case studies: balancing a dynamic wound environment
TRANSCRIPT
Balancing a Dynamic Wound Environment: Multicenter Experience with a Novel Antimicrobial Foam Dressing Containing PHMB
March 2009
Supplement to
OWMO S T O M Y W O U N D M A N A G E M E N T
This ancillary publication is provided as a courtesy to Ostomy Wound Management through a grant from Covidien. This publicationwas not subject to the Ostomy Wound Management peer-review process.
Supplement to OWM • March 2009 3
Table of Contents
4 Moderator’s IntroductionCarolyn Cuttino, RN, BS, CWOCN
8 Survey Summary: Open-Label Customer Acceptance andPreference Evaluation of KendallTM AMD Antimicrobial Foam
Dressings
10 Antimicrobial Foam Dressings on Moderately to HeavilyDraining Wounds Treated in Home Health Care
Bridget Mejza, RN, BSN, CWOCN
11 Addressing Redness, Soreness, and Increased Drainagefrom Tube Sites Using an Antimicrobial Foam Dressing
Susan Krause, RN, MSN, CWOCN
13 Changing Healing Trajectory of a Postsurgical WoundUsing Topical Polyhexamethylene Biguanide-Impregnated
Antimicrobial Foam Dressing: A Case StudyMarek K. Dobke, MD
16 Antimicrobial Foam Dressing Used in the Treatment of aDiabetic Foot UlcerRobert Feldman, DPM
18 Inhibiting Bacterial Growth in Venous Ulcers Using an Antimicrobial Foam Dressing
Mary Foote, RN, MSN, CANP, CWCN, ED.Dc
20 Antimicrobial Foam Dressing Used in the Treatment of Wounds in Patients With Compromised Vascular
and Arterial SufficiencyMark T. Herrington, FNP-C
22 Moderator’s Final CommentaryCarolyn Cuttino, RN, BS, CWOCN
EDITORIAL STAFFCLINICAL EDITOR Lia van Rijswijk, RN, MSN,CWCN
EDITOR Barbara C. Zeiger
ASSOCIATE EDITOR Chimere G. Holmes
EDITORIAL ASSISTANT Lauren Grant
SPECIAL PROJECTS EDITOR Stephanie Wasek
BUSINESS STAFFEXECUTIVE VICE PRESIDENT Peter Norris
VICE PRESIDENT/PUBLISHER Jeremy [email protected] NATIONAL SALES MANAGERS Adrian Hoppel [email protected]
Matthew [email protected]
NATIONAL SALES ASSOCIATES Kristen [email protected]
CLASSIFIED SALES ASSOCIATE Erin Fehr
CIRCULATION MANAGER Bonnie Shannon
HMP COMMUNICATIONS, LLCPRESIDENT Bill Norton
CONTROLLER Meredith Cymbor-Jones
CREATIVE DIRECTOR Vic Geanopulos
PRODUCTION MANAGER Elizabeth McTamney
PRODUCTION/CIRCULATION DIRECTOR Kathy Murphy
AUDIENCE DEVELOPMENT MANAGER Bill Malriat
HUMAN RESOURCES Anita Dallasta
MEETING PLANNER Tracy Nocks
MEETING PLANNER Mary Beth Pollart
MANAGER OF WEB DEVELOPMENT Tim Shaw
MANAGER OF INFORMATION SERVICES Fred Klumpp
HMP COMMUNICATIONS HOLDINGS, LLCCHAIRMAN & CHIEF EXECUTIVE OFFICER Paul Mackler
PRESIDENT & CHIEF OPERATING OFFICER Jeff Hennessy
CHIEF FINANCIAL OFFICER Ken Fisher
83 General Warren Blvd.Suite 100 Malvern, PA 19355 (800) 237-7285
Ostomy Wound Management (ISSN 0889-5899) is published monthly byHMP Communications, 83 General Warren Boulevard, Suite 100,Malvern, PA 19355; phone: (800) 237-7285;e-mail: [email protected].
Postmaster: Send address changes to Ostomy Wound Management, 83 General Warren Blvd.; Suite 100; Malvern, PA 19355 Periodicals postage paid at Malvern, PA and at additional mailing offices.
Change of Address: For change of address, mail your old and new address to:HMP Communications; OWM Subscriptions83 General Warren Boulevard, Suite 100; Malvern, PA 19355or fax to OWM Subscriptions at: (610) 560-0502
Subscriptions: U.S. $75.00 for one year. International $115.00Single or replacement copies: U.S. $14.50; International $17.50Call 1-800-237-7285, ext 5 for the Subscription Dept.or E-mail: [email protected].(Mail subscription requests to the address above)
HMP Communications LLC (HMP) is the authoritative source for compre-hensive information and education servicing healthcare professionals.HMP’s products include peer-reviewed and non-peer-reviewed medicaljournals, national tradeshows and conferences, online programs and cus-tomized clinical programs. HMP is a wholly owned subsidiary of HMPCommunications Holdings LLC. Discover more about HMP’s products andservices at: www.hmpcommunications.com.
© 2009, HMP Communications, LLC, (HMP). All rights reserved. Reproductionin whole or in part prohibited. Opinions expressed by authors, contributors, andadvertisers are their own and not necessarily those of HMP Communications,the editorial staff, or any member of the editorial advisory board. HMP Commu-nications is not responsible for accuracy of dosages given in articles printedherein. The appearance of advertisements in this journal is not a warranty, en-dorsement or approval of the products or services advertised or of their effec-tiveness, quality or safety. HMP Communications disclaims responsibility for anyinjury to persons or property resulting from any ideas or products referred to inthe articles or advertisements. Content may not be reproduced in any form with-out written permission. Rights, Permission, Reprint and Translation informationis available at www.hmpcommunications.com.
LLC,
OWMO S T O M Y W O U N D M A N A G E M E N T

Balancing a Dynamic Wound Environment
4 Supplement to OWM • March 2009
Chronic wounds are a financialburden to the healthcare sys-tem and impact the quality of
life of people who must live with them dayaer day, month aer month, or even yearaer year. Chronic wounds will continueto drive rising healthcare costs as the pop-ulation ages and chronic diseases that con-tribute to wound development increase inprevalence. Chronic wounds are a chal-lenge to all healthcare workers.
Healthcare providers in all sites of serv-ice are challenged by today’s changing en-vironment. Pay-for-performance is here,and Medicare is taking the lead to ensurequality care for beneficiaries. Medicare nolonger will pay for many conditions con-sidered preventable when best practicesare followed. In this pay-for-performanceenvironment, clinical and financial successwill depend on the ability of the providerto prevent wounds and wound complica-tions, and provide interventions that willfacilitate healing. Acute care facilities nolonger can bill for services related to thecare of patients who develop pressure ul-cers aer admission or for some surgicalwound infections that develop during ahospital stay. is can be an importantissue in a hospital’s bottom line when pos-sibly 15% of elective surgery cases and30% of contaminated surgeries lead tohealthcare-associated infections that pro-long stays and increase treatment costs.1
Pay-for-performance quality indicators are
also being developed in the skilled andhome care arenas. Pressure ulcers, wound in-fections, dehydration, and urinary tract in-fections are some of the clinical conditionsbeing considered as monitors for qualitycare in these settings. Adequately managingthese conditions hopefully will prevent un-necessary emergency room visits and hospi-talizations and help decrease the financialimpact of these conditions. All sites of serv-ice must focus on proactive, preventive careand evidence-based management. Regard-less of setting, clinicians must be able to pro-vide management strategies for the chronicwound that will do more than just treat. In-terventions must include strategies thatcost-effectively forestall complications andpromote healing.
Another major factor affecting chronicwound care is the emergence of infectionsthat are antibiotic-resistant. Healthcare-associated methicillin-resistant Staphylo-coccus aureus (HA-MRSA) andcommunity-acquired methicillin-resistantS. aureus (CA-MRSA) are occurring inepidemic proportions, prompting clini-cians to look for ways to prevent and man-age potential wound infectionscost-effectively.
Cost-effective wound managementmeans closing the wound as soon as pos-sible. This can be accomplished by early,accurate diagnoses to determine etiolo-gies and dictate appropriate managementmodalities; and by prompt, aggressive
topical care that can modify the alteredchronic wound environment and preventcomplications such as infection. For treat-ment to be effective, the wound bed mustbe prepared to heal: devitalized tissue re-moved, wound bioburden controlled,moisture managed, and adjunctive modal-ities utilized when necessary.
Bioburden ControlAlthough chronic wounds are fre-
quently contaminated or colonized withbacteria, many go on to heal without com-plications. However, when a balance can-not be maintained between the host andquantity and virulence of bacteria, healingis delayed. High bacterial counts increasemetabolic demands and affect the amountof oxygen available to the wound, whichinterferes with healing. e clinician mustbe able to recognize this imbalance and in-tervene with strategies that will managethe high bioburden present.
Obvious signs of high bacterial countsmanifest in the classical clinical symptomsof a local infection: redness, edema,warmth, pain, and purulent drainage.However, some wounds with high bacte-rial counts do not exhibit the classicalsymptoms of infection. ese woundsmay have the following characteristics: fri-able granulation tissue, increased odor/ordrainage, increased pain, wound deterio-ration, and a plateaued or nonhealingstate. Wounds with these characteristics
Moderator’s Introduction
Carolyn Cuttino, RN, BS, CWOCN, Medical University of South Carolina, Charleston, SC

Supplement to OWM • March 2009 5
have been coined “critically colonized”and represent a potentially infected, non-healing wound. Including these woundcharacteristics in routine assessment mayhelp in the earlier identification of poten-tial infection. Many recognized wound-treatment guidelines recommendremoving nonviable or necrotic tissue thatharbors micro-organisms and using a top-ical antimicrobial dressing to manage bac-terial imbalance and return the wound toa healthy, healing environment.
In addition, it’s my experience that mostchronic wounds are polymicrobial, con-taining multiple species of micro-organ-isms. is is a concern because thesynergistic relationship among multiplespecies may determine the virulence of theorganisms present in the wound. enumber or quantity and the virulence, aswell as the host resistance, determine thepotential for infection. e most impor-tant indicator of a local or systemic oreven covert infection as described in “crit-ical colonization” is the host response tothe prevalence and virulence of the bacte-ria present in the wound. Patients with co-morbidities and conditions known tonegatively affect healing (eg, diabetes, im-munosuppression, advanced age, and end-stage diseases) will be at increased risk forwound infections. Patients requiring cer-tain medications or those with poor circu-lation and perfusion problems also will beat risk. Further, many patients in the afore-mentioned group may not be able tomount an inflammatory response thatwould demonstrate possible overt signs ofinfection. Many patients with wound in-fections may go undiagnosed if only theusual signs and symptoms of infection are
used in the assessment. is underscoresthe need for the clinician to recognizeclues as to why the wound may be slow ornonhealing and to implement appropriatestrategies for bioburden control, such asappropriate antimicrobial dressings.
• Systemic approaches to infectioncontrol. Evidence-based guidelines forbioburden control are lacking, perhapsdue to the difficulty in conducting con-trolled studies in chronic wounds or per-haps inconsistent interpretation ofavailable data. e subject does seem to bemired in controversy, oen leaving clini-cians at a loss for the correct approach.Literature reviews by O’Meara et al andHutchison et al suggest that evidence forusing systemic antibiotics in chronicwound healing is insufficient and demandthat other criteria be used in guiding theuse of systemic antibiotics.2 ere aremany recommendations based on expertopinion regarding the benefit of early in-tervention with systemic broad-spectrumantibiotics for suspected infections in di-abetic foot ulcer.3 e CDC warns againstindiscriminately using antibiotics, espe-cially those with broad-spectrum activity,because they tend to generate antibioticresistance. ese findings point to theneed to consider wound cultures if sys-temic antibiotics are to be prescribed. ASwedish audit revealed that 60.1% ofchronic wound patients had received an-tibiotic therapy during a 6-month surveyperiod.2 ere is a fragile balance betweenprescribing antibiotics for chronic woundsand the risks of developing antibiotic re-sistant organisms. e worldwide out-break of HA-MRSA and CA-MRSA isextremely concerning and one reason
clinicians continuously look for other ef-fective treatments to manage woundbioburden. Adding dressings to controlsurface bacteria seems like a logical ap-proach in conjunction with systemic ther-apy and should be considered as part ofthe management equation. More researchon antibiotics and wound bioburden inchronic wounds is needed.
• Topical strategies. e clinician man-aging an individual with a chronic woundmust choose the topical therapy that willbest meet the needs of the patient andwound. Topical therapy must address re-moval of necrotic/avascular tissue, bacterialbalance and moisture balance. Debride-ment can be accomplished in many waysand rids the wound of devitalized tissue,senescent cells, and also decreases surfacebacteria. Moisture balance is important, aswounds heal faster in a controlled moist en-vironment; this is accomplished by selectingthe dressing that addresses the wound’scharacteristics. Dressings can donate mois-ture, assist with moisture retention, or ab-sorb excessive exudates. Managing woundbioburden becomes critical when the sur-face bacteria are out of bacterial balance andthe clinical symptoms of critical coloniza-tion are present. e widespread problem ofantibiotic resistance and the controversy inthe healthcare community as to the causeand remedy of the situation dictate that theclinician make decisions based on each pa-tient’s needs, risk factors, dressing capabili-ties, environment, resources, and care goals.In managing wound bioburden, the goal isto prevent critical colonization and/or in-fection and facilitate a healthy wound en-vironment. Another consideration is theaforementioned increasing problem of

Balancing a Dynamic Wound Environment
6 Supplement to OWM • March 2009
HA-MRSA and CA-MRSA in chronicwounds, which demands rigorous barriertechniques to avoid cross-contamination.Although local wound care for MRSA in aninfected or nonhealing wound gets little at-tention, it would seem logical that control-ling the organism in the wound bed ordressing would decrease the bacterial loadand diminish cross-contamination poten-tial. Clinicians need to consider this a keystrategy in preventing the spread of organ-isms that contribute to wound infections.
Topical antimicrobials. Using systemictherapy to control bioburden is controversial,and current wound care literature presentsconflicting data on use of topical antimicro-bial strategies in wound management.
Antibiotics. Landis4 discusses concernswith topical antibiotics causing antimicro-bial resistance, host sensitivities and contactdermatitis. Controlled trials support the useof topical mupirocin for S. aureus andGroup A beta hemolytic Streptococcus.Rodeheaver5 supports using some topical an-tibiotics when an antimicrobial agent isdeemed necessary to reduce bacterial levelsin wounds (mafenide acetate, metroniadi-zole, mupirocin, Polysporin, silver sulfadi-azine, and nitrofurazone). Clinicians oenuse alternative antibacterial strategies due toincreasing concerns of resistance and effortsto restrict the prophylactic use of antibiotics.
Antiseptics. Antiseptics are much lesslikely to generate resistance because they tar-get multiple sites. However, cell toxicity andefficacy are major concerns, and literaturereviews oen present differing interpreta-tions. Some traditional antiseptics (hydro-gen peroxide, acetic acid, iodine, andDakins) have conflicting data and should beused with caution. Considerations such as
dosing, concentration, and exposure timemust be balanced against potential harm-ful effects when seeking to control bacte-ria in wounds. In a wound that does nothave the ability to heal, antimicrobial con-trol becomes more important than howmany cells may be killed, and these agentsmay be used to dry out the wound surface.Antimicrobial agents combined withmodern dressings provide a safe, effectiveoption for managing wound bioburden inhealable wounds. Literature supportsusing sustained-released antimicrobialdressings in wound care and demonstratesthat modern antimicrobial dressings donot impede healing. Studies supportingtopical antimicrobials in chronic woundshave postulated that the benefits maycome from their ability to deliver highlocal concentrations of antimicrobialproperties irrespective of vascular supply,avoidance of systemic effects, and a low in-cidence of resistance.2
Topical antiseptics. Some widely usedtopical antiseptics are silver-sustained re-lease dressings and cadexomer iodine.ese antibacterials have been used for sev-eral years and have been proven to providesafe, nontoxic, broad-spectrum activityagainst Gram-positive and Gram-negativeorganisms, MRSA, vancomycin-resistantEnterococci (VRE) bacteria, fungi, andyeast. Both silver and cadexomer iodine arebiocides whose mode of action is differentfrom antibiotics, which act specifically andeffectively against narrow ranges of bacte-ria, contributing to resistance problems.Broad-sprectrum antimicrobial agents actacross three target areas: the cell mem-brane, cytoplasmic organelles and the bac-teria’s nucleic acid.6
Antimicrobial Wound Dressings
Another available antimicrobial is theKendallTM AMD antimicrobial foamdressing (Covidien, Mansfield, MA).ese dressings are impregnated withpolyhexamethylene biguanide (PHMB),a biocide that has been used for manyyears without any known resistance.4
PHMB is a synthetic compound similarin structure to naturally occurring antimi-crobial peptides (AMPs), molecules pro-duced at the wound site by inflammatoryneutrophils and keratinocytes that helpprotect against infection. PHMB attachesitself to the bacterial cell membrane, caus-ing a structural change that kills the bac-teria. In common resistance, bacteriaprotect themselves by pumping some an-tibiotics out of the cell using efflux pumps.e structural change to the cell wallscaused by the PHMB is an advantage be-cause the bacteria cannot use their effluxpumps to pump out the PHMB.1
PHMB has been incorporated into avariety of common wound dressings: Ker-lixTM AMD gauze dressings, ExcilonTM
drain sponges, CurityTM AMD gauzedressings and packing strips, and TelfaTM
AMD nonadherent dressings impreg-nated with 0.2% PHMB have beenproven to effectively kill many clinicallyrelevant bacteria within the dressing. Invitro studies demonstrated broad-spec-trum activity against Gram positive andGram negative organisms and fungi.1 Onesignificant study showed that KerlixAMD gauze decreased growth of MRSAand VRE at 24 and 48 hours and exhib-ited a 3 to 6 log reduction of MRSA anda 4 to 5 log reduction of VRE at 30 min-utes and 2 hours post-inoculation of the

Supplement to OWM • March 2009 7
dressing.7 In human studies, the ExcilonAMD drain sponge demonstrated amarked decrease in MRSA and P. aerugi-nosa around tracheostomy sites.8 e re-sults of another study of 24 delayedsurgical closures, pressure ulcers, and dia-betic foot wounds packed with KerlixAMD gauze showed a decrease in totalnumber of bacteria and number of speciespresent compared to the control dressingwith no antimicrobial agent. e bacterialdecrease was accompanied by improvedhealing in the wounds covered with thePHMB dressing.9 Many case studies forsurgical incisions and pressure ulcers re-ported similar results, as well as decreasesin wound size and reduced cost of care.One significant study reported a decreasein vascular site infections from 4.6% be-fore the PHMB dressings to 0.4% aer 5years of routine use. e estimated savingswas $817,176 and was reported to havebeen associated with dressing substitutionand no other apparent changes in practiceor patient population.1
While managing bacteria on the woundsurface is important for healing, it is alsoimportant to prevent cross-contaminationand prevent bacteria from entering the en-vironment from the dressing or from en-tering the wound from the environment.Studies of PHMB dressings have proventhem effective in preventing bacteria fromentering the wound through the dressingand in killing the bacteria in the dressing.1
e following series of case studies willlook at a new PHMB-impregnated foamdressing. e Kendall AMD foam dressinghas 0.5% PHMB impregnated in ab-sorbent foam. Antimicrobial efficacy of thefoam is reflected in an in vitro study that
showed an ~8.87 log reduction in MRSAgrowth at 24 hours. e log reduction at 3days and 7 days was ~9.36 and ~8.88, re-spectively.10 Another in vitro study com-pared the antimicrobial efficacy of thePHMB dressing with that of several silvertechnologies and one nonsilver antimicro-bial dressing. Kendall AMD antimicrobialfoam dressings demonstrated a >3 log re-duction for 7 days for MRSA, VRE, and P.aeruginosa. e silver technologies testeddid not show consistent efficacy against allthree organisms for 7 days. e only testedantimicrobials that showed 7-day efficacyagainst all three organisms were the nonsil-ver biguanide antiseptics, Kendall AMDantimicrobial foam dressings (PHMB),and Johnson & Johnson BiopatchTM
(CHG), both of which showed >3 log re-duction for 7 days against all three organ-isms.11 e Kendall foam dressing is highlyabsorbent, which is needed for woundswith high bioburden because of the exces-sive drainage usually present. Chronicwound fluid not only contains high levelsof bacteria, but also high levels of proteases,which can create an unhealthy environ-ment for healing. Foam dressings that pro-vide antimicrobial control and moisturebalance by absorbing excessive drainage areideal choices for many chronic wounds.
All chronic wounds will eventually be-come colonized with bacteria, puttingthem at risk for critical colonization, in-fection, and delayed healing. Traditionalwound dressings are not able to managethe bioburden of the wound, and bacteriawill grow unchallenged. If we can managebacteria in the dressing and prevent cross-contamination; if we can maintain a heal-ing colonized wound by managing
bacteria on the wound surface; if we canprevent the progression and proliferationof bacteria across the bioburden spectrum;and if we can use products that can be in-corporated easily into routine protocolsand inventories, our goal of quality, cost-effective care can be accomplished. isgoal can be achieved when clinicians makeinformed decisions about management ofwound bioburden. e following casestudies demonstrate some of the decisionsand rationale for selecting the KendallAMD foam dressing.
References1. Moore K, Gray D. Using PHMB antimicrobial to
prevent wound infection. Wounds UK. 2007; 3(2):96-102.
2. Howell-Jones RS, Wilson MJ, Hill KE, et al. A re-view of the microbiology, antibiotic usage and re-sistance in chronic skin wounds. J of AntimicrobChemother. 2005;55(2):143-149.
3. e International Working Group on the DiabeticFoot (1999). e International Consensus on theDiabetic Foot. e International Working Groupon the Diabetic Foot, Amsterdam, Netherlands.
4. Landis S, Ryan S, Woo K, Sibbald RG. Infectionsin chronic wounds. In: Krasner DL, RodeheaverGT, Sibbald RG (eds). Chronic Wound Care, 4thedition. Malvern, PA:HMP Communica-tions;2007:299-321.
5. Rodeheaver G, Ratliff C. Wound cleansing, woundirrigation, wound disinfection. In: Krasner DL,Rodeheaver GT, Sibbald RG (eds). Chronic WoundCare, 4th edition. Malvern, PA:HMP Communi-cations;2007:331-342.
6. Sibbald RG, Growne AC, Coutts P, Queen D.Screening evaluation of an ionized nanocrystallinesilver dressing in chronic wound care. OstomyWound Management. 2001;47(10):38-43.
7. Gallant-Behm CL, et al. Comparison of in vitrodisc diffusion and time kill-kinetic assays for theevaluation of antimicrobial wound dressing effi-cacy. Wound Rep Reg. 2005;13:412-421.
8. Motta GJ, Trigilia D. e effect of an antimicrobialdrain sponge dressing on specific bacterial isolatesat tracheostomy sites. Ostomy Wound Manage.2001;51:60-66.
9. Motta GJ, Milne CT, Corbett LG. Impact of an-timicrobial gauze on bacterial colonies in woundsthat require packing. Ostomy Wound Manage.2004;50: 48-62.
10. Kirker KR, Fisher ST, James G, McGhee D, ShahCB. Efficacy of COPA AMD foam dressingagainst MRSA. Center for Biofilm Engineering,Montana State University, Bozeman, MT, and Co-vidien.
11. McGhee D. Activity of Antimicrobial DressingsUsing Clinically Relevant Organisms—MRSA,VRE, and P. aeruginosa. Bioscience R&D/Materi-als Development, Patient Care & Safety Products,Covidien, Inc.
8 Supplement to OWM • March 2009
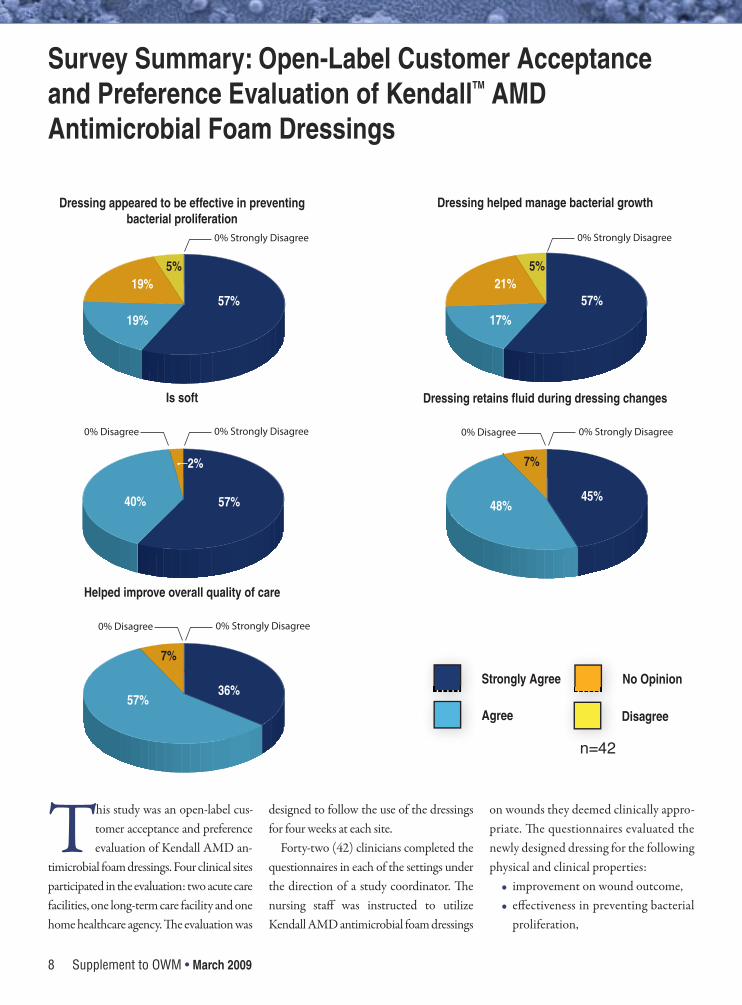
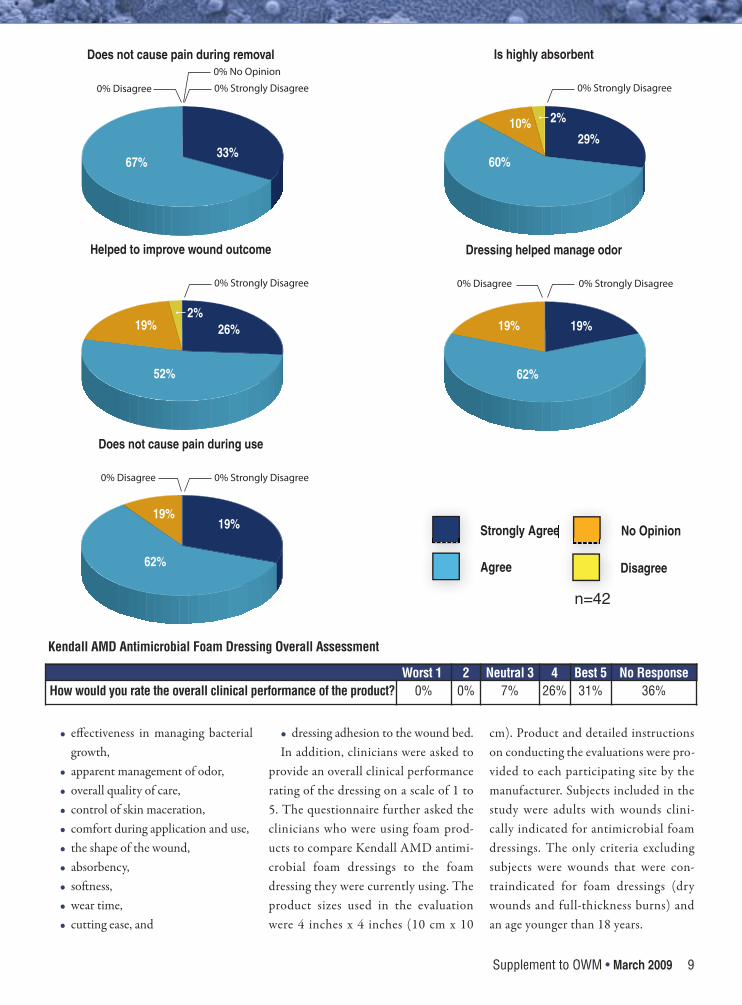
This study was an open-label cus-tomer acceptance and preferenceevaluation of Kendall AMD an-
timicrobial foam dressings. Four clinical sitesparticipated in the evaluation: two acute carefacilities, one long-term care facility and onehome healthcare agency. e evaluation was
designed to follow the use of the dressingsfor four weeks at each site.
Forty-two (42) clinicians completed thequestionnaires in each of the settings underthe direction of a study coordinator. enursing staff was instructed to utilizeKendall AMD antimicrobial foam dressings
on wounds they deemed clinically appro-priate. e questionnaires evaluated thenewly designed dressing for the followingphysical and clinical properties:
• improvement on wound outcome,• effectiveness in preventing bacterial
proliferation,
Dressing appeared to be effective in preventing bacterial proliferation
57%19%
19%5%
0% Strongly Disagree
Dressing helped manage bacterial growth
57%17%
21%5%
0% Strongly Disagree
Is soft
57%17%
21%5%
0% Strongly Disagree
57%
2%
40%
0% Disagree
Dressing retains fluid during dressing changes
45%
7%
0% Strongly Disagree
48%
0% Disagree
Helped improve overall quality of care
36%
7%
0% Strongly Disagree
57%
0% Disagree
Strongly Agree
Agree
e No Opinion
Disagree
Survey Summary: Open-Label Customer Acceptanceand Preference Evaluation of KendallTM AMDAntimicrobial Foam Dressings
n=42
Supplement to OWM • March 2009 9
• effectiveness in managing bacterialgrowth,
• apparent management of odor,• overall quality of care,• control of skin maceration,• comfort during application and use, • the shape of the wound,• absorbency,• soness,• wear time,• cutting ease, and
• dressing adhesion to the wound bed.In addition, clinicians were asked to
provide an overall clinical performancerating of the dressing on a scale of 1 to5. The questionnaire further asked theclinicians who were using foam prod-ucts to compare Kendall AMD antimi-crobial foam dressings to the foamdressing they were currently using. Theproduct sizes used in the evaluationwere 4 inches x 4 inches (10 cm x 10
cm). Product and detailed instructionson conducting the evaluations were pro-vided to each participating site by themanufacturer. Subjects included in thestudy were adults with wounds clini-cally indicated for antimicrobial foamdressings. The only criteria excludingsubjects were wounds that were con-traindicated for foam dressings (drywounds and full-thickness burns) andan age younger than 18 years.
Does not cause pain during removal
33%
0% Strongly Disagree
67%
0% Disagree
0% No Opinion
Is highly absorbent
29%
0% Strongly Disagree
60%
10% 2%
Helped to improve wound outcome
26%
0% Strongly Disagree
52%
19%2%
Dressing helped manage odor
19%
0% Strongly Disagree
62%
19%
0% Disagree
Does not cause pain during use
19%
0% Strongly Disagree
62%
19%
0% Disagree
Strongly Agree
Agree
e No Opinion
Disagree
Worst 1.. 2 Neutral 3 4 Best 5 No ResponseHow would you rate the overall clinical performance of the product? 0% 0% 7% 26% 31% 36%
Kendall AMD Antimicrobial Foam Dressing Overall Assessment
n=42
Balancing a Dynamic Wound Environment
10 Supplement to OWM • March 2009
Wounds oen are complexand difficult to heal. eymay persist for months or
years due to underlying disease processesor complications within the healingprocess. Nonhealing or slow-healingwounds represent a major health burdenand drain resources and contribute sub-stantially to disability, morbidity, and cost.e treatment of chronic wounds has aprofound effect on the participant’s qual-ity of life.1
Efficient strategies for wound healinghave become crucial for the survival ofhome health agencies (HHAs). Treatingwounds in home health settings can be ex-pensive and time-consuming. Comor-bidities and variable home environmentscan lead to challenges associated withwound healing and infection prevention.2
Treating BioburdenTreating wounds requires a comprehen-sive approach that includes addressing theunderlying etiology of the wound, remov-ing causative factors, and attending to sys-temic needs of the patient.3 According toBryant and Nix,4 an important step inwoundbed preparation is removing bacte-rial burden. Bacteria in wounds competefor the limited supply of oxygen and nu-trients available in the wound. All woundscontain some level of bacteria — the chal-lenge is to achieve a level of bacterial bur-den or bioburden the host can manage.
Wound bioburden has four recognizedstages: contamination, colonization, criticalcolonization, and infection. Contaminationis the presence of nonreplicating micro-or-ganisms on the wound surface arising fromnormal flora that normally do not elicit a re-sponse from the body. Colonization refersto the presence of replicating bacteria, with-out a response from the body. Bacteria lev-els in these phases are not pathogenic anddo not necessitate treatment with systemicor local antibiotics.4
When a wound progresses to the criti-cal colonization phase, healing is arrestedas a result of bacteria competition for nu-trients and oxygen. Wounds in this phaseare progressing toward the final infectionstage even while bacteria have not pene-trated the tissues or evoked the classic clin-ical presentation of infection (eg, redness,warmth, fever, pain, edema). Because bac-teria have not penetrated the tissues, sys-temic antibiotics are not indicated.However, appropriate use of topical an-timicrobials can prevent progression to in-fection and assist wounds in theirprogression toward healing.4
According to Tomaselli,5 the most pop-ular antimicrobial products used by homecare agencies contain silver. Silver prod-ucts are available in a variety of dressings.ey provide antimicrobial protectionthat may reduce wound bioburden. is isalso important for home care agencies fi-nancially, because efficient wound healing
can decrease expensive nurse visits and im-prove patient outcomes. A drawback ofsilver products is that they are very costly.
Financial Challenges of HomeHealth AgenciesHHAs are currently reimbursed byMedicare using a Prospective PaymentSystem, or PPS. Under PPS, Medicarepays HHAs a predetermined base pay-ment, adjusted for the health conditionand care needs of the beneficiary.6
HHAs have a set amount of money touse for all services and supplies used bythe patient at home during a 60-dayepisode; thus, HHAs need to prudentlyuse supplies and distribute home carevisits to fit the predetermined base pay-ment. HHAs are anticipating the Cen-ters for Medicare and Medicaid Serviceschanging to a pay-for-performancemodel (currently in the demonstrationphase), where agencies are rewarded forimprovements based on measurementsof quality, efficiency and outcomes.6 Up-coming changes are encouraging agen-cies to become even more conscious oftheir use of staffing and supplies.
Polyhexamethylene Biguanide e antiseptic polyhexamethylenebiguanide (PHMB) has been added towound dressings. It has been found to beeffective against a broad spectrum ofmicro-organisms, fungi, and yeast.
Antimicrobial Foam Dressings on Moderately to HeavilyDraining Wounds Treated in Home Health Care Bridget Mejza, RN, BSN, CWOCN, VNA of Southeast Connecticut, Waterford, CT

Supplement to OWM • March 2009 11
PHMB’s structure and mode of action aresimilar to antibacterial peptides that func-tion by disrupting microbial membranes.No known resistance has been reported.3
Motta et al7 also report that PHMB hasminimal to no odor; is nonfoaming,chemically stable, and nonvolatile; andhas low mammalian toxicity. A variety ofwound care products contain PHMB.8
Mulder et al8 evaluated the cellulosewound dressing antimicrobial on 12 pa-tients with 26 wounds of various etiolo-gies. PHMB dressing use resulted inelimination of Pseudomonas aeruginosa,diptheroid Gram-positive rods, beta-he-molytic Streptococcus, and Enterobacteraerogenes in some patients and decreasedlevels of Staphylococcus aureus, P. aerugi-nosa, and Proteus mirabilis in others.
In an animal study by Cazzaniga et al,9
three pigs received 18 wounds — ninewere treated with PHMB gauze dressingsand nine with plain gauze, followed by apolyurethane film dressing to maintain amoist environment. e dressings were
challenged on the surface with a suspen-sion of P. aeruginosa and cultured at 24,48 and 72 hours. e results showed thatfewer organisms invaded the wounds withthe PHMB dressing.
Motta et al7 compared bacterial countsusing gauze containing PHMB and gauzewith no antimicrobial in wounds that re-quired packing. Using PHMB-treatedgauze resulted in a larger reduction of thetotal number of microbial isolates, thenumber of polymicrobial counts, and thelog colony counts as compared to the reg-ular gauze dressing. In addition, chronic,nonhealing wounds in case studies ofPHMB-treated dressing use showed im-provement and progression toward heal-ing. Although PHMB antimicrobialproducts cost slightly more than theirnon-antimicrobial equivalents, they costless than other antimicrobial dressings onthe market, especially silver.
Because of their absorbancy, foamdressings are used for moderately to heav-ily draining wounds. e foam provides a
desirable moist wound environment whiledrawing excess moisture away from theskin. Foam dressings are a popular choicein home care patients — they decreasenursing-visit frequency because they canhandle drainage so well that patients re-quire less-frequent skilled-nurse visits fordressing changes.
A study was conducted through theVNA of Southeast Connecticut to test afoam dressing on a variety of moderatelyto heavily draining wounds. e studypurpose was to find a cost-effective way tohelp keep microbial counts down and effi-ciently manage wound drainage in orderto help heal patients’ wounds and increasetheir quality of life.
Case ReportMr. R is a 72-year-old man who had beentreated with negative pressure woundtherapy (NPWT) for a surgical wound ofhis right calf since July 14, 2008. Hismeasurements on September 24 were 11.5cm x 2 cm x .02 cm (see Figure 1). At that
Addressing Redness, Soreness, and Increased Drainage from Tube Sites Using an Antimicrobial Foam DressingSusan Krause, RN, MSN, CWOCN, Senior Specialist, Wound Healing Department, Sharp Metro Campus, Sharp Memorial Hospital, San Diego, CA
Patients with tubes and drains are at risk for skininfection and skin irritation around the tubes. Treat-ing these conditions can be painful, costly, andtime-consuming when frequent dressing changesare required.
Case Report Ms. D is 53 years old with gastrointestinal dysmotil-ity. She has a J-tube through which she receivessome of her medications. (Patient was dischargedbefore medications could be ascertained). She alsohas a biliary drainage tube. She receives chronictotal parenteral nutrition (TPN) through a port-a-cath T-tube.
Ms. D was admitted to hospital with a high fever(>102 F); line sepsis was suspected. She had previ-ously been instructed to clean her tube sites with al-cohol wipes and to cover them with Tegadermdressings (3M, St. Paul, MN) because of a reported
history of methicillin-resistant Staphylococcus au-reus (MRSA) infection. She reported having fol-lowed these instructions for just 1 day beforeadmission.
A site culture uncovered light Pseudomonasaeruginosa, Escherichia coli, a small amount of van-comycin-resistant Enterococcus faecium and Can-dida albicans (not usually seen in a J-tube site, inthis author’s experience) in the J-tube. The T-tubeculture yielded a small amount of MRSA and rarecolonies of E. coli.
The amount of exudate had required Ms. D tochange the dressings around the tube sites severaltimes a day. Her clinician wanted to provide a dress-ing with antimicrobial coverage as well as some de-gree of absorbency, so the patient would not haveto change the dressings as often. The clinical profileof the KendallTM AMD antimicrobial foam dressingseemed well-suited to the situation, and the new
dressing was applied.Ms. D was an inpatient for 2 days. On day 2, she
reported that she liked the dressing because sheonly needed to change it once a day and it was han-dling all the drainage. She also reported that is wascomfortable and did not irritate her already compro-mised skin.
Moderator’s Commentaryis study points out another type of patient that maybenefit om an absorptive, antimicrobial dressing: thosewith tubes and drains. e author further highlights thechallenges of dealing with these patients. A dressing thataddresses bioburden and exudate management that iscomfortable, easily changed, and requires only daily (orfewer) changes can be very helpful to both patient andcaregiver. It appears that at the time of discharge, the pa-tient was very satisfied with this dressing regimen.

Balancing a Dynamic Wound Environment
12 Supplement to OWM • March 2009
time, Mr. R had increased yellow drainageand a wound culture was positive forStaphylococcus. NPWT was discontinuedthat day and he was started on KendallTM
AMD antimicrobial foam dressing. Mr. Rand his spouse were very happy to stopNPWT; it was cumbersome to carry andhe found it difficult to have his leg at-tached to the unit, especially as his mobil-ity increased.
Mr. R’s spouse changed the foam dress-ing every other day aer he showered. She
was able to apply dressing, did not com-plain of difficulties with use, and securedit with transparent dressing or paper tape.
On October 14, a WOCN visited Mr.R. His wound dimensions had decreasedto 7 cm x 0.5 cm x 0 cm, with a smallamount of serous drainage on the dressingand some scabbing around the periphery(see Figure 2). e wound bed was dry, soa small amount of wound gel was appliedto the wound bed for added moisture. epatient was instructed to continue every
other day with the dressing change, untilhealing was complete.
References1. Coutts P, Sibbald RG. e effect of a silver con-
taining hydrofiber dressing on superficial woundbed and bacterial balance of chronic wounds. In-ternational Wound J. 2005;2(4): 348-356.
2. Sargent RL. (2006, April). e use of antimicro-bial gauze in a home care setting: a cost effective,proactive wound management plan. Available atTyco Health Care Group Web site:http://www.kendallamd.com/pdf/H-5867In-galsHomeWP.pdf. Accessed October 6, 2007.
3. White RJ, Cutting K, Kingsley R. Topical an-timicrobials in the control of wound bioburden-part 1. Ostomy Wound Manage. 2006;52(8):26-58.
4. Bryant RA, Nix DP. Wound infection: diagnosisand management. In Nancy A. Stotts (Ed.),Acute & chronic wounds: current managementconcepts, 3rd ed. St Louis: Mosby Elsevier;2007:161-175.
5. Tomaselli N. e rold of topical silver prepara-tions in wound healing. J of Wound Ostomy &Continence Nursing. 2006;33(4):367-378.
6. Centers For Medicare & Medicaid Services.(27). Home Health PPS Overview. Available atU.S. Department of Health & Human ServicesWeb site: http://www.cms.hhs.gov/Home-HealthPPS/. Accessed October 6, 2007.
7. Motta GJ, Milne CT, Corbett LO. Impact of an-timicrobial gauze on bacterial colonies inwounds that require packing. Ostomy WoundManagement. 2004;50(8);48-62.
8. Mulder GD, Cavorsi JP, Lee DK. Polyhexameth-ylene biguanide (PHMB): an addendum to cur-rent topical antimicrobials. Wounds.2007;19(7):173-182.
9. Cazzaniga A, Serralta, V, Davis S, et al. e effectof an antimicrobial gauze dressing impregnatedwith 0.2-percent polyhexamethylene biguanideas a barrier to prevent pseudomonas aeruginosawound infection. Wounds. 2002;14(5):169-176.
Moderator’s Commentarye author provides insight into chronic
wound management in today’s home care arena.She discusses the importance of managing woundbioburden and why home care agencies must lookfor ways to manage wounds, supplies, and e-quency of visits in cost-effective ways. Ms. Mejzaalso very succinctly outlines some of the evidencebehind these PHMB dressings by summarizingsome of the clinical studies.
In this case study, the key to success was an effec-tive (specific for Staphylococcus and able to absorbdrainage) dressing that could be changed easilyevery other day by a family member. is is a verymanageable treatment plan for home care and letsthe nurse visit periodically to assess wound progress,monitor for infection, and re-enforce family educa-tion. ese dressings will be especially important inthe home care nurse’s arsenal of topical therapies.
Figure 1
Figure 2
Supplement to OWM • March 2009 13
Ayoung woman’s surgically openpost-panniculectomy methi-cillin-resistant Staphylococcus
aureus (MRSA) infected, unstable, re-fractory wound was not healing success-fully using Dakin’s solution and silverproducts to address infection. After top-ical application of an antimicrobial foamdressing, signs of infection resolved andthe wound healed.
Case ReportMs. O is a 25-year-old obese AmericanIndian woman with a history of alcoholabuse and insulin-dependent diabetesmellitus (IDDM). She underwent apanniculectomy in order to control re-current intertrigo of the lower abdomi-nal wall skin and to improveambulation. Postoperatively, she devel-oped a wound hematoma.
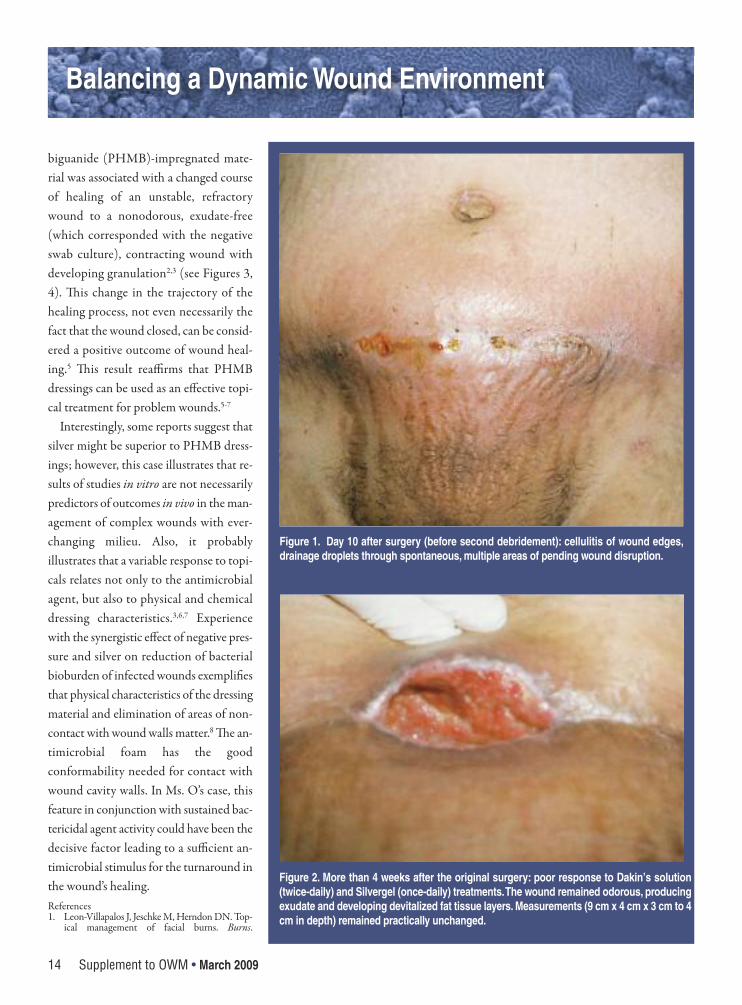
e suprapubic wound was opened 7days aer Ms. O’s surgery: e hematomawas drained and the wound was irrigatedand re-closed. Subsequently, Ms. O devel-oped cellulitis; a swab-culture from thesmall draining wound disruptions re-vealed methicillin-resistant S. aureus(MRSA) (see Figure 1). e wound wasopened, re-debrided, and treated with0.025% Dakin’s solution soaks and subse-quently with Elta Silver Gel (Swiss-Amer-ican, Carrollton, TX), once the presence
of the MRSA was confirmed. For 3 weeks,the wound remained unstable and odor-ous, exhibited a significant amount of ex-udate and progressive build-up of necroticsubcutaneous fat layers, and showed noinclination to contract (see Figure 2).Topical treatment was changed toKendallTM AMD antimicrobial foamdressings applied once daily. e woundstabilized, odor and exudate productionceased, and the wound wall became vascu-lar and granulating. Aer 1 week, woundsize was reduced by more than 50% andcultured negative (see Figure 3). Within 2weeks aer initiating use of the antimicro-bial foam dressing, Ms. O’s wound con-tracted and closed spontaneously.Perioperatively and during the woundcomplication treatment, Ms. O remainedin stable and in good overall condition,without any signs suggestive of systemicinfection. Ms. O was not receiving sys-temic antibiotics with the exception of theroutine perioperative prophylaxis (Ancef,GlaxoSmithKline, Philadelphia, PA).
DiscussionInitially, before the result of swab culturewas known, this odorous, exudativewound was treated with modified Dakin’ssolution at a concentration 0.025%.Dressings with Dakin’s cotton soaks werechanged twice daily. It was expected that
modified Dakin’s solution would be ther-apeutically efficacious because it preservesgeneral bactericidal properties and has rel-atively few detrimental effects.1 BecauseMs. O did not show any signs of systemicinfection and in light of the poor penetra-tion in devitalized tissue of systemic an-tibiotics, wound management continuedto utilize topical agents. Silver-releasingdressing was considered: Elta SilverGelTM
(Swiss-American Products, Carrollton,TX), designed to provide a moist healingenvironment and known to provide sus-tained and effective silver-ion release tothe wound to inhibit the growth of S. au-reus and MRSA, appeared to be a logicalalternative.1 Data indicating that silverions do not inhibit angiogenesis and mi-crovascularization reaffirmed the notionthat a silver-based, moisture-retainingwound dressing would be an appropriate,evidence-based treatment choice decisionfor this IDDM patient.1,4 However, thesilver-releasing topical did not seem tospeed granulation or contracture or re-duce exudate (a sign of bioburden), so thewound management regimen waschanged again.
e antimicrobial foam dressing thatwas introduced — Kendall AMD antimi-crobial foam dressings — is, like silver,known to exert a bactericidal effect onMRSA. Topical 0.5% polyhexamethylene
Changing Healing Trajectory of a Postsurgical WoundUsing Topical Polyhexamethylene Biguanide-ImpregnatedAntimicrobial Foam Dressing: A Case StudyMarek K. Dobke, MD, Division of Plastic Surgery, Department of Surgery, University of California San Diego
Balancing a Dynamic Wound Environment
14 Supplement to OWM • March 2009
biguanide (PHMB)-impregnated mate-rial was associated with a changed courseof healing of an unstable, refractorywound to a nonodorous, exudate-free(which corresponded with the negativeswab culture), contracting wound withdeveloping granulation2,3 (see Figures 3,4). is change in the trajectory of thehealing process, not even necessarily thefact that the wound closed, can be consid-ered a positive outcome of wound heal-ing.5 is result reaffirms that PHMBdressings can be used as an effective topi-cal treatment for problem wounds.5-7
Interestingly, some reports suggest thatsilver might be superior to PHMB dress-ings; however, this case illustrates that re-sults of studies in vitro are not necessarilypredictors of outcomes in vivo in the man-agement of complex wounds with ever-changing milieu. Also, it probablyillustrates that a variable response to topi-cals relates not only to the antimicrobialagent, but also to physical and chemicaldressing characteristics.3,6,7 Experiencewith the synergistic effect of negative pres-sure and silver on reduction of bacterialbioburden of infected wounds exemplifiesthat physical characteristics of the dressingmaterial and elimination of areas of non-contact with wound walls matter.8 e an-timicrobial foam has the goodconformability needed for contact withwound cavity walls. In Ms. O’s case, thisfeature in conjunction with sustained bac-tericidal agent activity could have been thedecisive factor leading to a sufficient an-timicrobial stimulus for the turnaround inthe wound’s healing. References1. Leon-Villapalos J, Jeschke M, Herndon DN. Top-
ical management of facial burns. Burns.
Figure 1. Day 10 after surgery (before second debridement): cellulitis of wound edges,drainage droplets through spontaneous, multiple areas of pending wound disruption.
Figure 2. More than 4 weeks after the original surgery: poor response to Dakin’s solution(twice-daily) and Silvergel (once-daily) treatments. The wound remained odorous, producingexudate and developing devitalized fat tissue layers. Measurements (9 cm x 4 cm x 3 cm to 4cm in depth) remained practically unchanged.
Supplement to OWM • March 2009 15
2008;34(7):903–911.2. Ratliff CR, Getchell-White SI, Rodeheaver GT.
Quantitation of bacteria in clean, nonhealing,chronic wounds. Wounds. 2008;20(10):279–283.
3. Streed SA, Loehne HB. Preventing infections toimprove wound care outcomes: an epidemiologicalapproach. Wounds. 2007;19(11):320–330.
4. Ring A, Goertz O, Steinstraesser L, Cotaru C,Muhr G, Steinau H-U, Langer S. Silver ion-releas-ing dressing (Contreet) does not disturb angiogen-esis and microvascularization in vitro. Wounds.2007;19(2):39–45.
5. Franz MG, Kuhn A, Wright T, Wachtel TL, Rob-son MC. Use of the wound healing trajectory as anoutcome determinant for acute wound healing.Wound Rep Reg. 2000;8(6):511–516.
6. Kirsner R. Infection and intervention. Wounds.2003;15(5):127–128
7. Wright JB, Lam K, Olson ME, Burrell RE. Is an-timicrobial efficacy sufficient ? A question concern-ing the benefits of new dressings. Wounds.2003;15(5):133–142.
8. Gabriel A, Heinrich C, Shores JT, Baqai WK,Rogers FR, Gupta S. Reducing bacterial bioburdenin infected wounds with vacuum assisted closureand a new silver dressing – a pilot study. Wounds.2006;18(9):245-255.
Moderator’s Commentaryis case study highlights some common prob-lems that healthcare providers face. A high-riskpatient (eg, obese, diabetic) undergoes electivesurgery and subsequently develops a wound in-fection. e wound was opened and debridedand treated with some topical antimicrobialdressings. Dakins was initially used because ofodor and drainage. Because of the poor responseto this therapy, a culture was done revealingMRSA. Another topical antimicrobial known tobe effective against MRSA was initiated (silverhydrogel). When signs of healing were not ob-served, the Kendall AMD foam was started be-cause of its bactericidal effect on MRSA. ewound responded positively and closed, indicat-ing that the Kendall AMD antimicrobial foamdressing was an effective solution for this wound. Dr. Dobke also makes another important point:e physical characteristics of a dressing can bean important aspect in the selection process.Wound fluid has been shown to have high levelsof proteases and excessive bacteria and needs tobe managed effectively. ese types of woundsmay benefit om a dressing that can manage ex-udate and bacterial bioburden. A foam dressingis an excellent option to meet these objectives. Oneother aspect of this case needs to be pointed out:Although many topical antimicrobials have re-ported to be effective against various organisms,in the ever-changing milieu of the chronic woundenvironment, the critical question is, “Is it work-ing?” If not, do something different.
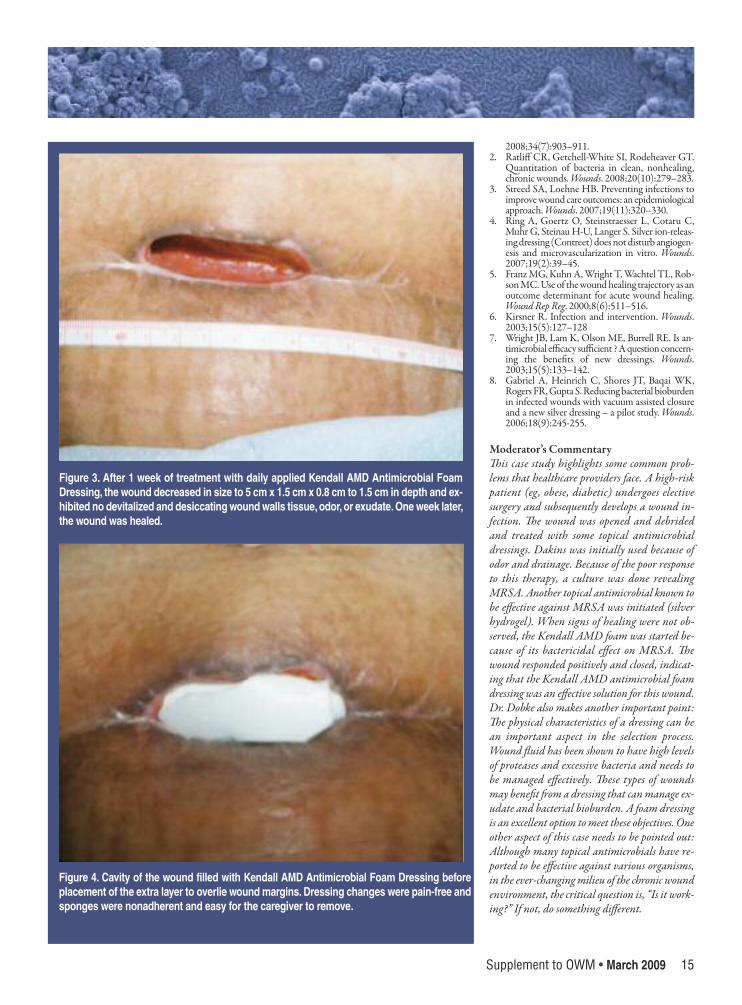
Figure 3. After 1 week of treatment with daily applied Kendall AMD Antimicrobial FoamDressing, the wound decreased in size to 5 cm x 1.5 cm x 0.8 cm to 1.5 cm in depth and ex-hibited no devitalized and desiccating wound walls tissue, odor, or exudate. One week later,the wound was healed.
Figure 4. Cavity of the wound filled with Kendall AMD Antimicrobial Foam Dressing beforeplacement of the extra layer to overlie wound margins. Dressing changes were pain-free andsponges were nonadherent and easy for the caregiver to remove.

Balancing a Dynamic Wound Environment
16 Supplement to OWM • March 2009
Diabetic foot wounds require of-floading, good control of bloodglucose, good vasculature, infec-
tion control, and nutritional status, all ofwhich are more problematic in patientswith diabetes. Topical products that addressany of the issues relevant to treatment pro-vide opportunities to improve care and pa-tient acceptance of protocols.
Case Report Mr. H is an 81-year-old Caucasian with
a 7-month history of a diabetic foot woundover the dorsolateral le foot just proximalto the fih metatarsophalangeal joint. Hisrelevant medications include insulin,coumadin, Fosamax (Merck and Co.,Whitehouse Station, NJ), metolazone,magnesium, aspirin, furosemide, allopuri-nol, metoprolol, isosorbide, simvastatin,losartan, and pantoprazole. Mr. H’s A1Clevels have ranged from 7.1 to 7.4 duringwound treatment and his physician believesthis is as well as he can be controlled. Addi-tional complications include pedal edema,which is mostly controlled by Unna bootsused for the past 2 months. He also had ad-verse reactions to Apligraf (Organogenesis,Canton, MA).
Mr. H’s wound occurred 18 monthsago and was healed at that time usingweekly debridment, Prisma, and Der-magraft (Smith and Nephew, Hull,UK). When his wound recurred, Prismaand Dermagraft were used again with-
out success. More recently, the woundwas managed using weekly debridment,Acticoat-7, Aqacel Ag, Prisma, Apligraf,Dermagraft, Unna boots and Ziox(Stratus Pharmaceuticals, Miami, FL).CT scan and X-rays were negative forosteomyelitis, bone pathology, or ab-scess and biopsy cultures were eventu-ally negative. Clinicians diagnosed adiabetic foot wound of the left foot (seeFigure 1).
It was not determined why the woundreturned. Mr. H is not very aware of thestresses or pressure on his foot or attentiveto his blood glucose control. He had agood bit of post-debridment bleeding andoccasional serous drainage. Mr. H’s clini-cians believed the new product had qual-ities that would make it more comfortableon his sensitive skin.
Use of KendallTM AMD antimicrobialfoam dressings was initiated to provide an-tibacterial coverage different than the tradi-tional silver (see Figure 2). Althoughresistance to silver exists only in the lab and
Antimicrobial Foam Dressing Used in the Treatment of aDiabetic Foot UlcerRobert Feldman, DPM, Medical Director, Bedford Memorial Hospital Wound Care Clinic, Bedford, VA
Figure 1
Figure 2
Supplement to OWM • March 2009 17
is not seen in wound care, it was determinedthat the wound was not progressing and adifferent type of antimicrobial might bemore useful. Silver had reduced the biobur-den (biopsy cultures were negative), but thefoam dressing provided broad-spectrum an-timicrobial coverage in addition to a morefavorable (ie, moist) wound environment.
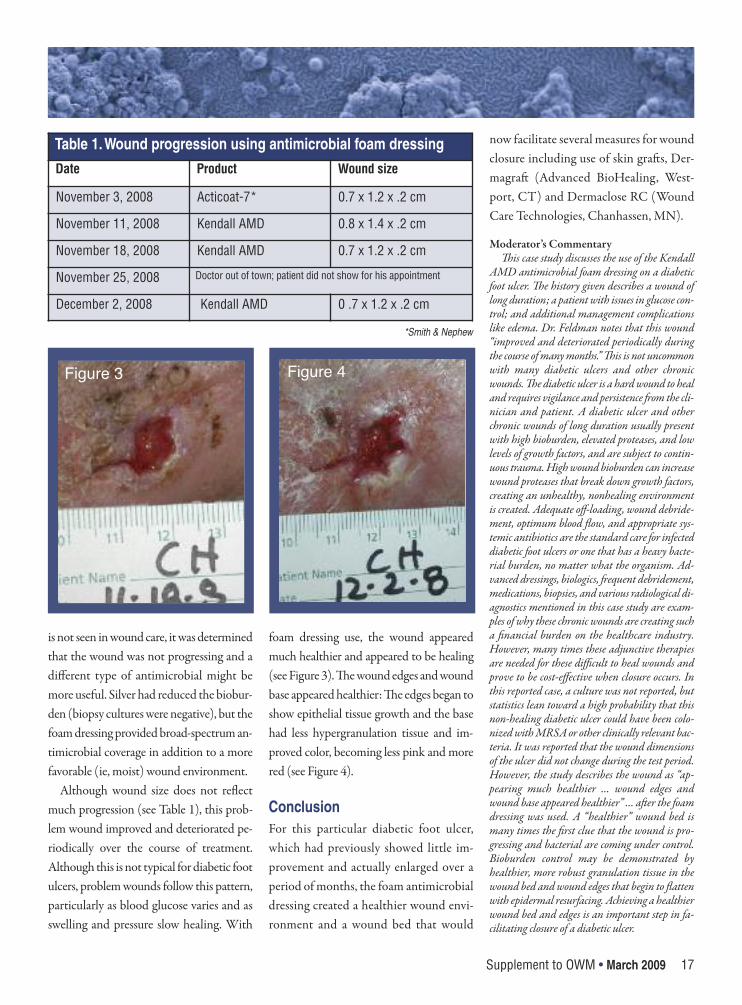
Although wound size does not reflectmuch progression (see Table 1), this prob-lem wound improved and deteriorated pe-riodically over the course of treatment.Although this is not typical for diabetic footulcers, problem wounds follow this pattern,particularly as blood glucose varies and asswelling and pressure slow healing. With
foam dressing use, the wound appearedmuch healthier and appeared to be healing(see Figure 3). e wound edges and woundbase appeared healthier: e edges began toshow epithelial tissue growth and the basehad less hypergranulation tissue and im-proved color, becoming less pink and morered (see Figure 4).
Conclusion For this particular diabetic foot ulcer,which had previously showed little im-provement and actually enlarged over aperiod of months, the foam antimicrobialdressing created a healthier wound envi-ronment and a wound bed that would
now facilitate several measures for woundclosure including use of skin gras, Der-magra (Advanced BioHealing, West-port, CT) and Dermaclose RC (WoundCare Technologies, Chanhassen, MN).
Moderator’s Commentaryis case study discusses the use of the Kendall
AMD antimicrobial foam dressing on a diabeticfoot ulcer. e history given describes a wound oflong duration; a patient with issues in glucose con-trol; and additional management complicationslike edema. Dr. Feldman notes that this wound“improved and deteriorated periodically duringthe course of many months.” is is not uncommonwith many diabetic ulcers and other chronicwounds. e diabetic ulcer is a hard wound to healand requires vigilance and persistence om the cli-nician and patient. A diabetic ulcer and otherchronic wounds of long duration usually presentwith high bioburden, elevated proteases, and lowlevels of growth factors, and are subject to contin-uous trauma. High wound bioburden can increasewound proteases that break down growth factors,creating an unhealthy, nonhealing environmentis created. Adequate off-loading, wound debride-ment, optimum blood flow, and appropriate sys-temic antibiotics are the standard care for infecteddiabetic foot ulcers or one that has a heavy bacte-rial burden, no matter what the organism. Ad-vanced dressings, biologics, equent debridement,medications, biopsies, and various radiological di-agnostics mentioned in this case study are exam-ples of why these chronic wounds are creating sucha financial burden on the healthcare industry.However, many times these adjunctive therapiesare needed for these difficult to heal wounds andprove to be cost-effective when closure occurs. Inthis reported case, a culture was not reported, butstatistics lean toward a high probability that thisnon-healing diabetic ulcer could have been colo-nized with MRSA or other clinically relevant bac-teria. It was reported that the wound dimensionsof the ulcer did not change during the test period.However, the study describes the wound as “ap-pearing much healthier … wound edges andwound base appeared healthier” … aer the foamdressing was used. A “healthier” wound bed ismany times the first clue that the wound is pro-gressing and bacterial are coming under control.Bioburden control may be demonstrated byhealthier, more robust granulation tissue in thewound bed and wound edges that begin to flattenwith epidermal resurfacing. Achieving a healthierwound bed and edges is an important step in fa-cilitating closure of a diabetic ulcer.
Table 1. Wound progression using antimicrobial foam dressing
Date Product Wound size
November 3, 2008 Acticoat-7* 0.7 x 1.2 x .2 cm
November 11, 2008 Kendall AMD 0.8 x 1.4 x .2 cm
November 18, 2008 Kendall AMD 0.7 x 1.2 x .2 cm
November 25, 2008 Doctor out of town; patient did not show for his appointment
December 2, 2008 Kendall AMD 0 .7 x 1.2 x .2 cm
*Smith & Nephew
Figure 3 Figure 4
Balancing a Dynamic Wound Environment
18 Supplement to OWM • March 2009
It is not unusual for a Class 3 venousstasis patient to experience increasedsusceptibility to infection associated
with exudate production and compressiontherapy. (A Class 1 patient presents withchanges to the skin surface — ie, swellingand scaling of the skin. Class 2 refers tochanges in coloration of the skin as fibrinleaks from the blood vessel into the inter-stitial region of the leg causing hemo-siderin staining. Scaling increases and taut,shiny skin called lipodermatosclerosis ap-pears. Class 3 venous disease is indicatedby broken skin, and ulcers with activeweeping, jagged edges, irregular shape,and partial thickness with variant degreesof pain. Most Class 3 cases experienceweeping of serous exudates to a moderateor copious degree.) is is particularlycommon due to the prevalence ofPseudomonas and fungal infections withinthis population. When products that donot address bacterial bioburden in exudateare le in place for several days, the moist,dark environment allows bacteria to thriveand grow. Changing compression therapymore frequently than two to three times aweek may defeat the purpose of usingproducts meant for less-frequent dressingchanges and decrease management effi-cacy of the venous stasis patient.
A patient was selected to try a newdressing based on the presence ofbioburden that was not responding to a
silver-impregnated alginate used in con-junction with compression therapy. ebiofilm was inhibiting his wounds fromcontracting in dimension and decreasingin exudate production.
Case ReportMr. E is a 77-year-old man with a history(at least 5 years) of venous disease that in-cludes intermittent ulcerations. e he-mosiderin staining present in both legs ismore advanced in the le gaiter whichshows lipodermatosclerosis. Mr. E’s his-tory also includes degenerative joint dis-ease, osteoarthritis, coronary arterydisease, hypercholesterolemia, and periph-eral vascular disease (PVD). e clinic hehad previously attended had been apply-ing topical clotrimazole with betametha-sone cream to the leg around the woundsand a silver alginate to the wounds, usingan Unna boot and light weight tubularelastic stocking as a covering. Mr. E’s sys-temic medications included an antihyper-tensive, a diuretic, potassium replacement,a vasodilator, and an anti-cholesterol drug.
Mr. E presented with Class 3 venousdisease to the left gaiter that was slow torespond to conservative treatment ren-dered by a wound clinic. He had beenattending a wound center twice weeklyfor 14 weeks for application of a silverdressing to two wound sites, followed byUnna boot application. In addition, Mr.
E applied pneumatic compression for 30minutes daily to his le leg.
Given his prolonged course of treat-ment and presentation of the wounds tothe medial leg and lateral malleoli, clini-cians believed Mr. E was resistant to theefficacy of the current dressing. He wasamenable to trying an alternative courseof treatment that may enhance healing. Inhis initial presentation, the woundslooked clean but had not contracted insize even with management of edema; hiswound dimensions had not contracted inthe 5 weeks before current interventionand the tissue was now friable, indicativeof his inability to combat the bioburden.
e decision was made to change thedressing every three to four days and initi-ate a protocol of cleansing with an isotonicwound cleanser, application of the antibac-terial foam, and covering with two-layercompression wrap system and Tubigrip(ConvaTec, Skillman, NJ). e KendallTM
AMD antimicrobial foam dressing was be-lieved to be a better alternative to combat-ing the biofilm than the silver dressing.
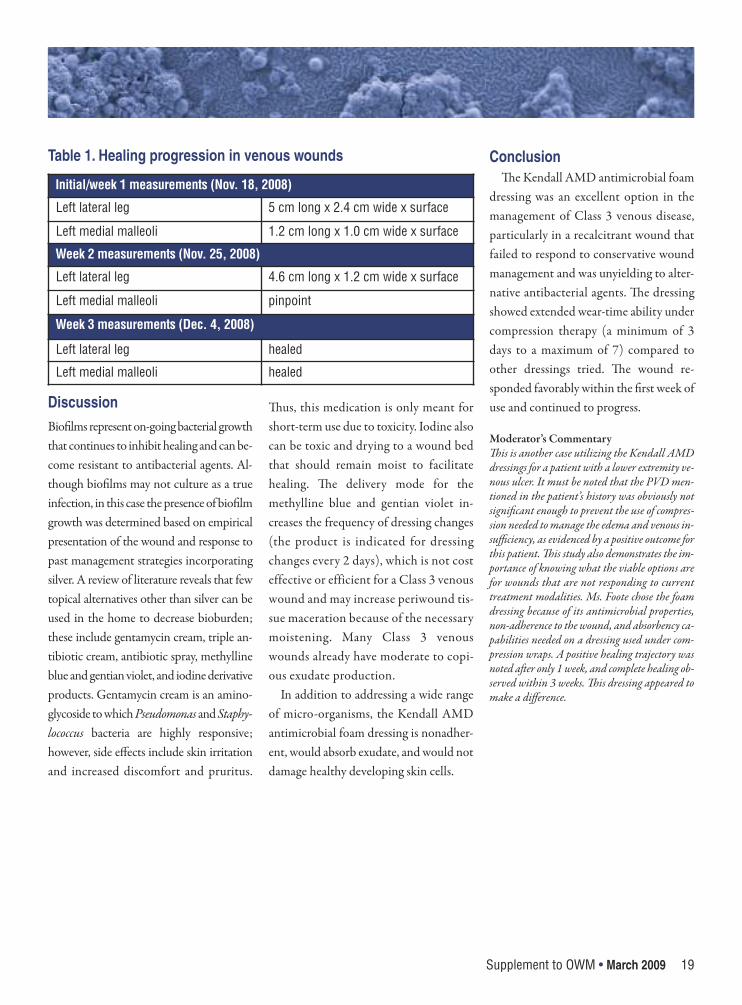
Within 1 week of product use, evidenceof wound contraction was noted in bothwounds. Compression therapy was consis-tent. In association with the type of anti-bacterial dressing, the biofilm growth wasinhibited, allowing for healing to progressquickly (see Table 1). Healing was com-plete within 3 weeks.
Inhibiting Bacterial Growth in Venous Ulcers Using anAntimicrobial Foam DressingMary Foote, RN, MSN, CANP, CWCN, ED.Dc, CEO, Wound Consultant, Woundcare On Wheels, Inc., Nerville, IL
Supplement to OWM • March 2009 19
DiscussionBiofilms represent on-going bacterial growththat continues to inhibit healing and can be-come resistant to antibacterial agents. Al-though biofilms may not culture as a trueinfection, in this case the presence of biofilmgrowth was determined based on empiricalpresentation of the wound and response topast management strategies incorporatingsilver. A review of literature reveals that fewtopical alternatives other than silver can beused in the home to decrease bioburden;these include gentamycin cream, triple an-tibiotic cream, antibiotic spray, methyllineblue and gentian violet, and iodine derivativeproducts. Gentamycin cream is an amino-glycoside to which Pseudomonas and Staphy-lococcus bacteria are highly responsive;however, side effects include skin irritationand increased discomfort and pruritus.
us, this medication is only meant forshort-term use due to toxicity. Iodine alsocan be toxic and drying to a wound bedthat should remain moist to facilitatehealing. e delivery mode for themethylline blue and gentian violet in-creases the frequency of dressing changes(the product is indicated for dressingchanges every 2 days), which is not costeffective or efficient for a Class 3 venouswound and may increase periwound tis-sue maceration because of the necessarymoistening. Many Class 3 venouswounds already have moderate to copi-ous exudate production.
In addition to addressing a wide rangeof micro-organisms, the Kendall AMDantimicrobial foam dressing is nonadher-ent, would absorb exudate, and would notdamage healthy developing skin cells.
Conclusione Kendall AMD antimicrobial foam
dressing was an excellent option in themanagement of Class 3 venous disease,particularly in a recalcitrant wound thatfailed to respond to conservative woundmanagement and was unyielding to alter-native antibacterial agents. e dressingshowed extended wear-time ability undercompression therapy (a minimum of 3days to a maximum of 7) compared toother dressings tried. e wound re-sponded favorably within the first week ofuse and continued to progress.
Moderator’s Commentaryis is another case utilizing the Kendall AMDdressings for a patient with a lower extremity ve-nous ulcer. It must be noted that the PVD men-tioned in the patient’s history was obviously notsignificant enough to prevent the use of compres-sion needed to manage the edema and venous in-sufficiency, as evidenced by a positive outcome forthis patient. is study also demonstrates the im-portance of knowing what the viable options arefor wounds that are not responding to currenttreatment modalities. Ms. Foote chose the foamdressing because of its antimicrobial properties,non-adherence to the wound, and absorbency ca-pabilities needed on a dressing used under com-pression wraps. A positive healing trajectory wasnoted aer only 1 week, and complete healing ob-served within 3 weeks. is dressing appeared tomake a difference.
Initial/week 1 measurements (Nov. 18, 2008)
Left lateral leg 5 cm long x 2.4 cm wide x surface
Left medial malleoli 1.2 cm long x 1.0 cm wide x surface
Week 2 measurements (Nov. 25, 2008)
Left lateral leg 4.6 cm long x 1.2 cm wide x surface
Left medial malleoli pinpoint
Week 3 measurements (Dec. 4, 2008)
Left lateral leg healed
Left medial malleoli healed
Table 1. Healing progression in venous wounds
Balancing a Dynamic Wound Environment
20 Supplement to OWM • March 2009
Caring for patients with compro-mised vascular and arterial suf-ficiency presents numerous
challenges. Patients providing their owncare may find it difficult to place the dress-ings and/or apply overlying compression.Wound drainage puts patients at risk forperiulcer maceration. Desloughing ormaintenance debridement decisions arelimited by patient pain and the marketwithdrawal of certain enzymatics. Al-though many of these patients receive sys-temic antibiotics, clinicians are open totrying products that address other woundissues, underscoring the desire to trial thenew foam dressing.
Case Report 1Ms. A is a 73-year-old woman with ahistory of diabetes mellitus, obesity, ve-nous insufficiency and lipodermatoscle-rosis. Her arterial flow was intact (toepressure adequate). She had multiple re-current infections, predominantly strep,methicillin-sensitive Staphylococcus au-reus and Pseudomonas.
Ms. A had multiple bilateral lower ex-tremity ulcers >1 year. e three ulcers onher le leg were the largest, one measuring6 cm (irregular shape), with a fibrinous baseand significant periulcer maceration andstasis dermatitis. She had one ulcer on herright leg that measured 2 cm; this ulcerhealed during treatment before initiation of
the study dressing. We chose to try theKendallTM AMD antimicrobial foam dress-ing relevant to her significant wounddrainage, as we believed it would bettermanage her secretions and periculcer mac-eration. e dressing was applied directlyover the wound and affixed with conformgauze and an overlying ACE wrap.
Ms. A found the study dressing to becomfortable and she exhibited no skin re-action, unlike her previous use of threedifferent silver dressings and one plain al-ginate dressing with which she reporteddiscomfort. Her treating clinicians foundthe absorptive capacity of the antimicro-bial foam dressing better than any otherdressing tried previously. Because Ms. Awas receiving systemic antibiotics at timeof dressing trial, clinicians were unable todetermine the effectiveness of the dress-ing’s antimicrobial properties.
Case Report 2 Eighty-two year old Mr. B had chroniculcerations on his left ankle with multi-ple previous hospitalizations for recur-rent infection. His medical historyincludes aortic valve replacement, con-gestive heart failure (CHF), anemia(multifactorial), and monoclonal gam-mopathy (suspected multiple myeloma).Arterial inflow is intact.
Mr. B’s ankle wounds included Stage IIlymphedema with a chronic le lateral
ulcer that had healed previously but fre-quently recurs, typical in a setting of non-compliance with leg elevation andPseudomonal infection. Venous insuffi-ciency was mild but edema was evident andrelated to the CHF. Mr. B’s wounds werepositive for methicillin-resistant S. aureus(MRSA), pansensitive Pseudomonas andoccasional other Gram negative organisms(Morganella, Citrobacter).
We chose to use Kendall AMD an-timicrobial foam dressing to addressheavy drainage from the wound andmultiple pathogenic organisms recentlycultured, hoping to provide some formof antimicrobial control to enhance hisoral antibiotics.
Mr. B found the dressing extremelycomfortable under two-layer compres-sion wrap, and the dressing’s absorptivecapacity was excellent. Mr. B did nothave any obvious skin intolerance. Be-cause Mr. B was receiving oral antibi-otics (minocycline) at the time of thetrial, the dressing’s antimicrobial prop-erties could not be assessed.
Case Report 3Ms. C is 64 years old and morbidlyobese (body mass index >40). Her med-ical history includes insulin-dependentdiabetes mellitus (IDDM) and periph-eral vascular disease (PVD) with suspi-cion of arterial insufficiency (she was
Antimicrobial Foam Dressing Used in the Treatment ofWounds in Patients With Compromised Vascular andArterial SufficiencyMark T. Herrington, FNP-C, Family Practice/Infectious Diseases, Kaiser Permanente, Honolulu, HI

Supplement to OWM • March 2009 21
undergoing vascular evaluation duringthe 2-week product trial).
Ms. C had a right lower-leg lateral as-pect ulcer measuring 8 cm x approxi-mately 5 cm with occasional fibronecroticcoating. e ulcer is usually painful anddifficult for Ms. C to access due to bodyhabitus so she has difficulty applying mostdressings and is oen forgetful/semi-non-compliant. She had been using compres-sion stockings in conjunction with variousfoam dressings. Ms. C also has experi-enced multiple recurrent infectionscaused by MRSA, Pseudomonas, Kleb-seilla, and Enterobacter species.
The antimicrobial foam dressing wasapplied to address copious drainage. Ms.C found the dressing uncomfortable be-cause it deformed surrounding skin
under compression. However, drainagewas controlled adequately and Ms. Cshowed no signs of skin sensitivity.Dressing use was discontinued due todifficulty of application and discomfort.
ConclusionThe Kendall AMD antimicrobial foamdressing appeared to work for highly ex-uding wounds. Antimicrobial activitycould not be assessed in this three-pa-tient trial — all of the patients with re-current cellulitis were receivingantibiotics at the time of the study. Thedressings showed yellowing around theedges; this probably did not affect theirefficacy but was noted by the patients.The dressing color easily displayed thecolors of the wound discharge.
Moderator’s Commentaryese cases demonstrate that exudate manage-
ment is excellent with these dressings. Two patientsreported that the dressings were comfortable withno skin sensitivities. Patients with venous insuffi-ciency and lower leg ulcers usually have largeamounts of drainage and dressings that can managethe exudate in conjunction with compression arenecessary. Many of these patients also present withskin problems like stasis dermatitis that may be sec-ondary to some type of sensitivity to products used.e fact that no sensitivities developed is important.It is also interesting that in the first two cases, thepatients had ulcers of long duration with historiesof multiple recurrent infections. MSSA, MRSAand Pseudomonas were among the organisms re-ported. is supports the data that many venous ul-cers are non-healing because of high bacterial counts.Although the patients were on systemic antibiotics,and any positive outcomes could not be contributeddirectly to the antimicrobial topical dressing, localwound bioburden control and prevention of crosscontamination always have positive outcomes whenmanaged effectively.
22 Supplement to OWM • March 2009
Balancing a Dynamic Wound Environment
Moderator’s Final Commentary
Carolyn Cuttino, RN, BS, CWOCN, Medical University of South Carolina, Charleston, SC
D iscussion throughout thispaper has focused on topicalmanagement of wound
bioburden. It has been demonstratedthrough laboratory studies, clinicalstudies, and these case presentationsthat the KendallTM AMD antimicrobialfoam dressings and other AMD dress-ings can be effective choices for manage-ment of MRSA, VRE, Pseudomonasaeruginosa and other clinically relaventbacteria in the chronic wound. The uti-lization of antimicrobial dressings forthe wound with clinical symptoms ofcritical colonization and even in con-junction with systemic antibiotics alsohas been discussed. But what about thecolonized wound with no signs and
symptoms of a potential problem or in-fection? Is there a place for a “prophy-lactic” or “proactive” dressing that willprevent critical colonization and poten-tial wound infections from occurring,and, at the same time, manage excessive,unhealthy chronic wound fluid? Withthe increasing problem of wound infec-tions and non-payment for wound com-plications, with the increasing problemof HA-MRSA and CA-MRSA andother antibiotic resistant organisms, andwith the increasing financial burdenchronic wounds and their complica-tions are placing on the healthcare sys-tem, using a cost-effective, proactiveantimicrobial dressing that can effec-tively manage wound bioburden and
drainage and also provide an effectivebarrier to prevent cross-contaminationseems like a reasonable and viable strat-egy. Healthcare providers must be proac-tive in decisions about their managementof bioburden in chronic wounds.
Ms. Cuttino is a board-certified en-terostomal therapy nurse at the MedicalUniversity of South Carolina. She hasserved as a consultant in wound care foracute-care facilities, long-term-care facil-ities, and industry. Ms. Cuttino haschaired regional wound care meetings forthe past 10 years and has educated thou-sands of clinicians while receiving consis-tently excellent evaluations.
H6414