cardiovascular complications of cancer therapylar complications of cancer therapy. this topic was...
TRANSCRIPT
Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 7 0 , N O . 2 0 , 2 0 1 7
ª 2 0 1 7 B Y T H E A M E R I C A N CO L L E G E O F C A R D I O L O G Y F O U N DA T I O N
P U B L I S H E D B Y E L S E V I E R
I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
h t t p s : / / d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 7 . 0 9 . 1 0 9 6
FOCUS SEMINAR: CARDIO-ONCOLOGY
STATE-OF-THE-ART REVIEW
Cardiovascular Complications ofCancer TherapyBest Practices in Diagnosis, Prevention, and Management: Part 1
Hui-Ming Chang, MD, MPH,a Rohit Moudgil, MD, PHD,b Tiziano Scarabelli, MD, PHD,c Tochukwu M. Okwuosa, DO,d
Edward T.H. Yeh, MDa
ABSTRACT
Fro
Ca
Un
rec
Mi
to
Ma
Modern cancer therapy has successfully cured many cancers and converted a terminal illness into a chronic disease.
Because cancer patients often have coexisting heart diseases, expert advice from cardiologists will improve clinical
outcome. In addition, cancer therapy can also cause myocardial damage, induce endothelial dysfunction, and alter
cardiac conduction. Thus, it is important for practicing cardiologists to be knowledgeable about the diagnosis, prevention,
and management of the cardiovascular complications of cancer therapy. In this first part of a 2-part review, we will
review cancer therapy–induced cardiomyopathy and ischemia. This review is based on a MEDLINE search of
published data, published clinical guidelines, and best practices in major cancer centers. With the number of cancer
survivors expanding quickly, the time has come for cardiologists to work closely with cancer specialists to
prevent and treat cancer therapy–induced cardiovascular complications. (J Am Coll Cardiol 2017;70:2536–51)
© 2017 by the American College of Cardiology Foundation.
H eart diseases and cancer are the top 2 lead-ing causes of death in the United States.Because these maladies share several
common risk factors, many of our patients, espe-cially the elderly, are afflicted by both cancer andheart diseases. Furthermore, cancer therapies, eitherradiation treatment or chemotherapy, can cause car-diovascular complications. Thus, it is important forpracticing cardiologists to be familiar with the pre-vention, diagnosis, and management of cardiovascu-lar complications of cancer therapy. This topic wasreviewed in the Journal in 2009 (1). The purpose ofthis new State-of-the-Art Review is to provide an up-date in this emerging discipline that abounds with
m the aCenter for Precision Medicine, Department of Medicine, Univers
rdiology, University of Texas, MD Anderson Cancer Center, Houston, Texa
iversity, Richmond, Virginia; and the dDivision of Cardiology, Rush Univ
eived support from the National Institutes of Health (HL126916); and is
ssouri, School of Medicine. All other authors have reported that they have n
disclose.
nuscript received July 3, 2017; revised manuscript received September 24
exciting new developments. Cardiovascular compli-cations covered in this 2-part review are heart failure(HF), myocardial ischemia, myocarditis, hyperten-sion (HTN), pulmonary HTN, pericardial diseases,thromboembolism, QT prolongation and arrhyth-mias, and radiation-induced cardiovascular diseases.A MEDLINE search for each of these complicationswas performed; clinically relevant complicationswere selected based on experiences at the MDAnderson Cancer Center and centers affiliated withauthors of this review. Diagnostic and treatmentrecommendations are based on the best practicesdeveloped at MD Anderson Cancer Center and recentguidelines (2–6).
ity of Missouri, Columbia, Missouri; bDepartment of
s; cDivision of Cardiology, Virginia Common Wealth
ersity Medical Center, Chicago, Illinois. Dr. Yeh has
the Frances T. McAndrew Chair in the University of
o relationships relevant to the contents of this paper
, 2017, accepted September 26, 2017.

AB BR E V I A T I O N S
AND ACRONYM S
5-FU = 5-fluorouracil
ACS = acute coronary
syndrome(s)
ATE = arterial thrombotic
event
CAD = coronary artery disease
CIMP = chemotherapy-induced
cardiomyopathy
cTnI = cardiac troponin I
CVA = cerebral vascular
accident
ECG = electrocardiogram
EF = ejection fraction
FDA = U.S. Food and Drug
Administration
GLS = global longitudinal
strain
HF = heart failure
HTN = hypertension
MI = myocardial infarction
TDI = tissue Doppler imaging
VEGF = vascular endothelial
growth factor
VSP = vascular endothelial
growth factor signaling
pathway
J A C C V O L . 7 0 , N O . 2 0 , 2 0 1 7 Chang et al.N O V E M B E R 1 4 / 2 1 , 2 0 1 7 : 2 5 3 6 – 5 1 Best Practices in Cardio-Oncology: Part 1
2537
HEART FAILURE
HF due to chemotherapy has been long recognized as aserious side effect of daunorubicin, the first anthra-cycline used clinically (7). Although the anthracyclineclass of chemotherapy agents remains the major causeof chemotherapy-induced cardiomyopathy (CIMP),newer cancer therapy, such as trastuzumab or pro-teasome inhibitors, can also cause cardiomyopathy(Central Illustration, Table 1). It should also be recog-nized that patients can develop signs and symptoms ofclinical heart failure during chemotherapy; however,the cause of cardiac decompensation may be due tofluid overload, stress-induced cardiomyopathy, orprimary cancer, but not chemotherapy (2). CIMP hasbeen described in 1% to 5% of cancer survivors (8,9)and portends one of the worst survivals among car-diomyopathies (10). Early diagnosis and timely inter-vention has been shown to result in a superior clinicaloutcome in cancer patients treated with cardiotoxicchemotherapy (11).
DEFINITION. In the initial report by Von Hoff et al.(12), HF was defined as the presence of tachycardia,shortness of breath, neck vein distention, galloprhythms, ankle edema, hepatomegaly, cardiomegaly,and pleural effusion (12). With the advance of cardiacimaging, echocardiography or multigated acquisitionradionuclide ventriculography-based evaluation ofleft ventricular ejection fraction (EF) has recently beenincluded in the diagnostic criteria (4,13). In the tras-tuzumab clinical trials, drug-associated cardiotoxicityis defined as 1 or more of the following: 1) cardiomy-opathy characterized by a decrease in EF globally ordue to regional changes in interventricular septumcontraction; 2) symptoms associated with HF; 3) signsassociated with HF, such as S3 gallop, tachycardia, orboth; and 4) decline in initial EF of at least 5% to <55%with signs and symptoms of HF or asymptomaticdecrease in EF of at least 10% to <55% (14). This defi-nition does not include subclinical cardiovasculardamage, such as diastolic dysfunction and changesin LV strain, which may occur earlier in responseto some of the chemotherapeutic agents. CommonTerminology Criteria for Adverse Events has alsodefined cardiomyopathy and/or heart failure forthe purposes of uniform reporting. In CommonTerminology Criteria for Adverse Events 4.03,echocardiography and biomarkers were included toprovide a more precise definition of cardiotoxicity.
INCIDENCE AND PATHOGENESIS. Anthracyc l ines . In aretrospective review of 3 trials, the incidence ofdoxorubicin-related HF was found to be 5% at acumulative dose of 400 mg/m2, 16% at a dose of
500 mg/m2, and 26% at a dose of 550 mg/m2
(15). However, subclinical events occurred inabout 30% of the patients, even at thedoses of 180 to 240 mg/m2, about 13 yearsafter the treatments (16). Interestingly,histopathological changes, such asmyofibrillar loss and vacuolization, can beseen in endomyocardial biopsy specimensfrom patients who have received as little as240 mg/m2 of doxorubicin (17). Thesefindings suggest that there is no safedose of anthracycline. Even doses aslow as 100 mg/m2 have been associatedwith reduced cardiac function (16,18).Nonetheless, some patients had nosignificant cardiac complications despitereceiving doses as high as 1,000 mg/m2 (19).Individual susceptibility is most likely due togenetic variants in genes that regulateanthracycline cardiotoxicity (20). Other riskfactors for anthracycline toxicity includecumulative dose, intravenous bolusadministration, higher single doses, historyof prior irradiation, use of concomitantagents known to have cardiotoxicity, femalesex, underlying CV disease, age (young andelderly), delayed diagnosis, and increase incardiac biomarkers such as troponins during
and after administration (9,21–23).Doxorubicin poisons topoisomerase 2 to causedeoxyribonucleic acid (DNA) double-strand breakand demise of cancer cells. In the cardiomyocytes,doxorubicin targets topoisomerase 2b to induceDNA double-strand breaks, and doxorubicin-boundtopoisomerase 2b binds promoters of antioxidativeand electron-transport genes to reduce their tran-scripts and protein expression (24,25) (Figure 1).Doxorubicin-treated cells have a marked increasein reactive oxygen species and are defective in mito-chondria biogenesis. Thus, topoisomerase 2b accountsfor the 3 hallmarks of anthracycline-induced car-diotoxicity: myocyte death, reactive oxygen speciesgeneration, and mitochondriopathy. Reduced topo-isomerase 2b expression has been linked to a codingvariant in the retinoic receptor g gene, which predictssusceptibility to anthracycline-induced cardiotoxicityin childhood cancer (26).Alky la t ing agents . Alkylating agents add an alkylgroup to the DNA of rapidly dividing cells and, in thecase of bifunctional alkylating agents, cross-link the2 DNA strands, thereby inhibiting DNA replication andcell proliferation (27). Symptoms may include ar-rhythmias, conduction disorders, and fulminant HF(28,29). Alkylating agents such as cyclophosphamide

CENTRAL ILLUSTRATION Management of Cancer Therapy–Induced Cardiovascular Complications
Cancer patients often have co-existing heart diseases;Cancer therapies can cause cardiovascular (CV) complications
Cardiologists and cancer specialists should work together to identify high-risk patients & modify CV risk factors
Strategies for reducing cardiotoxicity:Anthracycline: Dose reduction, continuous infusion, liposomal doxorubicin, dexrazoxaneTrastuzumab: Avoid concomitant anthracyclineVSP inhibitors: Treat hypertension
Consider cardio-protection (Beta Blocker/ACE Inhibitors), if:Ejection fraction (EF) <50% or EF drop>10% Global Longitudinal Strain >15% dropMyocardial damage (assessed via troponin)
Withhold certain cancer therapies as a last resort:Anthracycline (withhold if EF<45%)Trastuzumab (withhold if EF<40%)
Ischemia workup:Stress test, cardiac catheterization
Treatment:As per ACC/AHA guidelines
If platelet count lower than 100,000/microliter of blood:Aspirin if platelet >10K
Dual anti-platelet therapy with aspirin and clopidogrel for drug eluting stents if platelet >30K
Cardiac catheterizationvia radial approach
Cardiomyopathy Ischemia
Chang, H.-M. et al. J Am Coll Cardiol. 2017;70(20):2536–51.
Best practices in the management of cancer therapy–induced cardiomyopathy and ischemia. ACC ¼ American College of Cardiology; ACEI ¼ angiotensin-converting
enzyme inhibitor; AHA ¼ American Heart Association; CV ¼ cardiovascular; EF ¼ ejection fraction; VSP ¼ vascular endothelial growth factor signaling pathway.
Chang et al. J A C C V O L . 7 0 , N O . 2 0 , 2 0 1 7
Best Practices in Cardio-Oncology: Part 1 N O V E M B E R 1 4 / 2 1 , 2 0 1 7 : 2 5 3 6 – 5 1
2538
induce electrocardiogram (ECG) alterations in the formof low QRS voltage and nonspecific T-wave orST-segment abnormalities (28,30,31). Acute symptomsusually occur within 1 to 2 weeks, last for a few days,and in some patients, resolve without any lateconsequences (28,29,31). The incidence of high-dosecyclophosphamide-induced HF has been reportedto be as high as 28% (32). Autopsies of patientswith cyclophosphamide-induced cardiotoxicity showhemorrhagic myocardial necrosis with interstitialedema and fibrin deposition. The risk of complicationsis higher in elderly patients and in those exposed toanthracycline or mediastinal irradiation (1,29,31).
Ifosfamide is an alkylating nitrogen mustard usedfor the treatment of lymphomas; sarcomas; andtesticular, breast, and lung carcinoma (33). There is adose-dependent increase in HF associated withifosfamide administration (33,34). Autopsy studies
demonstrated increased heart weight, small pericar-dial effusions, subendocardial hemorrhage, andpetechial lesions in the epicardium (29).
TARGETED THERAPIES AGAINST HER-2 PATHWAY.
Trastuzumab is a monoclonal antibody against thehuman epidermal growth factor receptor tyrosinekinase (HER2 or ErbB2), which regulates cell growthand repair (35). Overexpression of HER2 occurs inapproximately 25% of breast cancers and confersincreased proliferative and metastatic potential.HER-2 is expressed in cardiomyocytes and is requiredfor survival of cardiomyocytes (36). Mice deficient inHER-2 develop dilated cardiomyopathy and are moresensitive to doxorubicin (36).
Trastuzumab administration in HER2-positivebreast cancers led to significant reductions in recur-rence rate and overall mortality. A pivotal study in

TABLE 1 Anticancer Agents Associated With HF/Left Ventricular Dysfunction
Chemotherapy AgentsFrequencyof Use
Incidence(%) Prevention/Treatment
Anthracyclines
Doxorubicin þþþþ 3–26 Monitor EF, GLS, troponindexrazoxane, continuous infusion,liposomal preparation, BB/ACEI
Epirubicin þ 0.9–3.3
Idarubicin þþ 5–18
Alkylating agents
Cyclophosphamide þþþþ 7–28
Ifosfamide þþþ 17
Antimetabolites
Decitabine þþ 5
Clofarabine þ 27
Antimicrotubule agents
Docetaxel þþ 2.3–8.0
Monoclonal antibody-basedtyrosine kinase inhibitors
Trastuzumab þþþ 2–28 Avoid concomitant use withanthracyclines
Bevacizumab þþ 1.0–10.9
Adotrastuzumab emtansine þ 1.8
Pertuzumab þ 0.9–16.0
Small molecule tyrosine kinaseinhibitors
Pazopanib þþþþ 0.6–11.0 Treat hypertension aggressively
Ponatinib þ 3–15 Ischemia workup and treatment
Sorafenib þþþþ 1.9–11.0
Dabrafenib þþþþ 8–9
Sunitinib þþþþ 1–27
Dasatinib þþþþ 8–9
Lapatinib þþþþ 0.9–4.9
Trametanib þþþþ 7–11
Proteasome inhibitor
Carfilzomib þþ 7
Bortezomib þþ 2–5
Miscellaneous
Tretinoin þþþþ 6
Frequency of use was determined using inpatient and outpatient doses dispensed at MD Anderson Cancer Centerduring the time period of January 1, 2014, through December 21, 2014. þ ¼ <1,000 dosesdispensed; þþ ¼ 1,000–5,000 doses dispensed; þþþ ¼ 5,000–10,000 doses dispensed;and þþþþ ¼ >10,000 doses dispensed (1,2,24,29).
ACEI ¼ angiotensin-converting enzyme inhibitor; BB ¼ beta-blocker; EF ¼ ejection fraction; GLS ¼ globallongitudinal strain; HF ¼ heart failure.
J A C C V O L . 7 0 , N O . 2 0 , 2 0 1 7 Chang et al.N O V E M B E R 1 4 / 2 1 , 2 0 1 7 : 2 5 3 6 – 5 1 Best Practices in Cardio-Oncology: Part 1
2539
the metastatic setting demonstrated a 33% reductionin mortality at 1 year and an increase in median sur-vival by 5 months (37). HF occurred in 8% of patientswho received an anthracycline with cyclophospha-mide; however, the incidence of HF increased to 27%with the addition of trastuzumab (37). Subsequently,several large trials confirmed efficacy of trastuzumabin increasing disease-free survival from cancer, butalso established trastuzumab’s association with HF(38,39). In these trials, 1.7% to 4.1% of trastuzumab-treated patients developed HF when anthracyclinewas not part of the therapeutic regimen (38,39).Trastuzumab-related cardiotoxicity includes variousdegrees of LV systolic dysfunction, occasionallyleading to HF (40). Symptoms are usually mild ormoderate and improve following medical manage-ment and termination of drug administration (41,42).Improvement is usually seen in about 4 to 6 weeksafter trastuzumab withdrawal (43). After symptom-atic improvement, reinstitution of trastuzumabtreatment is usually possible (41–43).
Other targeted therapies against HER-2 arerelatively less cardiotoxic (44–46). Perez et al. (46)reviewed cardiac safety data in 44 clinical trials thatused lapatinib. Of these study patients, only 1.6%experienced a cardiac event, and of those, only 0.2%was symptomatic. The rate of cardiac events in thelapatinib group was similar to those who did notreceive lapatinib (44,46). Similarly, there was nosignificant increase in left ventricular dysfunctionwith the addition of pertuzumab to trastuzumab inthe NeoSphere study (47,48). In the CLEOPATRA(Clinical Evaluation of Pertuzumab and TrastuzumabTrial in Human Epidermal Growth Factor Receptor 2-positive Metastatic Breast Cancer) trial, the incidenceof cardiac adverse events was 14.5% in the pertuzu-mab plus trastuzumab plus docetaxel arm comparedwith 16.4% in the control-placebo plus trastuzumabplus docetaxel arm (49,50). However, in a head-to-head comparison between lapatinib and trastuzu-mab, patients treated with lapatinib have shorterdisease-free survival but more noncardiac toxicity,such as rash and diarrhea (51). Thus, one mustconsider both efficacy and toxicity in choosing drugs.Vascular endothel ia l growth factor s igna l ingpathway inh ib i tors . Vascular endothelial growthfactor signaling pathway (VSP) inhibitors includeantibodies such as bevacizumab, which binds tovascular endothelial growth factor (VEGF), and smallmolecule tyrosine kinase inhibitors such as sunitiniband sorafenib, which inhibit the downstream kinaseinvolved in VEGF receptor signaling (52). Cardiovas-cular side effects of VSP inhibitors include HTN,cardiomyopathy, conduction abnormalities, acute
coronary syndromes (ACS), and arterial thromboses.Several VSP inhibitors also block receptors that areinvolved in the compensatory response to stress inthe cardiomyocytes. When the heart is unable tocompensate for HTN induced by VSP inhibitors, itcould lead to HF (53). Therefore, maintaining goodblood pressure control during VSP inhibitor therapycan prevent HF (54).
Bevacizumab is the first- or second-line chemo-therapy for advanced solid tumors (55–61). Its usehas been associated with HTN, thromboembolism,and cardiomyopathy (62). Approximately 2% to 4% of
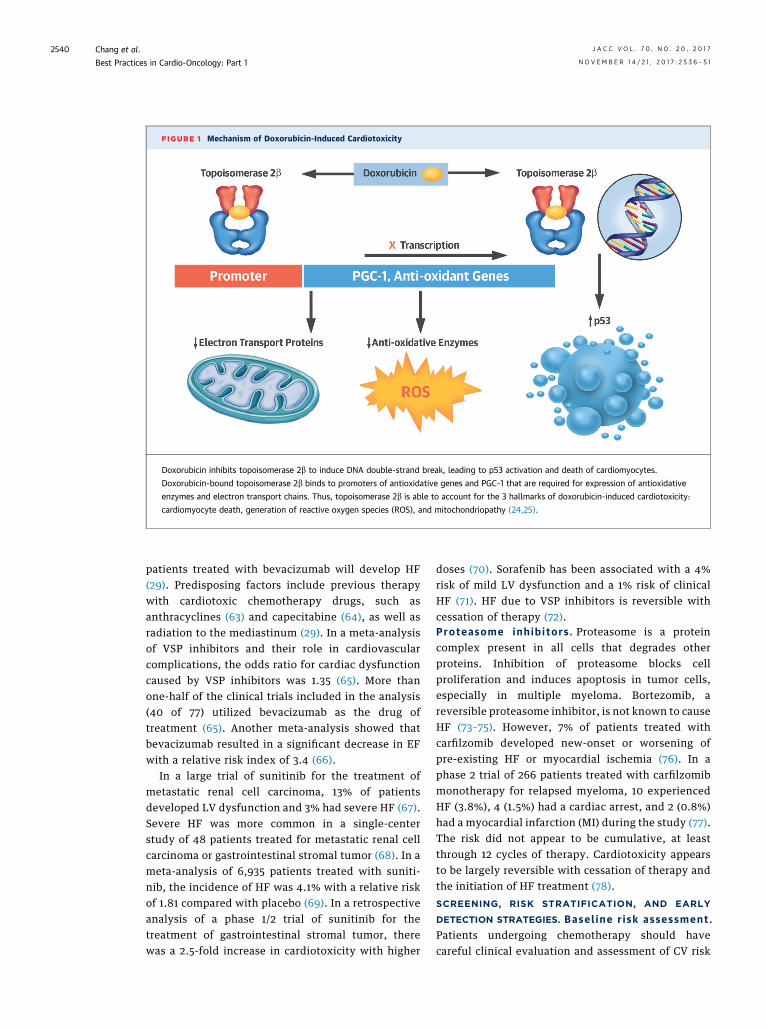
FIGURE 1 Mechanism of Doxorubicin-Induced Cardiotoxicity
Doxorubicin inhibits topoisomerase 2b to induce DNA double-strand break, leading to p53 activation and death of cardiomyocytes.
Doxorubicin-bound topoisomerase 2b binds to promoters of antioxidative genes and PGC-1 that are required for expression of antioxidative
enzymes and electron transport chains. Thus, topoisomerase 2b is able to account for the 3 hallmarks of doxorubicin-induced cardiotoxicity:
cardiomyocyte death, generation of reactive oxygen species (ROS), and mitochondriopathy (24,25).
Chang et al. J A C C V O L . 7 0 , N O . 2 0 , 2 0 1 7
Best Practices in Cardio-Oncology: Part 1 N O V E M B E R 1 4 / 2 1 , 2 0 1 7 : 2 5 3 6 – 5 1
2540
patients treated with bevacizumab will develop HF(29). Predisposing factors include previous therapywith cardiotoxic chemotherapy drugs, such asanthracyclines (63) and capecitabine (64), as well asradiation to the mediastinum (29). In a meta-analysisof VSP inhibitors and their role in cardiovascularcomplications, the odds ratio for cardiac dysfunctioncaused by VSP inhibitors was 1.35 (65). More thanone-half of the clinical trials included in the analysis(40 of 77) utilized bevacizumab as the drug oftreatment (65). Another meta-analysis showed thatbevacizumab resulted in a significant decrease in EFwith a relative risk index of 3.4 (66).
In a large trial of sunitinib for the treatment ofmetastatic renal cell carcinoma, 13% of patientsdeveloped LV dysfunction and 3% had severe HF (67).Severe HF was more common in a single-centerstudy of 48 patients treated for metastatic renal cellcarcinoma or gastrointestinal stromal tumor (68). In ameta-analysis of 6,935 patients treated with suniti-nib, the incidence of HF was 4.1% with a relative riskof 1.81 compared with placebo (69). In a retrospectiveanalysis of a phase 1/2 trial of sunitinib for thetreatment of gastrointestinal stromal tumor, therewas a 2.5-fold increase in cardiotoxicity with higher
doses (70). Sorafenib has been associated with a 4%risk of mild LV dysfunction and a 1% risk of clinicalHF (71). HF due to VSP inhibitors is reversible withcessation of therapy (72).Proteasome inh ib i tors . Proteasome is a proteincomplex present in all cells that degrades otherproteins. Inhibition of proteasome blocks cellproliferation and induces apoptosis in tumor cells,especially in multiple myeloma. Bortezomib, areversible proteasome inhibitor, is not known to causeHF (73–75). However, 7% of patients treated withcarfilzomib developed new-onset or worsening ofpre-existing HF or myocardial ischemia (76). In aphase 2 trial of 266 patients treated with carfilzomibmonotherapy for relapsed myeloma, 10 experiencedHF (3.8%), 4 (1.5%) had a cardiac arrest, and 2 (0.8%)had a myocardial infarction (MI) during the study (77).The risk did not appear to be cumulative, at leastthrough 12 cycles of therapy. Cardiotoxicity appearsto be largely reversible with cessation of therapy andthe initiation of HF treatment (78).
SCREENING, RISK STRATIFICATION, AND EARLY
DETECTION STRATEGIES. Basel ine r i sk assessment .Patients undergoing chemotherapy should havecareful clinical evaluation and assessment of CV risk

TABLE 2 Best Practices for Prevention, Monitoring, and Treatment of CIMP
Oncologist Cardiologist
Identify high-risk patients (pre-existingheart disease, diabetes, hyperlipidemia,young or old, female, plan for high-doseanthracycline therapy)
Modify cardiovascular risk factors (optimizecardiac medications, glucose control,diet, weight, exercise)
Order pre-treatment imaging (If EF <50%or institution low normal, refer tocardiologist)
Repeat imaging studies (obtain high-quality EF,consider contrast, 3-dimensional, strain)
Order biomarkers (troponin and BNP)
Consider noncardiotoxic alternatives(consider noncardiotoxic alternatives inhigh-risk patients)
Advise on cardioprotection (interpret imagingand biomarker results and discusswith oncologist)
Adjust therapy protocols (for anthracycline:dose reduction, continuous infusion,liposomal doxorubicin, dexrazoxane; foranti-HER2: avoid concomitant treatmentwith anthracyclines; for VSP inhibitors,treat HTN aggressively)
Institute cardioprotective medications(start BB or ACEI if EF <50%, EF drop>10%, abnormal GLS [>15% drop],or abnormal troponin)
Monitor during therapy (monitor with echocardiography at 3-month interval or symptom-driven;if cardioprotective medications were given, monitor at 1-month interval)
Withhold cardiotoxic therapy only as the last resort (for anthracycline EF <45%; for anti-HER2therapy EF <40%)
Monitor after completion of therapy (obtain post-therapy EF; repeat echocardiography in6 months or 1 yr; if EF remains abnormal, follow ACC/AHA HF guidelines)
Data from Yeh (2), Plana et al. (3), Zamorano et al. (4), and Armenian et al. (5).
ACC ¼ American College of Cardiology; AHA ¼ American Heart Association; BNP ¼ brain natriuretic peptide;CIMP ¼ chemotherapy-induced cardiomyopathy; HTN ¼ hypertension; VSP ¼ vascular endothelial growth factorsignaling pathway; other abbreviations as in Table 1.
J A C C V O L . 7 0 , N O . 2 0 , 2 0 1 7 Chang et al.N O V E M B E R 1 4 / 2 1 , 2 0 1 7 : 2 5 3 6 – 5 1 Best Practices in Cardio-Oncology: Part 1
2541
factors, such as coronary artery disease, diabetes, andhypertension (Table 2) (2–6). These risk factors shouldbe managed according to the American College ofCardiology (ACC)/American Heart Association (AHA)guidelines (79). This is especially important if cancertherapy is known to cause HF. Aggressive HTNmanagement is advised for patients treated with VSPinhibitors. Physical exercise has been shown toreduce cardiotoxicity in mouse models (80).
EF assessment is mandatory to establish baselinecardiac function before cardiotoxic cancer treatment(3). Echocardiography is the preferred modalityfor assessment of cardiac structure and function.A multigated acquisition radionuclide ventriculog-raphy scan has less interobserver variability; however,radiation exposure limits its utility as a cardiacmonitor. Cardiac magnetic resonance imaging can beused to obtain a precise EF; however, the use of car-diac magnetic resonance imaging is limited by its cost.Cardiac biomarkers, such as troponins and brainnatriuretic peptides (BNPs), can be used to monitor fordevelopment of cardiac dysfunction (3,5,6). However,it is not known whether routine monitoring of bio-markers is useful in changing clinical outcomes. Anumber of composite scores have been designed torisk-stratify cancer patients (81–83); however, theyhave not been validated in prospective studies.
Echocard iogram. The echocardiogram is the mostimportant tool for serial evaluation of the heartduring cancer therapy. EF should be determinedusing the biplane method of discs according to theAmerican Society of Echocardiography guideline (3).If the endocardial border is not distinct, ultrasoniccontrast should aid in endocardial border definitionand subsequent volume calculations. However,temporal EF variability may be up to 10%, with aconfidence interval of 95% in 2-dimensional EFreadings (84). Three-dimensional echocardiographyhas a temporal variability of 6% and is considered themost accurate EF measurement by echocardiography.Because CIMP is defined as a drop of EF of $10% or$5% or more in the presence of HF symptoms, anaccurate measurement of EF is paramount.
Myocard ia l s t ra in . Tissue Doppler imaging (TDI)and speckle-tracking strain imaging have emerged as2 quantitative techniques for estimating global andregional myocardial mechanical function and havethe potential to detect early signs of LV dysfunction(85,86). However, TDI is both user- and angle-dependent and is unable to differentiate trans-lational motion or tethering effects from myocardialcontractility. Speckle-tracking echocardiography isan angle-independent technique that uses an
image-processing algorithm for analyzing motion of‘‘speckles’’ or ‘‘fingerprints’’ within a 2-dimensionalechocardiography image, and it has replaced TDIstrain as the preferred method for quantitativeassessment of cardiac deformation (87,88).
Several studies have evaluated the utility of strainimaging for the detection of chemotherapy-associatedcardiotoxicity. Fallah-Rad et al. (89) evaluated 42patients with breast cancer overexpressing HER-2 whoreceived trastuzumab in the adjuvant setting afteranthracycline therapy. Within 3 months, peak globallongitudinal and radial strain detected preclinicalchanges in LV systolic function before a decrease inEF was observed several months later. A recentprospective multicenter study by Sawaya et al. (90)demonstrated that global longitudinal strain(GLS) <19% was predictive of subsequent cardiotox-icity and was present in all patients who laterdeveloped symptoms of HF. Negishi et al. (91) simi-larly showed that a$11% relative reduction in GLS waspredictive of subsequent trastuzumab-associatedcardiotoxicity.
Abnormalities in strain parameters can also beseen several years after a cardiotoxic exposure. In 75asymptomatic breast cancer survivors who receivedanthracycline with or without adjuvant trastuzumab,GLS was significantly decreased in the chemotherapygroup 6 years after therapy compared with controlsubjects (85,92). In another meta-analysis, GLSconsistently detected earlymyocardial changes during

Chang et al. J A C C V O L . 7 0 , N O . 2 0 , 2 0 1 7
Best Practices in Cardio-Oncology: Part 1 N O V E M B E R 1 4 / 2 1 , 2 0 1 7 : 2 5 3 6 – 5 1
2542
therapy (93). A 10% to 15% early reduction in GLSduring therapy appears to be the most useful param-eter for the prediction of cardiotoxicity. In late cancersurvivors, global radial and circumferential strain areconsistently abnormal, even with normal EF, but theirclinical value in predicting subsequent ventriculardysfunction or HF has not been explored (93).Biomarkers . The use of EF in the diagnosis of CIMPhas important limitations. First, the measurement ofEF is subject to technique-related variability, whichcan be higher than the thresholds used to definecardiotoxicity (14,84). Second, the reduction in EF isoften a late phenomenon (11,89,94,95). Hence, thereis a growing interest in identifying markers ofearly myocardial damage to predict the developmentof HF. Biomarkers are an economic and effectiveway of detecting myocardial dysfunction in appar-ently asymptomatic patients. The assessment oftroponin and BNP has shown incremental utility inidentifying patients at increased risk for adverseoutcomes (96–98).Troponins . Troponin is an important biomarker forACS and other myocardial damage (99–101). In anearly study, cardiac troponin I (cTnI) was elevatedin 32% of 204 patients receiving high-dose chemo-therapy, and an increase in cTnI occurred in morethan 50% of patients soon after drug administration(102). A follow-up study showed that patients withnegative cTnI (<0.08 ng/ml), immediately and1 month after chemotherapy, showed no EF reduc-tion and had low incidence of cardiac events (9). Incontrast, patients with positive cTnI had a higherincidence of adverse cardiac events, including HFand asymptomatic LV dysfunction (9).
Serial troponin measurements in patients withhematologic malignancies treated with anthracyclineshowed troponin elevation correlated with EFreduction (103). A persistent release of cTnI wasassociated with a probability of major cardiac eventswithin the first year of follow-up (9,22). In childrentreated with high-dose doxorubicin for acutelymphoblastic leukemia, cTnT increased in approxi-mately 30% of cases, and the amount of elevation waspredictive of cardiac dysfunction during follow-up(104,105). Thus, most studies showed a good corre-lation of elevated enzymes with LV dysfunction,especially in patients who were treated with high-dose anthracycline.
Dodos et al. (106) performed a series of cardiactroponin T (cTnT) measurements on the 3rd to 5th dayfollowing the first course of anthracycline and after thelast course. They did not observe troponin elevationfollowed by EF deterioration. In their study, cTnTlevels did not exceed the upper limit of the normal
range in all patients. Only 7% of patients had low-levelelevation of cTnT, and only 1 of these patients devel-oped a decrease in EF. McArthur et al. (107) studied agroup of patients treated with bevacizumab, doxoru-bicin, and cyclophosphamide followed by paclitaxel inearly-stage breast cancer. A total of 7 patients (9%)experienced either a symptomatic or asymptomaticEF decline. There was no association between EFchange and troponin elevation (107). These authorsspeculate that cTnI release could be missed becausesamples were drawn prior to chemotherapy (107).Thus, the utility of using troponins in predictingEF changes depends on the timing of blood drawnrelative to chemotherapeutic administration.
In patients with breast cancer who receiveanthracycline or trastuzumab, an elevation of high-sensitivity cTnI with a decrease in GLS of at least19% is highly specific in predicting CIMP (90). Basedon these data, an expert panel proposed thatcTnI should be measured at baseline and every3 weeks during trastuzumab therapy accompanied byechocardiography and GLS at baseline and every3 months (3). A small study concluded that anincrease in high-sensitivity troponins is a good pre-dictor of LV dysfunction (108). A high baseline levelof high-sensitivity troponins is also a predictor ofadverse outcomes (108).
BRAIN NATRIURETIC PEPTIDE. Natriuretic peptides areproduced by splitting a prohormone into the amino-terminal inactive form and the carboxy-terminalbiologically active hormone. The ventricle secretesbiologically active BNP and inactive amino-terminalpro-BNP in response to increased ventricular vol-ume and pressure (109). Clinical studies have utilizedBNP and amino-terminal pro-BNP as biomarkers ofCIMP, and although results are mixed, several studieshave indicated that these peptides could be goodearly indicators of cardiac damage (109–112).
In an early anthracycline study, an increase in BNPlevel correlated with E/A ratio increase, suggestingthat BNP level may be predictive of diastolicdysfunction. BNP increase during anthracyclinetreatment is usually transient and, in most cases, isnot predictive of clinical outcome. Only patients withpersistent elevation of BNP developed overt HF,which also suggests a potential use of BNP in long-term follow-up (113). Nousiainen et al. (114) foundno significant correlations between echocardiographyparameters and natriuretic peptides until the cumu-lative doxorubicin dose reached 500 mg/m2. Meinardiet al. (115) showed that during chemotherapy, con-centrations of BNP in plasma increase as EF decrease.Daugaard et al. (116) also found that neither baseline

J A C C V O L . 7 0 , N O . 2 0 , 2 0 1 7 Chang et al.N O V E M B E R 1 4 / 2 1 , 2 0 1 7 : 2 5 3 6 – 5 1 Best Practices in Cardio-Oncology: Part 1
2543
levels of N-terminal pro-atrial natriuretic peptide norBNP nor changes in these variables during therapywere predictive of a change in EF (116). However,persistent elevation of BNP may be an indicationof adverse cardiac outcomes (115,116). C-reactivepeptide (117–119), myeloperoxidase (117), galacetin-3(117,120,121), and ST-2 (121,122) have been investi-gated as potential biomarkers; however, they cannotbe recommended as routine tests at present.
PREVENTIVE STRATEGIES FOR ANTHRACYCLINE-
INDUCED CARDIOTOXICITY. Selecting a nonanthracyclineregimen. A randomized study of 3,222 women withHER-positive early breast cancer found that anonanthracycline-containing regimen has equalefficacy and less cardiotoxicity (123). With anonanthracycline regimen containing docetaxel,carboplatin, and trastuzumab (TCH), patients had a5-year disease-free survival rate of 81% comparedwith 84% in the anthracycline-containing regimen(ACT [doxorubicin, cyclophosphamide, docetaxel] orACT-H [doxorubicin, cyclophosphamide, docetaxel,trastuzumab]). Importantly, the TCH regimenhas much lower cardiotoxicity than ACT or ACT-H.Thus, TCH was proposed as an alternativenonanthracycline-containing regimen for HER-positive early breast cancers (Table 2).
Subst i tut ing doxorub ic in with less-card iotox icanthracyc l ines . Over the past 5 decades, morethan 2,000 modified anthracycline chemicals havebeen tested in an attempt to reduce cardiotoxicitywhile retaining tumoricidal efficacy. Although severalanthracycline derivatives have been evaluated inclinical trials, only epirubicin (124) and idarubicin(125) received approval for clinical use. However, acritical analysis by the Cochrane database identifiedno difference in cardiotoxicity between epirubicinand doxorubicin at equipotent doses (126).
Cont inuous infus ion . Replacing bolus administra-tion with slow infusions does not significantly affectanthracycline area under the curve, but it diminishesanthracycline Cmax and anthracycline accumulationin the heart (127). A Cochrane review (128) showed asignificantly lower rate of clinical HF with an infusionduration of 6 h or longer compared with a shorterinfusion duration in the adults. In the pediatricpopulations, the results of infusion of anthracyclinehave been disappointing. A randomized trial in chil-dren with high-risk acute lymphocytic leukemiafound that continuous infusion offered no additionalcardiac protection over bolus administration in amedian follow-up of 8 years post-diagnosis (129).A follow-up at 10 years also revealed no incrementaltherapeutic efficacy for infusion (130). Thus,
continuous infusion cannot be recommended in thepediatric population (131,132).PEGylated l iposomal doxorub ic in . PEGylatedliposomal doxorubicin comprises an aqueous coreof doxorubicin hydrochloride encapsulated in lipo-somes with a protective hydrophilic outer coating ofsurface-bound methoxypolyethylene glycol (133,134).Delivery of doxorubicin in a PEGylated liposomalform decreases the circulating concentrations offree doxorubicin and results in selective uptakeof the agent in tumor cells. In randomized trials,PEGylated liposomal doxorubicin was as effectiveas doxorubicin or other traditional combinationchemotherapies (135–140). Thus, PEGylated liposomaldoxorubicin is a useful option in the treatmentof various malignancies (141). However, the costassociated with administering this drug hasprevented its widespread adoption (142).Dexrazoxane. Dexrazoxane was originally devel-oped as an anticancer agent (143). Using fibroblastsfrom topoisomerase 2b knockout mice, Lyu et al. (144)showed that dexrazoxane is protective againstanthracycline-induced toxicity in a topoisomerase2b–dependent manner, linking dexrazoxane to thetopoisomerase 2b theory of anthracycline cardiotox-icity (25) (Figure 1).
The protective effect of dexrazoxane againstanthracycline-induced cardiotoxicity has beendemonstrated in numerous clinical trials in adultsand children (19,105,145–147). Dexrazoxane wasapproved in Europe and the United States forcardioprotection in patients treated with anthracy-clines (Cardioxane, Clinigen Group, Burton-on-Trent,United Kingdom; and Zinecard, Pfizer, New York,New York) with several generic preparations available(procard and cardynax). In addition, dexrazoxanehas been also approved for treatment of accidentalextravasation of anthracyclines (Savene, ClinigenGroup).
Unfortunately, 1 phase 3 trial suggested thatdexrazoxane may lower the efficacy of anthracyclinein treating breast cancer (19). In this trial, a significantdifference in objective response was reported(47% vs. 61%, respectively; p ¼ 0.019). Although ahigh response in the placebo group was quiteunusual, other endpoints (including survival or timeto progression) were not affected by dexrazoxane inthis study (19,148). A careful meta-analyses of allavailable randomized clinical trials found noevidence that dexrazoxane lowers doxorubicin’santicancer effect (149,150). However, the U.S. Foodand Drug Administration (FDA) has approved dexra-zoxane only in patients who have received more than300 mg/m2 of doxorubicin for metastatic breast

TABLE 3 Anticancer Agents Associated With Myocardial Infarction/Ischemia
Chemotherapy AgentsFrequencyof Use
Incidence(%)
Prevention/Treatment
Antimetabolites
Capecitabine þþþþ 3–9 Ischemia workupand treatment
Flourouracil þþþþ 1–68
Monoclonal antibody-basedtyrosine kinase inhibitors
Bevacizumab þþþ 0.6–8.5
Small molecule tyrosinekinase inhibitors
Nilotinib þþþþ 5.0–9.4
Ponatinib þ 12
Angiogenesis inhibitors
Lenalidomide þþþ 0–1.9
Antimicrotubule agents
Paclitaxel þþþþ <1.5
Frequency of use was determined using inpatient and outpatient doses dispensed at MD AndersonCancer Center during the time period of January 1, 2014, through December 21, 2014.þ¼<1,000doses dispensed; þþ ¼ 1,000–5,000 doses dispensed; þþþ ¼ 5,000–10,000 doses dispensed;and þþþþ ¼ >10,000 doses dispensed (1,2,24,29).
Chang et al. J A C C V O L . 7 0 , N O . 2 0 , 2 0 1 7
Best Practices in Cardio-Oncology: Part 1 N O V E M B E R 1 4 / 2 1 , 2 0 1 7 : 2 5 3 6 – 5 1
2544
cancer and who may benefit from continued doxo-rubicin treatment (151).
Another controversy about dexrazoxane pertainsto an increased risk of second malignancies in thepediatric cancer survivors. This was observed in sur-vivors of Hodgkin lymphoma who had receiveddexrazoxane in combination with doxorubicin andetoposide. It was postulated that combining thesedrugs could exceed a threshold above which topo-isomerase inhibitors caused genetic instability innormal tissues (152). This report led the EuropeanMedicine Agency to disapprove the use of dexrazox-ane in children. However, 2 studies of survivors ofchildhood acute lymphoblastic leukemia did notdetect an increased risk of second malignancies fromdexrazoxane (153,154). Thus, the risk/benefit analysissupports a wider clinical usage of dexrazoxane withthe possible exception of patients receiving etoposideor etoposide-anthracycline combinations.
PREVENTATIVE STRATEGIES AGAINST TRASTUZUMAB-
INDUCED CARDIOTOXICITY. The metastatic breastcancer trial showed that concurrent treatment oftrastuzumab and anthracycline had detrimentalcardiac outcomes (14,37). However, as anthracyclineand trastuzumab were not administered at the sametime, the incidence of HF drastically reduced. In theN9831 trial, the incidence of New York Heart Asso-ciation functional class III/IV HF or cardiac deathswas 0% in the control arm (anthracycline withouttrastuzumab) and 3.3% in the concurrent anthracy-cline/trastuzumab arm (155). In the B-31 study, thesetoxic effects occurred in 0.8% of the control group
(anthracycline without trastuzumab) and 4.1% ofthe anthracycline/trastuzumab arm. HF was notreported in the FinHer trial, in which trastuzumabwas omitted during the 3 cycles of epirubicin-containing regimen (156). These results were inmarked distinction to the 27% incidence of HF in theoriginal metastatic trials.
TREATMENT. Symptomatic and asymptomatic HFshould be treated according to the ACC/AHA guide-lines (Table 2) (157,158). We recommend HF treatmentwhen subclinical cardiotoxicity was detected by strainimaging and biomarkers (2,3). Many cancer patientswith overt or subclinical HF can be treated withangiotensin-converting enzyme inhibitors or beta-blockers to allow completion of the chemotherapy.Anthracycline-induced cardiotoxicity was consideredirreversible, whereas trastuzumab was reversible(43,159). Thus, a different EF cutoff threshold forwithholding therapy is recommended (Table 2) (2).It should be noted that cessation of cancer therapyshould be considered only as the last resort.Every effort should be made to manage HF to allowchemotherapy to continue. Patients with symptomaticand/or overt HF should be treated according to theACC/AHA HF guidelines (157,158).
ISCHEMIA
Cancer treatment, including radiation therapyand chemotherapy, is associated with accelerateddevelopment of coronary artery disease (CAD) and/orACS. Cancer itself can also create a pro-thromboticstate that promotes the development of ACS.Thus, chest pain in cancer patients needs to be inves-tigated promptly. Drugs that are commonly associatedwith ischemia in cancer patients were listed in Table 3.
INCIDENCE. Ant imetabol i tes . Chest pain is the mostcommon symptom associated with 5-fluorouracil(5-FU) administration. Less common side effectsinclude MI, arrhythmias, HF, cardiogenic shock,and sudden death (160,161). High doses of 5-FU(>800 mg/m2) and continuous 5-FU infusions arerecognized risk factors of cardiotoxicity (7.6%)compared with bolus injections (2%) (160,162,163).Other risks factors include pre-existingcardiovascular disease, prior mediastinal radiation,and concurrent use of other chemotherapeuticagents (161,162,164–170). Cardiac events are typicallyshort-lasting (up to 48 h) and tend to manifest within2 to 5 days after initiation of 5-FU (160). Ischemicalterations of the ECG have been reported in 68% ofpatients and are associated with biomarkerelevations in 43% of cases (163). The overallmortality ranges from 2.2% to 13% (162,166,171).

J A C C V O L . 7 0 , N O . 2 0 , 2 0 1 7 Chang et al.N O V E M B E R 1 4 / 2 1 , 2 0 1 7 : 2 5 3 6 – 5 1 Best Practices in Cardio-Oncology: Part 1
2545
Selective activation of capecitabine (oralprodrug of 5-FU), which occurs preferentially in can-cer cells, explains its lower cardiotoxicity comparedwith 5-FU. The incidence of capecitabine-inducedcardiotoxicity ranged between 3% and 9% (161,172–174). One prospective study that enrolled 644 pa-tients with no prior history of coronary artery diseasereported the occurrence of symptomatic ischemicchanges of the ECG in 5.2% of patients receivingcapecitabine (167). ECG changes, including ST-segment elevation, were seldom associated with anelevation of serum cardiac markers (163,165,175,176).Ant i -microtubule agents . Myocardial ischemiaand infarction have been reported in approximately3% of the patients receiving paclitaxel. In 198 patientstreated with paclitaxel for ovarian cancer, 0.5%experienced an MI (177). In the Cancer TherapyEvaluation Program’s Adverse Drug Reaction data-base, which followed more than 3,400 patients, theoverall incidence of grade 4 and 5 cardiac events wasonly 0.29% (177). These events occurred within2 weeks of paclitaxel administration (177) and wereobserved in patients with known cardiac risk factorsincluding HTN and CAD.
Cardiac ischemia has also been reported afteradministration of docetaxel. In a clinical trial withinoperable, locally advanced squamous cell carcinomaof the head and neck, 355 patients were randomized toreceive a standard regimen of cisplatin and 5-FU or thesame regimen plus docetaxel. Myocardial ischemiaoccurred in 1.7% of the docetaxel arm and in 0.6% ofthe control arm (178). Although not reported in theoriginal study, cardiac ischemia was listed as a sideeffect of docetaxel in the package insert (179).Ant ibody-based VEGF inh ib i tor . In a pooledanalysis of 1,745 cancer patients from 5 randomizedcontrolled trials, the overall incidence of arterialthrombotic events (ATEs) was significantly higher inthe bevacizumab group (3.8%) compared with thecontrol group (180). In the BRiTE (BevacizumabRegimens’ Investigation of Treatment Effects) study,1,953 patients receiving bevacizumab at 248 U.S. siteswere followed for over 20 months (181). The overallincidence of ATEs was 2%. Of these events, >57%were cerebrovascular cardiovascular accidents (CVAs)and transient ischemic attacks, whereas 30% were MI(50% lethal) (181). Independent risk factors for ATEsincluded age $75 years, poor performance status(Eastern Cooperative Oncology Group performancestatus score $1), pre-existing HTN, anticoagulationtherapy, and arterial disease (181).Smal l molecu lar tyros ine k inase inh ib i tors . In adouble-blind, international phase 3 trial that enrolled569 patients with unresectable, locally advanced, or
metastatic pancreatic cancer, CVAs and MI occurredin 4.6% of patients randomized to receive gemcita-bine plus erlotinib compared with 1.2% patientsassigned to gemcitabine plus placebo (182). Althoughthe incidence of CVA/MI was not published in theoriginal study by Moore et al. (182), it was reported bythe FDA in the erlotinib package insert (183).
Approximately 3% of patients in clinical trials haveexperienced myocardial ischemia with sorafenib.In an unpublished clinical trial, MI/ischemia occurredamong 2.7% of hepatocellular cancer patients treatedwith sorafenib compared with 1.3% of patients inthe placebo group (184). Similarly, sorafenib wasassociated with a higher incidence of MI/ischemiacompared with placebo in patients treated forrenal cell carcinoma (3% vs. <1%) (185). The incidenceof cardiac ischemia/MI in patients with differenttypes of cancer receiving sorafenib ranges from2% to 3% (184).
Proteasome inh ib i tors . The safety profile ofcarfilzomib was analyzed by Siegel et al. (186) in526 patients from 4 phase 2 clinical trials; based ontheir results, the use of carfilzomib was approvedby the FDA. In this analysis, the overall incidenceof myocardial ischemia was reported to be 3.4%.A significantly higher occurrence of ischemic eventswas reported in 2 subsequent phase 3, randomized,multicenter trials, the ASPIRE (Carfizomib, Lenalido-mide, and Dexamethasone vs Lenalidomide andDexamethasone in Subjects with Relapsed MultipleMyeloma) and ENDEAVOR (Carfilzomib and Dexa-methasone versus Bortezomib and Dexamethasonefor Relapsed Multiple Myeloma Patients) studies. Inthe ASPIRE study, the rate of ischemic heart diseasewas 5.9% versus 4.6% in the control group (187).Likewise, in the ENDEAVOR study, ischemic eventsoccurred at a rate of 3% compared with 2% in thecontrol group (188). Hence, high-risk patients shouldbe considered for an ischemic workup prior to startingcarfilzomib treatment (188).
PATHOPHYSIOLOGY. Persistent coronary spasmoccurring at the level of a pre-existing plaquewas observed during cardiac catheterization in apatient receiving continuous 5-FU infusion (189).Experimental work in rabbit aortic rings showed thatincremental doses of 5-FU–induced endothelium-independent vasoconstriction, secondary to proteinkinase C–mediated vasoconstriction of vascularsmooth muscle (190). An alternative mechanism ofcardiotoxicity postulates a direct toxic effect of5-FU on the coronary endothelium (191–193), withensuing endothelial injury leading to micro-thrombotic occlusions (191). Although undetectable

Chang et al. J A C C V O L . 7 0 , N O . 2 0 , 2 0 1 7
Best Practices in Cardio-Oncology: Part 1 N O V E M B E R 1 4 / 2 1 , 2 0 1 7 : 2 5 3 6 – 5 1
2546
by coronary angiography, endothelial injury andsmall vessel thrombosis could be key ultrastructuralfindings (192,193). 5-FU–induced endovascular injurycould be reduced by anticoagulants (194,195). Little isknown regarding the cardiotoxic effect of paclitaxel.Myocardial ischemia in association with paclitaxelis thought to be due to concurrent use of other drugsand pre-existing cardiac conditions (196). The poly-oxyethylated castor oil, known as Cremophor EL(BASF, Ludwigshafen, Germany), is used as a vehiclefor paclitaxel in the injectable formulation and maycontribute to the overall cardiotoxicity by inducinghistamine release (196).
VEGF stimulates endothelial cell proliferation tomaintain endothelial viability and vascular integrity(197). Consequently, bevacizumab administrationmay impair the regenerative potential of endothelialcells in response to stress. Exposed subendothelialcollagen can trigger tissue factor activation, resultingin thromboembolism (197,198). VEGF inhibition alsoimpairs the production of nitric oxide and prostacy-clin, as well as increases hematocrit and bloodviscosity via overproduction of erythropoietin, allof which heighten the thromboembolic risk (197).Carfilzomib was found to increase coronaryperfusion pressure and resting vasoconstriction tonein isolated rabbit heart and aorta (199). In addition,carfilzomib amplified the spasmogenic effectof noradrenaline and angiotensin II, curbed the anti-spasmogenic activity of nifedipine and nitroglycerin,and reduced the vasodilating effect of acetylcholine.
SCREENING, DIAGNOSIS, AND TREATMENT. Becausepre-existing CAD is a known risk factor for thedevelopment of chemotherapy-induced ACS, ischemicworkup should be initiated in all high-risk patientsbefore administration of drugs known to cause cardiacischemia (Table 3). Patients with suspected ACSshould be treated according to ACC/AHA guidelines(200,201). Besides statins and beta-blockers, the cor-nerstones of ACS treatment include percutaneouscoronary intervention as well as antiplatelet andanticoagulant therapy, all of which pose an incre-mental bleeding risk in cancer patients with throm-bocytopenia. Although prospective studies in thisspecific population are currently lacking, a retrospec-tive analysis carried out in cancer patients withthrombocytopenia and ACS showed that aspirinimproved the 7-day survival rate without increasingthe bleeding risk (202). Although case-specific con-siderations are warranted, life-saving interventionsshould not be denied to cancer patients withongoing ACS because of thrombocytopenia (203).The response to anticoagulants and antiplatelet
agents in patients with platelet counts >50,000/mlseems to be comparable to that observed in patientswith normal platelet counts (203). However, reducedheparin doses, ranging from 30 to 50 U/kg, maybe required for patients whose platelet countsare <50,000/ml (203). Dual antiplatelet therapy withaspirin and clopidogrel can be used for patients withplatelet counts >30,000/ml, whereas aspirin as a singleagent should be given to those with platelet counts>10,000/ml. With a platelet count below 10,000/ml,bleeding risk should be carefully evaluated against therisk of leaving the thrombotic event untreated (202).In cancer patients with ACS and thrombocytopenia,revascularization can still proceed with radial access,micropuncture kits, and closure devices for the arteryentry site. When the femoral access is chosen,prolonged groin pressure of at least 30 min should beinstituted to obtain hemostasis (204).
Patients treated with 5-FU or capecitabine shouldbe closely monitored for myocardial ischemia withserial ECGs. Preemptive use of coronary vasodilators,such as nitrates and calcium-channel blockers, shouldbe considered. In cancer patients who develop acutechest pain while receiving 5-FU or capecitabine, theoffending drugs should be withheld until diagnosticworkup is completed and anti-anginal therapy isinstituted. It is possible to re-challenge the patientswith close monitoring; however, an alternativeregimen that does not contain the offending drug is abetter option (160,164,166,173).
Temporary or permanent discontinuation of sor-afenib is also advised in the management of patientsdeveloping cardiac ischemia during or followingtreatment (184). There is a scarcity of data aboutre-challenge. Because patients who experienced astroke or MI within 12 months from enrollmenthave been excluded from the trials evaluating bev-acizumab, the safety of the drug in this high-riskpopulation is unknown (205). Treatment withbevacizumab should be promptly discontinued inpatients who develop severe ATEs during treatment.The safety of restarting bevacizumab after resolutionof an ATE has not been evaluated (205). As cardiaccomplications caused by carfilzomib are serious,high-risk patients, including those age $75 years,should undergo an ischemic workup prior to startingcarfilzomib treatment (202). Prompt discontinuationof carfilzomib is warranted when chest pain developsduring infusion.
ADDRESS FOR CORRESPONDENCE: Dr. Edward T.H.Yeh, Department of Medicine, University of Missouri,1 Hospital Drive, MA412, Columbia, Missouri 65212.E-mail: [email protected].

J A C C V O L . 7 0 , N O . 2 0 , 2 0 1 7 Chang et al.N O V E M B E R 1 4 / 2 1 , 2 0 1 7 : 2 5 3 6 – 5 1 Best Practices in Cardio-Oncology: Part 1
2547
RE F E RENCE S
1. Yeh ET, Bickford CL. Cardiovascular complica-tions of cancer therapy: incidence, pathogenesis,diagnosis, and management. J Am Coll Cardiol2009;53:2231–47.
2. Yeh ET. MD Anderson Practices in Onco-Cardiology, 2016. Available at: https://www.mdanderson.org/research/departments-labsinstitutes/departments-divisions/cardiology/research.html.
3. Plana JC, Galderisi M, Barac A, et al. Expertconsensus for multimodality imaging evaluation ofadult patients during and after cancer therapy:a report from the American Society of Echocardi-ography and the European Association ofCardiovascular Imaging. Eur Heart J CardiovascImaging 2014;15:1063–93.
4. Zamorano JL, Lancellotti P, RodriguezMunoz D, et al. 2016 ESC position paper on cancertreatments and cardiovascular toxicity developedunder the auspices of the ESC Committee forPractice Guidelines: The Task Force For CancerTreatments and Cardiovascular Toxicity of theEuropean Society of Cardiology (ESC). Eur Heart J2016;37:2768–801.
5. Armenian SH, Lacchetti C, Barac A, et al.Prevention and monitoring of cardiac dysfunctionin survivors of adult cancers: American Society ofClinical Oncology clinical practice guideline. J ClinOncol 2017;35:893–911.
6. Curigliano G, Cardinale D, Suter T, et al.Cardiovascular toxicity induced by chemotherapy,targeted agents and radiotherapy: ESMO clinicalpractice guidelines. Ann Oncol 2012;23 Suppl 7:vii155–66.
7. Tan C, Tasaka H, Yu KP, Murphy ML,Karnofsky DA. Daunomycin, an antitumor anti-biotic, in the treatment of neoplastic disease.Clinical evaluation with special reference tochildhood leukemia. Cancer 1967;20:333–53.
8. Hequet O, Le QH,Moullet I, et al. Subclinical latecardiomyopathy after doxorubicin therapy forlymphoma in adults. J Clin Oncol 2004;22:1864–71.
9. Cardinale D, Sandri MT, Colombo A, et al. Prog-nostic value of troponin I in cardiac risk stratifica-tion of cancer patients undergoing high-dosechemotherapy. Circulation 2004;109:2749–54.
10. Felker GM, Thompson RE, Hare JM, et al.Underlying causes and long-term survival inpatients with initially unexplained cardiomyopathy.N Engl J Med 2000;342:1077–84.
11. Cardinale D, Colombo A, Lamantia G, et al.Anthracycline-induced cardiomyopathy: clinicalrelevance and response to pharmacologic therapy.J Am Coll Cardiol 2010;55:213–20.
12. Von Hoff DD, Layard MW, Basa P, et al. Riskfactors for doxorubicin-induced congestive heartfailure. Ann Intern Med 1979;91:710–7.
13. Virani SA, Dent S, Brezden-Masley C, et al. Cana-dian Cardiovascular Society guidelines for evaluationand management of cardiovascular complications ofcancer therapy. Can J Cardiol 2016;32:831–41.
14. Seidman A, Hudis C, Pierri MK, et al. Cardiacdysfunction in the trastuzumab clinical trialsexperience. J Clin Oncol 2002;20:1215–21.
15. Swain SM, Whaley FS, Ewer MS. Congestiveheart failure in patients treated with doxorubicin:a retrospective analysis of three trials. Cancer2003;97:2869–79.
16. Vandecruys E, Mondelaers V, De Wolf D,Benoit Y, Suys B. Late cardiotoxicity after low doseof anthracycline therapy for acute lymphoblasticleukemia in childhood. J Cancer Surviv 2012;6:95–101.
17. Nysom K, Holm K, Lipsitz SR, et al. Relationshipbetween cumulative anthracycline dose and latecardiotoxicity in childhood acute lymphoblasticleukemia. J Clin Oncol 1998;16:545–50.
18. van der Pal HJ, van Dalen EC, Hauptmann M,et al. Cardiac function in 5-year survivors ofchildhood cancer: a long-term follow-up study.Arch Intern Med 2010;170:1247–55.
19. Swain SM, Whaley FS, Gerber MC, et al. Car-dioprotection with dexrazoxane for doxorubicin-containing therapy in advanced breast cancer.J Clin Oncol 1997;15:1318–32.
20. Aminkeng F, Ross CJ, Rassekh SR, et al.Recommendations for genetic testing to reducethe incidence of anthracycline-induced cardiotox-icity. Br J Clin Pharmacol 2016;82:683–95.
21. Braverman AC, Antin JH, Plappert MT,Cook EF, Lee RT. Cyclophosphamide cardiotoxicityin bone marrow transplantation: a prospectiveevaluation of new dosing regimens. J Clin Oncol1991;9:1215–23.
22. Cardinale D, Sandri MT, Martinoni A, et al.Myocardial injury revealed by plasma troponin Iin breast cancer treated with high-dosechemotherapy. Ann Oncol 2002;13:710–5.
23. Pichon MF, Cvitkovic F, Hacene K, et al. Drug-induced cardiotoxicity studied by longitudinalB-type natriuretic peptide assays and radionuclideventriculography. Vivo 2005;19:567–76.
24. Yeh ET, Chang HM. Oncocardiology–past,present, and future: a review. JAMA Cardiol 2016;1:1066–72.
25. Zhang S, Liu X, Bawa-Khalfe T, et al. Identifi-cation of the molecular basis of doxorubicin-induced cardiotoxicity. Nat Med 2012;18:1639–42.
26. Aminkeng F, Bhavsar AP, Visscher H, et al.A coding variant in RARG confers susceptibility toanthracycline-induced cardiotoxicity in childhoodcancer. Nat Genet 2015;47:1079–84.
27. Fu D, Calvo JA, Samson LD. Balancing repairand tolerance of DNA damage caused by alkylatingagents. Nat Rev Cancer 2012;12:104–20.
28. Floyd JD, Nguyen DT, Lobins RL, Bashir Q,Doll DC, Perry MC. Cardiotoxicity of cancertherapy. J Clin Oncol 2005;23:7685–96.
29. Yeh ET, Tong AT, Lenihan DJ, et al.Cardiovascular complications of cancer therapy:diagnosis, pathogenesis, and management.Circulation 2004;109:3122–31.
30. Schimmel KJ, Richel DJ, van den Brink RB,Guchelaar HJ. Cardiotoxicity of cytotoxic drugs.Cancer Treat Rev 2004;30:181–91.
31. Slordal L, Spigset O. Heart failure induced bynon-cardiac drugs. Drug Saf 2006;29:567–86.
32. Gottdiener JS, Appelbaum FR, Ferrans VJ,Deisseroth A, Ziegler J. Cardiotoxicity associatedwith high-dose cyclophosphamide therapy. ArchIntern Med 1981;141:758–63.
33. Quezado ZM, Wilson WH, Cunnion RE, et al.High-dose ifosfamide is associated with severe,reversible cardiac dysfunction. Ann Intern Med1993;118:31–6.
34. Kandylis K, Vassilomanolakis M, Tsoussis S,Efremidis AP. Ifosfamide cardiotoxicity in humans.Cancer Chemother Pharmacol 1989;24:395–6.
35. Yarden Y. The EGFR family and its ligands inhuman cancer. signalling mechanisms and thera-peutic opportunities. Eur J Cancer 2001;37 Suppl4:S3–8.
36. Crone SA, Zhao YY, Fan L, et al. ErbB2 isessential in the prevention of dilated cardiomy-opathy. Nat Med 2002;8:459–65.
37. Slamon DJ, Leyland-Jones B, Shak S, et al. Useof chemotherapy plus a monoclonal antibodyagainst HER2 for metastatic breast cancer thatoverexpresses HER2. N Engl J Med 2001;344:783–92.
38. Bird BR, Swain SM. Cardiac toxicity in breastcancer survivors: review of potential cardiacproblems. Clin Cancer Res 2008;14:14–24.
39. Hudis CA. Trastuzumab—mechanism of actionand use in clinical practice. N Engl J Med 2007;357:39–51.
40. Yavas O, Yazici M, Eren O, Oyan B. The acuteeffect of trastuzumab infusion on ECG parametersin metastatic breast cancer patients. Swiss MedWkly 2007;137:556–8.
41. Keefe DL. Trastuzumab-associated cardiotox-icity. Cancer 2002;95:1592–600.
42. Perez EA, Rodeheffer R. Clinical cardiactolerability of trastuzumab. J Clin Oncol 2004;22:322–9.
43. Ewer MS, Vooletich MT, Durand JB, et al.Reversibility of trastuzumab-related cardiotox-icity: new insights based on clinical course andresponse to medical treatment. J Clin Oncol 2005;23:7820–6.
44. Azim H, Azim HA Jr., Escudier B. Trastuzumabversus lapatinib: the cardiac side of the story.Cancer Treat Rev 2009;35:633–8.
45. Lenihan D, Suter T, Brammer M, Neate C,Ross G, Baselga J. Pooled analysis of cardiac safetyin patients with cancer treated with pertuzumab.Ann Oncol 2012;23:791–800.
46. Perez EA, Koehler M, Byrne J, Preston AJ,Rappold E, Ewer MS. Cardiac safety of lapatinib:pooled analysis of 3689 patients enrolled inclinical trials. Mayo Clin Proc 2008;83:679–86.
47. Baselga J, Gelmon KA, Verma S, et al. Phase IItrial of pertuzumab and trastuzumab in patientswith human epidermal growth factor receptor2-positive metastatic breast cancer thatprogressed during prior trastuzumab therapy.J Clin Oncol 2010;28:1138–44.

Chang et al. J A C C V O L . 7 0 , N O . 2 0 , 2 0 1 7
Best Practices in Cardio-Oncology: Part 1 N O V E M B E R 1 4 / 2 1 , 2 0 1 7 : 2 5 3 6 – 5 1
2548
48. Gianni L, Pienkowski T, Im YH, et al. Efficacyand safety of neoadjuvant pertuzumab andtrastuzumab in women with locally advanced,inflammatory, or early HER2-positive breast cancer(NeoSphere): a randomised multicentre, open-label, phase 2 trial. Lancet Oncol 2012;13:25–32.
49. Baselga J, Cortes J, Kim SB, et al. Pertuzumabplus trastuzumab plus docetaxel for metastaticbreast cancer. N Engl J Med 2012;366:109–19.
50. Swain SM, Ewer MS, Cortes J, et al. Cardiactolerability of pertuzumab plus trastuzumab plusdocetaxel in patients with HER2-positive meta-static breast cancer in CLEOPATRA: a randomized,double-blind, placebo-controlled phase III study.Oncologist 2013;18:257–64.
51. Gelmon KA, Boyle FM, Kaufman B, et al.Lapatinib or trastuzumab plus taxane therapyfor human epidermal growth factor receptor2-positive advanced breast cancer: final results ofNCIC CTG MA.31. J Clin Oncol 2015;33:1574–83.
52. Moslehi JJ. Cardiovascular toxic effects oftargeted cancer therapies. N Engl J Med 2016;375:1457–67.
53. Chintalgattu V, Ai D, Langley RR, et al.Cardiomyocyte PDGFR-beta signaling is anessential component of the mouse cardiacresponse to load-induced stress. J Clin Invest2010;120:472–84.
54. Chen MH, Kerkela R, Force T. Mechanisms ofcardiac dysfunction associated with tyrosine ki-nase inhibitor cancer therapeutics. Circulation2008;118:84–95.
55. Aghajanian C, Blank SV, Goff BA, et al.OCEANS: a randomized, double-blind, placebo-controlled phase III trial of chemotherapy with orwithout bevacizumab in patients with platinum-sensitive recurrent epithelial ovarian, primaryperitoneal, or fallopian tube cancer. J Clin Oncol2012;30:2039–45.
56. Friedman HS, Prados MD, Wen PY, et al.Bevacizumab alone and in combination withirinotecan in recurrent glioblastoma. J Clin Oncol2009;27:4733–40.
57. Giantonio BJ, Catalano PJ, Meropol NJ, et al.Bevacizumab in combination with oxaliplatin,fluorouracil, and leucovorin (FOLFOX4) for previ-ously treated metastatic colorectal cancer: resultsfrom the Eastern Cooperative Oncology GroupStudy E3200. J Clin Oncol 2007;25:1539–44.
58. Hurwitz H, Fehrenbacher L, Novotny W, et al.Bevacizumab plus irinotecan, fluorouracil, andleucovorin for metastatic colorectal cancer. N EnglJ Med 2004;350:2335–42.
59. Miller K, Wang M, Gralow J, et al. Paclitaxelplus bevacizumab versus paclitaxel alone formetastatic breast cancer. N Engl J Med 2007;357:2666–76.
60. Rini BI, Halabi S, Rosenberg JE, et al. Phase IIItrial of bevacizumab plus interferon alfa versusinterferon alfa monotherapy in patients withmetastatic renal cell carcinoma: final results ofCALGB 90206. J Clin Oncol 2010;28:2137–43.
61. Tewari KS, Sill MW, Long HJ 3rd, et al.Improved survival with bevacizumab in advancedcervical cancer. N Engl J Med 2014;370:734–43.
62. Galfrascoli E, Piva S, Cinquini M, et al. Risk/benefit profile of bevacizumab in metastatic coloncancer: a systematic review and meta-analysis. DigLiver Dis 2011;43:286–94.
63. D’Adamo DR, Anderson SE, Albritton K, et al.Phase II study of doxorubicin and bevacizumab forpatients with metastatic soft-tissue sarcomas.J Clin Oncol 2005;23:7135–42.
64. Miller KD, Chap LI, Holmes FA, et al.Randomized phase III trial of capecitabinecompared with bevacizumab plus capecitabine inpatients with previously treated metastatic breastcancer. J Clin Oncol 2005;23:792–9.
65. Abdel-Qadir H, Ethier JL, Lee DS,Thavendiranathan P, Amir E. Cardiovasculartoxicity of angiogenesis inhibitors in treatment ofmalignancy: a systematic review and meta-anal-ysis. Cancer Treat Rev 2017;53:120–7.
66. Escalante CP, Chang YC, Liao K, et al. Meta-analysis of cardiovascular toxicity risks in cancerpatients on selected targeted agents. SupportCare Cancer 2016;24:4057–74.
67. Motzer RJ, Hutson TE, Tomczak P, et al.Overall survival and updated results for sunitinibcompared with interferon alfa in patients withmetastatic renal cell carcinoma. J Clin Oncol2009;27:3584–90.
68. Telli ML, Witteles RM, Fisher GA, Srinivas S.Cardiotoxicity associated with the cancer thera-peutic agent sunitinib malate. Ann Oncol 2008;19:1613–8.
69. Richards CJ, Je Y, Schutz FA, et al. Incidenceand risk of congestive heart failure in patients withrenal and nonrenal cell carcinoma treated withsunitinib. J Clin Oncol 2011;29:3450–6.
70. Chu TF, Rupnick MA, Kerkela R, et al.Cardiotoxicity associated with tyrosine kinaseinhibitor sunitinib. Lancet 2007;370:2011–9.
71. Hall PS, Harshman LC, Srinivas S, Witteles RM.The frequency and severity of cardiovasculartoxicity from targeted therapy in advanced renalcell carcinoma patients. J Am Coll Cardiol HF 2013;1:72–8.
72. Uraizee I, Cheng S, Moslehi J. Reversiblecardiomyopathy associated with sunitinib andsorafenib. N Engl J Med 2011;365:1649–50.
73. Gupta A, Pandey A, Sethi S. Bortezomib-induced congestive cardiac failure in a patient withmultiple myeloma. Cardiovasc Toxicol 2012;12:184–7.
74. Hacihanefioglu A, Tarkun P, Gonullu E. Acutesevere cardiac failure in a myeloma patient due toproteasome inhibitor bortezomib. Int J Hematol2008;88:219–22.
75. Jerkins JH, Suciu A, Mazimba S, Calvo A.Bortezomib-induced severe congestive heartfailure. Cardiol Res 2010;1:20–3.
76. Maurea N, Spallarossa P, Cadeddu C, et al.A recommended practical approach to themanagement of target therapy and angiogenesisinhibitors cardiotoxicity: an opinion paper of theworking group on drug cardiotoxicity andcardioprotection, Italian Society of Cardiology.J Cardiovasc Med (Hagerstown) 2016;17 Suppl 1:e93–104.
77. Siegel DS, Martin T, Wang M, et al. A phase 2study of single-agent carfilzomib (PX-171-003-A1)in patients with relapsed and refractory multiplemyeloma. Blood 2012;120:2817–25.
78. Grandin EW, Ky B, Cornell RF, Carver J,LenihanDJ.Patternsof cardiac toxicityassociatedwithirreversible proteasome inhibition in the treatmentof multiple myeloma. J Card Fail 2015;21:138–44.
79. Goff DC Jr., Lloyd-Jones DM, Bennett G, et al.2013 ACC/AHA guideline on the assessment ofcardiovascular risk: a report of the American Col-lege of Cardiology/American Heart AssociationTask Force on Practice Guidelines. J Am CollCardiol 2014;63:2935–59.
80. Chicco AJ, Hydock DS, Schneider CM,Hayward R. Low-intensity exercise training duringdoxorubicin treatment protects against cardiotox-icity. J Appl Physiol (1985) 2006;100:519–27.
81. Dranitsaris G, Rayson D, Vincent M, et al. Thedevelopment of a predictive model to estimatecardiotoxic risk for patients with metastatic breastcancer receiving anthracyclines. Breast Cancer ResTreat 2008;107:443–50.
82. Ezaz G, Long JB, Gross CP, Chen J. Risk pre-diction model for heart failure and cardiomyopa-thy after adjuvant trastuzumab therapy for breastcancer. J Am Heart Assoc 2014;3:e000472.
83. Herrmann J, Lerman A, Sandhu NP, Villarraga HR,Mulvagh SL, Kohli M. Evaluation and managementof patients with heart disease and cancer: cardio-oncology. Mayo Clin Proc 2014;89:1287–306.
84. Thavendiranathan P, Grant AD, Negishi T,Plana JC, Popovic ZB, Marwick TH. Reproducibilityof echocardiographic techniques for sequentialassessment of left ventricular ejection fraction andvolumes: application to patients undergoing cancerchemotherapy. J Am Coll Cardiol 2013;61:77–84.
85. Yu AF, Steingart RM, Fuster V. Cardiomyopa-thy associated with cancer therapy. J Card Fail2014;20:841–52.
86. Gorcsan J 3rd, Tanaka H. Echocardiographicassessment of myocardial strain. J Am Coll Cardiol2011;58:1401–13.
87. Geyer H, Caracciolo G, Abe H, et al. Assess-ment of myocardial mechanics using speckletracking echocardiography: fundamentals andclinical applications. J Am Soc Echocardiogr 2010;23:351–69, quiz 453–5.
88. Perk G, Tunick PA, Kronzon I. Non-Doppler two-dimensional strain imaging byechocardiography—from technical considerationsto clinical applications. J Am Soc Echocardiogr2007;20:234–43.
89. Fallah-Rad N, Walker JR, Wassef A, et al.The utility of cardiac biomarkers, tissue velocityand strain imaging, and cardiac magnetic reso-nance imaging in predicting early left ventriculardysfunction in patients with human epidermalgrowth factor receptor II-positive breast cancertreated with adjuvant trastuzumab therapy. J AmColl Cardiol 2011;57:2263–70.
90. Sawaya H, Sebag IA, Plana JC, et al. Assess-ment of echocardiography and biomarkers for theextended prediction of cardiotoxicity in patientstreated with anthracyclines, taxanes, and trastu-zumab. Circ Cardiovasc Imaging 2012;5:596–603.

J A C C V O L . 7 0 , N O . 2 0 , 2 0 1 7 Chang et al.N O V E M B E R 1 4 / 2 1 , 2 0 1 7 : 2 5 3 6 – 5 1 Best Practices in Cardio-Oncology: Part 1
2549
91. Negishi K, Negishi T, Hare JL, Haluska BA,Plana JC, Marwick TH. Independent and incre-mental value of deformation indices for predictionof trastuzumab-induced cardiotoxicity. J Am SocEchocardiogr 2013;26:493–8.
92. Ho E, Brown A, Barrett P, et al. Subclinicalanthracycline- and trastuzumab-induced car-diotoxicity in the long-term follow-up of asymp-tomatic breast cancer survivors: a speckle trackingechocardiographic study. Heart 2010;96:701–7.
93. Thavendiranathan P, Poulin F, Lim KD,Plana JC, Woo A, Marwick TH. Use of myocardialstrain imaging by echocardiography for the earlydetection of cardiotoxicity in patients during andafter cancer chemotherapy: a systematic review.J Am Coll Cardiol 2014;63:2751–68.
94. Cardinale D, Colombo A, Torrisi R, et al.Trastuzumab-induced cardiotoxicity: clinical andprognostic implications of troponin I evaluation.J Clin Oncol 2010;28:3910–6.
95. Telli ML, Hunt SA, Carlson RW, Guardino AE.Trastuzumab-related cardiotoxicity: calling intoquestion the concept of reversibility. J Clin Oncol2007;25:3525–33.
96. Braunwald E. Biomarkers in heart failure.N Engl J Med 2008;358:2148–59.
97. Ky B, French B, Levy WC, et al. Multiplebiomarkers for risk prediction in chronic heartfailure. Circ Heart Fail 2012;5:183–90.
98. Zethelius B, Berglund L, Sundstrom J, et al.Use of multiple biomarkers to improve theprediction of death from cardiovascular causes.N Engl J Med 2008;358:2107–16.
99. Katus HA, Remppis A, Looser S, Hallermeier K,Scheffold T, Kubler W. Enzyme linked immunoassay of cardiac troponin T for the detection ofacute myocardial infarction in patients. J Mol CellCardiol 1989;21:1349–53.
100. Balk EM, Ioannidis JP, Salem D, Chew PW,Lau J. Accuracy of biomarkers to diagnose acutecardiac ischemia in the emergency department: ameta-analysis. Ann Emerg Med 2001;37:478–94.
101. Jaffe AS, Landt Y, Parvin CA,Abendschein DR, Geltman EM, Ladenson JH.Comparative sensitivity of cardiac troponin I andlactate dehydrogenase isoenzymes for diagnosingacute myocardial infarction. Clin Chem 1996;42:1770–6.
102. Cardinale D, Sandri MT, Martinoni A, et al.Left ventricular dysfunction predicted by earlytroponin I release after high-dose chemotherapy.J Am Coll Cardiol 2000;36:517–22.
103. Auner HW, Tinchon C, Linkesch W, et al.Prolonged monitoring of troponin T for thedetection of anthracycline cardiotoxicity in adultswith hematological malignancies. Ann Hematol2003;82:218–22.
104. Lipshultz SE, Miller TL, Scully RE, et al.Changes in cardiac biomarkers during doxorubicintreatment of pediatric patients with high-riskacute lymphoblastic leukemia: associations withlong-term echocardiographic outcomes. J ClinOncol 2012;30:1042–9.
105. Lipshultz SE, Scully RE, Lipsitz SR, et al.Assessment of dexrazoxane as a cardioprotectantin doxorubicin-treated children with high-risk
acute lymphoblastic leukaemia: long-termfollow-up of a prospective, randomised, multi-centre trial. Lancet Oncol 2010;11:950–61.
106. Dodos F, Halbsguth T, Erdmann E, Hoppe UC.Usefulness of myocardial performance index andbiochemical markers for early detection ofanthracycline-induced cardiotoxicity in adults.Clin Res Cardiol 2008;97:318–26.
107. McArthur HL, Rugo H, Nulsen B, et al.A feasibility study of bevacizumab plus dose-dense doxorubicin-cyclophosphamide (AC) fol-lowed by nanoparticle albumin-bound paclitaxel inearly-stage breast cancer. Clin Cancer Res 2011;17:3398–407.
108. Blaes AH, Rehman A, Vock DM, et al. Utilityof high-sensitivity cardiac troponin T in patientsreceiving anthracycline chemotherapy. VascHealth Risk Manag 2015;11:591–4.
109. Germanakis I, Anagnostatou N, Kalmanti M.Troponins and natriuretic peptides in themonitoring of anthracycline cardiotoxicity. PediatrBlood Cancer 2008;51:327–33.
110. Broeyer FJ, Osanto S, Ritsema van Eck HJ,et al. Evaluation of biomarkers for cardiotoxicity ofanthracyclin-based chemotherapy. J Cancer ResClin Oncol 2008;134:961–8.
111. Lee HS, Son CB, Shin SH, Kim YS. Clinicalcorrelation between brain natriutetic peptide andanthracyclin-induced cardiac toxicity. Cancer ResTreat 2008;40:121–6.
112. Mavinkurve-Groothuis AM, Kapusta L, Nir A,Groot-Loonen J. The role of biomarkers in theearly detection of anthracycline-induced car-diotoxicity in children: a review of the literature.Pediatr Hematol Oncol 2008;25:655–64.
113. Suzuki T, Hayashi D, Yamazaki T, et al.Elevated B-type natriuretic peptide levels afteranthracycline administration. Am Heart J 1998;136:362–3.
114. Nousiainen T, Vanninen E, Jantunen E, et al.Natriuretic peptides during the development ofdoxorubicin-induced left ventricular diastolicdysfunction. J Intern Med 2002;251:228–34.
115. Meinardi MT, van Veldhuisen DJ, Gietema JA,et al. Prospective evaluation of early cardiacdamage induced by epirubicin-containing adjuvantchemotherapy and locoregional radiotherapy inbreast cancer patients. J Clin Oncol 2001;19:2746–53.
116. Daugaard G, Lassen U, Bie P, et al. Natriureticpeptides in the monitoring of anthracyclineinduced reduction in left ventricular ejectionfraction. Eur J Heart Fail 2005;7:87–93.
117. Ky B, Putt M, Sawaya H, et al. Early increasesin multiple biomarkers predict subsequent car-diotoxicity in patients with breast cancer treatedwith doxorubicin, taxanes, and trastuzumab. J AmColl Cardiol 2014;63:809–16.
118. Onitilo AA, Engel JM, Stankowski RV, Liang H,Berg RL, Doi SA. High-sensitivity C-reactiveprotein (hs-CRP) as a biomarker for trastuzumab-induced cardiotoxicity in HER2-positive early-stage breast cancer: a pilot study. Breast CancerRes Treat 2012;134:291–8.
119. Sendur MA, Aksoy S, Yorgun H, et al.Comparison of the long term cardiac effects
associated with 9 and 52 weeks of trastuzumabin HER2-positive early breast cancer. Currentmedical research and opinion 2015;31:547–56.
120. de Boer RA, Voors AA, Muntendam P, vanGilst WH, van Veldhuisen DJ. Galectin-3: a novelmediator of heart failure development andprogression. Eur J Heart Fail 2009;11:811–7.
121. Feola M, Garrone O, Occelli M, et al.Cardiotoxicity after anthracycline chemotherapyin breast carcinoma: effects on left ventricularejection fraction, troponin I and brain natriureticpeptide. Int J Cardiol 2011;148:194–8.
122. Armenian SH, Gelehrter SK, Vase T, et al.Screening for cardiac dysfunction in anthracycline-exposed childhood cancer survivors. Clin CancerRes 2014;20:6314–23.
123. Slamon D, Eiermann W, Robert N, et al.Adjuvant trastuzumab in HER2-positive breastcancer. N Engl J Med 2011;365:1273–83.
124. Poole CJ, Earl HM, Hiller L, et al. Epirubicinand cyclophosphamide, methotrexate, and fluo-rouracil as adjuvant therapy for early breastcancer. N Engl J Med 2006;355:1851–62.
125. Li X, Xu S, Tan Y, Chen J. The effects ofidarubicin versus other anthracyclines for induc-tion therapy of patients with newly diagnosedleukaemia. Cochrane Database Syst Rev 2015:CD010432.
126. van Dalen EC, Michiels EM, Caron HN,Kremer LC. Different anthracycline derivates forreducing cardiotoxicity in cancer patients.Cochrane Database Syst Rev 2010:CD005006.
127. Minotti G, Menna P, Salvatorelli E, Cairo G,Gianni L. Anthracyclines: molecular advancesand pharmacologic developments in antitumoractivity and cardiotoxicity. PharmacolRev 2004;56:185–229.
128. van Dalen EC, van der Pal HJ, Kremer LC.Different dosage schedules for reducing car-diotoxicity in people with cancer receivinganthracycline chemotherapy. Cochrane DatabaseSyst Rev 2016;3:CD005008.
129. Lipshultz SE, Miller TL, Lipsitz SR, et al.Continuous versus bolus infusion of doxorubicin inchildren with all: long-term cardiac outcomes.Pediatrics 2012;130:1003–11.
130. Lipshultz SE, Cochran TR, Franco VI,Miller TL. Treatment-related cardiotoxicity insurvivors of childhood cancer. Nat Rev Clin Oncol2013;10:697–710.
131. Gupta M, Steinherz PG, Cheung NK,Steinherz L. Late cardiotoxicity after bolus versusinfusion anthracycline therapy for childhoodcancers. Med Pediatr Oncol 2003;40:343–7.
132. Levitt GA, Dorup I, Sorensen K, Sullivan I.Does anthracycline administration by infusion inchildren affect late cardiotoxicity? Br J Haematol2004;124:463–8.
133. Pignata S, Scambia G, Ferrandina G, et al.Carboplatin plus paclitaxel versus carboplatin pluspegylated liposomal doxorubicin as first-linetreatment for patients with ovarian cancer: theMITO-2 randomized phase III trial. J Clin Oncol2011;29:3628–35.
134. Sharpe M, Easthope SE, Keating GM,Lamb HM. Polyethylene glycol-liposomal

Chang et al. J A C C V O L . 7 0 , N O . 2 0 , 2 0 1 7
Best Practices in Cardio-Oncology: Part 1 N O V E M B E R 1 4 / 2 1 , 2 0 1 7 : 2 5 3 6 – 5 1
2550
doxorubicin: a review of its use in the managementof solid and haematological malignancies andAIDS-related Kaposi’s sarcoma. Drugs 2002;62:2089–126.
135. Al-Batran SE, Guntner M, Pauligk C, et al.Anthracycline rechallenge using pegylated lipo-somal doxorubicin in patients with metastaticbreast cancer: a pooled analysis using individualdata from four prospective trials. Br J Cancer2010;103:1518–23.
136. Keller AM, Mennel RG, Georgoulias VA, et al.Randomized phase III trial of pegylated liposomaldoxorubicin versus vinorelbine or mitomycin Cplus vinblastine in women with taxane-refractoryadvanced breast cancer. J Clin Oncol 2004;22:3893–901.
137. O’Brien ME, Wigler N, Inbar M, et al. Reducedcardiotoxicity and comparable efficacy in a phaseIII trial of pegylated liposomal doxorubicin HCl(CAELYX/Doxil) versus conventional doxorubicinfor first-line treatment of metastatic breast can-cer. Ann Oncol 2004;15:440–9.
138. Gordon AN, Fleagle JT, Guthrie D, Parkin DE,Gore ME, Lacave AJ. Recurrent epithelial ovariancarcinoma: a randomized phase III study of pegy-lated liposomal doxorubicin versus topotecan.J Clin Oncol 2001;19:3312–22.
139. Mutch DG, Orlando M, Goss T, et al. Ran-domized phase III trial of gemcitabine comparedwith pegylated liposomal doxorubicin in patientswith platinum-resistant ovarian cancer. J ClinOncol 2007;25:2811–8.
140. Pujade-Lauraine E, Wagner U, Aavall-Lundqvist E, et al. Pegylated liposomal Doxoru-bicin and Carboplatin compared with Paclitaxeland Carboplatin for patients with platinum-sensitive ovarian cancer in late relapse. J ClinOncol 2010;28:3323–9.
141. Duggan ST, Keating GM. Pegylated liposomaldoxorubicin: a review of its use in metastaticbreast cancer, ovarian cancer, multiple myelomaand AIDS-related Kaposi’s sarcoma. Drugs 2011;71:2531–58.
142. Smith DH, Adams JR, Johnston SR, Gordon A,Drummond MF, Bennett CL. A comparative eco-nomic analysis of pegylated liposomal doxorubicinversus topotecan in ovarian cancer in the USA andthe UK. Ann Oncol 2002;13:1590–7.
143. Creighton AM, Birnie GD. The effect of bis-dioxopiperazines on the synthesis of deoxy-ribonucleic acid, ribonucleic acid and protein ingrowing mouse-embryo fibroblasts. Biochem J1969;114:58P.
144. Lyu YL, Kerrigan JE, Lin CP, et al. Topo-isomerase IIbeta mediated DNA double-strandbreaks: implications in doxorubicin cardiotoxicityand prevention by dexrazoxane. Cancer Res 2007;67:8839–46.
145. Marty M, Espie M, Llombart A, et al. Multi-center randomized phase III study of the car-dioprotective effect of dexrazoxane (Cardioxane)in advanced/metastatic breast cancer patientstreated with anthracycline-based chemotherapy.Ann Oncol 2006;17:614–22.
146. Speyer JL, Green MD, Zeleniuch-Jacquotte A,et al. ICRF-187 permits longer treatment with
doxorubicin in women with breast cancer. J ClinOncol 1992;10:117–27.
147. Yu Y, Kalinowski DS, Kovacevic Z, et al. Thi-osemicarbazones from the old to new: iron che-lators that are more than just ribonucleotidereductase inhibitors. J Med Chem 2009;52:5271–94.
148. Swain SM, Vici P. The current and future roleof dexrazoxane as a cardioprotectant in anthra-cycline treatment: expert panel review. J CancerRes Clin Oncol 2004;130:1–7.
149. Seymour L, Bramwell V, Moran LA, for theThe Provincial Systemic Treatment Disease SiteGroup. Use of dexrazoxane as a cardioprotectantin patients receiving doxorubicin or epirubicinchemotherapy for the treatment of cancer. CancerPrev Control 1999;3:145–59.
150. van Dalen EC, Caron HN, Dickinson HO,Kremer LC. Cardioprotective interventions forcancer patients receiving anthracyclines. CochraneDatabase Syst Rev 2008:CD003917.
151. Schuchter LM, Hensley ML, Meropol NJ,Winer EP, American Society of Clinical OncologyChemotherapy and Radiotherapy Expert Panel.2002 update of recommendations for the use ofchemotherapy and radiotherapy protectants:clinical practice guidelines of the American Societyof Clinical Oncology. J Clin Oncol 2002;20:2895–903.
152. Tebbi CK, London WB, Friedman D, et al.Dexrazoxane-associated risk for acute myeloidleukemia/myelodysplastic syndrome and othersecondary malignancies in pediatric Hodgkin’sdisease. J Clin Oncol 2007;25:493–500.
153. Salzer WL, Devidas M, Carroll WL, et al. Long-term results of the pediatric oncology groupstudies for childhood acute lymphoblastic leuke-mia 1984-2001: a report from the Children’sOncology Group. Leukemia 2010;24:355–70.
154. Vrooman LM, Neuberg DS, Stevenson KE,et al. The low incidence of secondary acute mye-logenous leukaemia in children and adolescentstreated with dexrazoxane for acute lymphoblasticleukaemia: a report from the Dana-Farber CancerInstitute ALL Consortium. Eur J Cancer 2011;47:1373–9.
155. Romond EH, Jeong JH, Rastogi P, et al.Seven-year follow-up assessment of cardiacfunction in NSABP B-31, a randomized trialcomparing doxorubicin and cyclophosphamidefollowed by paclitaxel (ACP) with ACP plus tras-tuzumab as adjuvant therapy for patients withnode-positive, human epidermal growth factorreceptor 2-positive breast cancer. J Clin Oncol2012;30:3792–9.
156. Joensuu H, Kellokumpu-Lehtinen PL, Bono P,et al. Adjuvant docetaxel or vinorelbine with orwithout trastuzumab for breast cancer. N Engl JMed 2006;354:809–20.
157. Yancy CW, Jessup M, Bozkurt B, et al. 2017ACC/AHA/HFSA focused update of the 2013 ACCF/AHA Guideline for the Management of HeartFailure: a report of the American College of Car-diology/American Heart Association Task Force onClinical Practice Guidelines and the Heart FailureSociety of America. J Am Coll Cardiol 2017;70:776–803.
158. Yancy CW, Jessup M, Bozkurt B, et al. 2013ACCF/AHA guideline for the management of heartfailure: executive summary: a report of theAmerican College of Cardiology Foundation/American Heart Association Task Force on PracticeGuidelines. J Am Coll Cardiol 2013;62:1495–539.
159. Ewer MS, Lippman SM. Type IIchemotherapy-related cardiac dysfunction: timeto recognize a new entity. J Clin Oncol 2005;23:2900–2.
160. Meyer CC, Calis KA, Burke LB,Walawander CA, Grasela TH. Symptomatic car-diotoxicity associated with 5-fluorouracil. Phar-macotherapy 1997;17:729–36.
161. Van Cutsem E, Hoff PM, Blum JL, Abt M,Osterwalder B. Incidence of cardiotoxicity with theoral fluoropyrimidine capecitabine is typical ofthat reported with 5-fluorouracil. Ann Oncol2002;13:484–5.
162. de Forni M, Malet-Martino MC, Jaillais P,et al. Cardiotoxicity of high-dose continuousinfusion fluorouracil: a prospective clinical study.J Clin Oncol 1992;10:1795–801.
163. Bertolini A, Flumano M, Fusco O, et al. Acutecardiotoxicity during capecitabine treatment: acase report. Tumori 2001;87:200–6.
164. Anand AJ. Fluorouracil cardiotoxicity. AnnPharmacother 1994;28:374–8.
165. Cardinale D, Colombo A, Colombo N. Acutecoronary syndrome induced by oral capecitabine.Can J Cardiol 2006;22:251–3.
166. Jensen SA, Sorensen JB. Risk factors andprevention of cardiotoxicity induced by 5-fluorouracil or capecitabine. Cancer ChemotherPharmacol 2006;58:487–93.
167. Kosmas C, Kallistratos MS, Kopterides P,et al. Cardiotoxicity of fluoropyrimidines indifferent schedules of administration: a prospec-tive study. J Cancer Res Clin Oncol 2008;134:75–82.
168. Labianca R, Beretta G, Clerici M, Fraschini P,Luporini G. Cardiac toxicity of 5-fluorouracil: astudy on 1083 patients. Tumori 1982;68:505–10.
169. Rezkalla S, Kloner RA, Ensley J, et al.Continuous ambulatory ECG monitoring duringfluorouracil therapy: a prospective study. J ClinOncol 1989;7:509–14.
170. Schnetzler B, Popova N, Collao Lamb C,Sappino AP. Coronary spasm induced by capeci-tabine. Ann Oncol 2001;12:723–4.
171. Robben NC, Pippas AW, Moore JO. The syn-drome of 5-fluorouracil cardiotoxicity. An elusivecardiopathy. Cancer 1993;71:493–509.
172. Ng M, Cunningham D, Norman AR. The fre-quency and pattern of cardiotoxicity observedwith capecitabine used in conjunction with oxali-platin in patients treated for advanced colorectalcancer (CRC). Eur J Cancer 2005;41:1542–6.
173. Saif MW, Tomita M, Ledbetter L, Diasio RB.Capecitabine-related cardiotoxicity: recognitionand management. J Support Oncol 2008;6:41–8.
174. Walko CM, Lindley C. Capecitabine: a review.Clin Ther 2005;27:23–44.
175. Frickhofen N, Beck FJ, Jung B, Fuhr HG,Andrasch H, Sigmund M. Capecitabine can induce

J A C C V O L . 7 0 , N O . 2 0 , 2 0 1 7 Chang et al.N O V E M B E R 1 4 / 2 1 , 2 0 1 7 : 2 5 3 6 – 5 1 Best Practices in Cardio-Oncology: Part 1
2551
acute coronary syndrome similar to 5-fluorouracil.Ann Oncol 2002;13:797–801.
176. Papadopoulos CA, Wilson H. Capecitabine-associated coronary vasospasm: a case report.Emerg Med J 2008;25:307–9.
177. Arbuck SG, Strauss H, Rowinsky E, et al.A reassessment of cardiac toxicity associatedwith Taxol. J Natl Cancer Inst Monogr 1993:117–30.
178. Vermorken JB, Remenar E, van Herpen C,et al. Cisplatin, fluorouracil, and docetaxel inunresectable head and neck cancer. N Engl J Med2007;357:1695–704.
179. Sanofi. Taxotere prescribing information.2015. Available at: http://products.sanofi.us/Taxotere/taxotere.pdf. Accessed December 1,2015.
180. Scappaticci FA, Skillings JR, Holden SN, et al.Arterial thromboembolic events in patients withmetastatic carcinoma treated with chemotherapyand bevacizumab. J Natl Cancer Inst 2007;99:1232–9.
181. Kozloff M, Yood MU, Berlin J, et al. Clinicaloutcomes associated with bevacizumab-containing treatment of metastatic colorectalcancer: the BRiTE observational cohort study.Oncologist 2009;14:862–70.
182. MooreMJ, Goldstein D, Hamm J, et al. Erlotinibplus gemcitabine compared with gemcitabine alonein patients with advanced pancreatic cancer: a phaseIII trial of the National Cancer Institute of CanadaClinical Trials Group. J Clin Oncol 2007;25:1960–6.
183. U.S. Food and Drug Administration. Tarceva(erlotinib) label. 2010. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/021743s14s16lbl.pdf. Accessed April 1, 2010.
184. Bayer HealthCare Pharmaceuticals. Sorafenib(Nexavar) package insert. 2013. Available at: http://labeling.bayerhealthcare.com/html/products/pi/Nexavar_PI.pdf. Accessed November 1, 2013.
185. Escudier B, Eisen T, Stadler WM, et al. Sor-afenib in advanced clear-cell renal-cell carcinoma.N Engl J Med 2007;356:125–34.
186. Siegel D, Martin T, Nooka A, et al. Integratedsafety profile of single-agent carfilzomib: experi-ence from 526 patients enrolled in 4 phase IIclinical studies. Haematologica 2013;98:1753–61.
187. Stewart AK, Rajkumar SV, Dimopoulos MA,et al. Carfilzomib, lenalidomide, and dexametha-sone for relapsed multiple myeloma. N Engl J Med2015;372:142–52.
188. Amgen. Kyprolis (carfilzomib). Prescribinginformation. 2017. Available at: http://pi.amgen.com/w/media/amgen/repositorysites/pi-amgen-com/kyprolis/kyprolis_pi.ashx. Accessed May 1, 2017.
189. Shoemaker LK, Arora U, Rocha Lima CM.5-fluorouracil-induced coronary vasospasm.Cancer Control 2004;11:46–9.
190. Mosseri M, Fingert HJ, Varticovski L,Chokshi S, Isner JM. In vitro evidence thatmyocardial ischemia resulting from 5-fluorouracilchemotherapy is due to protein kinase C-medi-ated vasoconstriction of vascular smooth muscle.Cancer Res 1993;53:3028–33.
191. Cwikiel M, Eskilsson J, Albertsson M,Stavenow L. The influence of 5-fluorouracil andmethotrexate on vascular endothelium. Anexperimental study using endothelial cells in theculture. Ann Oncol 1996;7:731–7.
192. Cwikiel M, Eskilsson J, Wieslander JB,Stjernquist U, Albertsson M. The appearance ofendothelium in small arteries after treatment with5-fluorouracil. An electron microscopic study oflate effects in rabbits. Scanning Microsc 1996;10:805–18; discussion 819.
193. Cwikiel M, Zhang B, Eskilsson J,Wieslander JB, Albertsson M. The influence of 5-fluorouracil on the endothelium in small arteries.An electron microscopic study in rabbits. ScanningMicrosc 1995;9:561–76.
194. Jensen SA, Sorensen JB. 5-fluorouracil-basedtherapy induces endovascular injury having po-tential significance to development of clinicallyovert cardiotoxicity. Cancer Chemother Pharmacol2012;69:57–64.
195. Kinhult S, Albertsson M, Eskilsson J,Cwikiel M. Antithrombotic treatment in protectionagainst thrombogenic effects of 5-fluorouracil onvascular endothelium: a scanning microscopyevaluation. Scanning 2001;23:1–8.
196. Rowinsky EK, McGuire WP, Guarnieri T,Fisherman JS, Christian MC, Donehower RC. Car-diac disturbances during the administration oftaxol. J Clin Oncol 1991;9:1704–12.
197. Kamba T, McDonald DM. Mechanisms ofadverse effects of anti-VEGF therapy for cancer.Br J Cancer 2007;96:1788–95.
198. Kilickap S, Abali H, Celik I. Bevacizumab,bleeding, thrombosis, and warfarin. J Clin Oncol2003;21:3542, author reply 3543.
199. Chen-Scarabelli C, Corsetti G, Pasini E, et al.Spasmogenic effects of the proteasome inhibitorcarfilzomib on coronary resistance, vascular toneand reactivity. EBioMedicine 2017;21:206–12.
200. Amsterdam EA, Wenger NK, Brindis RG, et al.2014 AHA/ACC guideline for the management ofpatients with non-ST-elevation acute coronarysyndromes: a report of the American College ofCardiology/American Heart Association Task Forceon Practice Guidelines. J Am Coll Cardiol 2014;64:e139–228.
201. O’Gara PT, Kushner FG, Ascheim DD, et al.2013 ACCF/AHA guideline for the managementof ST-elevation myocardial infarction: areport of the American College of CardiologyFoundation/American Heart Association TaskForce on Practice Guidelines. J Am Coll Cardiol2013;61:e78–140.
202. Sarkiss MG, Yusuf SW, Warneke CL, et al.Impact of aspirin therapy in cancer patients withthrombocytopenia and acute coronary syndromes.Cancer 2007;109:621–7.
203. Iliescu C, Durand JB, Kroll M. Cardiovascularinterventions in thrombocytopenic cancer pa-tients. Tex Heart Inst J 2011;38:259–60.
204. Iliescu CA, Grines CL, Herrmann J, et al. SCAIexpert consensus statement: evaluation, man-agement, and special considerations of cardio-oncology patients in the cardiac catheterizationlaboratory (endorsed by the Cardiological Societyof India, and Sociedad Latino Americana de Car-diologia Intervencionista). Catheter CardiovascInterv 2016;87:E202–23.
205. Genentech Inc. Avastin (bavacizumab) label–prescribing information. 2016. Available at:https://www.gene.com/download/pdf/avastin_prescribing.pdf. Accessed December 1, 2016.
KEY WORDS cancer therapy,cardiomyopathy, cardiovascularcomplication, ischemia