carlos s. morales, md; foula kontonicolas md; anita volpe dnp; pierre f. saldinger md, facs royd...
TRANSCRIPT

Carlos S. Morales, MD; Foula Kontonicolas MD; Anita Volpe DNP; Pierre F. Saldinger MD, FACS Royd Fukumoto, MD, FACS
Department of Surgery and Department of Performance ImprovementDanbury Hospital, Danbury CT
Performance Improvement: Getting an Early Start


INTRODUCTION
• NSQIP - a measurement of surgical outcomes Why NSQIP for PI? - Standard methodology for abstraction and collection of data - Allows for equitable comparison of variables - Enables honest evaluation of system process
• SCIP - process measure– Timing of VTE or antibiotic prophylaxis

METHODS
• Resident Champion (RC) was started in July 2010, as a way to introduce residents to NSQIP/SCIP
NSQIP
1. Identify target2. Deep dive3. Identify involved
services4. Create taskforce5. Create action plan6. Implementation7. Monitor and
validate

METHODS
• The RC presents timely feedback on NSQIP and SCIP performance to other residents at our weekly residency program meeting
• The RC participates in multidisciplinary committees

• Residents as active participants of PI
• ACGME– Systems Based practice – Practice Based Learning and Improvement– Medical Knowledge– Patient Care– Professionalism– Interpersonal and communications skills

RESULTS
• Surgical Progress Note
• Accelerated computer tomography of the abdomen and pelvis (ACTAP)
• Modified risk assessment tool (MRAT) for VTE prevention

Surgical Progress Note• Incorporates 5 of the 10 core SCIP measures that are
pertinent to general surgery
- Appropriate antibiotic prophylaxis- Prophylactic antibiotics discontinued within 24 hours of surgery- Urinary catheter removed on postoperative day 2- Appropriate perioperative temperature management- Appropriate VTE prophylaxis
Increased SCIP compliance to 100% in those 5 measures over last quarter
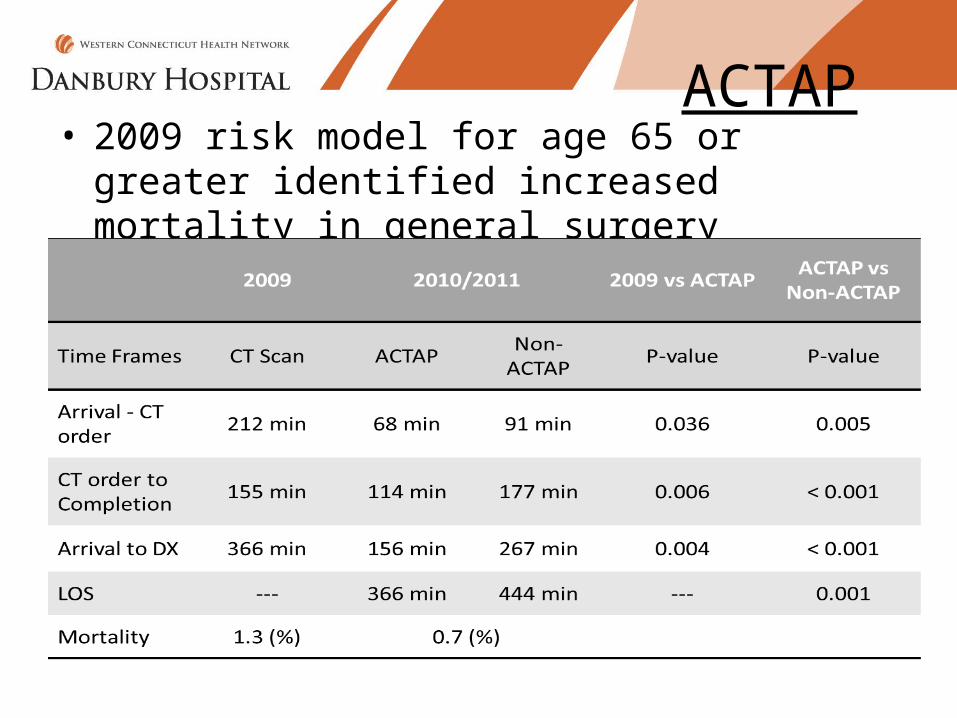
ACTAP• 2009 risk model for age 65 or greater identified
increased mortality in general surgery

MRAT
• In 2010, we were failing VTE SCIP measures, our O/E 1.14
• 48 patients with VTE were identified - 48% had inadequate prophylaxis based on
current guidelines
• MRAT

MRAT• Validation of the tool
• MRAT and the Caprini model was applied to 1000 patients
1.1% had a VTE score that differed from Caprini’s 0.1% would have required a change in prophylaxis
• O/E- 0.95

ConclusionsACGME Competencies
Practice-Based Learning and Improvement
Using NSQIP / SCIP data for performance improvement
Medical Knowledge Science supporting SCIP measuresScience supporting VTE prophylaxisPotential catastrophic events behind acute abdominal pain
Systems-based Practice Developing system wide protocols to address VTE prophylaxis and acute abdominal pain
Interpersonal and Communication Skills NSQIP / SCIP liaison to surgical residencyParticipation in multi-disciplinary committees
Professionalism Interaction with other physician departments and nursing in formulating and carrying out initiatives
Patient Care SCIP measures and relation to outcomesChanges in VTE ratesChanges in mortality in patients with abdominal pain