cardio vascular dysfunction - nursing lijan
TRANSCRIPT
Cardio Vascular Dysfunction
KEEP YOUR HEART HEALTHY
Objectives
At the end of this discussion, YOU will be able to:
• Review circulatory changes at birth
• Identify the classifications of Congenital Heart Diseases (CHD)
• Discuss the description and pathophysiology of each CHD
• Explain the therapeutic management and prognosis of each CHD
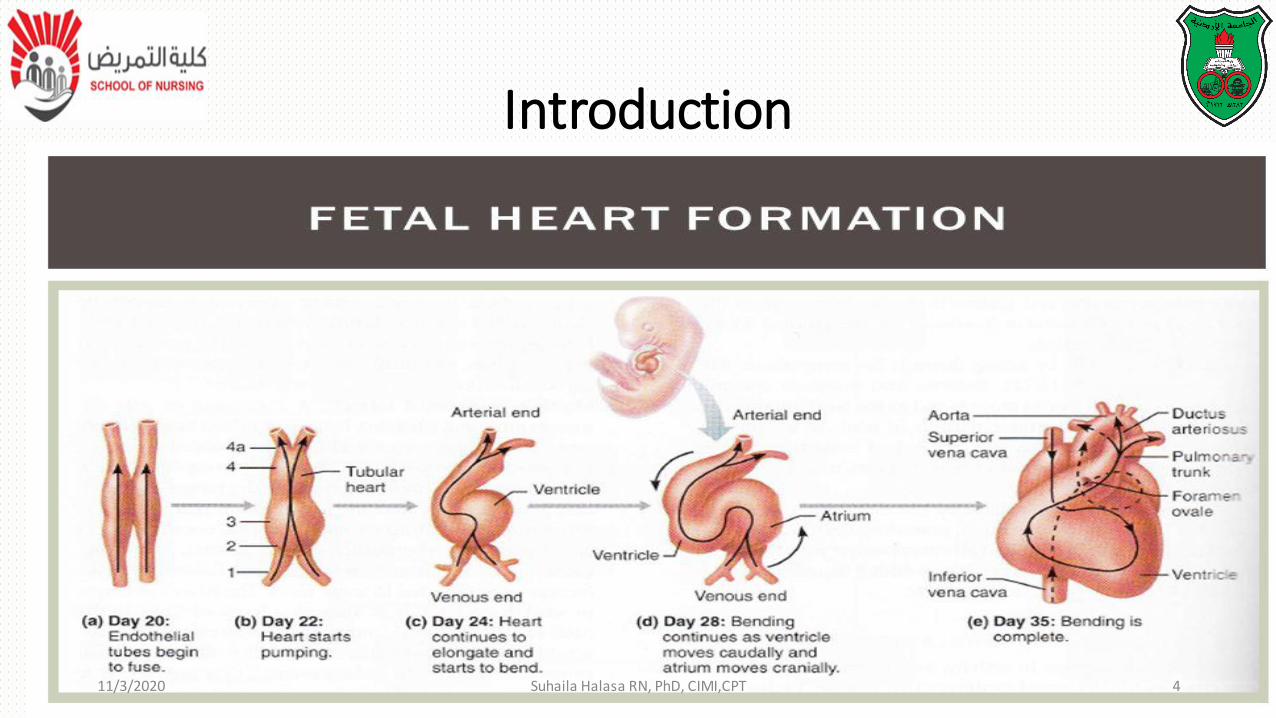
Introduction
11/3/2020 Suhaila Halasa RN, PhD, CIMI,CPT 4
Introduction
11/3/2020 Suhaila Halasa RN, PhD, CIMI,CPT 5
Introduction
11/3/2020 Suhaila Halasa RN, PhD, CIMI,CPT 6

https://www.youtube.com/watch?v=rYVGjbzmAtg
11/3/2020 Suhaila Halasa RN, PhD, CIMI,CPT 7
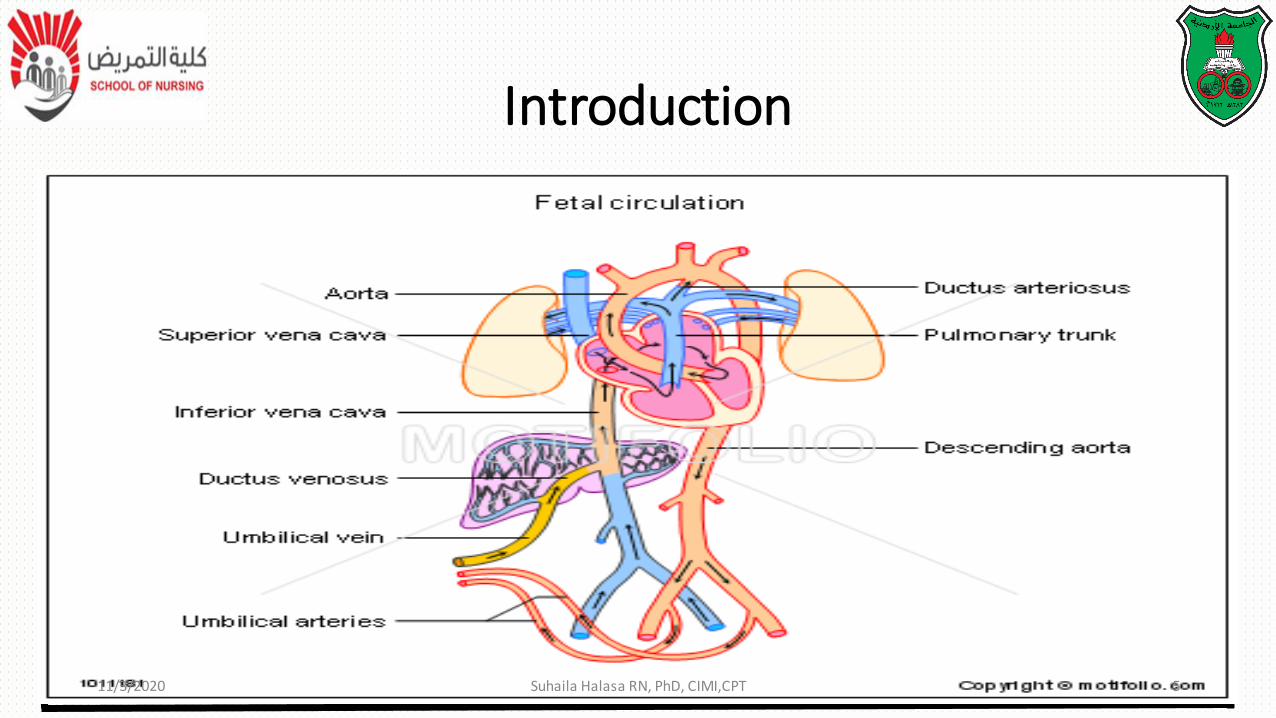
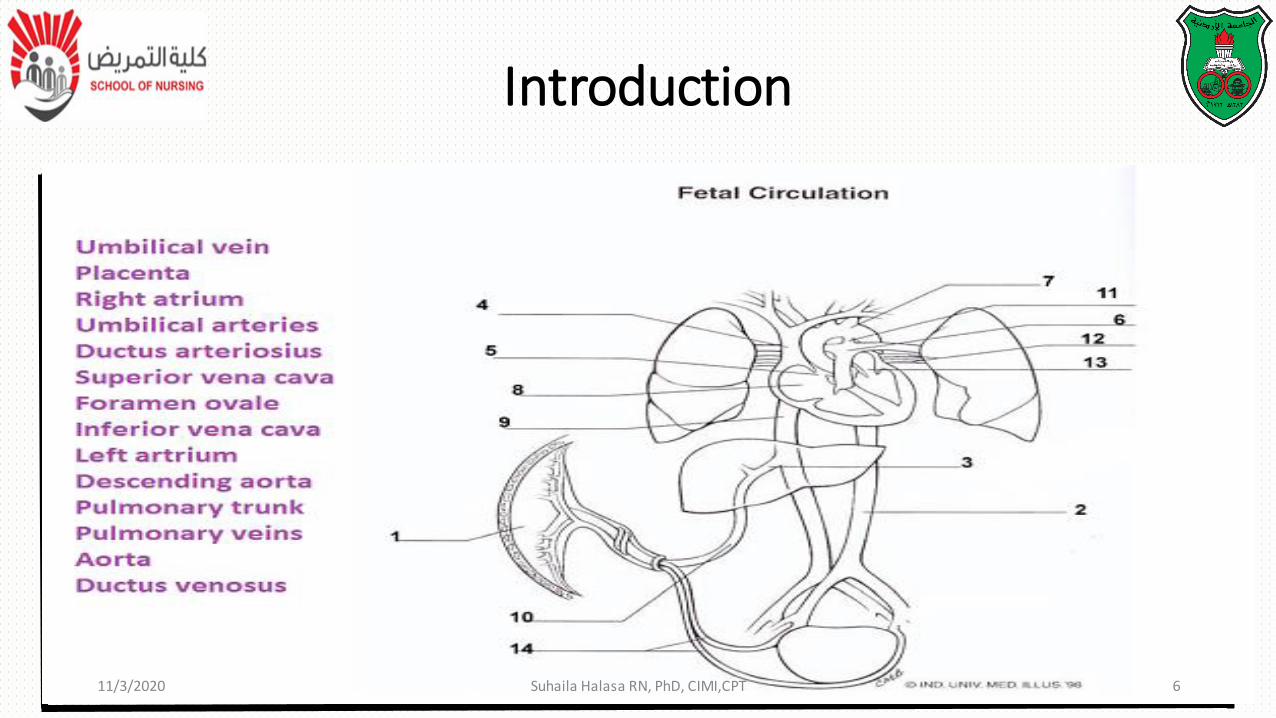
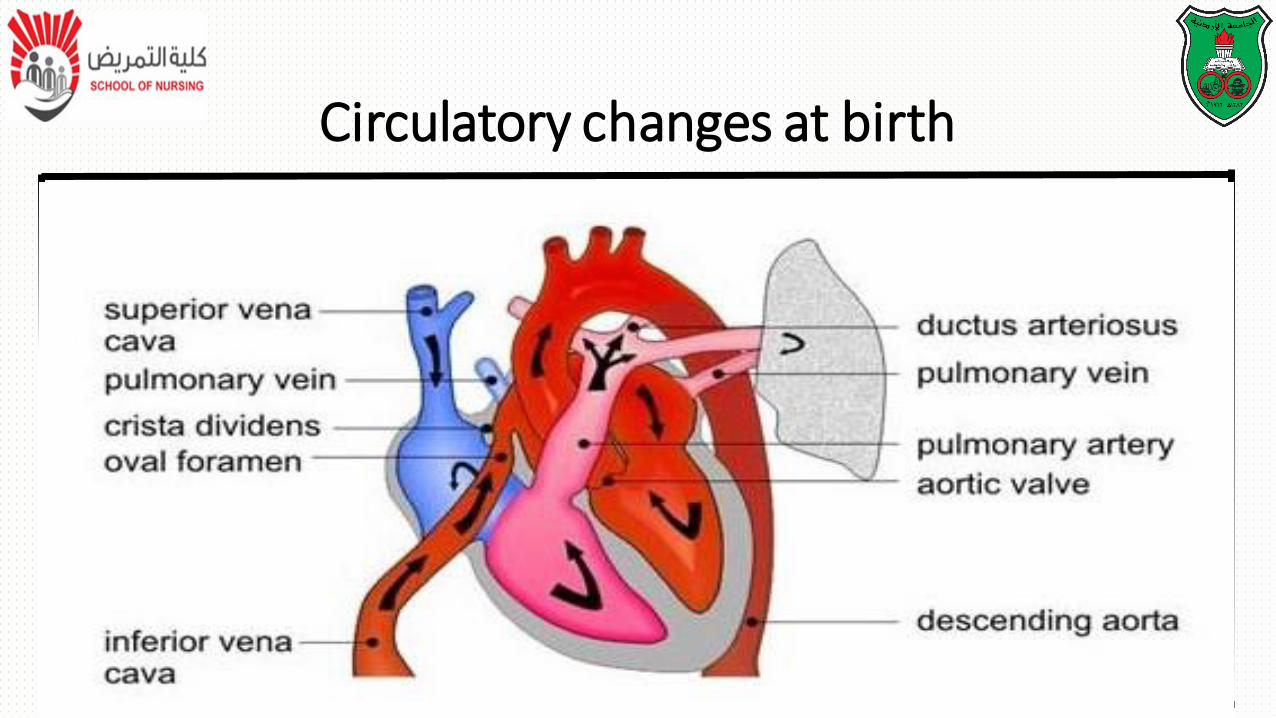
• During fetal life, blood carrying oxygen and nutritive material
from the placenta enters fetal system through the umbilical veins
• Oxygenated blood enters the heart by way of the inferior vena
cava
Circulatory changes at birth
• Because of the higher pressure of blood entering the right
atrium, it is directed posteriorly in a straight pathway across
the right atrium and through the foramen ovale to the left
atrium
Circulatory changes at birth
• In this way the better –oxygenated blood enters the left atrium and
ventricle to be pumped through the aorta to head and upper extremities
• Blood from the head and upper extremities entering the right atrium
from superior vena cava is directed down ward through the tricuspid
valve into the right ventricle
Circulatory changes at birth
• From here, it is pumped through the
pulmonary artery, where the major portion is
shunted to the descending aorta via the
ductus arteriosus
• Only small amount of blood flows to and
from non functioning fetal lung
Circulatory changes at birth
• Before birth, the pulmonary vascular resistance created by the collapsed
fetal lung causes greater pressure in the right side of the heart and
pulmonary artery
• At the same time, the free flowing placental circulation and the ductus
arteriosus produce a low vascular resistance in the reminder of the fetal
vascular system
Circulatory changes at birth
• With the cessation of placental blood flow from clamping of the umbilical cord and the expansion of lung at birth, the hemodynamics of fetal vascular system undergo pronounced and abrupt changes
• With the first breath, the lungs are expanded, the increased oxygen causes pulmonary vasodilation
• Pulmonary start to fall as systemic pressure, given the removal of the placenta start to rise
Circulatory changes at birth
• Normally, the foramen oval closes as the pressure in the left atrium
exceeds the pressure in the right atrium
• Ductus arteriosus starts to close in the presence of increased oxygen
concentration in the blood and other factors
Circulatory changes at birth
Circulatory changes at birth
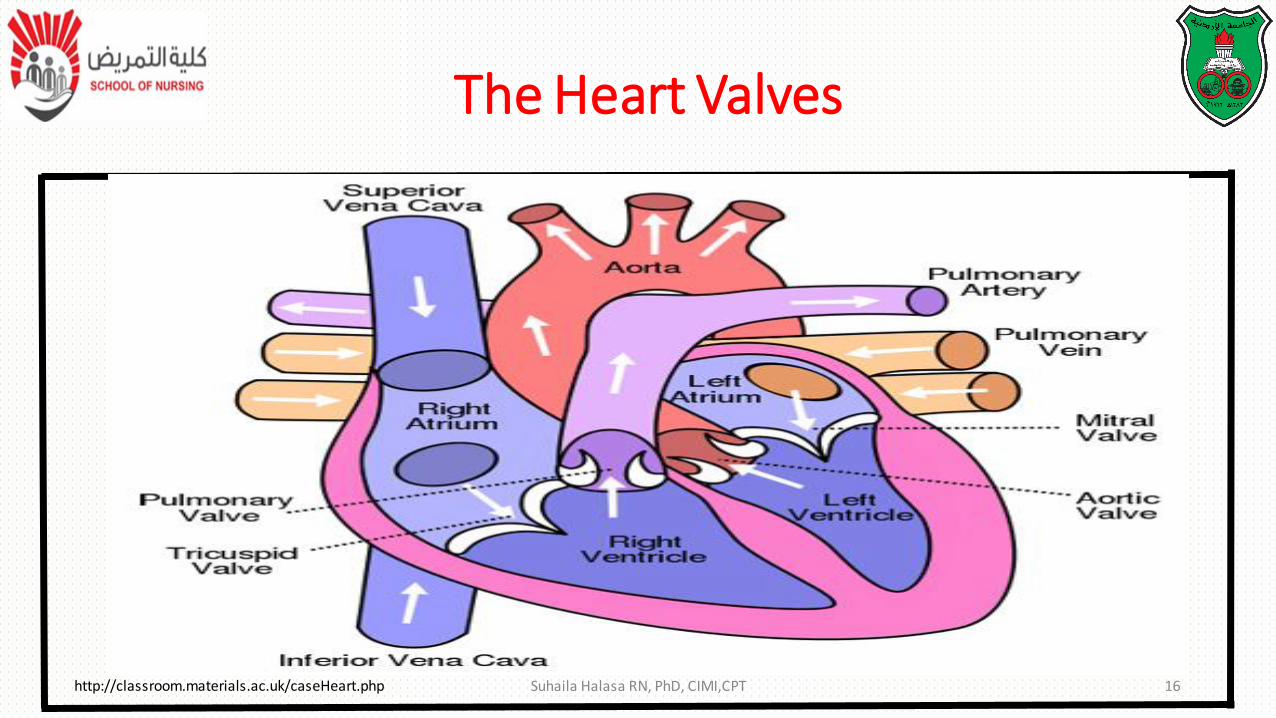
The Heart Valves
Suhaila Halasa RN, PhD, CIMI,CPT 16http://classroom.materials.ac.uk/caseHeart.php
• Normally the pressure on the right side of the heart is lower
than that on the left side, and the resistance in the pulmonary
circulation is less than that in the systemic circulation
Altered Hemodynamic
• Vessels entering in the champers have corresponding pressures
• Therefore, if an abnormal connection exist between the heart chambers
such as septal defect, blood will necessarily from an area of higher
pressure (left side) to one of lower pressure (right side)
Altered Hemodynamic
• Such a flow of blood is termed a left-to-right shunt
• Anomalies resulting in cyanosis may result from a change in pressure so
that the blood is shunted from the right to left side of the heart ( right-to
–left shunt) because of either increased pulmonary vascular resistance or
obstruction to blood flow through the pulmonic valve and artery
Altered Hemodynamic
• Cyanosis may also result from a defect that allows mixing of
oxygenated and deoxygenated blood within the heart
chambers or great arteries
Altered Hemodynamic

Please Wait ------
Please Wait ------YOU BROKE MY HEART-----
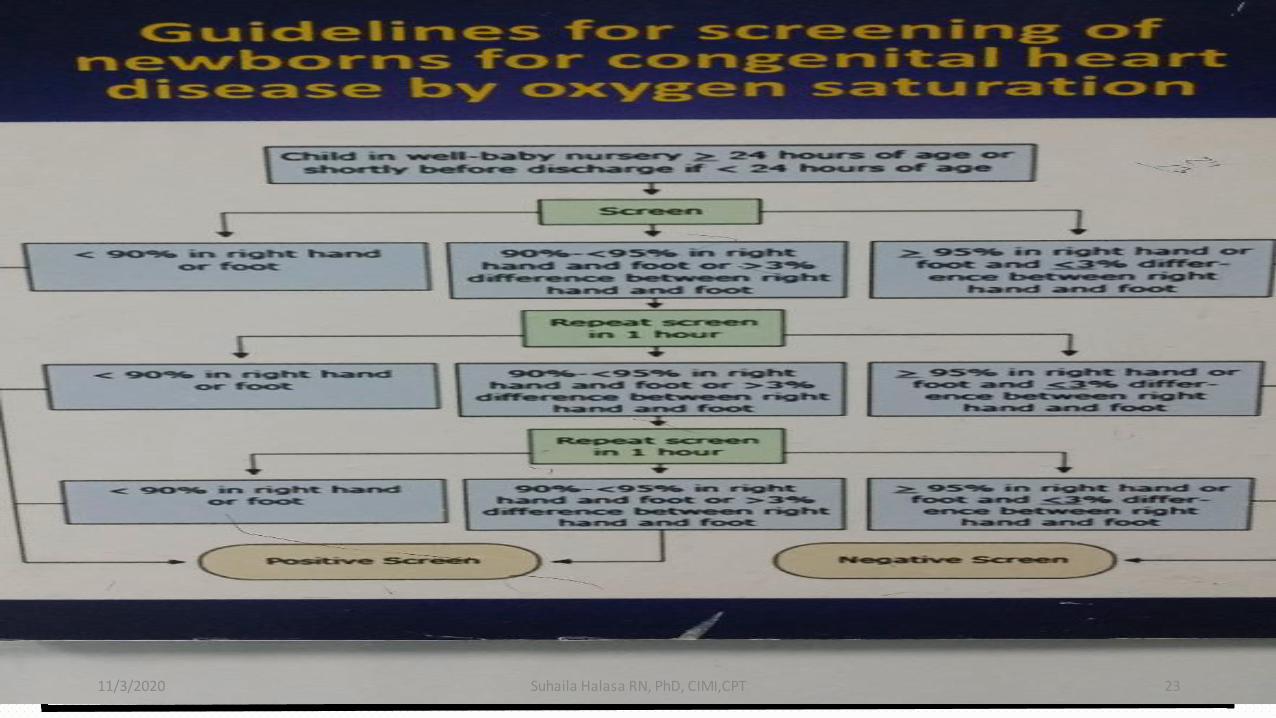
11/3/2020 Suhaila Halasa RN, PhD, CIMI,CPT 23
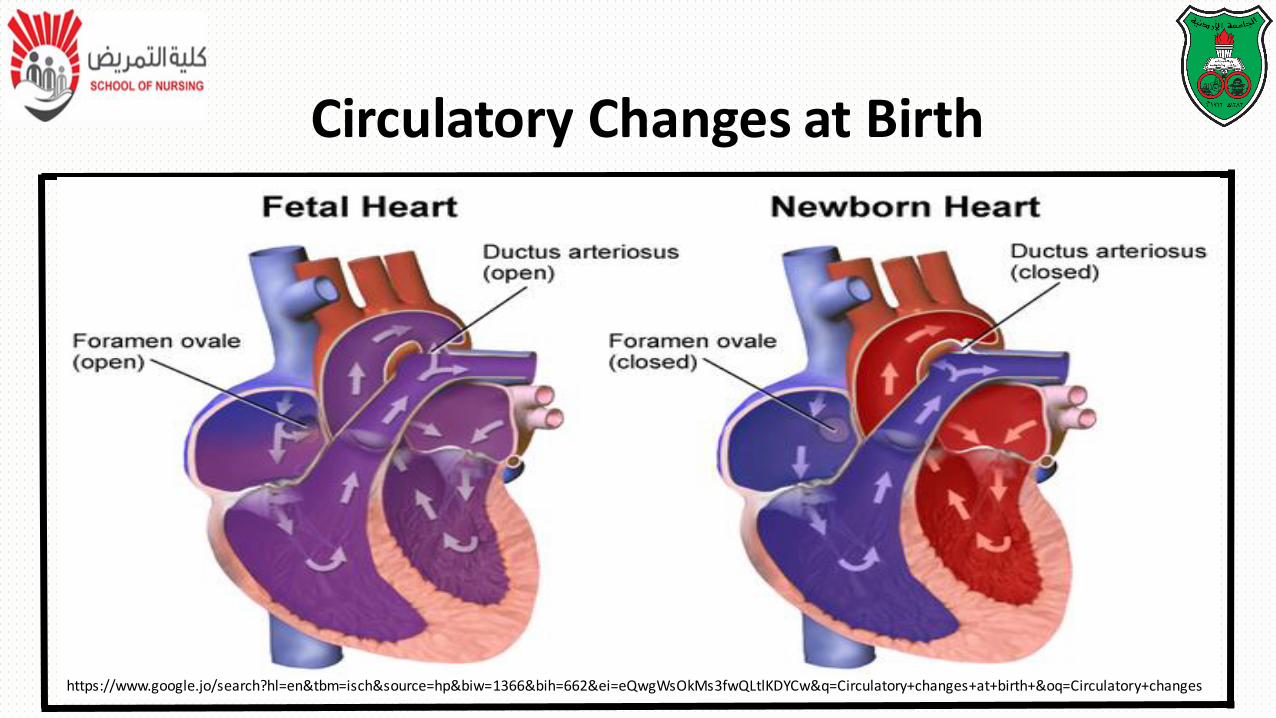
Circulatory Changes at Birth
https://www.google.jo/search?hl=en&tbm=isch&source=hp&biw=1366&bih=662&ei=eQwgWsOkMs3fwQLtlKDYCw&q=Circulatory+changes+at+birth+&oq=Circulatory+changes
Congenital Heart Defects
Causes:
• The exact etiology of CHD is unknown
• a complex interaction of genetic and environmental factors
Risk factors:
• Maternal factors (chronic illnesses such as diabetics)
• Alcohol consumption
Congenital Heart Defects
Risk factors:
• Exposure to environmental toxins
• Infections
• Family history
• Chromosomal abnormalities
• Syndromes
• Down syndrome (trisomy 21) and trisomy 13 and 18
More than 35 types of congenital heart defect (CHD) have been identified
• The Traditional classification is A cyanotic defects and cyanotic defects:
• Clinically, this system is challenging because children with A cyanotic defects may develop cyanosis
OR
• Children with cyanotic defects may appear pink
Classification of Congenital Heart Defects
• A more useful classification system is based on hemodynamic characteristic (blood flow patterns within the heart).
1.Increased pulmonary blood flow ( A cyanotic):
• Defects that allow blood flow from the higher pressure left side
of the heart to the lower pressure right side (left-to-right shunt)
result in increased pulmonary blood flow and cause CHF
Congenital Heart Disease CHD
1. Increased pulmonary blood flow ( A cyanotic):
Types:
• Atrial Septal defect (ASD)
• Ventricular septal defect (VSD)
• Patent ductus arteriosus (PDA)
Congenital Heart Disease CHD
A more useful classification system is based on hemodynamic characteristic (blood flow patterns within the heart).
2. Obstruction of blood flow from ventricles( A cyanotic):
• Coarctation of aorta (CoA)
• Aortic stenosis (AS)
• Pulmonic stenosis (PS)
Congenital Heart Disease CHD
3. Decrease blood flow ( cyanotic):
• Tetralogy of Fallot (ToF)
• Tricuspid atresia (TA)
4. Mixed blood flow ( cyanotic):
• Transposition of great arteries (TGA)
• Truncus arteriosus (TA)
Congenital Heart Disease CHD
https://www.youtube.com/watch?v=UNWxKDvBFik
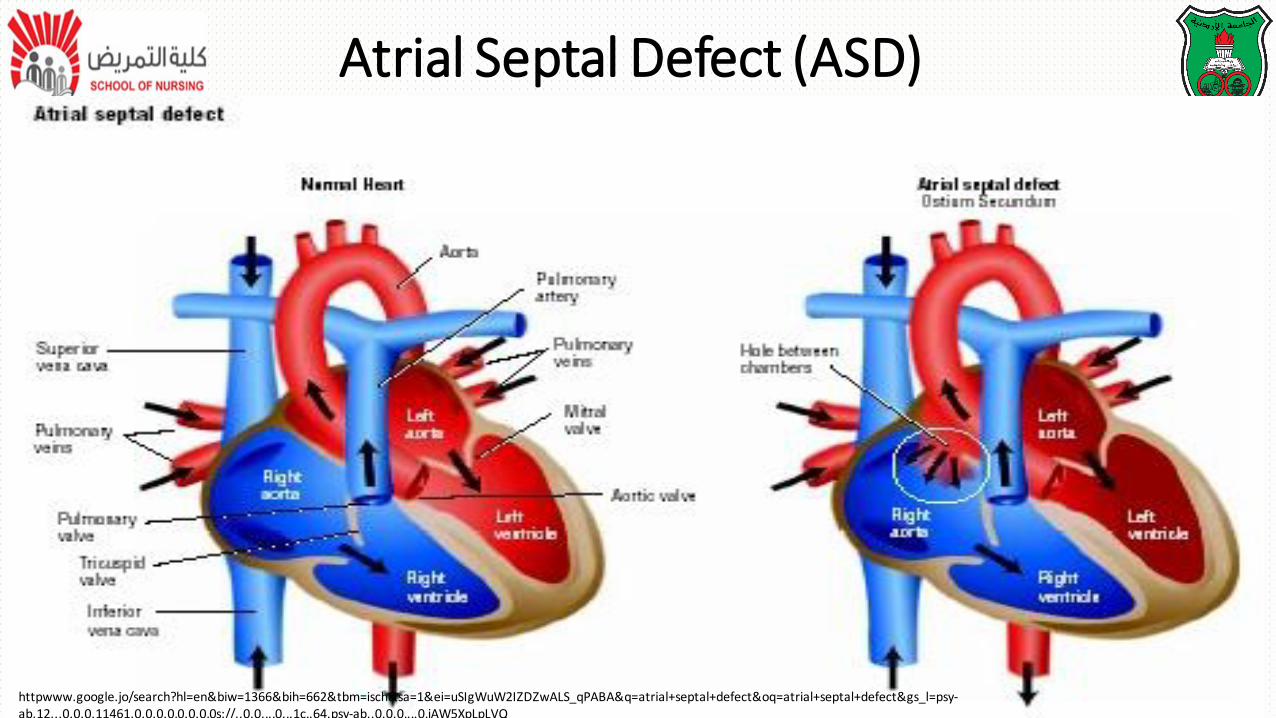
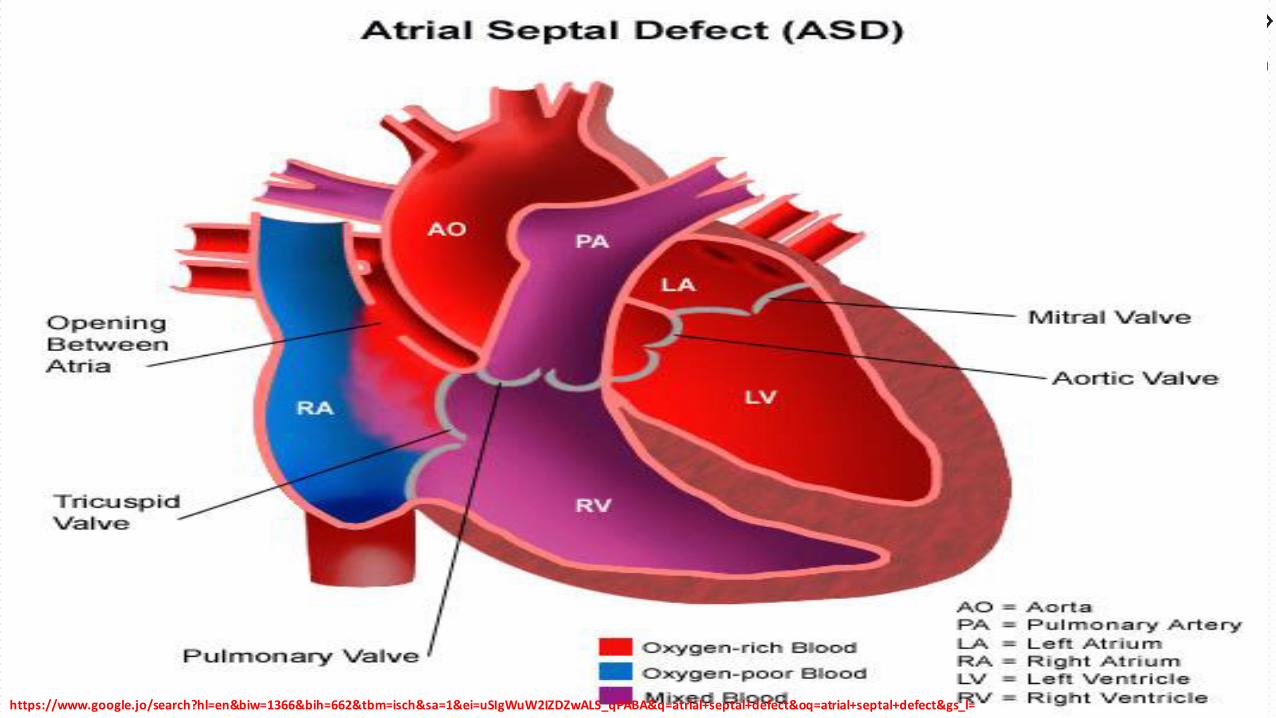
• Abnormal opening between the atria allowing blood from the higher
pressure left atrium to flow into the lower pressure right atrium
11/3/2020 Suhaila Halasa RN, PhD, CIMI,CPT 32
1. Increased pulmonary blood flow ( A cyanotic):
Types:❑ ASD1 (Ostium primum): opening at the lower end of the septum; may be
associated with mitral valve abnormalities
❑ ASD2: (Ostium secundom): opening near center of the septum
❑ Sinus venous defect: opening near junction of superior vena cava and
right atrium; may be associated with partial anomalous pulmonary venous connection
Atrial Septal Defect (ASD)
Atrial Septal Defect (ASD)
httpwww.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=1&ei=uSIgWuW2IZDZwALS_qPABA&q=atrial+septal+defect&oq=atrial+septal+defect&gs_l=psy-ab.12...0.0.0.11461.0.0.0.0.0.0.0.0s://..0.0....0...1c..64.psy-ab..0.0.0....0.jAW5XpLpLVQ
https://www.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=1&ei=uSIgWuW2IZDZwALS_qPABA&q=atrial+septal+defect&oq=atrial+septal+defect&gs_l=
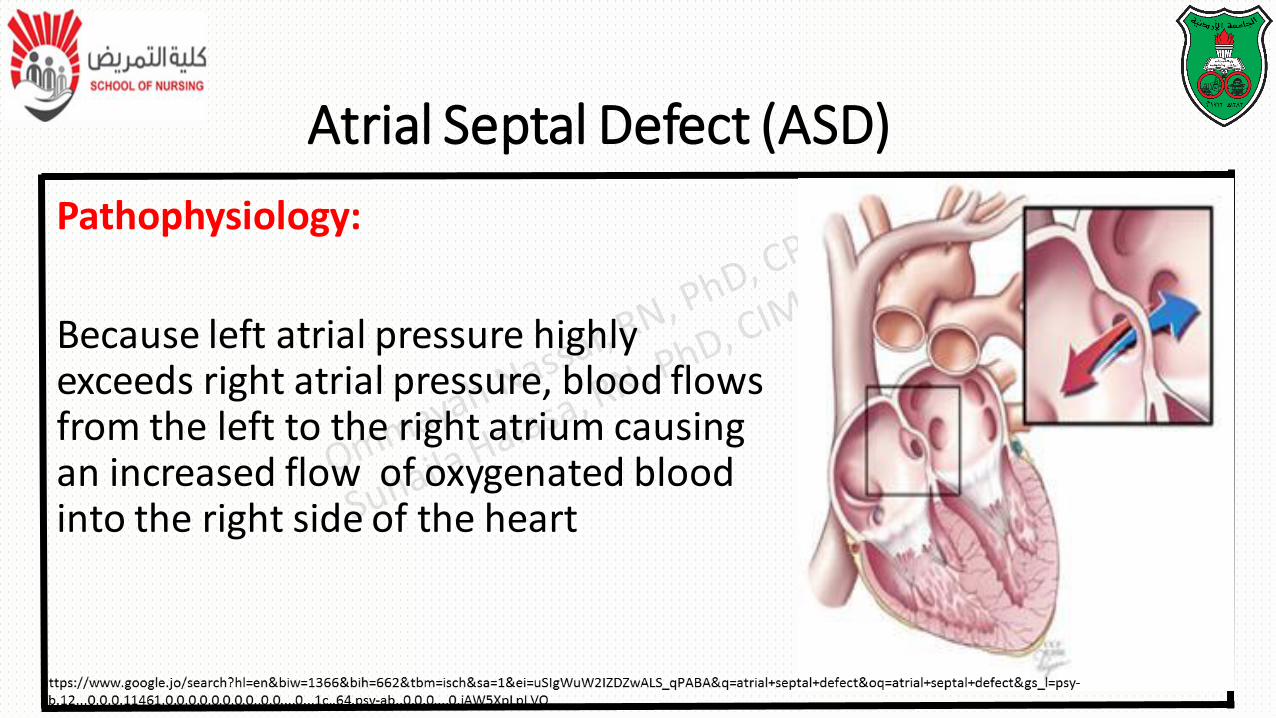
Pathophysiology:
Because left atrial pressure highly exceeds right atrial pressure, blood flows from the left to the right atrium causing an increased flow of oxygenated blood into the right side of the heart
Atrial Septal Defect (ASD)
Clinical manifestations:
• May be a symptomatic
• May develop congestive heart failure in
their 30s or 40s
• Systolic or diastolic murmur
Atrial septal defect (ASD)
Clinical manifestations:
• At risk of atrial dysrhythmia, pulmonary
obstructive disease and emboli formation later
due to chronically increased pulmonary blood flow
Atrial septal defect (ASD)
Surgical treatment:
• Surgical patch closure (pericardial Dacron patch) for moderate and large
defect
• A Dacron graft can be used as a stent to repair an artery, blood vessel, or
other hollow structure in the body
Atrial Septal Defect (ASD)
Surgical treatment:
• Open repair of cardiopulmonary bypass before school age
• The sinus venosus defect requires patch placement
• For ADS1: it might require mitral valve repair or replacement of the mitral valve
Atrial Septal Defect (ASD)
Therapeutic Management
Non surgical treatment:
• Transcatheter closure: ADS2 closure device during cardiac cauterization
• Child receive low dose aspirin for 6 months
• Prognosis: operative mortality is very low less that 1%
https://www.khanacademy.org/science/health-and-medicine/circulatory-system-diseases/acyanotic-heart-diseases/v/rn-ventricular-septal-defect
11/3/2020 Suhaila Halasa RN, PhD, CIMI,CPT 42
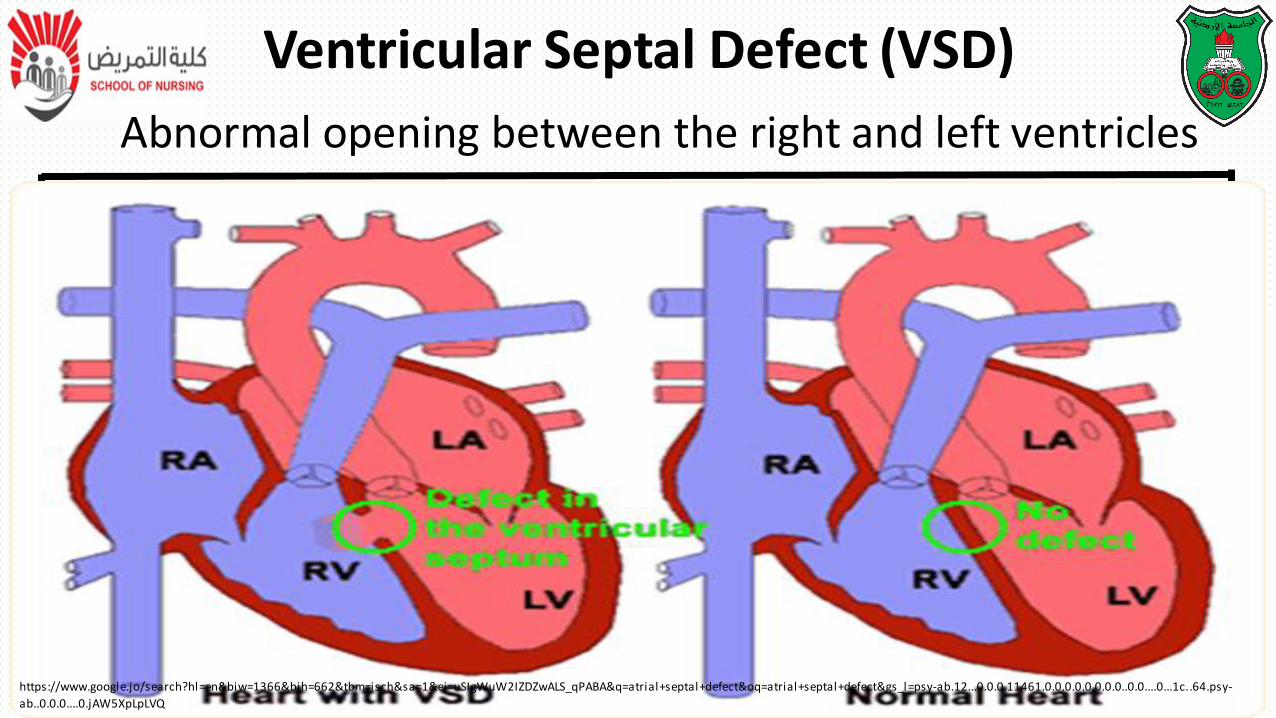
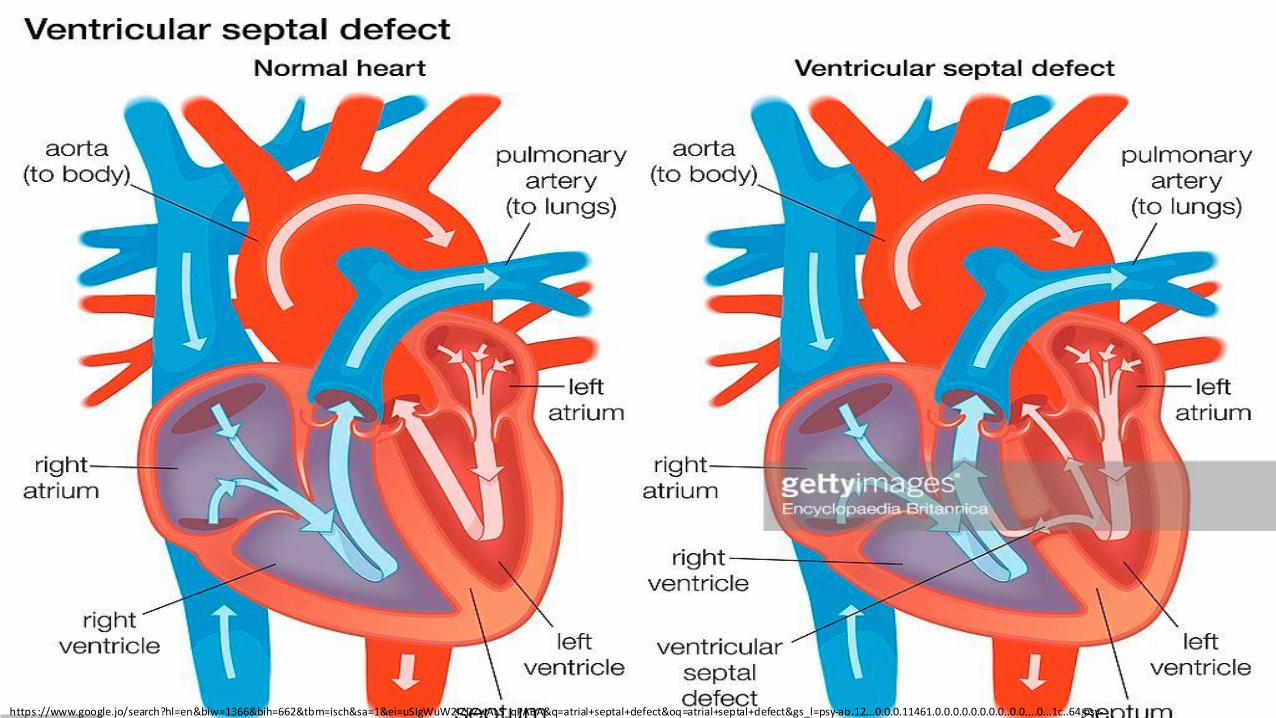
Abnormal opening between the right and left ventricles
Ventricular Septal Defect (VSD)
https://www.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=1&ei=uSIgWuW2IZDZwALS_qPABA&q=atrial+septal+defect&oq=atrial+septal+defect&gs_l=psy-ab.12...0.0.0.11461.0.0.0.0.0.0.0.0..0.0....0...1c..64.psy-
ab..0.0.0....0.jAW5XpLpLVQ
https ://www.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=1&ei=uSIgWuW2IZDZwALS_qPABA&q=atrial+septal+defect&oq=atrial+septal+defect&gs_l=psy-ab.12...0.0.0.11461.0.0.0.0.0.0.0.0..0.0....0...1c..64.psy-ab..0.0.0....0.jAW5XpLpLVQ
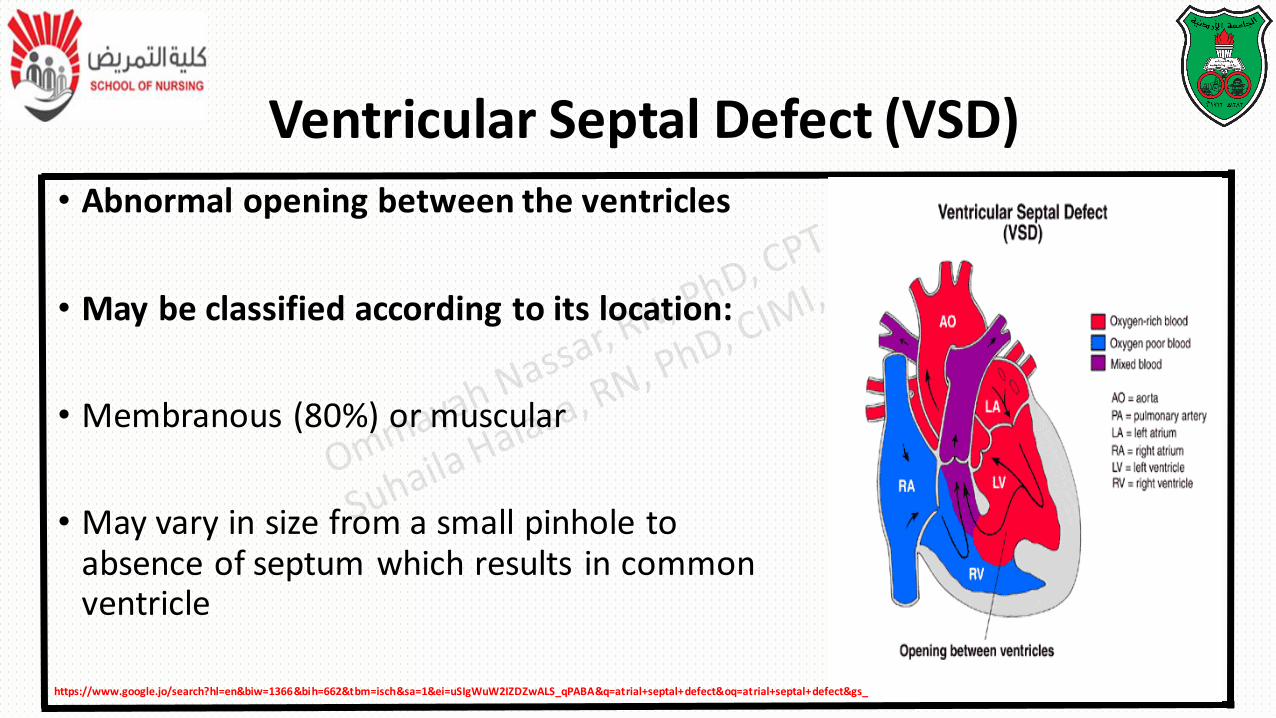
• Abnormal opening between the ventricles
• May be classified according to its location:
• Membranous (80%) or muscular
• May vary in size from a small pinhole to absence of septum which results in common ventricle
Ventricular Septal Defect (VSD)
https://www.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=1&ei=uSIgWuW2IZDZwALS_qPABA&q=atrial+septal+defect&oq=atrial+septal+defect&gs_
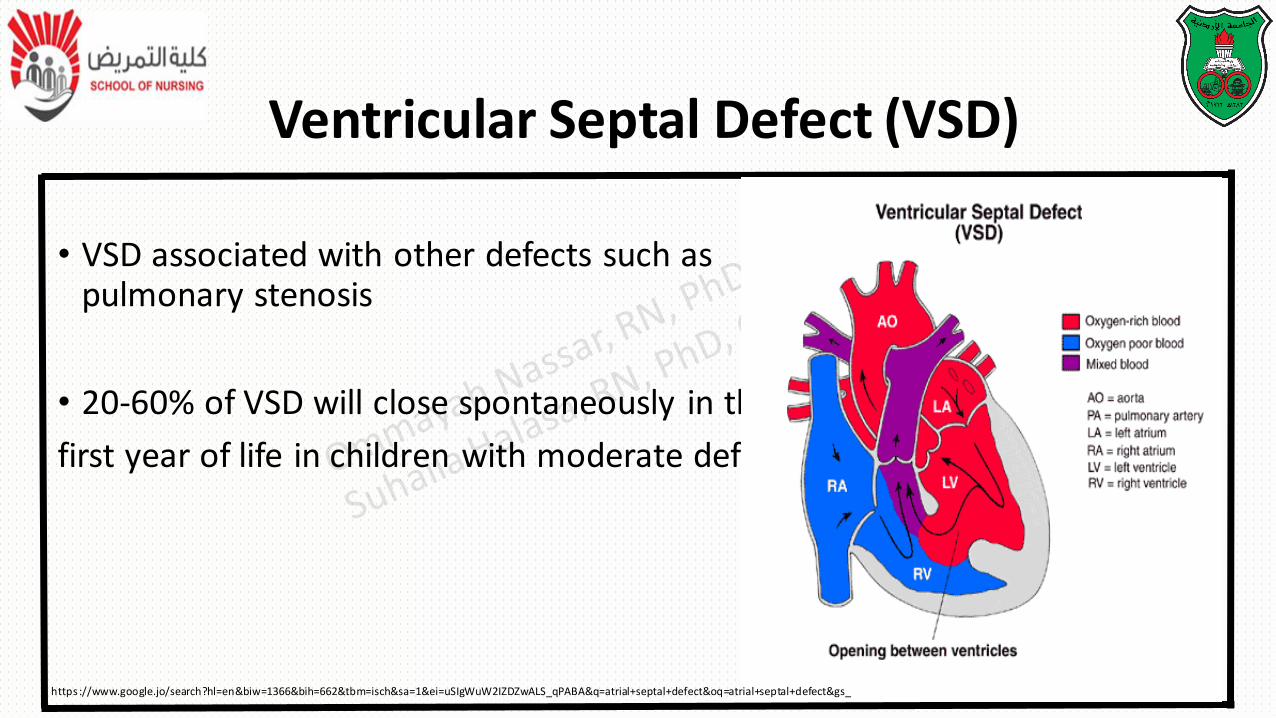
• VSD associated with other defects such as pulmonary stenosis
• 20-60% of VSD will close spontaneously in the
first year of life in children with moderate defect
Ventricular Septal Defect (VSD)
https ://www.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=1&ei=uSIgWuW2IZDZwALS_qPABA&q=atrial+septal+defect&oq=atrial+septal+defect&gs_
Pathophysiology:
Because the higher pressure within
the left ventricle and because the
systemic arterial circulation offer
more resistance than the pulmonary circulation,
blood flows through the defect into pulmonary artery
Ventricular Septal Defect (VSD)
Pathophysiology
• The increased blood volume is pumped into the lung lead to
increase pulmonary vascular resistance
• Increase pressure in the right ventricle as a result of left –to-
right shunt and pulmonary resistance causes muscle
hypertrophy
Pathophysiology
• If the right ventricle is unable to accommodate the increased
workload, the right atrium may also enlarge as it attempts to
overcome the resistance offered by incomplete right
ventricular emptying
Clinical manifestations:
• CHF common
• Holosystolic Murmur heard best at the left sternal border
• Children at risk of bacterial endocarditis and pulmonary vascular diseases
Ventricular Septal Defect (VSD)
Surgical repair:
• Palliative: pulmonary artery banding may be done in infant with multiple muscular defect
• Complete repair: (procedure of choice): small defect is repaired with suture
Ventricular Septal Defect (VSD)
Surgical repair:
• Large defect require patch (knitted Dacron Patch sewn over opening) through cardiopulmonary bypass
• Postoperative complications include:
residual VSD
conduction disturbances
Ventricular Septal Defect (VSD)
Transcatheter closure: device closure during cardiac catheterization for muscular defect
Prognosis: risk depends on the location of defect, the number of defects and presence of other defects
• Single muscular defect has low mortality Less than 2%
• Multiple muscular defect carry a higher risk
Ventricular Septal Defect (VSD)
• https://www.khanacademy.org/science/health-and-medicine/circulatory-system-diseases/acyanotic-heart-diseases/v/patent-ductus-arteriosus
• https://www.youtube.com/watch?v=7DKaCqubuSg
Patent Ductus Arteriosus
https://www.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=1&ei=lyMgWrvlGMbdwAKMgKW4BQ&q=Patent+ductus+arteriosus&oq=Patent+ductus+arteriosus&gs_l=
Patent Ductus Arteriosus
https://www.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=1&ei=lyMgWrvlGMbdwAKMgKW4BQ&q=Patent+ductus+arteriosus&oq=Patent+ductus+arteriosus&gs_l=psy-
ab.12..0l2j0i67k1j0l7.406300.411234.0.412512.33.11.0.0.0.0.193.758.0j5.7.0....0...1c.1j2.64.psy-ab..29.2.322.0..0i24k1.120.3a1yZeczj94
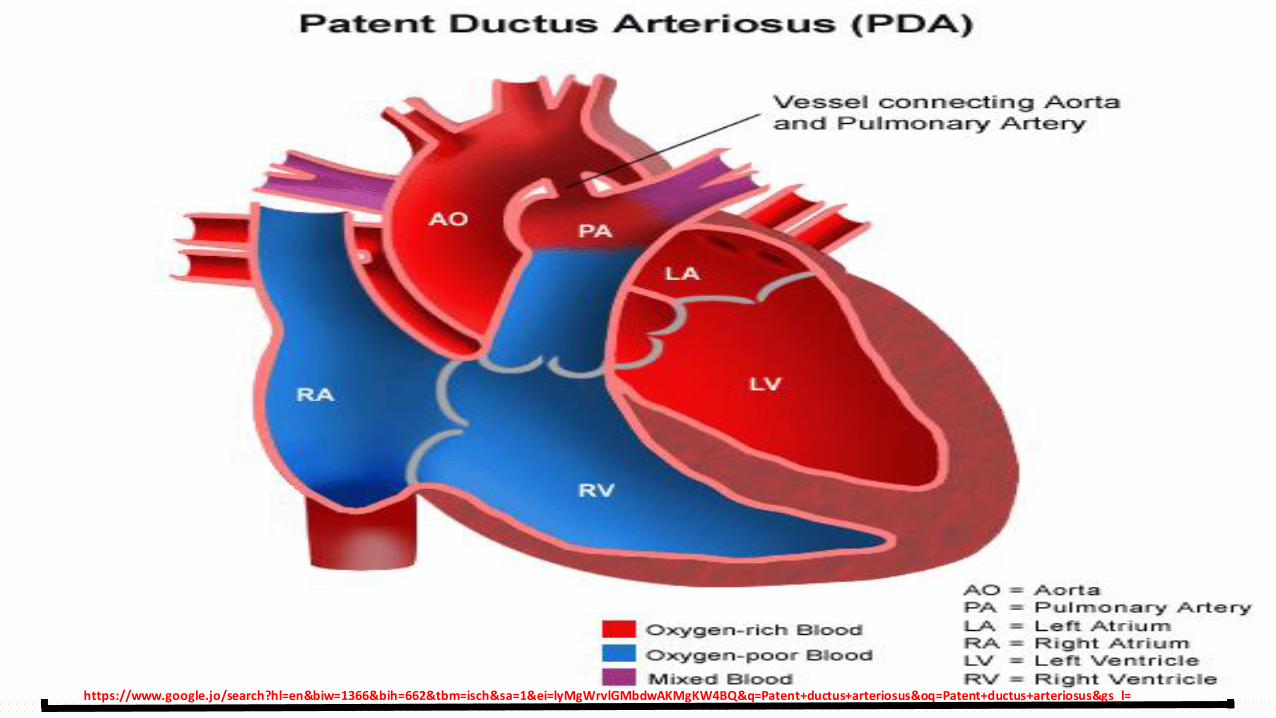
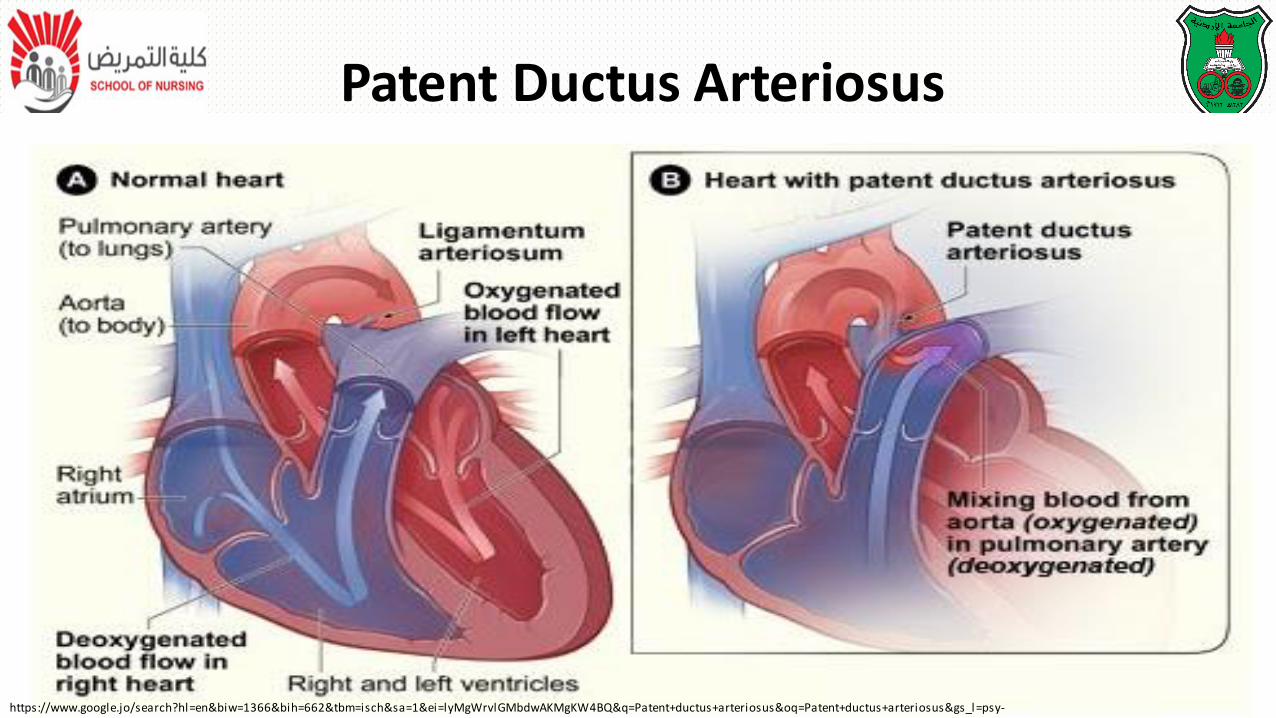
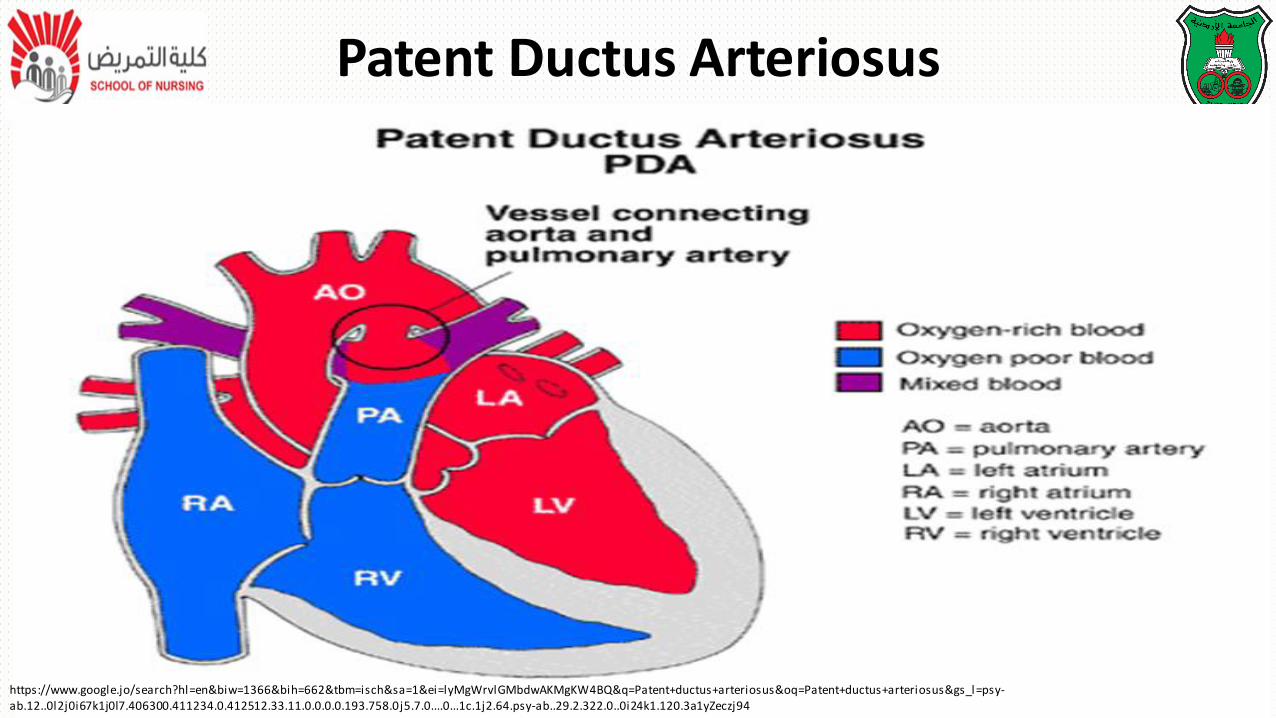
• Failure of fetal ductus arteriosus (artery connecting the aorta and
pulmonary artery) to close within the first week of life
• The continued patency of this vessels allows blood to flow from higher
pressure aorta to lower pressure pulmonary artery which cause left to
right shunt
Patent Ductus Arteriosus
Patent Ductus Arteriosus
https://www.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=1&ei=lyMgWrvlGMbdwAKMgKW4BQ&q=Patent+ductus+arteriosus&oq=Patent+ductus+arteriosus&gs_l=psy-ab.12..0l2j0i67k1j0l7.406300.411234.0.412512.33.11.0.0.0.0.193.758.0j5.7.0....0...1c.1j2.64.psy-ab..29.2.322.0..0i24k1.120.3a1yZeczj94
Pathophysiology
• At birth, the resistance in the pulmonary and systematic circulations is almost identical, so that resistance in pulmonary artery and aorta is equalized
• As systematic pressure comes to exceed the pulmonary pressure, blood begins to shunt from aorta across the duct of the pulmonary artery (left to right shunt)
Patent Ductus Arteriosus
Clinical Manifestations:
• May be asymptomatic or show signs of CHF
• There is a characteristics of machinery like murmur
• Widened pulse pressure and bounding pulse
• At risk of bacterial endocarditis and pulmonary vascular obstructive disease
Patent Ductus Arteriosus
Medical Management:
• Endomethacin ( prostaglandin inhibitor) to close PDA in preterm infants and some newborns
Surgical RX: ligation of the patent vessel via a left thoracotomy
Patent Ductus Arteriosus
Transcatheter treatment: coils to occlude the PDA during catheterization
Coil (loop) occlusion: is a procedure to close the opening between infant's aorta and pulmonary artery.
Prognosis: both surgical and non surgical procedures can done at low risk less than 1% mortality
Patent Ductus Arteriosus
• Obstructive defects are those in which blood existing the heart meets an
area of anatomic narrowing(stenosis)
• The pressure in the ventricle and great artery before the obstruction
increased and the pressure in the area beyond the obstruction is
decreased
Obstructive Defect
The location of narrowing usually near the valve as following:
• Valvular: at the site of valve itself
• Sub valvular: narrowing in the ventricle below the valve
• Supra valvular: narrowing in the great artery above the valve
Obstructive Defect
Coarctation of Aorta CoA
https://www.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=1&ei=lyMgWrvlGMbdwAKMgKW4BQ&q=Patent+ductus+arteriosus&oq=Patent+ductus+arteriosus&gs_l=psy-ab.12..0l2j0i67k1j0l7.406300.411234.0.412512.33.11.0.0.0.0.193.758.0j5.7.0....0...1c.1j2.64.psy-ab..29.2.322.0..0i24k1.120.3a1yZeczj94
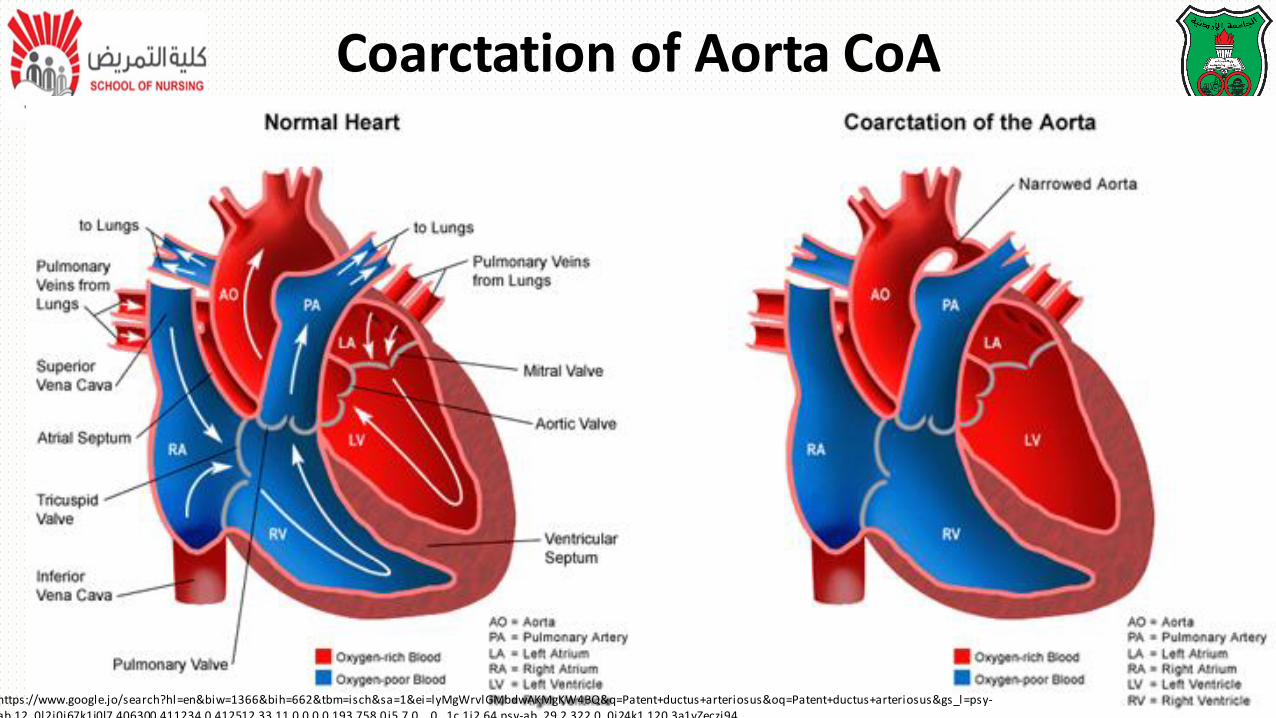
• Description:
- Localized narrowing near the insertion of the ductus arteriosus.
- Results in increased pressure proximal to the defect (head and upper
extremities) and decreased pressure distal to the obstruction( body and
lower extremities).
Coarctation of Aorta CoA
Pathophysiology:
• The effect of a narrowing within the aorta is increased pressure
proximal to the defect (upper extremities) and decreased pressure
distal to it (lower extremities).
Coarctation of Aorta CoA
Clinical manifestations:
- May have high blood pressure and bounding pulse in the arms
- Weak or absent femoral pulse and cool lower extremities with lower blood pressure.
- There are signs of CHF in infants.
- In infants with critical Coarctation the hemodynamics condition may deteriorate rapidly with sever acidosis and hypotension.
Coarctation of Aorta CoA
Clinical manifestations:
- Mechanical ventilation and is often necessary before surgery.
- Older children may experience dizziness, headaches, fainting, and epistaxis resulting from hypertension.
- At risk for hypertension, ruptured aorta, aortic aneurysm (enlargement or dilation of the aorta to greater than 1.5 times normal size), and stroke.
Coarctation of Aorta CoA
Surgical treatment:
The treatment of choice for:
- Infants less than 6 months of age
- Children with long-segment stenosis or complex anatomy
Coarctation of Aorta CoA
• Surgical treatment: Repair by:
- Either resection of the coarcted portion with an end-to end
anastomosis of the aorta
OR
- Enlargement of the constricted section using a graft of prosthetic
material or a portion of the left subclavian artery.
Coarctation of Aorta CoA
• Surgical treatment:
- Elective surgery for CoA is advised within the first 2 years of life (to
prevent hypertension at rest and exercise-provoked systemic hypertension
after repair
- There is a 5%-10% risk of recurrent narrowing in children who underwent
surgical repair as infants
Coarctation of Aorta CoA
• Transcatheter treatment:
- Angioplasty: (any procedure to widen vessels narrowed by stenosis or
occlusions)
- A primary intervention for CoA is being performed in some centers.
Coarctation of Aorta CoA
Prognosis:
- Low rates of morbidity and mortality
- Major long-term complications:
- Recoarctation
- Aortic aneurysm (weakening of the wall)
- Systemic hypertension
Coarctation of Aorta CoA
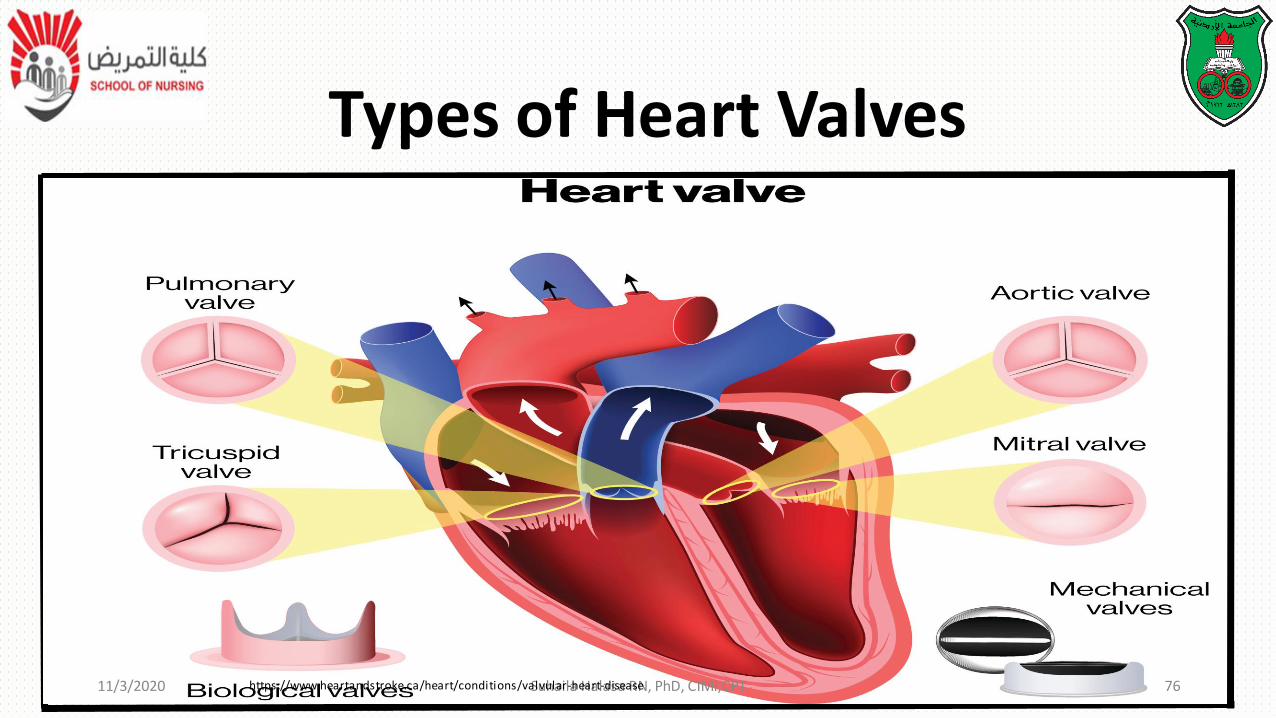
Types of Heart Valves
11/3/2020 Suhaila Halasa RN, PhD, CIMI,CPT 76https://www.heartandstroke.ca/heart/conditions/valvular-heart-disease
Aortic Stenosis
https://www.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=1&ei=lyMgWrvlGMbdwAKMgKW4BQ&q=Patent+ductus+arteriosus&oq=Patent+ductus+arteriosus&gs_l=psy-ab.12..0l2j0i67k1j0l7.406300.411234.0.412512.33.11.0.0.0.0.193.758.0j5.7.0....0...1c.1j2.64.psy-ab..29.2.322.0..0i24k1.120.3a1yZeczj94
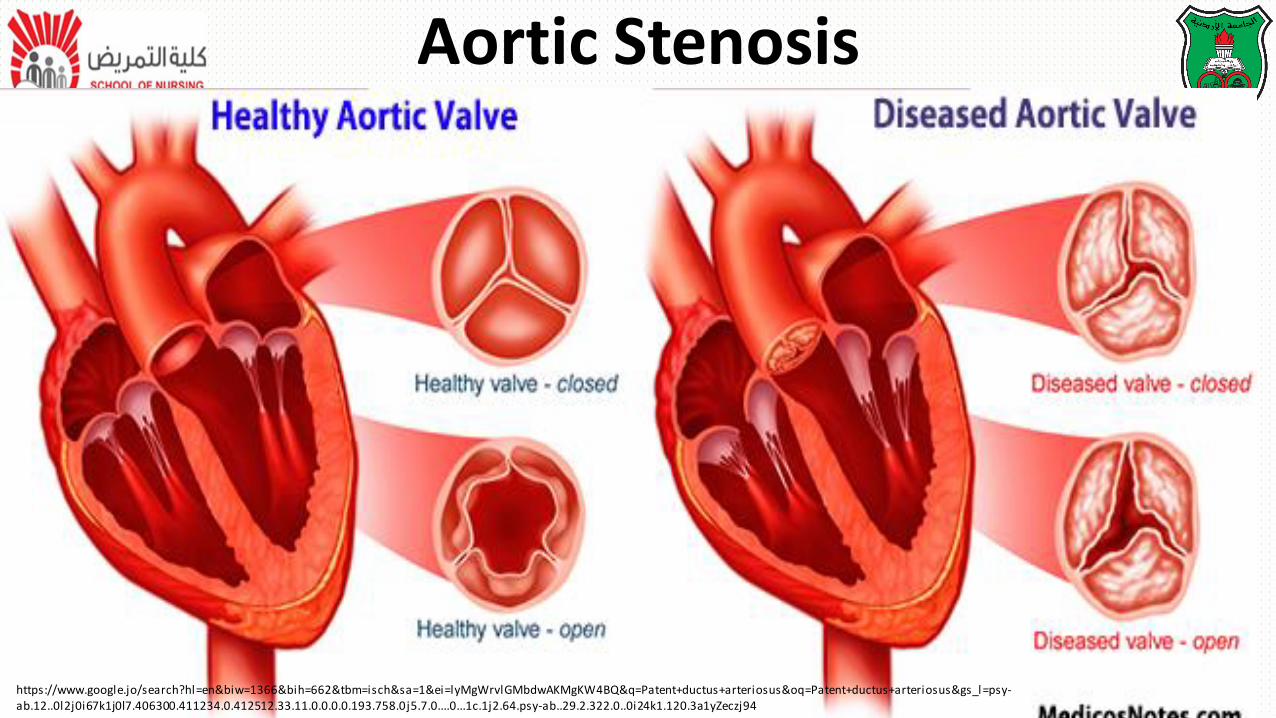
Description:
- Narrowing or stricture of the aortic valve,
- Causing resistance to blood flow in the left ventricle, decreased cardiac
output, left ventricular hypertrophy, and pulmonary vascular congestion.
Aortic Stenosis (AS)
Description:
- The prominent anatomic consequence of AS is the hypertrophy of the left
ventricular wall, which eventually will lead to increased end-diastolic
pressure, resulting in pulmonary venous and pulmonary arterial
hypertension.
Aortic Stenosis (AS)
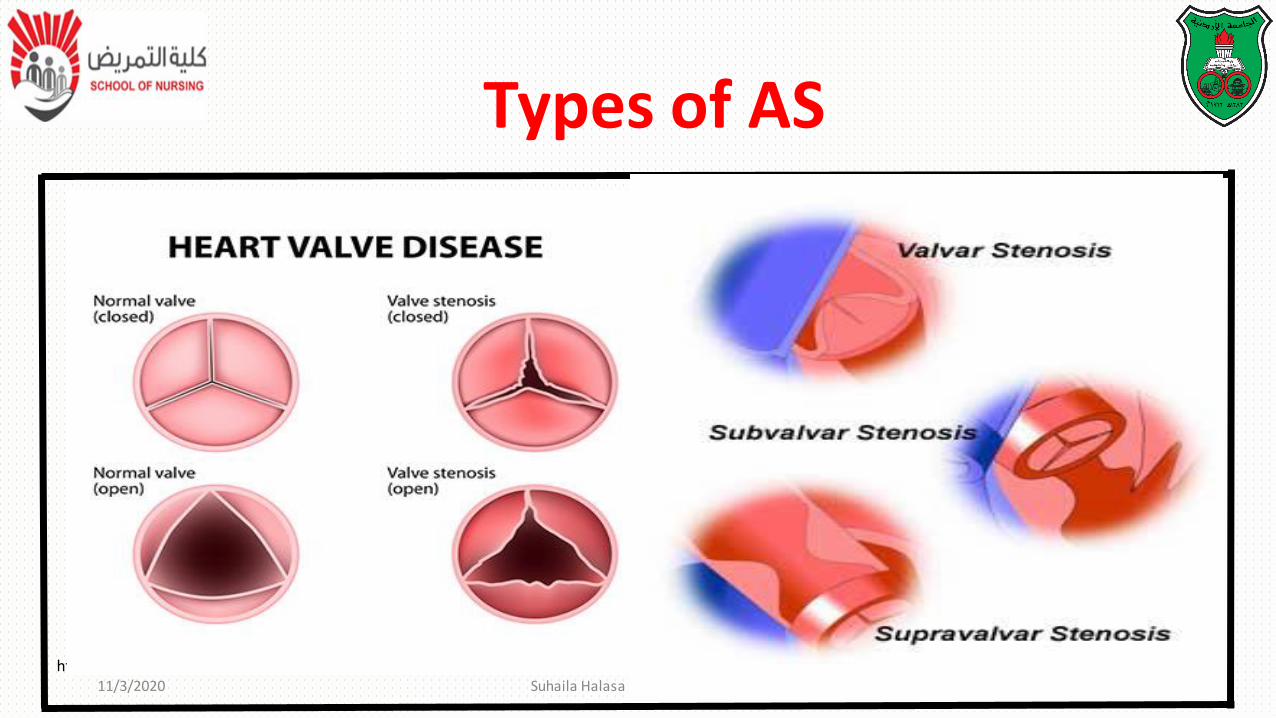
Types of AS
http://www.pted.org/?id=aorticstenosis611/3/2020 Suhaila Halasa RN, PhD, CIMI,CPT 80
Types of AS:
➢Valvular Aortic stenosis: anomaly of the valves result in a bicuspid
rather than tricuspid valve (the most common type)
➢Subvalvular stenosis: is a structure caused by fibrous ring below a
normal valve (obstruction in the ascending aorta)
Aortic Stenosis (AS)
Types of AS:➢Supravalvular stenosis: occurs infrequently an obstruction in the left
ventricular outflow
Valvular AS is a serious defect:• Obstruction tends to be progressive
• Sudden episodes of myocardial ischemia or low cardiac output (leads to death)
• Surgical repair rarely results in a normal valve
Aortic Stenosis (AS)
Clinical manifestations:
• Newborn with critical AS demonstrate signs of decreased cardiac output with faint pulses, hypotension, tachycardia, and poor feeding.
• Children show signs of exercise intolerance, chest pain, and dizziness when standing for a long period.
• A systolic ejection murmur may or may not be present.
• Children are at risk for bacterial endocarditis coronary insufficiency, and ventricular dysfunction.
Aortic Stenosis (AS)
• Valvular Aortic Stenosis:
• Surgical treatment:
- Balloon dilation in the catheterization laboratory is the first-line procedure.
- Aortic valvotomy is performed under inflow occlusion.
Aortic Stenosis (AS)
❑Prognosis:
- Aortic valve (palliative procedure) replacement offers a good treatment option
and may lead to normalization of left ventricular size and function.
- Results of aortic valvotomy (cutting through a stenosed cardiac valve to relieve
the obstruction)
Aortic Stenosis (AS)
❑Prognosis:
- Aortic valvotomy remains a palliative procedure, and
approximately 25% of children require additional surgery within
10 years for recurrent stenosis.
Aortic Stenosis (AS)
• Nonsurgical treatment:
- The narrowed valve is dilated using balloon angioplasty in the catheterization laboratory. this procedure is usually the first intervention
- Complication include aortic insufficiency or Valvular regurgitation, tearing of the valve leaflets, and loss of pulse in the catheterized limb.
Aortic Stenosis (AS)
• Subvalvular aortic stenosis:
(obstruction in the left ventricular outflow)
- Surgical treatment:
- if the obstruction results from narrowing of the left ventricular outflow tract and a small aortic valve annulus, a patch may be required to enlarge the entire left ventricular outflow tract and annulus and replace the aortic valve; this is known as the Konno procedure.
Aortic Stenosis (AS)
• Subvalvular aortic stenosis:
(obstruction in the left ventricular outflow)
- Prognosis:
- mortality is less than 5%, about 20% patients develop recurrent subaortic stenosis and require additional surgery.
Aortic Stenosis (AS)
• Subvalvular aortic stenosis:
(obstruction in the left ventricular outflow)
- Konno procedure:
- It involves the replacement of the aortic valve and the widening of the ventricular septum in the region of the valve with a patch
- Prognosis: mortality is less than 5%, about 20% patients develop recurrent subaortic stenosis and require additional surgery.
Aortic Stenosis (AS)
https ://www.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=1&ei=lyMgWrvlGMbdwAKMgKW4BQ&q=Patent+ductus+arteriosus&oq=Patent+ductus+arteriosus&gs_l=psy-
ab.12..0l2j0i67k1j0l7.406300.411234.0.412512.33.11.0.0.0.0.193.758.0j5.7.0....0...1c.1j2.64.psy-ab..29.2.322.0..0i24k1.120.3a1yZeczj94
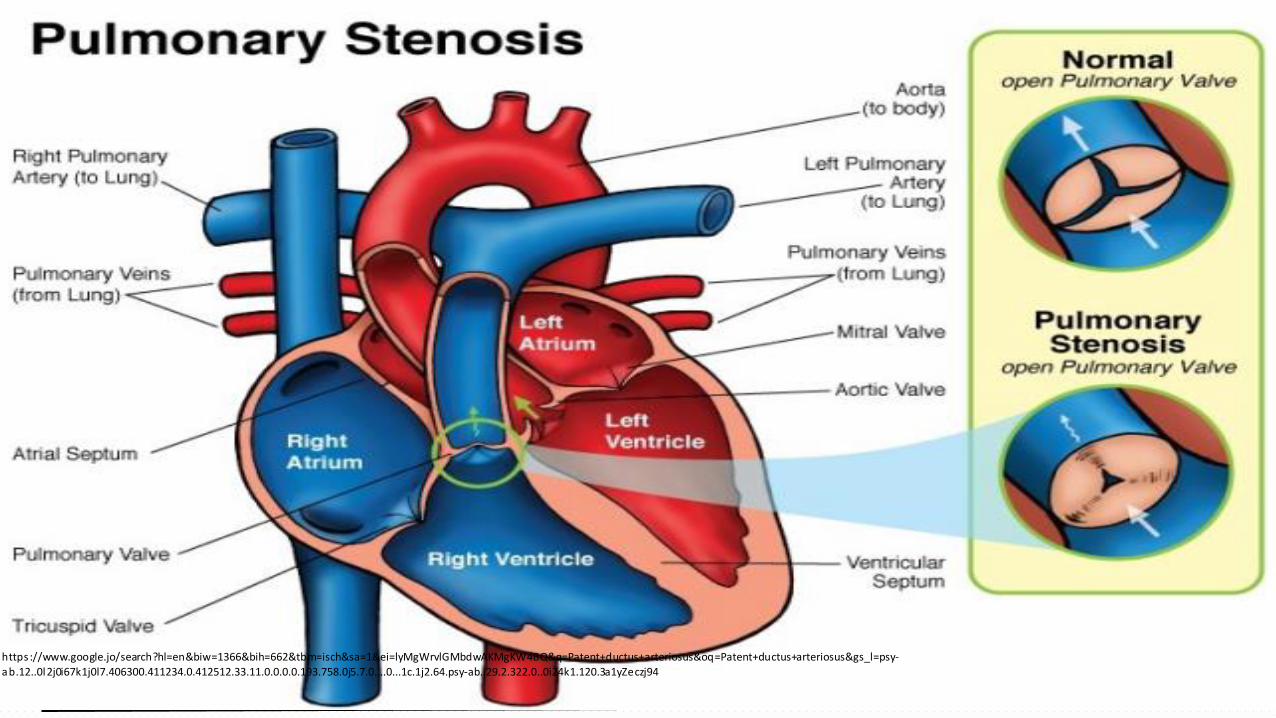
Pulmonic Stenosis (PS)
• Description:
- Narrowing at the entrance to the pulmonary artery.
- Resistance to blood flow causes right ventricular hypertrophy and decreased
pulmonary blood flow.
Pulmonic Stenosis (PS)
• Description:
• Pulmonary atresia is the extreme form of Pulmonic stenosis (PS) in that
there is total fusion of the commissures and no blood flow to the lungs
• The right ventricle may be hypoplastic.
Pulmonic Stenosis (PS)
• Pathophysiology:- Resistance to blood flow causes right ventricular hypertrophy
- If right ventricular failure develops, then ----
- Right atrial pressure increases --- may result in reopening of the foramen
oval
- Shunting of deoxygenated blood into the left atrium – systemic cyanosis
Pulmonic Stenosis (PS)
• Pathophysiology:
• If PS is sever:
- HF occurs
- associated defect (patent ductus arteriosus) to
compensates for obstruction by shunting blood from aorta
to the pulmonary artery and into the lung
Pulmonic Stenosis (PS)
• Clinical manifestations:
- May be asymptomatic
- Some have mild cyanosis HF
- Progressive narrowing causes increased symptoms
- Newborns with sever narrowing will be cyanotic
- Aloud systolic ejection murmur at the upper left sternal border may be present.
Pulmonic Stenosis (PS)
• Clinical manifestations:
- In sever ill Children, the murmur may be much softer due to decreased cardiac output and shunting of blood.
- Cardiomegaly is evident on chest radiographic films
- Children at risk for infective endocarditis
Pulmonic Stenosis (PS)
• Surgical treatment:
• Need for surgical treatment is rare with widespread use of balloon angioplasty techniques.
- Pulmonary valvotomy with cardiopulmonary bypass is necessary
Pulmonic Stenosis (PS)
• Transcatheter treatment:
- Balloon angioplasty in the cardiac catheterization laboratory to dilate the valve
- It is treatment of choice for discrete PS in most centers and can be done safely in neonates
Pulmonic Stenosis (PS)
• Prognosis:
- Risk is low for both surgical and nonsurgical procedures.
- Mortality rate is low, slightly higher in neonates
- Both balloon dilation and surgical valvotomy leave the pulmonic valve
incompetent because they involve opening the fused valve leaflets.
- Long term problem with restenosis or valve incompetence may occur.
Tetralogy of Fallot TOF
https ://www.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=1&ei=lyMgWrvlGMbdwAKMgKW4BQ&q=Patent+ductus+arteriosus&oq=Patent+ductus+arteriosus&gs_l=psy-ab.12..0l2j0i67k1j0l7.406300.411234.0.412512.33.11.0.0.0.0.193.758.0j5.7.0....0...1c.1j2.64.psy-ab..29.2.322.0..0i24k1.120.3a1yZeczj94
Tetralogy of Fallot TOF
11/3/2020 Suhaila Halasa RN, PhD, CIMI,CPT 102https://www.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=1&ei=lyMgWrvlGMbdwAKMgKW4BQ&q=Patent+ductus+arteriosus&oq=Patent+ductus+arteriosus&gs_l=psy-ab.12..0l2j0i67k1j0l7.406300.411234.0.412512.33.11.0.0.0.0.193.758.0j5.7.0....0...1c.1j2.64.psy-ab..29.2.322.0..0i24k1.120.3a1yZeczj94
https://www.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=1&ei=lyMgWrvlGMbdwAKMgKW4BQ&q=Patent+ductus+arteriosus&oq=
https://www.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=1&ei=sysgWoesGYjTwALA64KgCw&q=Tetralogy+of+Fallot+TOFy8-CFY
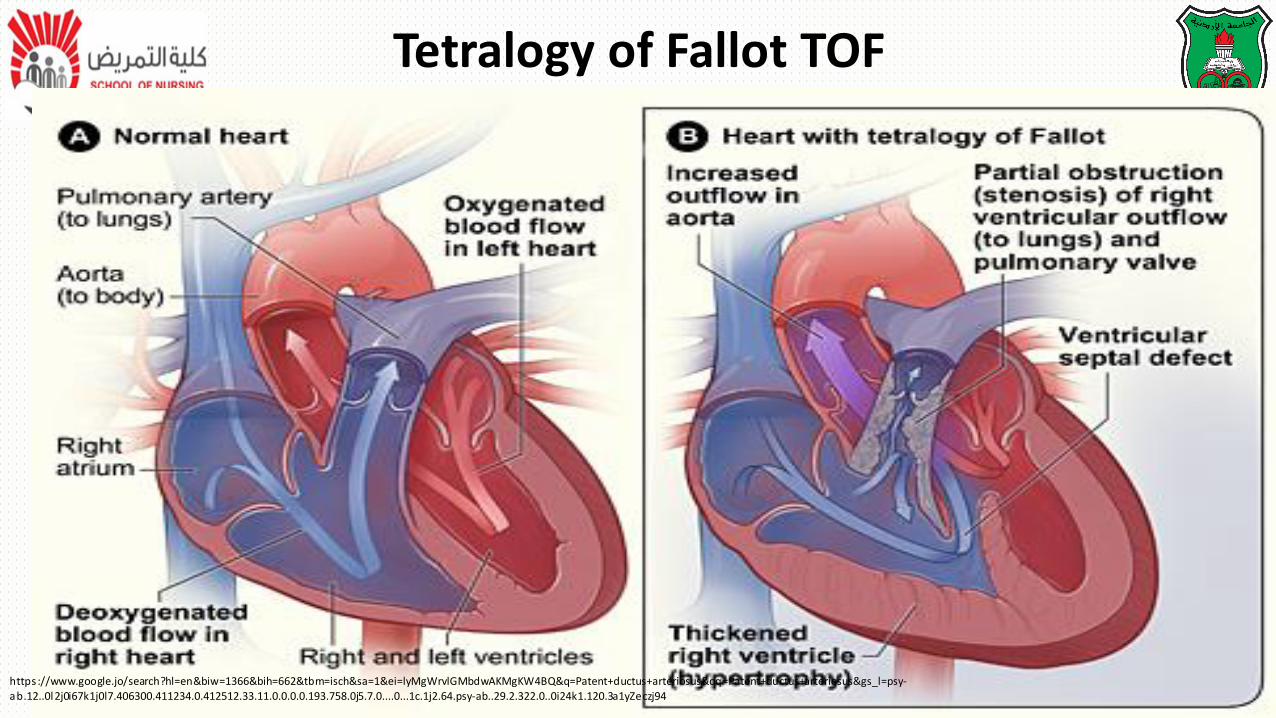
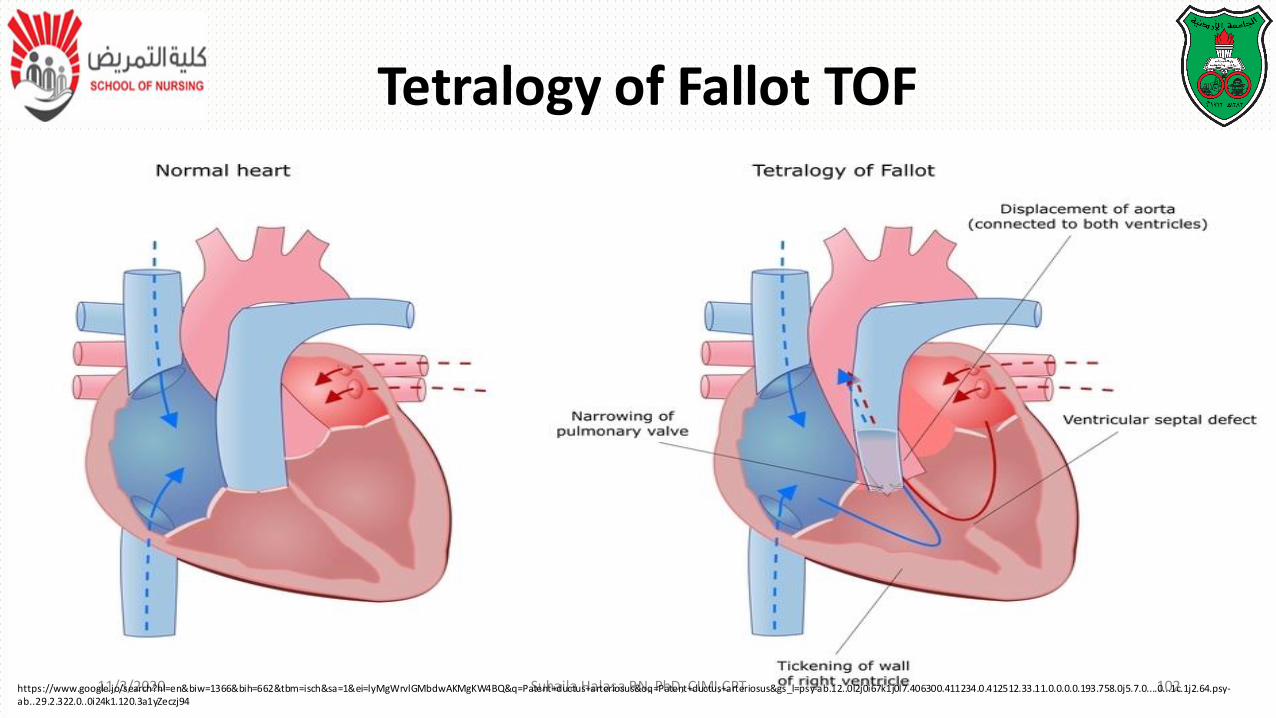
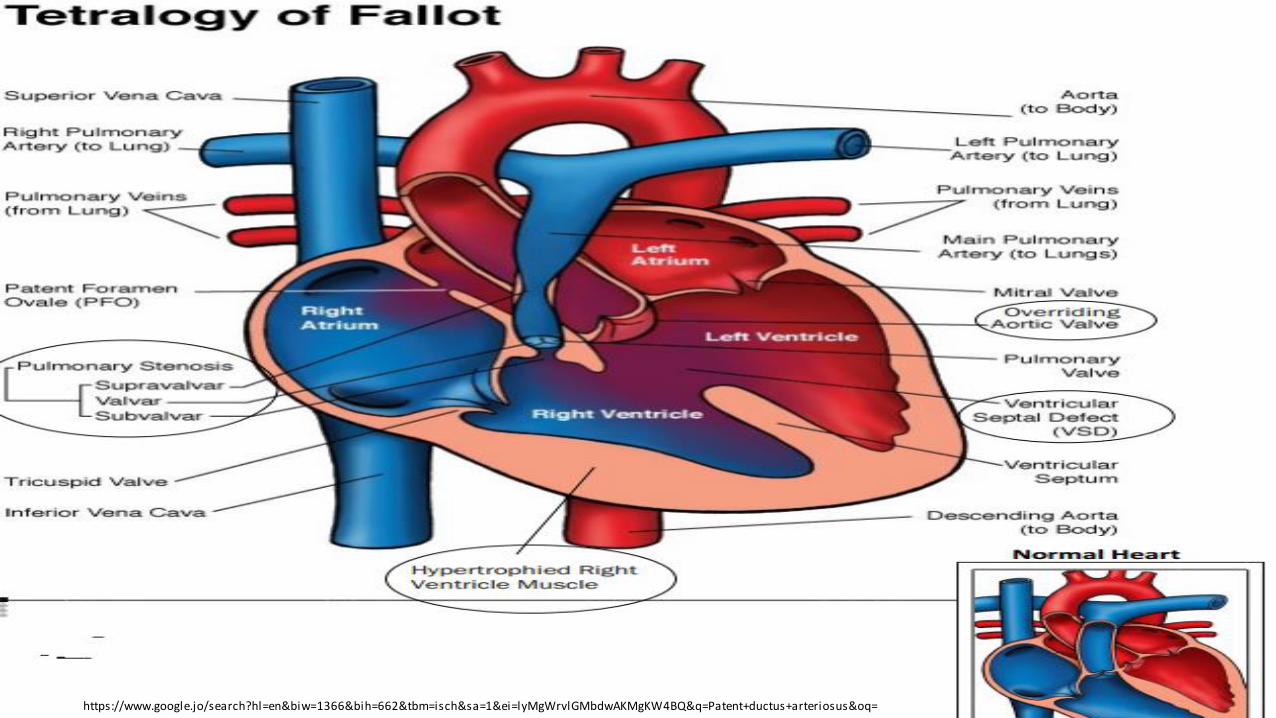
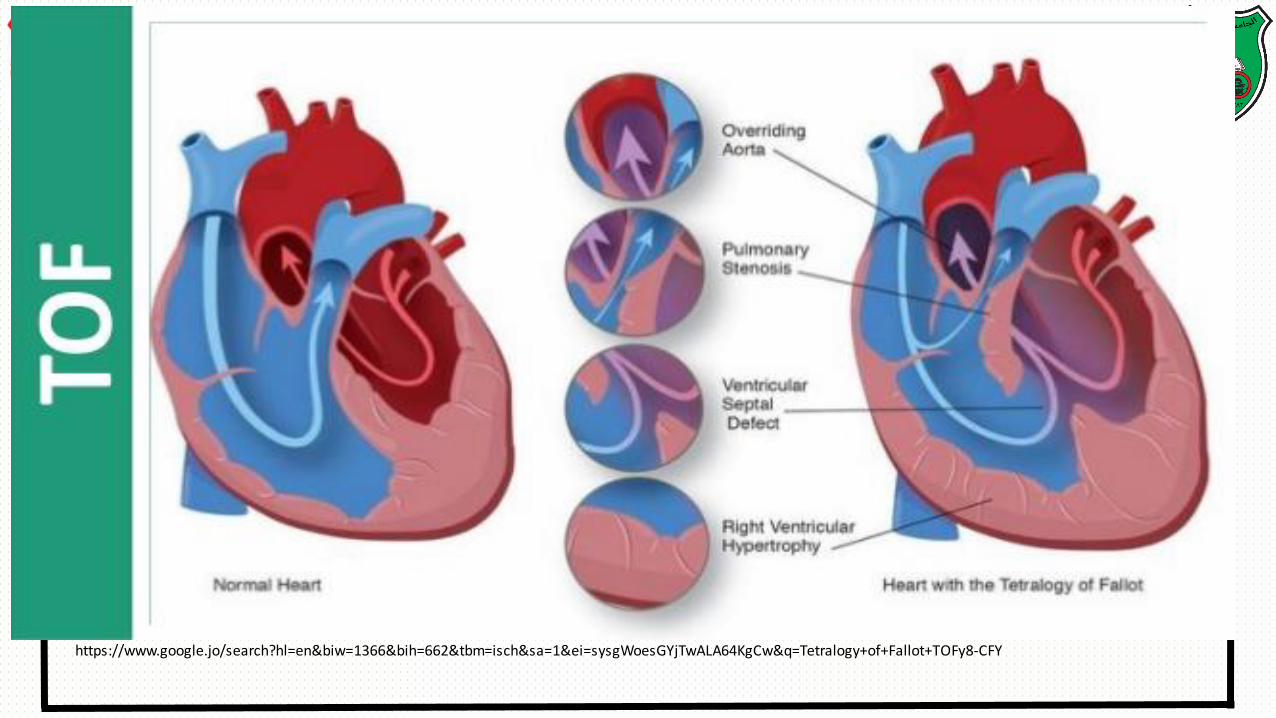
Tetralogy of Fallot TOF• Description:
The classic form includes four defects:
1. Ventricular septal defect VSD
2. Pulmonic Stenosis PS
3. Overriding aorta
4. Right ventricular hypertrophy
Tetralogy of Fallot TOF
• Clinical manifestations:
- Some infants may be acutely cyanotic at birth.
- Others have mild cyanosis that progresses over the first year of life as the PS worsens.
- There is a characteristic systolic murmur that is often moderate in intensity.
Tetralogy of Fallot TOF
• Clinical manifestations:
- Blue spells: acute episodes of cyanosis, dyspnea,
restlessness, decreased arterial PO2, decrease of
already compromised pulmonary blood flow, and
hypoxia
https://www.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=
Tetralogy of Fallot (TOF)
• Clinical manifestations:
- Infants may be acutely cyanotic at birth.
- Others have mild cyanosis that progresses over the first year of life
- Moderate systolic murmur
- Anoxic spells occur when the infant’s oxygen requirements exceed the blood supply,
usually during crying or after feeding.
Tetralogy of Fallot (TOF)
Children are at risk for:
- emboli
- seizure
- loss of consciousness
- sudden death following an anoxic spell.
Tetralogy of Fallot TOF
• Surgical treatment:
- Complete repair: elective repair is usually performed in the first year of life. when increasing cyanosis and the development of hypercyanotic spells.
- Complete repair involves closure of the VSD and resection of the stenosis, with placement of a pericardial patch to enlarge the right ventricular outflow tract.
Tetralogy of Fallot TOF
• Prognosis:
- Mortality rate for total correction is less than 3%
- Complications:
- Chronic regurgitation with right ventricular enlargement
- Aortic root dilation and oartic valve insufficiency
- Arrhymias
- Sudden cardiac death
• Many complex cardiac anomalies are classified together in the mixed
categories because survival in the post natal depend on mixing of blood
from the pulmonary and systemic circulations within the heart champers
• Fully saturated systemic blood flow mixes with desaturated pulmonary
blood flow
Mixed Defects
• Pulmonary congestion occurs because the differences pulmonary artery pressure and aortic pressure favor pulmonary blood flow
• Cardiac output decreases because of a volume load in the ventricle
• Children have variable picture that combines some degree of desaturation and signs of CHF
Mixed Defects
• Transposition of great vessels cause sever cyanosis in the first days of life and later cause CHF
• Truncus arteriosus causes sever CHF in the first weeks of life and mild desaturation
Mixed Defects
• Description:
• Great vessels are switched that the aorta arises from the right ventricle and the main pulmonary artery arises from the left ventricle.
• It causes complete separation from the two circulation.
• Transposition of great vessels cause sever cyanosis in the first days of life and later cause CHF
Mixed Defects
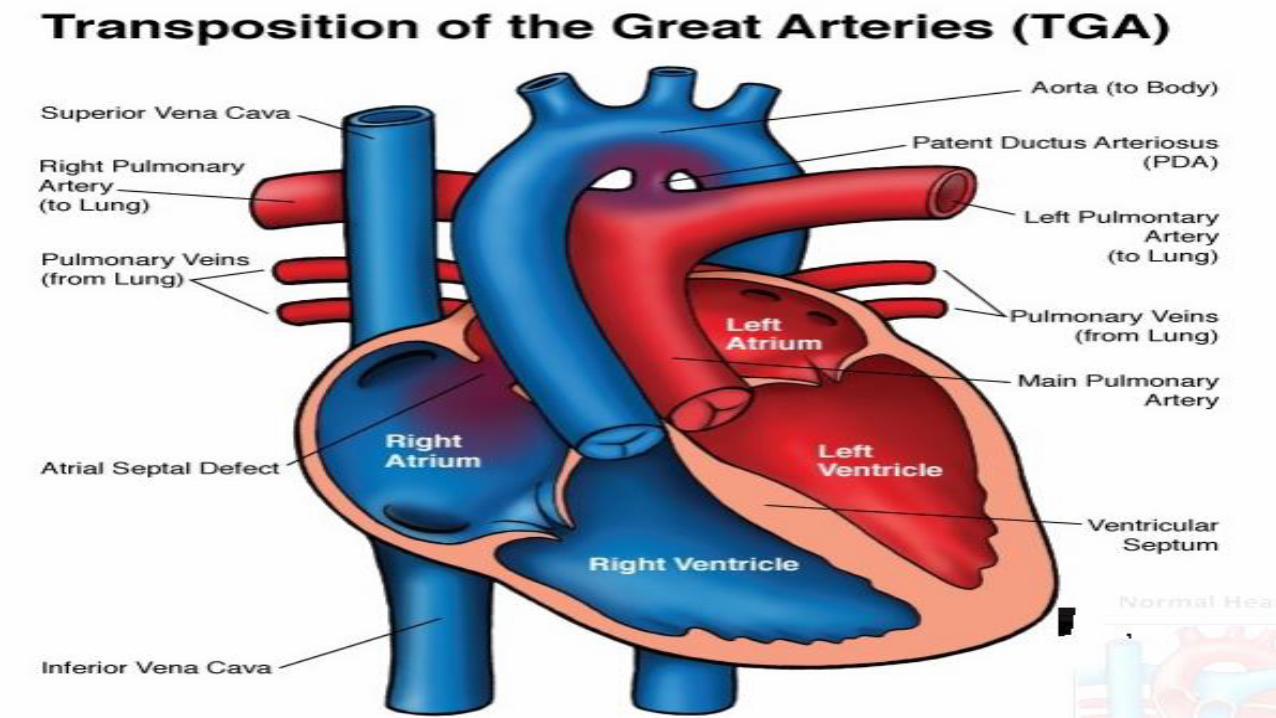
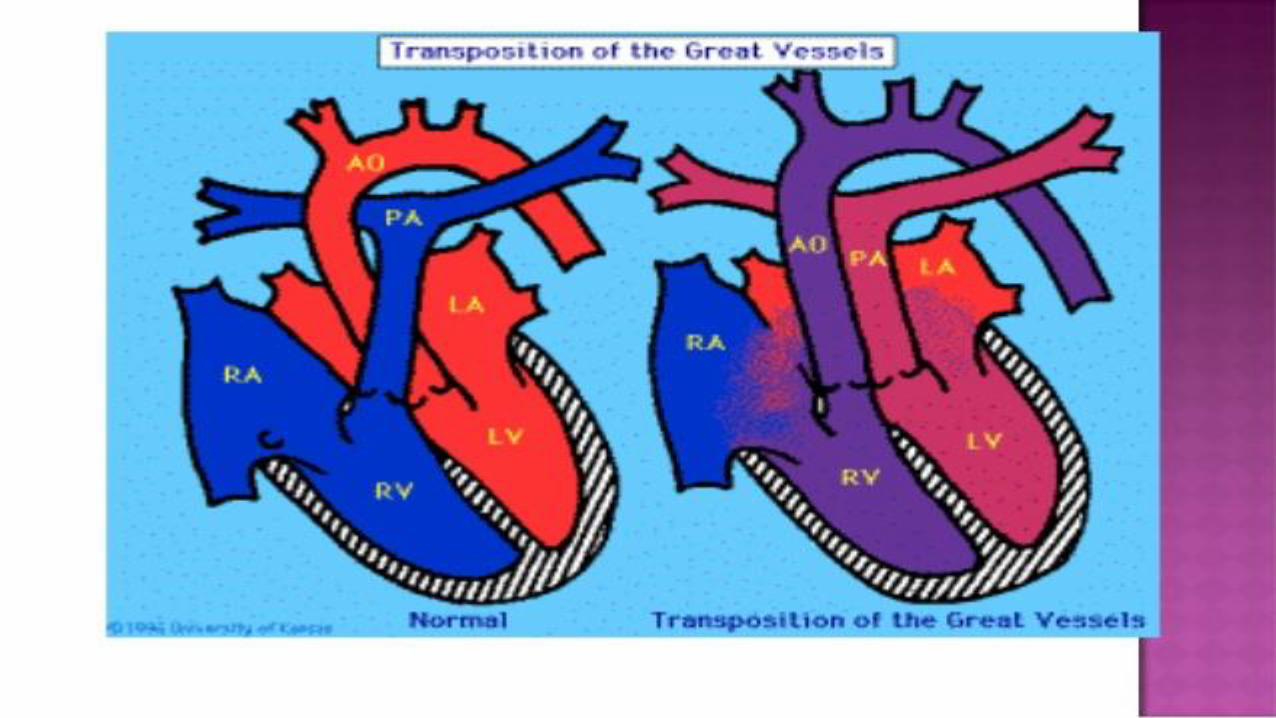
Transposition of Great Arteries (TGA)
•Description:
- Great vessels are switched that the aorta arises from the right ventricle
and the main pulmonary artery arises from the left ventricle causing
complete separation from the two circulation.
• Associated defects such as septal defect or PDA permit blood to enter the
systemic circulation and/or the pulmonary circulation for mixing of
saturation and desaturation blood.
Transposition of Great Arteries (TGA)
• The most common defect associated with TGA is a patent foramen ovale
• VSD (increase the incidence of HF, because it permits blood to flow from
the right to the left ventricle, into the pulmonary artery then to the lung)
Transposition of Great Arteries (TGA)
Transposition of Great Arteries (TGA)
Clinical manifestation:
- Depends on the type and size of the defect.
- Newborns with minimal defect are severely cyanotic and depressed at
birth.
- Children with large septal defect or a PDA may be less cyanotic but have
symptoms of HF
- Cardiomegaly is usually evident a few weeks after birth .
Transposition of Great Arteries (TGA)
• Therapeutic management:
- Prostaglandin (PGE1) IV may be given preoperatively to maintain potency
and ensure adequate systemic blood flow
- Anti-congestive measures –digoxin, diuretics, increased caloric density of formula and after loud reduction.
Transposition of Great Arteries (TGA)
• Pharmacologic treatment:
- Prostaglandin (PGE1) should be initiated to maintain potency of the PDA.
- Anti-congestive measures –digoxin, diuretics, increased caloric density of formula
• Surgical treatment:
- Cardiac catheterization and balloon atrial septostom
- Repair by 3 months of life.
- A definitive repair consists of switching the right/left structures.
- Arterial switch procedure
Transposition of Great Arteries (TGA)
• Pharmacologic treatment:
- Prostaglandin (PGE1) should be initiated to maintain potency of the PDA.
- Anti-congestive measures –digoxin, diuretics, increased caloric density of formula
• Surgical treatment:
- Cardiac catheterization and balloon atrial septostomy
- Repair by 3 months of life.
Transposition of Great Arteries (TGA)
•Surgical treatment:
- A definitive repair consists of switching the right/left structures.
- Arterial switch procedure
- Potential complications of the arterial switch include narrowing at the great artery anastomoses or coronary artery insufficiency.
Truncus Arteriosus (TA)
Truncus Arteriosus (TA)
https://www.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=1&ei=YTIgWoPxE8zOwAKitI-YCQ&q=Truncus+arteriosus&oq=Truncus+arteriosus&gs_l=
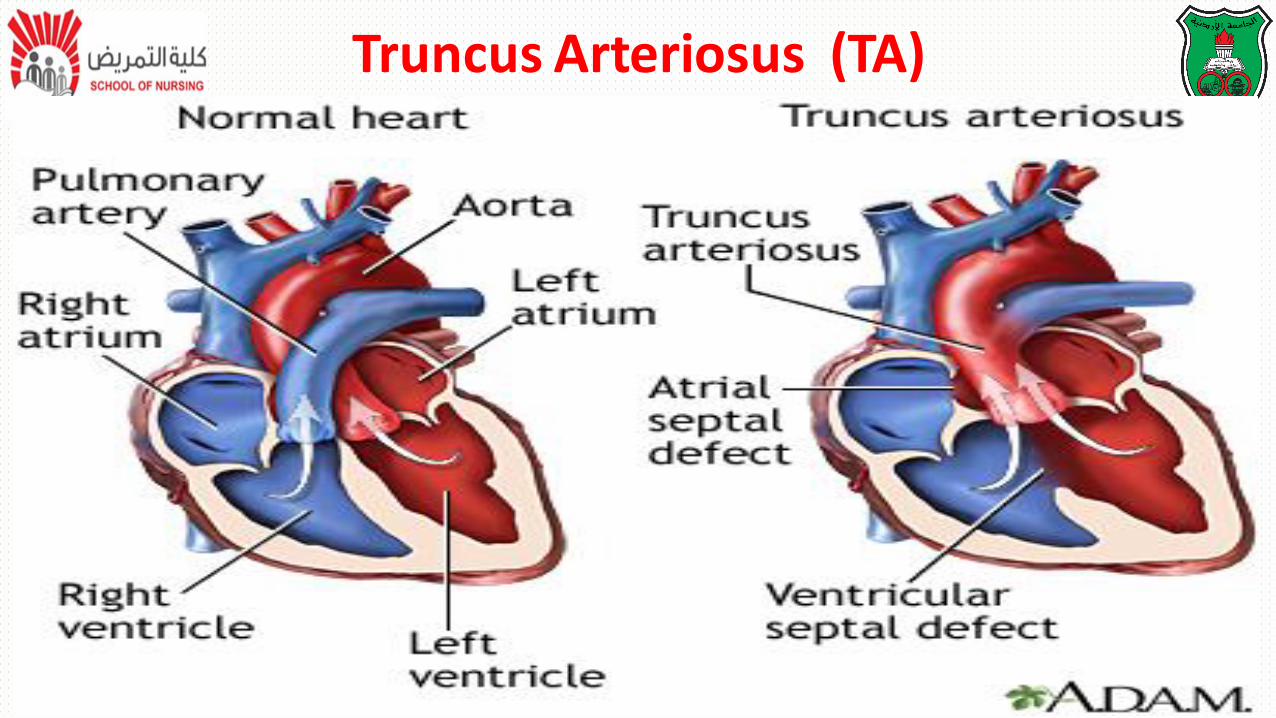
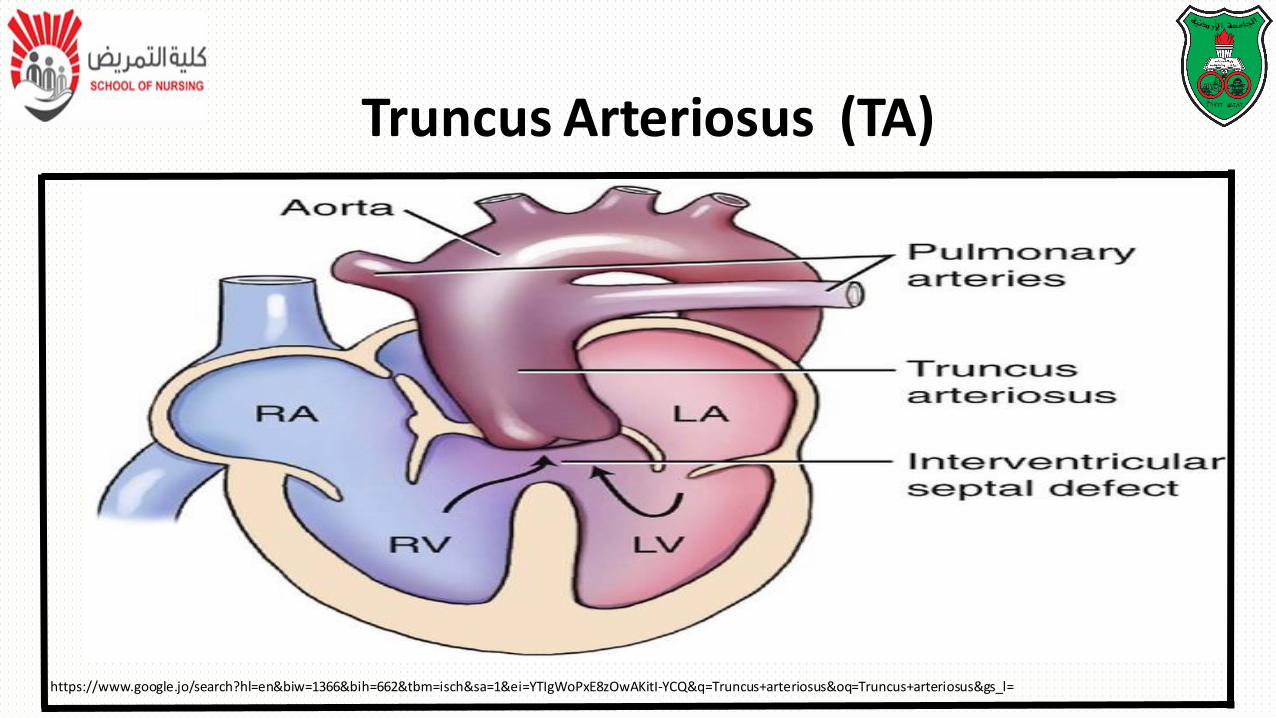
Truncus Arteriosus (TA)Descriptions:
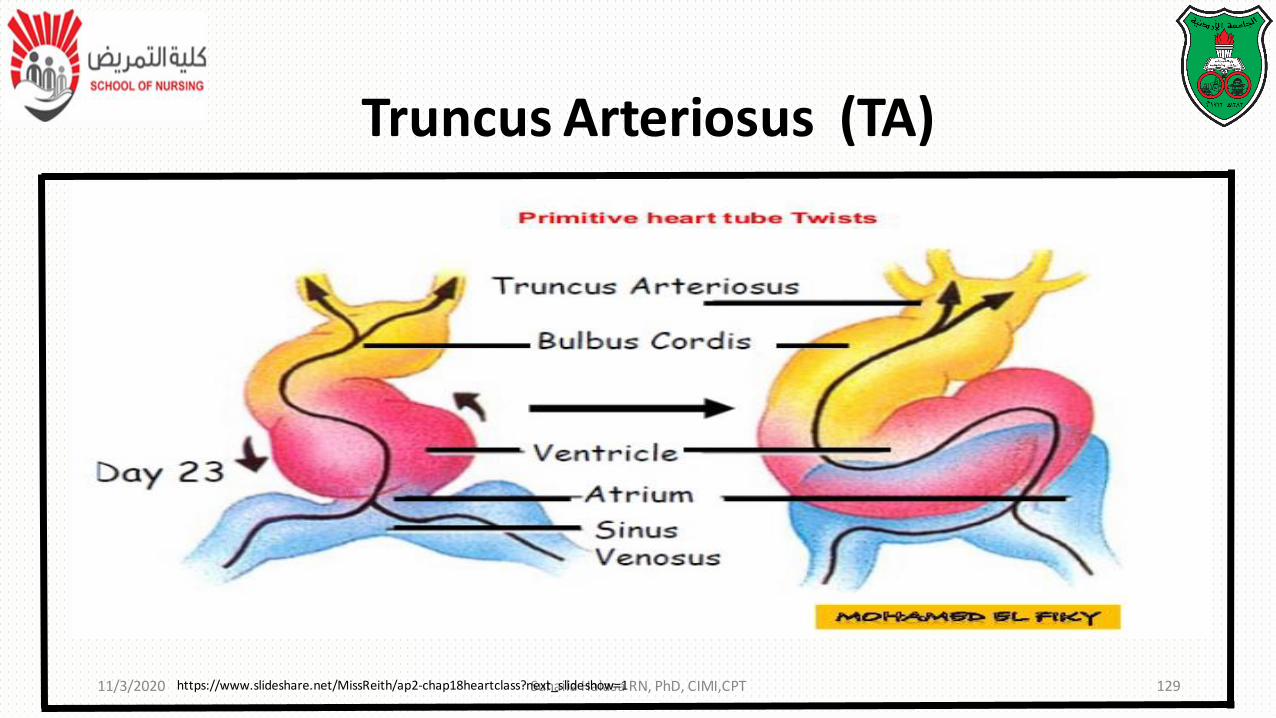
• Failure of normal separation and division of the embryonic bulbar trunk
into the pulmonary artery and aorta results in -----
- Development of a single vessel that overrides both ventricles
- Blood from both ventricles mixes in the common great artery, causing
desaturation and hypoxemia.
Truncus Arteriosus (TA)
11/3/2020 Suhaila Halasa RN, PhD, CIMI,CPT 129https://www.slideshare.net/MissReith/ap2-chap18heartclass?next_slideshow=1
Truncus Arteriosus (TA)
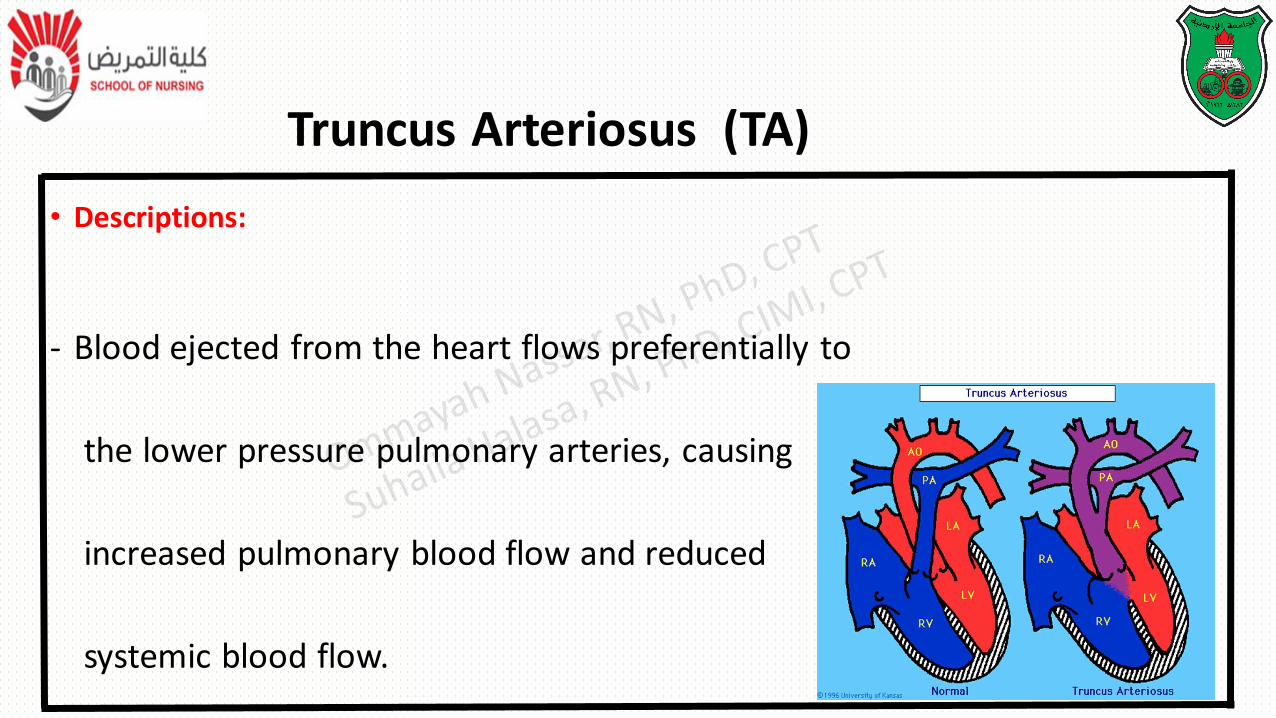
• Descriptions:
- Blood ejected from the heart flows preferentially to
the lower pressure pulmonary arteries, causing
increased pulmonary blood flow and reduced
systemic blood flow.
Truncus Arteriosus (TA)
• Descriptions:
- There are three types:
➢Type I: a single pulmonary trunk arises near the base of the truncus and divides into the left and right pulmonary arteries
➢Type II: the left and right pulmonary arteries arise separately but in close proximity and at the same level from the back of the truncus
➢Type III: the pulmonary arteries arise independently from the sides of the truncus.
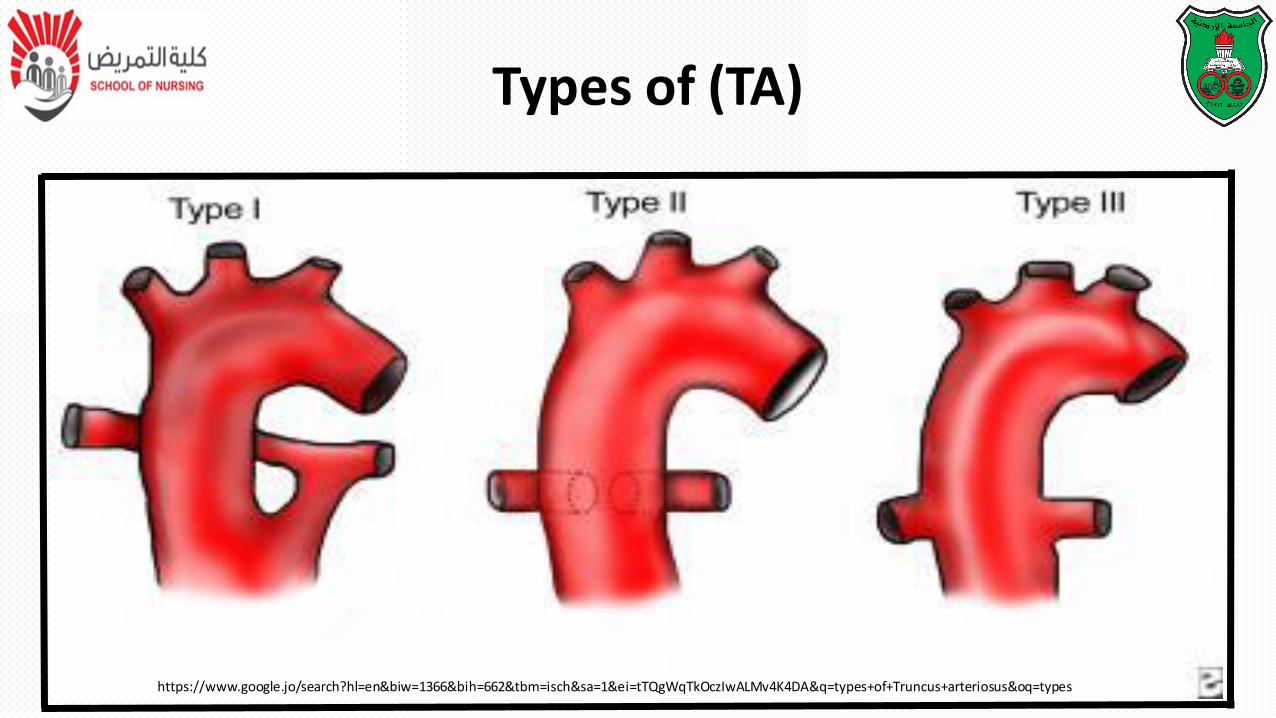
Types of (TA)
https://www.google.jo/search?hl=en&biw=1366&bih=662&tbm=isch&sa=1&ei=tTQgWqTkOczIwALMv4K4DA&q=types+of+Truncus+arteriosus&oq=types
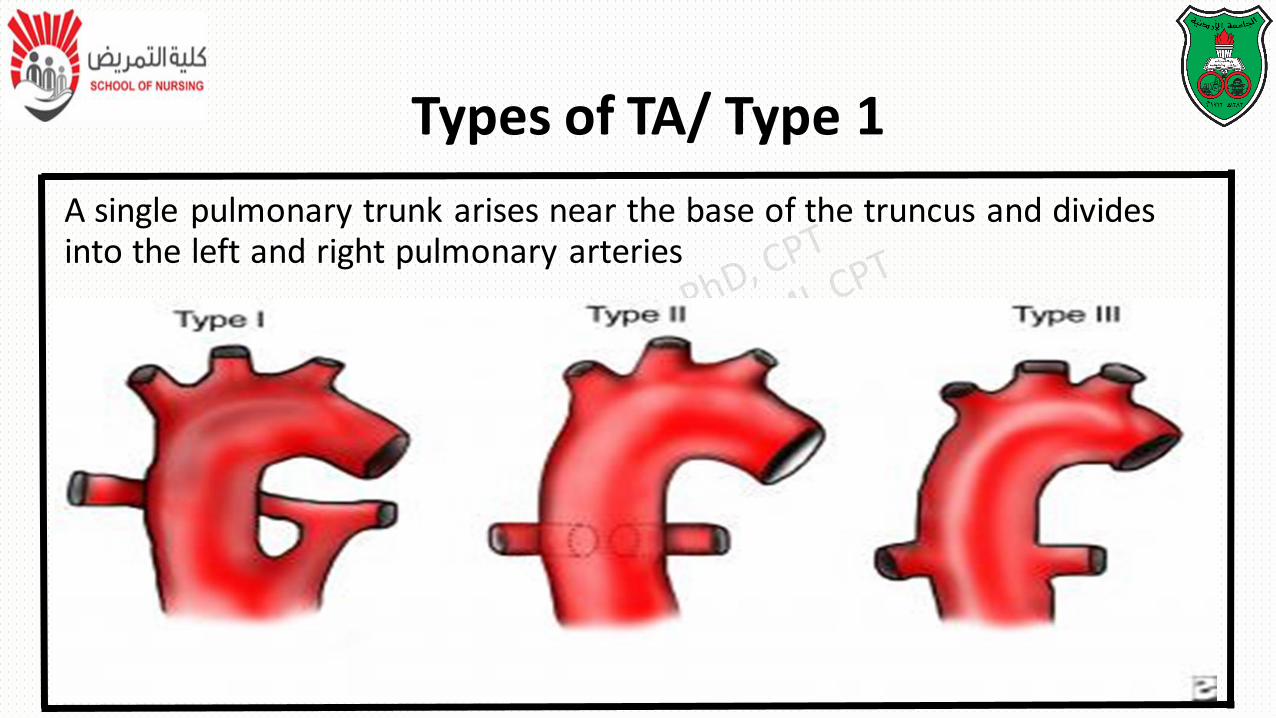
A single pulmonary trunk arises near the base of the truncus and divides into the left and right pulmonary arteries
Types of TA/ Type 1
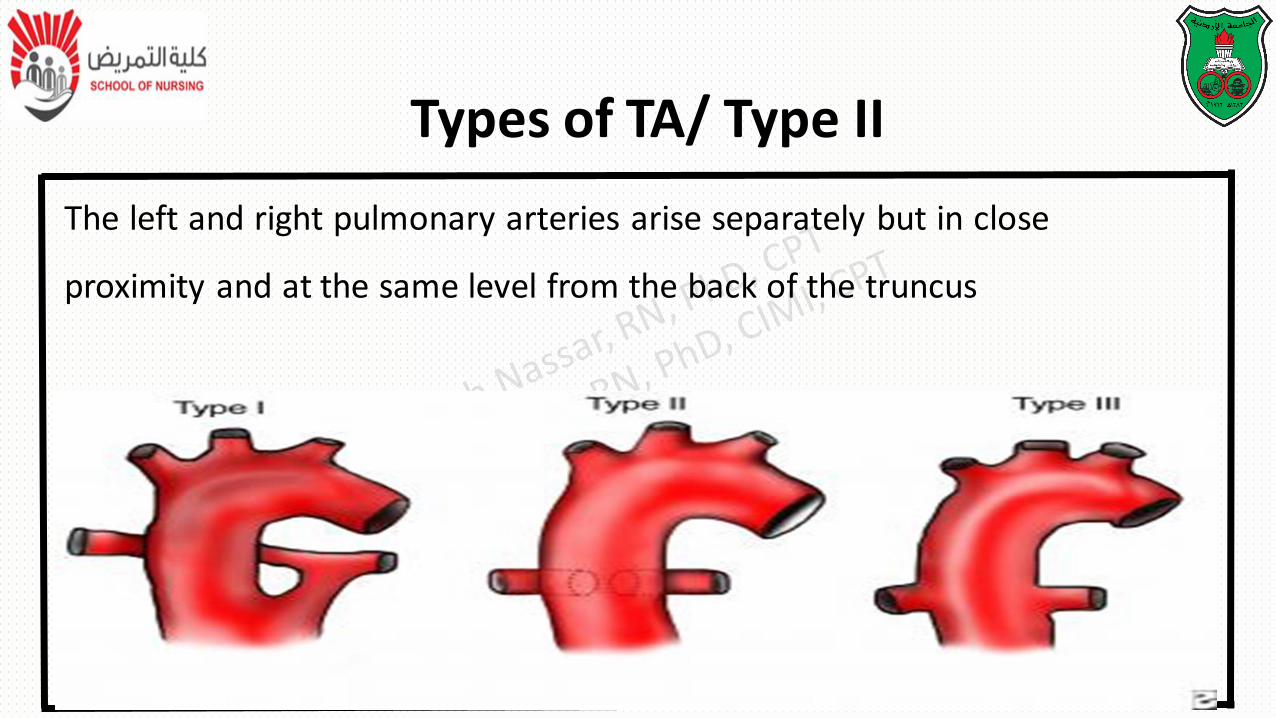
The left and right pulmonary arteries arise separately but in close
proximity and at the same level from the back of the truncus
Types of TA/ Type II
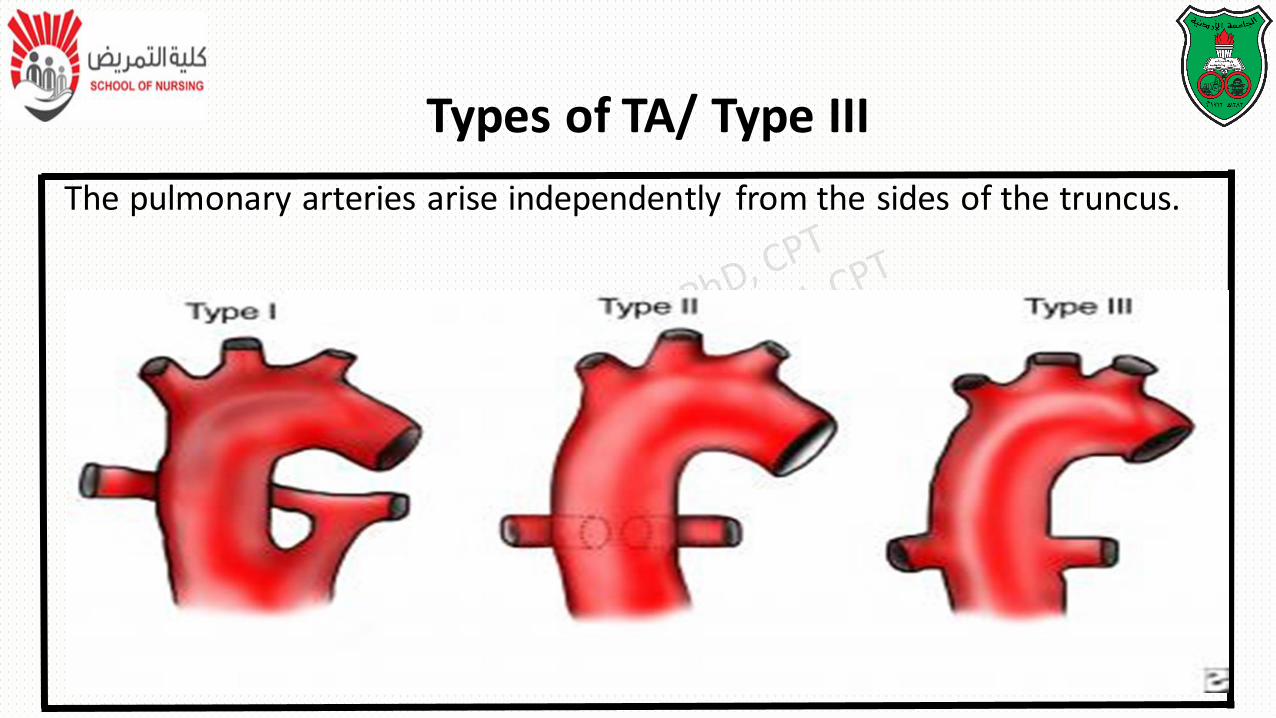
The pulmonary arteries arise independently from the sides of the truncus.
Types of TA/ Type III
Pathophysiology
• Blood ejected from the left and right ventricles enters the
common trunk, mixing pulmonary and systemic circulations.
• Blood flow is distributed to the pulmonary and systemic
circulations according to the relative resistances of each system.
Pathophysiology
• The amount of pulmonary blood flow depends on the size of the pulmonary
arteries and the pulmonary vascular resistance.
• The resistance to pulmonary blood flow is less than systemic vascular
resistance, resulting in better blood flow to the lungs.
• Pulmonary vascular disease develops at an early age in children with TA
Clinical Manifestations of TA
• Most infants are symptomatic with moderate to severe HF
• cyanosis
• poor growth
• activity intolerance.
• There is a characteristic murmur.
• Surgical treatment:
• Early repair in the first few month of life.
• It involves closing the VSD so that the TA receives the outflow from the
left ventricle, excising the pulmonary arteries from the aorta, and
attaching them to the right ventricle by means of a homograft
Therapeutic Management of TA
Truncus Arteriosus (TA)
• Postoperative complications:
• persistent heart failure, bleeding, pulmonary artery hypertension, dysrhythmias, and residual VSD.
• Prognosis:
- Mortality is greater than 10%
Assist in measures to improve cardiac function:
• Administering correct dose of digoxin, observing for signs of toxicity and
instituting parental teaching regarding drug administration at home
• Drug is not given if pulse rate below 90-110 beats /min in infant and
young children or below 70 in older children
Nursing Care Management
Decrease cardiac demand:
• Infants require rest and conservation of energy for feeding
• Organize nursing activities to allow for interrupting periods of sleep
• Minimize infant crying
• Small frequent meals every 3 hours
• Reduce unnecessary stress for older children by explanation of what
happening to reduce anxiety
Nursing Care Management
Reduce respiratory distress:
• Carful assessment, positioning and oxygen administration
• Respirations are counted for full one minute during a resting state
• Elevate the head of the bed
Nursing Care Management
• Sleep on several pillows or semi-Fowler or high Fowler position
• Provide humidified O2 by nasal cannula, hood or mask
• Protect the child from persons with respiratory infections
Nursing Care Management
• Maintain nutritional status
• Children metabolic rate is greater because of poor cardiac function and increased heart and
Respiratory rates
• They need more calories because they cant take adequate food due to fatigue
Nursing Care Management
•Assist in measure to promote fluid loss
•When diuretics are given
•Record intake and output
•Monitor weight
Nursing Care Management

• Support child and family
Nursing Care Management