characteristics of unplanned hospital admissions due to drug-related problems in cancer patients
TRANSCRIPT

ORIGINAL ARTICLE
Characteristics of unplanned hospital admissions dueto drug-related problems in cancer patients
Alexandre Chan & Deren Soh & Yu Ko & Yu-Chu Huang &
Joen Chiang
Received: 11 September 2013 /Accepted: 3 February 2014# Springer-Verlag Berlin Heidelberg 2014
AbstractBackground Studies have examined drug-related problems(DRPs) that have led to hospital admissions in the generalpopulation. However, there is a lack of information on thecharacteristics of DRPs in the cancer population.Objective The objective of this study was to investigate thetype, causality, severity, and preventability of DRPs that resultin unplanned hospitalizations among cancer patients.Methods This was a prospective, cohort study conducted intwo oncology wards between July and December 2012. Allpatients who were diagnosed with solid tumor or lymphomaand required unplanned hospitalization were included. Theincidence of DRPs among hospital admissions was captured,and the nature of the DRPs (causality, severity, and prevent-ability) was characterized.Results There were 1,299 admissions and 1,275 were eligiblefor analysis. Among the 1,275 eligible admissions, 158(12.4 %) were considered to be associated with a DRP. Inthe 158 admissions associated with DRPs, 164 DRPs werefound. The majority of the DRP-related admissions wereadverse drug reactions (ADRs) (n=155/164, 94.5 %), proba-ble (n=98, 59.8 %), moderately severe (n=155, 94.5 %), andprobably or definitely preventable (n=86, 52.4 %). Mostpatients with DRPs recovered and were discharged. Febrileneutropenia was the most common adverse drug reaction, anddrug combinations involving antihypertensives and long-term
corticosteroids raised the risks for potential drug-drug interac-tions among patients with cancer.Conclusion The incidence of DRP-induced unplanned hospi-tal admissions was 12.4 % among cancer patients. Approxi-mately half of these were preventable events.
Keywords Drug-related problems . Hospital . Drug-druginteractions . Oncology
Introduction
According to the Pharmaceutical Care Network Europe(PCNE), a drug-related problem (DRP) is defined as an eventor a circumstance involving drug therapy that actually orpotentially interferes with desired health outcomes [1]. Pa-tients with cancer are vulnerable to DRPs because chemother-apeutic drugs possess narrow therapeutic indices and are oftencytotoxic to healthy cells at therapeutic doses [2]. In additionto chemotherapy and supportive care medications to preventside effects or manage symptoms, many patients manifestcomorbidities that may require additional medications, whichmay further increase the risk of manifesting adverse effects.
Previous studies have shown that patients with cancer oftenexperience hospitalizations due to the manifestations of DRPsduring their cancer treatment [3, 4]. In one study, the numberof adverse drug reactions (ADRs) experienced by patientsadmitted into a cancer center was high, with an average of2.7 ADRs per admission [5]. In another study, an evaluation ofunplanned hospital admissions discovered that 13 % of suchadmissions were associated with an ADR, the most commonof which was febrile neutropenia [3]. ADRs can be potentiallyfatal and are a leading cause of death [6]. Another commonlyobserved DRP among cancer patients is drug-drug interac-tions (DDIs). Cancer patients are at particular risk for DDIs asthey receive numerous medications for their cancer and other
A. Chan (*) :D. Soh :Y. Ko :Y.<C. HuangDepartment of Pharmacy, Faculty of Science, National University ofSingapore, Block S4, 18 Science Drive 4, 117543 Singapore,Singaporee-mail: [email protected]
A. Chan : J. ChiangDepartment of Pharmacy, National Cancer Center Singapore,Singapore, Singapore
Support Care CancerDOI 10.1007/s00520-014-2160-0

comorbidities, together with supportive care medications suchas antiemetics, analgesics, anti-infective agents, and growthfactors [7]. One study revealed that 27% of ambulatory cancerpatients had potential DDIs, with most involving anticoagu-lants and antihypertensives [8]. Furthermore, we have previ-ously identified potential DDI coprescriptions in 5.4 % ofpatients receiving oral anticancer agents [9].
There is a scarcity of published information on the preva-lence of ADR-related hospitalizations among cancer patients.The majority of previously published studies have focused onpatients who were not diagnosed with cancer. In the literature,there is also a lack of epidemiological data investigating theDRP-associated hospitalizations among Asian patients withcancer. Hence, the primary objective of this study was toinvestigate the type, causality, severity, and preventability ofthe DRPs that led to hospitalizations among cancer patients.This study aimed to evaluate the patterns of DRPs in cancerpatients to prevent DRP-related hospitalizations. Knowing thetype and characteristics of the DRPs patients commonly facewould allow health policy makers to design appropriate man-agement pathways for this group of patients.
Methods
Study design
This was a prospective, observational study of cancer patientsadmitted to two oncology wards at Singapore General Hospi-tal between July and December 2012. The hospital isSingapore’s largest tertiary acute hospital and serves over amillion people annually. This study was reviewed and ap-proved by the local institutional review board. The patients’informed consent was not required in this study.
Patients
All patients who were diagnosed with solid tumor or lympho-ma and required unplanned hospitalization were included inthis study. Patients under the age of 21 and those receivingtreatment within a clinical trial were excluded.
Data collection
All patient information was recorded using a data collectionform designed for this study. Data were collected from pa-tients’ medical and pharmacy records. During the initialscreening process, the medical records of all of the patientswere examined to determine whether their admission wasassociated with a DRP. Data such as medications used beforeadmission, current chemotherapy regimen, and pertinent labresults were collected. Among the admissions that were clas-sified as non-DRP related, only the patients’ demographics,
cancer diagnoses, and comorbid illness data were collected(Fig. 1). Using this set of collated data, the DRPs that contrib-uted to hospitalizations were classified by their type, causality,severity, and preventability.
Description of DRPs
Several descriptions were used to characterize the DRPs inthis study, including their identification, causality, severity,and preventability.
Identification of DRPs All DRP admissions were classifiedinto six different types in accordance with the PCNE DRPclassification V5.01 [1]. Micromedex® 2.0 DRUG-REAX®was used as a reference to identify all of the DRPs [10].
Causality of DRPs The Naranjo algorithm was used to esti-mate the causality of DRP types I, II, and III (i.e., adversereactions, interactions, and drug choice problems) [11]. Anoth-er causality classification by Hallas et al. was used to estimatethe causality of DRP types IV, V, and VI (i.e., dosing problems,drug use problems, and other problems) [12]. DRP causality
Fig. 1 Study procedure
Support Care Cancer

was ranked as definite, probable, possible, or doubtful. OnlyDRPs that fell under the definite, probable, or possible catego-ries were considered to be DRPs and included in the analysis.Doubtful drug-related admissions were excluded.
Severity of DRPs A classification scheme developed byMcDonnell and Jacobs to assess the level of severity was usedfor all of the DRPs [13]. DRP severity was ranked fromminoror moderate to severe.
Preventability of DRPs Preventability was determined using aseries of modified questions from the criteria of Schumockand Thornton [5]. DRP preventability was ranked as definitelypreventable, probably preventable, or not preventable.
Statistical considerations
Descriptive statistics were used to summarize the patientdemographic data. The number and percentages of differentDRP characteristics were tabled for analyses. Independentsample t test was used to determine whether there were anydifferences between the ages of patients with and withoutDRPs. Chi-square test was used to determine whether therewere any differences in the genders of patients with andwithout DRPs. Statistically significant results are those withp values <0.05. All of the statistical analyses were performedusing SPSS version 19 (SPSS Inc., Chicago, IL).
Results
Demographics
A total of 1,299 admissions (1,275 deemed eligible for anal-ysis) were processed between July and December 2012.Twenty-five admissions were excluded. Specifically, 11 pa-tients were below 21 years old, 13 patients were participatingin clinical trials, and the cause of admission was unclear for 1patient. Nine hundred and fifty-nine patients were admitted,217 of whom had repeated admissions that were included inthe total admissions (Table 1). The mean age was 61.3 years(standard deviation=12.8), and 527 of the patients (55.0 %)were male. The most common cancer type was gastrointesti-nal cancer (25.5 %). Sixty percent of all of the patients (n=573) manifested at least one comorbidity, and the most com-mon comorbidity was hypertension (n=379, 39.5 %).
Patients with DRPs were significantly younger (58.1 vs.61.7 years, p=0.03) than those without DRPs. A significantlyhigher proportion of patients with DRPs were female (54.3 %,p=0.015) compared to patients without DRPs. This correlateswith the higher proportion (28.3 %) of breast cancer incidencein patients with DRPs, as compared to a 10.9 % breast cancerincidence in patients without DRPs.
Among all 1,275 admissions, 158 (12.4 %) were consid-ered to be associated with a DRP. For admissions that were notassociated with a DRP, the most common cause of admissionwas disease progression (n=431, 33.8 %) where the patientexperienced symptoms that were due to tumor growth ormetastasis. Other causes of hospitalizations included electiveadmissions for chemotherapy (n=171, 13.4 %) and treatmentof infections (n=145, 11.4 %) (Table 2).
Identification and causality of DRPs
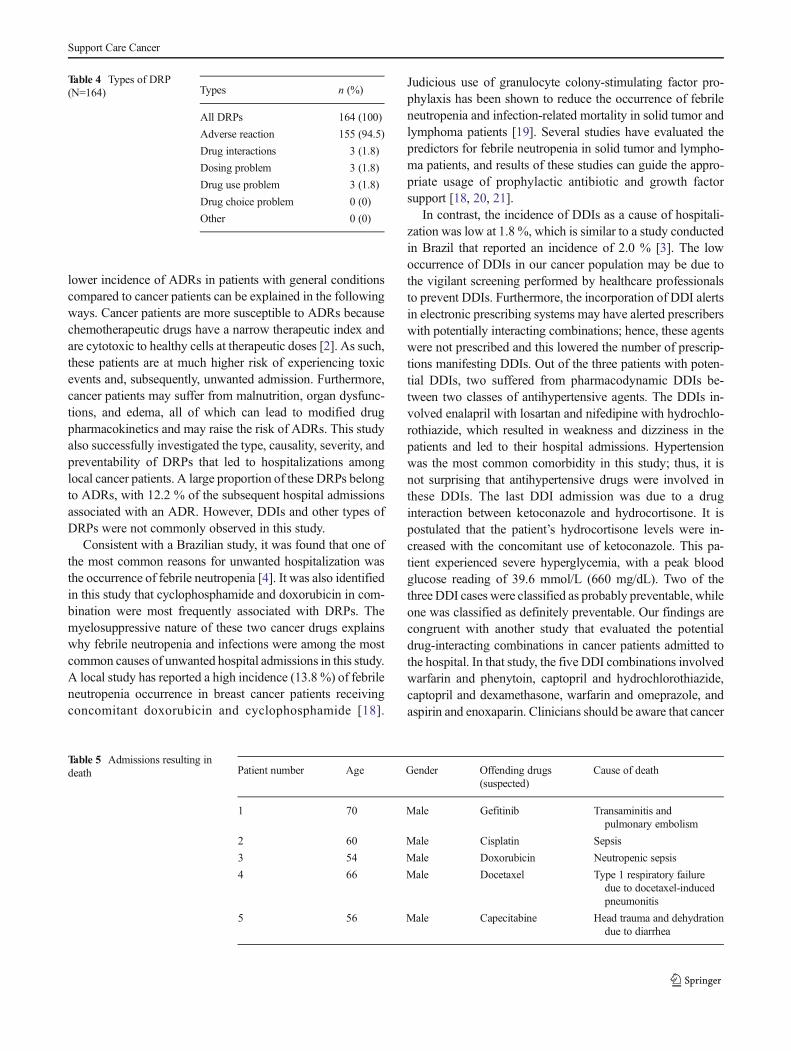
Among the 158 admissions associated with DRPs, 164 DRPswere identified. The analysis results on the causality of all 164DRPs suggested that the majority of the DRPs were probablein nature (n=98, 59.8 %) (Table 3). There were six patientswho had more than one DRP during an admission: twoadmissions were associated with two different ADRs, threeadmissions were associated with both ADR and DDI, and oneadmission was associated with an ADR and a drug overdose.The different DRP types are summarized in Table 4. DDIincidence was found to be low (n=3, 1.8 %). The majorityof the DRP-related admissions were due to ADRs (n=155,94.5 %), while the other types of DRPs were uncommon.Overall, 12.2% (155/1,275) of the admissions were associatedwith ADRs. Among all 164 DRPs, some patients experiencedmultiple symptoms that led to hospitalization. The most com-mon causes of admission were infections (n=42),gastrointestinal-related ADRs (nausea, vomiting, and diar-rhea) (n=38), and neutropenic fever (n=32).
Two hundred and sixty-two drugs were associated with the164 DRPs found. The cytotoxic agents most commonly asso-ciated with DRPs included cyclophosphamide (n=35), doxo-rubicin (n=25), cisplatin (n=25), docetaxel (n=18), and pac-litaxel (n=16).
Severity of DRPs
In terms of the severity, the majority of the DRPs wereclassified as moderately severe (n=155, 94.5 %). Of the sevensevere DRPs, four were found in five patients who died as aresult. The remaining patient experienced a moderately severeDRP. The reasons for mortality in those five patients aresummarized in Table 5. All of them were male and weretaking different drugs. All of the suspected offending drugsinvolved antineoplastic agents. Patient 5’s DRP was classifiedas moderately severe. The other four patients’ DRPs wereclassified as severe.
Preventability of DRPs
Regarding the preventability, 86 DRPs (52.4 %) were catego-rized as probably preventable or definitely preventable innature (Table 3), with majority of them being classified as
Support Care Cancer

probably preventable. Seventy-five admissions (45.7 %) werenot preventable. There were three patients who had receivedtheir chemotherapy in other institutions before being referredto our institution for admission. This resulted in a lack ofpatient information to assess DRP preventability levels, andtherefore, these three admissions were not categorized.
Discussion
Information regarding the frequency of ADRs as causes ofhospitalizations in oncology is scarce. However, ADR-
associated hospitalizations in patients with general conditionshave been examined in several reports. Several studies con-ducted in developed countries such as the UK, Spain, andAustralia have reported that the incidence of ADR-associatedhospitalizations ranges from 1.7 to 6.9 % [14–17], which islower than the incidence of 12.2% identified in this study. The
Table 1 Patient characteristics(N=959)
a Patientsmay havemore than onecomorbid illness
N (%)
Characteristics Patients with DRPs Patients without DRPs All patients
All admissions 127 (100) 832 (100) 959 (100)
Mean age, standard deviation 58.1, 12.7 61.7, 12.8 61.3, 12.8
Gender
Male 58 (45.7) 469 (56.4) 527 (55.0)
Female 69 (54.3) 363 (43.6) 432 (45.0)
Cancer type
Gastrointestinal 19 (15.1) 226 (27.2) 245 (25.5)
Lung 19 (15.1) 154 (18.5) 173 (18.0)
Breast 36 (28.3) 91 (10.9) 127 (13.2)
Lymphoma 15 (11.9) 90 (10.8) 105 (10.9)
Genitourinary 9 (7.1) 57 (6.9) 66 (6.9)
Gynecologic 7 (5.5) 38 (4.6) 45 (4.7)
Other 22 (17.3) 176 (21.2) 198 (20.6)
Metastatic disease 50 (39.4) 410 (49.3) 460 (48.0)
Comorbid illnessa
Yes 79 (62.2) 494 (59.4) 573 (59.7)
Hypertension 43 (33.9) 336 (40.4) 379 (39.5)
Dyslipidemia 38 (29.9) 227 (27.3) 263 (27.4)
Diabetes mellitus 24 (18.9) 153 (18.4) 177 (18.5)
Liver disease 8 (6.3) 29 (3.5) 37 (3.9)
Renal disease 4 (3.1) 29 (3.5) 33 (3.4)
Table 2 Causes ofadmissions (N=1,275) Causes n (%)
All admissions 1,275 (100)
DRP 158 (12.4)
Unclear 1 (0.1)
Non-DRP
Disease progression 431 (33.8)
Others 239 (18.7)
Chemotherapy 171 (13.4)
Infection 145 (11.4)
Examination 94 (7.4)
Other treatment 31 (2.4)
Accident 5 (0.4)
Table 3 Characteristics of DRP (N=164)
DRP characteristics Frequency % (n)
Causality
Probable 59.8 (98)
Possible 39.0 (64)
Definite 1.2 (2)
Doubtful 0 (0)
Severity
Moderate 94.5 (155)
Severe 4.3 (7)
Minor 1.2 (2)
Preventability
Not preventable 45.7 (75)
Probably preventable 37.2 (61)
Definitely preventable 15.2 (25)
Not applicablea 1.8 (3)
a Unable to assess preventability due to lack of patient information
Support Care Cancer
lower incidence of ADRs in patients with general conditionscompared to cancer patients can be explained in the followingways. Cancer patients are more susceptible to ADRs becausechemotherapeutic drugs have a narrow therapeutic index andare cytotoxic to healthy cells at therapeutic doses [2]. As such,these patients are at much higher risk of experiencing toxicevents and, subsequently, unwanted admission. Furthermore,cancer patients may suffer from malnutrition, organ dysfunc-tions, and edema, all of which can lead to modified drugpharmacokinetics and may raise the risk of ADRs. This studyalso successfully investigated the type, causality, severity, andpreventability of DRPs that led to hospitalizations amonglocal cancer patients. A large proportion of these DRPs belongto ADRs, with 12.2 % of the subsequent hospital admissionsassociated with an ADR. However, DDIs and other types ofDRPs were not commonly observed in this study.
Consistent with a Brazilian study, it was found that one ofthe most common reasons for unwanted hospitalization wasthe occurrence of febrile neutropenia [4]. It was also identifiedin this study that cyclophosphamide and doxorubicin in com-bination were most frequently associated with DRPs. Themyelosuppressive nature of these two cancer drugs explainswhy febrile neutropenia and infections were among the mostcommon causes of unwanted hospital admissions in this study.A local study has reported a high incidence (13.8 %) of febrileneutropenia occurrence in breast cancer patients receivingconcomitant doxorubicin and cyclophosphamide [18].
Judicious use of granulocyte colony-stimulating factor pro-phylaxis has been shown to reduce the occurrence of febrileneutropenia and infection-related mortality in solid tumor andlymphoma patients [19]. Several studies have evaluated thepredictors for febrile neutropenia in solid tumor and lympho-ma patients, and results of these studies can guide the appro-priate usage of prophylactic antibiotic and growth factorsupport [18, 20, 21].
In contrast, the incidence of DDIs as a cause of hospitali-zation was low at 1.8 %, which is similar to a study conductedin Brazil that reported an incidence of 2.0 % [3]. The lowoccurrence of DDIs in our cancer population may be due tothe vigilant screening performed by healthcare professionalsto prevent DDIs. Furthermore, the incorporation of DDI alertsin electronic prescribing systems may have alerted prescriberswith potentially interacting combinations; hence, these agentswere not prescribed and this lowered the number of prescrip-tions manifesting DDIs. Out of the three patients with poten-tial DDIs, two suffered from pharmacodynamic DDIs be-tween two classes of antihypertensive agents. The DDIs in-volved enalapril with losartan and nifedipine with hydrochlo-rothiazide, which resulted in weakness and dizziness in thepatients and led to their hospital admissions. Hypertensionwas the most common comorbidity in this study; thus, it isnot surprising that antihypertensive drugs were involved inthese DDIs. The last DDI admission was due to a druginteraction between ketoconazole and hydrocortisone. It ispostulated that the patient’s hydrocortisone levels were in-creased with the concomitant use of ketoconazole. This pa-tient experienced severe hyperglycemia, with a peak bloodglucose reading of 39.6 mmol/L (660 mg/dL). Two of thethree DDI cases were classified as probably preventable, whileone was classified as definitely preventable. Our findings arecongruent with another study that evaluated the potentialdrug-interacting combinations in cancer patients admitted tothe hospital. In that study, the five DDI combinations involvedwarfarin and phenytoin, captopril and hydrochlorothiazide,captopril and dexamethasone, warfarin and omeprazole, andaspirin and enoxaparin. Clinicians should be aware that cancer
Table 4 Types of DRP(N=164) Types n (%)
All DRPs 164 (100)
Adverse reaction 155 (94.5)
Drug interactions 3 (1.8)
Dosing problem 3 (1.8)
Drug use problem 3 (1.8)
Drug choice problem 0 (0)
Other 0 (0)
Table 5 Admissions resulting indeath Patient number Age Gender Offending drugs
(suspected)Cause of death
1 70 Male Gefitinib Transaminitis andpulmonary embolism
2 60 Male Cisplatin Sepsis
3 54 Male Doxorubicin Neutropenic sepsis
4 66 Male Docetaxel Type 1 respiratory failuredue to docetaxel-inducedpneumonitis
5 56 Male Capecitabine Head trauma and dehydrationdue to diarrhea
Support Care Cancer

patients who are long-term users of corticosteroids and anti-hypertensives are at higher risk for potential DDIs that maylead to unwanted admissions.
It is essential to note that over half of the DRPs wereconsidered to be preventable, and more steps could be takento avoid such potentially fatal consequences and ensure drugsafety in cancer patients. There are several ways to preventDRPs from occurring that minimize the risk of hospitalizationamong cancer patients. Physicians play a pivotal role byreducing unnecessary prescriptions and understanding theissues associated with DRPs and polypharmacy. Medicationreview and reconciliation conducted by pharmacists and theprevention of polypharmacy can lower the risks of a DRP. Achallenge to preventing DRPs from occurring is patient com-pliance. More can be done to enhance compliance by chang-ing drug administration frequency for patients’ conveniencewithout compromising clinical outcomes. Another way toimprove compliance is by emphasizing the importance ofcompliance via drug counseling implemented by pharmacistsduring dispensing. Patients who are at a high risk of DRPssuch as those receiving multiple drugs or drugs that are morelikely to cause DRPs, females, and geriatric patients should beidentified. Healthcare professionals should be aware of thesehigh-risk patients and spend more time monitoring them.
This study has its limitations. Although the study popula-tion is representative of general cancer patients in the publicsetting, information from a single institution may not begeneralizable to other settings. This study includes a mix poolof solid tumor and lymphoma patients, which may not berepresentative in other healthcare settings.Moreover, althoughthis was a prospective study, information collected on druguse at admission may be incomplete as it may have missedover-the-counter drug use, which would not be found in studydatabases. It could be argued that our assessment of DRPseverity was limited by subjectivity and misclassification;however, the evaluation of DRP characteristics was performedby applying systemic assessment algorithms such as theNaranjo algorithm.
Conclusion
This prospective study identified that 12.4 % of hospitaliza-tions among cancer patients were associated with DRPs.Among these DRPs, approximately half were preventable.This study provides a better understanding of the characteris-tics of DRPs that lead to hospitalizations, which may assisthealthcare professionals to be more vigilant in drug prescrib-ing, dispensing, and monitoring to prevent future DRPs fromoccurring. DRPs in cancer patients can be severe and evenfatal, and more care must be taken to avoid DRPs for thisgroup of patients. Future studies should evaluate the feasibilityto incorporate routine medication reviews conducted by
pharmacists in patients with cancer, in order to reduce theoccurrence of polypharmacy and associated DRPs.
Conflict of interest None.
References
1. Pharmaceutical Care Network Europe Foundation. PCNEClassification for drug related problems May 2006 2006
2. CohenMR, Anderson RW, Attilio RM, Green L, Muller RJ, PruemerJM (1996) Preventing medication errors in cancer chemotherapy. AmJ Health-Syst Pharm 53(7):737–746
3. Miranda V, Fede A, Nobuo M et al (2011) Adverse drug reactionsand drug interactions as causes of hospital admission in oncology. JPain Symptom Manage 42(3):342–353
4. van der Hooft CS, Dieleman JP, Siemes C et al (2008) Adverse drugreaction-related hospitalisations: a population-based cohort study.Pharmacoepidem Dr S 17(4):365–371
5. Lau PM, Stewart K, DooleyM (2004) The ten most common adversedrug reactions (ADRs) in oncology patients: do they matter to you?Support Care Cancer 12(9):626–633
6. Lazarou J, Pomeranz BH, Corey PN (1998) Incidence of adversedrug reactions in hospitalized patients: a meta-analysis of prospectivestudies. JAMA 279(15):1200–1205
7. Riechelmann RP, Zimmermann C, Chin SN et al (2008) Potentialdrug interactions in cancer patients receiving supportive care exclu-sively. J P Symptom Manage 35(5):535–543
8. Riechelmann RP, Tannock IF, Wang L, Saad ED, Taback NA,Krzyzanowska MK (2007) Potential drug interactions and duplicateprescriptions among cancer patients. J Natl Cancer Inst 99(8):592–600
9. Ko Y, Tan SL, Chan A et al (2012) Prevalence of the coprescriptionof clinically important interacting drug combinations involving oralanticancer agents in Singapore: a retrospective database study. ClinTher 34(8):1696–1704
10. Micromedex 2.0. Accessed 21/07/201311. Naranjo CA, Busto U, Sellers EM et al (1981) A method for estimat-
ing the probability of adverse drug reactions. Clin Pharmacol Ther30(2):239–245
12. Hallas J, Harvald B, Gram LF et al (1990) Drug related hospitaladmissions: the role of definitions and intensity of data collection,and the possibility of prevention. J Intern Med 228(2):83–90
13. McDonnell PJ, Jacobs MR (2002) Hospital admissions resultingfrom preventable adverse drug reactions. Ann Pharmacother 36(9):1331–1336
14. Carrasco-Garrido P, de Andres LA, Barrera VH, de Miguel GA,Jimenez-Garcia R (2010) Trends of adverse drug reactions related-hospitalizations in Spain (2001–2006). BMCHealth Serv Res 10:287
15. Ehsani JP, Jackson T, Duckett SJ (2006) The incidence and cost ofadverse events in Victorian hospitals 2003–04. Med J Aust 184(11):551–555
16. Pirmohamed M, James S, Meakin S et al (2004) Adverse drugreactions as cause of admission to hospital: prospective analysis of18 820 patients. BMJ (Clinical research ed) 329(7456):15–19
17. van der Hooft CS, SturkenboomMC, van Grootheest K, Kingma HJ,Stricker BH (2006) Adverse drug reaction-related hospitalisations: anationwide study in The Netherlands. Drug Saf 29(2):161–168
18. Chan A, Chen C, Chiang J, Tan SH, Ng R (2012) Incidence of febrileneutropenia among early-stage breast cancer patients receivinganthracycline-based chemotherapy. Support Care Cancer 20(7):1525–1532
Support Care Cancer

19. Kuderer NM, Dale DC, Crawford J, Lyman GH (2007) Impact ofprimary prophylaxis with granulocyte colony-stimulating factor onfebrile neutropenia and mortality in adult cancer patients receivingchemotherapy: a systematic review. J Clin Oncol 25(21):3158–3167
20. Chan A, Lee CP, Chiang J, Ng R (2013) Breakthrough febrileneutropenia and associated complications among elderly cancer
patients receiving myelosuppressive chemotherapy for solid tumorsand lymphomas. Support Care Cancer 21(8):2137–2143
21. Ng JH, Ang XY, Tan SH, Tao M, Lim ST, Chan A (2011)Breakthrough febrile neutropenia and associated complications inNon-Hodgkin's lymphoma patients receiving pegfilgrastim. ActaHaematol 125(3):107–114
Support Care Cancer