cerebral palsy: prevalence, predictability, and parental...
TRANSCRIPT

Cerebral Palsy: Prevalence, Predictability,and Parental CounselingRyan M. McAdams, MD,*
Sandra E. Juul, MD, PhD*
Author Disclosure
Drs McAdams and
Juul have disclosed
no financial
relationships relevant
to this article. This
commentary does
contain a discussion
of an unapproved/
investigative use of a
commercial
product/device.
AbstractCerebral palsy (CP) is the most common cause of severe physical disability inchildhood, occurring in approximately 2 in 1,000 liveborn infants. Although theprevalence of CP appears to have stabilized in the past 2 decades, recent studiessuggest that severe CP may be decreasing. Neuroimaging studies help identifyabnormal neuroanatomic findings, which are found in most affected children. Neu-ropathology identified by magnetic resonance imaging (MRI) corresponds well toclinical descriptions of motor impairment in children who have CP. Clinical riskfactors, combined with imaging studies, can help identify a subpopulation of infantswho are at high risk for poor neurodevelopmental outcome. Counseling caregivers onfuture adverse developmental risks can be challenging for the clinician in the neonatalintensive care unit (NICU), especially because the cause of CP remains unexplained inmost cases and is typically diagnosed outside the neonatal period. Early counseling offamilies of at-risk neonates may function as the starting point for parental adaptationto a lifelong condition that requires ongoing services and adjustments to promote theoverall health and well-being of their child.
Objectives After completing this article, readers should be able to:
1. Define cerebral palsy (CP).2. Discuss the epidemiology and risk factors for CP.3. Address the capabilities of neuroimaging to predict and classify CP.4. Review the neonatologist’s role in discussing and disclosing information to families
related to long-term outcome in infants at risk for CP.
IntroductionCP is the most common cause of severe physical disability in childhood. (1) This lifelongcondition may alter the trajectory of many aspects of a child’s development, both primarilyand secondarily. In the United States, it is estimated that approximately 764,000 childrenand adults manifest one or more of the symptoms of CP and that 10,000 babies bornannually develop CP (United Cerebral Palsy, http://www.ucp.org/uploads/media_items/cerebral-palsy-fact-sheet.original.pdf, accessed March 2011). Loss of productivity,dependency, progressive deterioration of motor physical function, recurrent use of reha-bilitation services, and reduced life expectancy all contribute to the economic burden,which has been reported in different global settings. (2) The Centers for Disease Controland Prevention has estimated the average lifetime costs per person who has CP to be$921,000 (in 2003 dollars), with lifetime costs for all affected people who were born in2000 to be $11.5 billion. (3) The Danish Cerebral Palsy Register, which has registeredabout 50% of the Danish population of individuals who have CP since 1950, estimated thelifetime cost of CP at about €860,000 for men and about €800,000 for women($1,317,200 and $1,225,600, respectively, for 2008 exchange rates).
DefinitionCP is an umbrella term describing multiple diseases originating early in life that arecharacterized by variable motor impairments due to unspecified causes and cerebralpathologies. No definitive diagnostic tests are available. The current definition of CP was
*Department of Pediatrics, University of Washington, Seattle, WA.
Article neurology
e564 NeoReviews Vol.12 No.10 October 2011
by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from

published in 2005, based on the conclusions of an Inter-national Workshop consisting of experts in the field ofdevelopmental disorders:
“Cerebral palsy describes a group of disorders of thedevelopment of movement and posture, causing activitylimitation, that are attributed to nonprogressive distur-bances that occurred in the developing fetal or infantbrain. The motor disorders of cerebral palsy are oftenaccompanied by disturbances of sensation, cognition,communication, perception, and/or behavior, and/orby a seizure disorder.” (4)
The definition excludes progressive brain disorders aswell as neurodevelopmental disabilities lacking aberra-tions of movement and posture. Although the brainpathology in patients who have CP is static, motor abilityimpairments related to CP may change over time. Vari-ous secondary conditions that are not a part of theprimary disabling condition but occur as a result of thecondition may adversely affect function and quality oflife. (5)
CP should not be viewed as a singular diagnosisbecause the term CP encompasses multiple etiologicdiagnoses. It is best considered a descriptive label basedon a broad range of presentations that include type,severity, and bodily distribution of primary motor im-pairment, associated nonmotor neurologic and behav-ioral impairments, functional deficits, and cerebral pa-thology. A similar clinical pattern of CP may resultdespite different causes at different developmental stages;alternatively, a similar cause may produce variable clinicalpatterns of CP. Thus, clinical classification provides in-sufficient insight into the cause of CP. Although the CPlabel does not specify a particular cause or pathology,affected children are typically grouped into phenotypicsubtypes based on the distribution of limb weakness andtype of tone abnormality. CP is categorized as spastic,ataxic, or dyskinetic, and the distribution is categorizedas bilateral or unilateral. Most cases of CP among chil-dren born preterm are of the spastic type, rather than theathetotic or dyskinetic types. (6) The most commonspastic subtypes in these children are diplegic (bilaterallimb involvement) or hemiplegic (unilateral limb in-volvement). The diagnosis of CP is typically made afterthe age of 2 years, but identification of the patterns ofaberrant motor posture and function associated with CPcan be made as early as 6 months of age. (7)
PrevalenceApproximately 2 in 1,000 liveborn children sufferfrom CP. (8)(9) Globally, the reported incidence andprevalence of CP varies by region, population, age,
and severity, which may limit the generalizability ofpopulation-based results. Determining who to include inpopulation-based CP registers or surveillance systemsremains a challenge because of the lack of universalagreement on age cutoffs for determining nonprogres-sion of CP.
Tracking trends of gestational age-specific CP preva-lence along with gestational age-specific survival is im-portant to clarify if improved survival is linked to in-creased prevalence of CP. Because neonatal intensivecare is dynamic, survival and outcome trends should beevaluated periodically to assess the effectiveness and sus-tained improvement in care practices. Focusing on peakCP prevalence rates in population-based studies con-ducted over long time intervals may misrepresent recenttrends reflecting decreased CP prevalence associated withimproved survival. The true prevalence of CP may beunderreported because severely impaired infants may diebefore developing findings that are diagnostic of CP orbefore their abnormalities meet criteria for a diagnosis ofCP. In addition, if children who have mild CP are notbrought in by their parents for evaluation, the trueprevalence of CP in population studies is underreported.
Prevalence in Term InfantsThe risk of CP among term infants is much lower than inpreterm infants, although most CP is associated withterm deliveries because most infants are born at term.Globally, CP prevalence data show some geographicdifferences, but overall, population-based reports haveshown a fairly stable rate among the term group at 1 to1.5 per 1,000 live births. (10)(11)(12)(13)(14) Al-though the overall prevalence of CP has been stable,recent studies suggest that severe CP may be decreasing,as demonstrated by studies of children who had CP bornat term from Iceland and Sweden showing a significantdecrease in the proportion that had two or more associ-ated impairments. (14)(15) Affected Icelandic childrenborn at term from 1997 to 2003 had better gross motorabilities, were less likely to suffer from epilepsy, and weremore likely to have the diplegic subtype of CP whencompared with those born from 1990 to 1996. (14)Data from the Surveillance of Cerebral Palsy in Europenetwork, a population-based CP register representingthe largest international collaboration of CP registers inthe world, demonstrated significant changes in the prev-alence of spastic CP subtypes in children born withbirthweights of at least 2,500 g born between 1980 and1998. (8) The bilateral spastic form increased from 0.58(95% confidence interval [CI], 0.41 to 0.80) in 1980 to0.33 (CI, 0.22 to 0.46) in 1998, and the unilateral
neurology cerebral palsy
NeoReviews Vol.12 No.10 October 2011 e565 by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from

spastic form increased from 0.37 (CI, 0.23 to 0.58) to0.46 (CI, 0.34 to 0.62), with a concurrent reduction inneonatal mortality from 1.7 (CI, 1.4 to 2.1) to 0.9 (CI,0.7 to 1.1) per 1,000 live births. Similar decreasingtrends in the proportion of infants weighing more than2,500 g who had spastic diplegia (62% in 1988 to1993 and 44% in 1994 to 1998) have been reported inSlovenia. (16) Additional population-based research isneeded to determine if functional status and severity ofassociated comorbid conditions among affected childrenof various birthweights and gestational ages are alsoimproving over time.
The risk for CP in term deliveries may vary, de-pending on the timing of birth within the term period.Moster and associates (17) reported a prevalence of CPof 1.15 per 1,000 births (CI, 1.10 to 1.20) based on apopulation-based follow-up study using the MedicalBirth Registry of Norway. CP was diagnosed in 1,938 of1,682,441 singleton children born between 1967 and2001 whose gestational ages were 37 through 44 weeks.Delivery at 40 weeks’ gestation was associated with thelowest risk of CP (0.99 per 1,000; 95% CI, 0.90 to1.08) compared with delivery at 37, 38, or later than41 weeks’ gestation, which was associated with an in-creased risk of CP. Whether the timing of delivery (tooearly or too late between 37 and 44 weeks) increases therisk of CP or if fetuses predisposed to CP have a distur-bance in the timing of their delivery is unclear.
Prevalence in Very Low-birthweight InfantsGestational age and birthweight are interrelated factorsthat both affect CP risk. (14) In a large national Nor-wegian registry study that included 903,402 liveborninfants, those born between 23 and 27 weeks’ gestationwere 78 times more likely to have CP than those born atterm. (18) Although children born before 32 weeks’gestation have an increased prevalence of CP (up to10%), they contribute to less than 2% of neonatal sur-vivors and to a minority (approximately 20% to 25%)of all CP in developed countries. (19) A prospectivepopulation-based North of England Collaborative Cere-bral Palsy Survey demonstrated a prevalence of CP insingletons of 8.9 (72/8,082) per 1,000 neonatal sur-vivors whose birthweights were between 1,500 and2,499 g based on 5-year cohort data from 1996 to 2000.(20) Reported CP prevalence rates vary from 19 to 152per 1,000 live births for very preterm and very low-birthweight (VLBW) infants. (9)(21)(22)(23)(24) Thisbroad range reflects differences in regional infant mortal-ity rates, which influence the prevalence of CP in thesurviving population, as well as sample size differences
and changes in practice over time. A limitation of cur-rently available population studies is that the reported CPprevalence rates are often derived from patient cohortsthat include pooled data spanning the past 3 decades, atime period during which neonatology care practiceshave dramatically changed, thus diminishing the utilityof this information for parental counseling.
Several epidemiologic studies have shown that as sur-vival of extremely preterm infants has increased, theprevalence of CP initially increased, then stabilized, andsubsequently declined. (23)(25) For example, in North-ern Alberta, 2,318 infants of 20 to 27 weeks’ gestationalage whose birthweights were 500 to 1,249 g were liveborn from 1974 to 2003. (24) Overall, CP prevalencerates peaked in 1992 to 1994 at 131 per 1,000 live births,decreasing to 19 per 1,000 live births in 2001 to 2003.From 1992 to 1994 and 2001 to 2003, population-based survival increased in VLBW infants from 4% to 31%(P�0.001) for infants born at 20 to 25 weeks gestationalage and from 23% to approximately 75% (P�0.001) forinfants born at 26 to 27 weeks gestational age. As survivalof VLBW infants increased, the prevalence of CP de-creased. From 1992 to 1994 and 2001 to 2003, the CPrate decreased from 110 to 22 per 1,000 live births forinfants born between 20 and 25 weeks gestational ageand from 155 to 16 per 1,000 live births for infants bornbetween 26 and 27 weeks gestational age. (24) Thesefluctuations likely correspond with advances in obstetricand neonatal care that improve survival of very preterminfants. As new gestational survival boundaries arecrossed, the gestation-specific prevalence of CP tends toincrease, then decline as neonatal management tech-niques are refined. (19)
NeuroimagingThorough understanding of the pathogenesis, causes,and timing of different CP subtypes and severities re-mains elusive because CP is a complex heterogeneousdisorder diagnosed on clinical manifestations. To addressthis shortcoming, neuroimaging is currently recom-mended as a standard evaluation for children who haveCP. (26) Abnormal neuroanatomic findings are found in80% to 90% of children who have CP and are detectedmore often with MRI than with computed tomography(CT) scan, with white matter damage being the mostcommon abnormality seen. (27) Population studies toidentify MRI findings in children who have CP mayreveal characteristic pathologic neuroimaging patternsassociated with specific neurologic subtypes, CP severitylevels, and other categorical variables and ultimatelyserve as a biomarker for future outcomes. (28) Newer
neurology cerebral palsy
e566 NeoReviews Vol.12 No.10 October 2011
by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from

analysis techniques, such as functional connectivity MRI,volumetric analysis, and surface-based morphometry, arebeing investigated as tools to provide insight into altera-tions in structural and functional brain maturation asso-ciated with preterm birth. (29)
MRI for Predicting CPNeuropathology identified by MRI corresponds wellwith clinical descriptions of motor impairment in chil-dren who have CP. MRI findings of unilateral pathologyare typically associated with unilateral impairment,periventricular white-matter damage with lower limbspastic impairment (with upper limb involvement in-creasingly proportional to increasing damage), and basalganglia damage with dyskinetic impairment. (19) Asym-metric myelination in the posterior limb of the internalcapsule on MRI at 40 weeks postmenstrual age is associ-ated with subsequent hemiplegia in infants who haveperiventricular hemorrhagic infarction. (30) For infantswho have periventricular leukomalacia (PVL), bilateralabnormalities in the posterior limb of the internal cap-sule are associated with spastic diplegia or quadriplegia.(31) Brain malformations such as schizencephaly, liss-encephaly, polymicrogyria, and heterotopia have allbeen associated with spastic CP. These migrational dis-orders, found more commonly in children who have CPborn at term (�37 weeks gestational age) compared withpreterm, are characterized by varying levels of abnormalgyral and sulcal development and are more common inchildren who have hemiplegia, which also occurs morefrequently in children born at term. (27)
Abnormal findings on MRI at term-equivalent ages invery preterm infants strongly predict adverse neurodevel-opmental outcomes at 2 years of age. (32) The EuropeanCerebral Palsy Study, a cross-sectional population studycarried out in eight centers in Europe, demonstratedcorrelations between MRI findings and types of motorimpairments. (33) This study identified 585 childrendiagnosed with CP after the age of 2 years who were bornbetween 1996 and 1999, of which 431 were clinicallyassessed and 351 had brain MRI scans. White-matterinjury was found in 71.3% of the children who haddiplegia (n�87), 34.1% of those who had hemiplegia(n�31), and 35.1% of those who had quadriplegia(n�20). In general, children who had posterior-only orposterior and middle white-matter injury were found tohave spastic diplegia, whereas children who had spasticquadriplegia demonstrated damage across posterior,middle, and anterior brain regions per MRI. Most of thepreschool-age children who had hemiplegia (89%) anddiplegia (69%) were walking compared with only 9% of
those who had quadriplegia. Feys and associates (34)evaluated the relationship between neuroradiologic find-ings (MRI and CT scan) and upper limb function in 53children evaluated at a mean age of 5 years 7 months (SD4 y 6 mo) who had hemiplegic CP. Children in the PVLgroup (brain lesions occurring in the late second andearly third trimester) had better upper limb function thanthose in the congenital cortical-subcortical group (brainlesions occurring in the late third trimester or around thetime of birth).
The presence of white-matter lesions on MRI orcranial ultrasonography is a strong predictor of CP.(27)(32)(35)(36) A prospective longitudinal study of167 very preterm infants who had MRIs at term-equivalent ages and long-term neurodevelopmentalfollow-up evaluation at 2 years of age corrected forprematurity demonstrated that white-matter abnormali-ties, especially those that are moderate and severe, wereuseful markers for the elevated risk of severe cognitivedelay, severe psychomotor delay, CP, and neurosensoryimpairment. (32) However, a substantial proportion ofchildren who had moderate-to-severe white-matter ab-normalities were free of severe impairment at 2 years ofage. Children who have spastic syndromes frequentlyhave white-matter injury; children who have extrapyra-midal syndromes often have basal ganglia abnormalitieson imaging. (37)
PVL, a form of white-matter injury, is the most com-mon cause of CP in preterm infants. (38) PVL can resultin a cystic necrosis of white-matter tracts or diffusenoncystic lesions, which are now the predominant lesionsseen in preterm infants. A strong relationship exists withthe finding of cystic PVL and the development of CP.Fewer than 5% of preterm infants in whom repeatedultrasonography shows only increased periventricularechogenicity without cysts subsequently develop overtCP, although substantially more show evidence of cog-nitive dysfunction. (38) Diffusion tensor imaging hasdemonstrated significant variability in white-matter in-jury patterns in patients who have PVL, with the mostfrequent injury occurring to the retrolenticular part ofthe internal capsule, posterior thalamic radiation, supe-rior corona radiata, and commissural fibers. (39) PVLmay be seen in all subtypes of CP, but it is the primarylesion in patients who have spastic diplegia and likelyreflects a cerebral injury that occurred in utero. (33)(40)
Determining the timing of brain injury and whether itwas acquired pre- or postnatally remains challenging.Although white-matter injury such as PVL is believed tooccur before about 34 weeks of gestation, 25% of thewhite-matter injury group in the European Cerebral
neurology cerebral palsy
NeoReviews Vol.12 No.10 October 2011 e567 by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from

Palsy Study were born at term. (33) In a hospital-basedstudy of 130 children who had spastic CP, Kulak andassociates (40) reported that almost 50% the childrenwho had PVL were born at term and had no historiessuggestive of perinatal asphyxia or low birthweight.From a Quebec population-based registry (REPACQ),Towsley and colleagues (28) reported that 41 of the213 children who underwent neuroimaging studies(MRI or CT scan) had evidence of PVL and 15 (37%)were born at term. However, the REPACQ study dem-onstrated several characteristic differences between termand preterm children affected by both PVL and CP. (41)Spastic hemiplegia was significantly more common inthe term group (8/15 [53.3%]) than the preterm group(5/26 [19.2%]), whereas spastic diplegia was more com-mon in the preterm group (9/26 [34.6%]) than theterm group (2/15 [13.3%]). Superior motor outcomeswere more common in the term group, with 80% (12/15) able to ambulate independently compared withonly 46.1% (12/26) of preterm children. These differ-ences reveal that despite a common radiologic pattern,term and preterm children affected by both PVL and CPexhibit clinicopathologic distinctions that may be relatedto differences in prenatal and perinatal risk factors andthe timing of acquired brain injury.
Limitations of MRI in Identifying andPredicting CP
MRI and clinical findings do not always correlate well.Normal neuroanatomy is present in 10% to 20% of indi-viduals who have CP, (19)(27) and up to 25% of childrenwho have significant lesions such as PVL noted on MRIdo not develop any neurologic disorder. (42) In addi-tion, the location of brain lesions does not always coor-dinate with the topography of functional disabilities inchildren who have CP. The bilateral periventricular le-sions that are often seen in those who have hemiplegiaexemplify this apparent discrepancy. (34) Etiologic inter-pretations of anatomic image findings are commonlymade, despite insufficient evidence to support these as-sociations. Although abnormal MRI findings may corre-late with poor neurologic outcomes in children who haveCP, physicians should acknowledge the limitations ofMRI in accurately predicting the timing of neurologicinsult and the severity of long-term neurodevelopmentalproblems when discussing findings with families of in-fants at risk for CP. Physicians need to weigh the poten-tial risks associated with sedation and the costs associatedwith MRI in children who have CP with the benefit ofproviding families with an improved understanding ofneuropathology related to their child’s clinical findings.
Ultrasonography for Predicting CPCranial ultrasonography has been used extensively inpreterm infants to identify maturation-dependent neuro-logic injury. The presence of more than one abnormalultrasonographic finding has been associated with anincreased risk of developing quadriparesis or more severeforms of CP. (43) Echolucency and ventriculomegalyon ultrasonography are associated with subsequent CP.(32)(35)(43)(44) Ventriculomegaly identified closer toterm appears to be more predictive of CP than ventricu-lomegaly in the first 2 weeks after birth in very preterminfants. (43)(45) Cerebellar injury in term and preterminfants is associated with a high prevalence of long-term pervasive neurodevelopment disabilities. (46)(47)Messerschmidt and associates (48) studied the role ofthe cerebellum in neurodevelopment in 31 sex- andgestational age-matched pairs of former preterm infants(mean gestation, 27.0�1.6 wks) followed up at a mini-mum age of 24 months. Disrupted cerebellar develop-ment detected on cranial ultrasonography was asso-ciated with impairment of neuromotor and mental de-velopmental outcomes in preterm infants independentfrom supratentorial brain injury. Mixed (spastic–ataxic,spastic–dyskinetic) CP was diagnosed in 48% of affectedpatients, whereas none of the patients in the controlgroup had mixed CP.
Specific patterns of white-matter injury (eg, PVL) areassociated with increased risks of CP and can be detectedusing cranial ultrasonography. Himpens and coworkers(49) reported on the predictive value of ultrasonographyin 163 (16.1%) of 1,015 children who underwent cranialultrasonography during infancy in the NICU over an11-year period (1995 to 2005). CP was noted in 4% ofchildren who had normal ultrasonographic findings andin 30% of children who had abnormal findings. Infantswho had PVL grade III or greater were 79 times morelikely to develop CP (95% CI, 22 to 282). (49) Intra-ventricular hemorrhage (IVH), which is seen in pre-term infants also at risk for PVL, has been associated withpoor neurologic outcomes, including CP. IVH gradesIII and IV are significant predictors of major neurologicdamage, (50) whereas IVH grades I and II detected bycranial ultrasonography are not significant predictors ofCP. (51)
Limitations of Ultrasonography in Identifyingand Predicting CP
Limitations of cranial ultrasonography include poor sen-sitivity for diffuse white-matter abnormalities detected byMRI, (44)(52)(53) inability to image cortical and cere-bellar structures adequately, (54) and dependency on
neurology cerebral palsy
e568 NeoReviews Vol.12 No.10 October 2011
by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from

patent fontanelles to perform imaging that requires asufficient angle of insonation (anterior fontanelle) toassess the periventricular white matter. (44) Cranialultrasonography through the mastoid fontanelle candemonstrate injury, such as posterior fossa hemorrhage,missed by using the routine anterior fontanelle approachbut confirmed by MRI. (54)
Neuroimaging and CP in the Low-incomeSetting
Data regarding the clinical spectrum of CP in developingcountries are limited, and neuroimaging data are evenless relevant, despite the majority of births and cases ofbirth asphyxia occurring in these settings. In low-incomecountries, birth asphyxia is much more common thanin high-income countries, (55) which may influence thesubtype distribution in the CP population. Birth as-phyxia has been highly associated with CP in developingcountries. (56)(57) In north India, Singhi and asso-ciates (57) reported a history of birth asphyxia in 71%(25/35) of children who had spastic quadriplegia, with91.4% (32/35) having abnormal findings on brain MRIs(18/35 with diffuse encephalopathy). Failure to studythe epidemiology of CP in low-income settings morethoroughly limits our understanding of CP in areas of theworld where most people live. This epidemiologic short-coming needs to be addressed to appreciate fully theimpact and distribution of CP globally. Furthermore,understanding the contributing factors to the CP pop-ulation can guide global efforts targeting potentiallyhigh-yield interventions (eg, training health-care staffin newborn resuscitation and care of low-birthweightbabies) to decrease the development or severity of CPworldwide.
Parental CounselingBiomarkers allowing for the accurate prediction of whichneonate will develop CP are lacking. Clinical risk factorssuch as extreme prematurity, IVH, sepsis, or necrotizingenterocolitis, when combined with results of imagingstudies, can identify a subpopulation of infants that is athigh risk for poor neurodevelopmental outcome. De-spite this, a large European study demonstrated that atdischarge from the special care infant unit, 47.3% ofparents reported that they were unaware of any concernabout their child who later developed CP. (33) A chal-lenge for neonatologists is that the diagnosis of CP is notmade in the neonatal period but evolves over time. Theinherent heterogeneous nature of CP impedes the abilityto make an expeditious diagnosis, which may negativelycomplicate the initial disclosure process of communicat-
ing a diagnosis clearly to the family that may have animpact on future family adaptation and well-being. (58)A substantial number of children who eventually arediagnosed with CP come from the NICU environment.Therefore, early counseling of parents of neonates athigh risk for CP may function as the starting point forparental adaptation to a lifelong condition that requiresongoing services and adjustments to promote the overallhealth and well-being of their child. Table 1 lists somepotential future morbidities associated with CP. Parentsmay benefit from proactive informative counseling toeducate them about aspects of CP without provokingunnecessary anxiety, particularly given the limitationsin definitive prognostic capabilities during the neonatalperiod for future mobility function. (59) At the time ofdischarge from the NICU, neonatologists should com-municate to pediatricians any concerns for future dis-abilities in at-risk patients to avoid potential negativeaffects on parental satisfaction, delayed timing of diagno-sis, or inadequate provision of proper resources thatultimately may prevent optimal patient care.
Cranial ultrasonography is commonly obtained inthe NICU and may be useful in predicting severeneurodevelopmental abnormalities in preterm infants.(30)(31)(60) However, normal findings neither excludethe possibility that an infant may develop CP nor predictthat an infant may develop CP. In the ELGAN study of1,053 infants born before 28 weeks’ gestation diagnosedwith CP at 2 years of age, 43% (51/120) of children who
Table 1. Morbidities AssociatedWith Cerebral Palsy● Cognitive impairments● Epilepsy: 20% to 40% of patients● Behavior problems: 5 times more likely in children
who have CP● Pain● Weakness● Speech impairment: up to 80% of patients● Low visual acuity: up to 75% of all children who
have CP● Gastrointestinal and feeding problems: 50% of
children who have CP● Dental caries● Developmental enamel defects● Gingival health, tooth wear, oral mucosal health, and
malocclusion problems● Swallowing dysfunctions and dysarthria symptoms● Stunted growth: 25% of children who have CP● Under- or overweight problems: 50% of children
neurology cerebral palsy
NeoReviews Vol.12 No.10 October 2011 e569 by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from
had CP had normal cranial ultrasonography study re-sults. (43) Due to false-negative and false-positive re-sults, clinicians counseling parents based on cranial ultra-sonography findings alone should communicate therange of predicted results, including that 1) early abnor-malities may resolve; 2) even when abnormalities arepersistent, plasticity of the brain may modify the associ-ation between ultrasonographic abnormalities and im-pairments; and 3) an infant whose neonatal ultrasonog-raphy results are normal may develop CP or anotherdevelopmental impairment, even though the probabilityis low. (53)
Neonatologists counseling caregivers of neonates atrisk for CP should be aware of the potential for futuredirect negative ramifications on the caregivers. Childrenwho have long-term functional limitations, such as withCP, require a high level of care, which may have anegative impact on the physical and mental health of thecaregivers compared with the health of caregivers ofchildren who are not so affected. (61)(62) Caregivers ofchildren who have CP have higher levels and chronicityof distress, emotional and cognitive problems, physicalproblems, and financial strain compared with the generalpopulation. (61) When their child is diagnosed with CP,mothers may experience loss of both an “ideal” child andexpectations of “normal” motherhood. (63) Early dis-cussions in the NICU and in high-risk infant follow-upclinics informing caregivers of the possible negative im-pacts of caring for a child who has CP may allow for earlylifestyle adjustments through potential managementstrategies to minimize stress.
Counseling caregivers on future adverse developmen-tal risks can be challenging, especially because the causeof CP remains unexplained in most cases. More seriouscounseling should be given to the parents of infants whoare the most likely to develop CP based on abnormalneuroimaging findings and other risk factors associatedwith CP (Table 2).
Himpens and colleagues (64) recently proposed apredictive model based on perinatal characteristics andneonatal ultrasonographic-detected brain injuries toidentify specific infants at risk for developing CP. There isno single perfect approach to conveying serious, life-changing, and typically overwhelming medical informa-tion to caregivers, but certain strategies striving for im-proved communication are worthy of consideration.Ideally, counseling should involve both parents whenpossible or someone who can provide support to a singleparent and in a setting with minimal interruptions thatallows for privacy immediately after the counseling.(58)(65) Neonatologists should be direct, clear, sympa-
thetic, honest, and open, with a balanced viewpointwhen discussing the potential for future impairments;acknowledge the limitations of accurate predictionsgiven current diagnostic capabilities; and allow ampletime for parents to ask questions. (58)(65) Providingsufficient information has been very important whenassessing levels of parental satisfaction with disclosure ofa disability. (66) Parents should be offered the chance fortimely further discussion of potential future diagnoseswith the professionals present at the original interview.Providing parents with resources (written information ortrusted web sites) on CP and early support programs mayimprove their understanding and satisfaction with theirchild’s heath care. The availability of professional supportfrom a social worker, psychologist, or other health-careworker at the time of counseling, particularly when aformal diagnosis of a life-impacting disability such CP ismade, may help accommodate parental needs in adjust-ing to unfavorable news. Keeping parents of infants athigh risk for the development of long-term disabilitieswell-informed in the NICU, before the formal diagnosisof CP, may lead to better long-term parental copingmechanisms and subsequent better care for the affectedchild.
Table 2. Characteristic RiskFactors Associated WithCerebral Palsy PrevalenceRatesIncreased Prevalence
● Deprived socioeconomic populations● Male sex● Racial disparity: In the United States, prevalence
highest among African American males● Preterm premature rupture of membranes● Low Apgar scores● Perinatal asphyxia● Multiple gestation● Intrauterine infections● Chorioamnionitis● Mechanical ventilation >7 d
Decreased Prevalence
● Preeclampsia● Antenatal magnesium sulphate therapy● Antenatal corticosteriods● Caffeine: neonatal therapy
neurology cerebral palsy
e570 NeoReviews Vol.12 No.10 October 2011
by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from

References1. Koman LA, Smith BP, Shilt JS. Cerebral palsy. Lancet. 2004;363:1619–16312. Wang B, Chen Y, Zhang J, Li J, Guo Y, Hailey D. A preliminarystudy into the economic burden of cerebral palsy in China. HealthPolicy. 2008;87:223–2343. Office CDC Epidemiology Program. Economic costs associatedwith mental retardation, cerebral palsy, hearing loss, and visionimpairment–United States, 2003. MMWR Morb Mortal Wkly Rep.2004;53:57–594. Bax M, Goldstein M, Rosenbaum P, et al. Proposed definitionand classification of cerebral palsy, April 2005. Dev Med ChildNeurol. 2005;47:571–5765. Doralp S, Bartlett DJ. The prevalence, distribution, and effect ofpain among adolescents with cerebral palsy. Pediatr Phys Ther.2010;22:26–336. Hack M, Costello DW. Trends in the rates of cerebral palsyassociated with neonatal intensive care of preterm children. ClinObstet Gynecol. 2008;51:763–7747. Rosenbaum P. The definition and classification of cerebralpalsy: are we any further ahead in 2006? NeoReviews. 2006;17:e569–e5748. Sellier E, Surman G, Himmelmann K, et al. Trends in prevalenceof cerebral palsy in children born with a birthweight of 2,500 g orover in Europe from 1980 to 1998. Eur J Epidemiol. 2010;25:635–6429. Winter S, Autry A, Boyle C, Yeargin-Allsopp M. Trends in theprevalence of cerebral palsy in a population-based study. Pediatrics.2002;110:1220–122510. Dolk H, Parkes J, Hill N. Trends in the prevalence of cerebralpalsy in Northern Ireland, 1981–1997. Dev Med Child Neurol.2006;48:406–41211. Topp M, Uldall P, Greisen G. Cerebral palsy births in easternDenmark, 1987–90: implications for neonatal care. Paediatr Peri-nat Epidemiol. 2001;15:271–27712. Wu YW, Croen LA, Shah SJ, Newman TB, Najjar DV. Cere-bral palsy in a term population: risk factors and neuroimagingfindings. Pediatrics. 2006;118:690–69713. Drummond PM, Colver AF. Analysis by gestational age ofcerebral palsy in singleton births in north-east England 1970–94.Paediatr Perinat Epidemiol. 2002;16:172–18014. Sigurdardottir S, Thorkelsson T, Halldorsdottir M, Thora-rensen O, Vik T. Trends in prevalence and characteristics of cerebralpalsy among Icelandic children born 1990 to 2003. Dev Med ChildNeurol. 2009;51:356–363
15. Himmelmann K, Beckung E, Hagberg G, Uvebrant P. Grossand fine motor function and accompanying impairments in cerebralpalsy. Dev Med Child Neurol. 2006;48:417–42316. Burja S, Seme-Ciglenecki P, Gajsek-Marchetti M, HajdinjakD, Levanic A, Kodelic B. Epidemiological study of cerebral palsy inthe Maribor region. Wien Klin Wochenschr. 2004;116(suppl 2):39–4317. Moster D, Wilcox AJ, Vollset SE, Markestad T, Lie RT.Cerebral palsy among term and postterm births. JAMA. 2010;304:976–98218. Moster D, Lie RT, Markestad T. Long-term medical and socialconsequences of preterm birth. N Engl J Med. 2008;359:262–27319. Blair E. Epidemiology of the cerebral palsies. Orthop ClinNorth Am. 2010;41:441–45520. Glinianaia SV, Rankin J, Colver A. Cerebral palsy rates by birthweight, gestation and severity in North of England, 1991–2000singleton births. Arch Dis Child. 2011;96:180–18521. Surman G, Newdick H, Johnson A. Cerebral palsy rates amonglow-birthweight infants fell in the 1990s. Dev Med Child Neurol.2003;45:456–46222. Himmelmann K, Hagberg G, Beckung E, Hagberg B, Uve-brant P. The changing panorama of cerebral palsy in Sweden. IX.Prevalence and origin in the birth-year period 1995–1998. ActaPaediatr. 2005;94:287–29423. Vincer MJ, Allen AC, Joseph KS, Stinson DA, Scott H,Wood E. Increasing prevalence of cerebral palsy among very pre-term infants: a population-based study. Pediatrics. 2006;118:e1621–e162624. Robertson CM, Watt MJ, Yasui Y. Changes in the prevalenceof cerebral palsy for children born very prematurely within apopulation-based program over 30 years. JAMA. 2007;297:2733–274025. Platt MJ, Cans C, Johnson A, et al. Trends in cerebral palsyamong infants of very low birthweight (�1500 g) or born prema-turely (�32 weeks) in 16 European centres: a database study.Lancet. 2007;369:43–5026. Ashwal S, Russman BS, Blasco PA, et al. Practice parameter:diagnostic assessment of the child with cerebral palsy: report of theQuality Standards Subcommittee of the American Academy ofNeurology and the Practice Committee of the Child NeurologySociety. Neurology. 2004;62:851–86327. Korzeniewski SJ, Birbeck G, DeLano MC, Potchen MJ, Pan-eth N. A systematic review of neuroimaging for cerebral palsy.J Child Neurol. 2008;23:216–22728. Towsley K, Shevell MI, Dagenais L; Consortium REPACQ.Population-based study of neuroimaging findings in children withcerebral palsy. Eur J Paediatr Neurol. 2011;15:29–3529. Mathur AM, Neil JJ, Inder TE. Understanding brain injuryand neurodevelopmental disabilities in the preterm infant: theevolving role of advanced magnetic resonance imaging. SeminPerinatol. 2010;34:57–6630. De Vries LS, Groenendaal F, van Haastert IC, Eken P, Rade-maker KJ, Meiners LC. Asymmetrical myelination of the posteriorlimb of the internal capsule in infants with periventricular haemor-rhagic infarction: an early predictor of hemiplegia. Neuropediatr.1999;30:314–31931. Roelants-van Rijn AM, Groenendaal F, Beek FJ, Eken P,van Haastert IC, de Vries LS. Parenchymal brain injury in thepreterm infant: comparison of cranial ultrasound, MRI and neuro-developmental outcome. Neuropediatr. 2001;32:80–8932. Woodward LJ, Anderson PJ, Austin NC, Howard K, Inder TE.
American Board of Pediatrics Neonatal-PerinatalMedicine Content Specifications• Know the indications for and limitations of
various neuroimaging studies and be ableto recognize normal and abnormalstructures and changes during developmentand growth.
• Know the approximate risk of cerebral palsy in very low birthweight, moderately low birth weight, and normal birth weightinfants.
• Know the prenatal, perinatal, and neonatal risk factors for thedevelopment of cerebral palsy
neurology cerebral palsy
NeoReviews Vol.12 No.10 October 2011 e571 by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from

Neonatal MRI to predict neurodevelopmental outcomes in preterminfants. N Engl J Med. 2006;355:685–69433. Bax M, Tydeman C, Flodmark O. Clinical and MRI correlatesof cerebral palsy: the European Cerebral Palsy Study. JAMA. 2006;296:1602–160834. Feys H, Eyssen M, Jaspers E, et al. Relation between neurora-diological findings and upper limb function in hemiplegic cerebralpalsy. Eur J Paediatr Neurol. 2010;14:169–17735. Mirmiran M, Barnes PD, Keller K, et al. Neonatal brain mag-netic resonance imaging before discharge is better than serial cranialultrasound in predicting cerebral palsy in very low birth weightpreterm infants. Pediatrics. 2004;114:992–99836. Ancel PY, Livinec F, Larroque B, et al. Cerebral palsy amongvery preterm children in relation to gestational age and neonatalultrasound abnormalities: the EPIPAGE cohort study. Pediatrics.2006;117:828–83537. Accardo J, Kammann H. Hoon AH Jr. Neuroimaging incerebral palsy. J Pediatr. 2004;145(2 suppl):S19–S2738. Deng W, Pleasure J, Pleasure D. Progress in periventricularleukomalacia. Arch Neurol. 2008;65:1291–129539. Nagae LM, Hoon AH Jr, Stashinko E, et al. Diffusion tensorimaging in children with periventricular leukomalacia: variability ofinjuries to white matter tracts. AJNR Am J Neuroradiol. 2007;28:1213–122240. Kulak W, Sobaniec W, Goscik M, Olenski J, Okurowska-Zawada B. Clinical and neuroimaging profile of congenital brainmalformations in children with spastic cerebral palsy. Adv Med Sci.2008;53:42–4841. Lasry O, Shevell MI, Dagenais L. Cross-sectional comparisonof periventricular leukomalacia in preterm and term children. Neu-rology. 2010;74:1386–139142. Olsen P, Paakko E, Vainionpaa L, Pyhtinen J, Jarvelin MR.Magnetic resonance imaging of periventricular leukomalacia and itsclinical correlation in children. Ann Neurol. 1997;41:754–76143. Kuban KC, Allred EN, O’Shea TM, et al. Cranial ultrasoundlesions in the NICU predict cerebral palsy at age 2 years in childrenborn at extremely low gestational age. J Child Neurol. 2009;24:63–7244. De Vries LS, Van Haastert IL, Rademaker KJ, Koopman C,Groenendaal F. Ultrasound abnormalities preceding cerebral palsyin high-risk preterm infants. J Pediatr. 2004;144:815–82045. Ment LR, Vohr B, Allan W, et al. The etiology and outcome ofcerebral ventriculomegaly at term in very low birth weight preterminfants. Pediatrics. 1999;104:243–24846. Limperopoulos C, Bassan H, Gauvreau K, et al. Does cere-bellar injury in premature infants contribute to the high prevalenceof long-term cognitive, learning, and behavioral disability in sur-vivors? Pediatrics. 2007;120:584–59347. Limperopoulos C, Robertson RL, Sullivan NR, Bassan H, duPlessis AJ. Cerebellar injury in term infants: clinical characteristics,magnetic resonance imaging findings, and outcome. Pediatr Neu-rol. 2009;41:1–848. Messerschmidt A, Fuiko R, Prayer D, et al. Disrupted cere-bellar development in preterm infants is associated with im-paired neurodevelopmental outcome. Eur J Pediatr. 2008;167:1141–1147
49. Himpens E, Oostra A, Franki I, Van Maele G, VanhaesebrouckP, Van den Broeck C. Predictability of cerebral palsy and its char-acteristics through neonatal cranial ultrasound in a high-risk NICUpopulation. Eur J Pediatr. 2010;169:1213–121950. de Vries LS. Neurological assessment of the preterm infant.Acta Paediatr. 1996;85:765–77151. Patra K, Wilson-Costello D, Taylor HG, Mercuri-Minich N,Hack M. Grades I-II intraventricular hemorrhage in extremely lowbirth weight infants: effects on neurodevelopment. J Pediatr. 2006;149:169–17352. Inder TE, Anderson NJ, Spencer C, Wells S, Volpe JJ. Whitematter injury in the premature infant: a comparison between serialcranial sonographic and MR findings at term. AJNR Am J Neuro-radiol. 2003;24:805–80953. O’Shea TM, Counsell SJ, Bartels DB, Dammann O. Magneticresonance and ultrasound brain imaging in preterm infants. EarlyHum Dev. 2005;81:263–27154. Steggerda SJ, Leijser LM, Wiggers-de Bruine FT, van derGrond J, Walther FJ, van Wezel-Meijler G. Cerebellar injury inpreterm infants: incidence and findings on US and MR images.Radiology. 2009;252:190–19955. Black RE, Cousens S, Johnson HL, et al. Global, regional, andnational causes of child mortality in 2008: a systematic analysis.Lancet. 2010;375:1969–198756. Sciberras C, Spencer N. Cerebral palsy in Malta 1981 to 1990.Dev Med Child Neurol. 1999;41:508–51157. Singhi PD, Ray M, Suri G. Clinical spectrum of cerebral palsyin north India–an analysis of 1,000 cases. J Trop Pediatr. 2002;48:162–16658. Dagenais L, Hall N, Majnemer A, et al. Communicating adiagnosis of cerebral palsy: caregiver satisfaction and stress. PediatrNeurol. 2006;35:408–41459. Rosenbaum P. Classification of abnormal neurological out-come. Early Hum Dev. 2006;82:167–17160. Horsch S, Skiold B, Hallberg B, et al. Cranial ultrasound andMRI at term age in extremely preterm infants. Arch Dis Child FetalNeonatal Ed. 2009;95:F310–F31461. Brehaut JC, Kohen DE, Raina P, et al. The health of pri-mary caregivers of children with cerebral palsy: how does it comparewith that of other Canadian caregivers? Pediatrics. 2004;114:e182–e19162. Byrne MB, Hurley DA, Daly L, Cunningham CG. Healthstatus of caregivers of children with cerebral palsy. Child CareHealth Dev. 2010;36:696–70263. Huang YP, Kellett UM, St John W. Cerebral palsy: experiencesof mothers after learning their child’s diagnosis. J Adv Nurs. 2010;66:1213–122164. Himpens E, Oostra A, Franki I, Vansteelandt S, Vanhaeseb-rouck P, den Broeck CV. Predictability of cerebral palsy in ahigh-risk NICU population. Early Hum Dev. 2010;86:413–41765. Baird G, McConachie H, Scrutton D. Parents’ perceptions ofdisclosure of the diagnosis of cerebral palsy. Arch Dis Child. 2000;83:475–48066. Hasnat MJ, Graves P. Disclosure of developmental disability: astudy of parent satisfaction and the determinants of satisfaction.J Paediatr Child Health. 2000;36:32–35
neurology cerebral palsy
e572 NeoReviews Vol.12 No.10 October 2011
by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from

NeoReviews Quiz
1. The current definition of cerebral palsy (CP) was published in 2005 based on the conclusions of aninternational workshop of experts in the field of developmental disorders. Of the following, the mostaccurate statement regarding CP is that it:
A. Involves aberrations of movement and posture.B. Is a progressive neurodevelopmental disorder.C. Is viewed as a homogeneous disorder of a single cause.D. Originates during early childhood after infancy.E. Spares disturbances of sensation and behavior.
2. A 14-week-old infant, who weighed 610 g at birth at an estimated gestational age of 24 weeks, is beingdischarged from the neonatal intensive care unit. Scheduling for neurodevelopmental follow-up of theinfant is being arranged. The mother is concerned about possible CP and inquires about when such adiagnosis is usually made. Of the following, the definitive diagnosis of cerebral palsy is typically made afterthe corrected age of:
A. 6 months.B. 12 months.C. 18 months.D. 24 months.E. 36 months.
3. According to a population-based follow-up study using the Medical Birth Registry of Norway, theprevalence of CP among infants born at term is estimated at 1.15 per 1,000 births. The risk of CP in theseinfants varies, depending on the timing of birth within the term period. Of the following, the gestationalage at birth within the term period most associated with a reduced risk of CP is:
A. 37 weeks.B. 38 weeks.C. 39 weeks.D. 40 weeks.E. 41 weeks.
4. Abnormal neuroanatomic findings are seen on neuroimaging in 80% to 90% of children who have CP. Ofthe following, the most common neuroanatomic abnormality among such children involves the:
A. Basal ganglia.B. Commissural fibers.C. Limb of internal capsule.D. Periventricular white matter.E. Superior corona radiata.
neurology cerebral palsy
NeoReviews Vol.12 No.10 October 2011 e573 by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from

5. Cerebral palsy is categorized into phenotypic subtypes based on the distribution of limb involvement andtype of muscle tone abnormality. Of the following, the most common phenotype of CP among preterminfants is:
A. Ataxic hemiplegia.B. Athetoid monoplegia.C. Dyskinetic quadriparesis.D. Epileptiform dyskinesia.E. Spastic diplegia.
6. Early counseling of the parents of a neonate at high risk for CP may function as the starting point forparental adaptation to their infant’s lifelong condition and its associated morbidities. Of the following, themost frequent morbidity associated with CP is:
A. Dental caries.B. Epilepsy.C. Feeding problems.D. Speech impairment.E. Stunted growth.
neurology cerebral palsy
e574 NeoReviews Vol.12 No.10 October 2011
by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from

DOI: 10.1542/neo.12-10-e5642011;12;e564NeoReviews
Ryan M. McAdams and Sandra E. JuulCerebral Palsy: Prevalence, Predictability, and Parental Counseling
ServicesUpdated Information &
http://neoreviews.aappublications.org/content/12/10/e564including high resolution figures, can be found at:
References
-1http://neoreviews.aappublications.org/content/12/10/e564.full#ref-listThis article cites 65 articles, 14 of which you can access for free at:
Subspecialty Collections
y_subhttp://classic.neoreviews.aappublications.org/cgi/collection/neurologNeurologyc_disorders_subhttp://classic.neoreviews.aappublications.org/cgi/collection/neurologiNeurologic Disordersborn_infant_subhttp://classic.neoreviews.aappublications.org/cgi/collection/fetus:newFetus/Newborn Infantfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
https://shop.aap.org/licensing-permissions/in its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://classic.neoreviews.aappublications.org/content/reprintsInformation about ordering reprints can be found online:
by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from

Strip of the Month: November 2011Charlotte Clock, MD,*
Leonardo Pereira, MD,
MCR*
Author Disclosure
Drs Clock and Pereira
have disclosed no
financial relationships
relevant to this
article. This
commentary does not
contain a discussion
of an unapproved/
investigative use of a
commercial
product/device.
Electronic Fetal Monitoring Case Review SeriesElectronic fetal monitoring (EFM) is a popular technology used to establish fetal well-being. Despite its widespread use, terminology used to describe patterns seen on themonitor has not been consistent until recently. In 1997, the National Institute of ChildHealth and Human Development (NICHD) Research Planning Workshop publishedguidelines for interpretation of fetal tracings. This publication was the culmination of 2years of work by a panel of experts in the field of fetal monitoring and was endorsed in 2005by both the American College of Obstetricians and Gynecologists (ACOG) and theAssociation of Women’s Health, Obstetric and Neonatal Nurses (AWHONN). In 2008,ACOG, NICHD, and the Society for Maternal-Fetal Medicine reviewed and updated thedefinitions for fetal heart rate patterns, interpretation ,and research recommendations.Following is a summary of the terminology definitions and assumptions found in the 2008NICHD workshop report. Normal values for arterial umbilical cord gas values andindications of acidosis are defined in Table 1.
Assumptions from the NICHD Workshop
● Definitions are developed for visual interpretation, assuming that both the fetal heart rate(FHR) and uterine activity recordings are of adequate quality
● Definitions apply to tracings generated by internal or external monitoring devices● Periodic patterns are differentiated based on waveform, abrupt or gradual (eg, late
decelerations have a gradual onset and variable decelerations have an abrupt onset)● Long- and short-term variability are evaluated visually as a unit● Gestational age of the fetus is considered when evaluating patterns● Components of fetal heart rate FHR do not occur alone and generally evolve over time
DefinitionsBaseline Fetal Heart Rate
● Approximate mean FHR rounded to increments of 5 beats/min in a 10-minute segmentof tracing, excluding accelerations and decelerations, periods of marked variability, andsegments of baseline that differ by �25 beats/min
● In the 10-minute segment, the minimum baseline duration must be at least 2 minutes(not necessarily contiguous) or the baseline for that segment is indeterminate
● Bradycardia is a baseline of �110 beats/min; tachycardia is a baseline of�160 beats/min
● Sinusoidal baseline has a smooth sine wave-like undulating pattern, with waves havingregular frequency and amplitude
Baseline Variability
● Fluctuations in the baseline FHR of two cycles per minute or greater, fluctuations areirregular in amplitude and frequency, fluctuations are visually quantitated as the ampli-tude of the peak to trough in beats per minute
● Classification of variability:Absent: Amplitude range is undetectableMinimal: Amplitude range is greater than undetectable to 5 beats/minModerate: Amplitude range is 6 to 25 beats/minMarked: Amplitude range is �25 beats/min
*Assistant Professor, Division of Maternal-Fetal Medicine, Oregon Health and Sciences University, Portland, OR.
strip of the month
e668 NeoReviews Vol.12 No.10 October 2011

Accelerations
● Abrupt increase in FHR above the most recently deter-mined baseline
● Onset to peak of acceleration is �30 seconds, acme is�15 beats/min above the most recently determinedbaseline and lasts �15 seconds but �2 minutes
● Before 32 weeks’ gestation, accelerations are definedby an acme �10 beats/min above the most recentlydetermined baseline for �10 seconds
● Prolonged acceleration lasts �2 minutes but �10 min-utes
Late Decelerations
● Gradual decrease in FHR (onset to nadir �30 seconds)below the most recently determined baseline, withnadir occurring after the peak of uterine contractions
● Considered a periodic pattern because it occurs withuterine contractions
Early Decelerations
● Gradual decrease in FHR (onset to nadir �30 seconds)below the most recently determined baseline, withnadir occurring coincident with uterine contraction
● Also considered a periodic pattern
Variable Decelerations
● Abrupt decrease in FHR (onset to nadir �30 seconds)● Decrease is �15 beats/min below the most recently
determined baseline lasting �15 seconds but �2 min-utes
● May be episodic (occurs without a contraction) orperiodic
Prolonged Decelerations
● Decrease in the FHR �15 beats/min below the mostrecently determined baseline lasting �2 minutes but�10 minutes from onset to return to baseline
Decelerations are tentatively called recurrent if they oc-cur with �50% of uterine contractions in a 20-minuteperiod.
Decelerations occurring with �50% of uterine contrac-tions in a 20-minute segment are intermittent.
Sinusoidal Fetal Heart Rate Pattern
● Visually apparent, smooth sine wavelike undulatingpattern in the baseline with a cycle frequency of 3 to5/minute that persists for �20 minutes.
Uterine Contractions
● Quantified as the number of contractions in a 10-minute window, averaged over 30 minutes.
Normal: �5 contractions in 10 minutesTachysystole: �5 contractions in 10 minutes
InterpretationA three-tier Fetal Heart Rate Interpretation system hasbeen recommended as follows:
● Category I FHR tracings: Normal, strongly predictiveof normal fetal acid-base status and require routinecare. These tracings include all of the following:
�Baseline rate: 110 to 160 beats/min�Baseline FHR variability: Moderate�Late or variable decelerations: Absent�Early decelerations: Present or absent�Accelerations: Present or absent
● Category II FHR tracings: Indeterminate, require evalu-ation and continued surveillance and reevaluation. Exam-ples of these tracings include any of the following:
�Bradycardia not accompanied by absent variability�Tachycardia�Minimal or marked baseline variability�Absent variability without recurrent decelerations�Absence of induced accelerations after fetal stimula-
tion�Recurrent variable decelerations with minimal or
Table 1. Arterial Umbilical Cord Gas ValuespH PCO2 (mm Hg) PO2 (mm Hg) Base Excess
Normal* >7.20 <60 >20 <�10(7.15 to 7.38) (35 to 70) (�2.0 to �9.0)
Respiratory Acidosis <7.20 >60 Variable <�10Metabolic Acidosis <7.20 <60 Variable >�10Mixed Acidosis <7.20 >60 Variable >�10
*Normal ranges from Obstet Gynecol Clin North Am. 1999;26:695.
strip of the month
NeoReviews Vol.12 No.10 October 2011 e669

moderate variability�Prolonged decelerations�Recurrent late decelerations with moderate variability�Variable decelerations with other characteristics,
such as slow return to baseline
● Category III FHR tracings: Abnormal, predictive ofabnormal fetal acid-base status and require promptintervention. These tracings include:
�Absent variability with any of the following:y Recurrent late decelerationsy Recurrent variable decelerationsy Bradycardia
�Sinusoidal pattern
Data from Macones GA, Hankins GDV, Spong CY,Hauth J, Moore T. The 2008 National Institute of ChildHealth and Human Development workshop report onelectronic fetal monitoring. Obstet Gynecocol. 2008;112:661–666 and American College of Obstetricians andGynecologists. Intrapartum fetal heart rate monitoring:nomenclature, interpretation, and general managementprinciples. ACOG Practice Bulletin No. 106. Washing-ton, DC: American College of Obstetricians and Gyne-cologists; 2009.
We encourage readers to examine each strip in thecase presentation and make a personal interpretation ofthe findings before advancing to the expert interpreta-tion provided.
strip of the month
e670 NeoReviews Vol.12 No.10 October 2011

Case PresentationHistory
A 38-year-old G2P1001 at 37 6/7 weeks gestationpresents to labor and delivery from clinic after she hadtwo elevated blood pressures greater than 140/90 andtrace proteinuria. She also has a headache and new onsetupper extremity swelling. She denies any visual changesor right upper quadrant pain. She has irregular uterinecontractions and active fetal movement. She denies leak-ing of fluid or vaginal bleeding. Her pregnancy is com-plicated by advanced maternal age. She declined geneticscreening. Her prenatal laboratory tests are all normal.
Case ProgressionOn physical examination, her blood pressure is 140/103 mm Hg and she has a urine dipstick of 1�(30 mg/dL) of protein. She meets the criteria for severe pre-eclampsia based on her headache. (1) Her cervix is 30%effaced, 1 cm dilated, and negative 3 station. Alllaboratory values were normal, except for a slightlyincreased AST of 45 U/L. A decision is made toproceed with induction of labor secondary to severepreeclampsia. A fetal heart tracing is obtained onadmission (Fig. 1).
Figure 1. EFM strip #1.
strip of the month
NeoReviews Vol.12 No.10 October 2011 e671

Findings from electronic fetal monitoring (EFM)strip #1 are:
● Variability: Moderate● Baseline rate: 135 beats/min● Episodic Pattern: Acceleration● Periodic Pattern: None● Uterine Contractions: Every 5 minutes● Interpretation: Category I tracing● Differential Diagnosis: Normal fetal tracing.
● Action: No intervention required. The patient is ad-mitted for induction of labor.
A Foley balloon was placed for cervical ripening. Fourhours later, the balloon is expelled and she is found to be50%/5 cm/�2. She is started on pitocin, and 1 hourlater she received an epidural for pain control. She isexamined 8 hours later and is found to be 60%/6 cm/�1. She undergoes artificial rupture of membranesand has light meconium. The fetal tracing is shown inFigure 2.
Figure 2. EFM strip #2.
Figure 1. EFM strip #1
strip of the month
e672 NeoReviews Vol.12 No.10 October 2011

Findings from EFM Strip #2 are:
● Variability: Moderate● Baseline rate: 120 beats/min● Episodic Pattern: None● Periodic Pattern: None observed● Uterine Contractions: Every 3 minutes● Interpretation: Category I Tracing● Differential Diagnosis: Normal fetal tracing. The ma-
ternal pulse oximeter demonstrates that the maternal
heart rate also occasionally is 120 beats/min. It isimportant to distinguish the maternal and fetal heartrates.
● Action: Overall, the tracing is reassuring due to mod-erate variability. Induction of labor can continue.
The pitocin is continued and 4 hours later she remains6 cm dilated. An intrauterine pressure catheter is placedto assess the uterine contractions. The fetal tracing isshown in Figure 3.
Figure 3. EFM strip #3.
Figure 2. EFM strip #2.
strip of the month
NeoReviews Vol.12 No.10 October 2011 e673

Findings from EFM Strip #3 are:
● Variability: Moderate● Baseline Rate: 120 beats/min● Episodic Pattern: Accelerations● Periodic Pattern: None● Uterine Contractions: Occurring every 3 minutes, last-
ing 50 seconds● Interpretation: Category I tracing● Differential Diagnosis: Normal tracing, with evidence
of fetal well-being indicated by moderate variabilityand accelerations. The patient may not be progressingdue to inadequate uterine contractions. With theplacement of the intrauterine pressure catheter, theuterine power can be documented.
● Action: No intervention required.
Three hours later, the patient is re-evaluated. No cervicalexam is performed. The fetal heart tracing is shownbelow (Fig. 4).
Figure 4. EFM strip #4.
Figure 3. EFM strip #3.
strip of the month
e674 NeoReviews Vol.12 No.10 October 2011

Findings from EFM Strip #4 are:
● Variability: Moderate● Baseline rate: 125 beats/min● Episodic Pattern: Accelerations● Periodic Pattern: None● Uterine Contractions: Occurring every 2 minutes● Interpretation: Category I tracing
● Differential Diagnosis: Normal tracing, with evidenceof fetal well-being indicated by moderate variabilityand accelerations.
● Action: No intervention required.
Ninety minutes later, the patient has increasing pain withcontractions. Her cervical examination is 90%/9/0. An-other fetal heart tracing is shown below (Fig. 5).
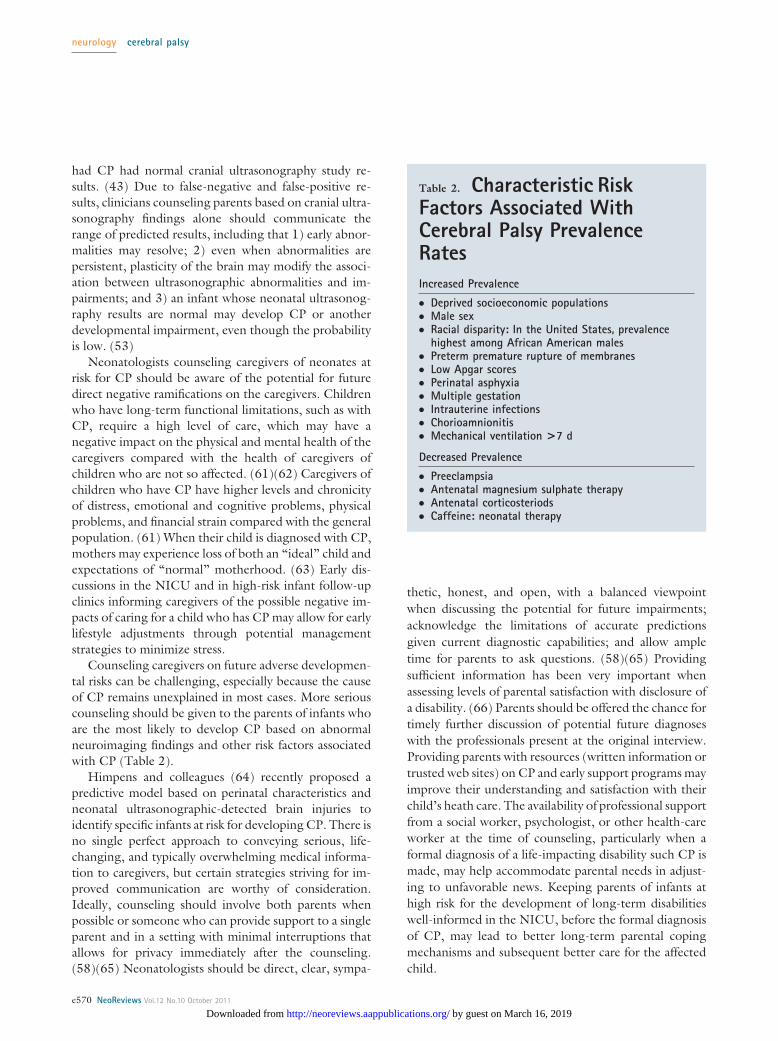
Figure 5. EFM strip #5.
Figure 4. EFM strip #4.
strip of the month
NeoReviews Vol.12 No.10 October 2011 e675
Findings from EFM Strip #5 are:
● Variability: MinimalBaseline rate: 150 beats/min● Episodic Pattern: None● Periodic Pattern: Recurrent variable decelerations● Uterine Contractions: Occurring every 3–4 minutes● Interpretation: Category II● Differential Diagnosis: The differential diagnosis in-
cludes umbilical cord compression, uteroplacental un-
derperfusion or uteroplacental dysfunction. Variabledecelerations are normally well tolerated, however ifthey continue to be repetitive or more severe, acidemiacan develop.
● Action: The fetal status should be monitored closely.
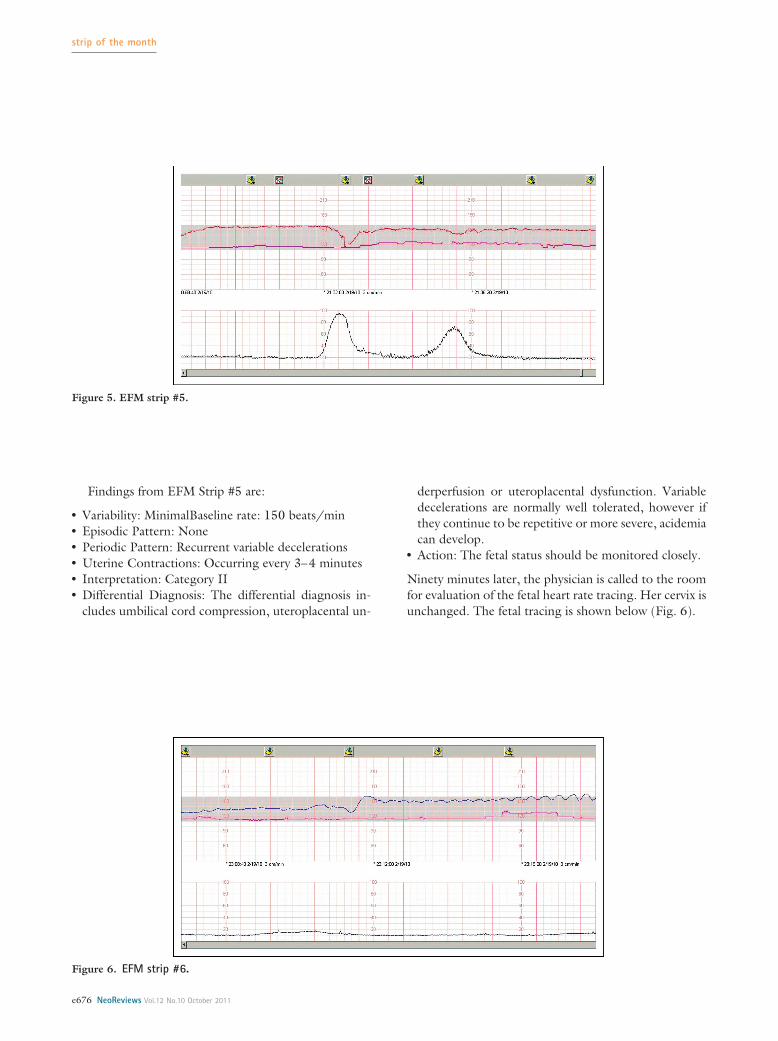
Ninety minutes later, the physician is called to the roomfor evaluation of the fetal heart rate tracing. Her cervix isunchanged. The fetal tracing is shown below (Fig. 6).
Figure 6. EFM strip #6.
Figure 5. EFM strip #5.
strip of the month
e676 NeoReviews Vol.12 No.10 October 2011

Findings from EFM Strip #6 are:
● Variability: Minimal/moderate● Baseline Rate: 140 rising to 150 beats/min● Episodic Pattern: None● Periodic Pattern: Variable deceleration and possible
sinusoidal pattern● Uterine Contractions: None documented● Interpretation: Category III● Differential Diagnosis: Sinusoidal patterns can be asso-
ciated with fetal anemia, use of certain drugs, fetalasphyxia/hypoxia, fetal infection, fetal cardiac anoma-lies, and fetal sleep cycles. This patient had not receivedany new medications.
● Action: Due to the concerning fetal heart tracing,immediate delivery is indicated.
Decision is made to proceed with cesarean delivery dueto the sinusoidal heart rate pattern. The fetal heart ratetracing in the operating room is shown below (Fig. 7).
Figure 7. EFM strip #7.
Figure 6. EFM strip #6.
strip of the month
NeoReviews Vol.12 No.10 October 2011 e677

Findings from EFM Strip #7 are:
● Variability: Absent● Baseline Rate: 160 beats/min● Episodic Pattern: Sinusoidal heart rate pattern● Periodic Pattern: None● Uterine Contractions: None documented● Interpretation: Category III● Differential Diagnosis: Unchanged● Action: Unchanged
The patient’s epidural was not adequate after a boluswas infused; therefore, she received general anesthesia.Twenty-eight minutes from the decision for cesarean,the baby is delivered. There is an abruption notedupon entry into the uterine cavity. The patient isadmitted to the intensive care unit secondary to thegeneral anesthesia and abruption. Her internationalnormalized ratio (INR) is elevated at 1.36; however,she recovers and is transferred to the mother–babyunit on postoperative day 1.
OutcomeA viable male infant is delivered by cesarean section. Heweighs 2,880 g (6 lb; 5.6 oz) and has Apgar scores of 1 at1 minute, 3 at 5 minutes, 5 at 10 minutes, and 7 at15 minutes. The blood gas is shown below. This isconsistent with a mixed acidosis. A large blood clot iscleared from his throat, and bloody mucus is suctionedfrom his throat following intubation. He receives posi-tive pressure ventilation (PPV) and chest compressionsand responds appropriately. He is placed on continuouspositive airway pressure for 30 minutes and then isweaned to room air. His hemoglobin is 19.1 g/dL,which is normal. He is observed in the neonatal intensivecare unit for 48 hours and then transferred to the pa-tient’s room on day 2 after birth and is discharged homeon day 4.
Placental abruption is the premature separation of theplacenta before delivery, which occurs in approximately 1in 100 deliveries. It is a known complication of severepreeclampsia. (2) It is a clinical diagnosis usually consist-ing of vaginal bleeding, abdominal pain, increased uter-
Table 2. Arterial Umbilical Cord Gas ValuespH PCO2 (mm Hg) PO2 (mm Hg) Base Excess
Normal* >7.20 <60 >20 <�10(7.15 to 7.38) (35 to 70) (�2.0 to �9.0)
Respiratory Acidosis <7.20 >60 Variable <�10Metabolic Acidosis <7.20 <60 Variable >�10Mixed Acidosis <7.20 >60 Variable >�10Patient 7.05 67 <10 �15.0
*Normal ranges from Obstet Gynecol Clin North Am. 1999;26:695.
Figure 7. EFM strip #7.
strip of the month
e678 NeoReviews Vol.12 No.10 October 2011

ine tone, tachysystole, and a nonreassuring fetal heartrate tracing. In 10% to 20% of abruptions, there may beno vaginal bleeding. (3) The nonreassuring fetal heartrate tracing can consist of late decelerations, minimalvariability, fetal tachycardia, or, as in our patient, a sinu-soidal pattern. A sinusoidal heart rate pattern by defini-tion is a visually apparent, smooth sine wavelike undulat-ing pattern in the baseline with a cycle frequency of 3 to5 minutes that persists for �20 minutes. This pattern hasbeen seen with fetal anemia, use of certain drugs, fetalasphyxia/hypoxia, fetal infection, fetal cardiac anoma-lies, and fetal sleep cycles. (4) A true sinusoidal pattern
can be an ominous sign of fetal jeopardy and promptintervention is required.
References1. ACOG Committee on Practice Bulletins—Obstetrics. ACOG
practice bulletin. Diagnosis and management of preeclampsiaand eclampsia. Obstet Gynecol. 2002;99:159–167
2. Kramer MS, Usher RH, Pollack R, et al. Etiologic determi-nants of abruptio placentae. Obstet Gynecol. 1997; 89:221–226
3. Oyelese Y, Ananth CV. Placental abruption. Obstet Gynecol.2006; 108:1005–1016
4. Modanlou HD, Murata Y. Sinusoidal heart rate pattern: reap-praisal of its definition and clinical significance. J Obstet Gynae-col Res. 2004;30:169–180
CorrectionIn the article entitled “Cerebral Palsy: Prevalence, Predictability, and Parental Counseling”in the October issue (NeoReviews 2011;12:e564–e574), at the bottom of page e565, thetext incorrectly states: “The bilateral spastic form increased from 0.58 (95% confidenceinterval [CI], 0.41 to 0.80) in 1980 to 0.33 (CI, 0.22 to 0.46) in 1998 . . .” This sentenceshould read “The bilateral spastic form decreased from 0.58 to 0.33 . . .”. The journalregrets the error.
strip of the month
NeoReviews Vol.12 No.10 October 2011 e679

DOI: 10.1542/neo.12-10-e5642011;12;e564NeoReviews
Ryan M. McAdams and Sandra E. JuulCerebral Palsy: Prevalence, Predictability, and Parental Counseling
http://neoreviews.aappublications.org/content/12/10/e564located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://neoreviews.aappublications.org//content/12/11/e679.full.pdf An erratum has been published regarding this article. Please see the attached page for:
Online ISSN: 1526-9906. Illinois, 60007. Copyright © 2011 by the American Academy of Pediatrics. All rights reserved. by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village,it has been published continuously since 2000. Neoreviews is owned, published, and trademarked Neoreviews is the official journal of the American Academy of Pediatrics. A monthly publication,
by guest on March 16, 2019http://neoreviews.aappublications.org/Downloaded from