cardiology/ekg board review - philadelphia college … • review general method for ekg...
TRANSCRIPT

Cardiology/EKGBoardReviewMichaelJ.BradleyD.O.DME/ProgramDirector
FamilyMedicineResidency

ObjecCves
• ReviewgeneralmethodforEKGinterpretaCon• Reviewspecificpointsof“datagathering”and“diagnoses”onEKG
• ReviewtreatmentconsideraCons• Reviewclinicalcases/EKG’s• BoardexamconsideraCons

EKG

EKG–12Leads
• AnteriorLeads-V1,V2,V3,V4• InferiorLeads–II,III,aVF• LeVLateralLeads–I,aVL,V5,V6• RightLeads–aVR,V1

11StepMethodforReadingEKG’s
• “DataGathering”–steps1-4– 1.StandardizaCon–makesurepaperandpaperspeedisstandardized
– 2.HeartRate– 3.Intervals–PR,QT,QRSwidth– 4.Axis–normalvs.deviaCon

11StepMethodforReadingEKG’s
• “Diagnoses”– 5.Rhythm– 6.Atrioventricular(AV)BlockDisturbances– 7.BundleBranchBlockorHemiblock of– 8.PreexcitaCon ConducCon– 9.EnlargementandHypertrophy– 10.CoronaryArteryDisease– 11.UgerConfusion
• TheOnlyEKGBookYou’llEverNeedMalcolmS.Thaler,MD

HeartRate
• RegularRhythms

HeartRate
• IrregularRhythms

Intervals
• MeasurelengthofPRinterval,QTinterval,widthofPwave,QRScomplex

QTc
• QTc=QTintervalcorrectedforheartrate– UsesBazeg’sFormulaorFridericia’sFormula
• LongQTsyndrome–inheritedoracquired(>75meds);torsadesdeponites/VF;syncope,seizures,suddendeath

Axis

Rhythm
• 4QuesCons– 1.ArenormalPwavespresent?– 2.AreQRScomplexesnarroworwide(≤or≥0.12)?– 3.WhatisrelaConshipbetweenPwavesandQRS
complexes?– 4.Isrhythmregularorirregular?
• Sinusrhythm=normalPwaves,narrowQRScomplexes,1Pwavetoevery1QRScomplex,andregularrhythm

TypesofArrhythmias
• Arrhythmiasofsinusorigin• Ectopicrhythms• ConducConBlocks• PreexcitaConsyndromes

AVBlock• DiagnosedbyexaminingrelaConshipofPwavestoQRS
complexes• FirstDegree–PRinterval>0.2seconds;allbeats
conductedthroughtotheventricles• SecondDegree–onlysomebeatsareconductedthrough
totheventricles– MobitzTypeI(Wenckebach)–progressiveprolongaConofPRintervalunClaQRSisdropped
– MobitzTypeII–All-or-nothingconducConinwhichQRScomplexesaredroppedwithoutPRintervalprolongaCon
• ThirdDegree–Nobeatsareconductedthroughtotheventricles;completeheartblockwithAVdissociaCon;atriaandventriclesaredrivenbyindividualpacemakers


BundleBranchBlocks
• DiagnosedbylookingatwidthandconfiguraConofQRScomplexes

BundleBranchBlocks
• RBBBcriteria:– 1.QRScomplex>0.12seconds– 2.RSR’inleadsV1andV2(rabbitears)withSTsegmentdepression
andTwaveinversion– 3.ReciprocalchangesinleadsV5,V6,I,andaVL
• LBBBcriteria:– 1.QRScomplex>0.12seconds– 2.BroadornotchedRwavewithprolongedupstrokeinleadsV5,V6,I,
andaVLwithSTsegmentdepressionandTwaveinversion.– 3.ReciprocalchangesinleadsV1andV2.– 4.LeVaxisdeviaConmaybepresent.

BundleBranchBlocks

Hemiblocks
• DiagnosedbylookingatrightorleVaxisdeviaCon
• LeVAnteriorHemiblock– 1.NormalQRSduraConandnoSTsegmentorTwavechanges– 2.LeVaxisdeviaCongreaterthan-30°– 3.NoothercauseofleVaxisdeviaConispresent
• LeVPosteriorHemiblock– 1.NormalQRSduraConandnoSTsegmentorTwavechanges– 2.RightaxisdeviaCon– 3.NoothercauseofrightaxisdeviaConispresent

BifascicularBlock
• RBBBwithLAH– RBBB–QRS>0.12secandRSR’inV1andV2withLAH–leVaxisdeviaCon
• RBBBwithLPH– RBBB–RS>0.12secandRSR’inV1andV2withLPH–rightaxisdeviaCon

PreexcitaCon• Wolff-Parkinson-White(WPW)Syndrome
– 1.PRinterval<0.12sec– 2.WideQRScomplexes– 3.Deltawavesseeninsomeleads
• Lown-Ganong-Levine(LGL)Syndrome–– 1.PRinterval<0.12sec– 2.NormalQRSwidth– 3.Nodeltawave
• CommonArrhythmias– ParoxysmalSupraventricularTachycardia(PSVT)–narrowQRS’saremorecommonthanwideQRS’s
– AtrialFibrillaCon–canberapidandleadtoventricularfibrillaCon

PreexcitaCon
WPW LGL

SupraventricularArrhythmias• PSVT-regular;Pwavesretrogradeifvisible;rate150-250bpm;
caroCdmassage:slowsorterminates• Fluger–regular;saw-toothedpagern;2:1,3:1,4:1,etc.block;
atrialrate250-350bpm;ventricularrate½,⅓,¼,etc.ofatrialrate;caroCdmassage:increasesblock
• FibrillaCon–irregular;undulaCngbaseline;atrialrate350to500bpm;variableventricularrate;caroCdmassage:mayslowventricularrate
• MulCfocalatrialtachycardia(MAT)–irregular;atleast3differentPwavemorphologies;rate–usually100to200bpm;someCmes<100bpm;caroCdmassage:noeffect
• PAT–regular;100to200bpm;characterisCcwarm-upperiodintheautomaCcform;caroCdmassage:noeffect,ormildslowing

SupraventricularArrhythmias

RulesofAberrancyVentricularTachycardia Paroxysmal
supraventricularTachycardia
ClinicalCluesClinicalHistory Diseasedheart Usuallynormalheart
CaroCdMassage Noresponse Mayterminate
CannonAWaves Maybepresent Notseen
EKGCluesAVDissociaCon Maybeseen Notseen
Regularity Slightlyirregular Veryregular
FusionBeats Maybeseen Notseen
IniCalQRSdeflecCon MaydifferfromnormalQRScomplex
SameasnormalQRScomplex

VentricularArrhythmias
TorsadesdePointes
PVC’s

AtrialEnlargement• LookatPwavesinleadsIIandV1• Rightatrialenlargement(Ppulmonale)– 1.IncreasedamplitudeinfirstporConofPwave– 2.NochangeinduraConofPwave– 3.PossiblerightaxisdeviaConofPwave
• LeVatrialenlargement(pmitrale)– 1.Occasionally,increasedamplitudeofterminalpartofPwave
– 2.Moreconsistently,increasedPwaveduraCon– 3.NosignificantaxisdeviaCon

VentricularHypertrophy• LookattheQRScomplexesinallleads• Rightventricularhypertrophy(RVH)
– 1.RAD>100°– 2.RaCoofRwaveamplitudetoSwaveamplitude>1inV1and<1inV6
• LeVventricularhypertrophy(LVH)
PrecordialCriteria LimbLeadCriteriaRwaveinV5orV6+SwaveinV1orV2>35mm
RwaveinaVL>13mm
RwaveinV5>26mm RwaveinaVF>21mm
RwaveinV6>18mm RwaveinI>14mm
RwaveinV6>RwaveinV5
RwaveinI+SwaveinIII>25mm

MyocardialInfarcCon
• Dx–Hx,PE,serialcardiacenzymes,serialEKG’s
• 3EKGstagesofacuteMI– 1.Twavepeaksandtheninverts– 2.STsegmentelevates– 3.Qwavesappear

QWaves
• CriteriaforsignificantQwaves– Qwave>0.04secondsinduraCon– Qwavedepth>⅓heightofRwaveinsameQRScomplex
• CriteriaforNon-QWaveMI– Twaveinversion– STsegmentdepressionpersisCng>48hoursinappropriateclinicalse{ng

LocalizingMIonEKG• InferiorinfarcCon–leadsII,III,aVF
– OVencausedbyocclusionofrightcoronaryarteryoritsdescendingbranch
– ReciprocalchangesinanteriorandleVlateralleads• LateralinfarcCon–leadsI,aVL,V5,V6
– OVencausedbyocclusionofleVcircumflexartery– Reciprocalchangesininferiorleads
• AnteriorinfarcCon–anyoftheprecordialleads(V1-V6)– OVencausedbyocclusionofleVanteriordescendingartery– Reciprocalchangesininferiorleads
• PosteriorinfarcCon–reciprocalchangesinleadV1(STsegmentdepression,tallRwave)– OVencausedbyocclusionofrightcoronaryartery

LocalizingMIonEKG

STsegment• ElevaCon– SeenwithevolvinginfarcCon,Prinzmetal’sangina– Othercauses–JpointelevaCon,apicalballooningsyndrome,acutepericardiCs,acutemyocardiCs,hyperkalemia,pulmonaryembolism,Brugadasyndrome,hypothermia
• Depression– SeenwithtypicalexerConalangina,non-QwaveMI– Indicatorof+stresstest

ElectrolyteAbnormaliCesonEKG
• Hyperkalemia–peakedTwaves,prolongedPR,flagenedPwaves,widenedQRS,mergingQRSwithTwavesintosinewave,VF
• Hypokalemia–STdepression,flagenedTwaves,Uwaves
• Hypocalcemia–prolongedQTinterval• Hypercalcemia–shortenedQTinterval

Drugs• Digitalis– TherapeuCclevels–STsegmentandTwavechangesinleadswithtallRwaves
– Toxiclevels–tachyarrhythmiasandconducConblocks;PATwithblockismostcharacterisCc.
• MulCpledrugsassociatedwithprolongedQTinterval,Uwaves– Sotalol,quinidine,procainamide,disopyramide,amiodarone,dofeClide,dronedarone,TCA’s,erythromycin,quinolones,phenothiazines,variousanCfungals,someanChistamines,citalopram(onlyprolongedQTinterval–dose-dependent)

EKG∆’sinotherCardiacCondiCons• PericardiCs–DiffuseSTsegmentelevaConsandTwaveinversions;largeeffusionmaycauselowvoltageandelectricalalternans(alteringQRSamplitudeoraxisandwanderingbaseline)
• MyocardiCs–conducConblocks• HypertrophicCardiomyopathy–ventricularhypertrophy,leVaxisdeviaCon,septalQwaves

EKG∆’sinPulmonaryDisorders
• COPD–lowvoltage,rightaxisdeviaCon,andpoorRwaveprogression.
• Chroniccorpulmonale–PpulmonalewithrightventricularhypertrophyandrepolarizaConabnormaliCes
• Acutepulmonaryembolism–rightventricularhypertrophywithstrain,RBBB,andS1Q3T3(withTwaveinversion).SinustachycardiaandatrialfibrillaConarecommon.

EKG∆’sinOtherCondiCons• Hypothermia–Osbornwaves,prolongedintervals,sinusbradycardia,slowatrialfibrillaCon,bewareofmuscletremorarCfact
• CNSDisease–diffuseTwaveinversionwithTwaveswideanddeep,Uwaves
• Athlete’sHeart–sinusbradycardia,nonspecificSTsegmentandTwavechanges,RVH,LVH,incompleteRBBB,firstdegreeorWenckebachAVblock,possiblesupraventriculararrhythmia

UgerConfusion
• Verifyleadplacement• RepeatEKG• RepeatstandardizedprocessofEKGanalysis-starCngoverfromthebeginningwithbasics–rate,intervals,axis,rhythm,etc.andproceedthroughenCrestepwiseanalysis
• ConsiderCardiologyconsultaCon

ArrhythmiaIndicaConstoConsultCardiology
• DiagnosCcormanagementuncertainty• MedicaConsnotcontrollingsymptoms• PaCentisinhigh-riskoccupaConorparCcipatesinhigh-riskacCviCes(pilot,scubadriving)
• PaCentsprefersintervenConoverlong-termmeds• PreexcitaCon• Underlyingstructuralheartdisease• Associatedsyncopeorothersignificantsymptoms• WideQRS

CareConsideraConsPriortoCardiologyConsult
• ThoroughHxandPE• Basiclabs• EKGandrepeatEKG• Holtermonitor• Echocardiogram• Acuityofcarerequired–considerrisks,hemodynamicstability

PacemakerConsideraCons
• Third-degree(complete)AVblock• SymptomaCclesserdegreeAVblockorbradycardia
• SuddenonsetofvariouscombinaConsofAVblockandBBBduringacuteMI
• Recurrenttachycardiasthatcanbeoverdrivenandterminatedbypacemakers

OsteopathicConsideraCons
• Treatments–– LymphaCcs–thoracicinlet,abdominaldiaphragm,ribraising,lymphaCcpumps
– SympatheCcs(T1-T6)–cervicalganglion,ribraising,T1-T6,Chapman’sreflexes,T10-L2foradrenal/kidney
– ParasympatheCcs–OA/AA/cranial–vagusnerve

ClinicalCases/EKG’s

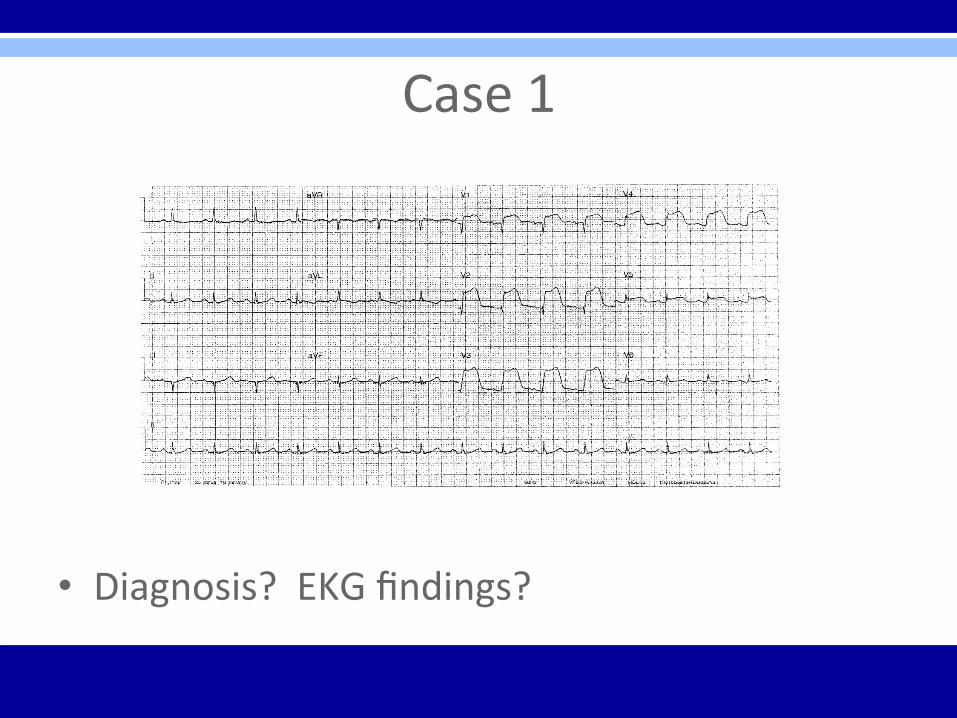
Case1• 53yearoldcaucasianfemalewith4dayhxofseverecentralchestpainonexerCon,previouslyalleviatedwithrest;nowworsenedoverlast24hoursandsustainedatrest
• PMHx–DM2,HTN,hyperlipidemia• Appearsunwell,inpain,sweaty,andgrey
Case1
• Diagnosis?EKGfindings?

Case1
• AcuteanteriorST-elevaConMIwith“tombstone”or“fireman’shat”inV1-V4
• Tx?LocalizaCon?

Case1• PCIstenCngofLAD
• Post-procedure=resolvingSTelevaCon;lossofominoustombstoneeffect;Qwavesdeveloping

Case2
• 45yomalepresentswithacuteSOBs/plongvacaConinParis
• PMHx-asthma,Crohn’sdisease,anxiety,GERD,tobaccoabuse
• VS37,148/92,130,26• PaCentappearsuncomfortablebutotherwiseunremarkableexam

Case2
• Diagnosis?EKGfindings?

Case2
• AcutePEwithsinustachycardia,aPVC,andS1Q3T3pagern

Case3
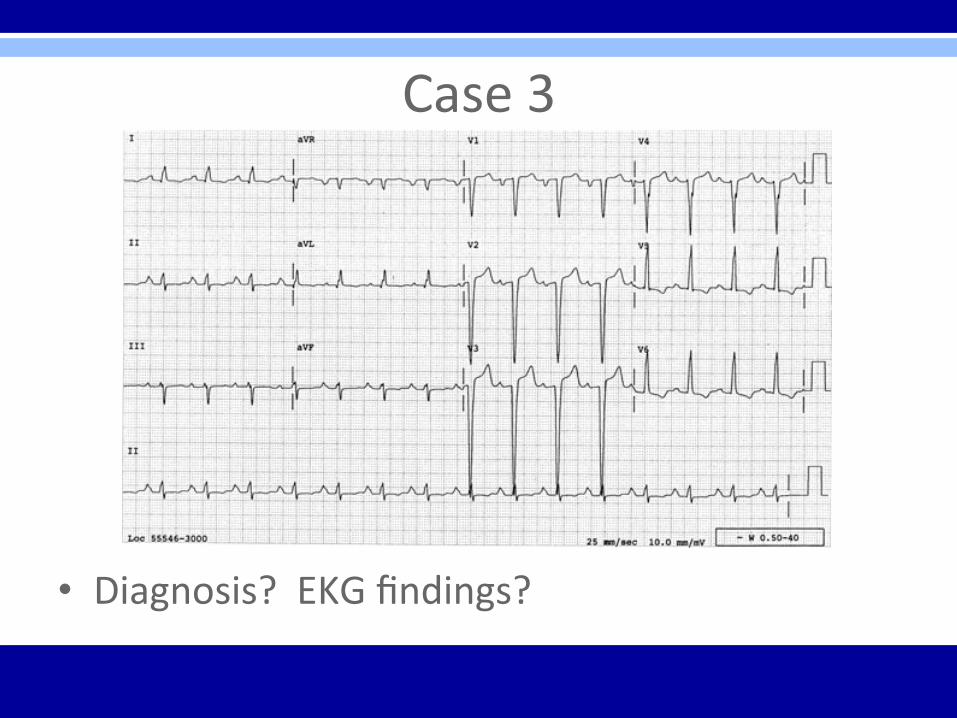
• 72yomalepresentstotheofficeforevaluaConpriortocataractsurgery
• Nocomplaints• PMHx–B/Lcataracts,OA,HTN,hyperlipidemia,andchroniclowbackpain
• VS37.2,152/86,74,14
Case3
• Diagnosis?EKGfindings?

Case3
• LVH–QRSvoltagecriteriainprecordialleadsandrepolarizaConchangesinV5,V6

Case4
• 27yofemalepresentstotheEDwithc/ochestdiscomfortandpalpitaConsaVerstudyingallnightforgraduateschoolexams
• Appearsnervousand“uneasy”withrapidpulse
• PMHx–unremarkable;nomeds,admitstooccasionalalcohol,non-smoker,deniesillicitdruguse,usedcoffeetostayawaketostudy

Case4
• Diagnosis?EKGfindings?

Case4
• SVT–regular,narrow-QRStachycardia,rateof160bpm

Case5
• 46yomalepresentstoEDwithc/osevereHApersisCngover5hoursdespiteacetaminophenandNSAIDagemptsasaborCvetherapy
• PMHx–occasionalleVshoulderpain,non-smoker
• ConstrucConworker• VSS;unremarkableexam

Case5
• Diagnosis?EKGfindings?

Case5
• NormalEKG

Case6
• 56yofemalepresentstofamilyphysicianwithc/olight-headednessandoccasionalflugerinherchest
• PMHx–anxiety,depression,obesity,smoker• Worksasretailstoremanager• VSS;coursebreathsounds,otherwiseunremarkableexam

Case6
• Diagnosis?EKGfindings?

Case6
• SeconddegreeAVblock–MobitzTypeI–Wenckebach(specifically3:2AVWenckebachphenomenonwhereevery3rdPwaveisblocked)

Case7
• 28yomalepresentsforcommercialdriver’slicense(CDL)evaluaCon
• Nocomplaints• VSS;asymptomaCc;examwithoutsignificantfindings

Case7
• Diagnosis?EKGfindings?

Case7
• TypicalpreexcitaCon(WPW)pagern• ShortPRintervalanddeltawavesinmanyleads
• TxiscloseobservaConunlesspaCenthashadSVToratrialfibrillaConwhichindicatestxwithablaConofaccessorypathway

Case8
• 32yomalepresentstoEDwithc/ofeelingsickforthelast6days
• Symptomsincludefevers,cough,anddifficultycatchinghisbreath
• PMHx–hyperlipidemia,obesity,metabolicsyndrome
• VS38.1,105,128/84,22

Case8
• Diagnosis?EKGfindings?

Case8
• AcutepericardiCs–diffuseSTelevaConwithPRsegmentdepressionisdiagnosCc

Case9
• 67yomalepresentstohiscardiologistforout-paCent6weekpost-hospitalvisit
• PrevioushospitalizaConfornon-cardiacchestpain
• Post-hospitalcardiacmeds–ACEinhibitor,betablocker,aspirin,nitrate
• Nocurrentcomplaints

Case9
• Diagnosis?EKGfindings?
Case9
• AtrialfibrillaCon–irregularlyirregularwithoutPwaves
• RBBB–wideQRSwithrsR’pagerninV1,broadSwavesinleadsIandaVL
• Inferiorinfarct–non-acute(>1week)pathologicQwavesininferiorleads(II,III,andaVF)
Case10
• 79yomalebroughttoEDviaEMSwithchestpain,SOB,andnear-syncope
• PMHx–unobtainablesecondarytopaCentdistress
• VS–36.9,140’s,82/40,28

Case10
• Diagnosis?EKGfindings?

Case10
• Monomorphicsustainedventriculartachycardia(VT)–couldrapidlydeteriorateintoVF,torsadesdepointes,asystole,orsuddendeath

Case11
• 82yofemaleadmigedtoacutecarehospitalsecondarytochestpain
• PMHx–HTN,DM2,CHF,obesity,depression• CardiologyplanningcardiaccatheterizaConsecondarytonewfindingduringiniCalconsultaCon

Case11
• Diagnosis?EKGfindings?

Case11
• LBBB–wideQRS;broad,notchedRwaveinV5,V6andIwithSTdepressionandTwaveinversion

Case12
• 59yomalepresentstoEDdiaphoreCcandindistress
• PMHx–HTN,ESRD,DM2,LeVBKA• VS–37.5,108,96/58,24

Case12
• Diagnosis?EKGfindings?

Case12
• Hyperkalemia–tallpeakedTwavespresentthroughout;otherprogressiveEKGchangesmayfollowwithincreasingpotassiumlevels–prolongedPRinterval,flagenedPwaves,wideningQRS,sinewaves
• Sinustachycardiaalsopresent

BonusCase
• 18yomaleundergoingmilitaryphysicalexamandevaluaConpriortobootcamp
• Nocomplaints• PMHx–denies• VSS;examunremarkable

BonusCase
• Diagnosis?EKGfindings?

BonusCase
• Reversedarmleads–invertedPwavesinleadIwithnormalRwaveprogressioninprecordialleads

BoardExamPoints
• EKG’slikelytohave1mainfinding• ClinicalcaselikelyincludedwitheachEKG• QuesConlikelytofocusonclinicalcaseaswellasEKG
• Straightforwardwithouttricksorobscurefindings(notlikelytosee“zebras”)
• Focusoncommonarrhythmias,commoncardiacdiagnoses,commonnon-cardiacEKGabnormaliCes,oremergent“can’tmiss”diagnoses

QuesCons?

Resources• SourcesandSuggestedReferences– TheOnlyEKGBookYou’llEverNeed-MalcolmS.Thaler– RapidInterpretaConofEKG’s–DaleDubin,M.D.– “…ExceptforOMT!”–DalePrag-Harrington– AmericanFamilyPhysician–November1,2015– UptoDate– blogatwordpress.com– cme.umn.edu– ekgcasestudies.com– healio.com– lifeinthefastlane.com– learntheheart.com