cms proposed changes for meaningful use in 2015-2017 mark segal, vice president, government and...
TRANSCRIPT

CMS Proposed Changes for Meaningful Use in 2015-2017Mark Segal, Vice President, Government and Industry Affairs, GE Healthcare ITMay 1, 2015

©2015 General Electric Company – All rights reserved.
This does not constitute a representation or warranty or documentation regarding the product or service featured. All illustrations are provided as fictional examples only. Your product features and configuration may be different than those shown. Information contained herein is proprietary to GE. No part of this publication may be reproduced for any purpose without written permission of GE.
DESCRIPTIONS OF FUTURE FUNCTIONALITY REFLECT CURRENT PRODUCT DIRECTION, ARE FOR INFORMATIONAL PURPOSES ONLY AND DO NOT CONSTITUTE A COMMITMENT TO PROVIDE SPECIFIC FUNCTIONALITY. TIMING AND AVAILABILITY REMAIN AT GE’S DISCRETION AND ARE SUBJECT TO CHANGE AND APPLICABLE REGULATORY CLEARANCE.
Customer is responsible for understanding and meeting the requirements of achieving meaningful use through use of HHS certified EHR technology and associated standards. Customer is responsible for understanding applicable GE documentation regarding Meaningful Use functionality and reporting specifications, and for using that information to confirm the accuracy of meaningful use attestation. Customer is responsible for ensuring an accurate attestation is made and GE does not guarantee incentive payments. Use of the product does not ensure customer will be eligible to receive payments.
* GE, the GE Monogram, Centricity and imagination at work are trademarks of General Electric Company.
General Electric Company, by and through its GE Healthcare division.
Centricity Practice Solution v12.0 and Centricity EMR v9.8 are certified ONC 2014 Edition compliant complete and modular EHRs. For additional certification and transparency information, visit www.gehealthcare.com/certifications.

Modifications to Meaningful Use in 2015-2017: Proposed RuleAligns with Stage 3 proposed rule
Removes redundant, duplicative and topped out measures
Modifies patient-focused Stage 2 measures for patient engagement
Single set of objectives & measures (with “stage” adjustments through 2017)
No changes to certified EHR technology required or CQM reporting
Aligns reporting period for all (including hospitals) to full calendar year
Reporting period in 2015 (only) is any continuous 90-day period

4
Changes to Stages 1 and 2
Medicare and Medicaid
All on single set of Stage 2 objectives and measures
Some Stage 1 adjustments
Core and Menu eliminated – all objectives required (with exceptions)• Stage 1: three menu items now required – med reconciliation,
patient education, public health (multiple options)
• Stage 2 hospitals: one menu now required (eRx)
Public Health has multiple consolidated measures• EP – 2/5 (1/5 if Stage 1) and Hospital 3/6 (2/6 if Stage 1)

2015-17 Proposed Objectives
1. Protect Electronic Health Information – minor changes per Stage 3
2. Clinical Decision Support – retain with alternate specs.
3. Computerized Provider Order Entry (CPOE) – retain with alternate exclusions/specs.
4. Electronic Prescribing (eRx) - retain with alternate exclusions
5. Summary of Care – retain Measure 2 with alternate exclusion and with no transport specification; delete Measure 1 (any method) and 3 (Test)
6. Patient Specific Education – retain with alternate exclusion
7. Medication Reconciliation -retain with alternate exclusion
8. Patient Electronic Access (V,D,T) – retain measure 1 and revise measure 2 thresholds, with alternate exclusion
9. Secure Electronic Messaging – retain
10. Public Health and Clinical Data Registry (CDR) Reporting– replace with consolidated Stage 3 objective and “active engagement” 5
6
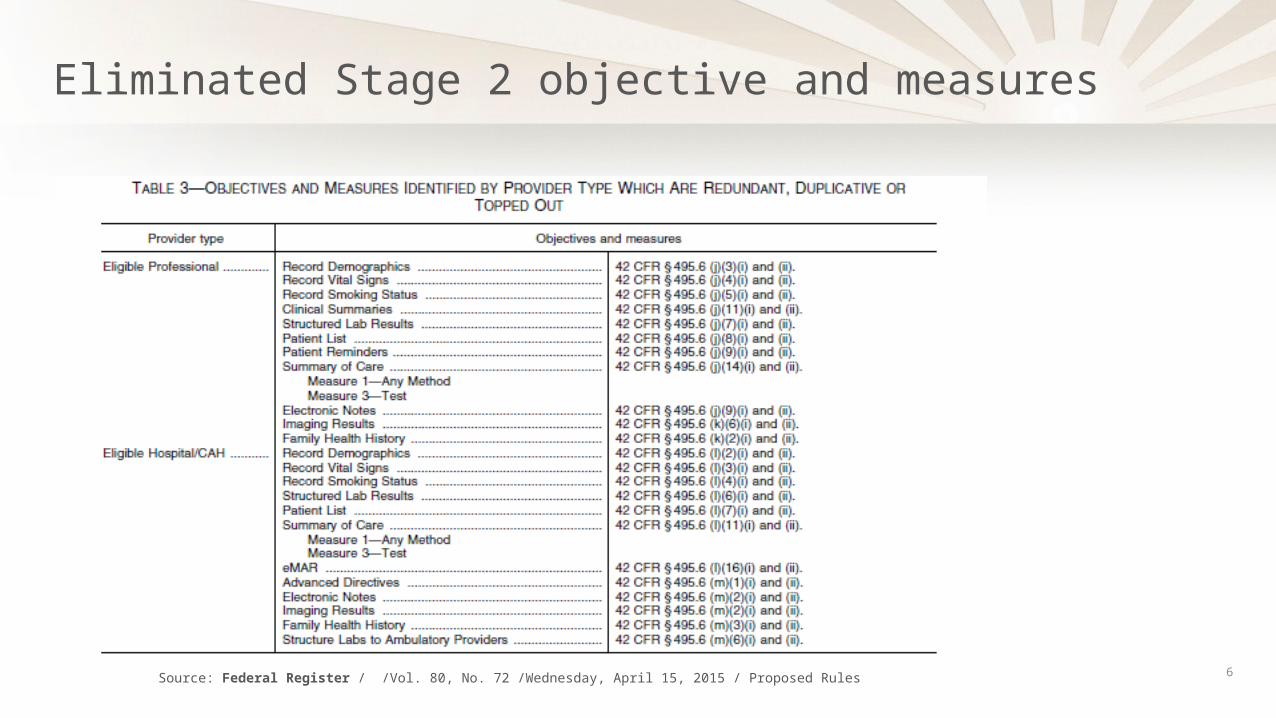
Eliminated Stage 2 objective and measures
Source: Federal Register / /Vol. 80, No. 72 /Wednesday, April 15, 2015 / Proposed Rules

2015Attest to modified version of Stage 2
with accommodations for Stage 1 providers
2016 Attest to modified version of Stage 2
2017 Attest to either modified version of Stage 2 or full version of Stage 3
2018 Attest to full version of Stage 3
2015 Modification Proposed Rule: Timeline

8
Timetable for revised meaningful use criteria
Source: Federal Register / /Vol. 80, No. 72 /Wednesday, April 15, 2015 / Proposed Rules

9
Alternate 2015 exclusions & specifications for Stage 1 providers Maintaining Stage 1 specifications for objectives and measures with lower threshold or other difference between Stages 1 and 2 (e.g., eRx).
Exclusion for Stage 2 measures with no equivalent Stage 1 measure or where provider did not plan to attest to now-required menu objective (e.g., 10% TOC electronic transmission)
Defined for each applicable objective and measure

10
Patient engagement changes
V,D,T – from 5% to one (1) patient seen (EP) or discharged (hospital)
Secure Messaging – from 5% to attestation that function enabled
These proposals are controversial and especially subject to revision after comments evaluated

11
Public Health changes
“Active engagement” vs. “ongoing submission” - Completed Registration to Submit Data:, Testing and Validation, or Production
Modified consolidated objective & five/six measures per Stage 3 NPRM
• EPs: 2/5 measures (Stage 1 – 1/5) and EH: 3/6 measures (Stage 2 – 2/5)
• Bidirectional exchange required for immunization registries but not included in 2014 edition certification – will be an issue for comment/clarification
• Exclusions and one registry can meet multiple measures
• New measures – Case Reporting (2015 edition cert), Public Health Registry split from “Specialized Registry” and includes Cancer Registry, Clinical Data Registry split from “Specialized Registry”, Electronic Reportable Laboratory Result Reporting (Hospitals only)

12
Public Health measures
Source: Federal Register / /Vol. 80, No. 72 /Wednesday, April 15, 2015 / Proposed Rules

13
Attestation and payment adjustments
Cannot attest before January 1, 2016
Deadline – February 29 (2015) and February 28 (2016)
Hospitals – any 90 days between 10/1/2014 and 12/31/2015
EPs – any 90 days between 1/1/2015 and 12/31/2015
For 2015, 7/1 (hospital) & 10/1 (EP) Stage 1, Year 1 attestation deadlines to avoid 2015 penalties not feasible; penalties reversed retroactively

14
Medicaid
No major changes
Alternate attestation option using CMS portal for Medicaid providers seeking to demonstrate meaningful use to avoid Medicare payment adjustment and who are prohibited from switching between Medicare and Medicaid EHR incentive programs.

Questions?
15