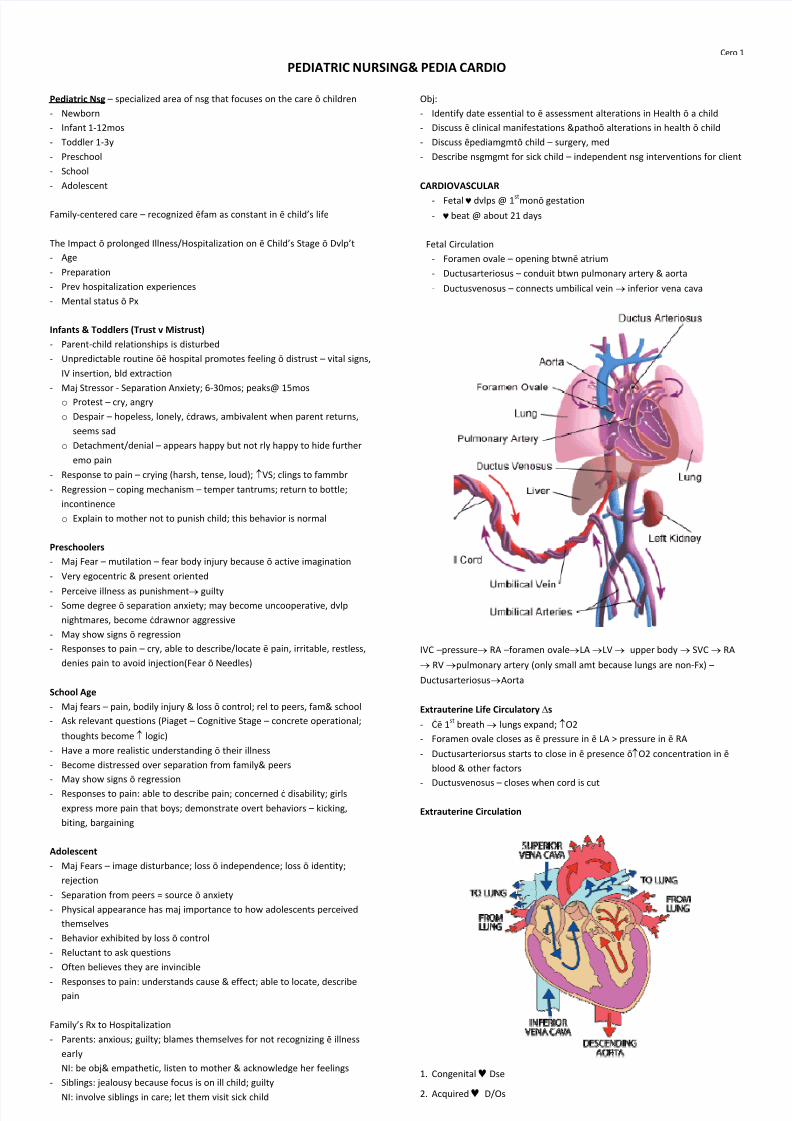
Cero 1 PEDIATRIC NURSING& PEDIA CARDIO Pediatric Nsg specialized area of nsg that focuses on the care children -Newborn -Infant 1-12mos -Toddler 1-3y -Preschool -School -Adolescent Family-centered care recognized fam as constant in childs life The Impact prolonged Illness/Hospitalization on Childs Stage Dvlpt -Age -Preparation -Prev hospitalization experiences -Mental status Px Infants & Toddlers (Trust v Mistrust) -Parent-child relationships is disturbed -Unpredictable routine hospital promotes feeling distrust vital signs, IV insertion, bld extraction -Maj Stressor - Separation Anxiety; 6-30mos; peaks@ 15mos oProtest cry, angry oDespair hopeless, lonely, draws, ambivalent when parent returns, seems sad oDetachment/denial appears happy but not rly happy to hide further emo pain -Response to pain crying (harsh, tense, loud); oVS; clings to fammbr -Regression coping mechanism temper tantrums; return to bottle; incontinence oExplain to mother not to punish child; this behavior is normal Preschoolers -Maj Fear mutilation fear body injury because active imagination -Very egocentric & present oriented -Perceive illness as punishment p guilty -Some degree separation anxiety; may become uncooperative, dvlp nightmares, become drawnor aggressive -May show signs regression -Responses to pain cry, able to describe/locate pain, irritable, restless, denies pain to avoid injection(Fear Needles) School Age -Maj fears pain, bodily injury & loss control; rel to peers, fam& school -Ask relevant questions (Piaget Cognitive Stage concrete operational; thoughts become o logic) -Have a more realistic understanding their illness -Become distressed over separation from family& peers -May show signs regression -Responses to pain: able to describe pain; concerned disability; girls express more pain that boys; demonstrate overt behaviors kicking, biting, bargaining Adolescent -Maj Fears image disturbance; loss independence; loss identity; rejection -Separation from peers = source anxiety -Physical appearance has maj importance to how adolescents perceived themselves -Behavior exhibited by loss control -Reluctant to ask questions -Often believes they are invincible -Responses to pain: understands cause & effect; able to locate, describe pain Familys Rx to Hospitalization -Parents: anxious; guilty; blames themselves for not recognizing illness early NI: be obj& empathetic, listen to mother & acknowledge her feelings -Siblings: jealousy because focus is on ill child; guilty NI: involve siblings in care; let them visit sick child Obj: -Identify date essential to assessment alterations in Health a child -Discuss clinical manifestations &pathoalterations in health child -Discuss pediamgmtchild surgery, med -Describe nsgmgmt for sick child independent nsg interventions for client CARDIOVASCULAR -Fetal kdvlps @ 1 st mongestation -kbeat @ about 21 days Fetal Circulation -Foramen ovale opening btwnatrium -Ductusarteriosus conduit btwn pulmonary artery & aorta -Ductusvenosus connects umbilical vein p inferior vena cava IVC pressurep RA foramen ovalepLA pLV p upper body p SVC p RA p RV ppulmonary artery (only small amt because lungs are non-Fx) DuctusarteriosuspAorta Extrauterine Life Circulatory (s -1 st breath p lungs expand; oO2 -Foramen ovale closes as pressure in LA > pressure in RA -Ductusarteriorsus starts to close in presence oO2 concentration in blood & other factors -Ductusvenosus closes when cord is cut Extrauterine Circulation 1.Congenital kDse 2. Acquired k D/Os