claudette ppt
TRANSCRIPT

Illness Behavior
Presentor:Claudette Kay Diaz
Illness us a highly personal state in which the person’s physical, emotional, intellectual, social,
developmental, or spiritual functioning is thought to be diminished. It is not synonymous with disease and
may or may not be related to disease. Types of Illness
Acute illness Chronic illness
Illness behavior is a coping mechanism which involves ways in which individuals describe, monitor and
interpret their symptoms, take remedial actions, and use the health care system.
How people behave when they are ill is highly individualized and affected by many variables such as,
age, sex, occupation, socioeconomic status, religion, ethnic origin, psychologic stability, personality,
education and modes of coping.
Disease can be described as an alteration in body functioning resulting in a reduction of capacities or
shortening of the normal life span.
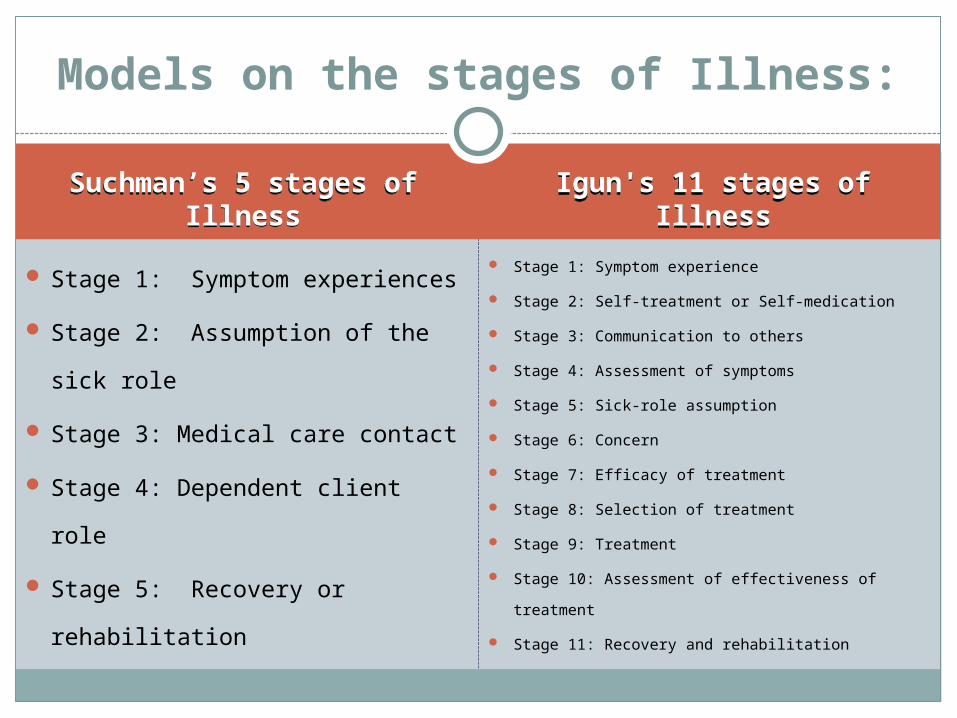
Suchman’s 5 stages of Illness
Suchman’s 5 stages of Illness
Igun's 11 stages of Illness
Igun's 11 stages of Illness
Stage 1: Symptom experiences
Stage 2: Assumption of the sick role
Stage 3: Medical care contact
Stage 4: Dependent client role
Stage 5: Recovery or rehabilitation
Stage 1: Symptom experience
Stage 2: Self-treatment or Self-medication
Stage 3: Communication to others
Stage 4: Assessment of symptoms
Stage 5: Sick-role assumption
Stage 6: Concern
Stage 7: Efficacy of treatment
Stage 8: Selection of treatment
Stage 9: Treatment
Stage 10: Assessment of effectiveness of treatment
Stage 11: Recovery and rehabilitation
Models on the stages of Illness:
Suchman’s five stages of Illness:

Stage 1: Symptom experience
- Cognitive aspect (believe something is wrong)
- Physical experience of symptoms
- Emotional response (fear or anxiety)
Stage 2: Assumption of the sick role
Accepts the sick role and seeks confirmation from family and friends
Continue with self- treatment
Excused from normal duties and expectations
Emotional responses common (withdrawal, anxiety, fear and depression)
Feels the need to seek professional health advice
Stage 3: Medical care contact
Seeks advice of a health professional to:
Validate real illness
Explain illness in understandable terms
Get reassurance that they will be alright or prediction of what the outcome will be

Stage 4: Dependent client role
Becomes dependent on the professional for help

Stage 5: Recovery or rehabilitation
Relinquish the dependent role
Resume former roles and responsibilities
Permanent disability requires major adjustments in functioning
Igun's eleven stages of Illness
Stage 2: Self-treatment or Self-medication
The person begins self treatment
If the person believes the symptoms are serious, he/she moves to the next stage
Stage 1: Symptom experience
The person experiences symptoms and realizes there is a problem
The person often gives meaning to the symptoms and labels them and responds emotionally to the symptoms
Stage 3: Communication to others
The person communicates symptoms to significant others or a health professional
Stage 4: Assessment of symptoms
The person assesses the symptoms to determine legitimacy and make tentative diagnosis

Stage 5: Sick-role assumption
The person assumes the sick-role
Stage 6: Concern
The person’s significant other(s) offer concern and support
Stage 7: Efficacy of treatment
The person assesses various treatments and sources of treatment
Stage 8: Selection of treatment
The person assesses various treatments and costs
The person may defer to health professional’s advice

Stage 9: Treatment
The person implements the treatment plan
Stage 10: Assessment of effectiveness of
treatment
The person assesses if treatment not effective
The person may return to earlier stage

Stage 11: Recovery and rehabilitation
The person returns to earlier health status before illness or experiences temporary or permanent disability

Sick Role Behavior

Parson’s four aspects of the sick role:
Being Sick’ is not simply a ‘state of fact’ or ‘condition’, it is a specifically
patterned social role. In Western Societies the sick role implies four major
expectations which comprise of two rights and two duties. (Parsons: 1951:436-
7).
The model of the sick role, which Talcott Parsons designed in the 1950s, was
the first theoretical concept that explicitly concerned medical sociology. In
contrast to the biomedical model, which pictures illness as a mechanical
malfunction or a microbiological invasion, Parsons described the sick role as a
temporary, medically sanctioned form of deviant behaviour.
1. Clients are not held responsible for their condition.
- Sick person generally not held responsible for their condition (absence of blame).
- Illness is considered to be beyond individual’s control’; therefore not simply curable by willpower.
2. Clients are excused from certain social roles and tasks.
-Sick person is temporarily exempt from ‘normal’ social roles.
-The more severe the sickness the greater the exemption.
3. Clients are obliged to try to get well as quickly as possible.
-Sick person is expected to see being sick as undesirable; thus they have an obligation to try to ‘get well’.
-In this context exemption from normal responsibilities is temporary and conditional upon wanting and trying to get better.
4. Clients or their families are obliged to seek competent help.
-The sick person has an obligation to seek technically competent help from a suitably qualified professional and to cooperate in the process of trying to recover.
Effects of Illness
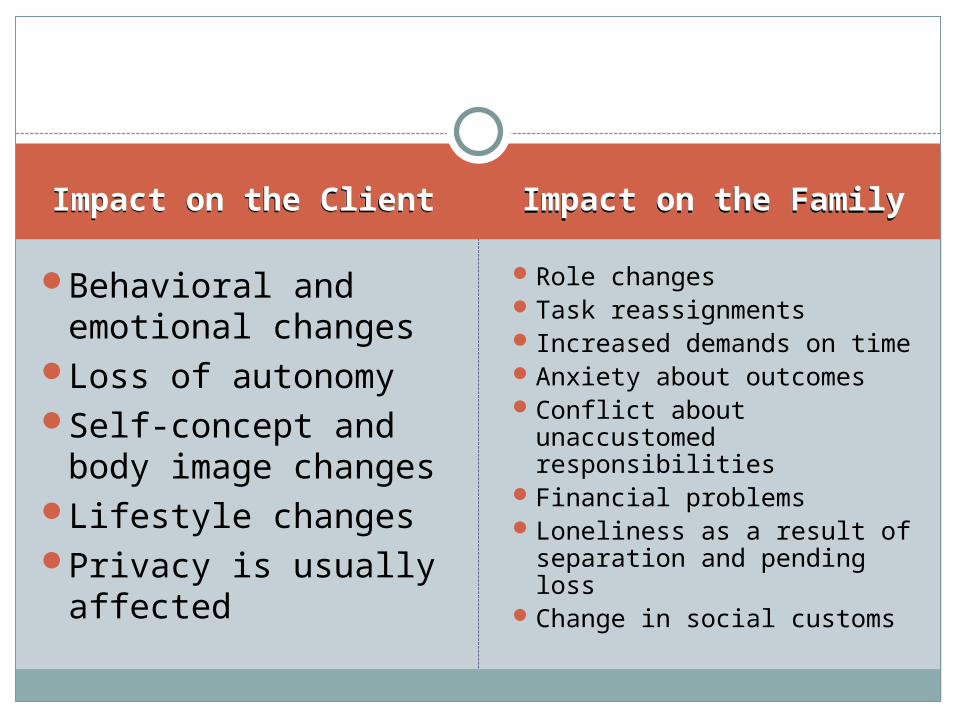
Impact on the ClientImpact on the Client Impact on the FamilyImpact on the Family
Behavioral and emotional changes
Loss of autonomy Self-concept and body
image changesLifestyle changes Privacy is usually affected
Role changesTask reassignments Increased demands on timeAnxiety about outcomesConflict about unaccustomed
responsibilitiesFinancial problemsLoneliness as a result of
separation and pending lossChange in social customs
Effects of Hospitalization
Privacy
When a client enters a hospital or a nursing facility, the loss of privacy is instantly obvious.
Autonomy
Hospitalized people frequently give up much of their autonomy—decisions about meals, hygienic practices and sleeping are frequently made for them.
Effects of Hospitalization
Lifestyle
Hospitalization marks a change in the lifestyle. Many hospitals determine what their clients should be doing and when they should be doing them.
Roles
People’s life roles frequently change when they are hospitalized.
Economics
Hospitalization often places a genuine financial burden on clients and their families.