building an integrated approach to improvement with...
TRANSCRIPT

© 2011 Institute for Healthcare Improvement
Building an Integrated Approach to Improvement with Lean, Six Sigma
and the Model for Improvement
23rd IHI National Forum 2011Dennis Deas, MBA
Robert Lloyd, Ph.D.
Kathy Luther, RN
Tuesday 6 December 2011
Session C9
© 2011 Institute for Healthcare Improvement
Objectives
• Describe the similarities and differences among Lean, Six Sigma, and the Model for
Improvement
• Determine which approach(es) are most appropriate for their organization
• Initiate a plan to build an integrated quality improvement strategy

© 2011 Institute for Healthcare Improvement
Faculty
Dennis Deas, MBASenior Director,
Healthcare Performance ImprovementKaiser Permanente
Robert Lloyd, Ph.D.Executive Director Performance Improvement
Institute for Healthcare Improvement
Kathy Luther, RNVice President
Institute for Healthcare Improvement
These presenters have nothing to disclose.
© 2011 Institute for Healthcare Improvement
Discussion Topics
• The foundation for improvement
• Compare and contrast Lean, Six Sigma and the Model for Improvement
• Case Study on integrating various models
• Determining which model is most appropriate for your organization

© 2011 Institute for Healthcare Improvement5
Deductive Phase
(general to specific)
Inductive Phase
(specific to general)
Source: R. Lloyd Quality Health Care, 2004, p. 153.
Theory
and Prediction
The Scientific Method provides the foundation for all improvement
© 2011 Institute for Healthcare Improvement
Source: Moen, R. and Norman, C. “Circling Back: Clearing up myths about the Deming cycle and seeing how it keeps evolving,” Quality Progress November, 2010:22-28.
Understanding the Timeline is Critical

© 2011 Institute for Healthcare Improvement
Adapted from R. Scoville, Ph.D., IHI Improvement Advisor
19th century Pragmatism played a major role in building knowledge for improvement
• Darwinian notions of variation, population, and selection infiltrated a wide range of disciplines:
• Epistemology – C.S. Pierce
• Psychology – William James, Edward Thorndike
• Sociology and education – George Mead, John Dewey
• Development – J.Baldwin, J.Piaget
• Law – Oliver Wendell Holmes
• Philosophy – B. Russell, K. Popper, L. Wittgenstein
• Some key notions
• Belief is observable only through action
• Action is inherently a ‘bet’ on its results
• Routinely successful action = ‘habit’ = ‘knowledge’
© 2011 Institute for Healthcare Improvement
Charles S. Peirce (1839–1914) The founder of American pragmatism. He wrote on a wide range of topics, from mathematics, to logic, semiotics and psychology.
William James (1842–1910) An influential psychologist and theorist of religion, as well as philosopher and a physician. First to be widely associated with the term "pragmatism" due mainly to Charles Peirce’s difficult personality.
“As a rule we disbelieve all the facts and theories for which we have no use.”
William James
Classical Pragmatists (1850-1950)

© 2011 Institute for Healthcare Improvement
C. I. Lewis (1883-1964)Perhaps the most important American academic philosopher active in the 1930s and 1940s. He was the founder of conceptual pragmatism and made major contributions in epistemology and logic, and, to a lesser degree, ethics. Lewis was also a key figure in the rise of analytic philosophy in the US. He also had a profound impact on Walter Shewhart and subsequently Edwards Deming..
John Dewey (1859–1952)Prominent philosopher of education, referred to his brand of pragmatism as “instrumentalism. “
Classical Pragmatists (1850-1950)
© 2011 Institute for Healthcare Improvement
Source: Moen, R. and Norman, C. “Circling Back: Clearing up myths about the Deming cycle and seeing how it keeps evolving,” Quality Progress November, 2010:22-28.
Understanding the Timeline is Critical

©Copyright 2009 IHI
1939
The Deming Wheel1. Design the product (with appropriate tests).2. Make it; test it in the production line and in the laboratory.3. Sell the product.4. Test the product in service, through market research. Find out
what user think about it and why the nonusers have not bought it.
1950
Development of the Shewhart Cycle
1986
Source: Moen, R. and Norman, C. “Circling Back” Quality progress, November 2010: 22-28.
Walter A. Shewhart(1891 – 1967)
The Shewhart Cycle for Learning and Improvement
Act Plan
Study Do
Act – Adopt the change, abandon it or run through the cycle again.
Plan – plan a change or test aimed at improvement.
Study – Examine the results. What did we learn? What went wrong?
Do – Carry out the change or test (preferably on a small scale).
(Deming, 1993)

© 2011 Institute for Healthcare Improvement
In the spring of 2010 the BMJ sponsored the Vin McLoughlin Symposium on the Epistemology of Improving Health Care. The papers that grew out of this symposium are freely available online under the BMJ journal’s unlock scheme:
http://qualitysafety.bmj.com/site/about/unlocked.xhtml
Knowledge for Improvement Continues to Evolve
BMJ Quality & SafetyApril 2011 Vol. 20, No Suppl. 1
Epistemology (from Greek epistēmē), meaning "knowledge, science", and (logos), meaning "study of" is the branch of philosophy concerned with the nature and scope (limitations) of knowledge.
It addresses the questions:
• What is knowledge?
• How is knowledge acquired?
• How do we know what we know?
© 2011 Institute for Healthcare Improvement
Variations on a Theme
• Baldrige Performance Excellence Program
• European Foundation for Quality Management (EFQM)
• International Organization for Standardization (ISO)
• Lean Enterprise (Toyota Production System, TPS)
• Six Sigma Methodologies (Design for Six Sigma, DFSS)
• Model for Improvement (MFI)

Six Sigma, Lean, MFI
Define
Six Sigma
Analyze
Measure
Improve
Control
Identify
Value
Understand
Value Stream
Eliminate
Waste
Establish
Flow
Enable Pull
Pursue
Perfection
Lean
Source: The Improvement Guide, API
Similarities
• Have disciplined processes and approaches
• Rely heavily on detailed measures
– Lean– process steps, value
– Six Sigma – Defects per 1,000,000 opportunities
– MFI – Process, outcome measures
• Have a specific language and tools
• Have a long history in the field
– Lean – Japanese production -Toyota-healthcare
– Six Sigma – Japanese – Motorola, GE-healthcare
– MFI – Shewhart, Deming, Japanese Union of Scientists and Engineers
(JUSE)
But, there is
no
“Rule Book”

Six Sigma Specifics
Define problem in detail
Measure a “defect”. Turn into “defects per million” - -Sigma Level
Analyze
In-depth analysis using process measures, flow charts, defect analysis to determine under what conditions defects occur
Improve Define and test changes aimed at reducing defects
Control What steps will you take to maintain performance
Tools: Flow charts, process maps, Prioritization matrix, force field analysis, etc
Define
DMAIC - steps
Analyze
Measure
Improve
Control
Six Sigma Level
Define
DMAIC
Analyze
Measure
Improve
Control
Sigma LevelDefects Per Million Opportunities
(DPMO)
1 690,000
2 308,537
3 66,807
4 6,210
5 233
6 3.4
Example: Ventilator Associated Pneumonia (VAP)
Defect = 1 VAP Opportunity = 1 Vent Day
1 VAP per 500 vent days = 2000 per 1,000, 000 (DPMO)
4.38 – Sigma Level
4.38
What if?
• Surgical site infections are 10 per quarter
• BSIs are 8 per line day
• VAPs are 3 per 1000 line days

Lean Specifics
• What is “Value” from the
customer’s point of view
• Develop “Value Stream (VS)” to
determine steps, value added,
identify waste
• Improve flow, cycle time and value
• Selected terms: Muda (Waste), VS,
5S, Kaizen, Pull Systems, Just In
Time, Poka Yoke (Mistake Proofing)
Identify
Value
Understand
Value Stream
Eliminate
Waste
Establish
Flow
Enable Pull
Pursue
Perfection
Model for Improvement (MFI)
• What are you trying to
solve?
• How will you know?
• What changes will you
make?
• Predict-Test-Observe
• Shewart cycle
• Reach your “aim”
• Hold the gain
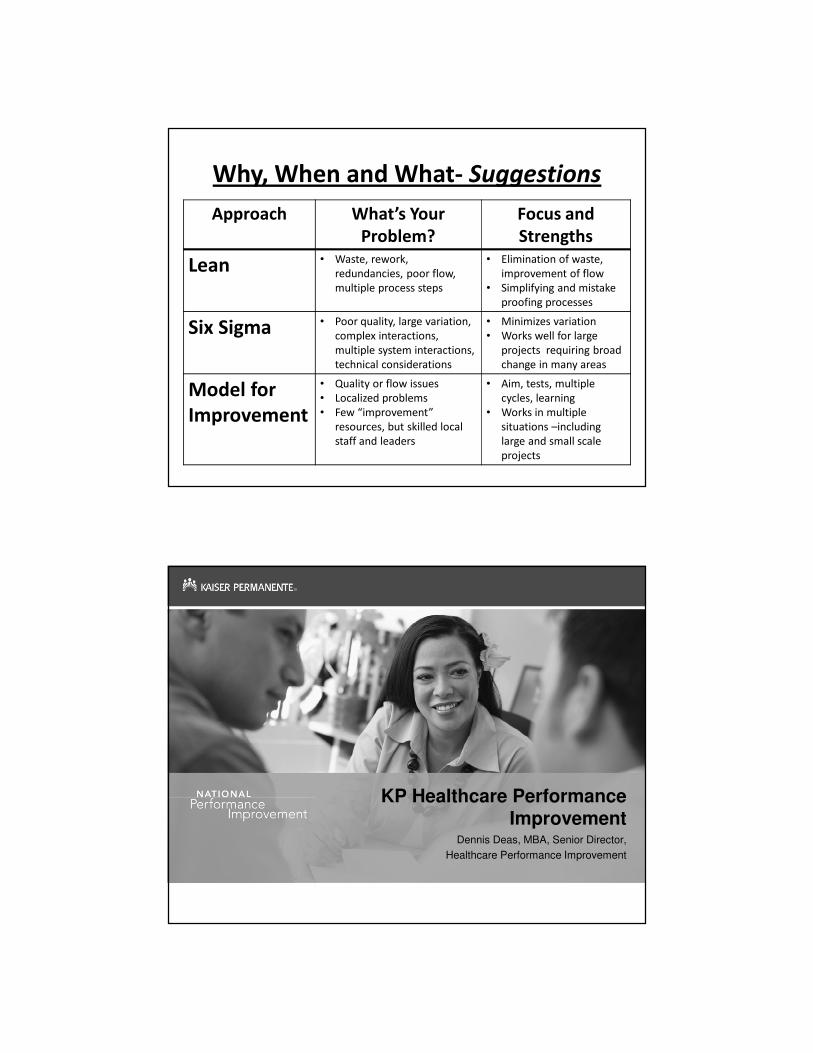
Why, When and What- Suggestions
Approach What’s Your
Problem?
Focus and
Strengths
Lean • Waste, rework,
redundancies, poor flow,
multiple process steps
• Elimination of waste,
improvement of flow
• Simplifying and mistake
proofing processes
Six Sigma • Poor quality, large variation,
complex interactions,
multiple system interactions,
technical considerations
• Minimizes variation
• Works well for large
projects requiring broad
change in many areas
Model for
Improvement
• Quality or flow issues
• Localized problems
• Few “improvement”
resources, but skilled local
staff and leaders
• Aim, tests, multiple
cycles, learning
• Works in multiple
situations –including
large and small scale
projects
KP Healthcare Performance Improvement
Dennis Deas, MBA, Senior Director,
Healthcare Performance Improvement

23
Are we Lean or Six Sigma?
“YES, but we are really what we strive to achieve, a world class organization”
- Lean: production and flow (waste and time reduction)
- Six sigma: decision making and defects (reducing failures)
- Tests of change: applying theory to real work
24
We Lead with a Principles and Systems Approach based
on the Attributes of a High Performing Organization
Best qualityBest service
Most affordableBest place to
work
KP needs to build capability in these six areas in order to achieve breakthrough performance
© Kaiser Permanente 2011 reproduce by permission only

25
These tenants are key to building capacity at the local levels and to aligning prior performance improvement initiatives
Leadership
Measurement
• Leadership engaged and aligned
• Set clear priorities based on vital few breakthrough performance areas
• Shape organizational strategy by priority areas, focusing on clinical, financial, employee, and patient indicators
• Cascade systems to communicate from macro to micro levels
Systems • Grow organizational leadership team capability to identify core business processes
• Establish local and national oversight infrastructure to manage improvement priorities and monitor progress
• Establish process map for those core areas and align improvement priorities with vital business needs
Learning
Culture
Capacity
• Build capacity to set outcomes and improvement process metrics for key areas
• Establish performance targets to achieve best in class at national level
• Use balanced scorecard system and time-trended metrics at front line departments to build visibility and accountability
• Surface best practices based on evident of performance
• Create sharing learning, spread systems, and capability to drive performance across enterprise
• Focus on top-down and bottom-up execution
• Establish oversight system at macro and micro levels by creating improvement infrastructure and staff
• Develop ability to execute from testing through spread of practice at all levels
• Embrace unified internal improvement methodology, representing multiple methods
• Deploy internally designed improvement curriculum, focused at several levels of staff and physicians
• Apply improvement skills immediately to improvement priorities
• Engage staff in improvement to make change meaningful
• Use Fellowship model to teach organizational level leaders deeper improvement skills
26
Top
do
wn
Re
du
ce
va
ria
tio
n
Learning system
• Economic and social context for change
• Models of workplace learning and innovation
• Team performance
• Define organizational needs
• Create system view
• Plan/ manage improvement
• Align with strategy
• ID drivers and portfolios
• Build capability to improve
• Engaging the hearts and minds of the front line
• Creating “line of sight” to strategic goals
• Define high performing unit-based teams
Bo
ttom
up
Le
arn
ing
an
d im
pro
ve
me
nt
Top Down and Bottom UpStrategic Alignment
Principles What we “do”
© Kaiser Permanente 2011 reproduce by permission only
Adapted from Batalden et al 2007

27
28
Just Do It IDEO
Innovation
Six sigma
N
N N
N
N
Y
YYY
N
N
Y
Y
Y
Is the Solution Known
?
Is Root Cause Known
?
Is it a New
Product or
Process ?
Is Cycle time
Reduction the
Objective ?
Is the Bottleneck Defect Driven
?
Does a Process
Management System
Exist ?
Recognize a Problem
N
Obvious root cause,obvious solution
Rapid Improvement EventObvious root
cause, non-data driven solution
Lean
Process Improvement Methodology Assignment
Process Management

29
Just Do It
• When the solution is known
• KP uses the assess, develop, test, implement/control approach
• Assess current state and data
• Identify the solution you will test
• Test the solution to insure sustainable integration into workflows
• Implement and control solution to insure sustained performance
• Take action if improvement not achieved
Add Diversions to Waiting Areas
Reduce No-Shows with Reminder Calls
Improve Signage
30
Rapid Improvement Events
• Employee involvement in developing and implementing recommendations
• Solutions will be generated via front line knowledge
• Root causes are known
• Simple tools used (fishbone, process map, Pareto)
• Data analysis, statistical tools not required
• Often involve Lean 6S & mistake proofing projects in workplace – Set, Sort, Shine, Standardize, Sustain, Safety
• Management commits to quickly making decisions on team recommendations (yes / no / further study required)
• 1-3 days of team meetings required w/ facilitator
• Less than 30 days to implement recommendations
• Little or no capital required
Improve Transport Response
Radiology Patient Flow
31
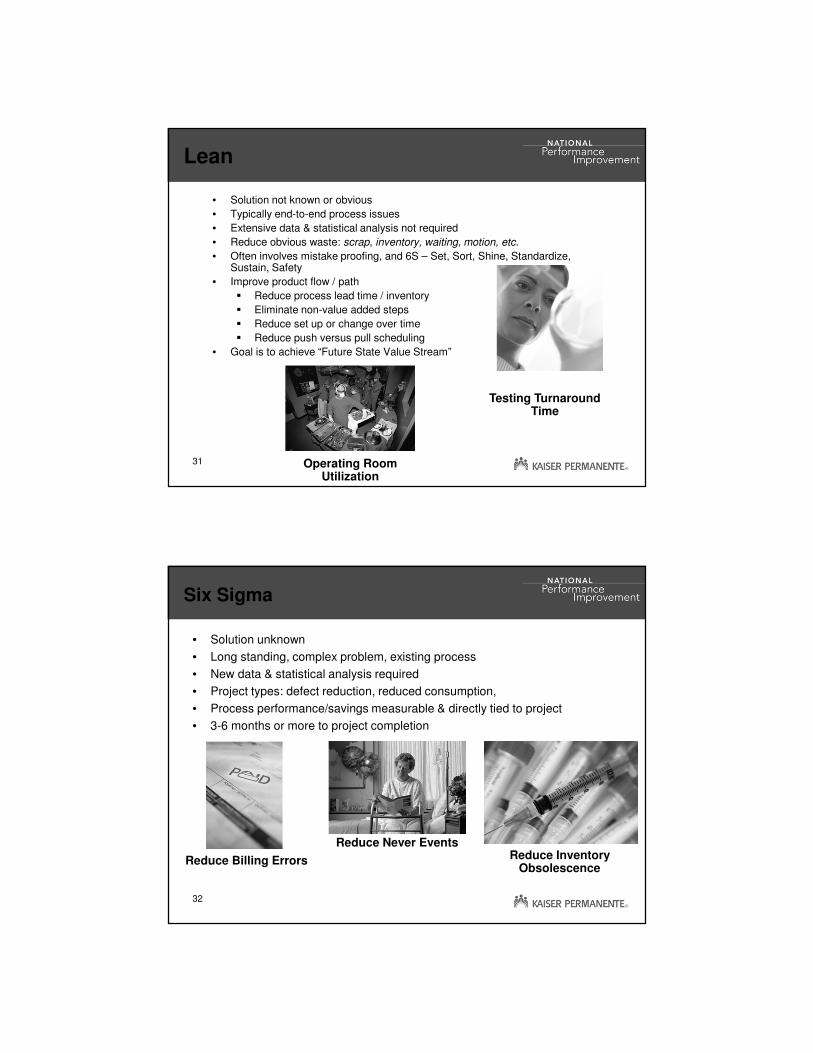
Lean
• Solution not known or obvious
• Typically end-to-end process issues
• Extensive data & statistical analysis not required
• Reduce obvious waste: scrap, inventory, waiting, motion, etc.
• Often involves mistake proofing, and 6S – Set, Sort, Shine, Standardize, Sustain, Safety
• Improve product flow / path
� Reduce process lead time / inventory
� Eliminate non-value added steps
� Reduce set up or change over time
� Reduce push versus pull scheduling
• Goal is to achieve “Future State Value Stream”
Operating Room Utilization
Testing Turnaround Time
32
Six Sigma
• Solution unknown
• Long standing, complex problem, existing process
• New data & statistical analysis required
• Project types: defect reduction, reduced consumption,
• Process performance/savings measurable & directly tied to project
• 3-6 months or more to project completion
Reduce Never EventsReduce Inventory
ObsolescenceReduce Billing Errors

33
What are our first steps?
• Assessment: problem statement, identification of root causes or flow charts and levers for improvement with drivers, prioritization of projects, scoping and resourcing using a charter
• Select/plan: defining what the focus will be – flow, defect reduction, redesign?
• Test: changes and application in real time before implementation
• Implement/control: Apply to processes locally to make part of core work and macro process standardization (ie. training, procedures)
34
Performance Improvement Project Checklist
� Org/Team Charter� Problem Statement
� Goal Statement
� Scope
� Team roles and time commitments
� Timeline/Milestones
� Project Prioritization
� Driver Diagram
Assess Develop/ ID Changes Test Implement/Control
� 6 S
� Identify Waste
� Cause and Effect (Fishbone)
� OPI (Output –Process – Input)
� FMEA (Failure Modes & Effects Analysis)
� Evidence-based Practice
� PDSA Action plan
� Test using PDSA Action Plan
� Annotated Run Charts
� PI Leadership Report
� Solutions Tested
� Work Instructions
� Visual Display
� Control Charts/ SPC
� Sustainability Plan with annotated run and control charts
� ROI Template
� Storyboard
� Project Closure Form
� Stakeholder Analysis
� Value Stream (with metrics)
� Process Flow Map
� Voice of the Customer
� Baseline measures
What are we trying to accomplish?How will we know the change is an improvement?What change can we make that will result in improvement?
Name:Medical Center/Region:Project Title:
Signed by:
<insert name> (HP Sponsor)
<insert name> (Labor Sponsor)
<insert name> (Finance Sponsor)
<insert name> (Med Group Sponsor if applicable)
<insert name> (IA)
� These subjects are taught in the Regular Institute (our version of
Green Belt training)
�We teach Spread & Scale, Patient Safety, Advanced Change
Management, Management Systems, Planned Experimentation,
Management Engineering, and Innovation in the Advanced Institute
(our version of Black Belt training)
35
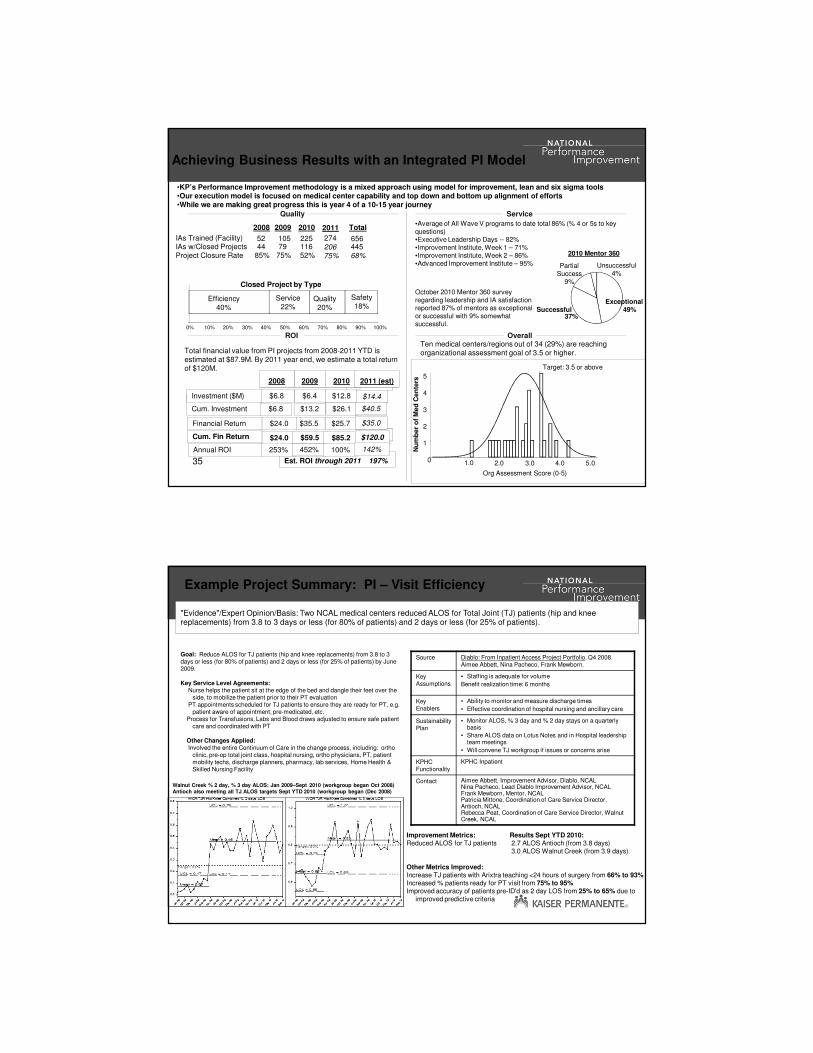
October 2010 Mentor 360 survey regarding leadership and IA satisfaction reported 87% of mentors as exceptional or successful with 9% somewhat successful.
Achieving Business Results with an Integrated PI Model
ROI Overall
Quality Service
•KP’s Performance Improvement methodology is a mixed approach using model for improvement, lean and six sigma tools•Our execution model is focused on medical center capability and top down and bottom up alignment of efforts•While we are making great progress this is year 4 of a 10-15 year journey
Est. ROI through 2011 197%
$24.0Cum. Fin Return
$25.7$35.5$24.0Financial Return
$13.2Cum. Investment
$12.8$6.4$6.8Investment ($M)
201020092008
Total financial value from PI projects from 2008-2011 YTD is estimated at $87.9M. By 2011 year end, we estimate a total return of $120M.
•Average of All Wave V programs to date total 86% (% 4 or 5s to key questions)•Executive Leadership Days -- 82%•Improvement Institute, Week 1 – 71%•Improvement Institute, Week 2 – 86%•Advanced Improvement Institute – 95%
2010 Mentor 360
Partial Success
9%
Successful37%
Exceptional49%
Unsuccessful4%
2008 2009 2010
IAs Trained (Facility) 52 105 225IAs w/Closed Projects 44 79 116
Closed Project by Type
Efficiency40%
Quality20%
Safety18%
Service22%
0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100%
Total
656445
$26.1
2011 (est)
$14.4
$40.5
$35.0
$59.5 $85.2 $120.0
$6.8
Annual ROI 253% 452% 100% 142%
0
1
2
3
4
5
2.0 3.0 4.0 5.0
Org Assessment Score (0-5)
Nu
mb
er
of
Med
Cen
ters
Target: 3.5 or above
1.0
Ten medical centers/regions out of 34 (29%) are reaching organizational assessment goal of 3.5 or higher.
Project Closure Rate 85% 75% 52% 68%
2011
27420675%
36
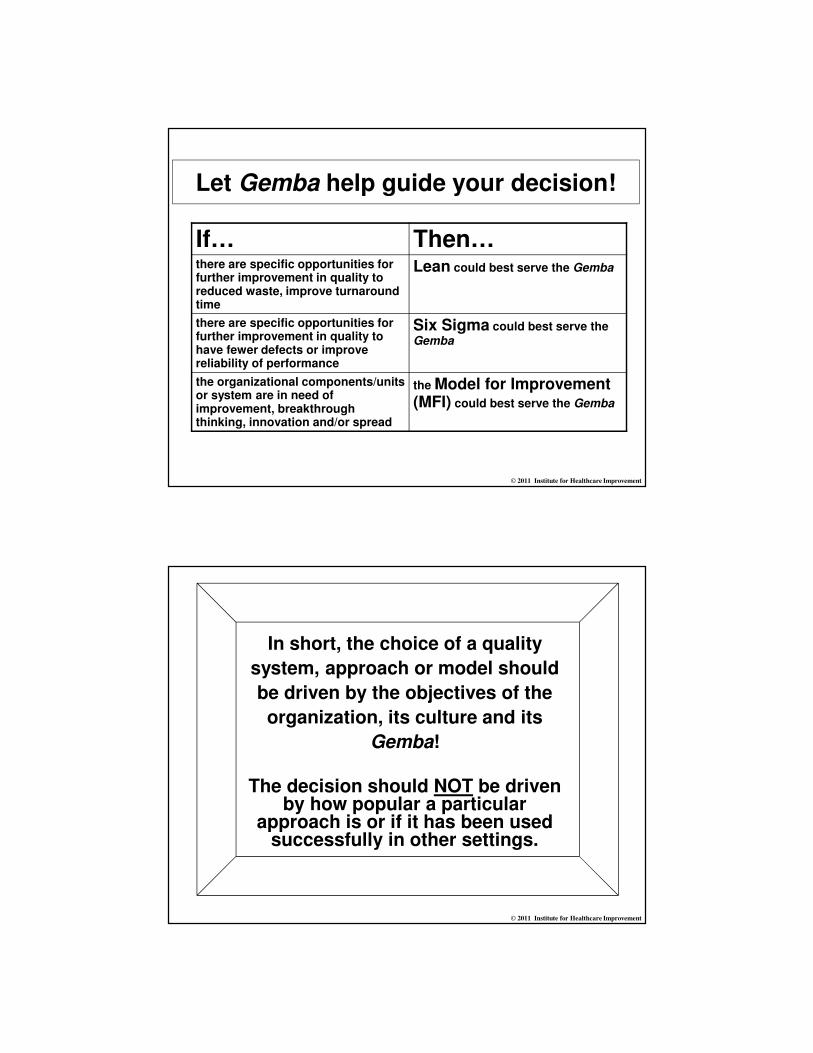
"Evidence"/Expert Opinion/Basis: Two NCAL medical centers reduced ALOS for Total Joint (TJ) patients (hip and knee replacements) from 3.8 to 3 days or less (for 80% of patients) and 2 days or less (for 25% of patients).
Example Project Summary: PI – Visit Efficiency
Source Diablo: From Inpatient Access Project Portfolio, Q4 2008. Aimee Abbett, Nina Pacheco, Frank Mewborn.
Key Assumptions
• Staffing is adequate for volume
Benefit realization time: 6 months
Key Enablers
• Ability to monitor and measure discharge times
• Effective coordination of hospital nursing and ancillary care
Sustainability Plan
• Monitor ALOS, % 3 day and % 2 day stays on a quarterly basis
• Share ALOS data on Lotus Notes and in Hospital leadership team meetings
• Will convene TJ workgroup if issues or concerns arise
KPHC Functionality
KPHC Inpatient
Contact Aimee Abbett, Improvement Advisor, Diablo, NCALNina Pacheco, Lead Diablo Improvement Advisor, NCALFrank Mewborn, Mentor, NCALPatricia Mittone, Coordination of Care Service Director, Antioch, NCAL Rebecca Peat, Coordination of Care Service Director, Walnut Creek, NCAL
Goal: Reduce ALOS for TJ patients (hip and knee replacements) from 3.8 to 3 days or less (for 80% of patients) and 2 days or less (for 25% of patients) by June 2009.
Key Service Level Agreements:Nurse helps the patient sit at the edge of the bed and dangle their feet over the
side, to mobilize the patient prior to their PT evaluationPT appointments scheduled for TJ patients to ensure they are ready for PT, e.g.
patient aware of appointment, pre-medicated, etc.Process for Transfusions, Labs and Blood draws adjusted to ensure safe patient
care and coordinated with PT
Other Changes Applied:Involved the entire Continuum of Care in the change process, including: ortho
clinic, pre-op total joint class, hospital nursing, ortho physicians, PT, patient mobility techs, discharge planners, pharmacy, lab services, Home Health & Skilled Nursing Facility
Improvement Metrics: Results Sept YTD 2010:Reduced ALOS for TJ patients 2.7 ALOS Antioch (from 3.8 days)
3.0 ALOS Walnut Creek (from 3.9 days)
Other Metrics Improved:Increase TJ patients with Arixtra teaching <24 hours of surgery from 66% to 93%Increased % patients ready for PT visit from 75% to 95%Improved accuracy of patients pre-ID'd as 2 day LOS from 25% to 65% due to
improved predictive criteria
Walnut Creek % 2 day, % 3 day ALOS: Jan 2009–Sept 2010 (workgroup began Oct 2008)Antioch also meeting all TJ ALOS targets Sept YTD 2010 (workgroup began (Dec 2008)

© 2011 Institute for Healthcare Improvement
So, where do I begin to untangle
all this stuff?
© 2011 Institute for Healthcare Improvement
“It should be fairly obvious that no single quality system, set of quality criteria or even quality philosophy is ever going to be the solution by itself to a firm’s
quality problems.”
H. Scott Tonk. “Integrating ISO 9001:2000 and Baldrige Criteria”Quality Progress August, 2000.

© 2011 Institute for Healthcare Improvement
“The main criterion for choosing a quality
system is how well it serves the needs of the
Gemba”
Kelly Allen, “Get Into Gemba” Quality Progress April, 2004
© 2011 Institute for Healthcare Improvement
Gemba (the real place)
• Literally translated to mean “The place of specific work” or “the “real place”
• Peter Scholtes (The Leader’s Handbook, McGraw-Hill, 1998) defines it as “the critical resources and sequence of interdependent activities that add value to the customer.”
• The Gemba for a manufacturing company could include product design and development, production, delivery and maintenance.
• The Gemba for a service organization might include service design, development and delivery, flow and customer service.
• In healthcare, Gemba could include a clinic visit with the physician, the physical therapy department, an OR procedure, the patient’s room or a home care visit.
• Activities related to finance, HR and IT are NOT Gemba but should support the Gemba.
• Understanding your organization's Gemba will help you decide which quality system or approach is most appropriate.
© 2011 Institute for Healthcare Improvement
Let Gemba help guide your decision!
If… Then…there are specific opportunities for further improvement in quality to reduced waste, improve turnaround time
Lean could best serve the Gemba
there are specific opportunities for further improvement in quality to have fewer defects or improve reliability of performance
Six Sigma could best serve the Gemba
the organizational components/units or system are in need of improvement, breakthrough thinking, innovation and/or spread
the Model for Improvement (MFI) could best serve the Gemba
© 2011 Institute for Healthcare Improvement
In short, the choice of a quality
system, approach or model should
be driven by the objectives of the
organization, its culture and its
Gemba!
The decision should NOT be driven by how popular a particular
approach is or if it has been used successfully in other settings.

© 2011 Institute for Healthcare Improvement
ExerciseUnderstanding your Gemba
1. Form small groups (about 8-10 people).
2. Each individual should write down what they think the Gemba of their unit or department is and then identify the Gemba of the entire organization (don’t talk to anyone while doing this).
3. Next, note some of the areas that support the Gemba. Use the worksheet provided on the next page.
4. As a group, discuss your individual ideas about Gemba and note similarities and differences within your group’s responses.
© 2011 Institute for Healthcare Improvement
Gemba Exercise Worksheet
The Gemba of my unit or
department
The Gemba of my organization
Units and departments that
support the Gemba
© 2011 Institute for Healthcare Improvement
Now, combine your knowledge of Gemba with the review of the approaches described earlier in the workshop and
complete the worksheet on the next page.
Use the following questions to guide your work:
1. Can you evaluate your current approach or model to QI in light of what you have learned today?
2. Does your current approach or model allow you to successfully achieve your Gemba?
3. What are some of the advantages and disadvantages of each approach for your organization?
Exercise: Selecting an Approach
© 2011 Institute for Healthcare Improvement
What will work best for your Gemba?
Quality Approach
Advantages Disadvantages
Six Sigma
Lean
The Model for Improvement

© 2011 Institute for Healthcare Improvement
Suggested Reading• BMJ Quality & Safety. Papers from the Vin McLaughlin Symposium on the
Epistemology of Improving health Care. April 12-16, 2010. BMJ Qual ity & Safety, April 2011, Vol. 20, No. Supplement 1.
• Edmonds, D. and Eidinow. Wittgenstein’s Poker: The Story of a Ten-Minute Argument between Two Great Philosophers. Harper Collins Publishers, 2001.
•• Lastrucci, C. The Scientific Approach: Basic principles of the Scientific Method.
Schenkman Publishing Company, Inc., 3rd printing 1967.
• Lewis, C. I. Mind and World Order. Reprinted by Dover Press, 1929.
• Moen, R. and Norman, C. “Circling Back: Clearing up myths about the Deming cycle and seeing how it keeps evolving,” Quality Progress November, 2010:22-28.
• Shewhart, W. A. Statistical Method from the Viewpoint of Quality Control. US Department of Agriculture. Dover Publications, 1939 (reprinted 1986).
• Wallace, W. The Logic of Science in Sociology. Aldine Publishing Company, 1971.
© 2011 Institute for Healthcare Improvement
Thanks for joining us this afternoon!
Please let us know if you have any questions.
Dennis [email protected]
Robert [email protected]
Kathy [email protected]

© 2011 Institute for Healthcare Improvement
“The greatest thing in the “The greatest thing in the “The greatest thing in the “The greatest thing in the world is not so much where world is not so much where world is not so much where world is not so much where
you stand, as in what you stand, as in what you stand, as in what you stand, as in what direction we are moving.”direction we are moving.”direction we are moving.”direction we are moving.”
~Oliver Wendell Holmes
Where are you headed?