be auseful alternative surgical option, especially in patients with-out neurologic deficit.
Nakamae et al28 described 2 cases of surgical treatmentusing intraoperative electrophysiological monitoring withtranscranial electric motor-evoked potentials and continu-ous spontaneous electromyography for patients with high-grade dysplastic spondylolisthesis in adolescence. They suc-cessfully performed the surgeries without any neurologicaldeficit using intraoperative electrophysiological monitoring.
Lateral FusionNarita et al48 studied 36 patients who underwent extremelateral interbody fusion (XLIF) for lumbar spine degenerativespondylolisthesis or lumbar spine degenerative scoliosis atL4–5 or at a lower level. During the operation, the psoasmajor muscle was dissected using an index finger fitted witha finger electrode, and the threshold values of the dilatorwere recorded before and after dissection. The historicalcontrols were 18 patients (who underwent the same proce-dure for the same indications without the use of the fingerelectrode). They had no serious neurological complicationsin any of the patients, but there was a significantly lowerincidence of transient neurological symptoms in the fingerelectrode group (7 [38%] out of 18 cases versus 5 [14%] out of36 cases; p ¼ 0.047). They suggest that this neuromonitoringsystem using a finger electrode may be useful to preventXLIF-induced neurological complications.
Grimm et al,49 in a retrospective chart review of periop-erative complications within the first year after extremelateral interbody fusion (involving 108 patients), found 25complications (23%) in patients who underwent the proce-dure. Four patients (3.7%) experienced major complications,including vertebral body fracture, contralateral nerve root
injury, dense quadriceps paresis, and persistent stenosis.There also were minor complications (approach-relatedthigh pain and/or paresthesias) that were all ultimatelyresolved. The authors state that dense femoral nerve palsyis a complication that may occur despite intraoperativeneurophysiological monitoring.
The femoral nerve preservation in transpsoas lateralaccess surgery of the spine with the aid of neuromonitoringwas addressed by Block et al,33 who proposed a theory andtechnique to utilize motor-evoked potentials to protect thefemoral nerve at risk in those procedures. On multipleoccasions, their neuromonitoring groups observed signifi-cantly degraded amplitudes of the femoral motor- and/orsensory-evoked potentials limited only to the surgical side.Most of these degraded response amplitudes rapidly re-turned to baseline values with a surgical intervention likethe removal of surgical retraction.
Cheng et al50 also debated the requirement for intra-operative neuromonitoring in 90° lateral transpsoas spinesurgery (lateral lumbar interbody fusion). Considering thatthe lateral approach to the lumbar spine requires passage nearor adjacent to the lumbar plexus, the mini-open lateral trans-psoas approachuses evokedelectromyography integrated intothe approach, and instrumentation that stimulates in direc-tional orientations and provides discrete threshold responsesto avoid the nerves of the lumbar plexus. Some lateral trans-psoas approaches to the lumbar spine have been developedthat do not advocate for the use of neuromonitoring, insteadrelying on direct visualization and avoidance of nerves (“shal-low-docking”). Theystate there is substantiallymore literaturedescribing the use of neuromonitoring in lateral transpsoassurgery, but reports of direct visualization and avoidance ofnerves (shallow-docking) are emergent.
Uribe et al34 reviewed intraoperative electromyographyneurophysiological monitoring methods and their applica-tion in minimally invasive spine surgery. They state that theuse of electromyography during the minimally invasivelateral transpsoas approach to the lumbar spine for interbodyfusion contributed to decrease the complication rate from30% to less than 1%. The authors consider that in addition toknowledge of the anatomy and image guidance, directionalintraoperative electromyography neurophysiological moni-toring is crucial to guarantee a safe passage through thepsoas muscle during the minimally invasive lateral retroper-itoneal approach.
Cost-benefit IssuesJames et al21 investigated the increase in the use of intra-operative neurophysiological monitoring during spine surgery,concluding that as thecostsof spinesurgeries continue to rise, itbecomes necessary to examine and justify the use of differentmedical technologies, including intraoperativeneurophysiolog-icalmonitoring,duringspinesurgery.Garcesetal,16consideringthewidespread use of intraoperativemonitoring inmany typesof spinal surgeries, with concerns about its overuse in routineand low-risk procedures, performed a retrospective databasereview of 112 patients undergoing a 1- or 2-level minimallyinvasive surgery for transforaminal lumbar interbody fusion.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Intraoperative Neurophysiological Monitoring for Spinal Fusion Vasques et al.174

They believe that the use of intraoperative monitoring forminimally invasive surgery for transforaminal lumbar inter-body fusion provides no added benefit. Ney et al,19 in a large,multiyear, nationally representative dataset, showed thatneurophysiological intraoperative monitoring was associatedwith better clinical outcomes in non-complex spine surgeries(with the largest benefits for laminectomies). The risk ofneurologic complications was 75% higher without the use ofneurophysiological intraoperativemonitoring.Additionally, theadjusted increase in hospital charges was of only 9%. They alsoemphasize that the actual cost of neurophysiological intra-operative monitoring is outweighed by a lifetime of lost wagesand health care costs from neurologic complications, includingspinal cord injury.6,19 Husain et al20 comment that this reduc-tion in complications is preferred to the higher-cost issue.
Theoccurrenceof iatrogenicneurologic deficit after lumbarspine surgery (mainly for degenerative spondylolisthesis,spondylosis, scoliosis, and lumbar stenosis) was reviewed byGhobrial et al,32 who worked with a population of 2,783patients in 12 studies. The authors state that those complica-tions were avoided with the use of neuromonitoring. Thirtypatients out of 731 (4.1%) patients had a new onset of aneurologic injury after anterior lumbar interbody fusion orlateral lumbar interbody fusion. Thirty-seven out of 2,052(1.9%) patients had a neurologic injury after posterior decom-pression and fusion. Screwmalpositionwas responsible for 11deficits. These data show that spinal surgery for lumbardegenerative disease carries a low but real chance of neuro-logic deficits. Gavrancic et al51 recommend specific tests forthe intraoperative neurophysiologicalmonitoringduring lum-bar spine surgerymonitoring. Yaylali et al52 propose the use ofintraoperative neurophysiological monitoring also in anteriorlumbar interbody fusion.
Eager et al,53 reviewing 2,069 spine cases, found 32 caseswith possible intraoperative events. There were 17 cases inwhich intraoperative neurophysiological monitoring changesaffected the course of the surgery and prevented possiblepostoperative neurological deficits (7 due to deformity correc-tion, 5 due to hypotension, 4 due to patient positioning, and 1due to a screw requiring repositioning), reinforcing the impor-tance of multimodality intraoperative neurophysiologicalmonitoring (including somatosensory-evoked potentials,transcranial electrical motor-evoked potentials, and spontane-ous and triggered electromyography) in spinal surgery.
McClendon et al,54 studying reoperation patients whoreceived operative correction of proximal junctional kypho-sis of the upper thoracic spine, used intraoperative neuro-physiological monitoring in all patients.
New DevelopmentsIn a recent study, Turner et al25 evaluated spinal cord perfu-sion (using a laser Doppler probe fixated to the dura at thelevel of the pedicle subtraction osteotomy and intrathecalpressure monitoring using a lumbar drain, somatosensory-evoked potential and motor-evoked potential) during adultspinal deformity surgery as a marker for the risk of spinalcord injury. The alterations of perfusion and potentialsguided the correction of the deformity. This was direct
evidence that fluctuations in spinal cord perfusion maycontribute to neurologic changes during adult spinal defor-mity surgery, contributing to the development of strategiesfor spinal cord protection during high-risk cases. Eck et al29
reported a case of a patient with an American Spinal InjuryAssociation grade B (ASIA B) spinal cord injury with partiallyintact baseline intraoperative neurophysiological monitor-ing who made a complete functional recovery postopera-tively, illustrating the potential prognostic value ofintraoperative neurophysiological monitoring.
Anesthesiahas a fundamental roleon intraoperativeneuro-physiological monitoring,26,27,55 as the drugs used may alterthe parameters intraoperatively.26 There are some options inthe choice of anesthesia during intraoperative neurophysio-logical monitoring, and this choice must consider the specificneeds of the procedure (as a more rapid awakening and thefeasibility of a rapidwake-up test when irreversible changes inneurophysiological monitoring are noted).27,35
The use of different criteria to alarm neurophysiologicalmonitoring during spine surgeries has also been addressed,and the reduction in amplitude potentials (sensitive ormotor-evoked potentials) with maximal stimulation formotor-evoked potentials could be a better warning alertthan the complete loss of any of these potentials.37 Thespecific needs of the neuromonitoring technique must bediscussedwith the surgeon in order to obtain the best resultspossible. There is a type of misplacement of lumbar pediclescrews associated with radicular pain in the standing andseated positions, that may not be detected by conventionalmonitoring, for example, suggesting the use of systematicpedicle track stimulation prior to the insertion of the lumbarpedicular screw.38 Actually, electrical stimulation enables areduction in the risk of medial positioning, minimizing theuse of intraoperative radiographs for thoracic screws.40
Concerning pediatric neurosurgical procedures, despitetheir recent application, neurophysiological monitoring rep-resents an important tool in the prevention and reduction ofpossible neurological lesions,39,46,56 and in some cases itmay inform the anatomical site for the corrective surgicalmaneuver to be performed.57
Even in those cases considered simple spine surgeries, theuse of intraoperative neurophysiological monitoring hasbeen proved useful, enabling the dynamic neurophysiologi-cal diagnosis, the differentiation of the compression at thecentral or foraminal levels, and the clinical awareness ofiatrogenic damage, thereby increasing safety.41 Even thoughintraoperative neurophysiological monitoring does not sub-stitute good surgical technique and care, it is an importanttool to provide relevant information to the spine surgeon,and it may provide the best chance to detect and possiblyavoid spinal cord and nerve root injuries.58 During spinesurgery, intraoperative neurophysiological monitoring is,thus, an effective method of monitoring the functionalintegrity of the spinal cord and nerve roots, reducing risksand improving postoperative results.42–44,59 The actualtrend is to use multimodal intraoperative neurophysiologi-cal monitoring on procedures near or involving neuralelements.46,56,58
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Intraoperative Neurophysiological Monitoring for Spinal Fusion Vasques et al. 175

Conclusion
The spine surgery team has the challenge of reconciling thetechnological developmentswith thebest interestof thehealthcare system and its growing costs. We believe that this recon-ciliation is feasible to the benefit of the patients health. Basedon the literature discussed, multimodal intraoperative neuro-physiological monitoring is an extremely useful tool in theprevention of surgery-related neural damages. We can alsoforesee that the use of this kind ofmonitoring will be essentialinall spinesurgicalprocedures that involvethemanipulationofor proximity to nervous structures.
References1 Elixhauser A, Andrews RM. Profile of inpatient operating room
procedures in US hospitals in 2007. Arch Surg 2010;145(12):1201–1208
2 Cramer DE, Maher PC, Pettigrew DB, Kuntz C IV. Major neurologicdeficit immediately after adult spinal surgery: incidence andetiology over 10 years at a single training institution. J SpinalDisord Tech 2009;22(08):565–570
3 Yadla S, Malone J, Campbell PG, et al. Early complications in spinesurgery and relation to preoperative diagnosis: a single-centerprospective study. J Neurosurg Spine 2010;13(03):360–366
4 Nasser R, Yadla S, Maltenfort MG, et al. Complications in spinesurgery. J Neurosurg Spine 2010;13(02):144–157
5 Campbell PG, Yadla S, Malone J, et al. Complications related toinstrumentation in spine surgery: a prospective analysis. Neuro-surg Focus 2011;31(04):E10
6 Ney JP, van der Goes DN, Watanabe JH. Cost-benefit analysis:intraoperative neurophysiological monitoring in spinal surgeries.J Clin Neurophysiol 2013;30(03):280–286
7 Welch WC, Rose RD, Balzer JR, Jacobs GB. Evaluation with evokedand spontaneous electromyography during lumbar instrumenta-tion: a prospective study. J Neurosurg 1997;87(03):397–402
8 Bilsky MH. Boachie-Adjei, Shields CB, Baldwin N. Thoracic andlumbar deformities. In: Benzel EC, editor. Spine surgery: tech-niques, complication avoidance, and management. Philadelphia:Elsevier Churchill Livingstone; 2005:796–823
9 Pahys JM, Guille JT, D’Andrea LP, Samdani AF, Beck J, Betz RR.Neurologic injury in the surgical treatment of idiopathic scoliosis:guidelines for assessment and management. J Am Acad OrthopSurg 2009;17(07):426–434
10 Silva EG, Kojo HD, Joaquim AF, Shaffrey CI. Scoliosis: currentoverview and treatment considerations. Arq Bras Neurocir2010;29(04):130–136
11 Kulik G, Pralong E, McManus J, Debatisse D, Schizas C. A CT-basedstudy investigating the relationship between pedicle screw pla-cement and stimulation threshold of compound muscle actionpotentials measured by intraoperative neurophysiological mon-itoring. Eur Spine J 2013;22(09):2062–2068
12 Magit DP, Hilibrand AS, Kirk J, et al. Questionnaire study ofneuromonitoring availability and usage for spine surgery. J SpinalDisord Tech 2007;20(04):282–289
13 Fehlings MG, Brodke DS, Norvell DC, Dettori JR. The evidence forintraoperative neurophysiological monitoring in spine surgery:does it make a difference? Spine 2010;35(9, Suppl)S37–S46
14 Hamilton DK, Smith JS, Sansur CA, et al; Scoliosis Research SocietyMorbidity and Mortality Committee. Rates of new neurologicaldeficit associated with spine surgery based on 108,419 proce-dures: a report of the scoliosis research society morbidity andmortality committee. Spine 2011;36(15):1218–1228
15 Cole T, Veeravagu A, Zhang M, Li A, Ratliff JK. Intraoperativeneuromonitoring in single-level spinal procedures: a retrospec-tive propensity score-matched analysis in a national longitudinaldatabase. Spine 2014;39(23):1950–1959
16 Garces J, Berry JF, Valle-Giler EP, Sulaiman WA. Intraoperativeneurophysiological monitoring for minimally invasive 1- and 2-level transforaminal lumbar interbody fusion: does it improvepatient outcome? Ochsner J 2014;14(01):57–61
17 Traynelis VC, Abode-Iyamah KO, Leick KM, Bender SM, GreenleeJD. Cervical decompression and reconstruction without intrao-perative neurophysiological monitoring. J Neurosurg Spine 2012;16(02):107–113
18 Lehman RA, Potter BK, KukloTR, et al. Probing for thoracic pediclescrew tract violation(s): is it valid? J Spinal Disord Tech 2004;17(04):277–283
19 Ney JP, van der Goes DN, Nuwer MR. Does intraoperative neuro-physiologic monitoring matter in noncomplex spine surgeries?Neurology 2015;85(24):2151–2158
20 Husain AM. Comment: Neurophysiologic intraoperativemonitor-ing in “low-risk” spine surgeries. Neurology 2015;85(24):2157
21 James WS, Rughani AI, Dumont TM. A socioeconomic analysis ofintraoperative neurophysiological monitoring during spine sur-gery: national use, regional variation, and patient outcomes.Neurosurg Focus 2014;37(05):E10
22 Legatt AD, Laarakker AS, Nakhla JP, Nasser R, Altschul DJ. Soma-tosensory evoked potential monitoring detection of carotid com-pression during ACDF surgery in a patient with a vascularlyisolated hemisphere. J Neurosurg Spine 2016;25(05):566–571
23 Kobayashi K, Imagama S, Ito Z, et al. Transcranial motor evokedpotential waveform changes in corrective fusion for adolescentidiopathic scoliosis. J Neurosurg Pediatr 2017;19(01):108–115
24 Chung HY, Suk KS, Lee HM, et al. Growing rod technique for thetreatment of the traumatic spinopelvic dissociation: a technicaltrick. Spine J 2016;16(03):e209–e214
25 Turner JD, Eastlack RK, Mirzadeh Z, Nguyen S, Pawelek J, MundisGM Jr. Fluctuations in Spinal Cord Perfusion During Adult SpinalDeformity Correction Identify Neurologic Changes: Proof of Con-cept. World Neurosurg 2016;85:365.e1–365.e6
26 Allison DW, Gertsch JH, Mahan MA, Sheean GL, Brown JM.Anesthesia considerations for monitoring TCMEPs in adults diag-nosed with poliomyelitis as children: a case report. Neurodiagn J2014;54(01):28–35
27 Sloan TB, Vasquez J, Burger E. Methohexital in total intravenousanesthesia during intraoperative neurophysiological monitoring.J Clin Monit Comput 2013;27(06):697–702
28 Nakamae T, Tanaka N, Nakanishi K, et al. Surgical treatment of high-grade dysplastic spondylolisthesis using intraoperative electrophy-siological monitoring: report of two cases and review of the litera-ture. Eur J Orthop Surg Traumatol 2013;23(Suppl 1):S121–S127
29 Eck JC, Martin CJ, Lapinsky A, Connolly PJ, Dipaola C. Doesintraoperative neurophysiological monitoring have predictivevalue for functional recovery following spinal cord injury? Acase report. J Clin Monit Comput 2013;27(01):93–96
30 Nair MN, Ramakrishna R, Slimp J, Kinney G, Chesnut RM. Left iliacartery injury during anterior lumbar spine surgery diagnosed byintraoperative neurophysiological monitoring. Eur Spine J 2010;19(Suppl 2):S203–S205
31 Thirumala PD, Cheng HL, Loke YK, Kojo Hamilton D, Balzer J,Crammond DJ. Diagnostic accuracy of somatosensory evokedpotential monitoring during scoliosis fusion. J Clin Neurosci2016;30:8–14
32 Ghobrial GM, Williams KA Jr, Arnold P, Fehlings M, Harrop JS.Iatrogenic neurologic deficit after lumbar spine surgery: A review.Clin Neurol Neurosurg 2015;139:76–80
33 Block J, Silverstein JW, Ball HT, et al. Motor evoked potentials forfemoral nerve protection in transpsoas lateral access surgery ofthe spine. Neurodiagn J 2015;55(01):36–45
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Intraoperative Neurophysiological Monitoring for Spinal Fusion Vasques et al.176

34 Uribe JS, Vale FL, Dakwar E. Electromyographicmonitoring and itsanatomical implications in minimally invasive spine surgery.Spine 2010;35(26, Suppl)S368–S374
35 Martin DP, Bhalla T, Thung A, et al. A preliminary study of volatileagents or total intravenous anesthesia for neurophysiologicalmonitoring during posterior spinal fusion in adolescents withidiopathic scoliosis. Spine 2014;39(22):E1318–E1324
36 Gavassi BM, Oliveira CEAS, Barsotti CEG, Santos FPE, Pratali RR,Ferreira RJR. Positioning of pedicle screws in adolescent idio-pathic scoliosis using electromyography. Coluna/Columna 2015;14(02):100
37 Dominici M, Comerlato EA, Ventura FD, Chaloult E. Accuracy oftwo different criteria for neurophysiological intraoperative mon-itoring (NIOM) in spine/spinal cord surgeries. Arq Bras Neurocir2014;33(01):1–5
38 González VG, Burgos-Flores J, Del-Olmo T, et al. Misplacement oflumbar pedicular screws that produce postoperative mechanicalradiculalgia with normal intraoperative neurophysiological sti-mulation: the value of neurophysiological stimulation at thepedicular mid-track. Coluna/Columna 2013;12(04):322–325
39 Habeych S,Miguel E. Intraoperative neurophysiologicalmonitoringin pediatrics: Current controversies. . Salud UIS 2012;44(01):7–16
40 García PC, Pérez MH, Lorensu PP, Rodríguez BD, Hernández PS,Rodrigo AA. Predictive value of electrical stimulation in cases ofmalposition of thoracic pedicle screws in spine surgery. Columna2012;11(02):169–170
41 Rodrigues LMR, Rosa FW, Ferreira RJ, Ueno F, Milani C. Herniatedlumbar disc surgery in triathlon athletes with intraoperative neu-rophysiologicmonitoring.Einstein (SaoPaulo)2011;9(04):530–533
42 Kai MR, Brooks JBB, Silva CAC, Rotta JM, Botelho R. The value ofmultimodal intraoperative monitoring during spinal surgery. ArqBras Neurocir 2011;30(01):3–6
43 Pasqualini W, Carvalho MOP, Kanno RM, Castellon AT, Tebet MA.Intraoperative neurophysiological monitoring of patients under-going idiopathic scoliosis surgical correction. Coluna/Columna2010;9(03):282–286
44 Collado-Corona MA, de Leo-Vargas R, Sandoval-Sánchez V, Díaz-Hernández A, Gutiérrez-Sougarret BJ, Shkurovich-Bialik P. Neu-rophysiological monitoring in spinal cord surgery. Cir Cir 2009;77(05):385–390
45 Agarwal N, Hamilton DK, Ozpinar A, Choi P, Hart R, Yaylali I.Intraoperative Neurophysiologic Monitoring for Adult Patients Un-dergoingPosteriorSpinalFusion.WorldNeurosurg2017;99:267–274
46 Rumalla K, Yarbrough CK, Pugely AJ, Koester L, Dorward IG. Spinalfusion for pediatric neuromuscular scoliosis: national trends,complications, and in-hospital outcomes. J Neurosurg Spine2016;25(04):500–508
47 Thirumala PD, Bodily L, Tint D, et al. Somatosensory-evokedpotential monitoring during instrumented scoliosis correctiveprocedures: validity revisited. Spine J 2014;14(08):1572–1580
48 Narita W, Takatori R, Arai Y, et al. Prevention of neurologicalcomplications using a neural monitoring system with a fingerelectrode in the extreme lateral interbody fusion approach.J Neurosurg Spine 2016;25(04):456–463
49 Grimm BD, Leas DP, Poletti SC, Johnson DR II. PostoperativeComplications Within the First Year After Extreme Lateral Inter-body Fusion: Experience of the First 108 Patients. Clin Spine Surg2016;29(03):E151–E156
50 Cheng I, Acosta F, Chang K, PhamM. Point-Counterpoint: The Useof Neuromonitoring in Lateral Transpsoas Surgery. Spine 2016;41(Suppl 8):S145–S151
51 Gavrancic B, Lolis A, Beric A. Train-of-four test in intraoperativeneurophysiologic monitoring: differences between hand and foottrain-of-four. J Clin Neurophysiol 2014;31(06):575–579
52 Yaylali I, Ju H, Yoo J, Ching A, Hart R. Intraoperative neurophy-siological monitoring in anterior lumbar interbody fusion sur-gery. J Clin Neurophysiol 2014;31(04):352–355
53 Eager M, Shimer A, Jahangiri FR, Shen F, Arlet V. Intraoperativeneurophysiological monitoring (IONM): lessons learned from 32case events in 2069 spine cases. Am J Electroneurodiagn Technol2011;51(04):247–263
54 McClendon J Jr, O’Shaughnessy BA, Sugrue PA, et al. Techniques foroperative correction of proximal junctional kyphosis of the upperthoracic spine. Spine 2012;37(04):292–303
55 Subramanian A,Wanta BT, Fogelson JL, Curry TB, Hannon JD. Timeto extubation during propofol anesthesia for spine surgery withsufentanil compared with fentanyl: a retrospective cohort study.Spine 2014;39(21):1758–1764
56 Şenköylü A, Zinnuroğlu M, Börçek A, Aktaş E, Güngör İ, BeyazovaM. Comparison of multimodal intraoperative neurophysiologicalmonitoring efficacy in early childhood and school aged childrenundergoing spinal surgery. Acta Orthop Traumatol Turc 2017;51(01):49–53
57 GavaretM, Pesenti S, Diop-SeneMS, Choufani E, Bollini G, Jouve JL.Intraoperative spinal cord monitoring: Lesional level diagnosis.Orthop Traumatol Surg Res 2017;103(01):33–38
58 Chen Y, Wang BP, Yang J, Deng Y. Neurophysiological monitoringof lumbar spinal nerve roots: A case report of postoperativedeficit and literature review. Int J Surg Case Rep 2017;30:218–221
59 Schär RT, Sutter M, Mannion AF, et al. Outcome of L5 radiculo-pathy after reduction and instrumented transforaminal lumbarinterbody fusion of high-grade L5-S1 isthmic spondylolisthesisand the role of intraoperative neurophysiological monitoring. EurSpine J 2017;26(03):679–690
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Intraoperative Neurophysiological Monitoring for Spinal Fusion Vasques et al. 177

Trochlear Nerve Schwannoma: Case Report andLiterature ReviewSchwannoma do nervo troclear: revisão da literatura erelato de casoMarcelo Lemos Viera da Cunha1,2 Mario Henrique Furlanetto Miranda3 Giulia Luiza Cecconello3
1Neurosurgeon, Hospital Regional do Oeste, Chapecó, SC, Brasil2Sitting Member of the Brazilian Society of Neurosurgery – SBN,São Paulo, SP, Brasil
3Medical Student, Universidade Comunitária da Região de Chapecó,Chapecó, SC, Brasil
Arq Bras Neurocir 2017;36:178–184.
Address for correspondence Marcelo Lemos Vieira da Cunha, MSc,Hospital Regional do Oeste, Rua Lauro Muller, 224e, apto 501, Centro, CEP89801-600, Chapecó, SC, Brasil (e-mail: [email protected]).
Keywords
► neurilemmoma► trochlear nerve► diplopia
Abstract Schwannomas arise from the Schwann cells of the peripheral and cranial nerves. Theyrepresent 8% of the primary cerebral neoplasms. Although schwannomas usually develop insensory nerves, most often on the vestibular and trigeminal nerves, in very rare cases theycan develop in motor nerves. We reported an unusual case of a 29-year-old woman withheadache, nausea, vomiting, and blurred vision ongoing for 3 years. Magnetic resonance ofthe brain showed a solid-cystic expanded injury, heterogeneous, with limits partially definedand epicenter on the pineal gland. The lesion presented hyposignal inT1 and isosignal inT2.An intense enhancement of the solid part was observed after contrast injection. Foci ofcalcification and absence of diffusion restrictionwere also observed. The patient underwentmicroneurosurgery with supracerebellar infratentorial approach in a seated position.Subtotal resection was performed with maintenance of calcified tumor tissue adhered tothe rightRosenthalbasal vein. In thepostoperativephase, thepatient remainedwithdiplopiawhen looking down; however, she reported improvement of headache and nausea.
Palavras-chave
► neurilemoma► nervo troclear► diplopia
Resumo Os schwannomas surgem das células de Schwann, dos nervos periféricos e cranianos erepresentam 8% das neoplasias cerebrais primárias. Apesar de os schwannomas sedesenvolverem comumente em nervos sensoriais, mais frequentemente no nervo vesti-bular e trigêmeo, em casos muito raros ele pode se desenvolver em nervos motores.Relatamos um caso raro, de uma paciente do sexo feminino, 29 anos, com quadro decefaleia, náuseas, vômitos e turvação visual há três anos. Ressonância magnética deencéfalo demonstrou lesão expansiva sólido-cística, heterogênea, com limites parcial-mentedefinidos e epicentronaglândula pineal. Apresentouhipossinal emT1e isossinal emT2.Houve intenso realce daparte sólida após injeçãode contraste. Foramobservados focosde calcificação e ausência de restrição à difusão. A paciente foi submetida a tratamentomicroneurocirúrgico com acesso infratentorial supracerebelar em posição sentada. Houveressecção subtotal commanutenção de tecido tumoral calcificado aderido a veia basal deRosenthal direita. No pós-operatório, a paciente permaneceu com diplopia na miradaocular para baixo, entretanto apresentou melhora de cefaleia e náuseas.
receivedMarch 5, 2017acceptedMay 2, 2017published onlineJune 16, 2017
DOI https://doi.org/10.1055/s-0037-1603919.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Review Article | Artigo de Revisão178

Introduction
Schwannomas arise from the Schwann cells and represent 8%of the primary cerebral neoplasms.1 They usually develop insensory nerves,most often in vestibular nerve.2,3 In very rarecases schwannomas can develop in motor nerves, includingthe trochlear nerve.2 Trochlear nerve schwannomas areextremely rare and, according to our review, there are 37surgical cases related in the literature, including ours.
Case Report
The case described is that of a female patient, 29 years-old,with headache associatedwith nausea, vomiting and blurredvision for 3 years. Imaging studies performed in anotherservice showed an expansive lesion, causing mass effect,resulting in hydrocephalus. The patient was submitted toventriculoperitoneal shunt, with improvement of the clinicalcondition. After the surgery, clinical follow-up was realized.
The patient was admitted in our service 2 years after theventriculoperitoneal shunt surgery. She had diplopia whenlooking down, headache and nausea refractory to the clinicaltreatment. Magnetic resonance imaging (MRI) of the brainshowed a solid-cystic expanded injury, heterogeneous, withlimits partially defined and epicenter on the pineal gland.The lesion presented hyposignal in T1 and isosignal in T2. Anintense enhancement of the solid part was observed aftercontrast injection (►Figs. 1, 2, 3). Foci of calcification andabsence of diffusion restriction were observed as well.
Cerebrospinal fluid examination did not show tumor cellsand the search for α-fetoprotein and human chorionicgonadotropin were negative. The patient underwent micro-neurosurgery with supracerebellar infratentorial approachin a seated position. The surgery was performed with ultra-sonic aspiration and central enucleation of the tumor, allow-ing a better mobility of the tumor capsule and dissection ofdeep veins and mesencephalic roof. Subtotal resection wasperformed, with maintenance of calcified tumor tissueadhered to the right Rosenthal basal vein due to profuse
bleeding when attempting resection of the tumor portion inthis topography (►Fig. 4).
The fourth nerve schwannomas typically show predomi-nance of Antoni B tissue, have frequent clusters of xanthom-atousmacrophages and are poor in Verocay bodies (these areoften more common in spinal tumors). Reticulin is abundantand distinctly pericellular in schwannomas.
Schwannomas are strongly and uniformly reactive forS-100 protein; they may be positive for epithelial mem-brane antigen (EMA), but not frquently, and do not exhibitthe membrane-characteristic pattern of meningioma.Microscopic patterns and immunohistochemical findingsin our case (►Fig. 5). In the postoperative phase, thepatient remained with diplopia when looking down,reporting improvement of headache and nausea.
Fig. 1 Coronal cut in T1 after contrast injection with expansive lesionin the topography of the pineal gland.
Fig. 3 Sagittal cut in T1 after injection of contrast with expansivelesion in the topography of the pineal gland.
Fig. 2 Axial cut in T1 after injection of contrast with expansive lesionin the topography of the pineal gland.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Trochlear Nerve Schwannoma Cunha et al. 179

Discussion
We did a literary review using the PubMed and COCHRANEplatforms searching for the following terms: trochlear nerveschwannoma and schwannoma surgery.
We found the occurrence of 37 surgical cases of trochlearschwannoma. The average age at diagnosis was 44.8 years,with a standard deviation of 15.1. The female gender waspredominant, with 21 cases (58.3%) (►Table 1).
Trochlear nerve schwannoma presents as initial symp-toms, in most cases, diplopia (60%), hemiplegia (43%), head-ache (40%) and cerebellar symptoms (37%), such as ataxia,dysmetria and nystagmus.29,33 In the present study, trochle-ar nerve palsy was evidenced in 17 (50%) of 34 cases
(►Table 1). In three case reports, intratumoral hemorrhageoccurred as a complication.7,26,33
Macroscopically, schwannomas are encapsulated, well-delimited, lobulated, generally grayishmasses, andmay haveareas of cystic alterations and xanthomatosis.36,37
Magnetic resonance imaging showed to be the most usedimaging exam in the evaluation of schwannoma.24,29,31,32,38
Computed tomography (CT) may also be used for the samepurpose.33 At CT, it tends to present as a single, well-circum-scribed and solid-appearing mass, located mainly in thecourse of the IV cranial nerve.32,38 At MRI, schwannomaspresent with hyposignal in T1, hypersignal in T2 and showanintense enhancement after intravenous administration ofgadolinium contrast.38
Schwannomas can be diagnosed with conventional tech-niques when they are small and located in the cerebellum-pontine cistern. However, when they reach very large sizesand the intracanalicular part is not obvious, it may bedifficult to discriminate them from meningiomas and me-tastases.39 So, the use of advanced imaging techniques maybe necessary. Studies with vestibular schwannomas by thecerebellar-angle have shown that, through diffusion-weight-ed imaging (DWI), it is possible to observe that the schwan-nomas solid component, usually isointense to brainparenchyma, presents an apparent diffusion coefficient(ADC) that ranges from 1.1 to 1.7 � 10–3 mm2/S, which isconsidered elevated when compared with the normal brainparenchyma (1.4 � 10–3mm2/S).40,41 This increased coeffi-cientmay reflect the lower cell density of the Antoni B cells ofschwannomas. However, the ADC alone cannot differentiateschwannoma from meningiomas. Even though schwanno-mas present a significantly higher average ADC value, there isconsiderable overlap among the values, which makes itdifficult to differentiatemeningiomas from schwannomas.41
Otherwise, it is possible to differentiate schwannomas frommeningiomas through magnetic resonance (MR) perfusion.The schwannomascerebral bloodvolume (CBV) is significantlysmaller when compared with meningiomas.42 Even if there isan overlap in the reason between the CBV of both entities, athreshold of 4.4 is the highest found in the schwannomas,while the meningiomas CBV average ranges from 6 to 9.42–44
Another way to differentiate meningiomas from schwan-nomas is throughMRproton spectroscopy,where the schwan-nomas show a myo-inositol peak of 3.55 pm and absence ofalanine.45 Meningiomas are characterized by a high cholinesignal with very low signs of creatine and N-acetylaspartate,and alanine presence.46
The trochlear nerve schwannomas are classified in threesubtypes: cisternal, cisternocavernous and cavernous.13 Inour review, 34 of the 37 cases evaluated were cystenal(91.8%), two cases (5.4%) were cisternocavernous and onecase (2.7%) was cavernous.
Contrary to what can be found in the literature regardingtrochlear schwannomas centered in the cisternal portion, thepresent case reports that the trochlear schwannomawas foundwith epicenter in the pineal gland. In our review, this onlyoccurred in one other occasion, generating a second reportedcase with this approach for the referred pathology. The
Fig. 5 Schwannoma strongly and uniformly reactive for S-100 proteinby immunohistochemistry.
Fig. 4 Axial cut of computed tomography with contrast confirmingpostoperative status.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Trochlear Nerve Schwannoma Cunha et al.180

Table
1Literary
review
oftroc
hlea
rne
rveschw
anno
mas.
Referenc
eAge/Se
x4thcran
ial
nervepalsy
Loca
tion
Surgeryap
proac
hFo
llow-up
King4
55/F
No
Ambien
tCistern
Subtem
poraltranstentorialtotheright
App
earanc
eof
fourth
cran
ialnerve
palsyon
the
righ
tsidean
dpa
resisin
therigh
tleg
Bogga
n532
/FYe
sAmbien
tCistern
Subtem
poraltranstentorialc
raniotom
yto
the
righ
tPe
rsistenc
eof
fourth
cran
ialn
erve
palsyon
the
righ
tside
andab
senc
eof
cornea
lrefl
exon
the
righ
tsideafter8mon
ths.
Leun
da6
54/M
Yes
Ambien
tCistern
Subtem
pora
ltranstentorialc
raniotom
yto
the
righ
tPe
rsistenc
eof
fourth
cran
ialn
erve
palsyon
the
righ
tsideafter1year.
Leun
da6
16/F
Yes
Cisternoc
averno
usSu
btem
poraltranstentorialc
raniotom
yto
the
left
Persistenc
eof
fourth
cran
ialn
erve
palsyon
the
left
side
after6mon
ths.
Yamam
oto7
37/F
Yes
Ambien
tCistern
Subtem
pora
ltranstentorialc
raniotom
yto
the
righ
tPe
rsistenc
eof
fourth
cran
ialn
erve
palsyon
the
righ
tsideafter1year.
Garen
818
/FNo
Ambien
tCistern
Subtem
poralc
raniotom
yto
theleft
Improv
emen
tof
thirdcran
ialn
erve
palsy.
Toku
riki9
43/M
No
Ambien
tCistern
Tempo
ralc
raniotom
yto
theright
App
earanc
eof
fourth
cran
ialnerve
palsyon
the
righ
tsideafter1mon
th.
Murak
awa1
023
/FNo
Ambien
tCistern
Pteriona
land
subo
ccipital
App
earanc
eof
fourth
cran
ialnerve
palsyon
the
righ
tside.
Mau
rice
-Williams1
156
/MNo
Ambien
tCistern
Lateralsub
occipital
cran
iotomyto
theleft
App
earanc
eof
fourth
cran
ialnerve
palsyon
the
left
side
after2years.
Samii1
253
/FYe
sAmbien
tCistern
Pteriona
lcraniotom
yto
theleft
Persistenc
eof
fourth
cran
ialn
erve
palsyon
the
left
side
.
Celli1
351
/MYe
sAmbien
tCistern
Subtem
pora
ltranstentorialc
raniotom
yto
the
righ
tPe
rsistenc
eof
fourth
cran
ialn
erve
palsyon
the
righ
tsideafter5years.
Lano
tte1
4NI
NI
Ambien
tCistern
NI
NI
Jack
woski15
26/F
Yes
Ambien
tCistern
Tran
stem
poralc
raniotom
yto
theleft
Persistenc
eof
light
fourth
cran
ialn
erve
palsy
ontheleft
side
.
Abe
1660
/MNo
Ambien
tCistern
Lateralsub
occipital
cran
iotomy
App
earanc
eof
paralysisin
theIV
pair.
Abe
1657
/MNo
Ambien
tCistern
Subtem
poraltranstentorialc
raniotom
yto
the
righ
tApp
earanc
eof
fourth
cran
ialn
erve
palsyafter
4mon
ths.
Dolen
can
dCos
cia1
768
/MNo
Ambien
tCistern
Lateralsub
occipital
cran
iotomyto
theright
App
earanc
eof
postop
erativefourth
cran
ial
nervepa
lsy,
butwithim
prov
emen
tin
2mon
ths.Im
prov
emen
tof
thehe
miparesisto
theleft
within2mon
ths.
Beppu
1866
/MNo
Ambien
tCistern
Lateralsub
occipital
cran
iotomyto
theright
App
earanc
eof
paralysisof
theab
duce
ntne
rve.
Santoren
eos1
935
/FNo
Ambien
tCistern
Subtem
poraltranstentorialc
raniotom
yApp
earanc
eof
fourth
cran
ialnerve
palsyon
the
left
side
.
Nad
karnia
ndGoe
l20
48/F
No
Ambien
tCistern
Subtem
poraltranstentorialc
raniotom
ySu
periorob
lique
musclewea
kness
(Con
tinue
d)
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Trochlear Nerve Schwannoma Cunha et al. 181

Table
1(Con
tinue
d)
Referenc
eAge/Se
x4thcran
ial
nervepalsy
Loca
tion
Surgeryap
proac
hFo
llow-up
Matsui21
61/M
Yes
Ambien
tCistern
Presigmoidtran
spetrosalc
raniotom
yto
the
righ
tPe
rsistenc
eof
fourth
cran
ialn
erve
palsyon
the
righ
tside.
Veshc
hev2
226
/FNo
Caverno
usSinu
sPteriona
lcraniotom
yto
theleft
App
earanc
eof
postop
erativefourth
cran
ial
nervepa
lsyon
theleft
side,
withsignificant
improv
emen
tin
4mon
ths.
Türe
2331
/MYe
sPine
alRe
gion
Infraten
torial
-Lateral
suprace
rebe
llar
Persistenc
eof
fourth
cran
ialn
erve
palsyon
the
left
side
.
Shen
ouda
2449
/MYe
sCisternoc
averno
usPresigmoidco
mbine
dtran
spetrosal
cran
iotomy
Persistenc
eof
fourth
cran
ialn
erve
palsyon
the
left
side
andde
afne
ss.
Du2
17/F
No
Ambien
tCistern
Orbitoz
ygom
atic
pteriona
lAsymptom
atic
Shen
oyan
dRa
ja25
54/F
No
Ambien
tCistern
Subtem
poraltranstentorial
App
earanc
eof
hemiane
sthe
siato
theleftafter
1year.
Ohb
a26
48/M
Yes
Ambien
tCistern
Anteriortran
spetrosal
Perm
anen
ceof
thefourth
cran
ialn
erve
palsy
ontherigh
tsideafter4mon
ths.
Gerga
nov2
752
/FYe
sAmbien
tCistern
Subo
ccipital
Perm
anen
ceof
dysfun
ctionin
thetroc
hlea
rne
rve.
Grigo
rian
andKo
robov
a28
47/F
NI
Ambien
tCistern
Retrom
astoidal
NI
Grigo
rian
andKo
robov
a28
44/F
NI
Ambien
tCistern
Paramed
iansubten
torial
suprace
rebe
llar
NI
Koha
ma2
947
/FNo
Ambien
tCistern
Posteriortran
spetrosalc
raniotom
yApp
earanc
eof
fourth
cran
ialnerve
palsyon
the
left
side
.
Bartalen
a30
50/F
Yes
Ambien
tCistern
Subtem
poral-transpe
tros
alPe
rsistenc
eof
diplopia
withpo
steriorsu
rgical
correc
tionby
mye
ctom
y.
Youn
es31
65/F
Yes
Ambien
tCistern
Pteriona
lIm
prov
emen
tof
fourth
cran
ialn
erve
palsy
after2yearspo
stop
erative.
Bouc
heran
dMicha
el32
64/M
Yes
Ambien
tCistern
Anteriortran
spetrosal
Persistenc
eof
fourth
cran
ialn
erve
palsyon
the
righ
tside.
Hatae
3344
/MYe
sAmbien
tCistern
Zygo
matic
tran
spetrosal
Persistenc
eof
fourth
cran
ialn
erve
palsyon
the
left
side
.
Samad
ian3
463
/MNo
Ambien
tCistern
Left
retros
sigm
oid
App
earanc
eof
fourth
cran
ialn
erve
palsy.
Cha
udhry3
524
/FNo
Ambien
tCistern
Paraoc
cipital
posteriorinterhem
isph
eric
tran
sten
torial,from
therigh
tside
App
earanc
eof
postop
erativefourth
cran
ial
nervepa
lsywitho
utco
mpletereso
lution
after
6mon
ths.
Emerge
nceof
ataxia,w
ithalmost
completereso
lution
after6mon
ths.
Cun
ha(present
stud
y)29
/FYe
sPine
alRe
gion
Supracereb
ellar–infraten
torial
Fourth
cran
ialn
erve
palsywith3mon
ths
postop
erativefollo
w-up.
Abb
reviations
:F,female;
M,male;
NI,no
tinform
ed.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Trochlear Nerve Schwannoma Cunha et al.182

incidenceof tumors in thepineal region ranges from0.4 to1%ofall primary brain tumors, with studies showing a higher per-centage of tumors in this region in children and adolescents,with rates ranging from 3 to 8%.47–51 As a differential diagnosisfor the pineal region, we must consider the tumors divided infour categories: germ cell tumors, pineal parenchyma tumors,pineal gland support tissue tumors (for example, astrocytomas)and tumors originating fromnearby structures (thalamic astro-cytomas, tumors of Plexus choroid).52
The most common tumors of the pineal region are thegerminative ones, responsible for 40 to 80% of the totalnumber, with germinoma being the main representa-tive.47,53 Tumors of the pineal parenchyma have a prevalenceof 11 to 40% of pineal tumors, and can be divided intopineocytes, pineoblastomas, papillary tumors of the pinealregion (PTPRs) and pineal parenchymal tumor of intermedi-ate differentiation (PPTID).53,54
Tumors derived from supporting tissues or structuresaround the pineal gland include astrocytomas, ependymo-mas, papillomas and carcinomas of the choroid plexus,lymphomas, gangliogliomas, dermoid and epidermoid cysts,meningiomas and metastases.55 According to our literaryreview, our study is the second case of trochlear schwan-noma that has its origin in the pineal region.
The therapeutic options for non-vestibular schwannomasinclude clinical observation through serial image analysis,microsurgery and stereotactic radiosurgery.56 Usually, whentreating asymptomatic tumors, clinical observationmay be areasonable alternative, especially in elderly patients or thosewith other comorbidities, since these tumors usually haveslow growth.56
According to our literature review, the most used surgi-cal approach in the cases of trochlear schwannoma is thetranstemperal subtemporal, performed in 13 of 36 cases,followed by transpetrosal (7 cases), lateral suboccipital(7 cases), pterional (5 cases), supracerebellar infratentorial(2 cases) supracerebellar subententorial (1 case), and para-occipital trastentorial (1 case) (►Table 1). In one case, thesurgical approach was not described.54 In our case, we usedthe intratentorial supracerebellar approach, the same oneused in the Ture study.23 The surgical approach used in theprevious case of trochlear schwannoma in the pinealgland was the posterior transtentorial interhemisphericparaoccipital.35
The postoperative of the previously reported cases dem-onstrated the difficulty and vulnerability in preserving thetrochlear nerve during surgery (►Table 1). Among the 17cases that did not present preoperative paralysis, 12 devel-oped a new trochlear paralysis in the postoperative period,and in only 2 cases there were significant improvements introchlear paralysis in the postoperative follow-up. From the17 cases in which the patients had IV paresis, in only 1trochlear function improvement happened, with diplopiaimprovement between 4 weeks and paralysis improvementafter 2 years postoperatively. However, in this same case,the MRI 3 months after surgery showed a small remnanttumor.31
Conclusion
Trochlear nerve schwannomas are extremely rare; however,they generally have a good neurosurgical resectability. Ourwork presents an unusual trochlear nerve schwannoma,corresponding to the wide range of the possible pathologicaldiagnoses when the region of the pineal gland is involved. Inaddition, our case also contrasts with the majority of thecases reported in the literature, which shows tumor epicen-ter furthest from nerve trajectory.
References1 Russell DS, Rubinstein LJ. Pathology of tumors of the nervous
system. 5th ed. Baltimore: Williams and Wilkins; 19892 Du R, Dhoot J, McDermott MW, Gupta N. Cystic schwannoma of
the anterior tentorial hiatus. Case report and review of theliterature. PediatrNeurosurg 2003;38(04):167–173
3 Ho KL. Schwannoma of the trochlear nerve. Case report. J Neu-rosurg 1981;55(01):132–135
4 King JS. Trochlear nerve sheath tumor; case report. J Neurosurg1976;44(02):245–247
5 Boggan JE, RosenblumML,Wilson CB. Neurilemmomaof the fourthcranial nerve. Case report. J Neurosurg 1979;50(04):519–521
6 Leunda G, Vaquero J, Cabezudo J, Garcia-Uria J, Bravo G. Schwan-noma of the oculomotor nerves. Report of four cases. J Neurosurg1982;57(04):563–565
7 Yamamoto M, Jimbo M, Ide M, Kubo O. Trochlear neurinoma.SurgNeurol 1987;28(04):287–290
8 Garen PD, Harper CG, Teo C, Johnston IH. Cystic schwannoma ofthe trochlear nerve mimicking a brain-stem tumor. Case report.J Neurosurg 1987;67(06):928–930
9 Tokuriki Y, Yamashita J, Kikuchi H, Asato R, Handa H. Trochlearnerve neurinoma–case report. Neurol Med Chir (Tokyo) 1988;28(01):70–73 [Tokyo]
10 Murakawa T, Sakai H, Ueda T, Yokoyama K, Takada M, Yamada H.Trochlear neurinoma: case report. Takayama Red Cross Hos-pKiyou 1988;12:163–167
11 Maurice-Williams RS. Isolated schwannoma of the fourth cranialnerve: case report. J NeurolNeurosurg Psychiatry 1989;52(12):1442–1443
12 Samii M, Draf W, Lang J. Surgery of the Skull Base: An Inter-disciplinary Approach. Berlin: Springer; 1989 pp. 335–7
13 Celli P, Ferrante L, Acqui M, Mastronardi L, Fortuna A, Palma L.Neurinoma of the third, fourth, and sixth cranial nerves: a surveyand report of a new fourth nerve case. SurgNeurol 1992;38(03):216–224
14 Lanotte M, Giordana MT, Forni C, Pagni CA. Schwannoma of thecavernous sinus. Case report and review of the literature.J NeurosurgSci 1992;36(04):233–238
15 Jackowski A,Weiner G, O’Reilly G. Trochlear nerve schwannomas:a case report and literature review. Br J Neurosurg 1994;8(02):219–223
16 Abe T, Iwata T, Shimazu M, et al. [Two cases of trochlear nerveneurinoma]. No ShinkeiGeka 1994;22(04):371–375
17 Dolenc VV, Coscia S. Cystic trochlear nerve neurinoma. Br JNeurosurg 1996;10(06):593–597
18 Beppu T, Yoshida Y, Wada T, et al. Trochlear and abducens nerveneurinomas accompanied by a cerebellopontine angle menin-gioma–case report. NeurolMedChir (Tokyo) 1997;37(05):416–421
19 Santoreneos S, Hanieh A, Jorgensen RE. Trochlear nerve schwan-nomas occurring in patients without neurofibromatosis: casereport and review of the literature. Neurosurgery 1997;41(01):282–287
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Trochlear Nerve Schwannoma Cunha et al. 183

20 Nadkarni TD, Goel A. Trochlear nerve neurinoma presenting aspathological laughter. Br J Neurosurg 1999;13(02):212–213
21 Matsui T, Morikawa E, Morimoto T, Asano T. Presigmoidtranspe-trosal approach for the treatment of a large trochlear nerveschwannoma–case report. Neurol Med Chir (Tokyo) 2002;42(01):31–35
22 Veshchev I, Spektor S. Trochlear nerve neuroma manifested withintractable atypical facial pain: case report. Neurosurgery 2002;50(04):889–891, discussion 891–892
23 Türe U, Ozduman K, Elmaci I, Pamir MN. Infratentorial lateralsupracerebellar approach for trochlear nerve schwannoma.J ClinNeurosci 2002;9(05):595–598
24 Shenouda EF, Ghosh A, Coakham HB. Trochlear nerve schwan-noma removed by combined petrosal approach. Br J Neurosurg2002;16(06):600–604
25 Shenoy SN, Raja A. Cystic trochlear nerve neurinoma mimickingintrinsic brainstem tumour. Br J Neurosurg 2004;18(02):183–186
26 Ohba S, Miwa T, Kawase T. Trochlear nerve schwannoma withintratumoral hemorrhage: case report. Neurosurgery 2006;58(04):E791, discussion E791
27 Gerganov V, Amir S, Koerbel A, Brandes A, Stan A, Madjid S. Cystictrochlear nerve schwannoma. Case report. SurgNeurol 2007;68(02):221–225
28 Grigorian IuA, Korobova AN. [Neurinomas of the trochlear nerve].Zh Vopr Neirokhir Im N N Burdenko 2008;(01):50–52
29 Kohama M, Murakami K, Endo T, Watanabe M, Tominaga T.Surgical and histological observations of trochlear neurinoma:case report. Neurol Med Chir (Tokyo) 2009;49(05):217–220
30 Bartalena T, Leoni C, Trossello MP, et al. Hourglass cystic schwan-noma of the trochlear nerve. Acta Biomed 2010;81(02):147–150
31 Younes WM, Hermann EJ, Krauss JK. Cisternal trochlear nerveschwannoma: improvement of diplopia after subtotal tumourexcision. Br J Neurosurg 2012;26(01):107–109
32 Boucher AB, Michael LM II. The middle fossa approach for theremoval of a trochlear schwannoma. Case Rep Neurol Med 2014;2014(01):672314
33 Hatae R, Miyazono M, Kohri R, Maeda K, Naito S. Trochlear nerveschwannoma with intratumoral hemorrhage presenting withpersistent hiccups: a case report. J NeurolSurg Rep 2014;75(01):e183–e188
34 Samadian M, Farzin N, Bakhtevari MH, Hallajnejad M, Rezaei O.Isolated trochlear nerve schwannoma presentingwith diplopia: Acase report and literature review. Interdisciplinary Neurosurgery2015;2(02):111–114
35 Chaudhry NS, Ahmad FU, Morcos JJ. Pineal region schwannomaarising from the trochlear nerve. J ClinNeurosci 2016;32:159–161
36 Stull MA, Moser RP Jr, Kransdorf MJ, Bogumill GP, Nelson MC.Magnetic resonance appearance of peripheral nerve sheathtumors. Skeletal Radiol 1991;20(01):9–14
37 al-Ghamdi S, Black MJ, Lafond G. Extracranial head and neckschwannomas. J Otolaryngol 1992;21(03):186–188
38 Feinberg AS, Newman NJ. Schwannoma in patients with isolatedunilateral trochlear nerve palsy. Am J Ophthalmol 1999;127(02):183–188
39 Press GA, Hesselink JR. MR imaging of cerebellopontine angle andinternal auditory canal lesions at 1.5 T. AJR Am J Roentgenol 1988;150(06):1371–1381
40 Sener RN. Diffusion magnetic resonance imaging of solid vestib-ular schwannomas. J Comput Assist Tomogr 2003;27(02):249–252
41 Yamasaki F, Kurisu K, Satoh K, et al. Apparent diffusion coefficientof human brain tumors at MR imaging. Radiology 2005;235(03):985–991
42 Hakyemez B, Erdogan C, Bolca N, Yildirim N, Gokalp G, Parlak M.Evaluation of different cerebral mass lesions by perfusion-weighted MR imaging. J MagnReson Imaging 2006;24(04):817–824
43 Kremer S, Grand S, Rémy C, et al. Contribution of dynamic contrastMR imaging to the differentiation between dural metastasis andmeningioma. Neuroradiology 2004;46(08):642–648
44 Yang S, Law M, Zagzag D, et al. Dynamic contrast-enhancedperfusion MR imaging measurements of endothelial permeabil-ity: differentiation between atypical and typical meningiomas.AJNR Am J Neuroradiol 2003;24(08):1554–1559
45 Cho YD, Choi GH, Lee SP, Kim JK. (1)H-MRS metabolic patterns fordistinguishing between meningiomas and other brain tumors.MagnReson Imaging 2003;21(06):663–672
46 Majós C, Julià-SapéM, Alonso J, et al. Brain tumor classification byproton MR spectroscopy: comparison of diagnostic accuracy atshort and long TE. AJNR Am J Neuroradiol 2004;25(10):1696–1704
47 Hoffman HJ, Yoshida M, Becker LE, Hendrick EB, Humphreys RP;Experience at the Hospital for Sick Children. Pineal region tumorsin childhood. Experience at the Hospital for Sick Children. 1983.PediatrNeurosurg 1994;21(01):91–103, discussion 104
48 Russell DS, Rubinstein LJ. Pathology of Tumors of the NervousSystem. 4th ed. Baltimore: Wiliams& Wilkins; 1977
49 Surawicz TS, McCarthy BJ, Kupelian V, Jukich PJ, Bruner JM, DavisFG. Descriptive epidemiology of primary brain and CNS tumors:results from the Central BrainTumor Registry of the United States,1990-1994. Neuro-oncol 1999;1(01):14–25
50 Kaatsch P, Rickert CH, Kühl J, Schüz J, Michaelis J. Population-based epidemiologic data on brain tumors in German children.Cancer 2001;92(12):3155–3164
51 Dolecek TA, Propp JM, Stroup NE, Kruchko C. CBTRUS statisticalreport: primary brain and central nervous system tumors diag-nosed in the United States in 2005-2009. Neuro-oncol 2012;14(5, Supp l5):v1–v49
52 Smith AB, Rushing EJ, Smirniotopoulos JG. From the archives ofthe AFIP: lesions of the pineal region: radiologic-pathologiccorrelation. Radiographics 2010;30(07):2001–2020
53 Hirato J, Nakazato Y. Pathology of pineal region tumors. J Neu-rooncol 2001;54(03):239–249
54 Louis DN, Ohgaki H, Wiestler OD, et al. The 2007 WHO classifica-tion of tumours of the central nervous system. ActaNeuropathol2007;114(02):97–109
55 Regis J, Bouillot P, Rouby-Volot F, Figarella-Branger D, Dufour H,Peragut JC. Pineal region tumors and the role of stereotacticbiopsy: review of the mortality, morbidity, and diagnostic ratesin 370 cases. Neurosurgery 1996;39(05):907–912, discussion912–914
56 Pollock BE, Foote RL, Stafford SL. Stereotactic radiosurgery: thepreferred management for patients with nonvestibular schwan-nomas? Int J RadiatOncolBiol Phys 2002;52(04):1002–1007
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Trochlear Nerve Schwannoma Cunha et al.184

Neurosarcoidosis Associated with PsychiatricSymptoms: Case Report
Neurossarcoidose associada com sintomas psiquiátricos:relato de caso
Maick Wilen Fernandes Neves1 Paulo Henrique Pires de Aguiar2 Telmo Augusto Barba Belsuzarri3
Wolnei Marques Zeviani3 João Flavio de Araújo Mattos3 Juliano Nery Navarro3
Renata de Melo Braga Marques4,5 Letícia Marissol de Souza Francisco4
1Pontifícia Universidade Católica de Campinas (PUC-Campinas),Campinas, São Paulo, Brazil
2Department of Neurosurgery, Hospital Santa Paula, São Paulo,São Paulo, Brazil
3Department of Neurosurgery, Hospital Celso Pierro, PUC Campinas,Campinas, São Paulo, Brazil
4Hospital Celso Pierro, Pontifícia Universidade Católica de Campinas(PUC-Campinas), Campinas, São Paulo, Brazil
5Centro de Atenção Integral à Saúde da Mulher (Caism), UniversidadeEstadual de Campinas (Unicamp), Campinas, São Paulo, Brazil
Arq Bras Neurocir 2017;36:185–189.
Address for correspondence Maick Wilen Fernandes Neves, MedicalResident, Pontifícia Universidade Católica de Campinas, Campinas,São Paulo, Brazil (e-mail: [email protected]).
Keywords
► sarcoidosis► neurosarcoidosis► psychiatric
manifestations► pathology
Abstract Background Sarcoidosis is a granulomatous disease predominant in women andblack men that has inflammatory origin of unknown etiology; neurosarcoidosis is a rareand critical presentation of the disease.Case description A 26-year-old black female presented frontal headache for 1 year, aswell as behavioral and mood changes for 15 days. Skull tomography and nuclearmagnetic imaging of the skull revealed damaged meninges, a right frontal bone lesion,and an intraparenchymal contrast-enhancing lesion. Screening with computed tomog-raphy (CT) scans was performed, and it showed signs of bronchiectasis in the lowerthird of the right lung, but it was asymptomatic. The biopsy showed signs of reactionallesion with the presence of non-caseating granulomas. After the treatment withcorticosteroids, the patient presented progressive improvement.Conclusions Neurosarcoidosis is a rare and critical pathology of sarcoidosis thatpresents a lytic bone lesion and clinical psychiatric symptoms; neurosarcoidosis is alsorare in the literature.
Resumo Introdução A sarcoidose é uma doença granulomatosa de origem inflamatória deetiologia desconhecida, predominante em mulheres e negros, sendo a neurosarcoi-dose uma apresentação da doença rara relacionada a gravidade.Relato de Caso Paciente com 26 anos, negra, apresenta quadro cefaleia frontal ha 1ano e há 15 dias apresentando sinais de alterações de comportamento e humor.
receivedApril 15, 2017acceptedJuly 18, 2017published onlineAugust 23, 2017
DOI https://doi.org/10.1055/s-0037-1606290.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
THIEME
Case Report | Relato de Caso 185

Introduction
Sarcoidosis is a multisystem inflammatory disease of un-known etiology in which non-caseating granulomas arefound in the affected organs (mainly the lungs, the skin,and the lymph nodes).1 The incidence of sarcoidosis in Brazilis of 10/100,000 inhabitants, and the worldwide incidence ofneurosarcoidosis is estimated to be � 0.2/100,000 inhabi-tants. The incidence of the disease is higher among womenand black men aged between 20 and 40 years, and it is rarelyseen in children.1–5
A genome study has shown that human leukocyte anti-gens (HLAs) DRB1 and DQB1 are risk factors for the associa-tion with sarcoidosis.6,7 Neurosarcoidosis is rare, and 5–15%of the patients with sarcoidosis will have the central nervoussystem, brain, and spine cord affected; among these, 50%willpresent symptoms.8–10
Case Report
A 26-year-old black female patient presented frontal head-ache for 1 year, as well as sadness, tearfulness, and decreasedappetite for the previous 15 days. She sought medical atten-tion and was treated with risperidone and clonazepam, butthere was no clinical improvement. During the neurologicalexamination, she presented time and space disorientation,so a skull tomography (►Fig. 1) was requested, evidencing
hypodensity and loss of cortical-subcortical differentiationin the right frontal region. Following the investigation,nuclear magnetic resonance imaging (MRI) was used, whichrevealed a meningeal lesion with infiltration of the cerebralparenchyma associated with lytic lesions in the cranialcalotte (►Fig. 2).
Thoracic and total abdominal screening tests were per-formed, and showed a focal lesion (1.6 cm) in the spleenwithlate uptake compatible with hemangioma and focal bronchi-ectasis in the lower lobe of the left lung (►Fig. 3), as well asbilateral subsegmental atelectasis. The echocardiogram andcerebrospinal fluid (CSF) examination were normal.
Meningeal and brain tissue biopsies were performed usinga surgery approach, with supraorbital access and right supra-ciliary incision. During this period, the patient was treatedwith corticoids due to cerebral edema and mass effect; sheshowed an improvement in the signs and symptoms.
The anatomopathological analysis showed a smallamount of granulomas in the bone region and meninges(►Fig. 4 and 5). Immunohistochemistry: CD99 negative,BCL6 negative, BCL2 negative, AE1/AE3 negative, CD68 posi-tive, kappa and lambda immunoglobulin chains positive, PAXpositivity (25%), KI67 focal positivity (10%), CD1a negative,HHF35 negative, calretinin negative, and S100 with focalpositivity < 2%. Thus, the morphological aspects and theimmunomarkers showed a limphohistiocytic lesion with apolytypic aspect compatible with a reactional lesion.
Tomografia de crânio e Ressonância nucelar magnética de crânio que evidenciaramlesão óssea frontal direita, comprometimento meninges e lesão intraparenquimatosacaptante de contraste. Realizado screening com tomografias que evidenciaram sinais debronquiectasia em terço inferior pulmão direito, assintomática. Biopsia indicandosinais de lesão reacional com presenças de granulomas não caseosos, Após amanutenção da corticoterapia, a paciente apresentou melhora progressiva.Conclusões A neurosarcoidose é uma patologia grave e rara da sarcoidose, nesse casoapresenta uma lesão óssea lítica e sintomas psiquiátricos, apresentação rara naliteratura.
Palavras-chave
► sarcoidose► neurosarcoidose► manifestações
psiquiátricas► patologia
Fig. 1 A Skull CT (axial cut) shows a lytic lesion in the right frontal region and loss of cortical-subcortical differentiation.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Neurosarcoidosis Associated with Psychiatric Symptoms Neves et al.186

Clinical Manifestations
The symptoms of sarcoidosis depend on the affected organ,and themost nonspecific are fever, weight loss, night sweats,and fatigue. Neurological and cardiac symptoms are rare;however, when they are present, they indicate severe ill-ness.4 The clinical presentation of neurosarcoidosis is usuallyoptic neuropathy, facial paralysis, meningitis, chronic men-ingitis, diabetes insipidus, hydrocephalus, elevated intracra-nial pressure, spinal cord syndromes, vasculitis, cerebralinfarction, dysfunctional hypothalamus, myelopathy, myop-athy, peripheral neuropathy, and encephalitis (►Table 1); thepresentation of psychiatric symptoms and osseous involve-ment is rare.3,10–14
Cranial nerve alteration is present in 50–75% of thepatients with neurosarcoidosis, and the most common af-fected nerves are, in descending order, cranial nerves VII, IIand VIII. Cranial nerve VII is unilaterally affected in 65% of thecases, and bilaterally affected in 35%;7,15 cranial nerve II isaffected in 5–25% of the patients.1 Bone involvement of theskull and bone involvement of the spine are rare; however,when the latter exists, it is located in the lower thoracicspine, or in the lumbar spine in most cases.16
Diagnosis
The diagnosis is based on the clinical condition and radio-logical presentations; MRI with contrast is the chosen exam,and laboratory tests such as CSF analysis must be evaluated.
Fig. 3 Thoracic tomography (axial cut).
Fig. 2 An MRI shows the frontal and interhemispheric pachymeningeal thickening, which is predominantly right, associated with contrastenhancement. The presence of impairment of the cranial calotte and infiltration of the superior frontal gyrus and frontobasal can be observed.
Fig. 5 Decalcified section of involved area of the skull (osseoustissue).
Fig. 4 Multiple non-caseating well-defined granulomas with fibrosisin the skull.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Neurosarcoidosis Associated with Psychiatric Symptoms Neves et al. 187

However, for the diagnostic confirmation, the exclusion ofother inflammatory granulomatous diseases is necessary.17
The investigation with thorax imaging usually shows strongindications for the diagnosis and helps distinguish it fromdifferential diagnoses (►Table 2).5
The Japanese Sarcoidosis Society and the Japanese Societyof Respiratory Disease presented new diagnostic criteria forneurosarcoidosis that must consider two of six exams: bilat-eral pillar lymphadenopathy; abnormal uptake of 67Ga scin-tigraphy; alveolar lavage fluid examination; elevated serumangiotensin-converting enzyme (ACE); negative tuberculinreaction; and elevated serum or urinary calcium level. Besidesthese exams, there must be a compatible clinical history.18
The definitive diagnosis is made by biopsy of brain tissue,evidencing inflammatory tissue associatedwithnon-caseatinggranuloma and systemic disease compatiblewith the diagnos-tic hypothesis; other possible causes must be excluded.19
Discussion
Pulmonarymanifestations are present in 90% of the patients,butmost of them are asymptomatic. Pulmonary involvementtends to be bilateral and asymmetrical, predominating in theupper lobes, and present atypical radiological aspects in 25%of the cases.20 Bronchiectasis is a typical, uncommon finding,mainly located in the lower lobes and unilateral, as presented
in this case report. Pulmonary fibrosis is another finding thatis present in bronchiectasis caused by sarcoidosis.
The psychiatric symptoms of apathy, agitation, delirium,hallucinations, irritability, lethargy, and depression improvewith the use of corticosteroids.15 Involvement of the skull isuncommon; when it involves the bone in general, the inci-dence is between 1–13%,16 and is usually asymptomatic, as inthe case presented here.
Brain parenchyma involvement may present multiplelesions (35%) or single lesions (10%) analyzed in the MRIcontrast phase.19 The MRI is the most sensitive test for thediagnosis of neurosarcoidosis, but a normal examinationdoes not rule out the diagnosis, especially if the patient isunder corticosteroid treatment. In MRI with contrast, lep-tomeningeal involvement is observed in 40% of the cases, andit is more common in the frontobasal and suprasellar re-gions.5,19 The CSF may present hyperproteinemia in 73% ofthe patients and lymphocytosis in 55%; normal CSF isuncommon.2,5,11
The non-caseating granuloma of sarcoidosis has immu-nological origin, and is formed by giant cells and epithelioidcells (consisting of histiocytes modified by T lymphocytes).The presence of giant and epithelioid cells is a sign of highcellular turnover. Granulomas are uniform, and have as theircomponents histiocytes of broad and eosinophilic cyto-plasm, oval or twisted vesicular nucleus, and prominentnucleoli.4,13,21 Fibrinoid necrosis is present in 35% of thecases.21
As radiological differential diagnoses we could mentionglioblastoma, lymphoma, abscess, metastasis and even var-iations of multiple sclerosis. Nevertheless, among the lesionsthat can affect the skull and brain, we can list metastasis,lymphoma; primary skull tumors, such as chondrosarcoma,chordoma, esthesioneuroblastoma andmalignant histiocytictumor; and tumor-like lesions, such as fibrous dysplasiaeosinophilic granuloma.22,23
The treatment is clinical, with prednisolone 40–80 mg(oral administration) at first; as an alternative for moresevere cases, intravenous methylprednisolone can beused.9 In case of refractoriness, there are options such as:mycophenolate, methotrexate, cyclophosphamide, azathio-prine, chloroquine and tumor necrosis factor alpha (TNF-α);7
another alternative is radiotherapy.15 In cases of systemicsuspicion of neurosarcoidosis, stereotactic biopsy can beused for confirmation.7
Conclusion
Neurosarcoidosis is a serious and rare condition. The dis-cussed case presented a single extracranial alteration:asymptomatic pulmonary bronchiectasis located in an atyp-ical region. The intracranial manifestations presented were:lytic bone lesion and psychiatric symptoms (rare occurrencein the literature). Thus, this case may contribute to thediagnosis of other cases with rare presentation.
Disclosure – Conflicts of InterestAuthors declare no conflicts of interest.
Table 1 Percentages of neurological signs and symptoms
Peripheral mononeuropathy 69%
Depression 60–66%
Stress 55%
Cranial nerve 50%
Headache 17–48%
Myelopathy 16–43%
Polyradiculoneuropathy 39%
Hydrocephalus 5–38%
Meningeal disease 10–20%
Seizures 15%
Osseous involvement 13%
Table 2 Differential diagnoses
Involvement of brainparenchyma
Meningeal involvement
Multiple sclerosis Bacterial meningitis
Cerebral metastasis Tuberculous meningitis
Cerebral lymphoma Carcinomatous meningitis
Neurotuberculosis Meningioma
Fungal infections of the brain Leukemic infiltration
Low- and high-grade glioma Meningeal plasmacytoma
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Neurosarcoidosis Associated with Psychiatric Symptoms Neves et al.188

References1 Vinas FC, Rengachary S. Diagnosis and management of neurosar-
coidosis. J Clin Neurosci 2001;8(06):505–5132 Agnihotri SP, Singhal T, Stern BJ, Cho TA. Neurosarcoidosis. Semin
Neurol 2014;34(04):386–3943 Celebi A, Deveci S, Gursoy AE, Kolukisa M. A case of isolated
neurosarcoidosis associated with psychosis. Neurosciences(Riyadh) 2013;18(01):70–73
4 Daldon PEC, Arruda LHF. Noninfectious granulomas: sarcoidosis.An Bras Dermatol 2007;82(06):559–571
5 Nozaki K, Judson MA. Neurosarcoidosis: Clinical manifestations,diagnosis and treatment. Presse Med 2012;41(6 Pt 2):e331–e348
6 Rybicki BA, Iannuzzi MC. Epidemiology of sarcoidosis: recentadvances and future prospects. Semin Respir Crit Care Med2007;28(01):22–35
7 Terushkin V, Stern BJ, Judson MA, et al. Neurosarcoidosis: pre-sentations and management. Neurologist 2010;16(01):2–15
8 Gonzalez-Granado LI. Reply: Presentations and outcomes of neu-rosarcoidosis: a study of 54 cases. QJM 2009;102(12):889–891
9 Nowak DA, Widenka DC. Neurosarcoidosis: a review of its intra-cranial manifestation. J Neurol 2001;248(05):363–372
10 RadwanW, Lucke-Wold B, Robadi IA, Gyuri K, Roberts T, Bathia S.Neurosarcoidosis: unsual presentations and considerations fordiagnosis and management. Postgrad Med J 2017;93:401–405
11 Besur S, Bishnoi R, Talluri SK. Neurosarcoidosis: rare initial pre-sentation with seizures and delirium. QJM 2011;104(09):801–803
12 Carlson ML, White JR Jr, Espahbodi M, et al. Cranial base mani-festations of neurosarcoidosis: a review of 305 patients. OtolNeurotol 2015;36(01):156–166
13 Manz HJ. Pathobiology of neurosarcoidosis and clinicopathologiccorrelation. Can J Neurol Sci 1983;10(01):50–55
14 Skowasch D, Pabst S, Wilhelm K, Grohé C. [Diabetes insipidus dueto neurosarcoidosis]. Pneumologie 2011;65(08):496–497
15 Joseph FG, Scolding NJ. Sarcoidosis of the nervous system. PractNeurol 2007;7(04):234–244
16 Smith JK, Matheus MG, Castillo M. Imaging manifestations ofneurosarcoidosis. AJR Am J Roentgenol 2004;182(02):289–295
17 Stjepanović MI, Vucinić VM, Jovanović D, Mijajlović M, TrifunovićVS, Stjepanović MM. Diagnosis of neurosarcoidosis–necessity ofbiopsy. Med Pregl 2014;67(3-4):97–99
18 Sakuta M, Kumamoto T, Iizuka T, Nishiyama K, Oritsu M. [Diag-nostic criteria of neurosarcoidosis]. No To Shinkei 2006;58(06):471–476
19 Bathla G, Singh AK, Policeni B, Agarwal A, Case B. Imaging ofneurosarcoidosis: common, uncommon, and rare. Clin Radiol2016;71(01):96–106
20 Nobrega BB, Meirellis GSP, Szarf G, Jasinowodolinski D, KavakamaJI. Pulmonary sarcoidosis: High-resolution computed tomogra-phy findings. J Bras Pneumol 2006;31(03):254–260
21 Mitchell DN, Scadding JG, Heard BE, Hinson KF. Sarcoidosis:histopathological definition and clinical diagnosis. J Clin Pathol1977;30(05):395–408
22 Ciarpaglini R, Otten P. Primary cranial vault lymphomawith braininfiltration: case report and review of the literature. Br J Neuro-surg 2012;26(05):756–758
23 Stark AM, Eichmann T, Mehdorn HM. Skull metastases: clinicalfeatures, differential diagnosis, and review of the literature. SurgNeurol 2003;60(03):219–225, discussion 225–226
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Neurosarcoidosis Associated with Psychiatric Symptoms Neves et al. 189

Anconeus Epitrochlearis Muscle as a Cause ofUlnar Nerve Compression at the Elbow
Músculo anconeu epitroclear como causa de compressãodo nervo ulnar no cotovelo
Luiz Fernando Cannoni1 Luciano Haddad1
1Neurológika Ltda, São Paulo, SP, Brazil
Arq Bras Neurocir 2017;36:190–193.
Address for correspondence Luiz Fernando Cannoni, PhD, RuaConselheiro Cotegipe, 543, Belenzinho, São Paulo, SP, CEP 03058-000,Brazil (e-mail: [email protected]).
Keywords
► ulnar nerve disease► ulnar neuropathy
Abstract Ulnar nerve entrapment is the second most common compressive neuropathy in theupper limb, after carpal tunnel syndrome (Dellon, 1986). One of the causes that mustbe considered is the accessory anconeus epitrochlearis muscle, which is present in 4%to 34% of the general population (Husarik et al, 2010; Vanderpool et al, 1968; Nellanset al, 2014).We describe a patient with symptoms of compression of the left ulnar nerve at theelbow and the result of the surgical treatment.The patient presented with hypoesthesia in the fourth and fifth fingers of the left hand,and reduction of strength in the fifth finger abduction. No alterations were found in thethumb adduction.Initially, the treatment was conservative (splint, physiotherapy, analgesics); surgicaltreatment was indicated due to the continuity of the symptoms.The ulnar nerve was surgically released and transposed, with complete recovery after6 months of follow-up.Ulnar nerve entrapment at the elbow by the anconeus epitrochlearis muscle is notcommon, but it must not be ignored (Chalmers, 1978). Ultrasonography (Jung et al,2013; Bargalló et al, 2010), elbowmagnetic resonance imaging (MRI) (Jeon, 2005), andelectromyography (Byun, 2011) can help establish the proper diagnosis.
Resumo A compressão do nervo ulnar é a segunda causa mais frequente de neuropatiacompressiva no membro superior, após a síndrome do túnel do carpo (Dellon,1986). Uma das causas que dever ser considerada é a presença do músculo anconeuepitroclear, que está presente em cerca de 4% a 34% da população (Husarik et al, 2010;Vanderpool et al, 1968; Nellans et al, 2014).Descrevemos uma paciente com sintomas de compressão do nervo ulnar esquerdo nocotovelo, e o resultado do tratamento cirúrgico.
receivedMay 31, 2017acceptedJuly 17, 2017published onlineAugust 28, 2017
DOI https://doi.org/10.1055/s-0037-1606276.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Case Report | Relato de Caso190

Introduction
Ulnar nerve entrapment is the secondmost common compres-siveneuropathyaftercarpal tunnel syndrome.1Theulnarnervecan be compressed at various points along its trajectory, butmost cases are localized on the elbow and the Guyon canal.10
Of the many causes of ulnar neuropathy, the most com-mon are traumatic and idiopathic in nature. The anconeusepitrochlearismuscle,first described by Scafer and Schaeffer,is a well-known, but rare cause of ulnar nerve entrapment atthe elbow.2 This muscle is present in 4% to 34% of the generalpopulation.1,3,11
Theanconeusepitrochlearis isananomalousmusclelocatedbetween the medial aspect of the ulnar olecranon and themedial epicondyle, and it is found inup to28%ofcadavers.1Theauthors report thecaseofa34-year-oldwomanwitha6-monthhistory of left elbow pain and distal motor and sensorysymptoms affecting her daily activities and quality of life. Aftera conservative treatment that included physiotherapy and theuse of a splint, and of analgesic and anti-inflammatory drugs,surgical excision of themuscle and decompression of the ulnarnerve was proposed.
The patient agreed to the disclosure of all data (includingsurgical pictures), signing the informed consent form. Noneof the authors had conflicts of interest.
Case Report
We describe the case of a 34-year-old female patient, a right-handed secretary who presented pain at the left forearm for6 months, followed by progressive sensitive and motordisturbances on the medial side of the left forearm. Shehad spent years answering telephone calls supporting herleft elbow on the table.
The patient presented hypoesthesia in the fourth and fifthfingers, and reduction of strength in thefifth finger abduction.Numbness and tingling were localized to the ulnar side of theforearm and the two ulnar side digits. Upon physical examina-tion, she had a positive Tinel sign on the medial surface of theelbow. Froment signwas also present. We did not observe anyalteration in the function of the abduction of the left thumb.
She was submitted to magnetic resonance imaging (MRI),radiography and electromyography (EMG) of the left elbow
to confirm the diagnosis. The EMG described compression ofthe nerve in the ulnar groove, with conduction block and alarge drop in nerve conduction velocity. Plain radiographs ofthe left upper limb were normal.
TheMRI showed ulnar nerve compression at the elbow bythe anconeus epitrochlearis muscle (►Fig. 1).
After a period of conservative treatment, surgical treat-ment was indicated and performed through a medial epi-condylar incision, with division of the anconeusepitrochlearis muscle (►Fig. 2), release of the ulnar nerve,and preservation of the branches to the flexor carpi ulnaris.The resection of the muscle is shown in ►Fig. 3
Nerve transposition to subcutaneous fatty tissue was per-formedwithout epicondylectomy. Recoveryof bothmotor andsensory nerve functions can be achieved if the source ofcompression is an anomalousmuscle that is treatedwith earlysurgical removal.9,12 In the follow-up period (6 months), thepatient was fully recovered.
This patient also complained about the symptomatology inthe right side, with a confirmed right anconeus epitrochlearismuscle by MRI, but on this side, the symptoms were verysmooth, leading to a conservative treatment.
A paciente apresentava hipoestesia no IV e V dedos da mão esquerda, e diminuição deforça na abdução do V dedo; não foram encontradas alterações na adução do polegar.Inicialmente, o tratamento foi conservador (uso de splint, fisioterapia e analgésicos); acirurgia foi indicada pela persistência dos sintomas.O nervo ulnar foi cirurgicamente liberado e transposto, com melhora total dossintomas após 6 meses de acompanhamento.A compressão do nervo ulnar no cotovelo não é comum, mas não deve ser ignorada(Chalmers, 1978). Ultrassonografia (Jung et al, 2013; Bargalló et al, 2010), ressonânciamagnética do cotovelo (Jeon, 2005) e eletromiografia (Byun, 2011) auxiliam nodiagnóstico.
Palavras-chave
► lesões do nervo ulnar► patologia do nervo
ulnar
Fig. 1 MRI of the left elbow depicting the ulnar nerve (blue arrow)and the anconeus epitrochlearis muscle (yellow arrow).
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Ulnar Nerve Compression by Anconeus Trochlearis Muscle Cannoni, Haddad 191

Anconeus Epitrochlearis Muscle
The anconeus epitrochlearis muscle is an accessory muscle ofthemedial elbow thatoriginates fromthemedial epicondyleofthe humerus and inserts on the olecranon process of the ulna,and as an extension of themedial head of the triceps brachii.12
Anatomical variations in forearm muscles are typicallyasymptomatic and discovered by chance.10–12 However, theanconeus epitrochlearismuscle is anatomically distinct fromthe triceps and is innervated by the ulnar nerve.12
This muscle is often present is animals with shoulderadduction. It is found in amphibians, reptiles and mostmammals. In mammals, it adducts and extends the elbow,supinates the forearm, and protects the ulnar nerve. Its mainrole in humans is to protect the ulnar nerve frommechanicalpressure during elbow extension; it likely assists the tricepswhile preventing ulnar nerve subluxation.12
The incidence of this muscle ranges from 4% to 34% invarious anatomical studies.2,3 When present, it is often bilat-eral,7 as it was in the case reported here. Although themusclehas nearly equal presence in both genders and on both sides ofthebody, it ismoreprevalentanddevelopedontheright side inmen, and on left side inwomen.7 It represents a cause of ulnar
nerve entrapment at the elbow, that must be considered indifferencial diagnose.5 It must be kept in mind that ultra-ssonography6,7 magnetic resonance image of the elbow8 andelectromyography9 can help in the diagnosis.
Surgical Technique
Given the lack of improvement of the symptoms after theconservative treatment, surgical decompression of the ulnarnervewasproposed.Thesurgerywasperformedundergeneralanesthesia. Thepatient had an anconeus epitrochlearismusclethat was observed after an MRI of the left elbow (►Fig. 1).
The muscle was dissected off the medial epicondyle(►Figs. 2 and 3), and the ulnar nervewas found underneath it.
Discussion
Ulnar neuropathy as a result of the presence of an anconeusepitrochlearis muscle is rarely reported in young patientswithout congenital elbow anomalies.
Complete excision of the muscle is widely accepted asdefinitive treatment, but whether or not to transpose theulnar nerve remains controversial.13
Byun et al9 discussed the electromyographic findings inpatients with ulnar neuropathy from anconeus epitrochlearismuscles compared with those with idiopathic cubital tunnelsyndrome. They suggested that there should be a high suspi-cion of an accessory muscle as the cause of the compressionrather than a more traditional cause when a relatively youngpatient presents with rapid onset of symptoms.
Furthermore, it was shown that edema in themuscle bellyof the anconeus epitrochlearis visualized on MRI is oftenassociated with ulnar nerve compression and neuritis.8
Ulnar neuropathy as a result of the presence of theanconeus epitrochlearis muscle usually has characteristicsthat are different from idiopathic disease, including youngerage at onset, more rapid progression with a short duration ofsymptoms, distinct neurophysiology with velocity drop orconduction block of the ulnar nerve, and edema of theanconeus epitrochlearis muscle upon MRI.8
In a comparative study with idiopathic ulnar neuropathy,thevelocitydropof theulnarnervewassignificantlyassociatedwith the presence of an anconeus epitrochlearis muscle.9
Conclusion
Although rare, the presence of the anconeus epitrochlearismuscle should be considered as a potential cause of ulnarneuropathy at the elbow, especially in young female patientswith a rapid progression of symptoms.
Conflicts of InterestAuthors declare no conflicts of interest.
References1 Dellon AL. Musculotendinous variations about the medial hum-
eral epicondyle. J Hand Surg [Br] 1986;11(02):175–181
Fig. 2 Exposition of the ulnar nerve (blue arrow) under the anconeusepitrochlearis muscle (yellow arrow).
Fig. 3 Resection of the anconeus epitrochlearis muscle.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Ulnar Nerve Compression by Anconeus Trochlearis Muscle Cannoni, Haddad192

2 Husarik DB, Saupe N, Pfirrmann CWA, Jost B, Hodler J, Zanetti M.Ligaments and plicae of the elbow: normalMR imaging variabilityin 60 asymptomatic subjects. Radiology 2010;257(01):185–194
3 Vanderpool DW, Chalmers J, Lamb DW, Whiston TB. Peripheralcompression lesions of the ulnar nerve. J Bone Joint Surg Br 1968;50(04):792–803
4 NellansK,GaldiB, KimHM,LevineWN.Ulnarneuropathyas a resultof anconeus epitrochlearis. Orthopedics 2014;37(08):e743–e745
5 Chalmers J. Unusual causes of peripheral nerve compression.Hand 1978;10(02):168–175
6 Jung JH, Kim KH, Choi SK, Shim JH. Usefulness of ultrasound fordetecting suspected peripheral nerve lesions in diagnosis ofperipheral neuropathy: case report and brief review of theliterature. J Korean Neurosurg Soc 2013;53(02):132–135
7 Bargalló X, Carrera A, Sala-Blanch X, et al. Ultrasound-anatomiccorrelation of the peripheral nerves of the upper limb. Surg RadiolAnat 2010;32(03):305–314
8 Jeon IH, Fairbairn KJ, Neumann L, Wallace WA. MR imaging ofedematous anconeus epitrochlearis: another cause of medialelbow pain? Skeletal Radiol 2005;34(02):103–107
9 Byun SD, Kim CH, Jeon IH. Ulnar neuropathy caused by ananconeus epitrochlearis: clinical and electrophysiological find-ings. J Hand Surg Eur Vol 2011;36(07):607–608
10 Hirasawa Y, Sawamura H, Sakakida K. Entrapment neuropathydue to bilateral epitrochleoanconeus muscles: a case report.J Hand Surg Am 1979;4(02):181–184
11 Masear VR, Hill JJ Jr, Cohen SM. Ulnar compression neuro-pathy secondary to the anconeus epitrochlearis muscle. J HandSurg Am 1988;13(05):720–724
12 O’Hara JJ, Stone JH. Ulnar nerve compression at the elbow causedby a prominent medial head of the triceps and an anconeusepitrochlearis muscle. J Hand Surg [Br] 1996;21(01):133–135
13 Macnicol MF. The results of operation for ulnar neuritis. J BoneJoint Surg Br 1979;61-B(02):159–164
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Ulnar Nerve Compression by Anconeus Trochlearis Muscle Cannoni, Haddad 193

Patient with Recurrent GlioblastomaResponding Favorably to Ketogenic DietCombined with Intranasal Delivery of PerillylAlcohol: A Case Report and Literature Review
Paciente com glioblastoma recorrente respondendopositivamente a dieta cetogênica combinada a álcoolperílico intranasal: relato de caso e revisão da literatura
Juliana Guimarães Santos1 Wanise Maria Souza Da Cruz2 Axel H. Schönthal3
Marcela D'alincourt Salazar4 Cristina Asvolinsque Pantaleão Fontes5 Thereza Quirico-Santos6
Clovis Orlando da Fonseca7
1Graduate Program in Medical Sciences, Universidade FederalFluminense, Niteroi, RJ, Brazil
2Department of Nutrition, Universidade Federal Fluminense, Niteroi,RJ, Brazil
3Department of Molecular Microbiology & Immunology, Keck Schoolof Medicine, University of Southern California, Los Angeles, USA
4Department of Experimental Therapeutics, Beckman ResearchInstitute of City of Hope, Duarte, CA91010, USA
5Service of Radiology, Department of Radiology, Antonio Pedro UniversityHospital, Universidade Federal Fluminense, Niteroi, RJ, Brazil
6Department of Cellular and Molecular Biology, Institute of Biology,Universidade Federal Fluminense, Niteroi, RJ, Brazil
7Service of Neurosurgery, Department of General and SpecializedSurgery, Antonio Pedro University Hospital, Universidade FederalFluminense, Niteroi, RJ, Brazil,
Arq Bras Neurocir 2017;36:194–199.
Address for correspondence Juliana Guimaraes Santos, MSc, MD,Universidade Federal Fluminense, Niterói, Rio de Janeiro, Brazil(e-mail: [email protected]).
Keywords
► ketogenic diet► perillyl alcohol► intranasal
administration► glioblastoma
multiforme► combination therapy► drug resistance
Abstract Introduction Monoterpene perillyl alcohol (POH) is cytotoxic to temozolomide-resistant glioma cells, regardless of its O6-methylguanine-methyltransferase (MGMT)promoter methylation status. Moreover, adherence to a ketogenic diet (KD) producedsuccessful outcomes in preclinical and clinical studies in the glioma setting.Case Presentation A 54-year-old Caucasian man had a confirmed diagnosis ofrefractory glioblastoma multiforme (GBM). The immunohistochemical evaluationwas negative for methylation, and failed to detect mutations in the isocitratedehydrogenase (IDH) 1 and 2 genes. In January 2016, the patient was enrolled in aclinical trial combining daily intranasal delivery of POH in combination with a KD. TheKDwas administered concomitantly with inhalation of POH (55 mg, 4 times a day) in anuninterrupted administration schedule for 3 months.
receivedJune 1, 2017acceptedJuly 11, 2017published onlineAugust 10, 2017
DOI https://doi.org/10.1055/s-0037-1605588.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Case Report | Relato de Caso194

Introduction
Glioblastoma multiforme (GBM) is the most commonmalig-nant primary brain tumor. Despite standard-of-care therapyconsisting of surgery and chemoradiation therapy, the dis-ease relapses in most patients, and the median survival isonly of � 15 months.1 One of the major mechanisms ofdisease relapse in GBM patients has been attributed to theenhanced ability of poorly differentiated glioma cells toinvade and infiltrate surrounding healthy tissue.2,3 In thisaspect, the vicinity and extension of the peritumoral edema(PTE) can be useful to predict clinical outcomes in patientswith a newly-diagnosed malignant glioma.4
Epilepsy develops in around 30–50% of patients withbrain tumors as a consequence of the brain swelling due tothe edema accompanying the lesion. Epilepsy is a debilitating
condition that causes distress and adversely affects thepatient’s quality of life.5,6 Antiepileptic drugs are commonlyused to treat these patients; however, such treatments areknown to exert detrimental neuropsychological effects andoften interact with the therapeutic regimen, such as chemo-therapeutic agents.5,7 Several studies have attempted toaddress this issue by analyzing how changes in the peritu-moral tissue correlate with the onset of seizures in patientswith brain tumors. Mounting evidence suggests that epilep-togenesis correlates with metabolic alterations, acidosis anddisruption of localized neural networks in the tumoral andperitumoral areas of the brain.8,9
Recent studies have suggested that consumption of a keto-genic diet (KD)might play a role in improving the outcomes ofcancer patients undergoing treatment and in minimizing thefrequencyof epileptic episodes.10–13 The typical KD consists of
Results The combination treatment was well-tolerated. The nutritional status andanthropometric measurements of the patient were measured. Adherence to the KDwas confirmed by measuring the levels of ketone bodies in the urine. Throughout thetreatment, a reduced frequency of seizures was observed. After three months ofadherence to the treatment, the patient presented with weight loss, reduced body fat,increased water retention, and a slight increase in bone and muscle mass. A follow-upmagnetic resonance imaging (MRI) scan after 3 months of treatment revealed markedreduction of the enhancing lesion.Conclusion Intranasal delivery of POH combinedwith concomitant adherence to a KDappeared to have a beneficial therapeutic effect in a patient with recurrent GBM.Further studies are needed to evaluate the efficacy of this therapeutic strategy in alarger cohort of treatment-refractory GBM patients.
Palavras-chave
► dieta cetogênica► álcool perílico► administração
intranasal► glioblastoma
multiforme► tratamento
combinado► resistência
medicamentosa
Resumo Introdução O monoterpeno álcool perílico (AP) é citotóxico para linhagens celulares deglioblastoma, independentemente do status do promotor de metilação O6-metilguanina-metiltransferase (MGMT).Alémdisso, a adesão àdieta cetogênica (DC) produziu resultadosbem sucedidos em desenho de estudos pré-clínicos e clínicos de glioma.Relato de Caso Homem, 54 anos, caucasiano, com diagnóstico de glioblastomamultiforme (GBM) recidivo. A avaliação imuno-histoquímica foi negativa para metila-ção e não detectou mutações do gene da isocitrato desidrogenase 1 e 2 (IDH1 IDH2). Emjaneiro de 2016, o paciente foi inscrito em um ensaio clínico da administraçãointranasal diária do AP combinada a DC. A DC foi administrada concomitantementecom inalação de AP (55 mg, 4 vezes ao dia) em um cronograma de administraçãoininterrupto durante 3 meses.Resultados O tratamento combinado foi bem tolerado. O estadonutricional e asmedidasantropométricas do paciente foram avaliadas. Aderência a DC foi confirmada pela presençade corpos cetônicos na urina. Ao longo do tratamento, observou-se redução da frequênciade convulsões. Após três meses de adesão ao tratamento, o paciente apresentou perda depeso, redução da gordura corporal, melhor hidratação e um aumento discreto da massaóssea e muscular. O acompanhamento da ressonância magnética após 3 meses detratamento revelou redução acentuada do volume da lesão.Conclusão A administração intranasal do AP combinada a DC sugere ter um efeitoterapêutico benéfico em pacientes com GBM recorrente. São necessários mais estudospara avaliar a eficácia desta estratégia terapêutica em uma coorte maior de pacientescom GBM refratários.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Ketogenic diet combined with intranasal delivery of perillyl alcohol for recurrent GBM Santos et al. 195

low amounts of carbohydrates, moderate amounts of protein,and high amounts of fat, aimed at stimulating fat metabolismwhile minimizing sugar availability. Adherence to a KD pro-motes a unique metabolic state resulting from elevated levelsof fat-derived ketone bodies and lower levels of blood sugar,which have been correlated with improved outcomes inpatients with diabetes, cancer and certain neurological dis-orders.10,14,15 In addition, KDs have shown to reduce thefrequency and severity of seizures in epileptic patients.12,16
In the context of cancer, KDs are presumed to counteractthe Warburg effect by depriving tumor cells of glucose andimproving mitochondrial activity.10,17 The Warburg effect ischaracterized by a metabolic shift from aerobic respirationtoward increased glycolysis and lactate production, despitethe availability of oxygen (aerobic glycolysis).18,19 Impor-tantly, a major consequence of the Warburg effect is theincreased cellular consumption of glucose as themain sourceof energy. Nevertheless, this glycolytic dependency mayprovide an opportunity for therapeutic intervention, basedon the assumption that a reduction in glucose availabilitymay lead to a decline in proliferation andmetastatic capacity,along with increased sensitivity to cytotoxic or targetedtherapies.13,19,20 The shift in the ratio of ketone bodiesover glucose is disadvantageous to tumor cells, since glu-cose-addicted cancer cells are less likely to utilize ketonebodies for energy, in contrast to normal cells, which cangenerate energy from either source.21
Emerging evidence indicates that KDsmay have beneficialeffects in patients with malignant glioma. Results from astudy in which adherence to a KD was combined withstandard chemoradiotherapy in a patient with GBM havedemonstrated that the patient went into complete remissionwhile presenting with reduced blood glucose levels.22 Sub-sequent case reports investigating this regimen have alsoshown a correlation between reduced serum glucose levelsand improved therapeutic responses.16,17,23 Altogether,there is intriguing evidence correlating KD and metabolicreprogramming with improved therapeutic responses tostandard-of-care regimens for the treatment of patientswith malignant glioma.13,17 We have published extensivelyon the antitumor effects of perillyl alcohol (POH), a naturallyoccurringmonoterpene related to limonene, in patients withrecurrentmalignant glioma. A significant proportion of thesepatients, who had presented with tumors refractory tostandard chemoradiotherapy, responded favorably to theintranasal delivery of POH.24–26
At the molecular level, reduced glucose availability maycause endoplasmic reticulum (ER) stress, which triggers theunfolded protein response (UPR) cellular process, consistingof an interplay of antagonistic mechanisms; the low tomoderate activity is cell-protective and supports chemoresistance, but more severe conditions aggravate thesemechanisms to the point in which the protective effortsare abandoned, and the cell death program is inducedinstead.27 As tumor cells frequently experience chronicstress conditions (due to hypoxia, hypoglycemia, acidifica-tion, oxidative stress, etc.), the protective components oftheir ER stress response are continuously engaged and thus,
less able to neutralize additional insults that trigger the ERstress response.28,29 The ER stress/UPR process has beendescribed as a potential therapeutic target in GBM,30 andthis cellular mechanism has been demonstrated to be tar-geted by POH in GBM cells in vitro.31,32 It is thus conceivablethat the concerted effect of KD-induced hypoglycemia to-gether with POH-induced responses may trigger severelyaggravated ER stress, resulting in tumor cell apoptosis.22
Based on our successful results in the clinical setting, weare now investigating whether adherence to a KD duringtreatment with intranasal POH can further improve thetherapeutic outcomes of glioma patients. In this manuscript,we report a case study of an adult patient with recurrentglioblastoma treated with this regimen.
Case Presentation
The present study was approved by our university (CAAE:14613313.8.0000.5243), and was performed at the univer-sity hospital. The patient signed a written informed con-sent form prior to enrolling in the clinical trial combiningKD with intranasal delivery of POH to assess the thera-peutic efficacy of this regimen. The POH was formulatedfor intranasal delivery, and the preparation was suppliedby a multidisciplinary laboratory of Pharmaceutical Scien-ces at the Universidade Federal do Rio de Janeiro, accord-ing to BR Patent Number PI 0107262–5. The KD wasadministered concomitantly with daily inhalation ofPOH for three months. Perillyl alcohol (55 mg; 0.3% v/v)was administered by inhalation 4 times a day, totaling266.8 mg/a day.
A 54-year-old Caucasian man with no significant pastmedical record or family history of brain tumor or neuro-logical disorders presented with a seizure in Septem-ber 2014. A magnetic resonance imaging (MRI) brain scanrevealed a regular space-occupying lesion in the left tem-poral-parietal lobe that was enhanced with gadolinium. Thepatient underwent a left temporal craniotomy with radicalresection of the primary brain tumor in January 2015.Following surgery, tumor resection was confirmed by anMRI scan. The diagnosis of malignant glioma was confirmedbased on complex histological features characterized byischemicnecrosis andglomeruloidmicrovascular proliferation.
The immunohistochemical analysis was negative forO6-methylguanine-methyltransferase (MGMT)methylation,and failed to detect mutations in the isocitrate dehydroge-nase (IDH) 1 and 2 genes. The patient underwent concomi-tant radiation therapy (59.4 Gy total) with chemotherapy(temozolomide [TMZ] 75 mg every day for 6 weeks). Then,after the conclusion of the radiation therapy, during theadjuvant phase, the patient received TMZ (150–200 mg)on a 28-day cycle with 5 days on and 23 days off for 3 cycles.In addition, the patient was treated for seizures andremained asymptomatic for eight months. At this moment(September 2015) the patient presented with complaints ofdizziness and headache. A new brain MRI revealed thepresence of a left temporalmasswith an intense surroundingvasogenic edema. The patient underwent an additional cycle
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Ketogenic diet combined with intranasal delivery of perillyl alcohol for recurrent GBM Santos et al.196

of TMZ treatment, but a new MRI scan showed no reduc-tion in the tumor lesion. The treatment was withdrawn inDecember 2015 because the patient was refractory to it, andpresented clinical adverse effects (headache, thrombocyto-penia, seizures), with an MRI scan showing no reduction inthe tumoral lesion, and the patient was then consideredout of therapeutic possibilities and referred to supportive(palliative) treatment. In January 2016, the patient was thenenrolled in the clinical trial with KD in combination withintranasal delivery of POH.
The anthropometric and biochemical status of the patientwas assessed at the time of inclusion in the study. The KDwasprescribed according to the following distribution: energy(25 kcal/kg); 1.5 g/kg protein; 25% carbohydrate; and50% lipids (cholesterol �200 mg/day; saturated fat < 7%;polyunsaturated fat < 10%, monounsaturated fat < 20%,and fibers between 20–30 g/day).33 The levels of ketonebodies in the urine were measured (15 mg/dl), and con-firmed the adherence to the KD. The KD was well-tolerated,without relevant changes in nutritional status, and no ad-verse symptoms were reported. The levels of ketone bodiesremained between 5–15 mg/dl throughout the duration ofthe treatment. A complete list of the parameters analyzedbefore and 3 months after adherence to the KD are shown in(►Table 1).
At the end of the study, the patient presented with aweight loss of 4.36%; a decrease in body fat of 8.5%, especiallyin the abdominal region (↓ 10 cm waist circumference[WC]); an 8.8%-increase in water retention; and increases
in bonemass (2%) andmuscle mass (1%). The KD reduced thetotal cholesterol level, the low-density lipoprotein (LDL)cholesterol and the triglycerides levels, improving the lipidprofile, although it also reduced the high-density lipoprotein(HDL) cholesterol level. The fasting blood glucose levels didnot change (►Table 1).
A follow-up MRI scan conducted after 3 months of KDcombined with intranasal POH therapy revealed markedreduction of the enhancing lesion (►Fig. 1) and significantclinical improvement. At three months after the completionof the therapeutic regimen, the patient was still beingtreated with low dose anti-seizure medication but no steroi-dal drugs. There were no signs of delayed toxicity or adverseevents caused by the combined KD/intranasal POH treat-ment (data not shown).
Discussion
Herein we report a case study of a patient with recurrentGBM that has been successfully treated with KD concomi-tantly with POH inhalation for three months without anyside effects. As a result, the patient showed tumor regressionand reduced peritumoral edema, which led to an overallimprovement in quality of life and lower frequency ofseizures.
The severity of the peritumoral brain edema significantlyinfluences the glioma prognosis by promoting tumor cellinvasion and increasing morbidity.4,25 Increased diffusion ofextracellular matrix components rich in proteases and
Table 1 Anthropometric and biochemical parameters before and after KD
Parameters Before KD Results After KD Results
Body mass (kg) 68.7 ��� 65.7 ↓ 3 kg; ↓4.4%
BMI (kg/m2) 23.7 eutrophic 22.7 eutrophic
WC (cm) 90.5 no risk of metaboliccomplications
80 no risk of metabolic complications
AC (cm) 30.5 94.4% (eutrophic) 27.5 85.1% (mild thinness)
TS (cm) 10 83.3% (mild thinness) 8 66.7% (severe thinness)
AMC (cm) 27.4 97.5% (eutrophic) 25 89% (mild thinness)
Biochemical Tests Before KD After KD Reference Values
Total cholesterol (mg/dL) 211 mg/dL 170 mg/dL normal range < 200 mg/dLa
LDL cholesterol (mg/dL) 113 mg/dL 93 mg/dL normal range < 100 mg/dLa
HDL cholesterol (mg/dL) 80 mg/dL 61 mg/dL normal range > 60 mg/dLa
Triglycerides (mg/dL) 92 mg/dL 81 mg/dL normal range < 150 mg/dLa
Fasting glucose (mg/dL) 77 mg/dL 74 mg/dL normal range < 100 mg/dLb
Urine ketone bodies negative positive positive (5–150 mg/dL)
Abbreviations: AC, arm circumference (men age 50–54.9 years, P50 at 32.3 cm); adequacy percentage of normal range 90–110%; mild thinness80–90% (NHANES II); AMC, arm muscle circumference (men aged 45–54.9 years, P50 at 28.1 cm); adequacy percentage of normal range > 90%;mild thinness ¼ 90% (NHANES II); BMI, body mass index (normal range (18.5–24.9); (WHO, 1995; WHO, 1997); HDL, high-density lipoprotein; KD,ketogenic diet; LDL, low-density lipoprotein; TS, triceps skinfold (men age 50–54.9 years, P50 at 12cm); adequacy percentage of normal range90–110%; severe thinness < 70% (NHANES II), WC, waist circumference (men increased risk of metabolic complications � 94 cm); AssociaçãoBrasileira para Estudo da Obesidade e SíndromeMetabólica (ABESO, 2009).4,5
Notes: Biochemical tests: aV Brazilian Guideline to Dyslipidemias and Prevention of Atherosclerosis (2013); bBrazilian Guideline to Diabetes2015–2016 (2015) Urine ketone bodies: ChoiceLine 10 Urinalysis – Roche.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Ketogenic diet combined with intranasal delivery of perillyl alcohol for recurrent GBM Santos et al. 197

tumor-derived growth factors into the peritumoral stromaduring tumor progression further modifies the microenvi-ronment and promotes neovascularization.34 Since the re-duction in the peritumoral edema in animals that were fedthe KD appears to be correlated with a decrease in theexpression levels of several proteins involved in malignantprogression, adherence to a KD might also represent arelevant tool to halt tumor progression.35 Our results show-ing a marked reduction in the peritumoral edema followingour therapeutic regimen combining the administration of aKD and intranasal POH were encouraging and consistentwith the literature, suggesting that the extent of the peritu-moral edema may impact the overall survival in patientswith GBM.2,36
Moreover, our results demonstrating a reduction in thefrequency of seizure episodes in a patient with recurrentGBM following combined administration of the KD andintranasal POH are consistent with an increasing body ofdata demonstrating the value of using a KD to managepatients with intractable epilepsy.12,37 Importantly, seizuresare often refractory to medication in patients with GBM, andcan persist after surgery.8 This is a major concern in themanagement of patients with GBM, as epilepsy develops in29–49% of the patients diagnosed with brain tumors.7,38 Inthis context, tumor-related epilepsy is a condition thatrequires an integrated treatment approach due to the sever-ity of the disease.39 An adequate high-fat, low-carbohydrate,protein-based KD might be useful in the treatment andmanagement of brain tumors because it appears to interferewith key epileptogenic mechanisms involving changes in pH,neurotransmitters, ion levels, and in the expression of volt-age-dependent channels and receptors in the tumoral andperitumoral brain tissues.9,21
Overall, the results of this study demonstrated that the KDwas well-tolerated and compatible with previous clinicalfindings. The KD-induced hypoglycemia can potentially bean adjuvant to standard treatments, such as surgery andchemoradiation, and also possibly to novel regimens, such asintranasal POH, in the recurrence setting.
Conflicts of InterestAuthors have no conflicts of interest.
References1 Stupp R, Mason WP, van den Bent MJ, et al; European Organisa-
tion for Research and Treatment of Cancer Brain Tumor andRadiotherapy Groups; National Cancer Institute of Canada Clin-ical Trials Group. Radiotherapy plus concomitant and adjuvanttemozolomide for glioblastoma. N Engl J Med 2005;352(10):987–996
2 Durst CR, Raghavan P, Shaffrey ME, et al. Multimodal MR imagingmodel to predict tumor infiltration in patients with gliomas.Neuroradiology 2014;56(02):107–115
3 Paw I, Carpenter RC, Watabe K, Debinski W, Lo HW. Mechanismsregulating glioma invasion. Cancer Lett 2015;362(01):1–7
4 Wu CX, Lin GS, Lin ZX, et al. Peritumoral edema on magneticresonance imaging predicts a poor clinical outcome in malignantglioma. Oncol Lett 2015;10(05):2769–2776
5 Armstrong TS, Grant R, Gilbert MR, Lee JW, Norden AD.Epilepsy ingliomapatients:mechanisms,management, and impactof anticonvulsant therapy. Neuro-oncol 2016;18(06):779–789
6 Bruna J, Miró J, Velasco R. Epilepsy in glioblastoma patients: basicmechanisms and current problems in treatment. Expert RevClinPharmacol 2013;6(03):333–344
7 Kargiotis O,Markoula S, Kyritsis AP. Epilepsy in the cancer patient.Cancer ChemotherPharmacol 2011;67(03):489–501
8 Pallud J, Capelle L, Huberfeld G. Tumoralepileptogenicity: howdoes it happen? Epilepsia 2013;54(Suppl 9):30–34
9 Shamji MF, Fric-Shamji EC, Benoit BG. Brain tumors and epilepsy:pathophysiology of peritumoral changes. Neurosurg Rev 2009;32(03):275–284, discussion 284–286
10 Allen BG, Bhatia SK, Anderson CM, et al. Ketogenic diets as anadjuvant cancer therapy: History and potential mechanism. Re-dox Biol 2014;2:963–970
11 Cross H. Epilepsy: behavioural, psychological, and ketogenic diettreatments. BMJ ClinEvid 2015
Fig. 1 Effect of ketogenic diet concomitant with perillyl alcoholinhalation in recurrent glioblastoma multiforme (GBM) patient. Re-presentative magnetic resonance imaging (MRI) scans show markedreduction of peritumoral edema and tumor size image after 3 monthsof treatment (B, D, F) in comparison with the first image obtainedbefore the treatment (A, C, E). Brain MRI axial fluid-attenuatedinversion recovery (FLAIR) (A-D) and T1-weighted image (T1W) withcontrast (E, F).
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Ketogenic diet combined with intranasal delivery of perillyl alcohol for recurrent GBM Santos et al.198

12 Rho JM. How does the ketogenic diet induce anti-seizure effects?Neurosci Lett 2017;637:4–10
13 Strowd RE III, Grossman SA. The Role of Glucose Modulation andDietary Supplementation in Patients With Central Nervous Sys-tem Tumors. Curr Treat Options Oncol 2015;16(08):36
14 Mobbs CV,Mastaitis J, Isoda F, PoplawskiM. Treatment of diabetesand diabetic complications with a ketogenic diet. J Child Neurol2013;28(08):1009–1014
15 Paoli A, Bianco A, Damiani E, Bosco G. Ketogenic diet in neuro-muscular and neurodegenerative diseases. BioMed Res Int 2014;2014:474296
16 Champ CE, Palmer JD, Volek JS, et al. Targeting metabolismwith aketogenic diet during the treatment of glioblastoma multiforme.J Neurooncol 2014;117(01):125–131
17 Seyfried TN, Flores R, Poff AM, D’Agostino DP, Mukherjee P.Metabolic therapy: a new paradigm for managing malignantbrain cancer. Cancer Lett 2015;356(2 Pt A):289–300
18 Liberti MV, Locasale JW. The Warburg Effect: How Does it BenefitCancer Cells? Trends Biochem Sci 2016;41(03):211–218
19 Lu J, Tan M, Cai Q. The Warburg effect in tumor progression:mitochondrial oxidative metabolism as an anti-metastasis me-chanism. Cancer Lett 2015;356(2 Pt A):156–164
20 Bhattacharya B, Mohd Omar MF, Soong R. TheWarburg effect anddrug resistance. Br J Pharmacol 2016;173(06):970–979
21 Kroemer G, Pouyssegur J. Tumor cell metabolism: cancer’sAchilles’ heel. Cancer Cell 2008;13(06):472–482
22 Zuccoli G, Marcello N, Pisanello A, et al. Metabolic management ofglioblastoma multiforme using standard therapy together with arestrictedketogenic diet: CaseReport. NutrMetab (Lond) 2010;7:33
23 Schwartz K, Chang HT, Nikolai M, et al. Treatment of gliomapatients with ketogenic diets: report of two cases treatedwith anIRB-approved energy-restricted ketogenic diet protocol and re-view of the literature. Cancer Metab 2015;3:3
24 da Fonseca CO, Linden R, Futur oD, Gattass CR, Quirico-Santos T.Ras pathwayactivation in gliomas: a strategic target for intranasaladministration of perillyl alcohol. Arch ImmunolTherExp (Warsz)2008;56(04):267–276
25 Da Fonseca CO, Silva JT, Lins IR, et al. Correlation of tumortopography and peritumoral edema of recurrent malignant glio-mas with therapeutic response to intranasal administration ofperillyl alcohol. Invest New Drugs 2009;27(06):557–564
26 DA Fonseca CO, Teixeira RM, Silva JC, et al. Long-term outcome inpatients with recurrent malignant glioma treated with Perillylalcohol inhalation. Anticancer Res 2013;33(12):5625–5631
27 Wagner M, Moore DD. Endoplasmic reticulum stress and glucosehomeostasis. CurrOpinClinNutrMetab Care 2011;14(04):367–373
28 Schonthal AH. Targeting endoplasmic reticulum stress for cancertherapy. Front Biosci (Schol Ed) 2012;4:412–431
29 Kato H, Nishitoh H. Stress responses from the endoplasmicreticulum in cancer. Front Oncol 2015;5:93
30 Peñaranda Fajardo NM, Meijer C, Kruyt FA. The endoplasmicreticulum stress/unfolded protein response in gliomagenesis,tumor progression and as a therapeutic target in glioblastoma.BiochemPharmacol 2016;118:1–8
31 ChoHY,WangW, Jhaveri N, et al. Perillyl alcohol for the treatmentof temozolomide-resistant gliomas. Mol Cancer Ther 2012;11(11):2462–2472
32 Henker C, Kriesen T, Fürst K, et al. Effect of 10 different poly-morphisms on preoperative volumetric characteristics of glio-blastoma multiforme. J Neurooncol 2016;126(03):585–592
33 Brazilian Cardiology Archives. Brazilian guideline of dyslipidemiaand prevention of atherosclerosis. Available in: http://publica-ções.cardiol.br/2014/diretrizes.asp. Acess2016 (November/11).
34 Zidlik V, Brychtova S, UvirovaM, ZiakD, Dvorackova J. The changesof angiogenesis and immune cell infiltration in the intra- andperi-tumoral melanoma microenvironment. Int J MolSci 2015;16(04):7876–7889
35 Woolf EC, Curley KL, Liu Q, et al. The Ketogenic Diet Alters theHypoxic Response and Affects Expression of Proteins Associatedwith Angiogenesis, Invasive Potential and Vascular Permeabilityin a Mouse Glioma Model. PLoS One 2015;10(06):e0130357
36 Lin ZX. Glioma-related edema: new insight into molecular me-chanisms and their clinical implications. Chin J Cancer 2013;32(01):49–52
37 Sampaio LP. Ketogenic diet for epilepsy treatment. ArqNeuropsi-quiatr 2016;74(10):842–848
38 Kaur T, Manchanda S, Saini V, Lakhman SS, Kaur G. Efficacy ofAnti-Epileptic Drugs in the Treatment of Tumor and Its Associa-ted Epilepsy: An in vitro Perspective. Ann Neurosci 2016;23(01):33–43
39 LillisKP,DullaC,MaheshwariA, etal.WONOEPappraisal:molecularand cellular imaging in epilepsy. Epilepsia 2015;56(04):505–513
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
Ketogenic diet combined with intranasal delivery of perillyl alcohol for recurrent GBM Santos et al. 199

C1-C4 Dorsal Column Stimulation for RefractoryOccipital Neuralgia Treatment. Case Report
Estimulação da coluna dorsal em C1-C4 para tratamentode neuralgia occipital refratária. Relato de caso
José Augusto Malheiros1,2 Sergio Augusto Vieira Cancado1 Célia Maria de Oliveira3
Wancler Albert Gomes dos Santos1
1Division of Neurosurgery, Hospital Felício Rocho, Belo Horizonte/MG, Brazil
2Division of Neurosurgery, Hospital Luxemburgo, Belo Horizonte/MG,Brazil
3Division of Nursing, Hospital das Clínicas, Universidade Federal deMinas Gerais (UFMG), Belo Horizonte/MG, Brazil
Arq Bras Neurocir 2017;36:200–202.
Address for correspondence Sergio Augusto Vieira Cancado, MD,MSc, Divisão de Neurocirurgia, Hospital Felício Rocho, Avenida doContorno 9530 - Prado, 30110-017, Belo Horizonte/MG, Brazil(e-mail: [email protected]; [email protected]).
Keywords
► occipital neuralgia► neurostimulation► spinal cord
stimulation► case report
Abstract Introduction Refractory occipital neuralgia is a difficult medical condition, especiallywhen the patient has already been submitted to occipital nerve neurectomy andradiofrequency rhizotomy. There is no case report of spinal cord stimulation in the C1-C4 cervical segments for this condition.Objective To evaluate if C1-C4 dorsal spinal cord stimulation is effective in a patientwith refractory occipital neuralgia who was already submitted to neurectomy andrhizotomy.Methods After obtaining the approval from the Ethics Committee of one of ourinstitutions, a unilateral laminectomy was performed between C3 and C4, and a neuro-stimulator leadwas conducted until the posterior portionof theC1arcwas in full view. Thenweperformedan intraoperative test to evaluate the correspondencebetweenpain locationand stimulation-induced paresthesias. We could not put the subcutaneous lead for suchcondition because of the scar tissue of the area and the previous neurectomy.Results After one year of follow up, we noticed a dramatic improvement in paincontrol, as well as medication withdrawal. The score of the visual analogue scale was 9before the surgery, and it dropped to 2 after 1 year of follow-up.Conclusion Spinal cord stimulation between the C1 and C4 cervical segments can bean option for selected cases of refractory occipital neuralgia, including those patientswho have already been submitted to neurectomy or rhizotomy.
Resumo Neuralgia occipital refratária é uma condição médica difícil, especialmente empacientes submetidos previamente a neurectomia nos nervos occipitais e rizotomiapor radiofrequência. Não há na literatura relato de estimulação da medula espinhalentre os níveis C1 e C4 para essa condição.
receivedFebruary 1, 2017acceptedMay 31, 2017published onlineJuly 6, 2017
DOI https://doi.org/10.1055/s-0037-1604177.ISSN 0103-5355.
Copyright © 2017 by Thieme RevinterPublicações Ltda, Rio de Janeiro, Brazil
Case Report | Relato de Caso200

Introduction
Refractory occipital neuralgia is a difficult medical condition,especially when the patient has already been submitted tooccipital nerve neurectomy and radiofrequency rhizotomy.There is no case report of spinal cord stimulation in the C1-C4cervical segments for this condition.
Presentation
The patient (SCTA) was a 42-year-old female with a medicalreport of 2 years of refractory pain in the occipital region. Shewas submitted to anesthetic and corticoid blocks, and experi-enced partial resolution for months. The surgical approach forneurectomy of the major and minor occipital nerves wasperformed, and the patient showed no improvement after3 months; instead, she experienced recurrence, worsening ofthe pain and refractoriness of the drugs (pregabalin 600 mg/day plus duloxetine 60 mg/day plus methadone 20 mg/day).During this period, she was referred to our service. Theproposed initial treatment was pulsed radiofrequency in theC2 ganglion and C3 root.We achieved a reduction of 30% in thescore of the visual analogue scale (VAS) after two attemptswith nomedicationwithdrawn.As therewas a large portion ofscar tissue in the occipital region, the introduction of a C1-C4spinal cord neurostimulator by laminectomy was proposed.
Technical Note
The patient was under general anesthesia, in the proneposition, with the head on a 3-pin holder. We performedunilateral exposure of the laminas of C1 until C4, and a smallC4 laminectomy for the placement of the neurostimulatorlead under the laminas of C2, C3 and C4 until the lateralportion of C1. We had to expose the C1 posterior arc andepidural space in order to guide the lead, andwe checked theradioscopy to make sure the 16-electrode surgical lead(Medtronic, Inc. Minneapolis, MN, US) was properly placed
(►Fig. 1). We turned the patient and performed an intra-operative awake test with an external trialing neurostimu-lator (Medtronic, Inc. Minneapolis, USA) to evaluate thecovering pain area. Once we matched the area of pain withthe neurostimulation, we connected the system and placedthe neurostimulator’s battery into the abdominal wall.
Results
There was an important improvement in pain with a signifi-cant reduction in the use of pain medication progressively.After 12 months of implantation, the visual analogue scalescore was 2, and the patient successfully achieved metha-done and pregabalin withdrawal. The patient is currentlyusing only duloxetine 60 mg/day (►Fig. 2).
Discussion
Occipital neuralgia is often controlled with muscle relaxants,physical therapy, and anesthetic blocks with corticosteroids.In refractory cases, the intervention option is necessary.1 Cur-rently, the most recommended interventions are performedwith botulin toxin2 or pulsed radiofrequency.3 If refractorinessoccurs, performinganeurectomyoragangliectomy4areoptionswith controversial results, because they canworsen the painfulcondition.1 In this case, the patient had already taken anestheticblocks with corticosteroids, with improvement only while theeffect of the anesthetic lasted. The patient underwent an opensurgery forneurectomy,but sheshowedno improvementafter3months. Pulsed radiofrequencywas then attempted twice, withthe condition showing little improvement. The option for spinalcord stimulation instead of peripheral nerve stimulation4,5wasmade because of the large portion of scar tissue in the occipitalregion and the medical report of neurectomy of the occipitalnerves. In this case,wecouldnot introduce theleadunder theC1arc (perhaps because of the previousmanipulation), andwehadtoexpose theC1posterior arc and theepidural space toplace the16-electrode surgical lead under C1.
Objetivos Avaliar se a estimulação da coluna dorsal da medula nos níveis C1 a C4 éeficaz no controle da dor em paciente com neuralgia occipital refratária já submetido aneurectomia e rizotomia.Métodos Após aprovação do Conselho de Ética de uma de nossas instituições, foirealizada laminectomia unilateral de C3 e C4, com posterior introdução do conjunto deeletrodos em placa, que foi posicionado até que a porção anterior do arco de C1estivesse sob visão direta. Posteriormente, foi realizado um teste intraoperatório paraavaliar a correspondência entre a área dolorosa e a parestesia induzida pela estimu-lação. Não possível optar pelo uso de eletrodo subcutâneo devido ao extenso tecidocicatricial secundário às cirurgias prévias.Resultados Melhora significativa da dor ocorreu ao longo de um ano de acompanha-mento, com redução progressiva da dose da medicação. O valor da escala visualanalógica no pré-operatório era 9, e após 1 ano de acompanhamento, reduziu para 2.Conclusão Estimulação da coluna dorsal damedula espinhal entre os seguimentos C1e C4 pode, em casos selecionados, ser uma opção terapêutica na neuralgia occipitalrefratária, incluindo pacientes que já foram submetidos a neurectomia e rizotomia.
Palavras-Chave
► neuralgia occipital► neuroestimulação► estimulação da
medula espinhal► relato de caso
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
C1-C4 Dorsal Column Stimulation for Refractory Occipital Neuralgia Treatment Malheiros et al. 201

As soon as there was correspondence between the area ofpain and the stimulated area, we decided to place the genera-tor at the same surgical time. Good pain control was achievedthrough a significant visual analogue scale reduction of 80%andwithdrawal fromthemedications. TheVASscoreof2 in theaffected area may be related to the area stimulation itself.
Theoption for thedorsal cord stimulatorbetweenC1andC4can allow adequate central control in these cases of refractoryoccipital neuralgia. It allows greater covering area by thestimulation and more programs possibilities in the follow-up control. Another advantage of dorsal cord stimulation atthis level is the anatomical characteristic of the cervical plexus
and the occipital nerves with numerous anastomoses as wellas the possibility of activation of adjacent cervical spinal areasand trigeminal nuclei.1,4 The greatest negative point of thetechnique presented is the port site of the surgery; the proce-dure should be performed by a neurosurgeonwith knowledgeof the anatomy of the occipital and cervical regions. Thepostoperative period was well-tolerated by our patient, witha good pain control outcome.
Spinal cord stimulation between the C1 and C4 cervicalsegments can be an option for selected cases of refractoryoccipital neuralgia, including those patients who have alreadybeen submitted to neurectomy or rhizotomy.
Conflicts of InterestThe authors have no conflicts of interest to discloseregarding the publication of this paper.
References1 Choi I, Jeon SR. Neuralgias of the Head: Occipital Neuralgia.
J Korean Med Sci 2016;31(04):479–4882 Harden RN, Cottrill J, Gagnon CM, et al. Botulinum toxin a in the
treatment of chronic tension-type headache with cervical myo-fascial trigger points: a randomized, double-blind, placebo-con-trolled pilot study. Headache 2009;49(05):732–743
3 Huang JH, Galvagno SM Jr, HameedM, et al. Occipital nerve pulsedradiofrequency treatment: a multi-center study evaluating pre-dictors of outcome. Pain Med 2012;13(04):489–497
4 Ducic I,HartmannEC,LarsonEE. Indicationsandoutcomesforsurgicaltreatment of patients with chronic migraine headaches caused byoccipital neuralgia. Plast Reconstr Surg 2009;123(05):1453–1461
5 Rodrigo-Royo MD, Azcona JM, Quero J, Lorente MC, Acín P, Azcona J.Peripheralneurostimulation in themanagementofcervicogenichead-ache: four case reports. Neuromodulation 2005;8(04):241–248
Fig. 1 Dorsal cord stimulation for occipital neuralgia. (A) Preoperative photograph of the patient. Note the scar from the previous procedureand the painful stitches drawn on the scalp. (B) Radioscopy in profile showing the position of the electrodes from C4 to C1. (C) Intraoperativeradioscopy in anterior-posterior view showing the position of the 16- electrode surgical lead.
8
5
32
0123456789
10
DLX 60mg DLX 60mg DLX 60mg DLX 60mg
MTD 20mg MTD 10mg -- --
PGB 600mg PGB 600mg PGB 300mg --
1 month 3 months 6 months 12 months
VAS Follow up
Fig. 2 Visual analogue scale follow-up after spinal cord stimulation.Visual analogue scale versus medication 1, 3, 6 and 12 months aftersurgery. Abbreviations: DLX, duloxetine; MTD, methadone; PGB,pregabalin; VAS, visual analogue scale.
Arquivos Brasileiros de Neurocirurgia Vol. 36 No. 3/2017
C1-C4 Dorsal Column Stimulation for Refractory Occipital Neuralgia Treatment Malheiros et al.202

Instructions to Authors
ISSN 0103-5355
Brazilian Neurosurgery (Arquivos Brasileiros de Neurocirurgia), an official journal of the Brazilian Society of Neurosurgery (Sociedade Brasileira de Neurocirurgia) and Portuguese Language Neurosurgery Society (Sociedades de Neurocirurgia de Língua Portuguesa), aims to publish scientifi c works in Neurosur-gery and related fi elds, unpublished and exclu-sive. The journal publishes papers written in Portuguese with abstracts in English or written in English with Portuguese abstracts.
Submitted articles shall be placed as one of the following categories:
• Original: result of clinical, epidemiological or experimental research. Abstracts of theses and dissertations.
• Review: review and update synthesis of spe-cifi c themes, with critical analysis and con-clusions. Databases and the period range must be specifi ed.
• Case Report: presentation, analysis and discus-sion of cases that present relevant interest.
• Technical Note: note on surgery techniques and/or surgical instruments.
• Miscellaneous: neurosurgery history, pro-fessional practice, medical ethics and other pertinent matters to the journal purpose.
• Letter to the Editor: critics and comments pre-sented in a brief ethical and instructive man-ner about published content in this journal. The copyright is safe to authors of the aimed subject. Letters, when accepted, will be pub-lished with authors reply.
General standards for publishing
• Article fi les for publishing must be submit-ted to the Editor, via http://www.editorial-manager.com/bns/.
• All articles will have a double blinded peer-review process, and no Article Publishing Charge (APC) – society funded. More about Open Access at http://open.thieme.com.
• Only new unpublished manuscripts will be ac-ceptable. Submitted articles must not be fullyor partially submitted to any other journal.
• The editorial board may reject or suggest changes in order to improve the clarity and structure of the text and maintain uniform-ity with the journal policy.
• Copyrights of articles published in the journal will belong exclusively to the Brazilian Neurosurgery and Thieme Publicações Ltda. The reproduction of articles or illustrations without prior consent is prohibited.
Standards for submission
Authors must send the following fi les:
1. Pub Letter (text fi le) stating the article has not yet been published partially or fully or submitted concomitantly to other journal.
2. Manuscript (text fi le).
3. Figures (Tiff , Jpeg, Pdf, Indd) sent in separate fi les with minimum resolution of 300 dpi.
4. Tables, charts and graphics (text fi le) sent separately.
Standards for articles structure
Articles must be structured with all the follow-ing items and paginated accordingly:
1. Title page: article title both in Portuguese and English; full name of all authors; academic or professional affi liation of each author; institutions names where the study took place; running title; corresponding author name, degree, full address, e-mail and phone number; followed by ICMJE CoI forms (http://www.icmje.org/confl icts-of-interest/).
2. Abstract: original articles need structured abstract with 250 words at the most: objec-tive, methods, results and conclusions; review articles, case reports, technical notes and miscellaneous need no structured abstract. Following the abstract comes keywords (six at the most), based on MeSH (Medical Subject Headings), published in Medline and available at: www.ncbi.nlm.nih.gov/mesh/.
3. Portuguese abstract: Portuguese version of title, abstract and keywords based on DeCS (Descritores em Ciências da Saúde, http://decs.bvs.br).
4. Main text: introduction; casuistry or mate-rial and methods; results; discussion; conclu-sion; acknowledgments.
5. References: number references as they are fi rst cited in the text with Arabic numerals. Use Vancouver style; list all authors until the sixth, using et al. after the third when more than six; when reference authors are cited in the text cite the fi rst and et al. for references with more that two authors; unpublished data or personal communication must be cited as such between parentheses and cannot be listed as reference; use journal abbreviation from Index Medicus; use the following examples:
Journal Article
Agner C, Misra M, Dujovny M, Kherli P, Alp MS, Ausman JI. Experiência clínica com oxime-tria cerebral transcraniana. Arq Bras Neurocir 1997;16(1):77–85
Book Chapter
Peerless SJ, Hernesniemi JA, Drake CG. Surgical management of terminal basilar and posterior cerebral artery aneurysms. In: Schmideck HH, Sweet WH, editors. Operative neurosurgical techniques. 3rd ed. Philadelphia: WB Saunders;1995:1071–86.
Book
Melzack R. The puzzle of pain. New York: Basic Books Inc Publishers; 1973.
Theses and dissertations
Pimenta CAM. Aspectos culturais, afetivos e terapêuticos relacionados à dor no câncer. [thesis]. São Paulo: Escola de Enfermagem da Universidade de São Paulo; 1995.
Annals and other congresso publications
Corrêa CF. Tratamento da dor oncológica. In: Corrêa CF, Pimenta CAM, Shibata MK, editores. Arquivos do 7º Congresso Brasileiro e Encontro Internacional sobre Dor; 2005 outubro 19–22; São Paulo, Brasil. São Paulo: Segmento Farma. pp. 110–20.
Available Article in ahead of print
International Committee of Medial Journal Editors. Uniform requirements for manuscripts submitted to biomedical journals. Writing and editing for biomedical publication. Updated October 2007. Available at: http://www.icmje.org. Access in: June 12, 2008.
6. Tables and charts: numbered by Arabic numerals according to its citation in the text; edited in double space, using separate sheets per table/chart; title right above; note, abbreviations, legends must follow right under;introduce only essential tables and charts; files must come separately.
8. Figures: digital formats (Tiff , Jpeg, Pdf, Indd) with minimum resolution of 300 dpi (trim 7.5 or 15 cm).
9. Legends and captions: numbered by Ara-bic numerals according to its citation in the text; edited in double space, using separate fi les; identify eventual labels present in the fi gure (arrows, characters, lines etc.); image previously published must have publisherauthorization and credits.
10. Ethics standards: No data or image identify-ing a patient can be used without formal consent; studies using human beings or animal trials must follow ethical standards from the International Committee of Medical Journals Editors – ICMJE, as well as approval of original institution’s Eth-ics Committee; confl icts of interest must have aICMJE form fi lled in by all authors (http://www.icmje.org/confl icts-of-interest/); commercial marks should be avoided; authors are the sole responsible for opinions and concepts in the published articles, as well as for the reference accuracy.
11. Other information: PDF proof will be sent to corresponding author for eventual queries and/or approval within 72 hours; except measure units, acronyms must be spelled out after its fi rst time mentioned.
Secretariat: R. Abílio Soares, 233/143, Paraíso. 04005-001, São Paulo, SP, Brazil. Phone:(+55 11) 3051-6075.Home page: www.sbn.com.br. e-mail: [email protected]



ADQUIRA JÁ EM http://www.thiemerevinter.com.br
Siga-nos: Facebook/ThiemeRevinter
A obra mais aguardada em Neurocirurgia!
MANUAL DE NEUROCIRURGIAOitava Edição
Mark S. Greenberg
Em sua Oitava Edição atualizada, o Manual de Neurocirurgia tem desfrutado de prestígio lendário nas prateleiras de todos os departamentos de neurocirurgia do mundo, por mais de um quarto de século. Reconhecido por sua abrangência e acessibilidade, este guia portátil, em um único volume, é o recurso indispensável para qualquer profissional envolvido no cuidado de pacientes com distúrbios do sistema nervoso central – tanto para residentes em neurocirurgia e enfermeiros quanto para especialistas e profissionais afins da área médica.
Este clássico da literatura abrange toda a extensão e profundidade da neurociência, incluindo distúrbios neurológicos hereditários e adquiridos, anomalias do desenvolvimento, além de tópicos mais obscuros, como toxinas que afetam os sistemas nervosos central e periférico. O texto também inclui condições tratadas primariamente por neurologistas, que podem vir a ser tratadas por um neurocirurgião, como Parkinsonismo, esclerose múltipla, doenças do neurônio motor e demência. As informações mais recentes sobre anatomia, fisiologia, diagnóstico diferencial e princípios atuais do tratamento não cirúrgico e cirúrgico são fornecidas, abrangendo todas as faixas etárias, desde as condições pediátricas até as geriátricas.
= Gráficos expandidos e ilustrações em quatro cores= Mais de 1600 páginas de informação prática, incluindo milhares de citações
bibliográficas, referências úteis e um índice detalhado= Princípios dos cuidados neurocríticos, com uma visão abrangente das
condições, desde SAH até traumatismo craniano e medular, incluindo complicações como perda de sal cerebral, ressangramento, vasospasmo e morte cerebral.
Abrangente e convenientemente compacto, esta é a referência diária indispensável, o parceiro de estudos perfeito para revisão e concursos, ideal para provas de título. É, com certeza, uma obra valiosa para legiões de residentes em neurocirurgia e uma ferramenta essencial para qualquer profissional que trabalhe com neurociência.
Medone Neurosurgery é a fonte online em neurocirurgia mais abrangente do mundo. Para uma avaliação gratuita, acesse a página: http://thieme.com/eneurotrial
1.662 Páginas – Papel CouchéFormato : 14 x 21 cmBrochuraRicamente Ilustrado em 4 CoresISBN: 978-85-67661-65-0Especialidades: Neurocirurgia, Neurologia
A obra mais aguardada em Neurocirurgia!