building the case for integrating the surgical services suite l md buyline
TRANSCRIPT

Building the Case For Integrating the Surgical Services SuiteJames Laskaris, EE, BMETom Watson, BS, RCVTLoretta Loncoske, BS, R.T. (R)
– Joined MD Buyline in 1986– 35 years in the fields of cardiology and
healthcare– Previously served as the Administrative
and Technical Director of Cardiology
Department, West Jefferson Medical
Center, New Orleans, LA– Registered in Noninvasive and Invasive
Cardiovascular Modalities, National
Society of Cardiovascular Technologies
– Joined MD Buyline in 1994– Over 30 years in the healthcare field– Previously served as Clinical
Engineering Department Director,
Service Master, Central, WI– Primary analyst of high end OR
technology– Covers legislative and reimbursement
impact on healthcare
Tom Watson, BS, RCVTSenior Clinical Analyst,
MD Buyline
James Laskaris, EE, BMESenior Emerging Technology Analyst,
MD Buyline
Presenters
– Joined MD Buyline in 1991– Over 30 years in the radiology field– Previously served as the Director of
Radiology, Florida Keys Memorial
Hospital– Member of ARRT and ASRT– Member of HIMSS and SMM
Loretta Loncoske, BS, R.T. (R) Senior Clinical Analyst,
MD Buyline
2

3
The Changing Healthcare Landscape
• HITECH Act is modernizing delivery of healthcare by
improving efficiencies with IT solutions
– Estimated to save ~$200 billion over the next 10 years
• Integrated surgical services includes integrated OR, interventional
hybrid OR and intraoperative iMRI/iCT
– Adoption is complicated by high cost and lack of direct ROI
– Integrated surgical services can lower costs in indirect ways
Reducing length of stay
Improving outcomes
Offering shorter recover time
– Controlling costs and improving quality of care are a major focus in healthcare

4
Agenda
• Review the following for integrated ORs, hybrid ORs and
intraoperative iMRI/iCT
– The Market
– Technology and Costs
– Vendors
– Clinical Outcomes
– Financial Considerations and Reimbursement
– Takeaways

5
Integrated OR: Introduction
• Integrated operating rooms (ORs) offer improved surgical experience
through the incorporation of multiple components
• Clinical studies have found integrated ORs decrease OR time and
improve outcomes
• Most direct costs in OR are fixed; labor is the best target to reduce
costs by:
– More efficient use of OR staff
– Increased patient volume
– Optimizing procedure time
• Time becomes the most important factor in offsetting costs

Do you currently have or are you thinking of investing in integrated OR?
• Yes, we currently have one
• We are considering one
• No
• Don’t know
Poll Question
6

7
Integrated OR: The Market
• ~37,000 ORs in the U.S. are performing 51.4 million inpatient surgical
procedures
• 20% of ORs have some form of integrated technology
• Integrated ORs are not applicable to all surgical settings and should be
targeted at high volume, high impact settings:
– Arteriography and angiocardiography (contrast material): 2.4 million
– Cardiac catheterizations: 1.0 million
– Endoscopy of small intestine with or without biopsy: 1.1 million
– Endoscopy of large intestine with or without biopsy: 499,000
– Balloon angioplasty of coronary artery/coronary atherectomy: 500,000
– Reduction of fracture: 671,000
– Insertion of coronary artery stent: 454,000
– Coronary artery bypass graft: 395,000
– Total knee and hip replacement: 1 million

8
Integrated OR: Technology and Costs
• Integrated ORs are custom designed for provider’s needs
– Typically utilize several different vendors' products for a functional system
Large variation in pricing
• Typical modules/functional features of an integrated OR systems
include:
Basic Automated Systems Telemedicine Real-Time Information

9
Integrated OR: Automation
• Automation allows surgeons greater
control of their environment by
linking individual pieces to a central
device
• Benefits of automation:
– Relieves strain on surgeons and staff from lengthy cases
– Surgical suite can be instantly configured
Avoid delays from reconfiguring equipment
More efficient use of nursing staff
Room wait time reduced by 10 minutes
Surgical time reduced by 15 minutes
• Cost* ranges from $20,000 to $50,000
– Upgrading individual pieces of equipment: $1,500 to $2,000 per device
*Source = MD Buyline

10
Integrated OR: Telemedicine
• Telemedicine allows the transfer of medical
information for diagnosis, therapy and
education between medical professionals
located remotely
• Benefits of Telemedicine:
– Easier for hospitals to incorporate new
procedures
– Removes the need for surgeons and staff
to leave practices to learn new techniques offsite
• Cost* ranges from $30,000 to $400,000 per room
– Pricing variation due to:
Inclusion of two-way communication
If system is closed to the facility or broadcasted
*Source = MD Buyline

11
Integrated OR: Real Time Information Packages
• Real time information packages allow for integration of high level
information into OR
• Benefits of Real time information:
– Access to PACS images, EHRs and lab reports
– Consultations between surgeons, radiologists, or pathologists without requiring
physical presence in the surgical suite
– Visual record of the surgery
• Cost* ranges from $20,000 to $500,000
per room
– Higher pricing is related to incorporation of
two-way communication
*Source = MD Buyline

12
Integrated OR: Vendor 1
• Option A
– IP conferencing platform utilizes hospital's network infrastructure to facilitate video-
conferencing and broadcasting from within the OR
• Option B
– HD digital video routing system, supports all video standards and resolutions
– System features: integrated surgical checklist, customizable room presets and centralized
OR equipment controls
• Option C
– Provides centralized storage for archiving and management of surgical videos and images
– Integration with hospital EMR allows direct access to surgical videos/images from patient
charts
Automation Cost* Telemedicine Cost* Real Time Information Cost*
$65,000 - $85,000 $100,000 - $180,000 $250,000+
*Source = MD Buyline
13
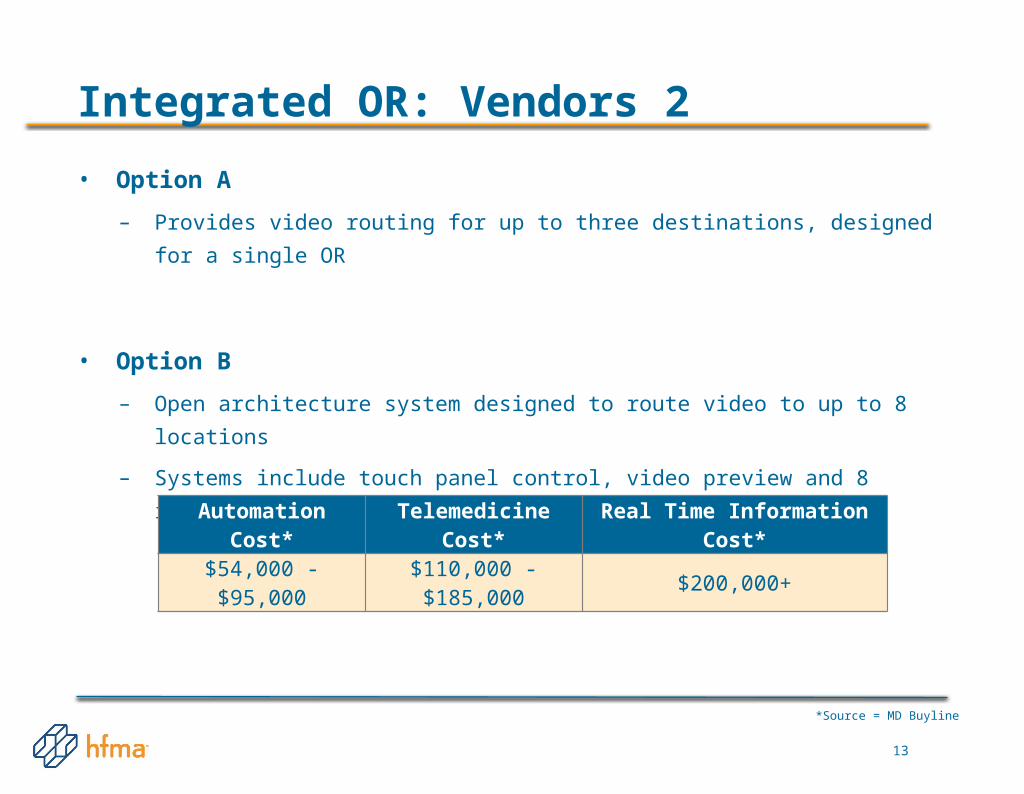
Integrated OR: Vendors 2
• Option A
– Provides video routing for up to three destinations, designed for a single OR
• Option B
– Open architecture system designed to route video to up to 8 locations
– Systems include touch panel control, video preview and 8 inputs
Automation Cost* Telemedicine Cost* Real Time Information Cost*
$54,000 - $95,000 $110,000 - $185,000 $200,000+
*Source = MD Buyline

14
Integrated OR: Vendors 3
• Option A
– Configured with HD video conferencing and HD streaming, multi-view windowing,
HD image capturing, HD video recording and hands-free VoIP communication
Automation Cost* Telemedicine Cost* Real Time Information Cost*
N/A $95,000 - $220,000 $220,000+
*Source = MD Buyline

15
Integrated OR: Vendor 4
• Option A
– Includes control of the scope surgical system, light source, insufflator, monitor,
image management, documentation system and OR environment
– Configuration includes audio/video visual capabilities (OR light cameras and
microphones), EHR, telemedicine and PACS interfacing
• Option B
– Offers control over all audio-visual components (routers, cameras, graphics
processors, flat panel displays, audio and video conferencing, etc.)
Automation Cost* Telemedicine Cost* Real Time Information Cost*
$50,000 - $85,000 $120,000 - $180,000 $200,000+
*Source = MD Buyline

16
Integrated OR: Vendor 5
• Option A
– Allows importation of EMR and PACS images in real time and control of endoscopic
towers and the OR environment
Automation Cost* Telemedicine Cost* Real Time Information Cost*
$20,000 - $65,000 $110,000 - $190,000 $200,000+
*Source = MD Buyline
17
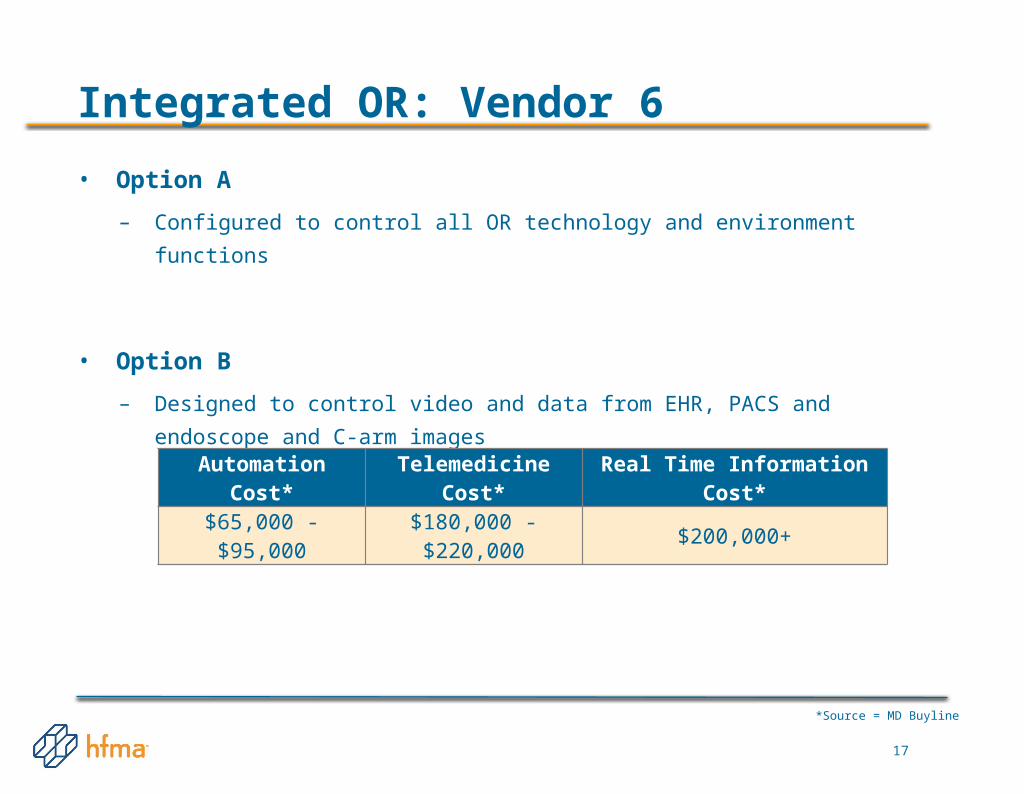
Integrated OR: Vendor 6
• Option A
– Configured to control all OR technology and environment functions
• Option B
– Designed to control video and data from EHR, PACS and endoscope and C-arm
images
Automation Cost* Telemedicine Cost* Real Time Information Cost*
$65,000 - $95,000 $180,000 - $220,000 $200,000+
*Source = MD Buyline

18
Integrated OR: Clinical Outcomes
• Integrated ORs improve efficiencies:
– Reduced number of unscheduled procedures from 25% to 14%
– Overtime events decreased from 28% to 21%
– Average savings of 78 minutes per case
– Frequency of “never-events” (foreign objects left inside the body or “wrong-site"
surgery) were cut by nearly half
– Increased precision
– Improved patient outcomes for neuro monitoring

19
Integrated OR: Financial Considerations and Reimbursement
• Lack of direct reimbursement
– CMS supports telemedicine for diagnostic and consult services
– No reimbursement for OR consults
• Opportunities for cost savings include:
– Increasing volume
– Decreasing time required for procedures
• Automating ORs saves:
– 5-18 minutes for minimally invasive orthopedic procedures
– An additional 30+ minutes for more reconstructive procedures
– 3-4 minutes of set up time for each case

20
Integrated OR: Financial Considerations and Reimbursement
*Source = MD Buyline
Mid-level procedure savings:
• $90 per case
• $49,500 per year*
High level procedure savings:
• $170 per patient
• $46,750 per year*

21
Integrated OR: Financial Considerations and Reimbursement
• Integrating an OR is difficult to sell on "Return on Investment" alone
• Automating several ORs in medium to large hospitals is financially viable
– Supported by CMS reimbursement
– Increase in revenue and profit seen over the term as compared to traditional
counterparts
• Automation technology can be too costly for low volume ORs

22
Integrated OR: Takeaways
• For the right facility, integrated OR is an attractive investment
– Provides additional revenue through increasing throughput, shortening procedural
time and improving patient outcomes
– Due to integrated OR’s significant cost, clinical and financial considerations must be
weighed carefully
Pros• Improved outcomes
- More precise surgeries
- Reduction in “never events”
• Improved efficiencies
- Reduced number of unscheduled procedures and overtime
- Higher throughput
Cons• High cost
• No direct reimbursement
• Multiple technology and applications
– Purchasing the right system is challenging
– Multiple vendors working together can make installation difficult

23
Hybrid OR: Introduction
• Hybrid ORs combine traditional angiographic imaging technology with
open-surgical capabilities
• Clinical applications include:
– Cardiovascular procedures
Interest began with transcatheter aortic valve replacement (TAVR) surgery
– Neurosurgery
– Thoracic surgery
– Endovascular procedures
• Hybrid ORs require significant financial investment and time to customize
– Utilization is key to making hybrid ORs financially attractive
Do you currently have or are you thinking of investing in hybrid OR technology?
• Yes, we currently have one
• We are considering one
• No
• Don’t know
Poll Question
24

25
Hybrid OR: The Market
• Market is increasing steadily
– Larger market trend toward minimally invasive surgical procedures that offer:
Less traumatic surgery
Shorter hospital stays
Quicker recovery times
Improved quality of life for the patient
• Growth is driven by the surgical side of the business
– Systems must comply with all surgical requirements
– TAVR alone does not offer sufficient caseload to maintain a reasonable ROI

26
Hybrid OR: Technology
• Extent of integration dependent on:
– Physicians using the room
– Volume
– Mix of procedures
• Four main components of a hybrid OR:
1. Imaging system (floor- or ceiling-mounted)
2. Imaging table/Surgical table option
3. Anesthesia gas lines
4. Surgical lights and booms
• Market focused on single plane solutions
– Growing interest in biplane technology in neurology
USF Health Communications

27
Hybrid OR: Imaging Vendor 1
• Option A
– Floor-based mobile unit uses laser guidance to move around the room
– Single room unit with all cables tethered to the ceiling
– Capital Costs*: $1,700,000 to $2,000,000
– Maintenance Costs*: $110,000 to $150,000 per year
*Source = MD Buyline

28
Hybrid OR: Imaging Vendor 2
• Option A
– Offered as both floor and ceiling mounted
system
Ceiling systems are more common
– Positions ceiling rails wider to allow:
Improved air flow
Reduced chance of contaminants in the
surgical field
– Capital Cost*: $1,100,000 to $1,400,000
– Maintenance Cost*: $70,000 to $90,000
per year
*Source = MD Buyline

29
Hybrid OR: Imaging Vendor 3
• Option A
– Ceiling-mounted positioner
– Capital Cost*: $1,000,000 to $1,200,000
– Maintenance Costs*: $75,000 to $95,000
per year
• Option B
– Floor-mounted positioner utilizing robotic arm
design technology to allow positioning of
floor mount away from table
– Capital Cost*: $1,400,000 to $1,900,000
– Maintenance Costs*: $100,000 to $125,000
per year*Source = MD Buyline

30
Hybrid OR: Imaging Vendor 4
• Option A
– Offered as both floor- or ceiling-mounted
Most configurations are floor-mounted
– Capital Costs*: $1,000,000 to $1,400,000
– Maintenance Costs*: $70,000 to $90,000 per year
*Source = MD Buyline

31
Hybrid OR: Table Options
• Application will influence table design
– Traditional surgical table designs are the most common
• Two main vendors provide surgical table solutions
– Tables are certify with imaging systems’ anti-collision software for patient and
equipment safety
– Imaging vendors may require purchase of interface option
– Installation, training and support are the OEM vendors responsibility
– Cost of surgical table options: $200,000 - $250,000*
*Source = MD Buyline

32
Hybrid OR: Table Vendor 1
• Full hybrid OR table-top
– Motor-driven movement simulate free-floating panning capability of traditional
imaging tables
• Capital Cost*: $225,000 to $300,000
• Maintenance Cost*: $8,000 to $15,000 per year
– Most facilities will maintain tables with in-house biomed support
*Source = MD Buyline

33
Hybrid OR: Table Vendor 2
• Two options
1. Motorized imaging table-top for interventional work
2. Traditional surgical table with flexible surgical breakdown features necessary for
a variety of surgical procedures
• Capital Cost*: $150,000 to $225,000
• Maintenance Cost*: $10,000 to $15,000 per year
– Most facilities will maintain tables with in-house biomed support
*Source = MD Buyline

34
Hybrid OR: Anesthesia Lines and Surgical Lights and Booms
• 3rd component of equipment planning – location of medical gas lines for
anesthesia
• 4th component of equipment planning – strategic planning of surgical lights
and booms
– Imaging vendors partner with major surgical light vendors
Providers should work through primary imaging vendor for lights/booms
Imaging vendor should take point on coordinating all vendors involved
*Source = MD Buyline
35
Hybrid OR: Clinical Challenges
• Areas Requiring Focus for Planning, Selection and Implementation
– Key Stakeholders: Interventional Cardiac, Interventional Vascular, Interventional
Neurology, Cardio-thoracic Surgery, Vascular Surgery or Neuro-Surgery
– Budget: Any budgetary constraints that might eliminate vendors or models or
configurations
– Projected Volume: Mix of patient procedures to maximize investment and provide optimal
Return on Investment
– Primary Focus: Interventional with surgical capabilities, or surgical focus with
interventional capabilities
– Gantry Orientation: Ceiling mounted, floor mounted or specialty design
– Table Requirements: This may come from the Key Stakeholders (Imaging Primary or
Surgical Primary)
– Table Vendor: Confirm validation with the imaging vendor of preference
– Surgical Lighting Vendor: Early identification is needed to ensure best outcomes from the
final integrated design of imaging, table and lighting
*Source = MD Buyline
36
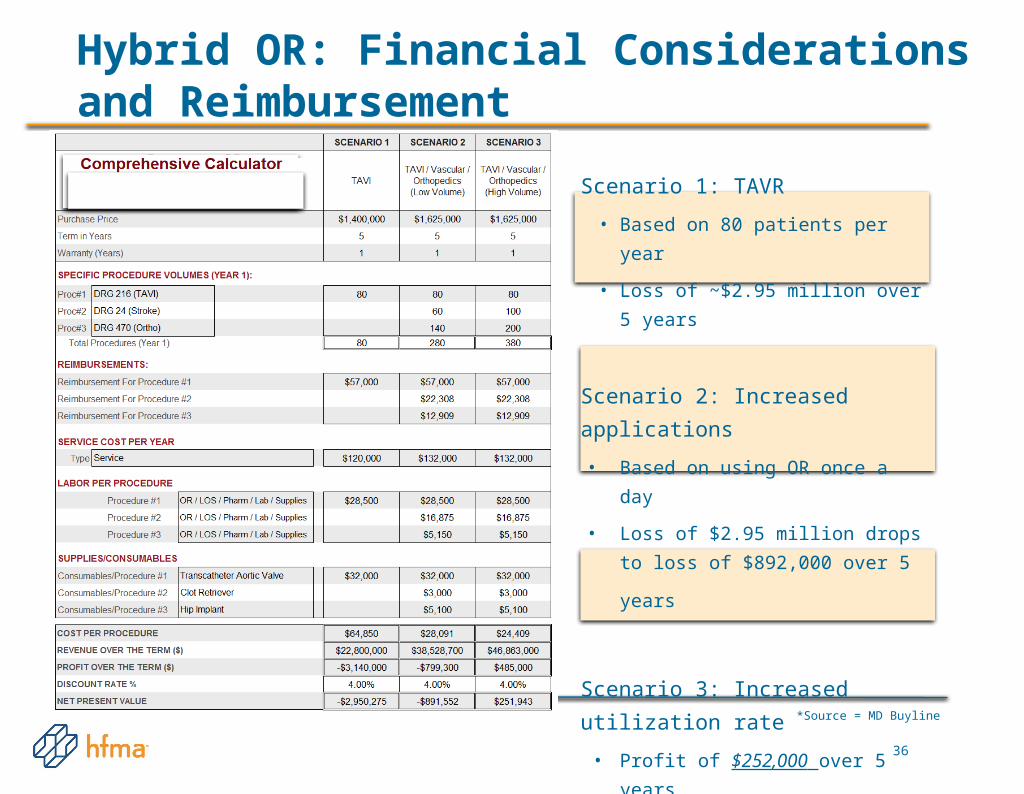
Hybrid OR: Financial Considerations and Reimbursement
Scenario 1: TAVR
• Based on 80 patients per year
• Loss of ~$2.95 million over 5 years
Scenario 2: Increased applications
• Based on using OR once a day
• Loss of $2.95 million drops to loss of
$892,000 over 5 years
Scenario 3: Increased utilization rate
• Profit of $252,000 over 5 years
*Source = MD Buyline

37
Hybrid OR: Takeaways
• Utilization and flexibility of the hybrid OR is paramount for maximizing
investment
– Versatility of the room for most facilities will be critical to success
– As minimally invasive procedures grow, so will the interest in hybrid OR
solutions Pros
• Consolidation of surgical and therapeutic approach
• Improved efficiency
• Provide leading edge interventional/surgical solutions
• For providers with high utilization rates and versatility, this can be a revenue generating technology
Cons• Challenging technology integration
• High cost for a multi-functional room
• No specific reimbursement
• Challenging medical specialty team approach (interventional/surgical/ anesthesia)
• May require cross department coordination
• Operational and supply management costs may be difficult to manage & track
• No single vendor solutions
38
iMRI: Introduction and Market
• Market growth is slow, driven primarily by neurosurgery applications
• iMRI offers improved clinical results:
– Improves tumor resection
– Reduces need for repeat surgeries
– Improves surgical safety
– Decreases patient length of stay
• iMRI costly, requiring:
– Specialized OR suites and instrumentation
– Longer anesthesia and OR times
– Significant time and personnel investment

Do you currently have or are you thinking of investing in iMRI?
• Yes, we currently have one
• We are considering one
• No
• Don’t know
Poll Question
39

40
iMRI: Technology
• Magnetic field strength: 1.2T, 1.5T and 3.0T
• Configuration: Stationary/fixed or mobile
– Fixed configuration: Patients transported to separate MRI room
All OR instruments/technology must be MRI compatible
– Mobile configuration: Magnet swings in and out of the surgical suite, patient remains
stationary
• Coupled with image-guided surgery systems for improved outcomes
• Other considerations:
– Planning time and physician agreement
– Integration of iMRI with equipment inside and outside the department
– Construction and installation
– Training
– Service costs
41
iMRI: Fixed Vendors
• Configuration1:
– MRI integrated into surgical navigation system
– Dual-room approach, sliding RF door allows rooms
to be used individually
– Cost : $4,500,000 to $6,500,000
• Configuration 2
– 1.5T or 3.0T MRI
– Dual room approach, OR room and MRI suite
– Pricing magnetic field strength dependent:
1.5T- $7,500,750
3.0T -$9,960,500
42
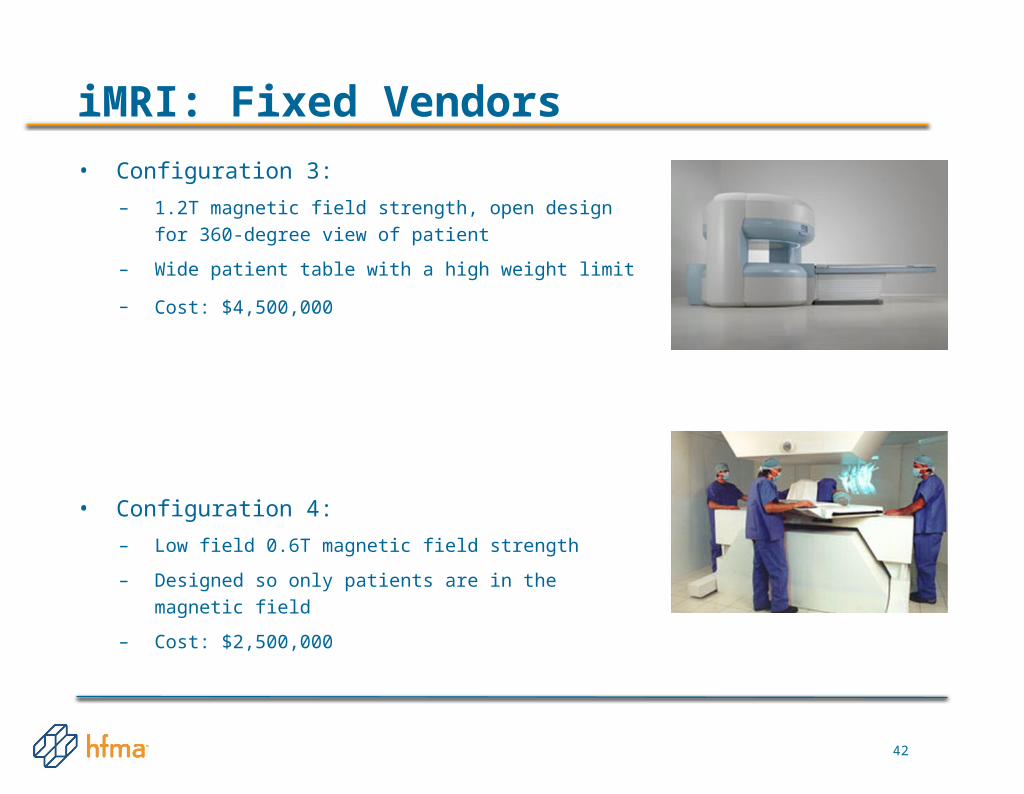
iMRI: Fixed Vendors
• Configuration 3:
– 1.2T magnetic field strength, open design for 360-degree
view of patient
– Wide patient table with a high weight limit
– Cost: $4,500,000
• Configuration 4:
– Low field 0.6T magnetic field strength
– Designed so only patients are in the magnetic field
– Cost: $2,500,000

43
iMRI: Mobile Vendors
• Configuration 1
– Ceiling mounted 1.5T or 3.0T magnet
– MRI compatible OR table
– Three possible room configurations available
– Pricing magnetic field strength dependent:
1.5T- $12,900,500
3.0T - $15,500,750
• Configuration 2
– 0.15 T magnet that can be retrofitted into existing ORs
– Two RF shielding options available:
Complete room shielding
Portable shield
– Cost: $1,700,600 (includes Portable RF Shielding)

44
iMRI: Clinical Outcomes
• Outcomes in neuro applications:
– Reduces the risk of damage to the brain
– Improves tumor resection and survival rates
– Confirms total tumor removal during surgery:
Decreases the need for repeat surgeries from 20.5% to 2.2%
Decreases patient length of stay and possibility of complications
Removes need for post-operative MRI
– Account for brain shift that occurs after removal of skull bone
Studies have found brain shift can vary
between 3 and 24 mm which changes
brain architecture significantly
University of Stuttgart
45
iMRI: Financial Considerations and Reimbursement
• Technology cost:
– iMRI with Image Guided Surgery (IGS): $2.5 million to $15 million
– IGS only: $500,000
– Service costs significantly increased with iMRI
• Other considerations
– Increased total anesthesia time, increased OR time and cost
– No difference in reimbursement for iMRI
• Financial investment of iMRI requires providers have
– High patient volumes
– Ability to expand iMRI use outside of neuro applications
– High population of private pay mix

46
iMRI: Takeaways
Pros• Improved outcomes
– More precise surgeries reduce the need for repeat procedures
– Better safety outcomes
• Use of non-ionizing radiation
– Useful in imaging soft tissues’ structure in organs like the brain, heart and eyes
Cons• High cost
• Limited applications
• No direct reimbursement
• Longer OR time
• Small space to work in
• Complexity involved in technology selection and planning

47
iCT: Introduction and Market
• Steady growth in intraoperative CT (iCT)
– Increased interest over the last six months
• Clinical applications for iCT:
– Cranial
– Spinal
– ENT
• Coupled with IGS to provide real-time, interactive CT for surgical cases
• Clinical studies support improved outcomes and safety
• High cost has limited adoption
– Head & Neck
– CMF
– Orthopedic
– Vascular Surgery

Of the two technologies, iMRI and iCT, which are you considering investing in?
• iMRI
• iCT
• Both
• Neither one
• Don’t know
Poll Question
48

49
iCT: Technology
• Configuration: Fixed and mobile CT scanners
– Mobile iCT is moved throughout facility for any intraoperative procedure
– Fixed or stationary iCT is in installed within the actual OR room
Used in conjunction with cardiac cath system and radiation oncology
• Coupled with image-guided surgery (IGS) to provide real-time, interactive
CT
• Construction and installation is simpler as compared to iMRI

50
iCT: Vendors
• Vendor 1:
– Received FDA clearance October 2014
– Mobile 64 mobile CT scanner
– Pricing will be set in Q1/Q2 of 2014
• Vendor 2:
– 20 to 64 slice count CT scanner on floor rails
– Designed for cardiac cath and radiation oncology applications
– Cost: . $1,000,000 - $1,200,000
• Vendor 3:
– Received FDA clearance September 2013
– Mobile 32 slice whole body CT scanner
– Offer multiple tabletops for neruo and spinal applications
– Cost: $1,000,000 - $1,225,500.

51
iCT: Vendors
• Vendor 4:
– Three portable CT products:
Option 1: 32-slice whole body, $900,000 - $1,100,000
Option 2: 8-slice, battery-operated for head and neck,
$400,000 - $750,000
Option 3: Used for imaging head and neck up to C5,
$350,000 - $450,000
• Vendor 6
– Fixed upright CT
– Applications include sinuses, skull and temporal bones at point of care
– Cost: $260,000 - $350,000
• Vendor 5
– Imaging system similar to mobile C-arm, targeted for
spinal fusion, cranial and orthopedic cases
– Cost: $1,000,000 - $1,500,000 (navigation system) or
$650,000 - $800,000 (without navigation system)

52
iCT: Clinical Outcomes
• Clinical outcomes:
– Improves intracranial and spinal tumors resection
– Accounts for brain shift that occurs after skull bone removal
– Improved efficacy for spinal surgery
Check position of the implants used
Determine extent of decompression
Check realignment during surgery
– Improved efficacy for vascular neurosurgery
Ability to image blood vessels
Provides rapid information related to critical impairment of brain perfusion
Eur Spine J. 2005 Sep;14(7):671-6. Epub 2005 Mar 1

53
iCT: Financial Considerations and Reimbursement
• Lack of direct ROI and limited financial incentive
– No difference in reimbursement through CMS for iCT
CMS may change reimbursement in the future as iCT adoption increases
– Technology cost is significant
Investment in iCT is considerably less costly than iMRI
• Substantial clinical improvements and diverse applications

54
iCT: Takeaways
Pros• Improved outcomes
– More precise surgeries reduces the need for repeat procedures
– Improved confidence for post-operative care
– Immediate recognition of intraoperative hemorrhage
• Diverse number of clinical applications
Cons• High cost
– iCT costs less than iMRI
• No direct reimbursement
• Challenging Cross-Team/Department Coordination
• Use of ionizing radiation

55
Conclusion
• Integrated OR, hybrid OR and iMRI/iCT have the potential to control costs
and improve the quality of care delivered
• Require substantial investment that must be set against clinical and
financial impacts
• Maximizing investments and realizing optimal results require:
– Coordinated team-based approach to planning, evaluation, selection and
execution
– Close management of key players
– Coordination to avoid both over- or under-buying
Q&A
56