case 31a & b - virtual pathology at the university of leeds€¦ · · 2014-09-02case 31a...
TRANSCRIPT

Case 31A & B
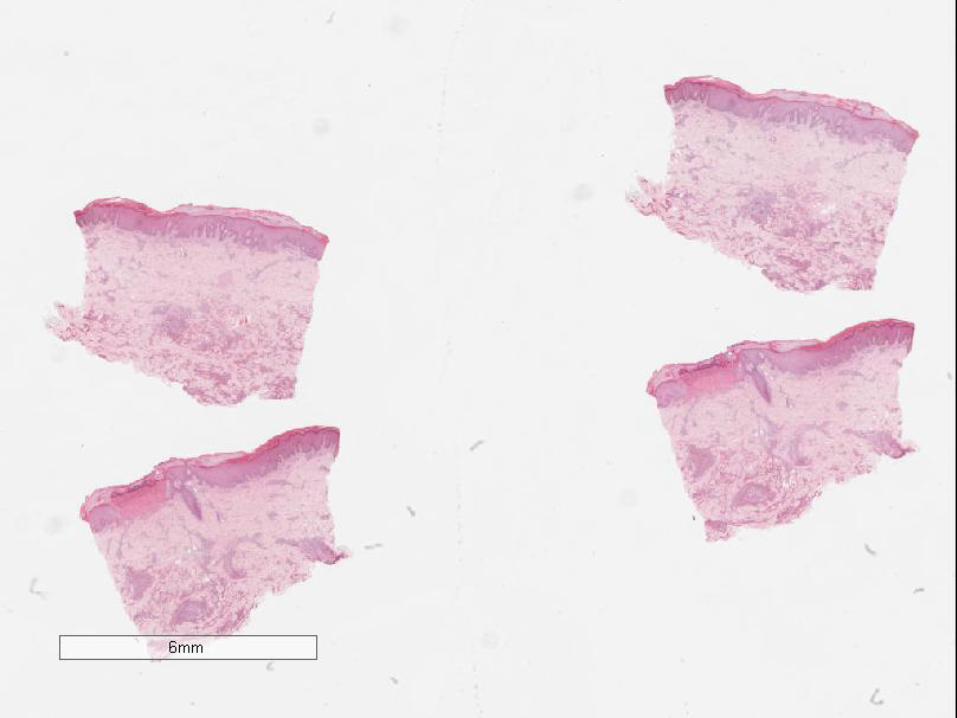
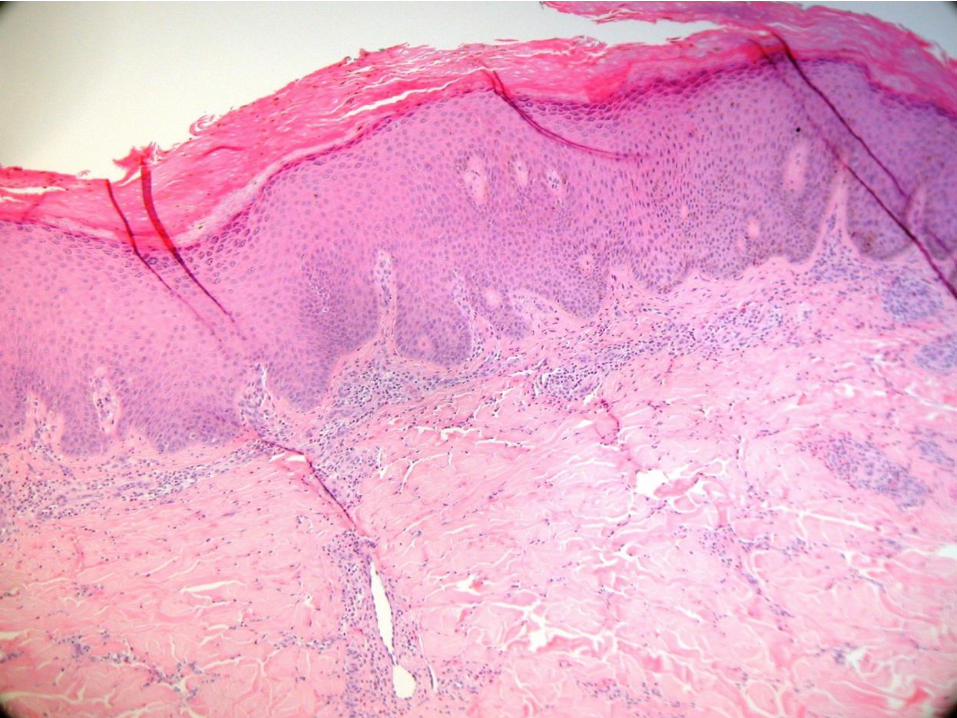
Male 30. Infiltrated scalp nodules and neck
lymphadenopathy for 6 months. Biopsy of
skin (A) and lymph node (B).
The best diagnosis is:
A. Haemangioma
B. Kimura disease
C. Kaposi’s sarcoma
D. Hodgkin’s lymphoma
E. Rosai-Dorfman disease

Initial presentation in community
• 31 year old Jamaican man
• Arrived in UK Nov 2010
• Presented Oct 2011 to GP
• Pruritic nodular prurigo-like rash
• Treated with Ivermectin for ? Scabies
• Incisional biopsy from lesion R thigh



• WCC 31.6 x 109/L
• Eosinophils 24 x
109/L
• Syphilis
• HIV
• Hep B+C
• ANA
• ENA
• UE
• LFT
• Stool
• Parasitic screen
• Urine dip






Case 31
Male 30. Infiltrated scalp nodules and neck
lymphadenopathy for 6 months. Biopsy of
skin (A) and lymph node (B).
The best diagnosis is:
A. Haemangioma
B. Kimura disease
C. Kaposi’s sarcoma
D. Hodgkin’s lymphoma
E. Rosai-Dorfman disease
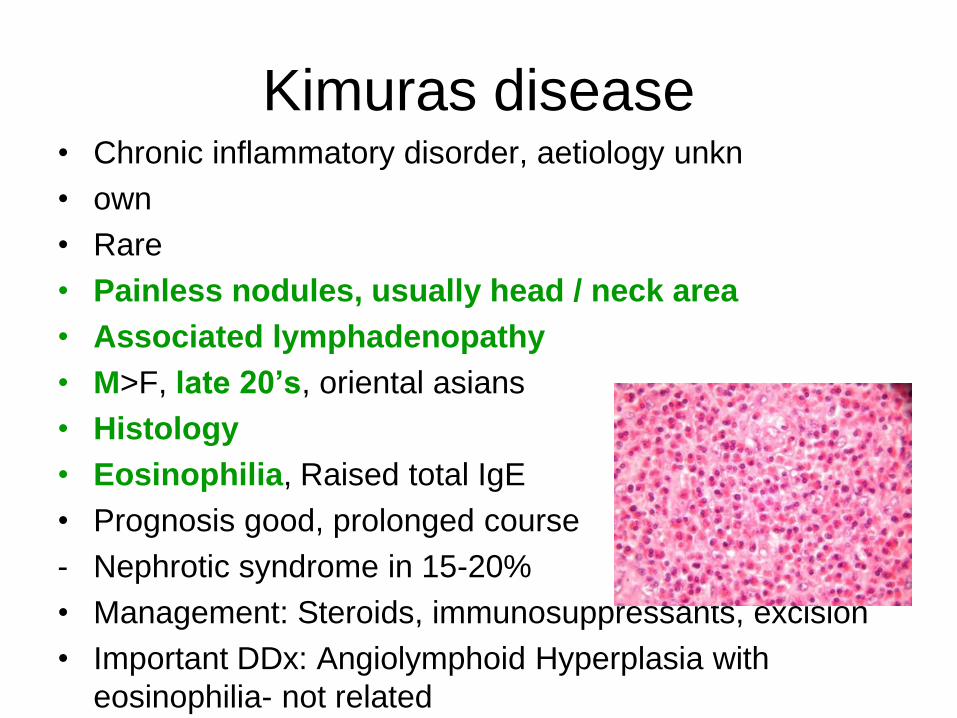
Kimuras disease • Chronic inflammatory disorder, aetiology unkn
• own
• Rare
• Painless nodules, usually head / neck area
• Associated lymphadenopathy
• M>F, late 20’s, oriental asians
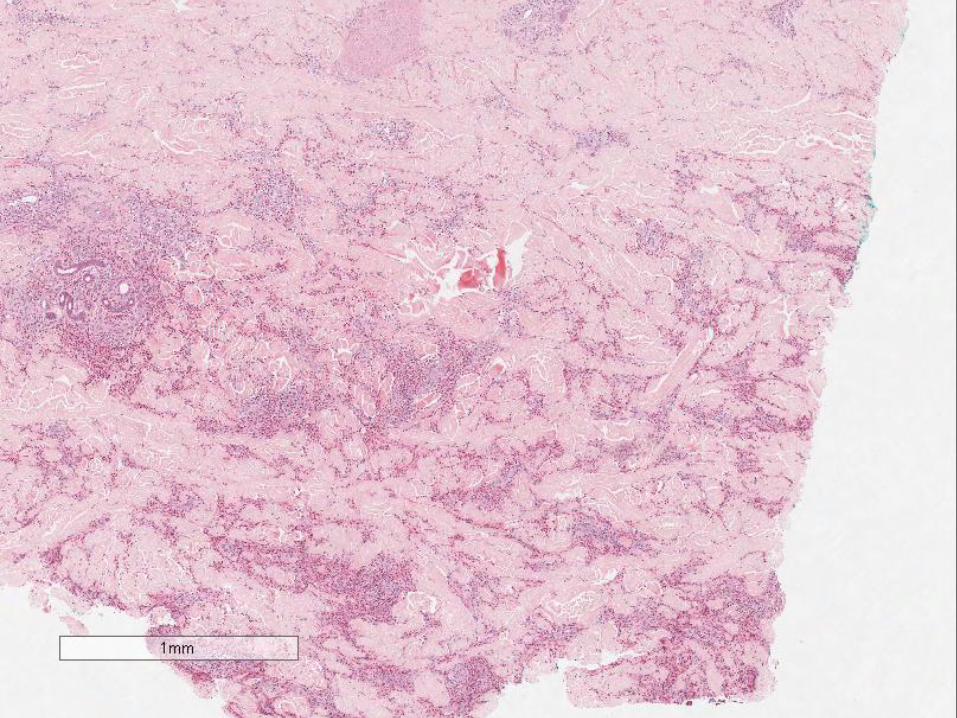
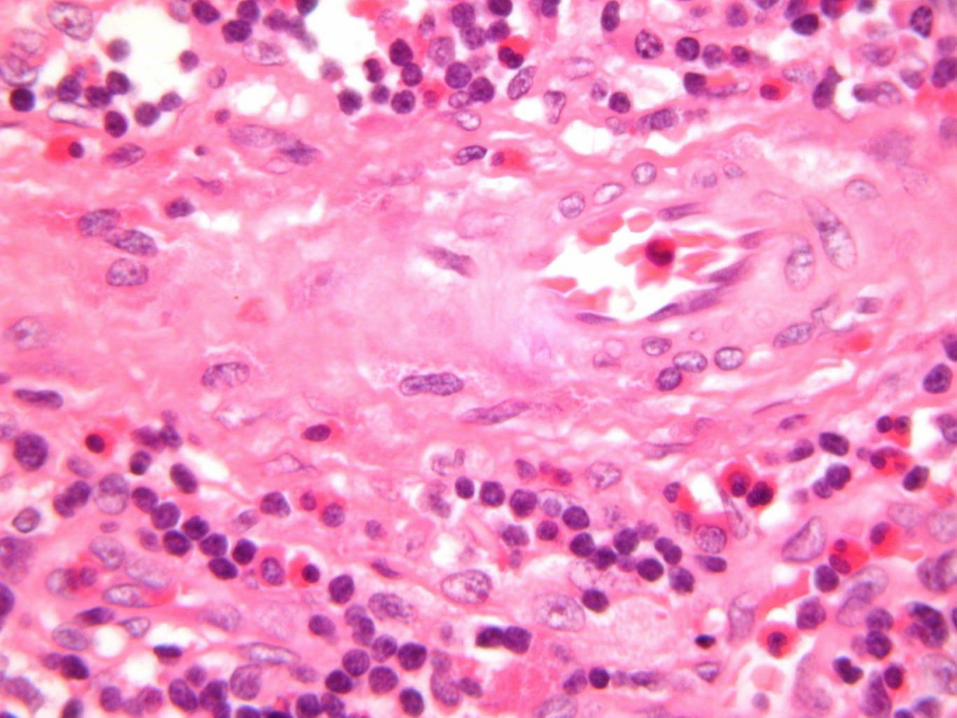
• Histology
• Eosinophilia, Raised total IgE
• Prognosis good, prolonged course
- Nephrotic syndrome in 15-20%
• Management: Steroids, immunosuppressants, excision
• Important DDx: Angiolymphoid Hyperplasia with
eosinophilia- not related
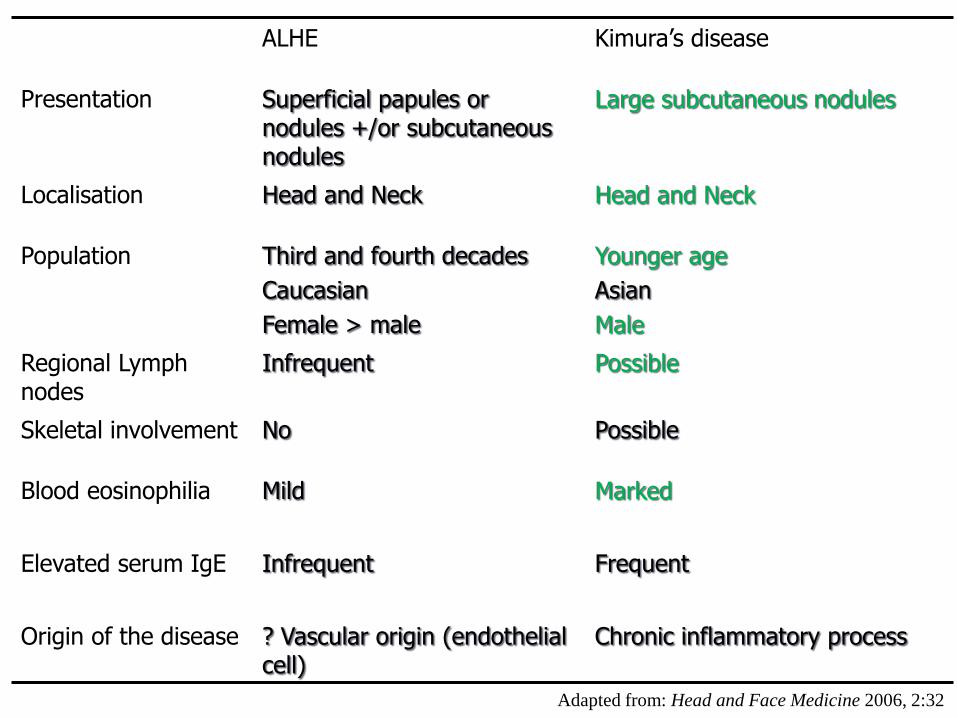
ALHE Kimura’s disease
Presentation Superficial papules or nodules +/or subcutaneous nodules
Large subcutaneous nodules
Localisation Head and Neck Head and Neck
Population Third and fourth decades
Caucasian
Female > male
Younger age
Asian
Male
Regional Lymph nodes
Infrequent Possible
Skeletal involvement No Possible
Blood eosinophilia
Mild Marked
Elevated serum IgE Infrequent
Frequent
Origin of the disease ? Vascular origin (endothelial cell)
Chronic inflammatory process
Adapted from: Head and Face Medicine 2006, 2:32

Differential Diagnoses
• Inflammatory angiomatous nodules
• ALHE
• Pyogenic granuloma
• Histiocytoid haemangioma
• Kaposi’s sarcoma
• Pseudolymphoma (lymphoid hyperplasia)
• Cutaneous lymphoma
• Kimura disease – different entity!! Not
ALHE