chronic renal failure(crf) shanghai ruijin hospital affiliated to shanghai second medical...
TRANSCRIPT
Chronic Renal Failure(CRF)
Shanghai Ruijin Hospital affiliated to Shanghai Second Medical University,
Dept.of Nephrology
Qian Ying

CRFDefinition: final stage of numorous renal diseases resulting fr
om progressive loss of glomerular, tubular and endocrine function in both kidneys. This leads to
disturbed excretion of end products of metabolism disturbed elimination of electrolytes and water disturbed secretion of hormones(eg. Erythropoietin, renin, pr
ostaglandins, active form of vitamin D)

CRF
Regional and racial incidence of CRF
• Britain 70-80/per million
• China 100/per million
• USA 60-70/per million

CRF
Etiology
diabetic nephropathy, hypertensive glomerular sclerosis, chronic GN
chronic GN, obstructive nephropathy, diabetic nephropathy
overseas
china

CRFPathogenesis (unknown)
uremic toxins
• small molecular weight:
urea, creatinine, uric acid, guanidine, phenol, amines, indoles
• middle molecular weight: PTH
• large molecular weight: 2-MG

CRF
Major hypothesis
• intact nephron hypothesis
final common pathway
(hemodynamically mediated glomerular injury)

CRFglomerular injuryglomerular injury
adaptive single nephron hyperfiltrationadaptive single nephron hyperfiltration
glomerular capillary plasma flow, hydraulic pressureglomerular capillary plasma flow, hydraulic pressure
Intact nephron hypertrophy and sclerosisIntact nephron hypertrophy and sclerosis

CRF
• Trade-off hypothesis
CRF Calcium phostate PTH SHPT bone,heart,blood,nerves injury
• Hypertension and compensatory hypertrophy of glomeruli
• Hypermetabolism of renal tubuli
• cytokines and lipid disturbances

CRF
• Stage 1: the normal stage of renal function
GFR>70 ml/min, BUN<6.5 mmol/L,
Scr<110 umol/L• Stage 2:imcompensation stage of renal
GFR 50-70 ml/min, 6.5 <BUN< 9 mmol/L,
110 <Scr< 178 umol/L
no any signs and symptoms except for the underlying disorders

CRF• Stage 3: azotemic stage GFR<50 ml/min,BUN>9 mmol/L Scr>178 umol/L there may be slight fatigue,anorexia and anemia• Stage 4: uremic stage GFR<25 ml/min,BUN>20 mmol/L Scr>445 umol/L a constellation of uremic syndrome may appear in t
his stage

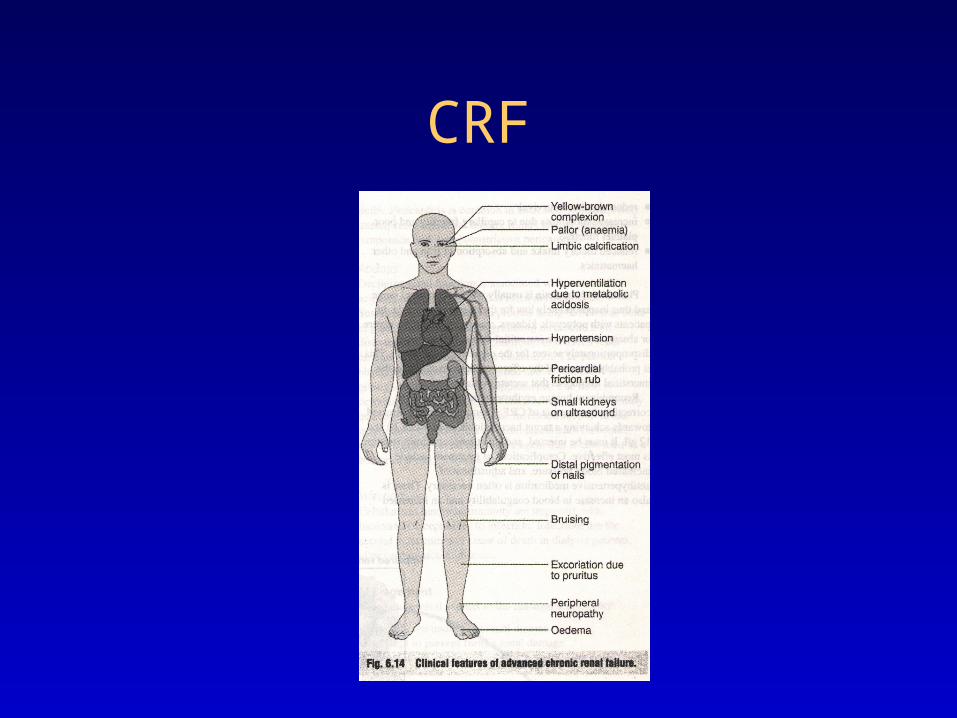
CRFSigns and symptoms of uremia
General Gastrointestinal tract Neuropathy Bone Blood Electrolyte disorders
Heart Skin Muscles Infection Lung Endocrine and
metabolic
CRF

CRF
Cardiovascular disorders
• Hypertension 80% Water and sodium retention
Alterations of RAAS
Glomerular capillary pressure> systemic arterial pressure

CRF
Atherosclerosis
hypertriglycerid, hypercholesterolemiahypertriglycerid, hypercholesterolemia
vascular calcificationvascular calcification
inadequate perfusion of the limbsinadequate perfusion of the limbs

CRF
Pericarditis• Uremic• Dialysis associated
Signs and symptoms• Chest pain• Friction rub• Pericardial effusion and tamponade

CRF
Hematologic disorders• Anemia, bleeding, granulocyte, platelet dysfunction
Causes:• Relative deficiency of erythropoietin• Decreased erythropoietin production• Reduced red cell survival• Increased blood loss• Folate and Iron deficiency• Hypersplenism

CRF
Neuropathy• Central nervous system Tiredness, insomnia, agitation, irritability, depression, regression, rebellion• Peripheral nervous system Restless leg syndrome the patient’s legs are jumpy during the night, painful paresthesis of extre
mities, twitching, loss of deep tendon reflexes , musclar weakness, sensory deficits

CRF
Renal osteodystrophyType I: high turn-over bone diseaseType II: low turn-over bone diseaseType III: mixture

CRF
Causes of renal osteodystrophy
• 1, 25(OH)2D3• calcium phosphate • SHPT
• malnutrition
• iron and aluminum overload

CRF
CRF
Water, electrolyte and acid-base disturbances
• potassium sodium • calcium phosphate • Metabolic acidosis
• magnesium

CRF
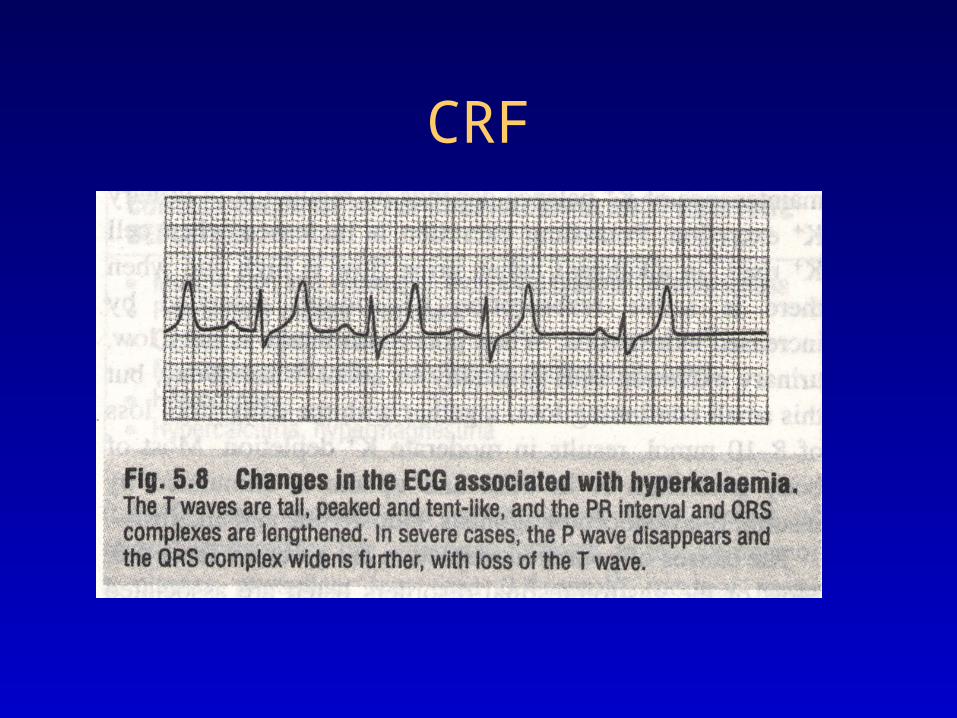
Diagnosis of hyperkalemia
• Plasma K>5.5mmol/L
• Plasma K>7.0mmol/L cardiac arrest
CRF

CRF
Causes of hyperkalemia Increased intake: rapid adminstration of K b
y mouth or intravenously Drugs containing K(chinese medical herbs) Impaired excretion Chronic renal failure(GFR<15ml/min)

CRF
Causes of hyperkalemia Shift of K out of cells Metabolic acidosis
Tissue breakdown
Bleeding into soft tissues, GI tract or body cavities
Hemolysis
Catabolic states

CRF
Diagnosis:• Case history• Physical examination• Laboratory studies including
urinalysis , renal function tests , biochemical analysis of blood
• X-ray, ultrosound and radiorenogram

CRF
Treatment of CRF Non-dialysis dialysis

CRF
Non-dialysis
• Diet therapy
• Treatment of reversible factors
• Treatment of the underlying disease
• Treatment of complcations of uremia
• Chinese medical herbs

CRF
Diet therapy
• Protein restriction (0.5-0.8mg/kg/d)
• Adequte intake of calories(30-35kcal/kg/d)
• Fluid intake:urine volume +500ml
• Low phosphate diet(600-1000mg/d)
• Supplement of EAA(ketosteril)

CRF
Reversible factors in CRF• Hypertension• Reduced renal perfusion (renal artery stenosis, hyp
otension , sodium and water depletion, poor cardiac function)
• Urinary tract obstruction• Infection• Nephrotoxic medications• Metabolic factors(calcium phosphate products )

CRFManagement of complications of uremia
Hyperkalemia• Identify treatable causes• Inject 10-20ml 10% calcium gluconate • 50% gluconate 50-100ml i.v.+insulin 6-12u• Infusion 250ml 5% sodium bicarbonate• Use exchage resin• Hemodialysis or peritoneal dialysis

CRF
Cardiac complications
• Diuretics
• Digitalis
• Treat hypertension
• dialysis

CRF
Antihypertensive therapy
Target blood pressure 130/85mmHg
• ACE inhibitors
• Angiotension II receptor antagonists
• Calcium antagonists-blockers
• vesodialators

CRF
Treatment of anemia
• Recombinant human erythropoietin(rhEPO)
• 2000-3000u BIW H
• Target hemoglobin 10-12g/L
• hemotocrit 30-33%

CRF
Side effects of rhEPO
• Hypertension
• Hypercoagulation
• Thrombosis of the AVF

CRF
rhEPO resistant
• Iron deficiency
• Active inflamation
• Malignancy
• Secondary hyperparathyroid
• Aluminum overload
• Pure red cell aplasia

CRF
Treatment of renal osteodystropy Low phosphate diet Calcium carbonate (1-6g/d) Vitamin D (0.25ug/d for prophylactic, 0.5ug/d f
or symptomatic, pulse therapy 2-4ug/d for severe cases)
parathyroidectomy

CRF
Renal replacement therapy
• Hemodialysis
• Peritoneal dialysis
• Renal transplantation

CRF
Indications of HD
• GFR<10ml/min
• the uremic syndrome
• hyperkalemia
• acidosis
• fluid overload

Hemodialysis
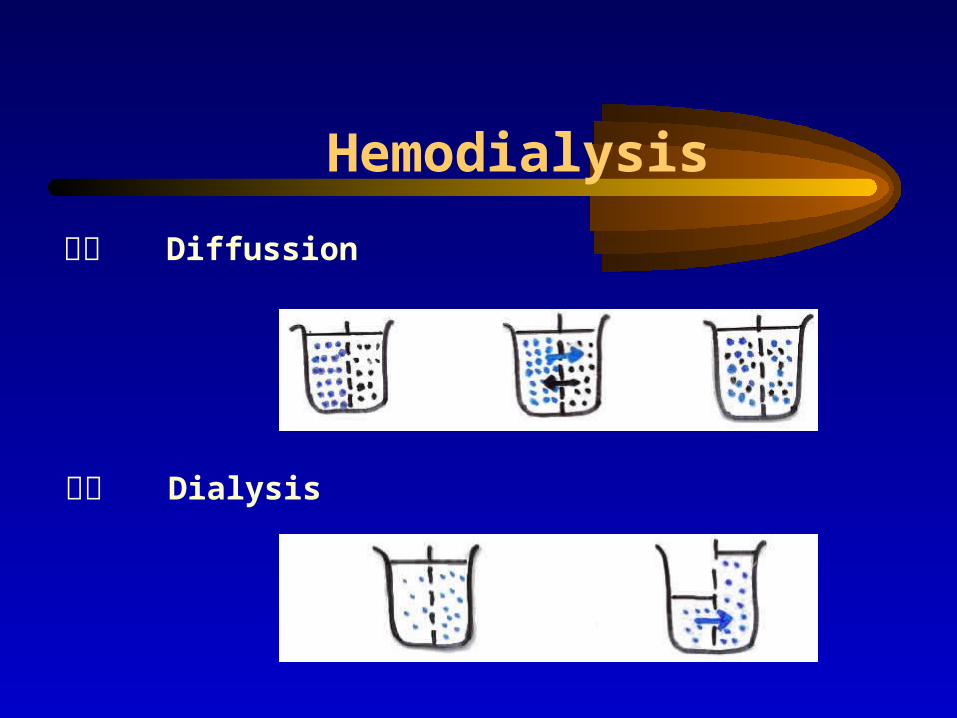
Hemodialysis
弥散 Diffussion
渗透 Dialysis

Hemodialysis
超滤 Ultrofiltration
对流 Conduction
正压 负压

Contraindications of HD
• Shoke
• Severe caidioc complications
• Severe bleeding
• malignency , sepsis
• poor condition in vascular system
CRF
Indications of CAPDchildold people with cardiovascular diseasedibetic nephropathytrouble of AVF

Choice of HD or CAPD
poorbetterEcnomic situation
poorgoodVascular condition
BleedingNo bleedingBlood
yesnoCardiovascular disease
eldlyyoungAge
PDHD
治疗

CRF
Indications of RT
• maitenance dialysis patients without contraindications of RT
• age<60 years

CRF
Prognosis
5-year survival Home HD 80% RT 60% Hospital HD 60% CAPD 50%

CRF
Drug dosing in CRF Redused dose and adminstration interval Ccr(ml/min)=[(140-years old)×body weight(k
g)]/[72×Scr(mg/dl)] for female: ×0.85
Acute heart failure in uremia (key treatment?)
• Diuretics
• Digitalis
• Treat hypertension
• dialysis
