bronchial cartilage in chronic bronchitis
TRANSCRIPT
Thorax (1969) 24, 607.
Bronchial cartilage in chronic bronchitisM. K. TANDON AND ALASTAIR H. CAMPBELL
From the Central Office, Repatriatiorl Departmenit, St. Kilda Road, South Melbournie, Victoria, A ustralia
An examination has been made of the amount of bronchial cartilage in the subsegmental bronchiof nine chronic bronchitics and seven controls. The axial pathway in four or five representativebronchopulmonary segments were carefully dissected in each lung. In each segment the meanextent of cartilage arranged circumferentially in the walls of the bronchi was significantly less inthe chronic bronchitic patient than in the controls. Of the 42 specimens from the variousbronchopulmonary segments of the controls, ithe cartilage was arranged circumferentially to thefifth generation or further in 33, but extended this far in only 14 of the 50 specimens from thechronic bronchitics. Using certain defined criteria, deficiency of cartilage was found in 25 of 50specimens from 11 lungs of the chronic bronchitics and in only one of 42 specimens from ninecontrol lungs. There was a negative correlation between the degree of bronchial gland enlarge-ment, as measured by the gland/ wall ratio, and the average extent of circumferentially arrangedcartilage along the bronchi (r= -0 8, P<0 01). Similarly, the number of bronchopulmonarysegments affected increased and the average extent of circumferentially arranged cartilagedecreased with increase in severity of the bronchitis. We think that the deficiency of bronchialcartilage in chronic bronchitics would favour collapse of the affected bronchi during forcefulexpiration or cough.
There have been conflicting claims concerning thestate of the bronchial cartilage in patients withchronic bronchitis or emphysema. Wright (1960)described a reduction in the number and size ofthe bronchial cartilaginous plates in patients withchronic bronchitis and emphysema. Smoothmuscle and fibrous tissue were also reduced inamount. Deficiency of bronchial cartilage withgeneralized bronchiectasis has been described inchildren (Williams and Campbell, 1960). In thesecases the deficiency may have been developmentalrather than acquired.
In two other investigations, deficiencies ofbronchial cartilage in selected bronchi could notbe demonstrated. Restrepo and Heard (1964) sec-tioned the bronchus to the basal segments and theinferior lingular bronchus and did not find anydifference in the area of the cartilage in patientswith bronchitis and emphysema compared withnormals. Similarly, Greenberg, Boushy and Jen-kins (1967) measured the width of the cartilage insections from the main stem, lobar, and segmentalbronchi and found no difference between patientswith emphysema and those without emphysema.The discrepancy between the various investiga-
tions could be due to examination of differentparts of the bronchial tree. Wright (1960) did notdescribe clearly which of the segmental bronchialgenerations had defective cartilage, but his obser-vations included bronchi more peripheral than thelobar and first generation segmental bronchi
examined by Restrepo and Heard (1964) andGreenberg et al. (1967).
In the present investigation a comparison hasbeen made of the amount of cartilage in thebranches of various segmental bronchi of patientswith chronic bronchitis and in controls.
METHODS AND MATERIALS
SUBJECTS The lungs were obtained at necropsy frommen who had died at the Repatriation General Hos-pital, Heidelberg, near Melbourne, Australia. Sevensubjects (aged 26-84 years) who had been withoutsymptoms of chronic bronchitis or emphysema duringlife served as controls and nine lungs were examinedfrom this group.Nine bronchitic subjects (aged 67-79 years) were
selected on the basis of persistent productive coughof several years' duration. In some, the severity ofthe condition had been assessed by pulmonary func-tion studies. Eleven lungs were examined from thisgroup.
EXAMINATION OF BRONCHI Particular attention wasgiven to detecting all the cartilage in segmentalbronchi and their branches. This was achieved bycareful dissection of the bronchi and by staining thecartilage with acid toluidine blue. The distances intothe bronchial tree were determined in terms of thenumber of bronchial generations along the bronchialpathway. The generations of the bronchi are the seg-men(ts of the tubes between successive subdivisions orbranches (Hayward and Reid, 1952).
In all counts of bronchial generations the segmental607

M. K. Tandon and Alastair H. Campbell
bronchi were counted as the first generation. Each ofthe two bronchi produced by the first division of thesegmental bronchus was regarded as belonging to thesecond generation. The four bronchi produced by thedivision of each of ithe two bronchi of the secondgeneration belong to the third generation, and so on.Each lung was fixed by intrabronchial injection of
8 % formol saline at a pressure of 30 cm. H20 for atleast one week.
Axial pathways in five representative broncho-pulmonary segments (apical segment of 'the lowerlobe, both segments of middle or lingular lobes, lateraland posterior segments of the lower lobe) were dis-sected in each lung. In several lungs the presence offibrosis or other factors reduced the number of satis-factory dissections to four segments. When the axialbronchus divided dichotomously, both branchingbronchi were traced.The d'ss-cted bronchial pathways were then drawn
and the generations carefully indicated on the draw-
_.iL
.. .
s r. '-.
t:
ing. The bronchi were then opened and stitched to awire mesh ready for staining; a second sketch wasmade of the opened bronchi.The staining procedure was based upon that des-
cribed by Stovin (1959). The bronchi were washed inrunning tap water to remove the formalin. Suturedto a chrome-plated wire mesh, they were itmmersedfor 16-24 hours in toluidine blue solution having apH between 1 and 2. By immersion in 70% alcoholfor about half an hour the toluidine blue was removedfrom tissues other than the cartilage. The specimenwas then dehydrated by immersion in absolute alco-hol two or three times depending upon thickness ofthe wall. The bronchi were then placed in cedar woodoil for four or five days until the non-cartilaginoustissues became transparent. The specimen was thenplaced in xylol in a Petri dish.
Generally, well-stained specimens were obtainedwith this proCedure. In one case, inspection showeduneven staining of the cartilage. Satisfactory staining
Ar _______
IAl
FIG. 1. Posterior basal segments from a control and from both lungs of a bronchitic subject. In the control, circum-ferentially arranged cartilage extends up to the 6th generation, whereas in the bronchitic it is seen up to the 3rdgeneration (right) and in the left up to the 5th generation in one axial branch and to the 2nd generation in another branch.
608
A- '4
*. .,. Aw

Bronchial cartilage in chronic bronchitis
was obtained by repeating the process. In anothercase, with poor and uneven staining, microscopicexamination showed non-staining of the cartilage. Thiscase was excluded.
In all other cases the staining appeared even andadequate.The presence or absence of cartilage observed
macroscopically in the well-stained specimens wasconfirmed by 'microscopic examination of sections of24 bronchial generations from four subjects (two con-trols and two bronchitics).With the help of the original drawings indicating
the bronchial generations, the level at which thebronchial cartilage ceased to be arrayed circumferen-tially was noted for each bronchopulmonary segment.The specimens were also examined for variation inthe size and distribution of the cartilaginous plates.AU the specimens were photographed to obtain a per-manent record.
From sections of the main lobar bronchi, thegland/wall ratio (Reid, 1960) was measured in allseven of the control group, and ranged between 0-26and 0-42 (average 0-34). In the bronohitic group it wasmeasured in six and ranged between 0 45 to 0-61(average 0 52).
It was not possible to assess the degree of emphy-sema present in the lungs examined, as dissection ofthe bronchopulmonary segments destroyed the paren-chyma.
RESULTS
The main difference between the chronic bron-chitics and the controls was shown by determiningthe distance along the axial pathways that cartilagewas arranged circumferentially. The cartilage wasregarded as being arranged circumferentially when
0 2 Cm 3 4 5
InferiorI 1-rori-r
k
p 4*:
.:1. a*
. ..
I.....A g
j ..
:4 A.: c
I.
5
O.:
I:^-Ad
"t
.i
k:
4 ...
..A.
uo
RO -'L"- S
FIG. 2. Lingular lobar segments of a control and a bronchitic case. Circumferentially arrangedcartilage in the superior and inferior segments of the control is seen up to 4th and 5th generationsrespectively, whereas in the bronchitic it is seen up to the 3rdgeneration in the superior and to the2nd generation in the inferior segment.
CONTROL
I I
609
M. K. Tandon and Alastair H. Campbell
pieces were scattered around the tube on allsides.
Examination of the segmental bronchi forseveral generations revealed that there was lessbronchial cartilage in the bronchitic subjects thanin the controls. The deficiency was less apparentin the first or second bronchial generations andaffected the more distal generations to a varyingdegree (Figs 1 and 2).
In all the bronchopulmonary segments exam-ined, the mean extent of the circumferentialarrangement of cartilage along the axial pathwayswas significantly less extensive in the chronicbronchitic patients than in the controls (Table I).The average extent of circumferential cartilage incertain segments in normal subjects studied byHayward and Reid (1952) have been included forcomparison. Considering the difference in tech-nique, their results compare reasonably closelywith those from normal lungs in this series.
TABLE IMEAN NUMBER OF BRONCHIAL GENERATIONS WITH
CARTILAGE CIRCUMFERENTIALLY ARRANGED
Normals Controls Chrnc ControlsBronchopulmonary (Hayward (This Chronic v.
Segments and Investiga- bjc tlc ChronicReid) tion) Subjects Bronchitics
All segments .. 54 4 0 P<0-01Apical segment-
lower lobe .. 4 5-1 3 9 P<001Middle lobe (lateraland medial) 4 4-8 3.5 P< 0-05
Lingula (superior andinferior) 5 4-4 1 29 P<001
Lateral basal segment 6-4 4-6 P<0*05Posterior basal seg-ment .. .. 6 6-3 4-8 P<00l
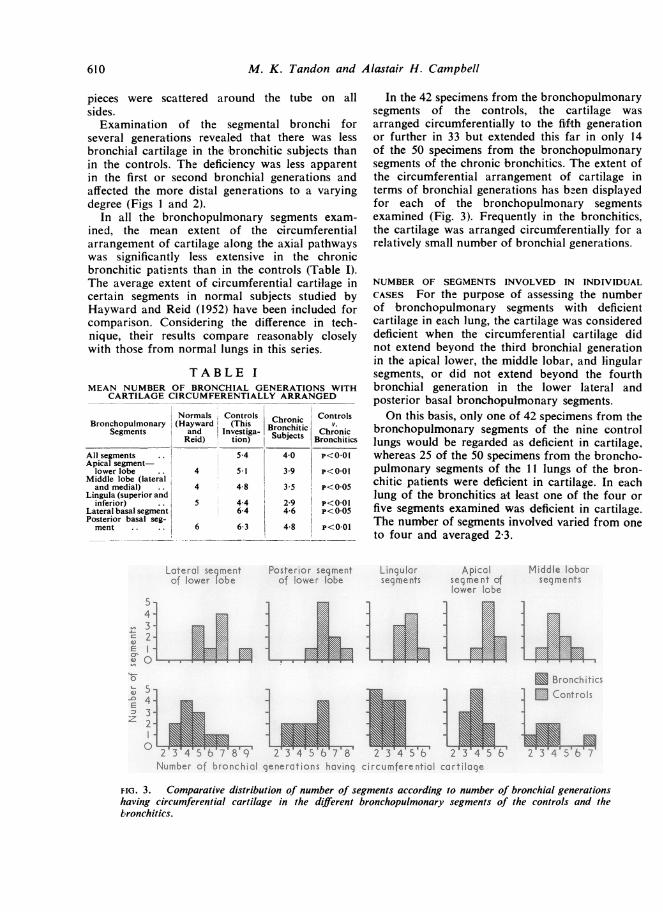
In the 42 specimens from the bronchopulmonarysegments of the controls, the cartilage wasarranged circumrferentially to the fifth generationor further in 33 but extended this far in only 14of the 50 specimens from the bronchopulmonarysegments of the chronic bronchitics. The extent ofthe circumferential arrangement of cartilage interms of bronchial generations has bzen displayedfor each of the bronchopulmonary segmentsexamined (Fig. 3). Frequently in the bronchitics,the cartilage was arranged circumferentially for arelatively small number of bronchial generations.
NUMBER OF SEGMENTS INVOLVED IN INDIVIDUALCASES For the purpose of assessing the numberof bronchopulmonary segments with deficientcartilage in each lung, the cartilage was considereddeficient when the circumferential cartilage didnot extend beyond the third bronchial generationin the apical lower, the middle lobar, and lingularsegments, or did not extend beyond the fourthbronchial generation in the lower lateral andposterior basal bronchopulmonary segments.On this basis, only one of 42 specimens from the
bronchopulmonary segments of the nine controllungs would be regarded as deficient in cartilage,whereas 25 of the 50 specimens from the broncho-pulmonary segments of the 11 lungs of the bron-chitic patients were deficient in cartilage. In eachlung of the bronchitics at least one of the four orfive segments examined was deficient in cartilage.The number of segments involved varied from oneto four and averaged 2-3.
Lotercl se-mentof lower robe
Posterior segmentof lowe r lobe
Lingulolr Apicolsegments segment of
lower lobe
- JI 2aEl
E Bronchitc;
E
02'34W56b7~8'91 23'45'6'.78 2'3456Number h4bronchial generations having circumferential cartilage
FIG. 3. Comparative distribution of number of segments according to number of bronchial generationshaving circumferential cartilage in the different bronchopulmonary segments of the controls and thebronchitics.
Middle loborseq me nts
610

Bronchial cartilage in chronic bronchitis
DEGREE OF DEFICIENCY OF CARTILAGE AND SEVERITYOF BRONCHITIS In controls and bronchitics inwhom the bronchial gland/wall ratio had beenmeasured, and in whom the bronchial cartilagehad been examined in five bronchopulmonarysegments, a comparison was made between thedeficiency of bronchial cartilage and the degree ofhypertrophy of the bronchial mucous glands.As shown in Fig. 4, there is a negative correla-
tion between the gland/wall ratio and the averageextent of the circumferentially arranged cartilagealong the axial pathways; the greater the hyper-trophy of the glands, the more deficient thebronchial cartilage (r= - 0-85, P<001).Four of the bronchitic patients had been shown
to have severe airway obstruction during life. Theforced expiratory volume/vital capacity ratio wasless than 20% in all four. All these patients hadhad bronchitis for more than 10 years. The otherfive bronchitic patients had not had respiratoryfunction tests and were judged to have moderatelysevere bronchitis on clinical grounds; the durationof bronchitis had been less than 10 years in allfive.
In each of these two groups of bronchitics andin the controls, the average number of segmentsper lung regarded as being deficient in bronchialcartilage and the average number of bronchial
0b
0-5*
04
032
0*2
0
0Bronchitics
| Controls|
* 0 @
0
0 00 o
3 4 5Average number of bronchial generations perlung having circumferential cortiloge
FIG. 4. The gland/wall ratio, studied in six bronchitic andseven control cases, showed a negative correlation with theaverage number of bronchial generations per lung havingcircumferential cartilage (r= - 085, P < 0-01).
2X
generations with circumferentially arrangedcartilage have been compared. It is shown inTable II that the number of bronchopulmonarysegments affected increased with the severity ofthe bronchitis, whereas the average extent ofcircumferentially arranged cartilage decreasedwith severity of the bronchitis.
TABLE IIRELATIONSHIP BETWEEN SEVERITY OF BRONCHITIS
AND DEFICIENCY OF CARTILAGE
Mean No. of Mean No. of BronchialSegments, per Generations withLung, Deficient Circumferentiallyin Cartilage Arranged Cartilage
Severe bronchitis 3 0 3-7Moderately severe bron-
chitis . . 2-0 4-1Controls .. 0- 1 5.4
'rU-_ _ r __-- -- _@__*- - _,r.__ -_s- s.-The signincance of these relationshups was testeu aster calculationof correlation coefficients. When the grade of bronchitis is comparedwith the mean number of segments with deficient cartilage in eachlung, r=0 85, P<0-01. Comparing the grade of bronchitis with themean number ofbronchial generations with circumferentially arrangedcartilage in the bronchopulmonary segments examined, r= -0-87,
DISCUSSION
Restrepo and Heard (1964) and Greenberg et al.(1967) failed to demonstrate deficiency of cartilagein selected bronchi from patients with bronchitisor emphysema. The bronchi examined by theseinvestigators were first generation segmental orlarger bronchi. In the present investigation, thedeficiency of cartilage was apparent in the bronchismaller than the first segmental generation.The walls of these bronchi, for several genera-
tions along axial pathways, normally receivesupport from the circumferentially arrangedcartilage to which is attached a fibroelastic net-work. When these bronchi have been dissectedfree, palpation reveals that for a distance into thesegment of about five divisions the tubes feelrelatively rigid and resist occlusion by externalpressure. Distal to this point they are readily com-presed (Hayward and Reid, 1952).During a forced expiration, the pressure in the
alveoli surrounding the bronchial tubes is raisedand is greater than the intraluminal pressure;thus the transmural pressure is positive and tendsto compress the bronchial tube. The degree ofcompression depends in part upon the complianceof the bronchial wall. It can be safely assumedthat bronchi which are normally supported bycircumferential cartilage will become more com-pliant if the cartilage becomes deficient. It islikely that such bronchi will tend to collapseduring forced expiration, considerably obstructingair flow through the affected bronchi.
0
0a
3-v
I I I
61 1

M. K. Tandon and Alastair H. Campbell
Collapse of subsegmental bronchi has been ob-served during life in patients with obstructive air-way disease (Rayl, 1965; Gayrard and Charpin,1968). Also a dynamic bronchographic study ofpost-mortem human lungs (Petty, Miercort, Ryan,Vincent, Filley, and Mitchell, 1965) has shownthat premature and excessive airway collapseoccurred in the intraparenchymal airways inpatients with severe symptoms of airway obstruc-tion. Excessive and premature airway collapse wasnot observed in normal lungs or in most lungswith mild emphysema. Moderate to severe emphy-sema with or without chronic bronchitis was pre-sent in the lungs with the most premature collapse.Lungs in which chronic bronchitis was the pre-dominant lesion also demonstrated varying degreesof airway collapse. As a 'working hypothesis',Petty et al. (1965) suggested that when sufficientdestruction of the alveolar tissue occurs, small andmedium sized intraparenchymal airways lose theradial traction forces that normally maintain thepatency of the conducting airways and that thisprocess allows the premature and excessivebronchial collapse observed.That loss of radial traction on the bronchi was
not the sole cause of the premature airway collapsecan be suggested as Petty et al. (1965) observedthat in one lung with very severe emphysemapremature airway collapse did not occur; and insome patients with bronchitis, but without severeemphysema, premature airway collapse occurred.
Irrespective of the role of diminished radialtraction on bronchial calibre, the findings of thepresent investigation suggest that, at least in part,the premature airway collapse of the intra-segmental bronchi observed by Petty et al. (1965)could have been contributed to by weakening ofthe bronchial walls through partial deficiency ofthe circumferentially arranged cartilage.'The cause of the deficiency of the bronchial
cartilage requires further investigation. Cartilagedeficiency associated with bronchiectasis has beenobserved by Williams and Campbell (1960) inchildren, and is probably a developmental abnor-mality. It is possible that minor grades of suchdevelopmental deficiency of bronchial cartilagemight persist into adult life.
However, all the men studied in the presentinvestigation had been healthy in their youth and
'See Addendum
fit for war service. They developed bronchitis inadult liffe. As the deficiency of the bronchial car-tilage is related to the severity of the chronicbronchitis, as judged by the glandular enlargementin the bronchial wall and clinical severity, it seemslikely that in these patients the deficiency of carti-lage has been acquired and may be due to atrophyfollowing repeated infection of the bronchialwalls. There was no indication that age led toatrophy of the cartilage as all the controls, exceptone, were over 50 years of age and the amount ofcartilage present compared closely with that ob-served in normals by Hayward and Reid (1952).
We wish to thank Dr. Peter Campbell for helpfuladvice, Dr. D. G. Buist for considerable assistance indeveloping the technique, and the Chairman of theRepatriation Commission for permission to publishthis paper.
ADDENDUM
Since completion of this paper, an article byMaisel, Silvers, Mitchell, and Petty (1968) has beenpublished dealing with causes of dynamic expira-tory airway collapse. They reported that at sitesof bronchial collapse absence or marked atrophyof cartilage, together with variable loss of base-ment membrane, mucous glands, vessels, smoothmuscle and collagen, were significant findings.
REFERENCESGayrard, P., and Charpin, J. (1968). Evaluation of the role of the
large bronchi in the genesis of air obstruction in normal subjectsand in various diseases. Amer. Rev. resp. Dis., 97, 1076.
Greenberg, S. D., Boushy, S. F., and Jenkins, D. E. (1967). Chronicbronchitis and emphysema; correlation of pathologic findings.Ibid., 96, 918.
Hayward, J., and Reid, L. McA. (1952). The cartilage of the intra-pulmonary bronchi in normal lungs, in bronchiectasis, and inmassive collapse. Thorax, 7, 98.
Maisel, J. C., Silvers, G. W., Mitchell, R. S., and Petty, T. L. (1968).Bronchial atrophy and dynamic expiratory collapse. Amer. Rev.resp. Dis., 98, 988.
Petty, T. L., Miercort, R., Ryan, S., Vincent, T., Filley, G. F., andMitchell, R. S. (1965). The functional and bronchographicevaluation of postmortem human lungs. Ibid., 92, 450.
Rayl, J. E. (1965). Tracheobronchial collapse during cough. Radiology,85, 87.
Reid, L. (1960). Measurement of the bronchial mucous gland layer:a diagnostic yardstick in chronic bronchitis. Thorax, 15, 132.
Restrepo, G. L., and Heard, B. E. (1964). Air trapping in chronicbronchitis and emphysema. Amer. Rev. resp. Dis., 90, 395.
Stovin, P. G. I. (1959). Congenital lobar emphysema. Thorax, 14, 254.Williams, H., and Campbell, P. (1960). Generalized bronchiectasis
associated with deficiency of cartilage in the bronchial tree. Arch.Dis. Childh., 35, 182.
Wright. R. R. (1960). Bronchial atrophy and collapse in chronicobstructive pulmonary emphysema. Amer. J. Path., 37, 63.
612