cardiopulmonary exercise testing interactive case … · cardiopulmonary exercise testing –...
TRANSCRIPT

CARDIOPULMONARY EXERCISE TESTING –INTERACTIVE CASE DISCUSSION
The Cardiologist’s point of viewLukas Trachsel

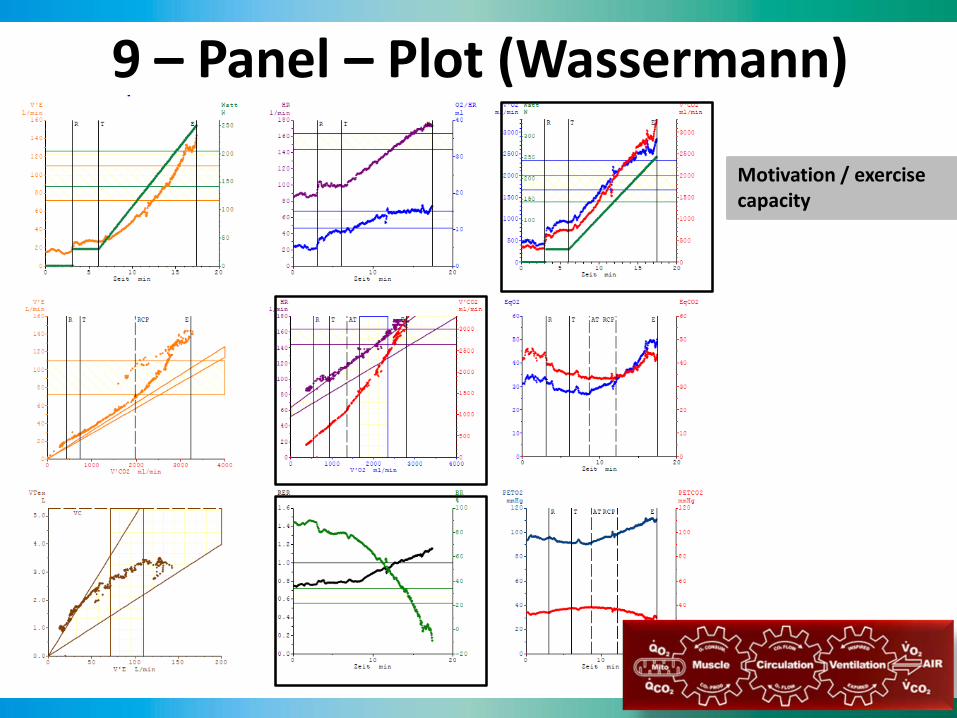
9 – Panel – Plot (Wassermann)
9 – Panel – Plot (Wassermann)
Motivation / exercisecapacity

9 – Panel – Plot (Wassermann)
Motivation / exercisecapacity
Ventilatory mechanicalrelevant panels

Oxygen uptake in response to acute exercise
COCardiacoutput
SVStrokevolume
HRHeart rate
Wassermann, Principles of Exercise Testing, 5th Edition
Perip.Circ.Dilate
Recruit
Pulm.Circ.RecruitDilate
C(a-v)o2Arterial-mixedvenous O2 diff. x10x2-3
VO2 = CO x C(a-v) O2
‘Fick equation’

9 – Panel – Plot (Wassermann)
Motivation / exercisecapacity
Ventilatory mechanicalrelevant panels
Cardio-circulatoryrelevant panels
VO2 = SV x HR x C(a-v) O2
VO2/HR = SV x C(a-v) O2
VO2/WR-Slope

9 – Panel – Plot (Wassermann)
Cooperation / exercisecapacity
Ventilatory mechanicalrelevant panels
Cardio-circulatoryrelevant panels
Gas exchange

Case Report• 61 year old male• 3-vessel CAD (12/2010)
– Non-STE-MI inferior 12/2010– CABG 12/2010 – Ejection fraction normal– Risk factors: cholesterol, BMI 30, familial history, former
smoker
• Suspected exercise induced asthma 07/2012– Body plethysmography 20.7.2012: borderline restriction
(TLC 76% predicted), dynamic lung volume normal, C0 diffusion capacity normal
• Annual ‘follow-up’: – Exercise intolerance for months, exertional dyspnoe
(NYHA II)

Spirometry

CAD, post-CABGExercise intolerance, NYHA II

CAD, post-CABGExercise intolerance, NYHA II

CAD, post-CABGExercise intolerance, NYHA II
VE/VCO2-Slope 35 (<30)
RER 1.15
BR 20%
VO2/WR-Slope 8.2 (> 8.6) O2 pulse 77% pred
CRF 77% pred
WR 76% pred

QUIZ QUESTION:
What is the most likely reason for the symptoms and for the reduced exercise capacity/CRF?
a) Respiratory limitationb) Cardio-circulatory limitation (unspecific)c) Cardio-circulatory limitation (suggestive ofischemia)d) Limitation of peripheral musclese) Others

CAD, post-CABGExercise intolerance, NYHA II
VO2/WR-Slope 8.2 (> 8.6) O2 pulse 77% pred
BR 20%
RER 1.15
CRF 77% pred
WR 76% pred
VE/VCO2-Slope 35 (<30)

PCI LAD distal LIMA-RIVA graft 15.09.2014

CAD, post-CABGSymptoms resolved
09.09.14Before PCI
23.09.14After PCI
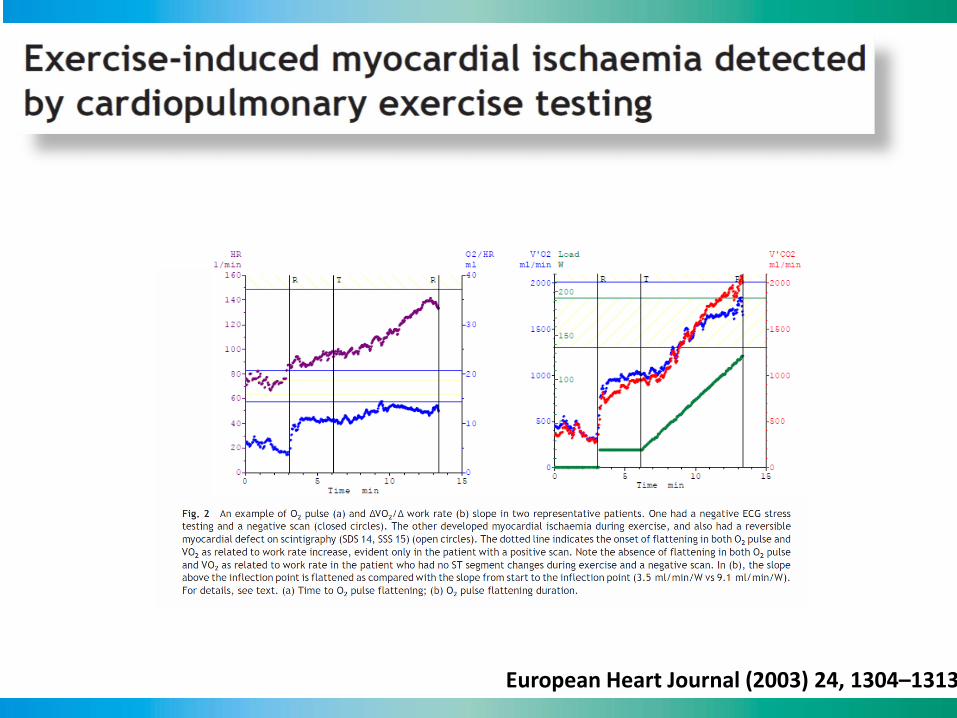
European Heart Journal (2003) 24, 1304–1313

European Heart Journal (2003) 24, 1304–1313

European Heart Journal (2003) 24, 1304–1313Int J Cardiol 174 (2014) 337–342
Case Report• 53 year old male
• Hypertensive heart disease
• Metabolic syndrome
• Syncope 2012
• Sent for disability evaluation by the insurance(‘IV-Abklärung’)
• Symptoms: dyspnoe on exertion (NYHA II-III), periodic chest pain (at rest, on exertion)

Spirometry

Hypertensive HD, metabolic syndromeNYHA II-III

Hypertensive HD, metabolic syndromeNYHA II-III

Hypertensive HD, metabolic syndromeNYHA II-III VO2/WR-Slope 8.9 (> 8.6)
O2 pulse 59% predVE/VCO2-Slope 38(<30)
CRF 64% pred
WR 54% pred
RER 1.29
BR 16%

QUIZ QUESTION:
What is the most unlikely reason for the reduced exercise capacity?
a) Heart failure with preserved ejection fractionb) Subacute pulmonary embolismc) Chronic thrombo-embolic pulmonary hypertension (CTEPH)d) Previously undetected aortic stenosise) COPD

RER 1.29
Hypertensive HD, metabolic syndromeNYHA II-III
VE/VCO2-Slope 38 (<30)
VO2/WR-Slope 8.9 (> 8.6)
PET Co2 32mm Hg(Rest: > 35mm Hg)
bath tub?
O2 pulse 59% pred
CRF 64% pred
WR 54% pred
BR 16%
RER 1.29

Ventilation-/Perfusion-Szintigraphy
Subsegmentary bilateral pulmonary emboli

Heart. 2007 Oct;93(10):1285-92.

European Heart Journal (2012) 33, 2917–2927
“Several CPX statements have been published by well-respected organizations in both the US and Europe. Despite these prominent reports and the plethora of pertinent medical literature
which they feature, underutilization of CPX persists.”

• New CPX indications and algorithms:
– CPX to assess perisurgical and postsurgical risk and long-term prognosis
– CPX to assess valvular disease/dysfunction
European Heart Journal doi:10.1093/eurheartj/ehw180
www.myswitzerland.com
Thank you!