cases of - pmj.bmj.com
TRANSCRIPT

397
SOME CASES OF GOUTBy DAVID LEvI, M.S., F.R.C.S.
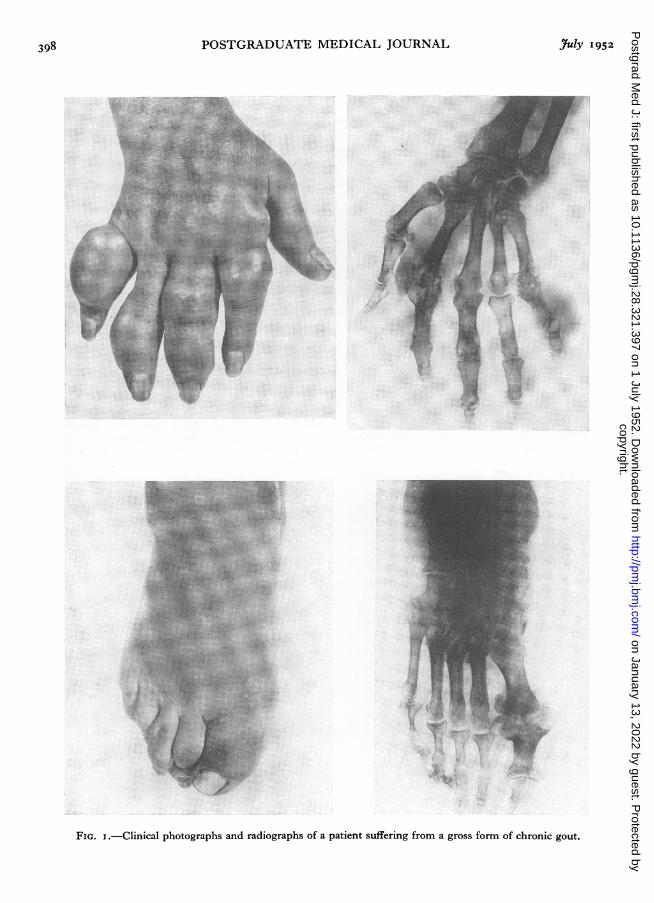
Under the highly artificial conditions in whichwe work, gout is considered to be within the pro-vince of the physician. It is therefore with somediffidence that I, as a general surgeon, write aboutit. During the last twenty-five years, however, Ihave discovered a number of patients sufferingfrom gout and have been able to direct them toexpert medical care. Many surgeons have banishedall thought of gout from their minds and this ismy plea, that in the investigation of a patientsuffering from pain which does not fall within arecognized orthopaedic classification, gout shouldbe considered before the patient is sent awaywithout a diagnosis being made or given a pro-longed course of useless symptomatic treatment.No one would miss the diagnosis in the patient
suffering from chronic gout chosen to illustratethis brief communication (Fig. i). The plasmauric acid was 8 mg. per ioo ml. (normal 2 to 4mg.). The radiographs show the typical punched-out erosions of bone. Gout seldom presentsitself in such a gross form; it may be hidden orlatent and may affect almost any joint in the body.For example, a medical colleague, a Fellow of theRoyal College of Physicians, suffered an obscurebut very painful arthritis of the hip joint and worea caliper for several months. He writes as follows:
' You ask for my experience of gout involvingthe hip. It must be fairly rare because orthopaedicsurgeons have never diagnosed it. Deposits in thelower lumbar region may also explain the attacksof lumbago and sciatica which occur in goutysubjects. Failure to recognize the aetiology maybe serious because immobilization in bed maymake the gout worse, whereas continuance ofactivitv and a sufficiency of salicylate will usuallyreliere tll the symptoms until the next attackcomes. My history is briefly this:'My family history revealed nothing relevant.
About the age of 42 bilateral inflammation of thefirst metatarso-phalangeal joints developed, worseon the right side. The diagnosis was " arthritisof unknown origin." The treatment was firstly ametatarsal bar which failed to give relief, than a
walking plaster. The arthritis gradually sub -sided.'About the age of 46 a persistent eczema without
obvious cause appeared; it was not diagnosed butwas probably gouty in origin. X-ray treatmentfailed but the condition subsided after some weeks.About the age of 47 arthritis developed in the righthip with symptoms slight at first, but becomingacute after immobilization in bed.
' Radiographs showed marked changes and lossof joint space. Gout was not diagnosed eventhough the blood uric acid was raised to 6.7 mg.!The condition was though to be infective arthritis.After five weeks of immobilization pain developedin the right knee and then suddenly an effusion.The whole episode resulted in seven months oftotal incapacity, during which time treatment wascarried out first by extension and then with a longplaster spica. This was followed by four monthsof partial incapacity in a short plaster spica.During this time there was one mild attack ofbilateral arthritis of the first metacarpo-phalangealjoints. Gout with various subsequent minorepisodes has been treated along accepted modernlines without incapacity.'
In the case of another medical colleague, aconsulting neurologist, the diagnosis was not sodifficult. He writes as follows:
' I can think of few ailments better suited to thepurpose of sharpening a doctor's sympathies bypersonal suffering than an attack of gout. Itsconnection with alcohol is often debated, but inmy case an attack has now been preceded on twooccasions by the luxury of a bottle of sparklingwine. The first time I had noticed paraesthesiaeover the distribution of the lateral cutaneous nerveof the left thigh for two weeks. The tinglingwaxed and waned and I wondered about apicalsepsis or perhaps whether I had bruised the nervein its fascial tunnel below the anterior superioriliac spine without noticing it at the time. Afterentertaining some friends on Asti Spumanti, how-ever, the paraesthesiae gave way at 3 a.m. toa severe ache in the same region, and a branch of
copyright. on January 13, 2022 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.28.321.397 on 1 July 1952. Dow
nloaded from
POSTGRADUATE MEDICAL JOURNAL
FIG. I.-Clinical photographs and radiographs of a patient suffering from a gross form of chronic gout.
.7IY I1952398copyright.
on January 13, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.28.321.397 on 1 July 1952. D
ownloaded from

LEVI: Some Cases of Gout
the superficial peroneal nerve became so tendernear the base of the first left metatarsal bone thatany pressure on it sent a shower of sparks towardsone side of the great toe.
' Two days later we entertained with a hock atdinner, and again about 3 a.m. I was aware of astinging pain, this time in the end of the leftmiddle toe. I thought I must have cut the toe-nail too short and drowsed fitfully until daylight.Then came the discovery: the tip of the middletoe was just like a cherry plum and tender to thetouch. My wife was amused. A colleague agreedwith the diagnosis of gout, and Colchicine, 1/120gr., repeated every six hours for about six doses,together with some acetylsalicylic acid, cleared illthe symptoms. The cherry plum appearance ofthe toe disappeared in a few days, but the super-ficial peroneal nerve remains not quite normal.
' My gouty diathesis did not declare itselfagain until the Minister of Health announcedsome overdue financial rewards to general prac-titioners. This coincided with our local B.M.A.dinner, and champagne was the order of theevening. Again at about 3 a.m. I was awakenedwith a feeling of a splinter of glass under the toe-nail, now in the second right toe. Four doses ofColchicine and all was well.'Gout may be the cause of a persistent painful
arthritis of the knee joint, as the following case-history illustrates:A woman, then aged thirty-two years, first
complained of a painful and swollen knee joint inI946. There was a previous history of an accidentin 1939 causing synovitis of both knees for whichshe had attended hospital as an out-patient. InI945 synovitis of one ankle joint developed for noobvious reason. On examination the right kneewas said to be swollen, tender and full of fluid.The radiographs showed early arthritic changesso nondescript that they are not worthy of repro-duction here. The sedimentation rate was 6(Westergren); the central nervous system appearednormal to clinical tests.The patient was given a course of diathermy
and faradism to the quadriceps with some relief,but the condition returned after three months.The sedimentation rate rose to the upper limit ofnormal (io and I2) and in I947 two courses ofpenicillin and one of gold were given withoutany result. Two courses of lactic acid injections,further physical treatment and histamine ionization
gave a measure of relief. A course of deep X-raytherapy was next contemplated.
I saw this patient in 1948, when there was alarge fusiform swelling of the right knee joint, thequadriceps muscle was wasted, the joint was dis-tended with fluid and movement was restricted.The plasma uric acid level proved to be 6. Thereaction to colchicine was dramatic-.the symptomssimply vanished and full movement of the kneewas regained during the following year. Latershe married and went abroad with her husbandand a good supply of colchicine.Gout may also mimic chronic strain of the
wrist or a lesion of the rotator cuff of the shoulder.It may also be a cause of recurrent attacks of painin the back. The following case-history illustratessome of these points:
In I952 a lady aged forty-eight years attendedthe out-patient department complaining of painfor three months in the right wrist, thumb andindex finger, with radiation up the arm to theshoulder. There was a recent history of a blowon the wrist from a swing door, but in fact shehad had intermittent pain in the wrist and also inthe back for a number of years. She had lived inthe tropics and had suffered from sprue. Thepicture was further complicated by a chronicsinus infection. She had been treated by hergeneral practitioner with all the usual ' rheumaticremedies.' On examination, movement of alljoints in the right upper limb was full and free.On palpation there were no tender areas. Cir-culation in the hand was good in all positions.Radiographs of the cervical spine, shoulder andwrist were reported as normal. The plasma uricacid was 4 mg. per ioo ml. Colchicine wasprescribed and produced immediate relief.
Colchicine dispensed indiscriminately to out-patients will seldom produce anything but dis-appointment. Given, however, to the right patientit is a ' wonder medicine ' and its peculiar taste isimmediately forgiven. Selection of the correctmedicine for the disease is no new game: it hasbeen practised with varying success from the timeof Hippocrates and even earlier. It is a mentalexercise in which the successful clinician excels.
AcknowledgmentThe clinical photographs were kindly taken by
Mr. Peter Hansell of the Photographic Departmentof the Westminster Hospital.
3uY-I I 952 399copyright.
on January 13, 2022 by guest. Protected by
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.28.321.397 on 1 July 1952. D
ownloaded from