cmh medication reconciliation journey 2011
DESCRIPTION
TRANSCRIPT
CITIZENS MEMORIAL HEALTHCARE
MEDICATION RECONCILIATION
JOURNEY
1
Designing the Process
• 2008 Strategic Plan identified Med Rec as a critical process requiring an action plan.
• MIB (make it better) initiated• Team established by action plan owner, to include clinical
leaders from all disciplines– Acute Care– Home Care/Hospice– Clinics– Long Term Care– Pharmacy– Physicians
2
• Each discipline/business unit identified a leader and a team of peers – Clinical staff– Information Specialists or Technicians– Quality/Performance Improvement staff
• A process flow diagram was drawn for each discipline– Informal FMEA (failure modes effects analysis) was
applied to each process, to identify weak steps or steps lending to failure
3
• Basic med. rec. education was developed and provided to all clinical staff.
• The first step included buy in by nurses and physicians to stop using and accepting: “resume all meds”.
• IS focused on designing improvements in the listing of medications, and methods for electronic med rec for transfers within the system.
4
Roll Out
• Initial process rolled out in Emergency Dept.• To Acute care and physicians
o An admission/discharge nurse was hired, med.rec. was part of this role’s responsibility
• Clinics with each visit• Home Care – learning to work with a new
software program• LTC is in initial process of rolling out for
admission from home 5

• Summer of 2010 joined the national collaboration with Primaris– Outlined processes again- new issues identified– Staff had designed “work arounds”– Staff focused on admission and discharge, ignoring
med rec at transfer
New focus on education of nurses, physicians, community:
6
Education in process or for consideration: New employee orientation Annual one/one competency for nurses Interactive Healthstream courses for
nurses One/one education with physicians
Monthly news letters with bits of med rec education
7
Community Education:Website paragraphsPrintable med list on websiteArticles in CMH quarterly magazineBrief articles in newspaper or on radioAccess to med list from electronic portals
possibly from Patient Friendly registration card
8
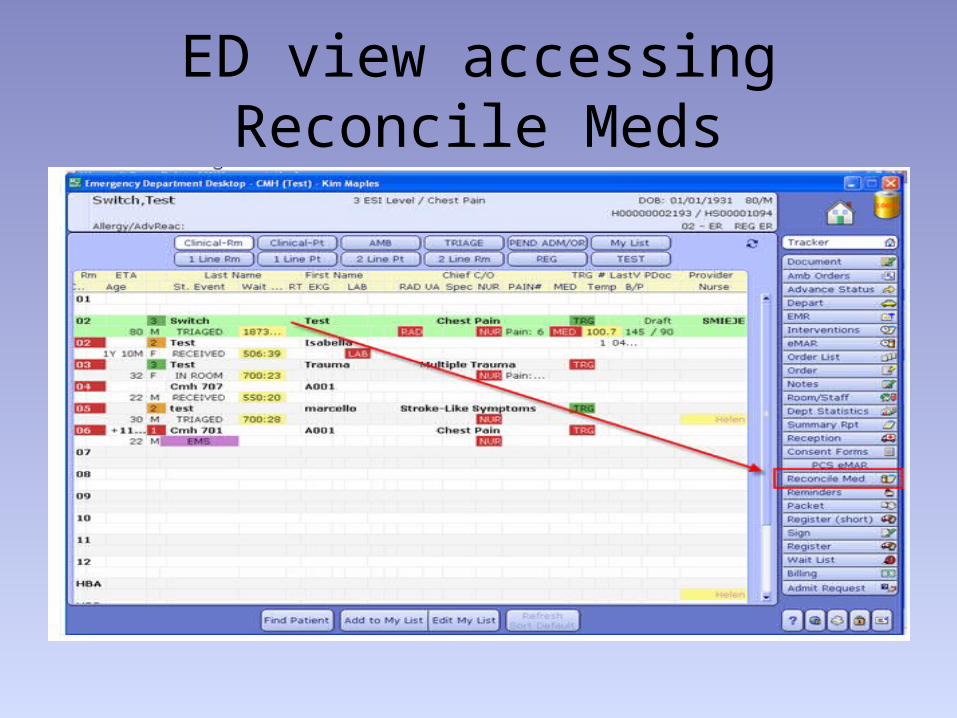
ED view accessing Reconcile Meds
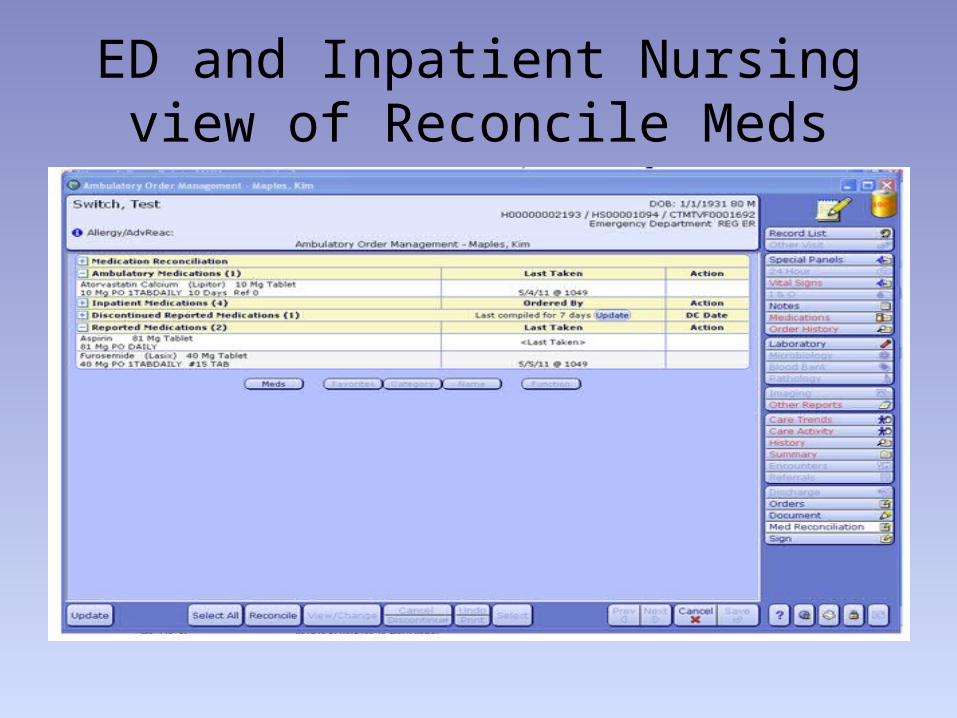
ED and Inpatient Nursing view of Reconcile Meds
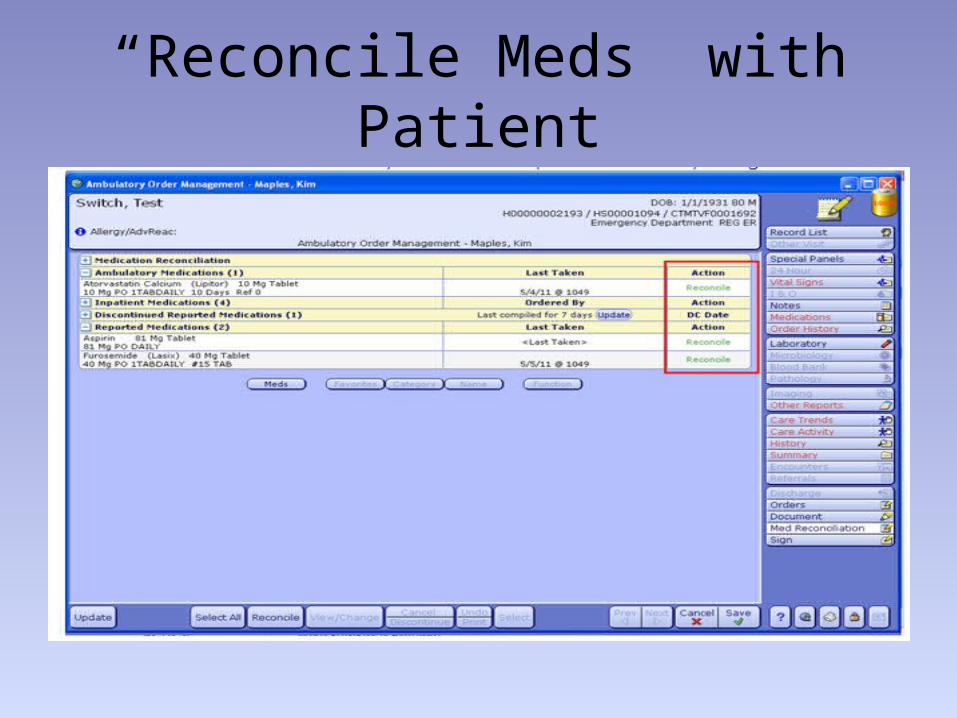
“Reconcile Meds” with Patient
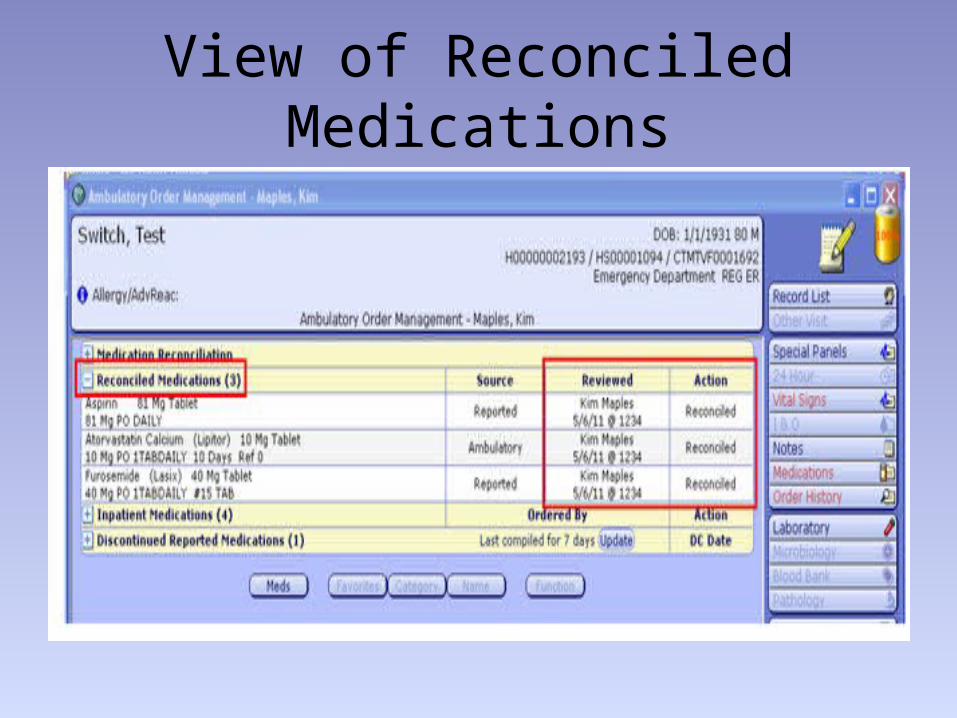
View of Reconciled Medications
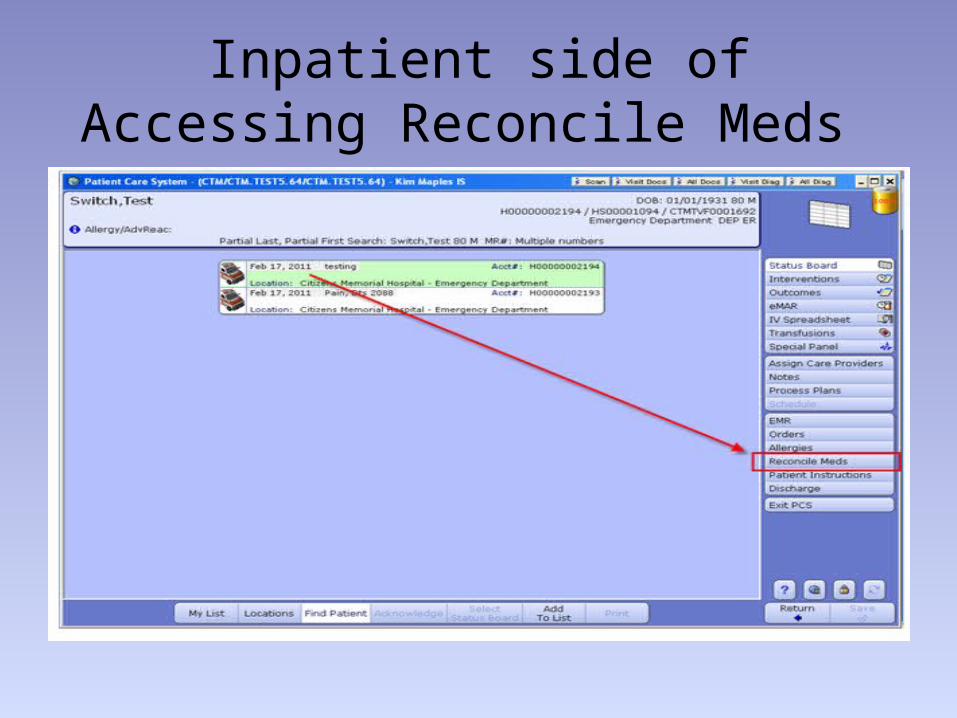
Inpatient side of Accessing Reconcile Meds
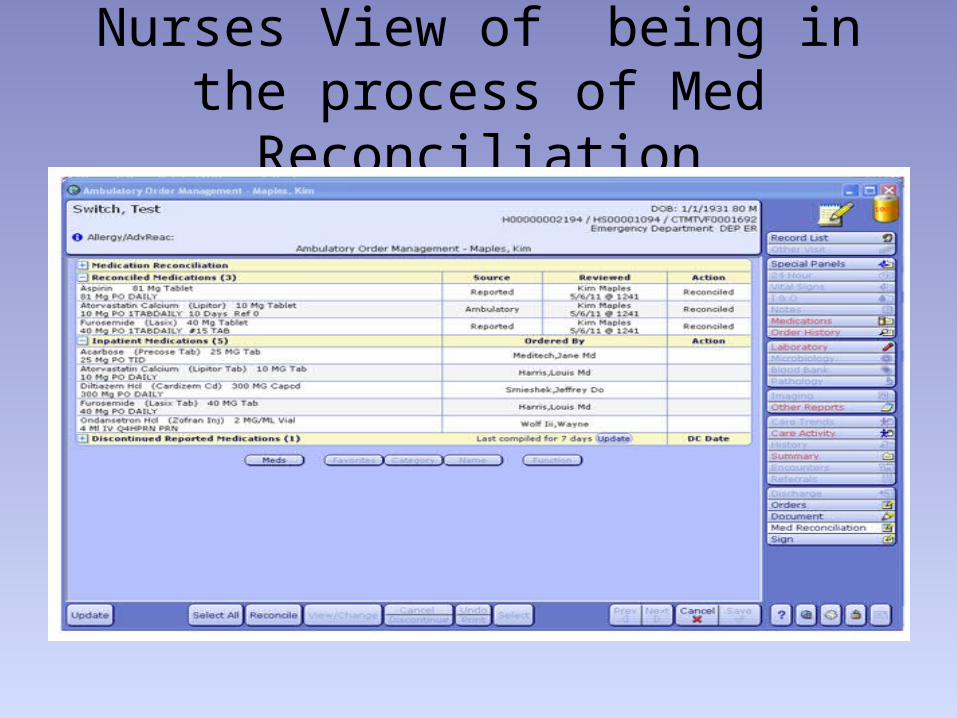
Nurses View of being in the process of Med Reconciliation
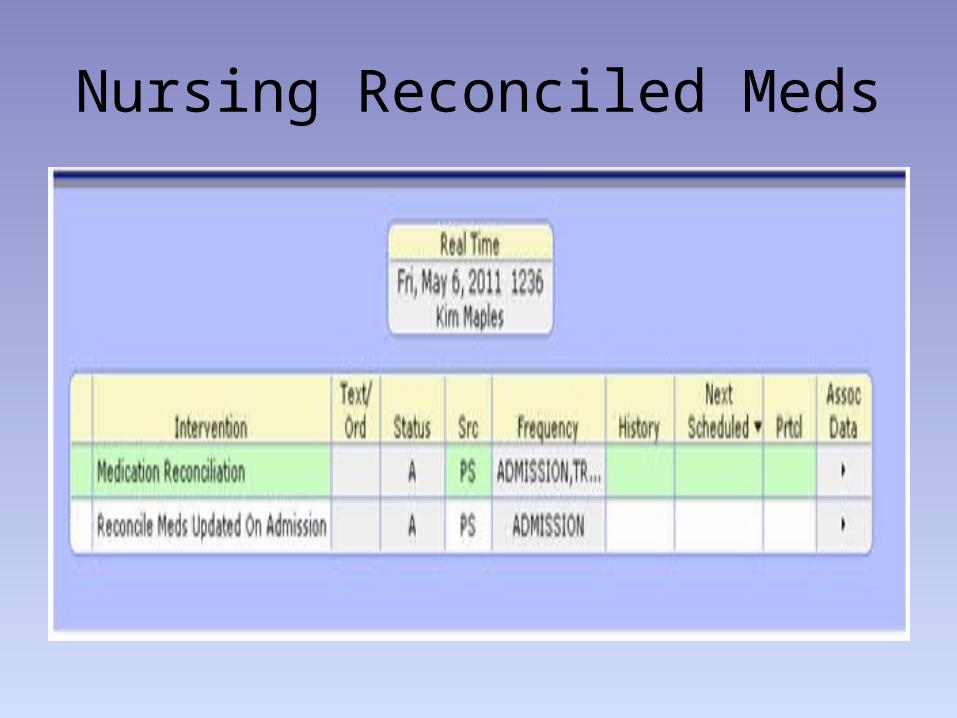
Nursing Reconciled Meds
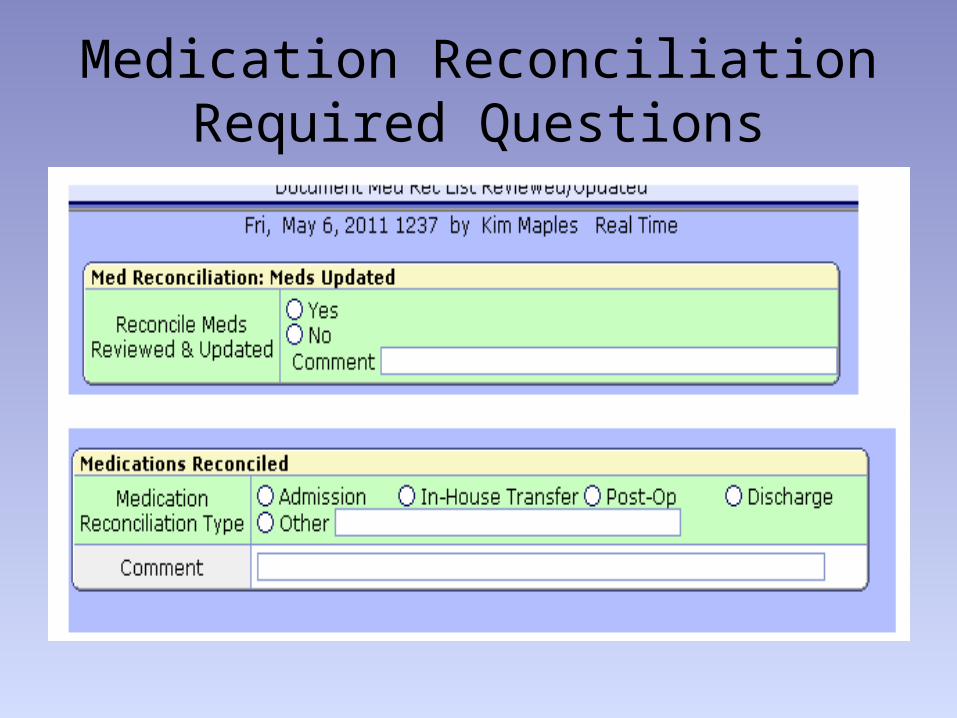
Medication Reconciliation Required Questions
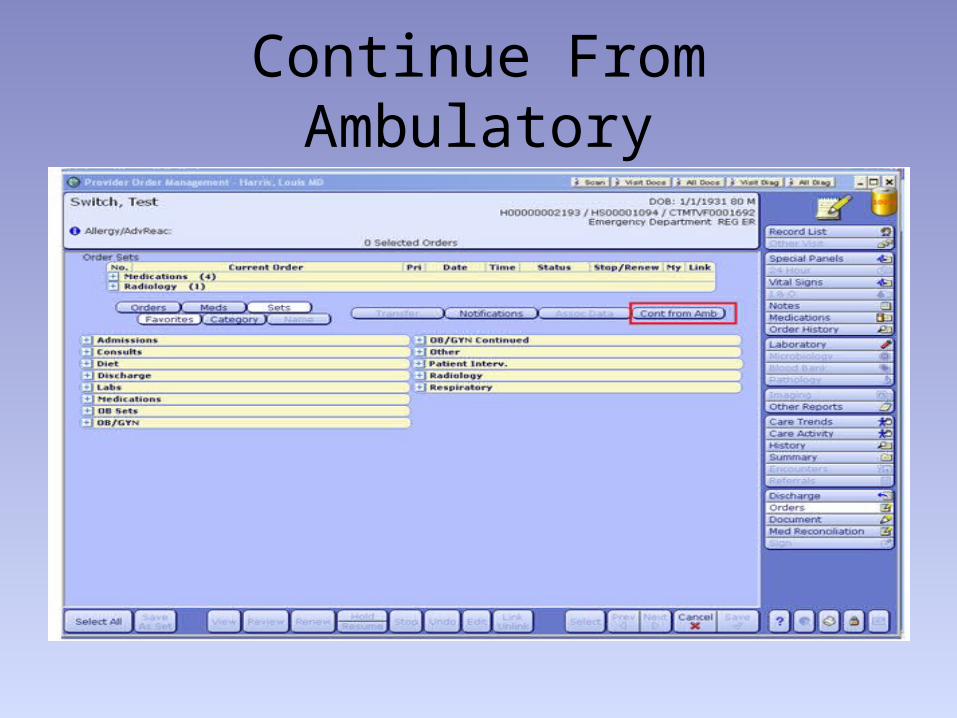
Continue From Ambulatory
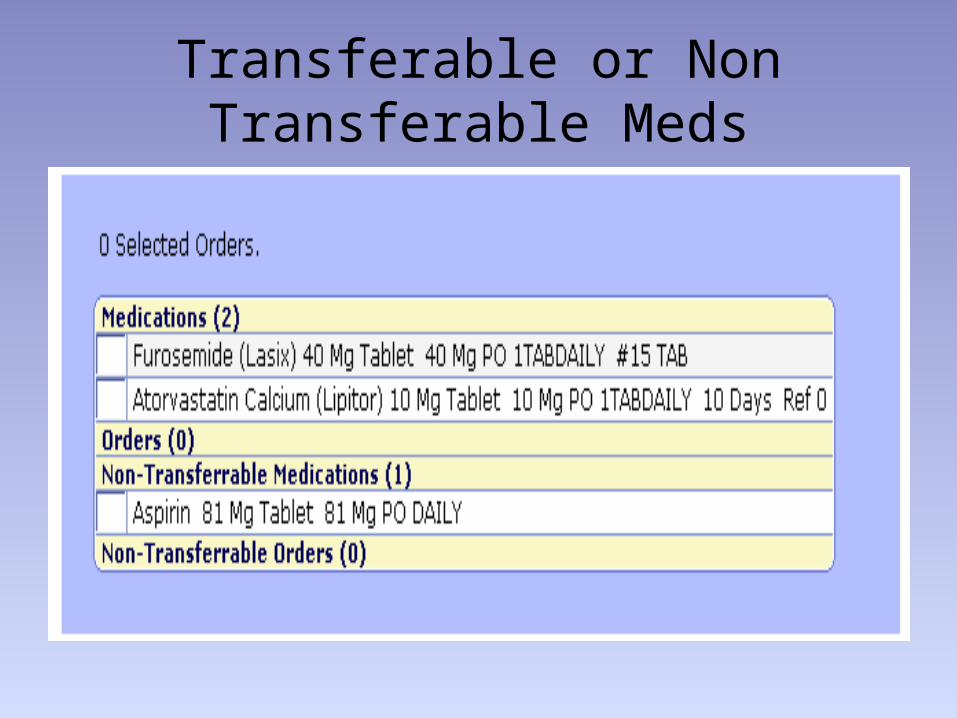
Transferable or Non Transferable Meds

Physician View of Discharge Med Reconciliation

LTCAdmission Medication process
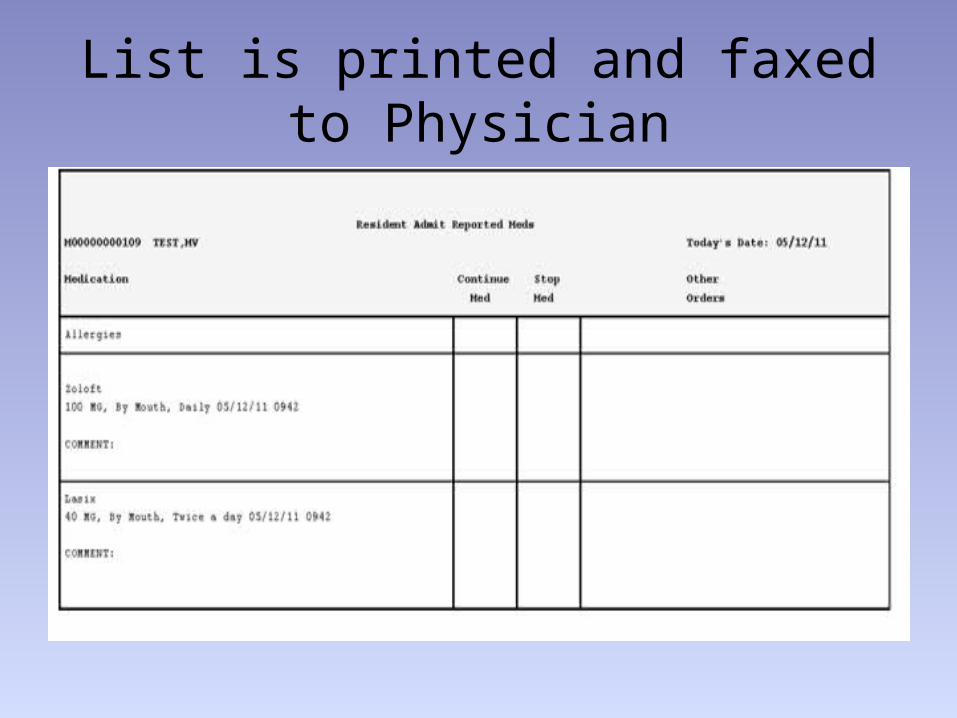
List is printed and faxed to Physician
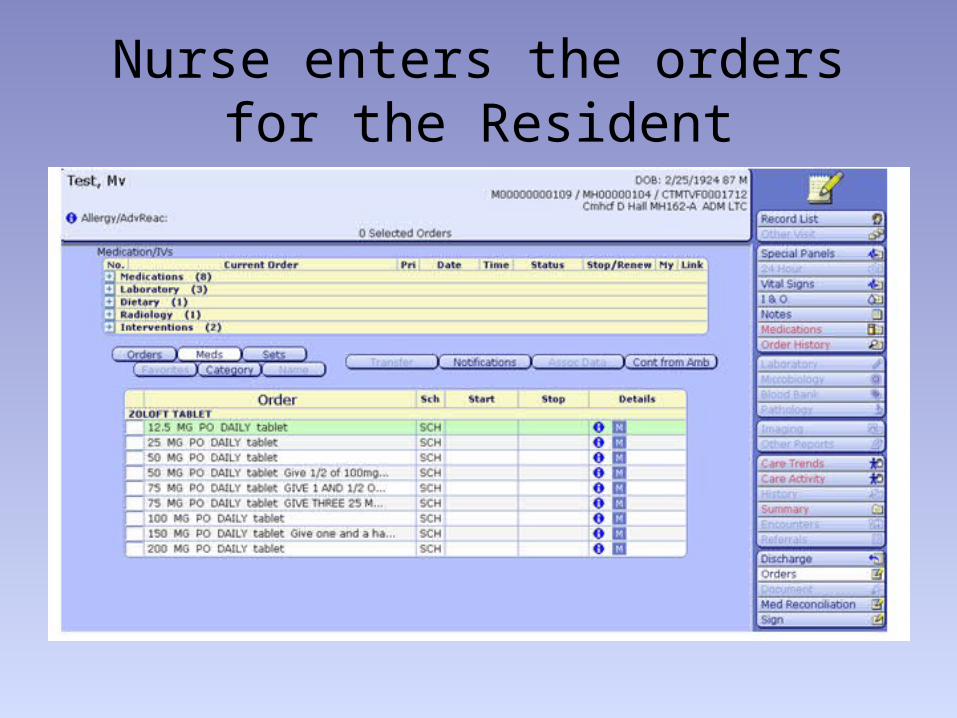
Nurse enters the orders for the Resident
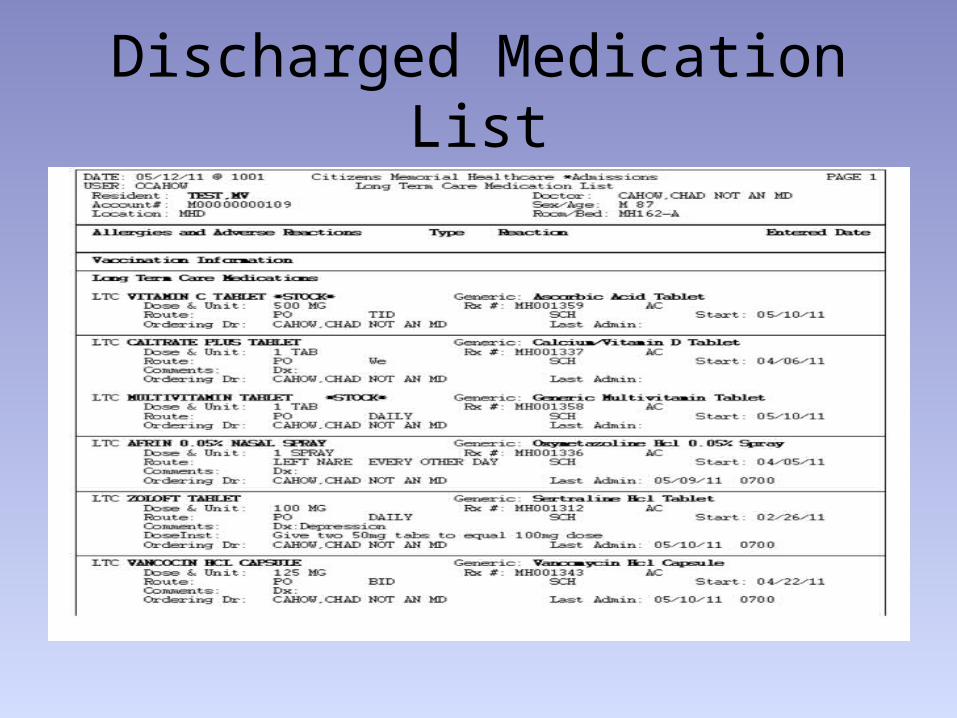
Discharged Medication List
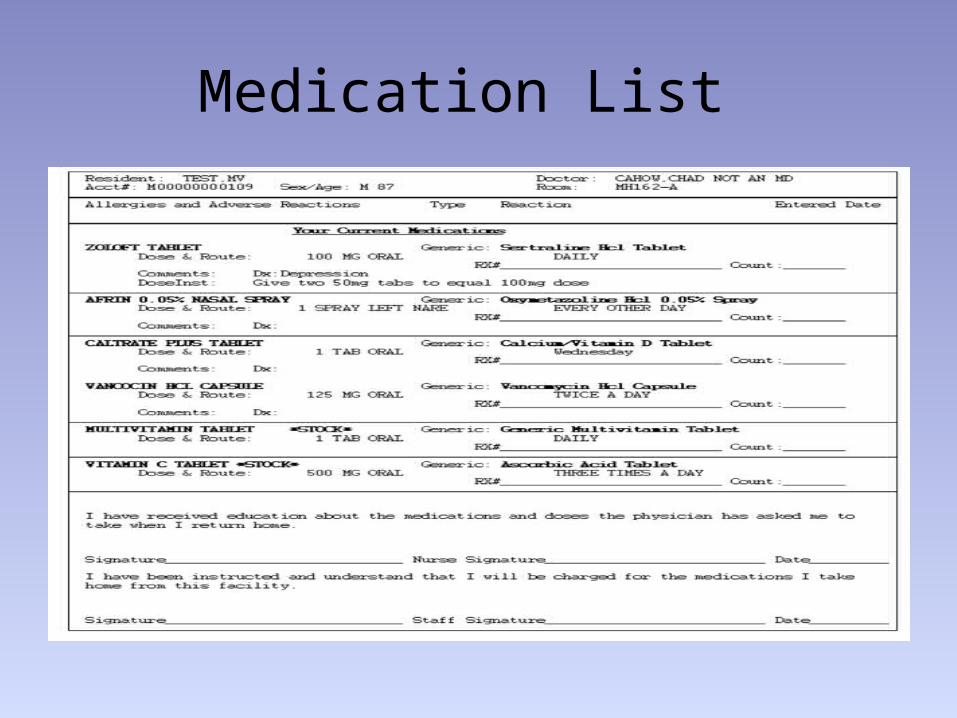
Medication List
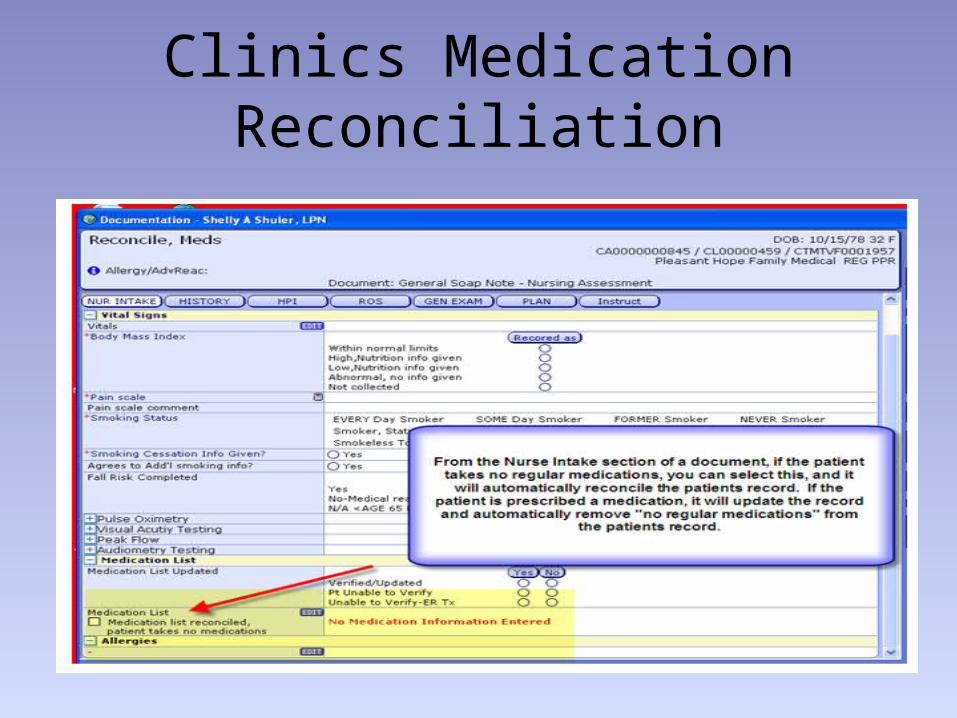
Clinics Medication Reconciliation
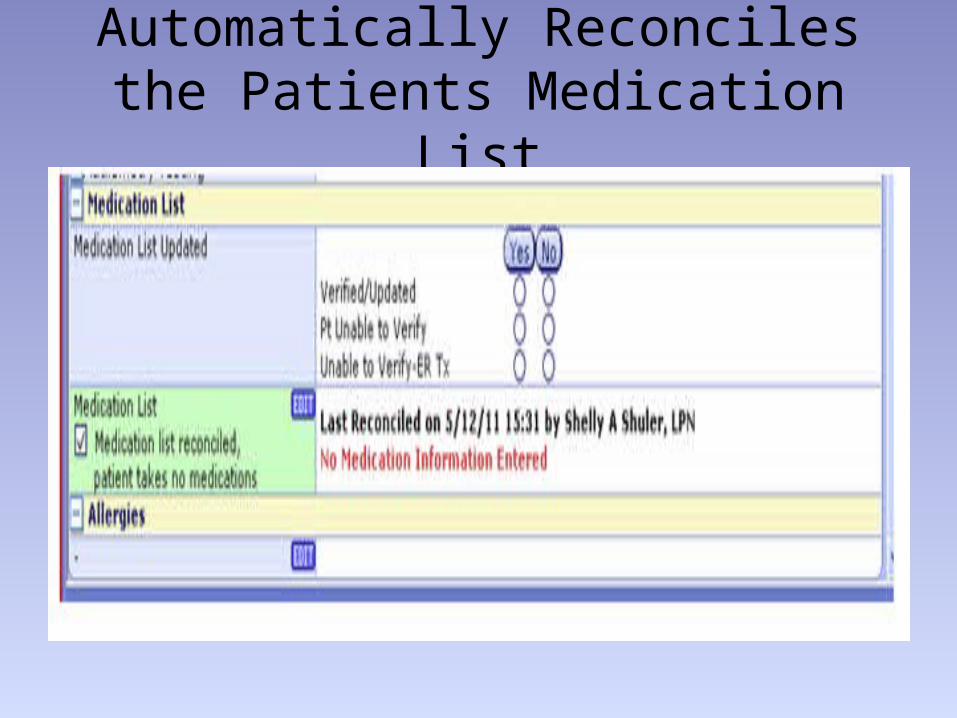
Automatically Reconciles the Patients Medication List
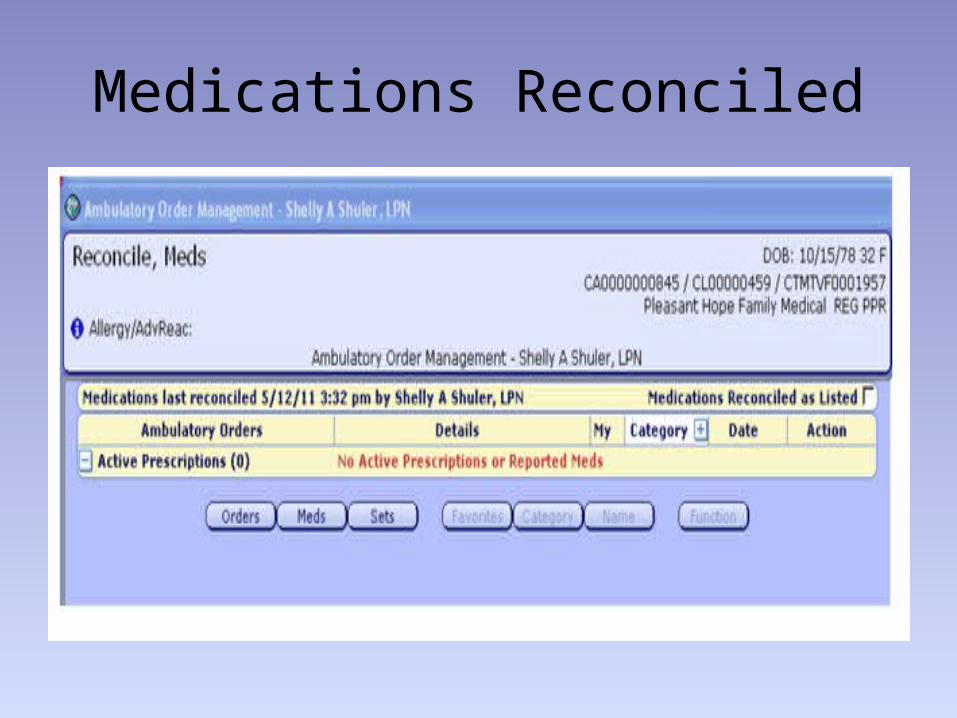
Medications Reconciled
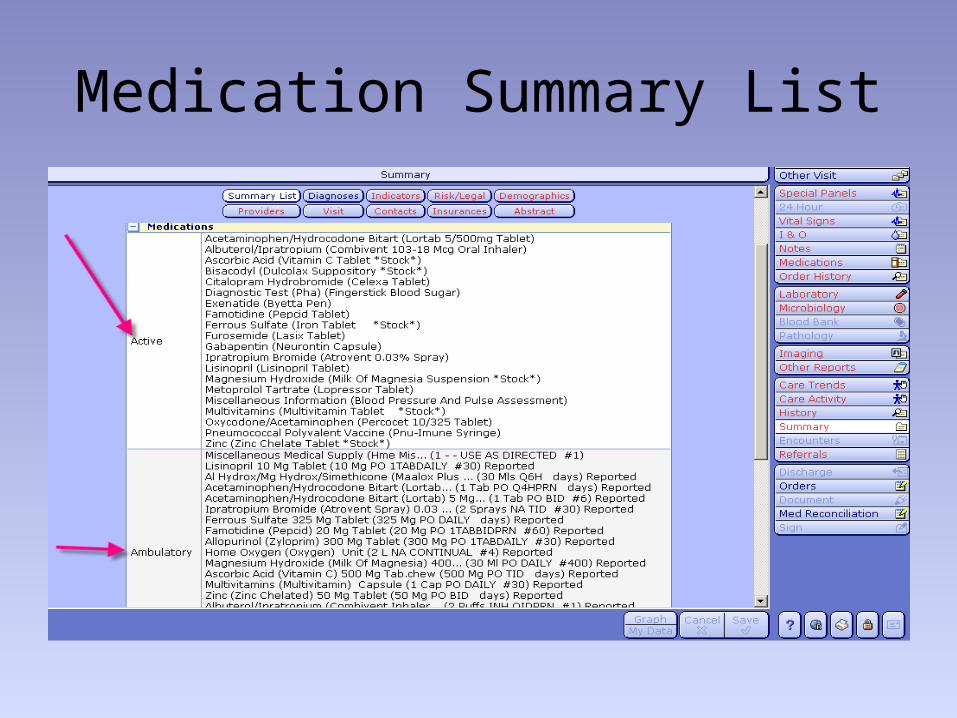
Medication Summary List
Lessons Learned
• Staff from all business units must know where to find the “source of truth”
• We can measure completion of med rec but it is very difficult to find the resources to track accuracy
• Staff becomes dependent on the system to guide the process
• Biggest Lesson Learned: We have a process now but if one person does not do their part completely the entire process is impacted and it is hard to identify errors.
29
For More Information or Clarification
• Aileen Kelley RN,BC CMH Quality Coordinator– [email protected]
• Michelle Cahow CMH IS Specialist– [email protected]
30