cognitive impairment in parkinson’s disease vanessa k. hinson, md, phd medical university of south...
TRANSCRIPT

Cognitive Impairment Cognitive Impairment in Parkinson’s Diseasein Parkinson’s Disease
Vanessa K. Hinson, MD, PhDVanessa K. Hinson, MD, PhD
Medical University of South CarolinaMedical University of South Carolina

PD: “More than a Movement PD: “More than a Movement Disorder”Disorder”
Non-motor symptoms often precede the Non-motor symptoms often precede the development of motor-symptomsdevelopment of motor-symptoms Olfactory dysfunction, constipation, Olfactory dysfunction, constipation,
depression, sleep disordersdepression, sleep disorders Early PD stages spare dopaminergic Early PD stages spare dopaminergic
nucleinuclei Late stage development of levodopa Late stage development of levodopa
refractory symptomsrefractory symptoms

Braak Stages of PDBraak Stages of PD
Stage IStage I Olfactory bulbOlfactory bulb
Nuclei IX and X in medullaNuclei IX and X in medulla Stage IIStage II Intermediate reticular zone, Intermediate reticular zone,
lower raphe, coeruleus-complex lower raphe, coeruleus-complex Stage IIIStage III Substantia Substantia
nigra,amygdala,hippocampusnigra,amygdala,hippocampus Stage IVStage IV Temporal mesocortex and Temporal mesocortex and
allocortexallocortex Stages V,VIStages V,VI High order sensory High order sensory
association areas of neocortex association areas of neocortex and prefrontal cortex.and prefrontal cortex.
Non-motor signs
Cognition,emotion
Braak H et al. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging 2003
Motor signs
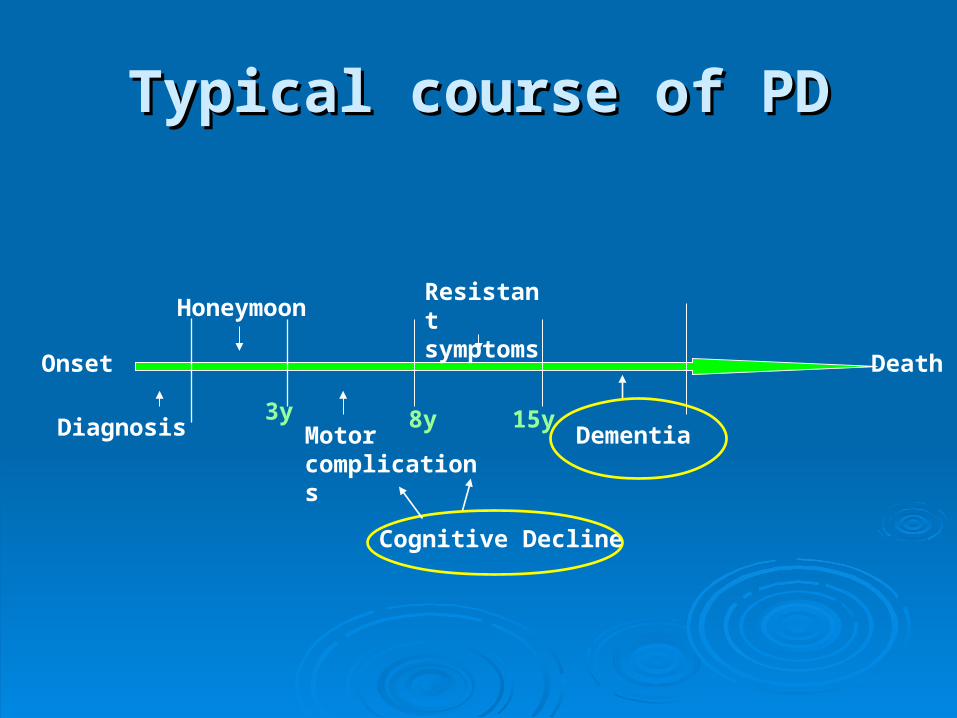
Typical course of PDTypical course of PD
Onset
Death
Diagnosis
Honeymoon
Motor complications
Resistant symptoms
Dementia
3y 8y 15y
Cognitive Decline

Non-Motor Symptoms in PDNon-Motor Symptoms in PD
DementiaDementia DepressionDepression AnxietyAnxiety HallucinationsHallucinations PainPain
DysphagiaDysphagia DroolingDrooling ConstipationConstipation Sleep problemsSleep problems Communication Communication
DisordersDisorders

SymptomsSymptoms Median Median frequencyfrequency
%rated symptom %rated symptom moderate or moderate or severesevere
Difficulty eatingDifficulty eating 33 7272
Difficulty Difficulty communicatingcommunicating
33 7979
Physical discomfortPhysical discomfort 33 7070
ConfusionConfusion 33 6868
DepressionDepression 33 6060
InsomniaInsomnia 22 4747
Shortness of breathShortness of breath 22 4040
ChokingChoking 22 4747
AnxietyAnxiety 22 6060
1=never, 2= a few times, 3= frequently, 4=almost all the time, 5=constantly
Goy ER, Carter JH, Ganzini L. Parkinson’s Disease at the End of Life: Caregiver Perspectives. Neurology 2007;69:611-12.

Impact of PD symptoms on Impact of PD symptoms on Quality of Life Quality of Life
Survey amongst 228 patients with > 5 year Survey amongst 228 patients with > 5 year disease durationdisease duration
Non-motor symptoms were rated to have Non-motor symptoms were rated to have greater impact on quality of life than motor greater impact on quality of life than motor symptoms symptoms
PD end-of-life caregiver survey confirms PD end-of-life caregiver survey confirms impact of non-motor symptomsimpact of non-motor symptoms
Non-motor symptoms impact risk for nursing Non-motor symptoms impact risk for nursing home placement and mortalityhome placement and mortality
PD nursing home follow-up PD nursing home follow-up studystudy
55% of nursing home patients had died on 55% of nursing home patients had died on follow-up follow-up 1 1 (mean, 40.2 m after data collection)(mean, 40.2 m after data collection)
Compared to 14% of those in the Compared to 14% of those in the communitycommunity
All living patients remained permanently in All living patients remained permanently in the nursing homethe nursing home
1: Goetz CG, Stebbins GT. Risk factors for nursing home placement in advanced Parkinson’s disease. Neurology 1993
Dementia in PDDementia in PD
~ 40% of patients~ 40% of patients More common in late-onset PD (>70 y)More common in late-onset PD (>70 y) Onset after years of PD motor symptomsOnset after years of PD motor symptoms Important risk factor for more rapidly Important risk factor for more rapidly
worsening disability and reduced survivalworsening disability and reduced survival

Dementia and PD mortalityDementia and PD mortality
Louis et al.Louis et al.11 showed mortality in PD 1.6 > showed mortality in PD 1.6 > than non-demented elderly subjectsthan non-demented elderly subjects
Those with PD and dementia had mortality Those with PD and dementia had mortality risk ratio of 4.9risk ratio of 4.9
1: Louis E, Marder K, Cote L, et al. Mortality From Parkinson’s Disease. Arch Neurol 1997

PD dementiaPD dementiaClinical featuresClinical features
““Subcortical dementia”Subcortical dementia” Executive dysfunctionExecutive dysfunction Difficulties with planning, sequencing, Difficulties with planning, sequencing,
complex goal-directed behaviorcomplex goal-directed behavior Impaired attention and concentrationImpaired attention and concentration Decreased processing speedDecreased processing speed Problems with free recall, help from Problems with free recall, help from
external cuingexternal cuing
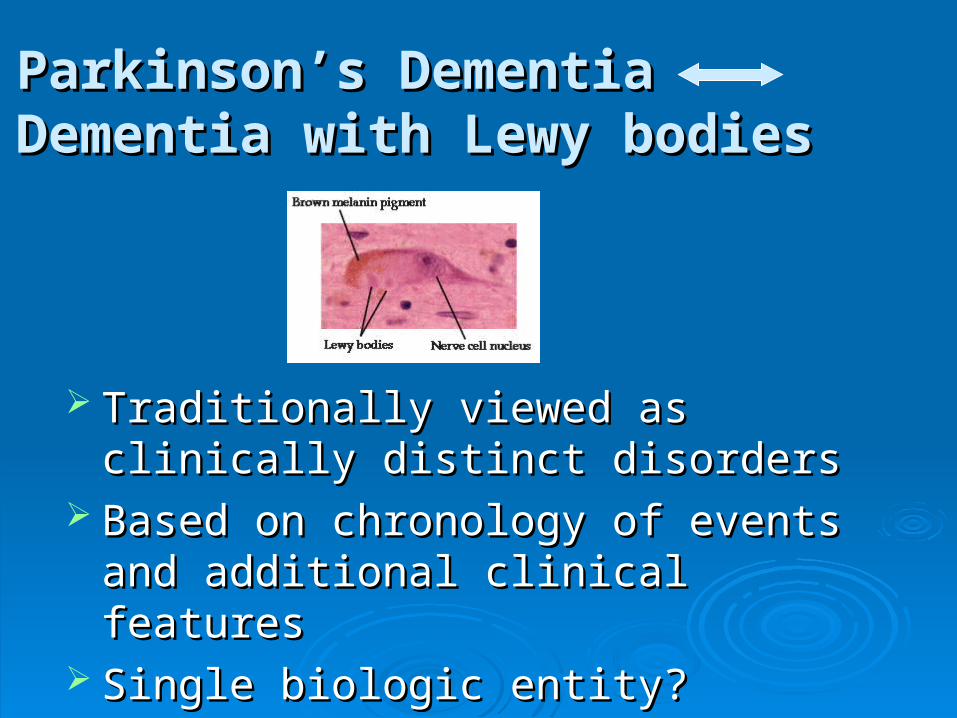
Parkinson’s DementiaParkinson’s DementiaDementia with Lewy bodiesDementia with Lewy bodies
Traditionally viewed as clinically distinct Traditionally viewed as clinically distinct disordersdisorders
Based on chronology of events and Based on chronology of events and additional clinical features additional clinical features
Single biologic entity? SynucleinopathySingle biologic entity? Synucleinopathy

Clinical DistinctionClinical DistinctionPDDPDD DLBDLB
> 1 year history of > 1 year history of motor symptoms motor symptoms before onset of before onset of dementiadementia**
Visual hallucinations Visual hallucinations late phenomenonlate phenomenon
Dysautonomia mildDysautonomia mild
< 1 year history of < 1 year history of motor symptoms motor symptoms before onset of before onset of dementia dementia **
Visual hallucinations Visual hallucinations earlyearly
Dysautonomia Dysautonomia prominent prominent
* McKeith criteria* McKeith criteria

Can MRI make the difference?Can MRI make the difference? VBM study Meyer et al. Neurology 2007VBM study Meyer et al. Neurology 2007 DLB compared to PDD:DLB compared to PDD: Greater temporal, parietal and occipital Greater temporal, parietal and occipital
atrophyatrophy
Neuropathological differencesNeuropathological differences
Ballard et al. (Neurology 2006): 57 Ballard et al. (Neurology 2006): 57 prospectively assessed patients with DLB prospectively assessed patients with DLB or PDDor PDD
Confirmed at autopsyConfirmed at autopsy PDD:PDD: threefold reduction in frequency of threefold reduction in frequency of
abundant plaquesabundant plaques 20% less cortical synuclein pathology20% less cortical synuclein pathology 30% greater cholinergic deficit30% greater cholinergic deficit

PDD/DLB conclusionPDD/DLB conclusion
Key substrates are the sameKey substrates are the same Differences in cortical pathologic lesions Differences in cortical pathologic lesions
and neurochemical deficitsand neurochemical deficits DLB/PDD Working Group:DLB/PDD Working Group:
Single biologic entity (synucleinopathy) for Single biologic entity (synucleinopathy) for research purposes targeting basic molecular research purposes targeting basic molecular processesprocesses
Distinction retained for clinical practice and Distinction retained for clinical practice and treatmenttreatment

Risk factors for PD DementiaRisk factors for PD Dementia
Advanced age at onset of motor Advanced age at onset of motor symptomssymptoms
Early occurrence of levodopa related Early occurrence of levodopa related confusion or psychosisconfusion or psychosis
Presence of speech and axial involvementPresence of speech and axial involvement DepressionDepression REM sleep behavior disorderREM sleep behavior disorder
Neurochemical deficitsNeurochemical deficitsDopaminergic deficit?Dopaminergic deficit?
Cognitive dysfunction correlates strongly with Cognitive dysfunction correlates strongly with non-levodopa responsive motor symptomsnon-levodopa responsive motor symptoms
Levodopa dose not reverse cognitive Levodopa dose not reverse cognitive dysfunctiondysfunction
No correlation between cell loss in substantia No correlation between cell loss in substantia nigra and dementianigra and dementia
Suggestive mainly of involvement of non-Suggestive mainly of involvement of non-dopaminergic systemsdopaminergic systems
In neocortical areas however: decrease in In neocortical areas however: decrease in dopamine correlates with dementiadopamine correlates with dementia

Neurochemical deficitsNeurochemical deficitsNoradrenergic/serotinergic Noradrenergic/serotinergic
pathways?pathways? Locus coeruleus damaged in PDLocus coeruleus damaged in PD Neuronal loss and norepinephrine depletion Neuronal loss and norepinephrine depletion
more severe in PDDmore severe in PDD Pilot data on Pilot data on αα1 and 1 and αα2 agonists improving 2 agonists improving
attention and spatial memoryattention and spatial memory** Serotinergic deficit and cell loss in raphe nucleus Serotinergic deficit and cell loss in raphe nucleus
has been described, but so far no correlated with has been described, but so far no correlated with dementiadementia
*Riekkinen et al Neuroscience 1999, Bedard et al. Clin neuropharm 1998

Neurochemical deficitsNeurochemical deficitsCholinergic deficit?Cholinergic deficit?
Severe cellular loss in nucleus basalis of Severe cellular loss in nucleus basalis of MeynertMeynert
Decrease in cholinergic innervation of the Decrease in cholinergic innervation of the cerebral cortexcerebral cortex
These deficits are correlated with These deficits are correlated with dementia dementia
PDD>DLB>ADPDD>DLB>AD Does this predict clinical response to Does this predict clinical response to
cholinergic therapy?cholinergic therapy?

Unifying hypothesisUnifying hypothesis
Dopaminergic deficit:Dopaminergic deficit: dysexecutive dysexecutive syndromesyndrome
Cholinergic deficit:Cholinergic deficit: memory, frontal memory, frontal lobe dysfunctionlobe dysfunction
Noradrenergic deficit:Noradrenergic deficit: impaired impaired attentionattention
Serotinergic deficit:Serotinergic deficit: depressiondepression
Treatment implications?
Treatment (Donezepil)Treatment (Donezepil)Ravina et al. JNNP 2005;76:934-939Ravina et al. JNNP 2005;76:934-939
Randomized double blind, placebo Randomized double blind, placebo controlled, crossover study in 22 subjects controlled, crossover study in 22 subjects with PDD. with PDD.
Donepezil was well tolerated and did not Donepezil was well tolerated and did not worsen PD.worsen PD.
There was a modest (not stat. sign.) There was a modest (not stat. sign.) benefit on aspects of cognitive function. benefit on aspects of cognitive function.

Treatment (Donezepil)Treatment (Donezepil)Aarsland et al.: JNNP 2002;72:708-712Aarsland et al.: JNNP 2002;72:708-712
Double blind, randomized, placebo Double blind, randomized, placebo controlled, crossover study in 14 patients controlled, crossover study in 14 patients with PD and cognitive impairmentwith PD and cognitive impairment
Donezepil: Mean MMSE score improved Donezepil: Mean MMSE score improved by 2.1 (SD 2.7) points (baseline/week 10)by 2.1 (SD 2.7) points (baseline/week 10)
Placebo: 0.3 (SD 3.2) point difference. Placebo: 0.3 (SD 3.2) point difference. Significant effect of donepezil on the Significant effect of donepezil on the
MMSE score compared with placebo MMSE score compared with placebo (p=0.013). (p=0.013).

Dementia in PDDementia in PDTreatmentTreatment
Cholinesterase inhibitors have been Cholinesterase inhibitors have been studied in randomized clinical trialsstudied in randomized clinical trials
Generally considered safeGenerally considered safe May exacerbate tremor May exacerbate tremor Modest efficacyModest efficacy Role of memantine uncertainRole of memantine uncertain

Neuroimaging correlatesNeuroimaging correlates
Conventional structural MRI: minimal or no Conventional structural MRI: minimal or no cortical or hippocampal atrophycortical or hippocampal atrophy
Some studies have shown increased Some studies have shown increased incidence of small vessel ischemic diseaseincidence of small vessel ischemic disease
Voxel based morphometry: automated, Voxel based morphometry: automated, unbiased method for voxel-wise unbiased method for voxel-wise comparison of high resolution MRI datacomparison of high resolution MRI data

Copyright ©2007 BMJ Publishing Group Ltd.
Beyer, M. K et al. J Neurol Neurosurg Psychiatry 2007;78:254-259
Figure: Areas of reduced grey matter in PD MCI compared with PD
Significant changes are found in the (A) left superior temporal gyrus, (B) left frontal lobe (precentral gyrus) and (C) right temporal lobe (inferior temporal
gyrus) and left temporal lobe (superior temporal gyrus) at p< 0.001.

Functional Neuroimaging Functional Neuroimaging
PET to study abnormal functional PET to study abnormal functional connectivityconnectivity
PD at rest: increased pallidothalamic and PD at rest: increased pallidothalamic and pontine activity, reduced activity in cortical pontine activity, reduced activity in cortical motor and association regionsmotor and association regions**
This network can be modulated by This network can be modulated by therapeutic interventions such as DBStherapeutic interventions such as DBS
* Eckert et. Al. Lancet Neurology 2007.

Parkinson’s Disease related cognitive pattern. A:PET. B: Correlation PDCP expression/CVLT. C: PDCP/MCI. D: PDCP expression over time (Eckert et al., Lancet Neurol 2007)

Diffuse Lewy bodies
Senile plaques, neurofibrillary tangles
Vascular disease
Pathology in PD dementia
Vascular Disease and PDDVascular Disease and PDDRole of homocysteineRole of homocysteine

Elevated Homocysteine in PD pts treated Elevated Homocysteine in PD pts treated with levodopawith levodopa
KuhnKuhn
20012001
54/13254/132 13.113.1 17.317.3
Rogers Rogers
20032003
32/20532/205 12.212.2 16.116.1
YasuiYasui
20002000
50/9050/90 10.210.2 16.316.3
Blandini Blandini
20012001
31/3031/30 10.810.8 16.916.9
Cts/pts Hcy/cts Hcy/pts

Homocysteine metabolism and Homocysteine metabolism and effects of levodopaeffects of levodopa
SAM= S-Adenosylmethionine. SAH= S-Adenosylhomocysteine. MTHFR: SAM= S-Adenosylmethionine. SAH= S-Adenosylhomocysteine. MTHFR: Methylenetetrahydrofolate reductase. CBS= Cystathionine betasynthase. Methylenetetrahydrofolate reductase. CBS= Cystathionine betasynthase. Vitamin cofactors in parenthesis.Vitamin cofactors in parenthesis.

HomocysteineHomocysteine
Risk factor for vascular disease and Risk factor for vascular disease and dementia dementia
Potential neurotoxic effectsPotential neurotoxic effects Hcy could adversely affect cognition in PD Hcy could adversely affect cognition in PD
through vascular and neurotoxic effectsthrough vascular and neurotoxic effects
Vascular effects of homocysteineVascular effects of homocysteine
Enhanced carotid atherosclerosis in PD, Enhanced carotid atherosclerosis in PD, correlation of severity of atherosclerosis correlation of severity of atherosclerosis with duration of levodopa treatment and with duration of levodopa treatment and degree of Hcy elevation (Nakaso et al.)degree of Hcy elevation (Nakaso et al.)
Alteration of LDL receptors, enhanced Alteration of LDL receptors, enhanced rate of plaque formation, proliferation of rate of plaque formation, proliferation of vascular smooth muscle and impaired vascular smooth muscle and impaired endothelial activity. endothelial activity.
Silent brain infarcts and white matter Silent brain infarcts and white matter hyperintensities have been linked to hyperintensities have been linked to elevations in Hcy. elevations in Hcy.

Vascular effects of homocysteineVascular effects of homocysteine
Rotterdam Scan Study: Hcy is independent risk Rotterdam Scan Study: Hcy is independent risk factor for the presence of silent brain infarcts factor for the presence of silent brain infarcts and white matter lesions. Highest Hcy group: 3 and white matter lesions. Highest Hcy group: 3 times the risk for small vessel disease compared times the risk for small vessel disease compared to the lowest quintile. to the lowest quintile.
Neuropathological study of 13 cases of PDD: Neuropathological study of 13 cases of PDD: presence of large and small vessel ischemic presence of large and small vessel ischemic disease in all patients (disease in all patients (ApaydinApaydin et al.). et al.).
Increase in white matter intensities on MRI in Increase in white matter intensities on MRI in PDD compared to PD (Beyer et al.). PDD compared to PD (Beyer et al.).

Neurotoxic effects of Neurotoxic effects of homocysteinehomocysteine
Oxidative injuryOxidative injury Impaired DNA-repairImpaired DNA-repair NMDA-mediated excitotoxic effectsNMDA-mediated excitotoxic effects Interaction with inflammatory Interaction with inflammatory
mechanisms mechanisms

Clinical data on Hcy and PDClinical data on Hcy and PD
Rogers: Hcy elevation correlated with Rogers: Hcy elevation correlated with presence of CAD in PD patientspresence of CAD in PD patients
O’Suilleabhain: study of Hcy levels, O’Suilleabhain: study of Hcy levels, cognition, mood, and motor function in 97 cognition, mood, and motor function in 97 subjects with PD.subjects with PD. Hyperhomocysteinemia was correlated with Hyperhomocysteinemia was correlated with
worse cognition and mood, but motor function worse cognition and mood, but motor function unaffected. unaffected.

Potential treatment of Potential treatment of hyperhomocysteinemiahyperhomocysteinemia
Vitamin supplementationVitamin supplementation COMT inhibitors (entacapone, tolcapone)COMT inhibitors (entacapone, tolcapone)

SummarySummary
PD dementia is common and clinically distinct PD dementia is common and clinically distinct from DLBfrom DLB
Impacts quality of life and mortalityImpacts quality of life and mortality Cholinergic deficitCholinergic deficit Lewy body/AD/vascular pathologyLewy body/AD/vascular pathology Role of levodopa induced Role of levodopa induced
hyperhomocysteinemia?hyperhomocysteinemia? Research emphasizes the non-dopaminergic Research emphasizes the non-dopaminergic
features of PD including PD dementiafeatures of PD including PD dementia Antisyncuclein therapiesAntisyncuclein therapies