burkitt nhl mainz 2010 - tumorzentrum-muenchen.de · p a1 b1 c1 a2 b2 c2 sc- apheresis (not...
TRANSCRIPT

Burkitt NHL Mainz 2010
1
Nicola Gökbuget
Goethe University Hospital, Department of Medicine II, Frankfurt GMALL Study Coordinator
German Consortium for Translational Cancer Research
Distribution of NHL Subtypes Harris et al, Ann Oncol, 1999
Dunleavy, Hematol Oncol Clin N Am 30 (2016)
Burkitt‘s Lymphoma Subtypes - I Dunleavy, Hematol Oncol Clin N Am 30 (2016)
Burkitt‘s Lymphoma Subtypes - II
• Intermediate-sized cells with round nuclei, multiple nucleoli, and a high proliferative index, as measured by Ki- 67 staining.
• The increased proliferation can cause spontaneous apoptosis leading to the characteristic starry sky pattern present in marrow and lymph nodes
Histology of Burkitt’s Lymphoma Casulo & Friedberg,Curr Hematol Malig Rep (2015)
Biological Characterisation of Mature B-ALL/Burkitt's Lymphoma
Morphology = FAB L3 morphology Immunophenotype sIg +
B-Cell associated antigens + (CD19, CD79a, CD22; 80% CD20+ TdT neg)
Pathology Burkitt‘s Leukemia/Lymphoma "starry sky" pattern CD19, CD20, CD22, and CD79a, and lack CD5 and CD23. Ki-67>95%,c-myc+
Cytogenetics/ mostly t(8;14) – cMYC / IgH Molecular genetics less frequently t(8;22); t(2;8)
in 5-25% EBV genomes in 25-40% associated with HIV-infection

Burkitt NHL Mainz 2010
2
Gene Expression Profiling in Burkitt‘s Lymphoma Hummel et al, New Engl J Med, 2006
WHO classification: Burkitt‘s Lymphoma includes - classical - atypic (Burkitt-like)
Gene expression analysis - Typical molecular signature of Burkitt‘s lymphoma identified - wide variability of histologic appearance (including
lymphoma with DLBCL appearance) - c-myc translocation not in all cases Conclusion 1. Patients with Burkitt‘s signature identified in DLBCL 2. Patients with c-myc identified in DLBCL
- Poorer outcome with CHOP-based protocols
WHO Classification for Lymphoid Neoplasias Swerdlow et al, Blood 2016
WHO Classification for Lymphoid Neoplasias Swerdlow et al, Blood 2016
Highlights of changes in 2016 WHO classification of lymphoid, histiocytic, and dendritic neoplasms
WHO Classification for Lymphoid Neoplasias Swerdlow et al, Blood 2016
Myc as single hit Myc and BCL2 and/or BCL6
Pathogenesis of B-ALL/Burkitt‘s Lymphoma
Hecht et al, JCO, 2000 Blum et al, Blood, 2004
• C-myc is a Helix-loop-heli leucine zipper transcription factor (BHLH-LZIP) • C-myc is juxtaposed to immunoglobuline gene loci
- 80%: t(8;14), IgH-c-myc - 20%: t(2;8),t(8;22) kappa or lambda light chain-c-myc
• C-myc proto-oncogene induces 27 different genes
• Mutations in TCF3 and/or its negative regulator ID3 are detected in 70% of sporadic and 40% of endemic BL
• In sporadic BL, ID3 mutations (58%) more common than TCF3 mutations (11%) or mutations of both genes (13%)
• TCF3: Role in normal B-cell development by regulating the transcription of immunoglobulin and other B-cell-restricted genes
Recurrently mutated genes in aggressive lymphomas determined by RNA-seq Schmitz et al, Nature 2012

Burkitt NHL Mainz 2010
3
Recurrently mutated genes in aggressive lymphomas determined by RNA-seq Schmitz et al, Nature 2012
CDK-4/6 inhibitor
TCF-3 promotes antigen-independent (tonic) B-cell-receptor signaling Tonic B-cell-receptor signaling sustains BL survival by engaging the PI3 kinase pw
TCF-3 promotes cell-cycle progression by trans-activating CCND3, encoding a D-type cyclin that regulates the G1–S phase transition.
CCND3 mutations stabilize cyclin D3 protein expression and drive proliferation.
BET-Inhibitor
Clinical Characteristics of Burkitt‘s Leukemia/Lymphoma
Mature B-ALL Burkitt‘s NHL (N=148) (N=130)
Male predominance 67% 69%
Older age > 50 34% 24%
WBC > 50,000/µL 13% -
Elevated LDH 100% 56%
Lymphadenopathy 54% 83%
CNS involvement 20% 5%
Extranodal involvement 40% 76%
Population-based data
Castillo, Cancer 2013;119:3672-9
Median age: 49 yrs
US SEER Registry Data On Burkitt‘s
Castillo, Cancer 2013;119:3672-9 US SEER Registry Data On Burkitt‘s
Castillo, Cancer 2013;119:3672-9 US SEER Registry Data On Burkitt‘s

Burkitt NHL Mainz 2010
4
Castillo, Cancer 2013;119:3672-9 US SEER Registry Data On Burkitt‘s
Prognostic score: 1 point age 40 to 59 yrs
or black race
2 points age 60 to 79 yrs or stage III/IV disease
4 points age 80 yrs 4 risk groups: 0 or 1 points, low risk 2 points, low-intermediate risk 3 points, high-intermediate risk 4 points, high risk
Castillo, Cancer 2013;119:3672-9 US SEER Registry Data On Burkitt‘s
Principles of Therapy
Treatment Design in B-ALL and Burkitt‘s Lymphoma
Important Agents Results in Burkitt‘s NHL (Ziegler 1977) and pediatric studies (Patte 2001, Reiter 1999) • HD alkylating agents • HDMTX • HDAraC
General • Cell doubling time: 25 hrs (Iversen 1974) • A prolonged time-period should be covered with
cytostatic drug concentrations: each cell should enter cell cycle once (Murphy 1985)
è 4-5 d cycles è Fractionated drugs or continuous infusion è Short intervals
Rationale for short intensive „non-NHL“ protocols“ incl.
fractionated HD Cyclo/Ifo HDMTX and HDAraC
- Results in Burkitt NHL
(Ziegler et al, 1977) - Results of pediatric procotols
(Patte et al 2001;Reiter et al, 1999) - Results in adult mature B-ALL
Burkitt and High-Grade NHL Dozzo, Adolescent Health, Medicine and Therapeutics, 2017 Features of Current Protocols for Burkitt‘s NHL

Burkitt NHL Mainz 2010
5
Therapieergebnisse bei Burkitt-Lymphom mit kurzen, intensiven Therapien und Rituximab
Reiter et al, Blood 94 (10):3294, 1999
Diagnoses Total 413
Burkitt 266 B-ALL 56 DLBCL Centroblastic 42 Immunoblastic 6 Mediastinal 8 NHL, not class. B-cell 30
Event Free Survival
GMALL Study B-ALL/NHL 2002
Rationale for B-ALL/NHL Study 2002
Chemotherapy • Reduction of MTX dose from 3 g/m² to 1.5 g/m² since no improvement but more toxicity in B-NHL90
• Inclusion of HDAC (cycle C x 2) - to improve antileukemic activity and CNS prophylaxis
Immunotherapy • anti-CD20 (Rituximab) in combination with chemo cycles - expression of CD20 > 80% in mature B-ALL
Stem cell transplantation • SC apheresis in pts without donor • SCT in CR1 for high risk patients ?
A1 B1 P C1 A2 B2 C2
SC- Apheresis
(not obligatory)
antiCD20 antiCD20 antiCD20 antiCD20 antiCD20 antiCD20
Multicentre Study to Optimize Therapy of B-ALL and High-grade Non-Hodgkin’s Lymphoma in Adults
(GMALL B-ALL/NHL 2002)
Patients 15-55 years
Failure of therapy
Salvage SCT (allo, auto, MUD)
antiCD20 antiCD20
End of therapy for
Stage I/II with CR after 2 cycles
MedTU CNS-inv. CRu, PR
Irradiation
1 2 5 8 12 15 18 Weeks
21 24 28
End of therapy after 4 cycles if: stage I/II CR after 2 cycles no extranodal involvement,no Med TU
A1 B1 P C1 A2 B2 C2
SC- Apheresis
(not obligatory)
antiCD20 antiCD20 antiCD20 antiCD20 antiCD20 antiCD20 1
Multicenter Study to Optimize Therapy of B-ALL and High-grade Non-Hodgkin’s Lymphoma in Adults (GMALL-B-ALL/NHL 2002)
Rituximab in combination with Chemotherapy
Patients 15-55 years Failure of therapy
Salvage SCT (allo, auto, MUD)
antiCD20 antiCD20
End of therapy in Stage I/II with CR after 2 cycles
MedTU CNS-inv. CRu, PR
Irradiation
1 2 5 8 12 15 18 Weeks
21 24 28
A1 * B1 * P A2 * B2 * A3 * B3 *
antiCD20 antiCD20 antiCD20 antiCD20 antiCD20 antiCD20 1 antiCD20 antiCD20
Patients > 55 yrs
Failure of therapy
Salvage SCT (allo, auto, MUD)
Rituximab 375 mg/m2 8x

Burkitt NHL Mainz 2010
6
GMALL B-ALL/NHL 2002: Patient Flow
Hoelzer et al, Blood 2014
GMALL B-ALL/NHL 2002: Patient Flow
Hoelzer et al, Blood 2014
GMALL B-ALL/NHL 2002: Patient Characteristics - I
Hoelzer et al, Blood 2014
OS GMALL B-ALL/NHL 2002: Patient Characteristics - II
Hoelzer et al, Blood 2014
OS
GMALL B-ALL/NHL 2002: Overall Response and Outcome
Hoelzer et al, Blood 2014
Overall Survival Burki- Leukemia / Lymphoma GMALL B-‐ALL/NHL 2002
0.80 ± 0.02 (N=363)
Hoelzer et al, Blood 2014

Burkitt NHL Mainz 2010
7
Progression Free Survival Burki- Leukemia / Lymphoma GMALL B-‐ALL/NHL 2002
0.75 ± 0.03 (N=363)
Hoelzer et al, Blood 2014
Overall Survival Burki- Leukemia / Lymphoma GMALL B-‐ALL/NHL 2002
No CHOP Pretreatment: 0.80 ± 0.02 (N=349) CHOP Pretreatment: 0.77 ± 0.12 (N=14) P=0.99
Hoelzer et al, Blood 2014
Overall Survival Burki- Leukemia / Lymphoma GMALL B-‐ALL/NHL 2002
Male: 0.84 ± 0.02 (N=253) Female: 0.70 ± 0.05 (N=110) P=0.004
Hoelzer et al, Blood 2014
Subgruppen- Analysen und Prognosefaktoren
ALTER
Overall Survival Burki- Leukemia / Lymphoma GMALL B-‐ALL/NHL 2002
≤55 yrs: 0.86 ± 0.02 (N=265) >55 yrs: 0.62 ± 0.05 (N=98) P<0.0001
Hoelzer et al, Blood 2014
Faktoren Alter (<> 55) LDH <>250 Stadium 1-‐2 vs 3-‐4 KM-‐Befall ZNS-‐Befall aaIPI (0-‐1 vs 2-‐3) Extranodalbefall Geschlecht
MulYvariat-‐Analyse: Overall Survival
Signifikant 0.0014 HR: 2.5 0.02 HR: 4.4 0.01 HR: 2.4 0.006 HR: 2.2
Burkitt NHL Mainz 2010
8
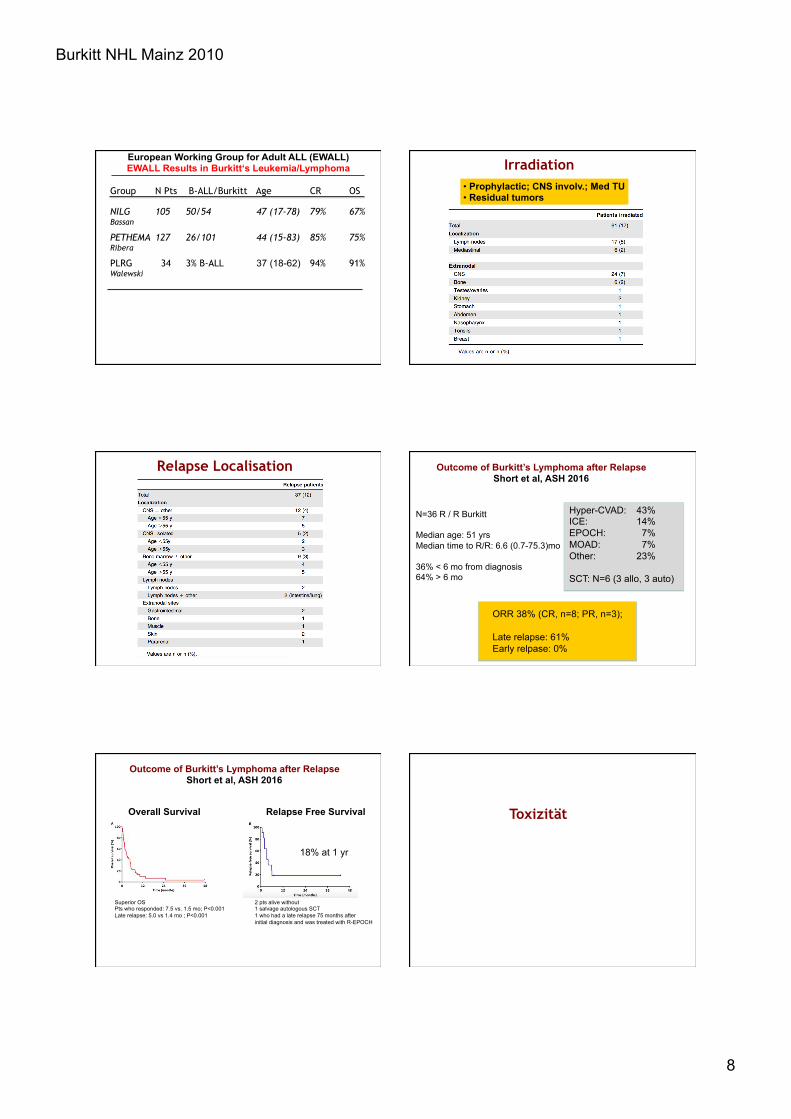
European Working Group for Adult ALL (EWALL) EWALL Results in Burkitt‘s Leukemia/Lymphoma
Group N Pts B-ALL/Burkitt Age CR OS
NILG 105 50/54 47 (17-78) 79% 67% Bassan
PETHEMA 127 26/101 44 (15-83) 85% 75% Ribera
PLRG 34 3% B-ALL 37 (18-62) 94% 91% Walewski
Irradiation • Prophylactic; CNS involv.; Med TU • Residual tumors
Relapse Localisation Outcome of Burkitt’s Lymphoma after Relapse Short et al, ASH 2016
Hyper-CVAD: 43% ICE: 14% EPOCH: 7% MOAD: 7% Other: 23% SCT: N=6 (3 allo, 3 auto)
N=36 R / R Burkitt Median age: 51 yrs Median time to R/R: 6.6 (0.7-75.3)mo 36% < 6 mo from diagnosis 64% > 6 mo
ORR 38% (CR, n=8; PR, n=3); Late relapse: 61% Early relpase: 0%
Overall Survival
2 pts alive without 1 salvage autologous SCT 1 who had a late relapse 75 months after initial diagnosis and was treated with R-EPOCH
Outcome of Burkitt’s Lymphoma after Relapse Short et al, ASH 2016
Relapse Free Survival
18% at 1 yr
Superior OS Pts who responded: 7.5 vs. 1.5 mo; P<0.001 Late relapse: 5.0 vs 1.4 mo ; P<0.001
Toxizität

Burkitt NHL Mainz 2010
9
Toxizität B-ALL/Burkitt < 55 yrs
Hoelzer et al, Blood 2014
Toxizität B-ALL/Burkitt > 55 yrs
79 73 72 73 58 52 407
29% 52% 76%
43% 42% 33%
49% 31%
A2
37%
72%
62%
43% 18%
27%
49%
28%
1% 12% 21%
1% 14% 38%
3% 21% 22%
1% 3%
8% 18% 2% 1%
16% 30% 13% 21% 9% 17%
Toxizität B-ALL/Burkitt < 55 yrs
1% 1%
2% 1% 1 2 1 1% 1
• Allopurinol; Uratoxidase bei Patienten mit hohem Risiko eines Tumorlysesyndroms
• Leukovorin adaptiert an MTX-Spiegel • Vermeidung von Begleitmedikation, die zu einer bezögerten MTX-
Ausscheidung beitragen können oder potentiell nephrotoxisch sind • Wässerung vor, während und nach HDMTX Hydration
(Bilanzierung) • Forcierte Diurese nach MTX • Urinalkalisierung (Urin-pH >7,5 vor während und nach MTX) • Tägliche Kontrollen der Nieren- und Leberfunktion • Mukositisprophylaxe • Antiinfektiöse Prophylaxe • G-CSF nach den Zyklen
Maßnahmen der Supportivtherapie bei Burkitt-Lymphom/Leukämie
Critical Issues in the Management of Burkitt’s NHL Dozzo et al, Adolescent Health, Medicine and Therapeutics, 2017 Need to reduce Incidence of Severe Mucositis
Rationale
- Poor quality of life if oIII-IV mucositis
- Need of i.v. morphins
- Entry of pathogens – increase risk of infections ?
- Treatment delays and reduced time-dose-intensity

Burkitt NHL Mainz 2010
10
Need to reduce Incidence of Severe Mucositis
Options
- Improved supportive care
Risk factors for delayed MTX-elimination
- 3rd space e.g pleural effusion - urine pH<7 - i.v. fluid <3L/m2/24h - overweight - comedication (MTX-interference, nephrotoxic, Vitamin C,
iv. contrast X-ray or CT) - advanced age - baseline hepatic dysfunction - baseline renal insufficiency - intrathecal MTX § Cave: Orally neutral beverages (no coke,yoghurt,butter milk) § In case of delayed clearance and/or renal insufficiency:
Carboxypeptidase
Schwartz S, et al., ASH 2006, abstract 2439 Relling MV et al., J Clin Oncol 1994, 12: 1667
NSAR‘s, ß-Lactame, PPI‘s, TMP/SMX, nephrotox. Subst
Need to reduce Incidence of Severe Mucositis
Options
- Reduced dose of MTX Favourable survival in elderly Burkitt‘s NHL (0.5 g MTX) but CNS relapses in eldery B-ALL
- Reduced infusion time of MTX (4 h vs 24 hrs) HDMTX 4 hr infusion less toxic Equally effective in low risk but less effective in high risk
- Reduction of anthracyclines
- Reduced number of cycles Equally effective in low risk but less effective in high risk Cairo et al, Blood 2007, Patte et al, Blood 2007
- Prophylaxis: G-CSF, Caphosol, Palifermin (KGF)
HIV-positive Burkitt NHL
B-ALL/NHL Protocol in AIDS-associated Burkitt- or Burkitt-like Lymphoma
Hoffmann et al, Leukemia & Lymphoma, 2006
Retrospective multicenter trial in 6 German HIV centers CHOP vs GMALL B-ALL 86/90 (MTX: 0.5 – 3.0 g/m²) CHOP B-NHL90
N 31 20
CD4 >200 43% 78% B-ALL 0 25%
CR 40% 75% Survival 2 y 34% 55% Death on tx 10% 10%
HAART 32% 65% Intensive B-ALL regimen is feasible in HIV infected patients
even in combination with HAART
B-ALL/NHL Protocol in AIDS-associated Burkitt- Lymphoma Oriol et al, Haematologica 2003 Prospective multicenter trial
GMALL B-ALL 90 (MTX: 3.0 g/m²) in HIV+ vs HIV- pts HIV+ HIV-
N 14 39 Age 45 (23-65) 35 (15-74) B-ALL 43% 64% Stage III/IV 57% 23% On HAART 36%
CR 71% 77% Survival 2 y 55% 43%
No difference in outcome between HIV+ vs HIV- pts HAART feasible and probably beneficial

Burkitt NHL Mainz 2010
11
Therapy in HIV+ Adult Burkitt‘s NHL Summary
§ Improved results with short intensive regimens particularly in advanced stage Burkitt NHL
§ Achievement of CR first goal since long-term survival achievable in CR pts only
§ HAART compatible and probably favourable
§ Prognostic factors (?): - Age - Poor performance - CD4 count < 200, < 100/µl - Later stage - i.v. drug abuse
New approaches: § Rituximab+chemotherapy feasible in 2 studies
Alternative Strategies ?
N Engl J Med 2013;369:1915-25.
From the Center for Cancer Research, National Cancer Institute, Bethesda
N Engl J Med 2013;369:1915-25.
2013 – N Engl J Med - Series
Study Overview
• Toxic high-dose chemotherapy may not be necessary to cure Burkitt's lymphoma in adults and patients with immunodeficiency.
• An infusion-based chemotherapy program with modest toxicity administered mainly in outpatients resulted in an overall survival rate of 90 to 100%.
Dunleavy, Hematol Oncol Clin N Am 30 (2016)
DA-EPOCH-R for HIV-neg
Intrathecal methotrexate 12 mg on day 1 and 5 of cycles 3-6.
SC-EPOCH- RR for HIV-pos
Pts should receive 6 cycles of treatment. If the tumor masses shrink > 20% between the end of cycle 4 and 6, administer two additional cycles.
Pts have at least 3 cycles with 1 cycle beyond CR as determined by combined CT and FDG-PET criteria
EPOCH-R for Burkitt’s Lymphoma

Burkitt NHL Mainz 2010
12
Dunleavy, Hematol Oncol Clin N Am 30 (2016) EPOCH-R for Burkitt’s Lymphoma
DA-EPOCH-R: 6 cycles in all but one; one patient 9 cycles. 74% received at least dose level 3 37% received dose level 4 SC-EPOCH-RR: 45% received 3 cycles 55% 4 cycles, and doses were not escalated.
Characteristics of the Patients.
Dunleavy K et al. N Engl J Med 2013;369:1915-1925
LR: Resected stage I or abd. stage II IMR: Neither LR nor HR HR: BM >25 a/o. CNS
Kaplan–Meier Estimates of Freedom from Disease Progression and Overall Survival.
Dunleavy K et al. N Engl J Med 2013;369:1915-1925
Adverse Events.
Dunleavy K et al. N Engl J Med 2013;369:1915-1925
Risk-Adapted Therapy in Adults with Burkitt Lymphoma: Preliminary Report of a Multicenter
Prospective Phase II Study of DA-EPOCH-R Dunleavy et al, ASH 2015
Inclusion criteria: Newly diagnosed BL Age 18 years or older HIV negative or positive Low-risk (LR): normal LDH, ECOG 0-1, stage I or II, max tumor size < 7cm è 3 cycles of DA-EPOCH-R (no i.th. prophylaxis) High-risk (HR): All other è 6 cycles (i.th. prophylaxis d 1 and 5 on cycles 3-6)
Risk-Adapted Therapy in Adults with Burkitt Lymphoma: Preliminary Report of a Multicenter
Prospective Phase II Study of DA-EPOCH-R Dunleavy et al, ASH 2015
Enrolled: 77 pts Age: 45 (19-78) yrs Male: 82% Stage III or IV: 64% Elevated LDH: 53% CNS: 10% HIV+: 26% LR: 14% HR: 86%

Burkitt NHL Mainz 2010
13
Risk-Adapted Therapy in Adults with Burkitt Lymphoma: Preliminary Report of a Multicenter
Prospective Phase II Study of DA-EPOCH-R Dunleavy et al, ASH 2015
2 deaths on treatment in the HR arm secondary to infection.
Median follow-up: 25 mo No significant difference: HR vs LR HIV pos vs neg Age ≥ 40y vs < 40y
NR
73%
>40: 40%
Median: 33y Median: 42y
100% c-myc
NR
NR
NR
>ULN: 53% > ULN: 74%
Dunleavy et al
63%
3%
13% 10% LMB HR
50% Bowel
67% III-IV
NR
NR
Dunleavy et al
GMALL B-ALL/B-NHL 2002 Conclusions
• Combination of Rituximab and intensive chemotherapy feasible • Response rate 80-90% in Burkitt
Overall survival ~ 90%
• Improvement in mature B-ALL, less for pts > 55 y à inclusion of HDAC
• Irradiation effective part of therapy • SCT: No prognostic factors à no indication for SCT in CR1 à Stem cell apheresis stopped
• Major toxicity: mucositis à No improvement by caphosol / KGF
Mature B-ALL/Burkitt‘s NHL
Future Prospects Improved molecular characterisation Reduction of toxicity • De-escalation in good responders and early stages ? • Improved prophylaxis of mucositis and infections ? Improved outcome in elderly B-ALL • Intensified CNS prophylaxis • HDAC based cycle • Increased Rituximab dose-intensity? Refined response evaluation and risk stratification e.g. • PET analysis • MRD analysis (Mussolin et al, JCO 2007)
Reduction of irradiation Application in • HIV+ pts with Burkitt‘s leukemia/lymphoma Improved salvage therapy – new drugs ?