case study on neonatal death reduction in china composition of country teams lingli zhang, ddg of...
TRANSCRIPT

Case study on neonatal death reduction in China
Composition of Country Teams
Lingli Zhang, DDG of MCH Dept., NHFPCRong Luo, Director of Policy Division, NCWCHYan Wang, Researcher on Child Health, NCWCHCao Ying, Safe the Children, China Program Sufang Guo, MCH Specialist, UNICEF China
1

[Country Profile]
Epidemiology and Demography: •Total population: 1.34 billion•Women (15-49 years): 380 million (28.5%)•Children <5 years: 76 million (5.7%)•Live births: 16 million
2
Heilongjiang
Jilin
Liaoning
Hebei
Guangdong
Hainan
Shandong
Jiangsu
BeijingTianjin
Shanghai
Fujian
Zhejiang
Hong KongMacao
Taiwan province
Xinjiang
Tibet
Qinghai
Sichuan
Yunnan
Gansu Inner Mongolia
Shaanxi
Ningxia Shanxi
Chongqing
Hubei
HunanGuizhou
Guangxi
Jiangxi
Henan
Anhui
EasternCentralWestern
Regions

Description of the bottleneck analysis process Key partners involved during the process
• Department of Maternal and Child Health, NHFPC
• National Center for Women and Children’s Health
• China CDC• PKU• UNTG on MCH, China
3

Description of the bottleneck analysis process
• As part of child survival strategy review in China• National consultation• UN partner consultation
4

Data Collection Methods
• Government Document review• Open published literature review• Key informer counseling: individual and
group
5

Update on the Situation of Children and Women
Focus areas/Outcomes of H&N program is based on the six WHO health system building blocks

Good progress has been made!MMR and U5MR trends, 2000-2012
22
MMR U5MR
Deaths per 1,000 live births
16
Target:22 Target:16

Age distribution of deaths among under-five childrenNew-born account for 50% of U5MR
8Source: Ministry of Health, China Health Statistical Yearbook, 2012
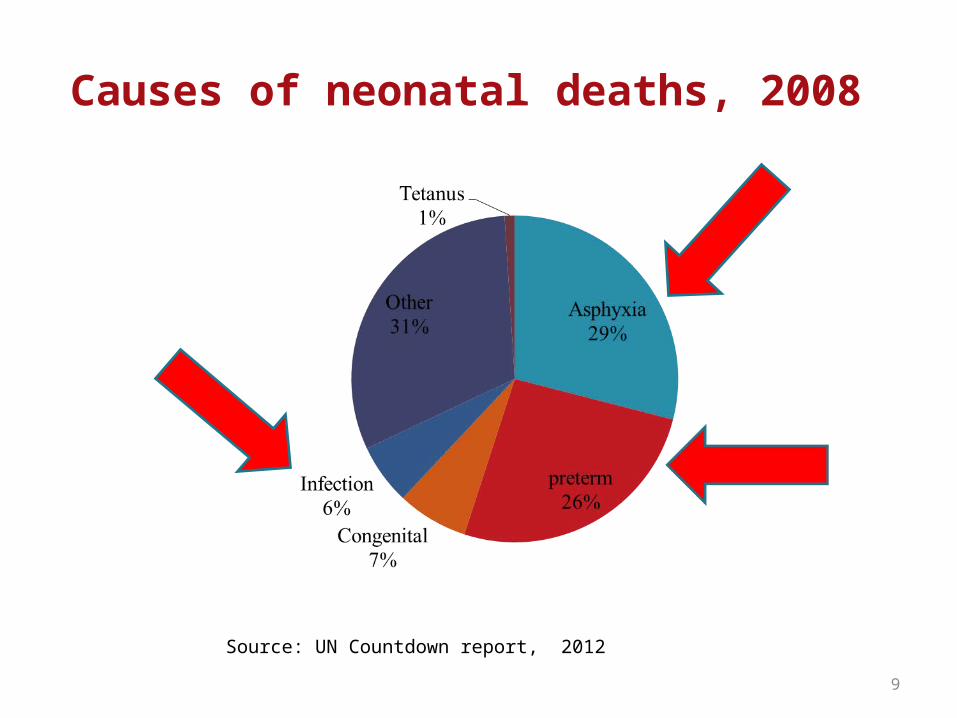
Causes of neonatal deaths, 2008
9
Source: UN Countdown report, 2012

In postnatal and infancy periods coverage of interventions is still low
10
Coverage of interventions across the continuum of care for maternal and child health, 2008 and 2011

As hospital delivery rate increased, newborn mortality rate reduced
NM
R (1/1000 LBs)
HD
R (%
)
Source: China Health Statistic Year Book, 2011

Access
• Physical access: National average:88%; • Financial access:
– Although health insurance coverage in general population reached 88% (2008) and 96% (2011), that figure was low among newborn
– Hospital delivery subsidy for rural women.
• Cultural access: HDR is still less than 50% in specific
areas due to direct and indirect cost such as transportation, accommodation and cultural/belief
12
Health Insurance coverage (%)
2003
2008
2011

Service delivery (including quality of care)
• Although quality of care has been improving, – only 56% of county level health facilities could provide
CEmONC – 31% of township level hospitals could provide BEmONC – 10% county and township level health facilities are not
qualified to provide BEmONC but they are providing BEmONC (MOH/UNICEF HR and facility survey).
• UNICEF is planning to work with MOH to develop standardized materials for in-service and pre-service training.
• Involving more sectors in health promotion/C4D is urgently needed.
13
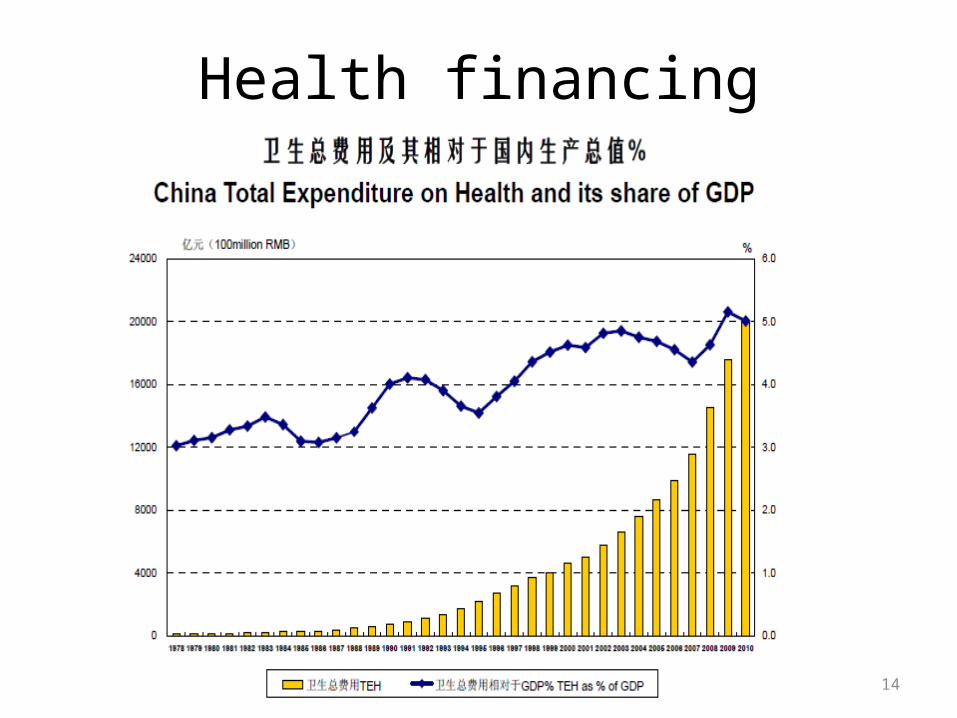
Health financing
14

• OOP
15
Leadership and governance
• MCH Law and NPAs for women and children exist, guidelines for MCH are available.
• Policies to address in-equities in recent health sector reform– Basic PH (free MCH service)– Priority PH program (Hospital delivery subsidy, folic acid supplement for pregnant women,
integrated of PMTCT of HIV/syphilis/HBV ).However, some of financial input is left for local government which makes the policy enforcement
weak.
• Code for marketing of breast milk substitutes/ baby friendly hospitals/ policies to encourage early initiation of breast feeding and exclusive breast feeding exist, but it is very weak and lacks enforcement and monitoring.
• Coordination mechanism for MCH is available (NPA).
16

Medical products, vaccine and technology
• Essential equipment are available in most of local health facilities.
• Some important essential drugs are not available. ORS is in essential drug list, but not necessary low osmolality ORS and not available in many clinics.
17

Information
• Maternal and child mortality surveillance system and MCH annual report system are available. Consolidated HMIS on MCH is planning.
18

Situation of health workforce is improved, disparity exists
Number of physician and nurses, per 1,000 population

Equity analysisEquity Analysis

Maternal mortality ratio, 2000-2012
21
22
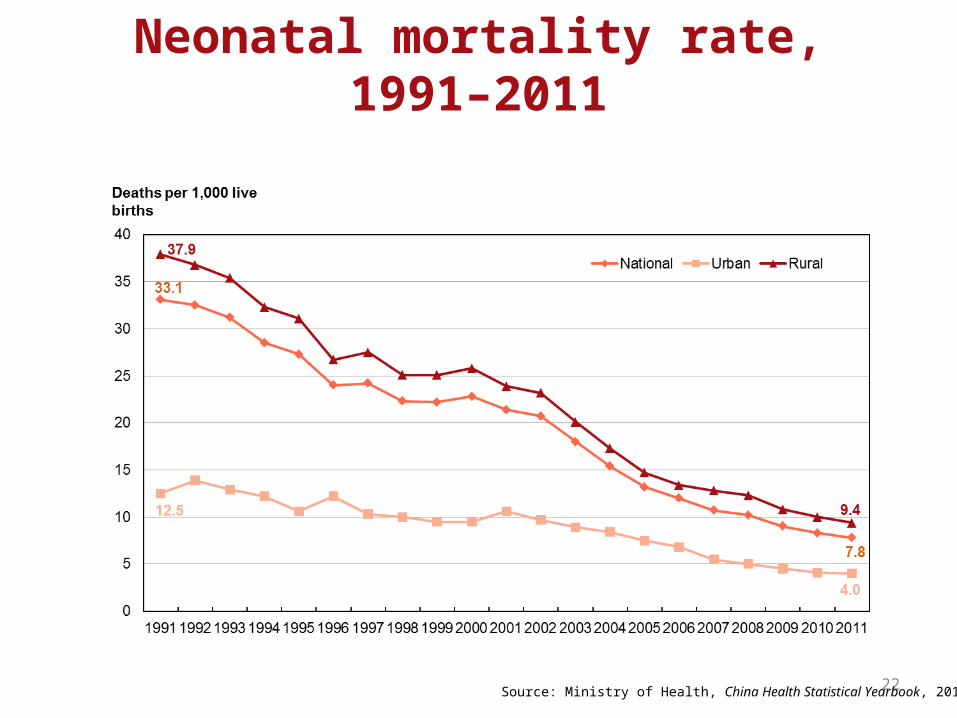
Neonatal mortality rate, 1991–2011
Source: Ministry of Health, China Health Statistical Yearbook, 2012

Despite overall progress,China is reducing U5M in an inequitable way
U5MR in provinces in China, 2011 Beijing
Jiangsu
Guangdong
Tianjin
Shanghai
Jilin
zhejiang
Hunan
Henan
Shandong
Fujian
Guangxi
Liaoning
Chongqing
Anhui
Shanxi
Hubei
Hebei
Jiangxi
Heilongjiang
Shaanxi
Sichuan
Guizhou
Hainan
Inner Mongolia
Ningxia
Gansu
Qinghai
Yunnan
Tibet
Xinjiang
Highest U5MR is 8x more than lowest U5MR:± 203,560 children can be saved yearly
should the whole country have the lowest U5MR
Source: MCMSS, 2011; extrapolation based on SOWC, 2012
2015 target

In western provinces and rural areasantenatal care (5 visits) coverage is still low
24
资料来源: Qun Meng, Ling Xu, Yaoguang Zhang, Juncheng Qian, Min Cai, Ying Xin, Jun Gao, Ke Xu, J Ties Boerma, Sarah L Barber , “ 2003—2011年中国医疗卫生服务的可及性及经济保护变化趋势分析:一项横断面研究”,《柳叶刀》, 2012 年 3 月 3 日,第 379 卷,第 9818 期,第 805-814 页
Description of the bottleneck analysis process Key partners involved during the process
• Department of Maternal and Child Health, Ministry of Health
• National Center for Women and Children’s Health
• China CDC• PKU• UNTG on MCH, China
25

Description of the bottleneck analysis process
• As part of child survival strategy review in China• National consultation• UN partner consultation
26

Data Collection Methods
• Government Document review• Open published literature review• Key informer counseling: individual and
group
27

Bottleneck analysis
28

Newborn care in generalPRIORITY BOTTLENECKS STRATEGIES AND SOLUTIONSLow health insurance coverage for newbornHigh OOP
Advocate national policy makers on financing of newborn health to reach free service for newborn care
Lack of costed newborn health package
Conduct costing exercise and develop costed plan
Limited budget for C4D on newborn health and lack of C4D plan for newborn care
Budgeted C4D plan for newborn care
Poor access in terms of physical, financial and cultural access in remote areas
MWR, CCT, C4D
Insufficient staff trained for newborn care (pediatricians, obstetricians, midwives, nurses) in county and lower level institution
Recruitment of staff (pediatricians, obstetricians, midwives, nurses);Incentives for staff to stay in stations ;Staff training based on identified needs;Training need to combine with the practice;
Standard training package for in-serve and pre-service
Update evidence based standard training model for in-service and pre-service
Few BFHs stick to BFH standardLow EIBF rate
Need strong enforcement and M&E for BFH
Quality of delivery and PNC care are poor
Training plan 29

Prevention and management of preterm birth PRIORITY BOTTLENECKS STRATEGIES AND SOLUTIONS
Cost-effective interventions is not applied in poor China (such as kangaroo mother care)Limited capacity on staff
Promotion of cost-effective intervention base on Chinese context
Long and short term plan
30
PRIORITY BOTTLENECKS STRATEGIES AND SOLUTIONS
Physical, financial and cultural barriers for accessing to health service
Focusing on targeted areas and improving access to HD through MWR, CCT,
Skilled care at birth
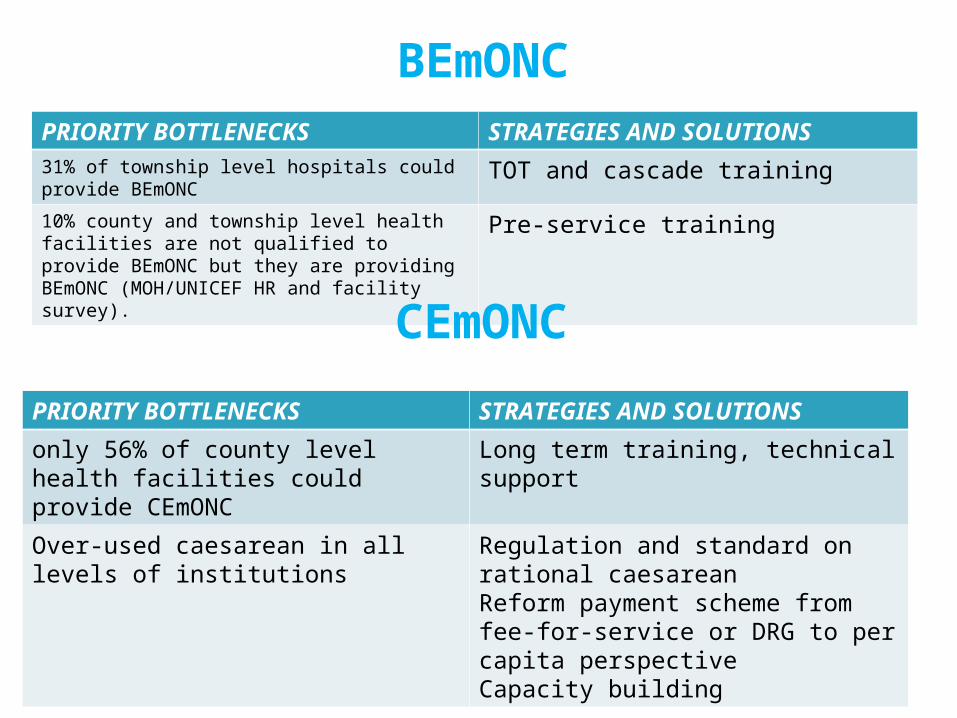
BEmONCPRIORITY BOTTLENECKS STRATEGIES AND SOLUTIONS31% of township level hospitals could provide BEmONC TOT and cascade training10% county and township level health facilities are not qualified to provide BEmONC but they are providing BEmONC (MOH/UNICEF HR and facility survey).
Pre-service training
31
PRIORITY BOTTLENECKS STRATEGIES AND SOLUTIONS
only 56% of county level health facilities could provide CEmONC
Long term training, technical support
Over-used caesarean in all levels of institutions
Regulation and standard on rational caesareanReform payment scheme from fee-for-service or DRG to per capita perspective Capacity building
CEmONC

32
Caesarean Section rate is still high
Caesarean section rate, 2003, 2008 and 2011
资料来源: Qun Meng, Ling Xu, Yaoguang Zhang, Juncheng Qian, Min Cai, Ying Xin, Jun Gao, Ke Xu, J Ties Boerma, Sarah L Barber , “ 2003—2011年中国医疗卫生服务的可及性及经济保护变化趋势分析:一项横断面研究”,《柳叶刀》, 2012 年 3 月 3 日,第 379 卷,第 9818 期,第 805-814 页

Basic Newborn Care PRIORITY BOTTLENECKS STRATEGIES AND SOLUTIONS
Low EIBF Introduction first embrace
Low EBF Government’s commitment on promotionBFHI
Poor quality of PNC Increase staffingIn-service, out of service training
33

Neonatal ResuscitationPRIORITY BOTTLENECKS STRATEGIES AND SOLUTIONS
Poor capacity in grass root level
• National policy: at least one staff received updated training on newborn resusitation
• Training of staffs from grass-root level• Introduce HBB in specific relevant
areasLack of essential equipment in gross root health facilities
Advocate and development of standard equipment package for MCH
34
PRIORITY BOTTLENECKS STRATEGIES AND SOLUTIONS
Kangaroo Mother care is not widely used Training and C4D
Kangaroo Mother Care

Per 1,000 LBs % of child death
Number before the name of province: GDP rank in reverse orderBlue: UNICEF project provinces
Red number: Per capita GDP rank in reverse order
Strategic directions

Thanks
Show your handif we reach you?!