colorectal cancer and hereditary colon cancer syndromes carol … · • understand the diagnostic...
TRANSCRIPT
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
1The screen versions of these slides have full details of copyright and acknowledgements
Carol A. Burke, M.D., FACG, FACP
Colorectal Cancer and Hereditary Colon Cancer Syndromes
1
Sanford R. Weiss MD Center for Hereditary Colorectal Neoplasia
Digestive Disease Institute
Cleveland Clinic, Cleveland, Ohio
Objectives
• Review the molecular and genetic basis of sporadic colorectal cancer (CRC)
• Identify the precursor lesions of CRC
2
• Understand the diagnostic features of the hereditary colorectal cancer syndromes
• Development management strategies for your patients with the hereditary cancer syndromes
Colorectal cancer precursors
3
70% Adenomatous Lesions
Chromosomal Instability (CIN) Microsatellite Stable (MSS)
30%Serrated LesionBRAF mutation
CpG Island Methylation (CIMP) Microsatellite Instability (MSI) or MSS
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
2The screen versions of these slides have full details of copyright and acknowledgements
Classification of colorectal polypsAdenomatous Lesions Serrated Lesions
• Tubular
• Tubulovillous
• Villous
• Hyperplastic Polyp– Microvesicular (MVHP)
– Goblet Cell (GCHP)
– Mucin Poor (MPHP)
4
• Sessile Serrated Adenoma/Polyp (SSP/A)– With cytological dysplasia
– Without cytologic dysplasia
• Traditional Serrated Adenoma (TSA)– With conventional dysplasia
– Without conventiona ldysplasia
WHO 2010
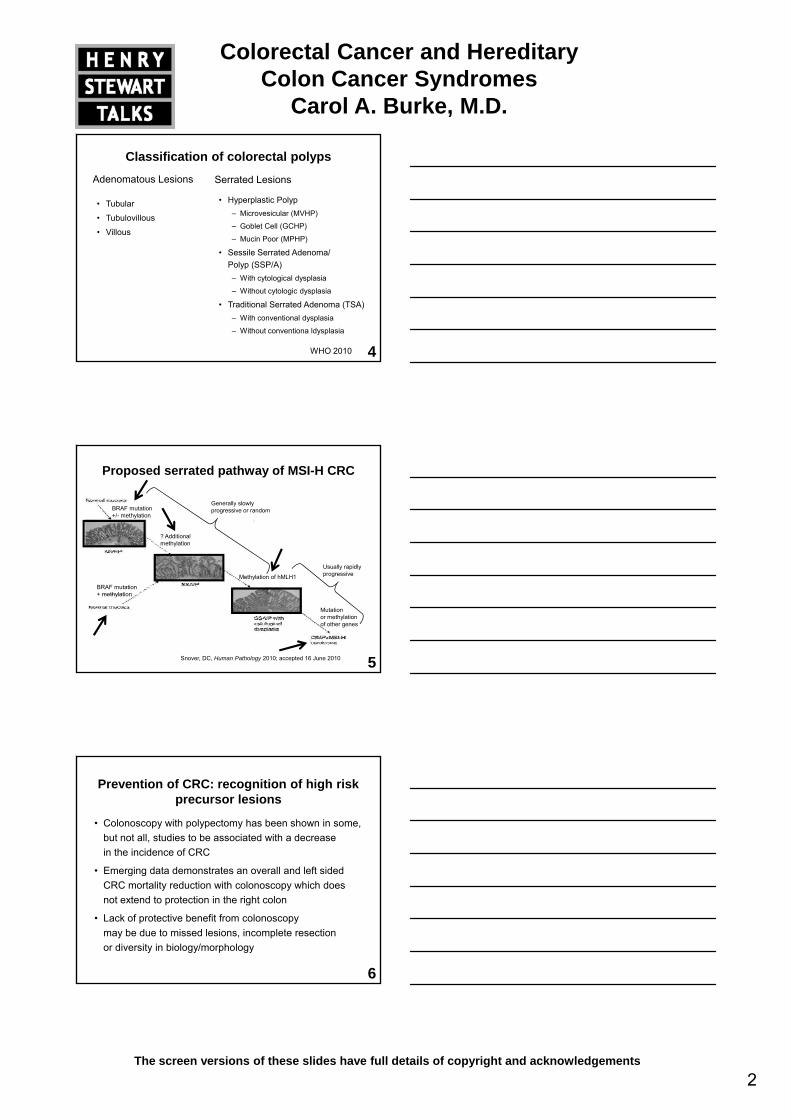
Proposed serrated pathway of MSI-H CRC
BRAF mutation+/- methylation
? Additional methylation
Generally slowly progressive or random
5Snover, DC, Human Pathology 2010; accepted 16 June 2010
BRAF mutation+ methylation
Methylation of hMLH1
Usually rapidly progressive
Mutation or methylation of other genes
• Colonoscopy with polypectomy has been shown in some, but not all, studies to be associated with a decrease in the incidence of CRC
• Emerging data demonstrates an overall and left sided
Prevention of CRC: recognition of high risk precursor lesions
6
• Emerging data demonstrates an overall and left sided CRC mortality reduction with colonoscopy which does not extend to protection in the right colon
• Lack of protective benefit from colonoscopy may be due to missed lesions, incomplete resection or diversity in biology/morphology
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
3The screen versions of these slides have full details of copyright and acknowledgements
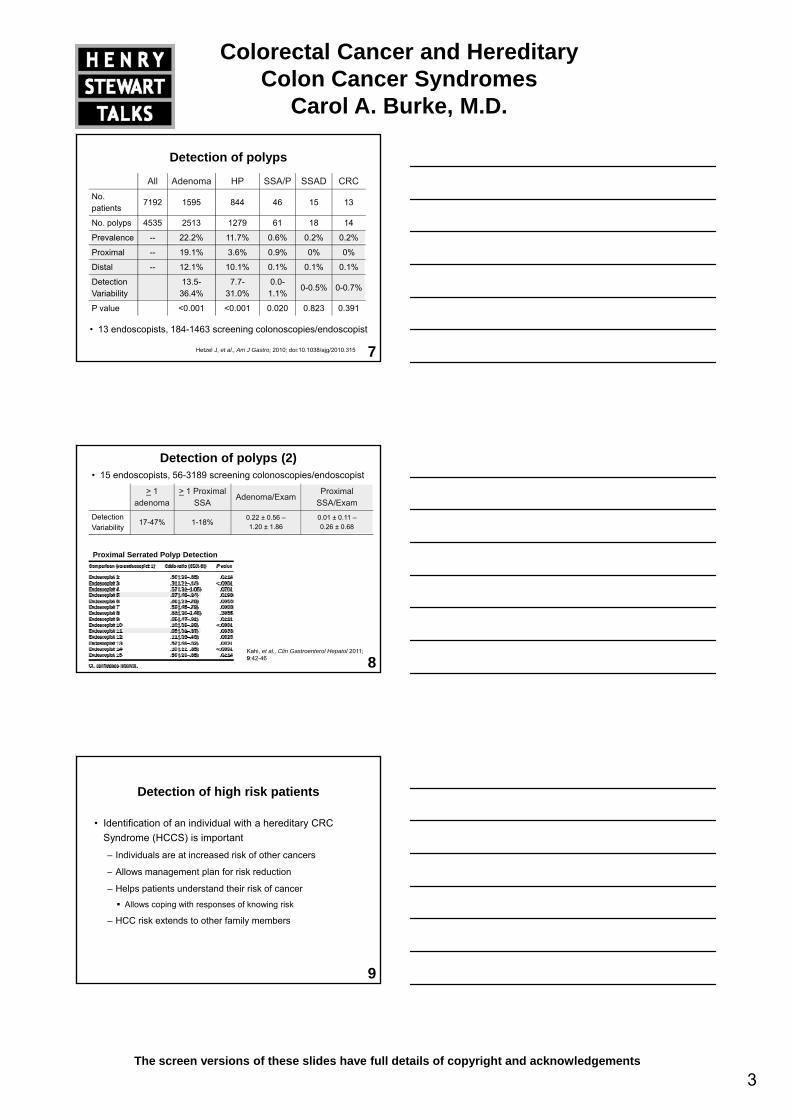
Detection of polyps
All Adenoma HP SSA/P SSAD CRCNo. patients
7192 1595 844 46 15 13
No. polyps 4535 2513 1279 61 18 14
Prevalence -- 22.2% 11.7% 0.6% 0.2% 0.2%
7
Proximal -- 19.1% 3.6% 0.9% 0% 0%
Distal -- 12.1% 10.1% 0.1% 0.1% 0.1%
DetectionVariability
13.5-36.4%
7.7-31.0%
0.0-1.1%
0-0.5% 0-0.7%
P value <0.001 <0.001 0.020 0.823 0.391
• 13 endoscopists, 184-1463 screening colonoscopies/endoscopist
Hetzel J, et al., Am J Gastro; 2010; doi:10.1038/ajg/2010.315
Detection of polyps (2)
> 1 adenoma
> 1 Proximal SSA
Adenoma/ExamProximal
SSA/ExamDetection Variability
17-47% 1-18% 0.22 ± 0.56 –1.20 ± 1.86
0.01 ± 0.11 –0.26 ± 0.68
Adenoma and proximal serrated polyp detection rates were strongly correlated, expressed as proportion of colonoscopies with at least 1 adenoma or proximal serrated polyp (Pearson correlation coefficient .86, P .0001)
• 15 endoscopists, 56-3189 screening colonoscopies/endoscopist
Proximal Serrated Polyp Detection
8Kahi, et al., Clin Gastroenterol Hepatol 2011; 9:42-46
Detection of high risk patients
• Identification of an individual with a hereditary CRC Syndrome (HCCS) is important
– Individuals are at increased risk of other cancers
All t l f i k d ti
9
– Allows management plan for risk reduction
– Helps patients understand their risk of cancer
Allows coping with responses of knowing risk
– HCC risk extends to other family members
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
4The screen versions of these slides have full details of copyright and acknowledgements
Hereditary colon cancer syndromes
• Rare
– < 10% of the new cases of colorectal cancer
• Diagnostic Clues:
10
– Early onset of colorectal neoplasia (< 50 years)
– Excessive number of polyps or multiple primary cancers
– Extracolonic benign or malignant tumors
– Multiple relatives, generations affected
Hereditary polyposis syndromes
Autosomal Dominant Autosomal Recessive
• Familial Adenomatous Polyposis (FAP)
Attenuated FAP (aFAP)
• MYH associated Polyposis (MAP)
11
– Attenuated FAP (aFAP)
• Peutz-Jeghers Syndrome (PJS)
• Juvenile Polyposis Syndrome (JPS)
• Cowden Syndrome - PTEN Hamartoma Tumor Syndrome
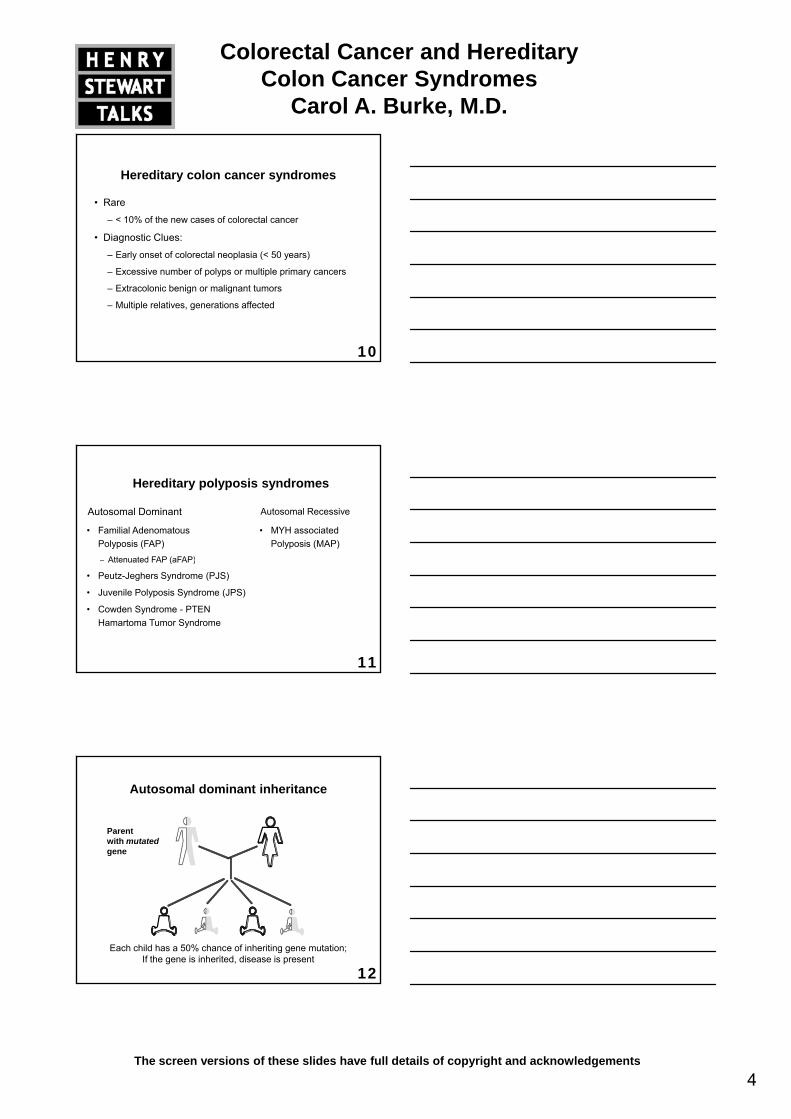
Parent with mutated gene
Autosomal dominant inheritance
12
Each child has a 50% chance of inheriting gene mutation;If the gene is inherited, disease is present
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
5The screen versions of these slides have full details of copyright and acknowledgements
Parent is carrier with MYH gene mutation
Parent is carrier with MYH gene mutation
Autosomal recessive inheritance (MAP)
13
Each child has a 25% chance of inheriting both MYH gene mutations (affected), a 50% chance of inheriting at least one MYH gene mutation,
and a 25% chance of inheriting no MYH gene mutations
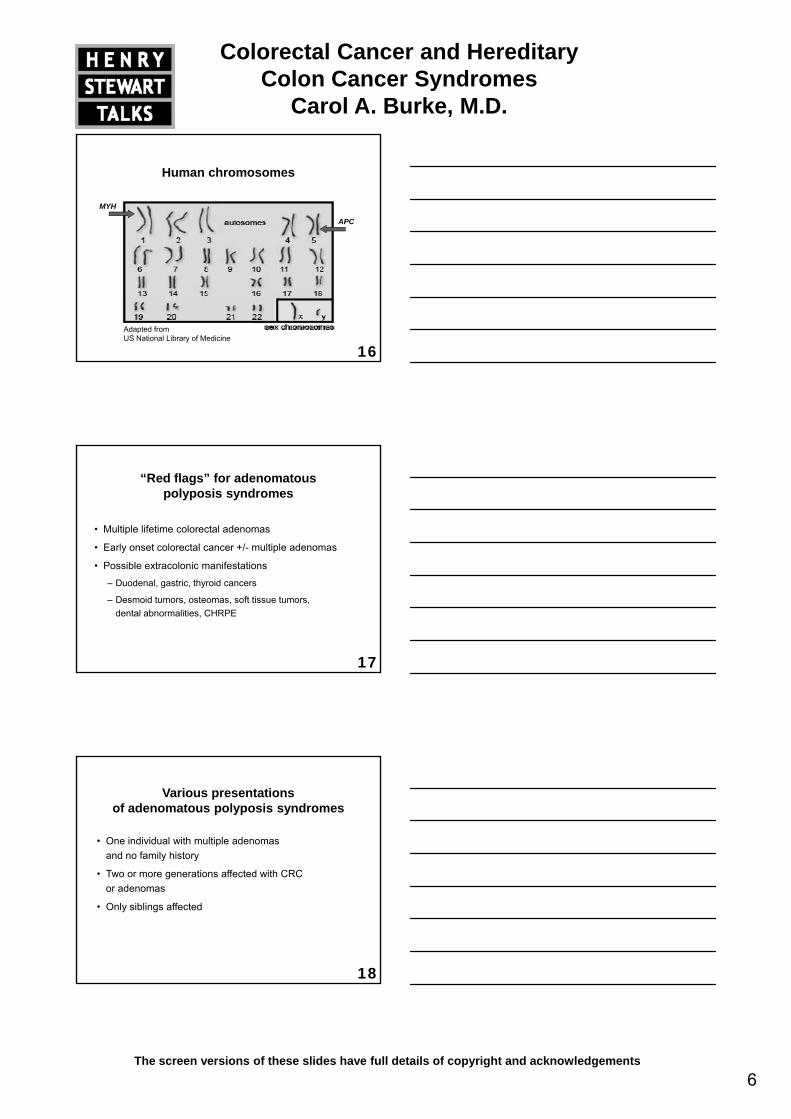
Hereditary polyposis syndromes
Syndrome Polyp Type Gene MutationFAP and attenuated FAP Adenomatous APC
MYH Associated Polyposis Adenomatous MYH
14
Peutz-Jeghers Syndrome Hamartomatous STK11 (aka LKB1)
Juvenile Polyposis Syndrome Hamartomatous SMAD4 or BMPR1A
Cowden Syndrome Hamartomatous PTEN
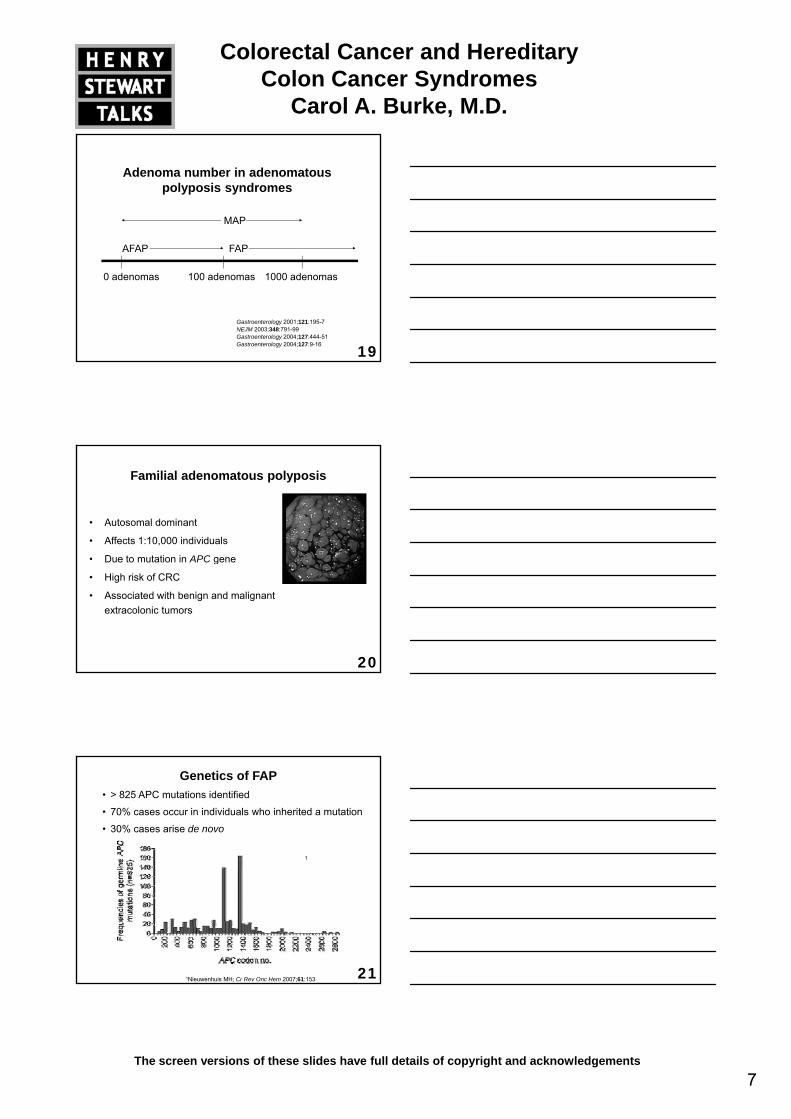
Adenomatous polyposis syndromes
15
MAP FAP/AFAP
The majority of genotypedadenomatous polyposissyndromes are caused by mutations in either APCor MYH genes
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
6The screen versions of these slides have full details of copyright and acknowledgements
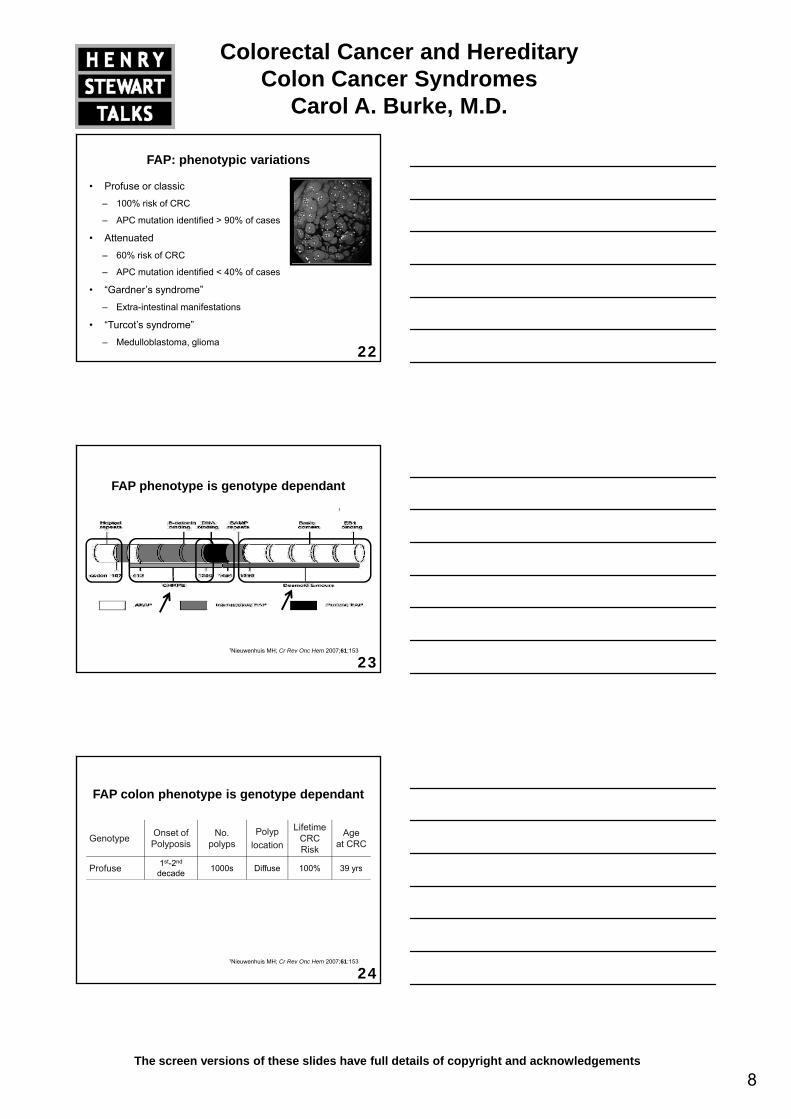
Human chromosomes
APC
MYH
16Adapted fromUS National Library of Medicine
“Red flags” for adenomatous polyposis syndromes
• Multiple lifetime colorectal adenomas
• Early onset colorectal cancer +/- multiple adenomas
17
• Possible extracolonic manifestations
– Duodenal, gastric, thyroid cancers
– Desmoid tumors, osteomas, soft tissue tumors, dental abnormalities, CHRPE
Various presentations of adenomatous polyposis syndromes
• One individual with multiple adenomas and no family history
ff C C
18
• Two or more generations affected with CRC or adenomas
• Only siblings affected
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
7The screen versions of these slides have full details of copyright and acknowledgements
FAPAFAP
MAP
Adenoma number in adenomatous polyposis syndromes
19
0 adenomas 100 adenomas 1000 adenomas
FAPAFAP
Gastroenterology 2001;121:195-7NEJM 2003;348:791-99Gastroenterology 2004;127:444-51Gastroenterology 2004;127:9-16
Familial adenomatous polyposis
• Autosomal dominant
• Affects 1:10,000 individuals
• Due to mutation in APC gene
20
• Due to mutation in APC gene
• High risk of CRC
• Associated with benign and malignant extracolonic tumors
Genetics of FAP• > 825 APC mutations identified
• 70% cases occur in individuals who inherited a mutation
• 30% cases arise de novo
1
211Nieuwenhuis MH; Cr Rev Onc Hem 2007;61:153
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
8The screen versions of these slides have full details of copyright and acknowledgements
FAP: phenotypic variations
• Profuse or classic
– 100% risk of CRC
– APC mutation identified > 90% of cases
• Attenuated
22
– 60% risk of CRC
– APC mutation identified < 40% of cases
• “Gardner’s syndrome”
– Extra-intestinal manifestations
• “Turcot’s syndrome”
– Medulloblastoma, glioma
FAP phenotype is genotype dependant1
231Nieuwenhuis MH; Cr Rev Onc Hem 2007;61:153
FAP colon phenotype is genotype dependant
Genotype Onset of Polyposis
No. polyps
Polyp location
Lifetime CRC Risk
Age at CRC
Profuse 1st-2nd1000s Diffuse 100% 39 yrs
24
Profuse decade 1000s Diffuse 100% 39 yrs
Intermediate 2nd-3rd
decade100s-1000s Diffuse 60-100% > 39 yrs
Attenuated 4th-5th
decade < 100 Right 60% 56 yrs
1Nieuwenhuis MH; Cr Rev Onc Hem 2007;61:153

Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
9The screen versions of these slides have full details of copyright and acknowledgements
Extra-intestinal features of FAP
• Desmoid tumors (15%)
• Thyroid carcinoma (2-17%)
• Adrenal adenoma (7-13% )
• Osteomas (50-90%)
Courtesy J. Church MD
25
• Supernumerary teeth (11-27%)
• CHRPE (70-80%)
• Soft tissue tumors (50%)– Lipoma, fibroma,
sebaceous cysts
• Hepatoblastoma (<2%)
Vasen H; Gut 2008;57:704
Gastric features of FAP• Fundic gland polyposis
– Prevalence: 88%LGD: 41%, HGD: 3%: Only in polyps > 10 mm
• Gastric adenomas– Prevalence: 10%
Usually antrum
26
– Usually antrum
• Gastric cancer: rare– Arises from fundic gland polyposis
CHRPE
Bianchi L, Burke CA, et al., Clin Gastro Hep 2007;6:180
Duodenal features of FAP
• Duodenal adenomas: 100%
• Adenomatous papilla: >60%1
– 89% if appearance abnormal
27
– 54% if appearance normal
• Periampullary/Duodenal cancer: 2-36%2
– When occurs, all die of malignant disease
– Cancer risk based upon stage of duodenal polyposis
2Groves C, Gut 2002;50:6361Burke C, GIE 1999;49:358
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
10The screen versions of these slides have full details of copyright and acknowledgements
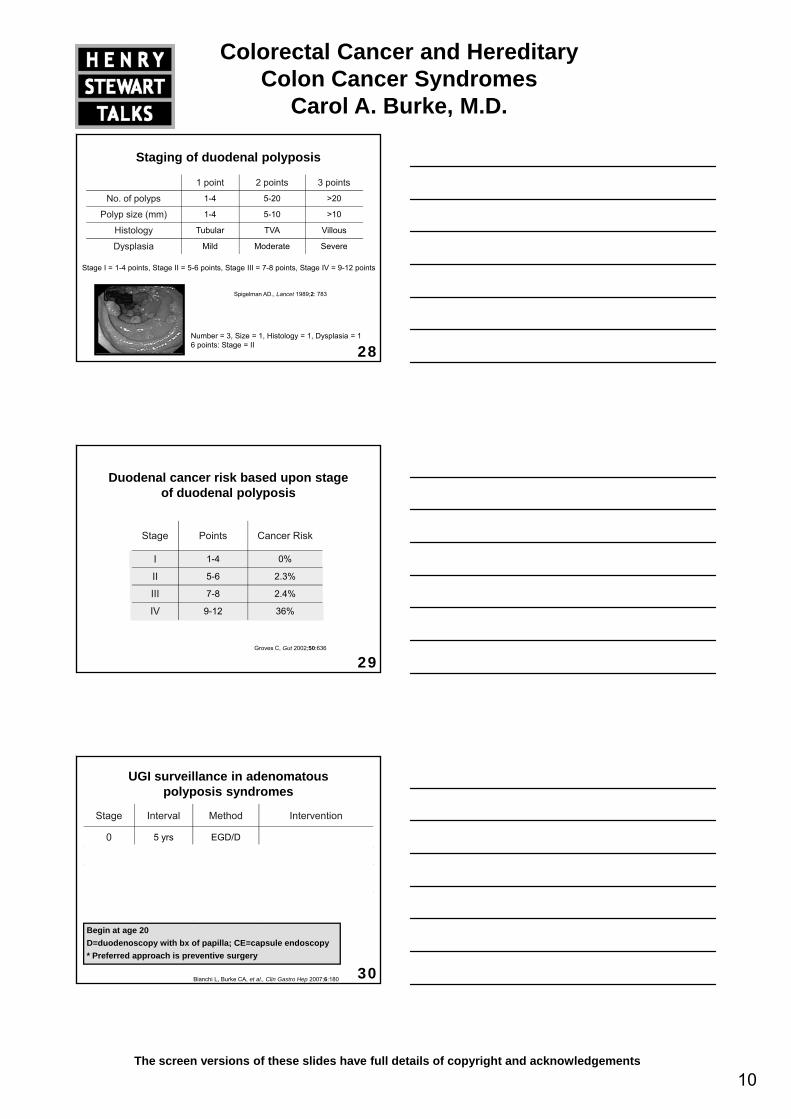
Staging of duodenal polyposis
1 point 2 points 3 points
No. of polyps 1-4 5-20 >20
Polyp size (mm) 1-4 5-10 >10
Histology Tubular TVA Villous
Dysplasia Mild Moderate Severe
28
Dysplasia Mild Moderate Severe
Spigelman AD., Lancet 1989;2: 783
Stage I = 1-4 points, Stage II = 5-6 points, Stage III = 7-8 points, Stage IV = 9-12 points
Number = 3, Size = 1, Histology = 1, Dysplasia = 16 points: Stage = II
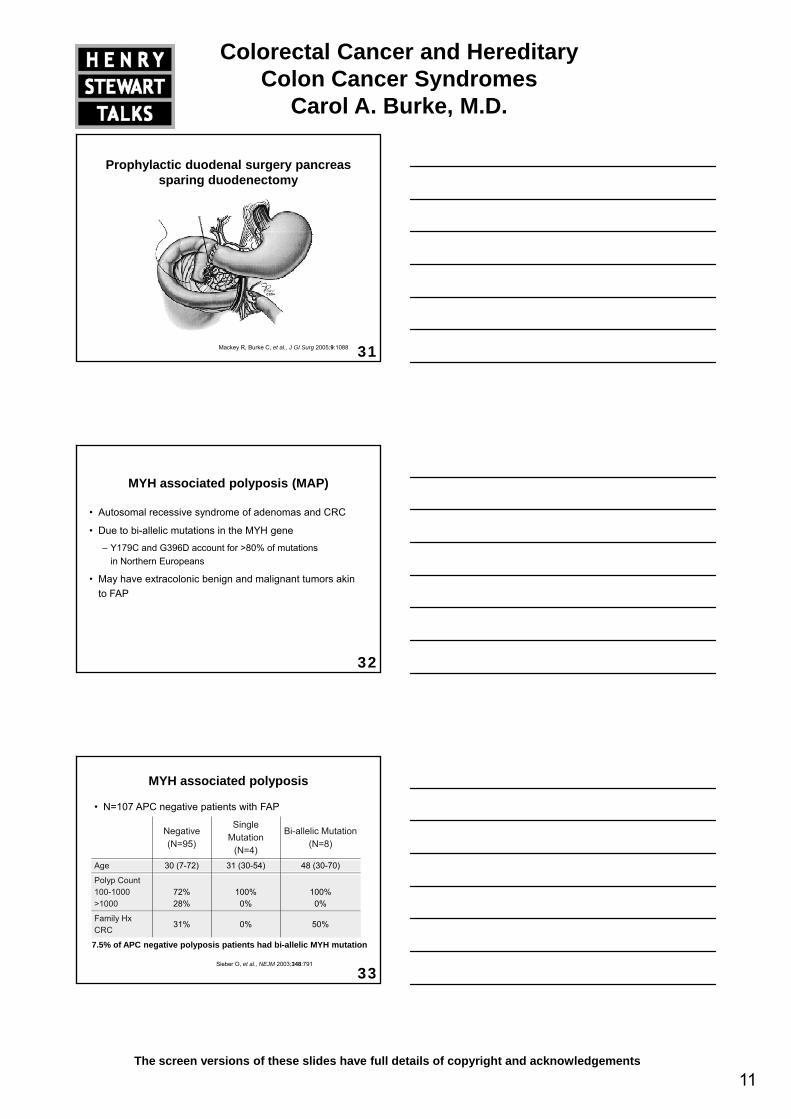
Duodenal cancer risk based upon stage of duodenal polyposis
Stage Points Cancer Risk
I 1 4 0%
29
I 1-4 0%
II 5-6 2.3%
III 7-8 2.4%
IV 9-12 36%
Groves C, Gut 2002;50:636
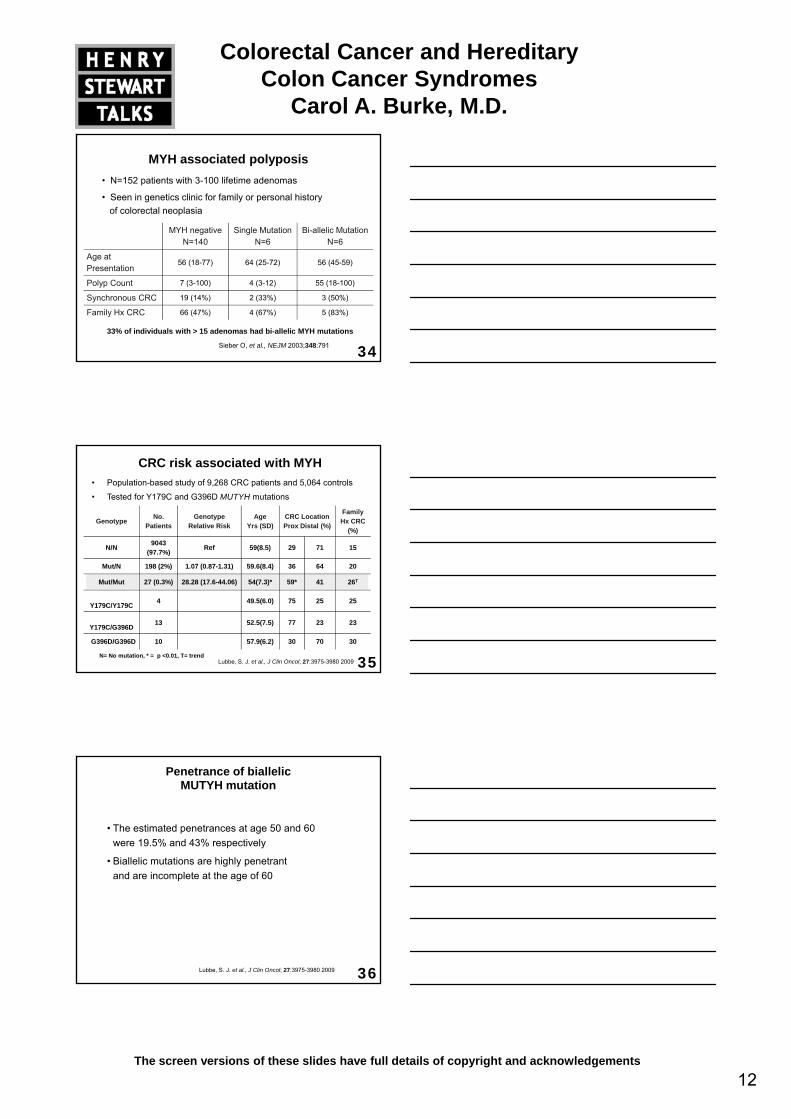
UGI surveillance in adenomatous polyposis syndromes
Stage Interval Method Intervention
0 5 yrs EGD/D
I-II 3 yrs EGD/D
1 EGD/D C l ib 400 BID/
30
III1 yr3 yrs
EGD/DCE
Celecoxib 400 BID/Polyp eradication
IV*6 mo3 yrs
EGD/DCE
Pancreas sparing duodenectomy
Bianchi L, Burke CA, et al., Clin Gastro Hep 2007;6:180
Begin at age 20D=duodenoscopy with bx of papilla; CE=capsule endoscopy* Preferred approach is preventive surgery
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
11The screen versions of these slides have full details of copyright and acknowledgements
Prophylactic duodenal surgery pancreas sparing duodenectomy
31Mackey R, Burke C, et al., J GI Surg 2005;9:1088
MYH associated polyposis (MAP)
• Autosomal recessive syndrome of adenomas and CRC
• Due to bi-allelic mutations in the MYH gene
– Y179C and G396D account for >80% of mutations i N th E
32
in Northern Europeans
• May have extracolonic benign and malignant tumors akin to FAP
MYH associated polyposis
• N=107 APC negative patients with FAP
Negative(N=95)
Single Mutation
(N=4)
Bi-allelic Mutation(N=8)
Age 30 (7-72) 31 (30-54) 48 (30-70)
33Sieber O, et al., NEJM 2003;348:791
g ( ) ( ) ( )
Polyp Count100-1000>1000
72%28%
100%0%
100%0%
Family Hx CRC
31% 0% 50%
7.5% of APC negative polyposis patients had bi-allelic MYH mutation
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
12The screen versions of these slides have full details of copyright and acknowledgements
MYH associated polyposis• N=152 patients with 3-100 lifetime adenomas
• Seen in genetics clinic for family or personal history of colorectal neoplasia
MYH negativeN=140
Single MutationN=6
Bi-allelic MutationN=6
34Sieber O, et al., NEJM 2003;348:791
Age at Presentation
56 (18-77) 64 (25-72) 56 (45-59)
Polyp Count 7 (3-100) 4 (3-12) 55 (18-100)
Synchronous CRC 19 (14%) 2 (33%) 3 (50%)
Family Hx CRC 66 (47%) 4 (67%) 5 (83%)
33% of individuals with > 15 adenomas had bi-allelic MYH mutations
CRC risk associated with MYH• Population-based study of 9,268 CRC patients and 5,064 controls
• Tested for Y179C and G396D MUTYH mutations
Genotype No. Patients
GenotypeRelative Risk
AgeYrs (SD)
CRC Location Prox Distal (%)
Family Hx CRC
(%)
N/N 9043 (97.7%)
Ref 59(8.5) 29 71 15
35
Mut/N 198 (2%) 1.07 (0.87-1.31) 59.6(8.4) 36 64 20
Mut/Mut 27 (0.3%) 28.28 (17.6-44.06) 54(7.3)* 59* 41 26T
Y179C/Y179C 4 49.5(6.0) 75 25 25
Y179C/G396D13 52.5(7.5) 77 23 23
G396D/G396D 10 57.9(6.2) 30 70 30
Lubbe, S. J. et al., J Clin Oncol; 27:3975-3980 2009N= No mutation, * = p <0.01, T= trend
Penetrance of biallelic MUTYH mutation
• The estimated penetrances at age 50 and 60 were 19.5% and 43% respectively
• Biallelic mutations are highly penetrant
36Lubbe, S. J. et al., J Clin Oncol; 27:3975-3980 2009
and are incomplete at the age of 60
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
13The screen versions of these slides have full details of copyright and acknowledgements
The odds ratio (OR)of colorectal cancer risk associated
with monoallelic Y179C and G396D mutations
No increased risk of colorectal cancer associated
37Lubbe, S. J. et al., J Clin Oncol; 27:3975-3980 2009
with monoallelic MYH mutations
Polyposis phenotype in MYH CRC
GenotypeNo.
PatientsSynchronous Polyp Number
0 < 3 >3
38
N/N 2640 79% 15% 6%
Mut/N 91 75% 19% 7%
Mut/Mut 14 29% 29% 42%
Lubbe, S. J. et al., J Clin Oncol; 27:3975-3980 2009
MAP phenotype
Age of Diagnosis 45 yrs (24-72)
Colon PhenotypeAttenuated (80%)10-100 adenomas > age 25> 100 adenomas > age 45
39
Polyp distribution Diffuse (50%), Proximal (40%)
CRC50% at time of Diagnosis; Mean age of 48 yrs (29-72)
Extracolonic tumors Duodenal polyposis, thyroid cancer, gastric cancer, renal cell cancer
Aretz S. Int J Ca 2006; 119:807N=392
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
14The screen versions of these slides have full details of copyright and acknowledgements
Colorectal surveillance of adenomatous polyposis syndromes
Procedure Age (yrs) Interval
Classic FAP Sigmoidoscopy* 10-12 1-2 yrs
aFAP/MYH Colonoscopy§ 18-20 1-2 yrs
40
Post operative Sigmoidoscopy Ileoscopy
1 yr
5 yrs
*Annual colonoscopy§ Surgery consultation once adenomas detected
Adenomatous polyposis syndromes surgical guidelines
• Severe polyposis
– Total Colectomy and ileorectal anastomosis
Proctocolectomy and IPAA (if rectal burden high
41
– Proctocolectomy and IPAA (if rectal burden high, > 20 polyps)
• Oligopolyposis (< 100 polyps)
– Colectomy may be necessary depending on polyp burden
Chemoprevention of FAP
• Colorectal polyposis
– Sulindac 150-200 mg BID- 50% reduction
– Celecoxib 400 mg BID- 28% reduction1
FDA approved in adults as an adjunct to endoscopy
42
FDA approved in adults as an adjunct to endoscopy
• Duodenal polyposis
– Celecoxib 400 mg BID1,2
– Significant improvement in polyp burden (blinded video assessment score)
1 Steinbach G, NEJM 2000;342:1947,
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
15The screen versions of these slides have full details of copyright and acknowledgements
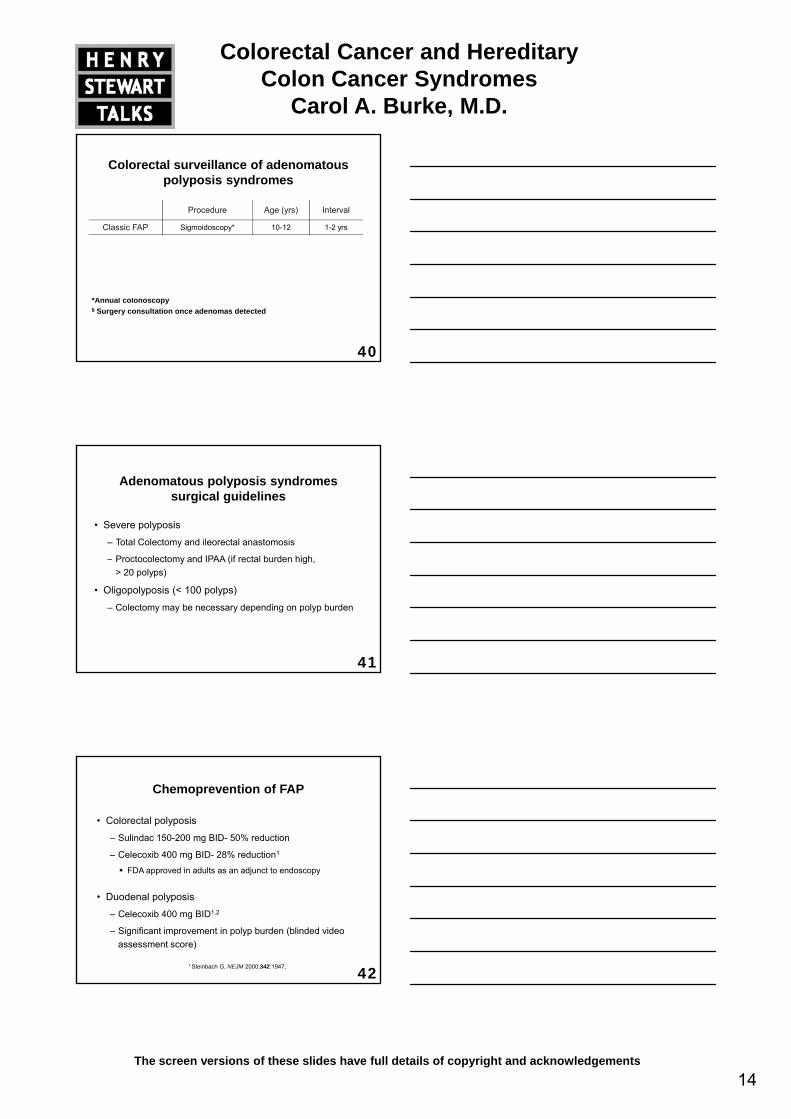
N=18 children, 10-14 yrs, 3 month study
Pediatric chemoprevention in FAPPo
lyps 80
100
120 + 39% + 70% - 44% -44%
43Lynch P, et al., Am J Gastro 2010;105: 1437-43
Num
ber o
f P
--
- - --
--
Pre Post Pre Post Pre Post Pre PostPlacebo 4 mg/kg 8 mg/kg 16 mg/kg
020
4060
Genetic testing in adenomatous polyposis syndromes
• ≥10 cumulative adenomas
• CRC <60 yo
D id
44
• Desmoids
• Relatives of known APC or MYH mutations carriers
Genetic testing for adenomatous polyposis syndromes (2)
• Up to 34% of APC negative FAP patients have biallelic MYH mutations
• APC and MYH testing should be performed concurrently
45
APC and MYH testing should be performed concurrently
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
16The screen versions of these slides have full details of copyright and acknowledgements
Results of APC genetic testing
• Patient with >100 adenomas
– Sequencing - <90%
– Deletion/duplication - 8-10%
46
• Patients with <100 adenomas
– Mutation detection <30%
MYH genetic testing
• Caucasian patients
– MYH mutation panel sequencing
Y179C and G396D
47
• Non-Caucasian patients
– MYH sequencing
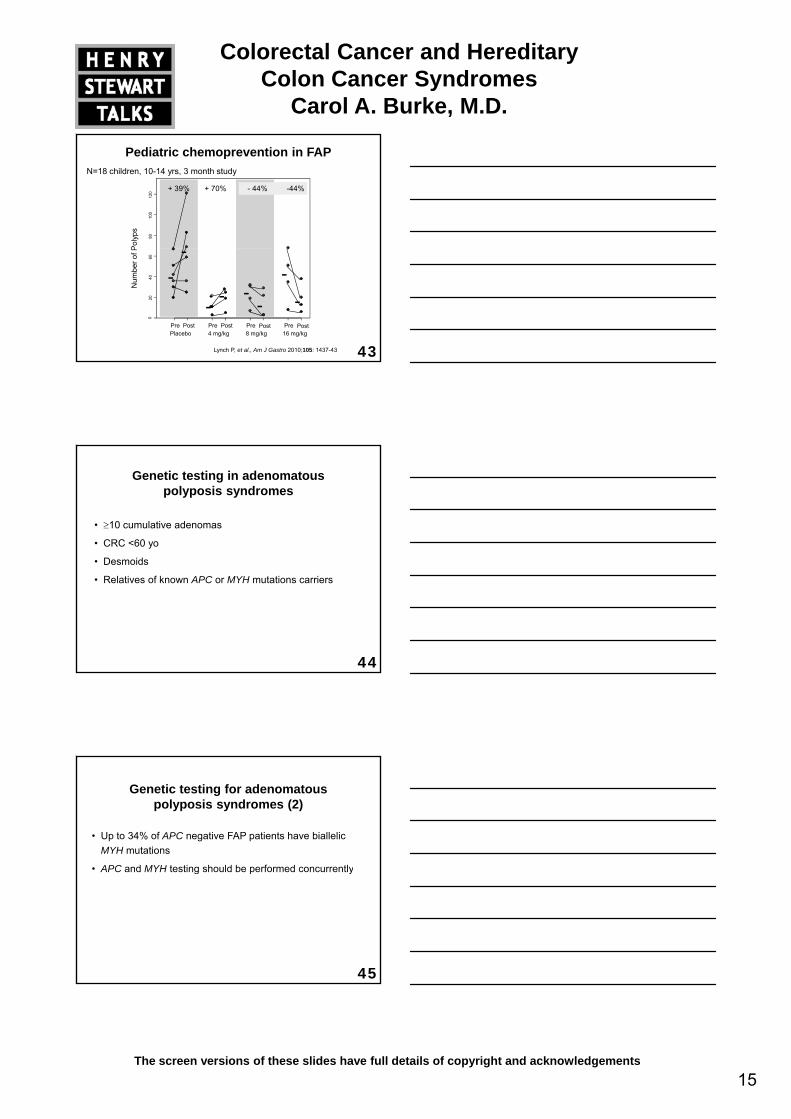
• Autosomal dominant
– 1 in 120,000 births
– 50% cases are inherited
– 50% of cases are de novo mutations
• Due to mutation in STK11 gene
Peutz-Jeghers syndrome (PJS)
48
• Due to mutation in STK11 gene
– Genetic testing positive in 90% of PJS patients
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
17The screen versions of these slides have full details of copyright and acknowledgements
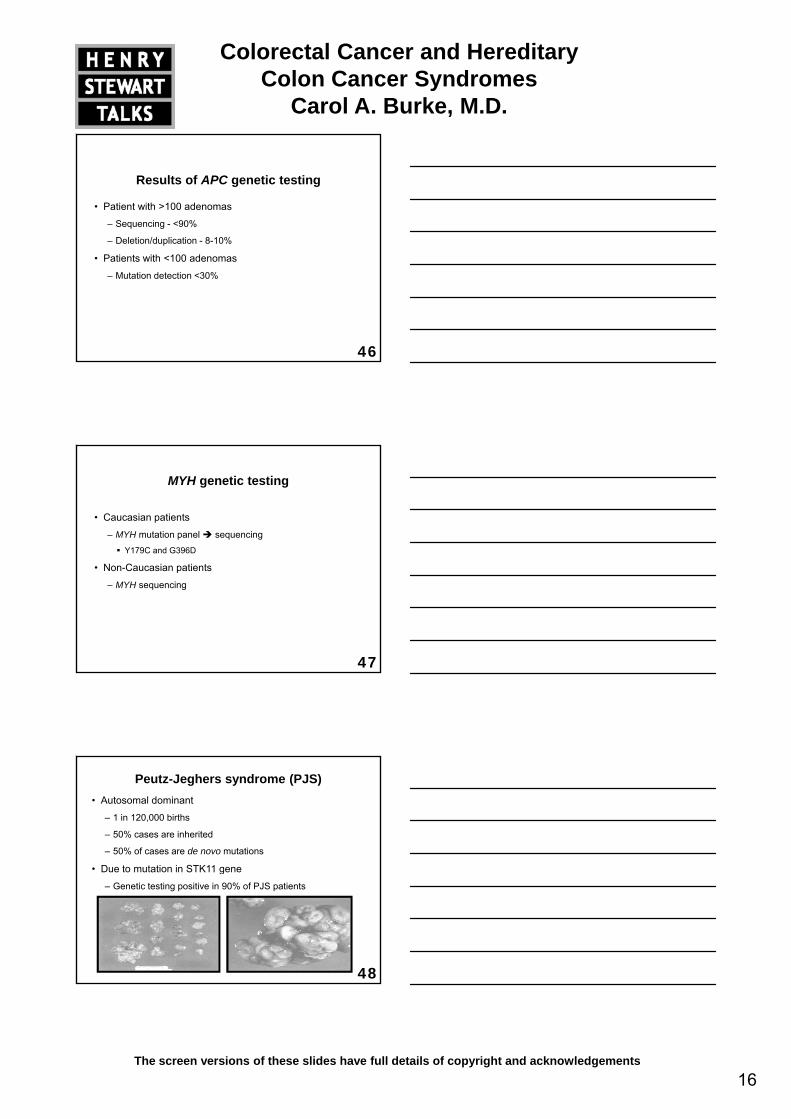
• Diffuse hamartomatous polyps
– 50% risk of SBO by age 20
• Muco-cutaneous pigmentation
Hallmarks of PJS
49
– Perioral region, digits, genital area
Diagnostic criteria for PJS
• > 3 hamartomatous polyps in GI tract or
• > 1 GI hamartoma and pigmentation or
• > 1 GI hamartoma and family history of PJS or
50
• > 1 GI hamartoma and family history of PJS or
• Family history of PJS and typical pigmentation
World Health Organization Classification of Tumours, Peutz-Jeghers Syndrome Diagnostic Criteria
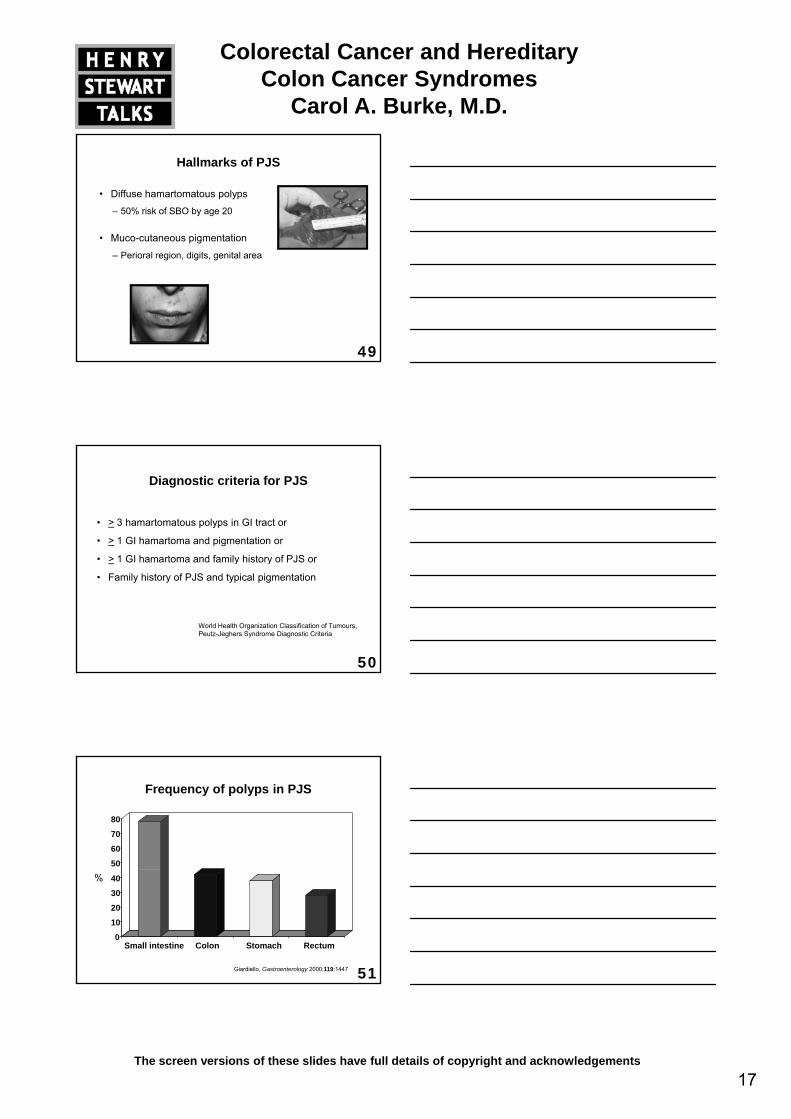
Frequency of polyps in PJS
50
60
70
80
51
%
Giardiello, Gastroenterology 2000;119:1447
0
10
20
30
40
Small intestine Colon Stomach Rectum
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
18The screen versions of these slides have full details of copyright and acknowledgements
• 90% lifetime risk
– 50% by age 50
• Intestinal and extra-intestinal
Cancer risk in PJS
52
• Unusual Gonadal Neoplasms
– Adenoma malignum of the cervix, ovarian sex cord tumors with annular tubules (SCTAT), or large cell calcifying Sertoli cell testicular tumors
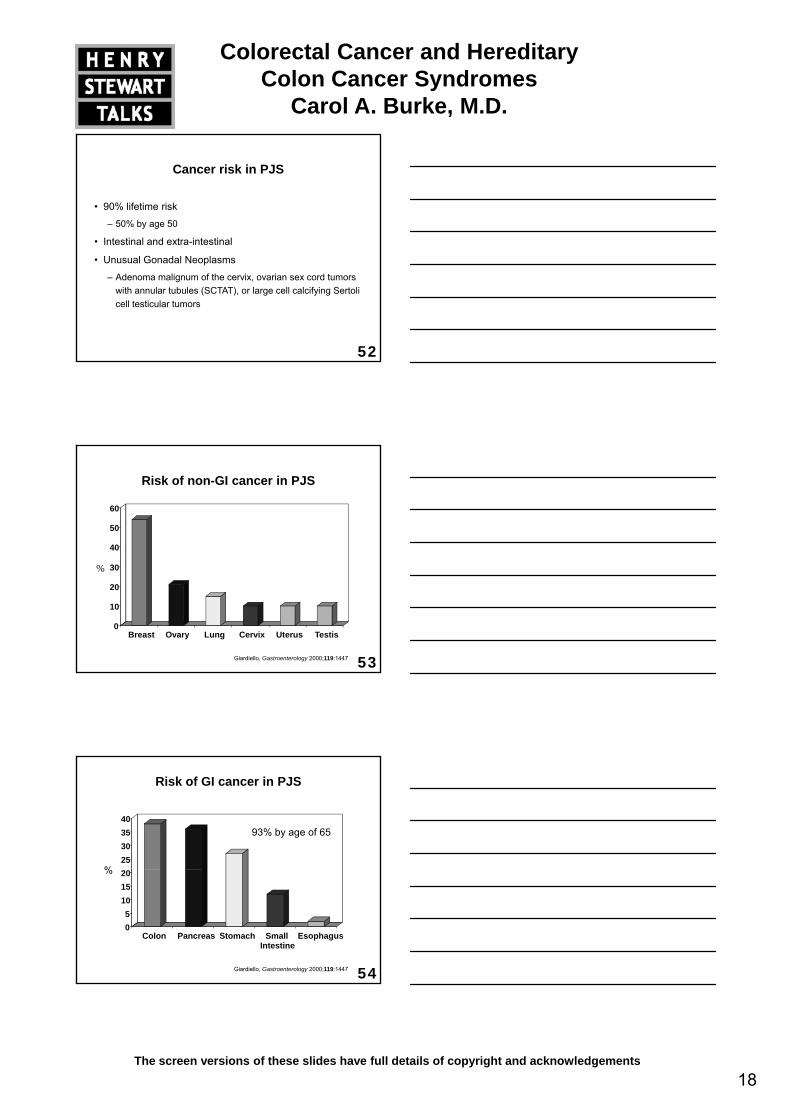
Risk of non-GI cancer in PJS
40
50
60
53
%
0
10
20
30
Breast Ovary Lung Cervix Uterus Testis
Giardiello, Gastroenterology 2000;119:1447
25303540
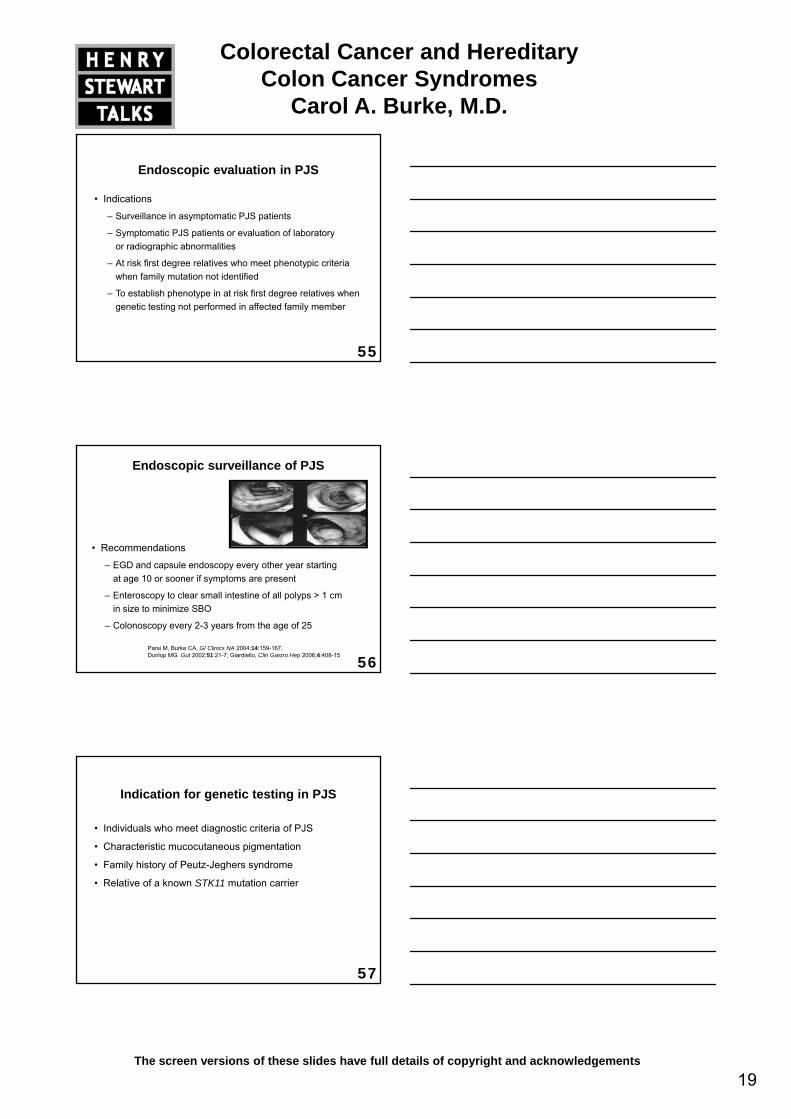
Risk of GI cancer in PJS
%
93% by age of 65
54
05
101520
Colon Pancreas Stomach SmallIntestine
Esophagus
%
Giardiello, Gastroenterology 2000;119:1447
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
19The screen versions of these slides have full details of copyright and acknowledgements
Endoscopic evaluation in PJS
• Indications
– Surveillance in asymptomatic PJS patients
– Symptomatic PJS patients or evaluation of laboratory or radiographic abnormalities
55
or radiographic abnormalities
– At risk first degree relatives who meet phenotypic criteria when family mutation not identified
– To establish phenotype in at risk first degree relatives when genetic testing not performed in affected family member
Endoscopic surveillance of PJS
• Recommendations
56
– EGD and capsule endoscopy every other year starting at age 10 or sooner if symptoms are present
– Enteroscopy to clear small intestine of all polyps > 1 cm in size to minimize SBO
– Colonoscopy every 2-3 years from the age of 25
Parsi M, Burke CA. GI Clinics NA 2004;14:159-167, Dunlop MG. Gut 2002;51:21-7; Giardiello, Clin Gastro Hep 2006;4:408-15
Indication for genetic testing in PJS
• Individuals who meet diagnostic criteria of PJS
• Characteristic mucocutaneous pigmentation
• Family history of Peutz-Jeghers syndrome
57
y y g y
• Relative of a known STK11 mutation carrier
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
20The screen versions of these slides have full details of copyright and acknowledgements
Genetic test results in PJS
• Sequencing - 30-69%
• Deletion/duplication - 30%
58
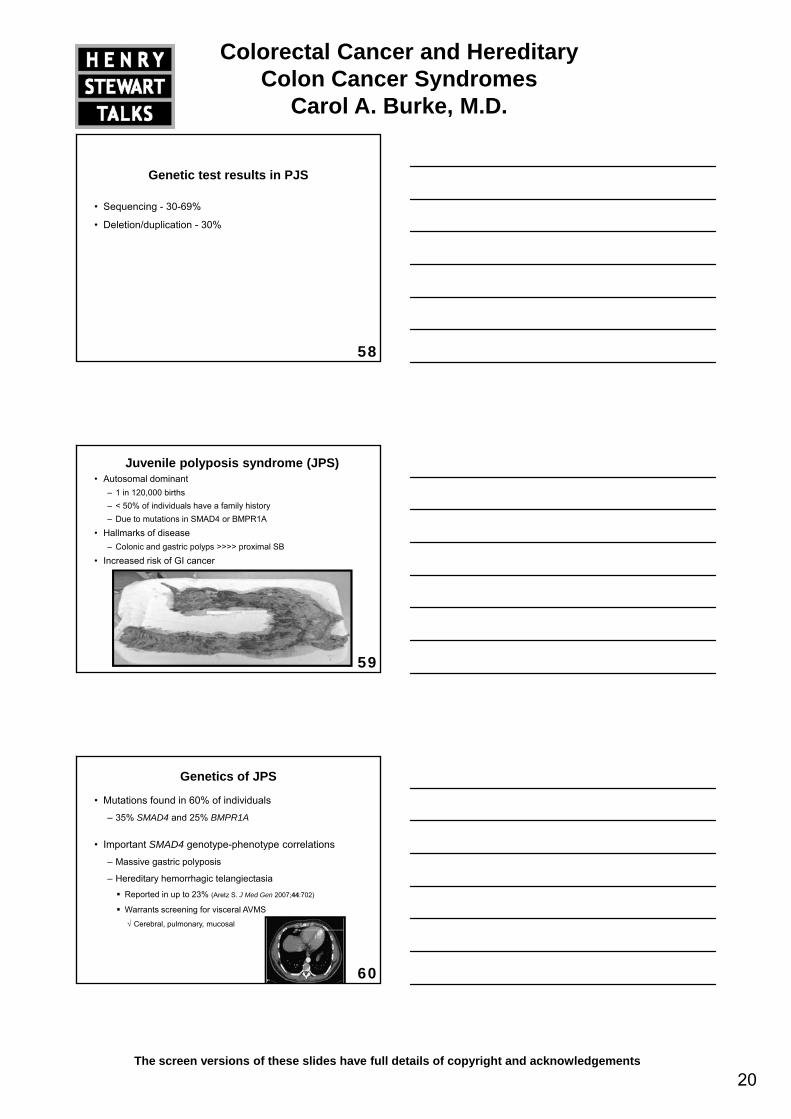
• Autosomal dominant– 1 in 120,000 births– < 50% of individuals have a family history– Due to mutations in SMAD4 or BMPR1A
• Hallmarks of disease– Colonic and gastric polyps >>>> proximal SB
Increased risk of GI cancer
Juvenile polyposis syndrome (JPS)
59
• Increased risk of GI cancer
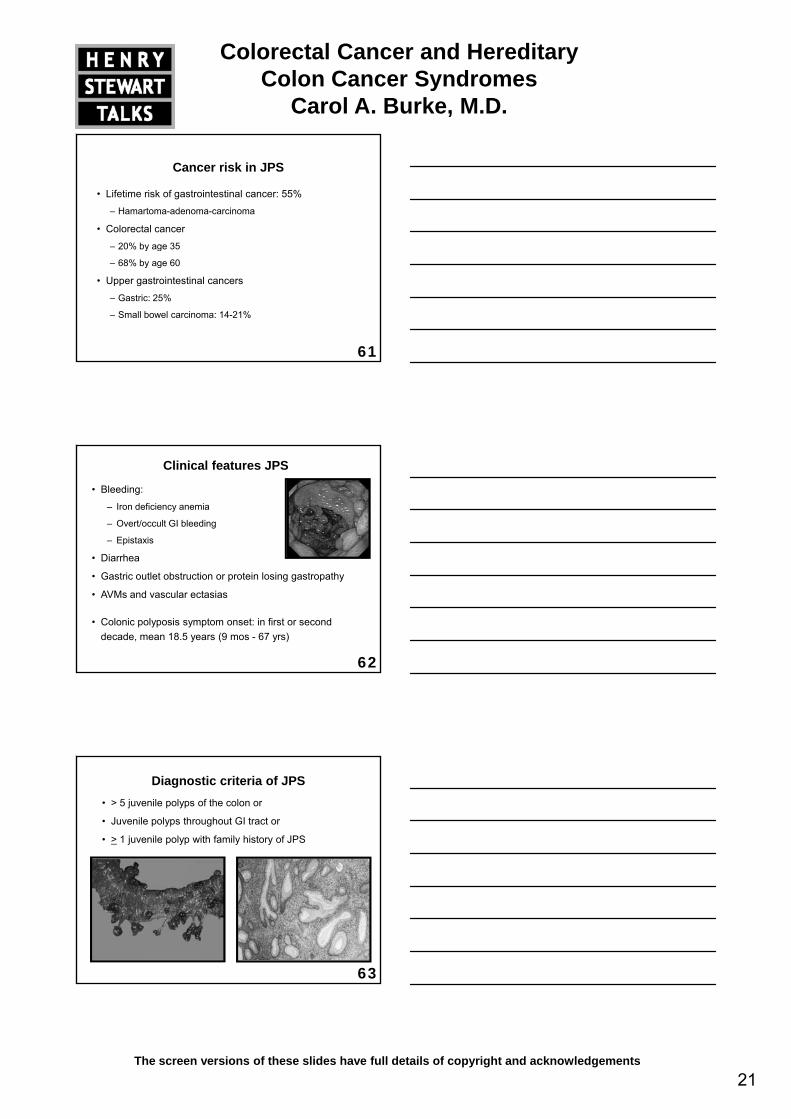
Genetics of JPS
• Mutations found in 60% of individuals
– 35% SMAD4 and 25% BMPR1A
• Important SMAD4 genotype-phenotype correlations
– Massive gastric polyposis
60
– Hereditary hemorrhagic telangiectasia
Reported in up to 23% (Aretz S. J Med Gen 2007;44:702)
Warrants screening for visceral AVMS√ Cerebral, pulmonary, mucosal
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
21The screen versions of these slides have full details of copyright and acknowledgements
Cancer risk in JPS
• Lifetime risk of gastrointestinal cancer: 55%
– Hamartoma-adenoma-carcinoma
• Colorectal cancer
– 20% by age 35
61
20% by age 35
– 68% by age 60
• Upper gastrointestinal cancers
– Gastric: 25%
– Small bowel carcinoma: 14-21%
Clinical features JPS
• Bleeding:
– Iron deficiency anemia
– Overt/occult GI bleeding
– Epistaxis
• Diarrhea
62
• Diarrhea
• Gastric outlet obstruction or protein losing gastropathy
• AVMs and vascular ectasias
• Colonic polyposis symptom onset: in first or second decade, mean 18.5 years (9 mos - 67 yrs)
Diagnostic criteria of JPS• > 5 juvenile polyps of the colon or
• Juvenile polyps throughout GI tract or
• > 1 juvenile polyp with family history of JPS
63
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
22The screen versions of these slides have full details of copyright and acknowledgements
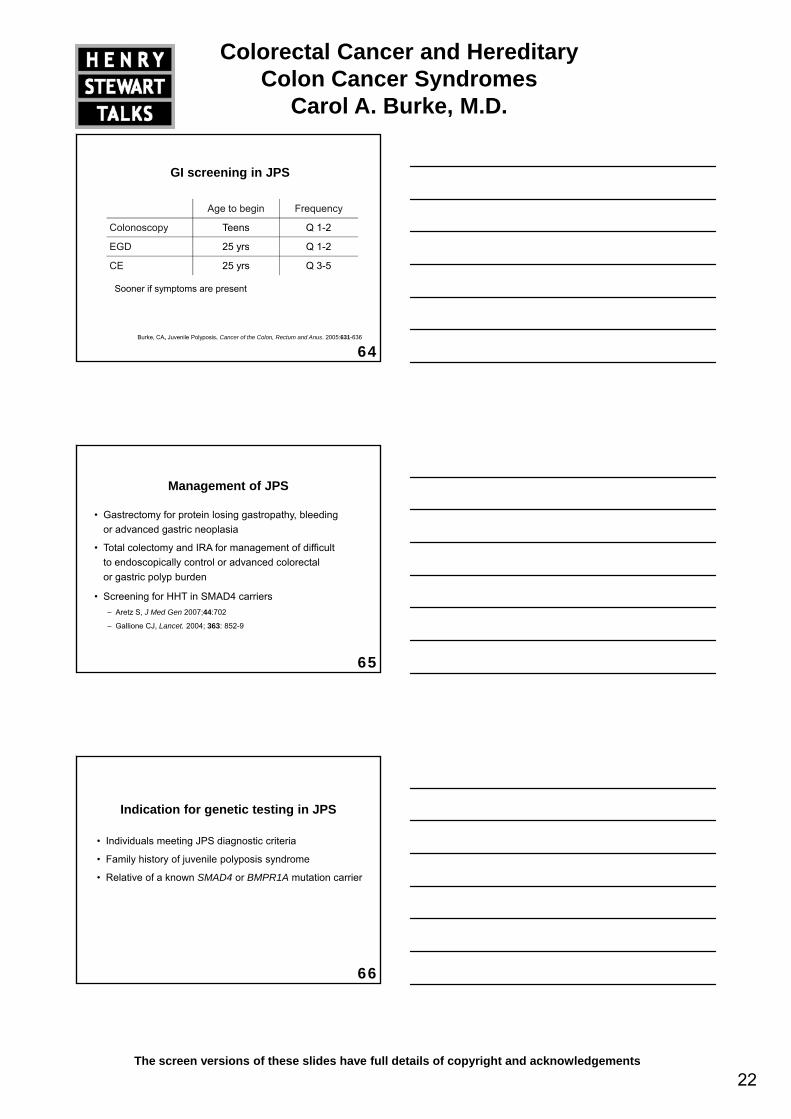
GI screening in JPS
Age to begin Frequency
Colonoscopy Teens Q 1-2
EGD 25 yrs Q 1-2
64Burke, CA, Juvenile Polyposis. Cancer of the Colon, Rectum and Anus. 2005:631-636
EGD 25 yrs Q 1 2
CE 25 yrs Q 3-5
Sooner if symptoms are present
Management of JPS
• Gastrectomy for protein losing gastropathy, bleeding or advanced gastric neoplasia
• Total colectomy and IRA for management of difficult t d i ll t l d d l t l
65
to endoscopically control or advanced colorectal or gastric polyp burden
• Screening for HHT in SMAD4 carriers– Aretz S, J Med Gen 2007;44:702
– Gallione CJ, Lancet. 2004; 363: 852-9
Indication for genetic testing in JPS
• Individuals meeting JPS diagnostic criteria
• Family history of juvenile polyposis syndrome
66
• Relative of a known SMAD4 or BMPR1A mutation carrier
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
23The screen versions of these slides have full details of copyright and acknowledgements
Genetic test results in JPS
• SMAD4 and BMPR1A
– Sequencing - 40%
– Deletion/duplication - 14%
67
Deletion/duplication 14%
Cowden’s syndrome
68Courtesy Brandie Leach, CGC
Cowden’s syndrome (2)
• Autosomal dominant
– 1 in 200,000 individuals
• Due to mutation in PTEN
– Detected in > 90% of individuals
69
– Detected in > 90% of individuals
• Hallmarks of disease
– Skin findings, macrocephaly
– Hamartomatous polyps
Lipomas, inflammatory, juvenile, ganglioneuromas, adenomas
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
24The screen versions of these slides have full details of copyright and acknowledgements
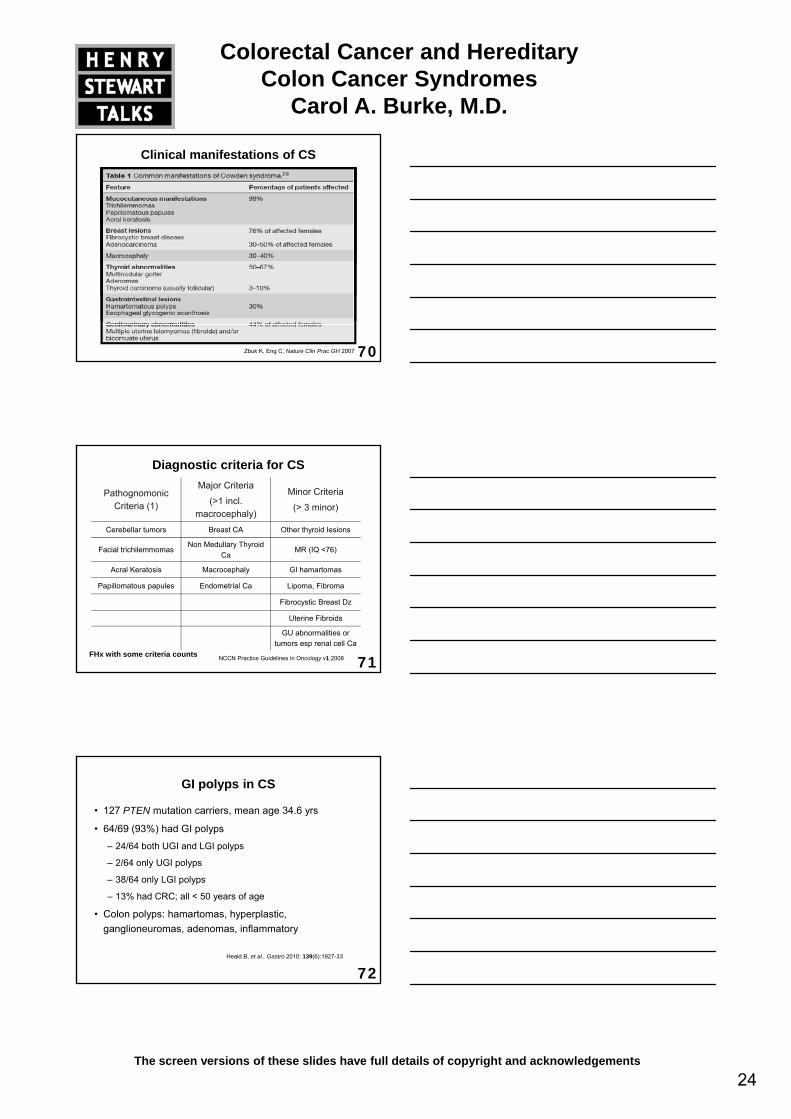
Clinical manifestations of CS
70Zbuk K, Eng C, Nature Clin Prac GH 2007
Diagnostic criteria for CS
Pathognomonic Criteria (1)
Major Criteria
(>1 incl. macrocephaly)
Minor Criteria
(> 3 minor)
Cerebellar tumors Breast CA Other thyroid lesions
Facial trichilemmomasNon Medullary Thyroid
CaMR (IQ <76)
71
Acral Keratosis Macrocephaly GI hamartomas
Papillomatous papules Endometrial Ca Lipoma, Fibroma
Fibrocystic Breast Dz
Uterine Fibroids
GU abnormalities or tumors esp renal cell Ca
FHx with some criteria counts NCCN Practice Guidelines in Oncology v1.2008
GI polyps in CS
• 127 PTEN mutation carriers, mean age 34.6 yrs
• 64/69 (93%) had GI polyps
– 24/64 both UGI and LGI polyps
– 2/64 only UGI polyps
72
– 38/64 only LGI polyps
– 13% had CRC; all < 50 years of age
• Colon polyps: hamartomas, hyperplastic, ganglioneuromas, adenomas, inflammatory
Heald B, et al., Gastro 2010: 139(6):1927-33
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
25The screen versions of these slides have full details of copyright and acknowledgements
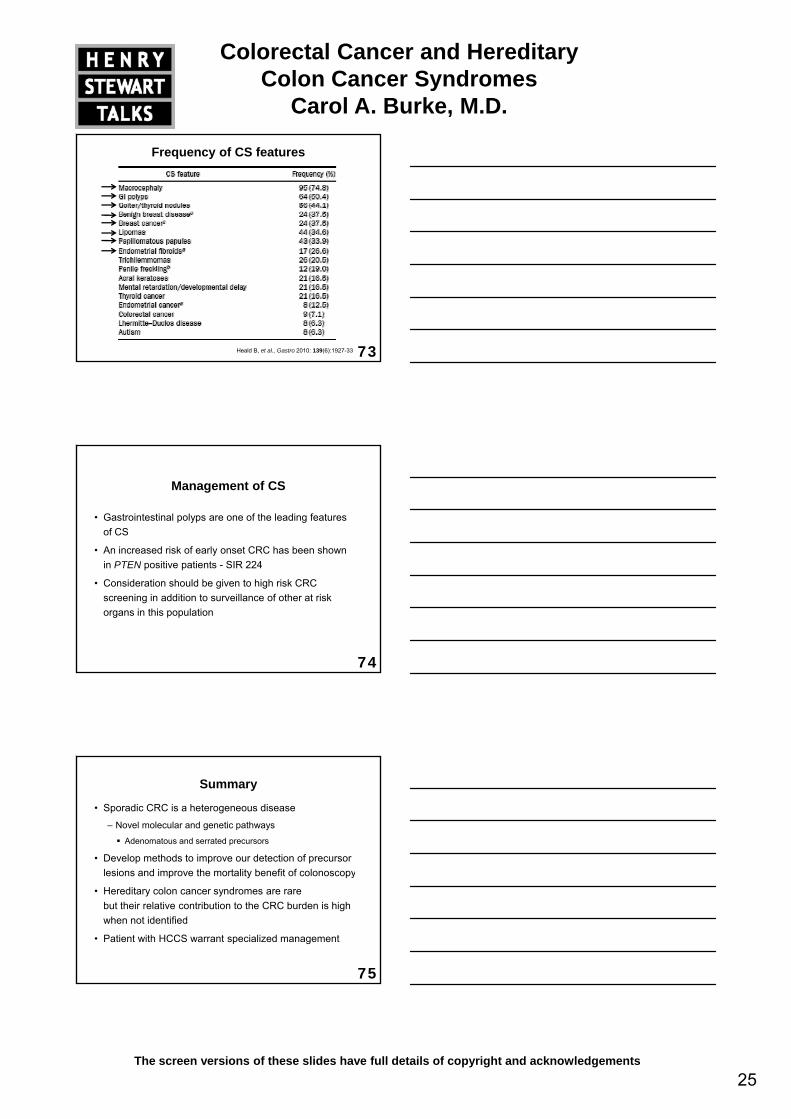
Frequency of CS features
73Heald B, et al., Gastro 2010: 139(6):1927-33
Management of CS
• Gastrointestinal polyps are one of the leading features of CS
• An increased risk of early onset CRC has been shown
74
in PTEN positive patients - SIR 224
• Consideration should be given to high risk CRC screening in addition to surveillance of other at risk organs in this population
Summary
• Sporadic CRC is a heterogeneous disease
– Novel molecular and genetic pathways
Adenomatous and serrated precursors
• Develop methods to improve our detection of precursor l i d i th t lit b fit f l
75
lesions and improve the mortality benefit of colonoscopy
• Hereditary colon cancer syndromes are rare but their relative contribution to the CRC burden is high when not identified
• Patient with HCCS warrant specialized management
Colorectal Cancer and Hereditary Colon Cancer Syndromes
Carol A. Burke, M.D.
26The screen versions of these slides have full details of copyright and acknowledgements
76