columbia links presents: on the edge: undiagnosed and untrated, teens and mental illness
DESCRIPTION
ÂTRANSCRIPT

1
www.columbialinks.org
A White Paper by the Columbia Links 2015 I-Team
THEUNDIAGNOSED AND UNTREATED
TEENS AND MENTAL ILLNESS

2
Special thanks to the Columbia Links I-Team:
Frederick H. Lowe, project managerKari Lydersen, project coordinator and mentorBrenda Butler, executive director, Columbia Links
I-Team student journalists:Solomon Davis (Marist High School), Amber Fry (Lindblom Math and Science Academy), Kiersten Lofton (Illinois Mathematics and Science Academy), Brandon Spencer (Urban Prep, West Side Campus), Christian Thorsberg (Northside College Prep)
Photos by Owen Lawson III Colin King, art director

3
"Focus on mental illness after Oregon mass shooting."
"Police confront a rising number of mentally ill suspects.”
"New York City launching $30 million mental-health initiative."
"Boys more likely to have antipsychot-ics prescribed, regardless of age."
"Minority youth: Needs for mental health services grow with population.”
"Mental health disorders are the most common diseases of childhood."
In its Children's Mental Health Re-port, the Child Mind Institute reported that of the 74.5 million children in the United States, an estimated 17.1 million have or have had a psychiatric disor-der—more than the number of children diagnosed with cancer, diabetes and AIDS combined.
The Columbia Links I-Team ad-dresses these issues and more in its wide-ranging white paper report on mental illness among juveniles, titled "On the Edge/Undiagnosed and Un-treated: Teens and Mental Illness." This summer, the I-Team, comprising five Chicago high school students, spent weeks reporting and writing articles that explore such topics as teens selling their ADHD medicines to other teens, the role of the African-American church in fighting or hindering the treatment of
The state of young mindsThe news headlines are very disturbing.
mental illness, how theatrical produc-tions are lifting the curtain on men-tal illness and sparking discussions, how the Chicago Public Schools treat students with mental illness, barriers to mental health care and how lead paint poisoning, found mostly in Afri-can-American and Hispanic neighbor-hoods, is linked to neurological damage and low IQs.
Black boys also suffer from microag-gressions in which others automatically assume they are criminals, affecting their self-esteem.
Why did the I-Team choose this topic? The student journalists said they have interacted with many students with mental illness, in schools and in their communities. Some get help; many do not. The I-Team members also wondered what happens to youth who are constantly bombarded by violence, who act out in violent ways and who are entrapped in the school-to-prison pipeline, incarcerated and then released to fend for themselves. The I-Team also wanted to explore why more isn’t being done to address mental illness among juveniles. At the end of this report, they have provided solutions that will help at-risk students, their families and their communities. The I-Team hopes to spark a citywide dialogue about how to recognize mental illness and how to help our relatives, friends and others who are facing mental health challenges.
The Columbia Links Staff

4
Kelvin Roston Jr. wrote and performed in “Twisted Mel-odies,” a one-man show that
portrayed the life of gifted singer/songwriter. Donny Hathaway. Hatha-way suffered from schizophrenia and took his own life at age 33.
Roston also has personal experi-ence with mental illness, but not in the way that Hathaway did, as he told me and other members of the Co-lumbia Links I-Team during a visit this summer.
The drama of life Raising the curtain on mental illness
Roston wrote “Twisted Melodies” inspired by the struggle to under-stand his own mother’s mental illness. When he was a child, his mother would often lay in bed for three days in a row, Roston said, and then go on a shopping spree the next day. His family didn’t like talking about his mom’s illness. Roston said that his granddad -- a minister -- would just tell him that his mom was “going through something,” and they would continue to pray for her.
Nobody really talked about what was going on. Everything was always sugar-coated.
He didn’t understand until much later that his mother lived with bipolar disorder. Now a minister, she is now handling the illness with medication. Roston says that his mother is his biggest critic, and for her to come see “Twisted Melodies” brought tears to his eyes.
“I saw a silhouette of a woman that looked like my mother in the crowd,” he said. “Somehow my fiancée got my mom to surprise me and come to
By Amber FryLindblom Math and Science Academy
Kelvin Roston Jr., who starred in and wrote the play "Twisted Melodies," about singer and songwriter Donny Hathaway, spoke to the I-Team about mental illness. Hathaway was diagnosed with schizophrenia and took his own life.

5
Chicago to see my show.” His mother came to the stage and
publicly praised Roston’s courage in writing the play and helping raise awareness of mental illness.
After each performance of the show’s 2015 run in Chicago, pro-duced by Congo Square Theatre, the cast and crew received comments from the audience. During these talkbacks, audience members would voluntarily discuss their own and their family members’ struggles with mental illness. Roston noted that this does not happen on an everyday basis.
"People, especially people of color, do not like to speak of mental illness because of the stigma," Roston said. "We feel like we are supposed to be the 'strong ones' and the ones who 'push through it' when in reality, we need help just like everyone else."
Many African-American families tend to say “what happens in this house stays in this house.” There-fore, many choose not to get outside help, because we are used to keeping all of our “dirty laundry” inside of
our families and our homes.Congo Square Theatre wants to
remount “Twisted Melodies” and tour it throughout the city to educate others.
With the Columbia Links I-Team, I went to the play “Coming Home” by the company Erasing the Distance. The cast and crew sat down with real people, listened to their stories and made them into a play. The pro-duction was held at the South Side Community Art Center, an old house converted into an art studio and the-ater. “Coming Home” was performed by five actors inside the former living room, and every seat was filled.
There was also a talkback after “Coming Home,” where many au-dience members shared personal stories and opinions. Tears were in the eyes of some audience mem-bers during and after the play. Like Congo Square Theatre, Erasing the Distance wants to bring the play anywhere they can to help spread the message.
During the talkbacks for both plays, audience members discussed the
roles of religion and medicine in dealing with mental illness. Some people said that religion does play a part in the healing process, others said that medicine is crucial.
Said one woman: “All we need is prayer, patience and pills,” which means that we need our religion, our patience and medication.
As Roston noted, theater and art can also help reduce the stigma and make it easier for people to get treat-ment for mental illness.
Roston said that each performance of “Twisted Melodies” is a step forward. More artists, playwrights and actors are talking about mental illness and addressing the different stereotypes, misconceptions and negative attitudes about mental illnesses and mentally ill people. Hopefully the word will get out about mental illnesses and we will all see a change in our culture’s attitudes towards this issue.
"Coming Home," a play staged at the South Side Community Art Center, raises the curtain about mental illness in the black community.

6
Christopher Griffin, pastor of Saint Martin’s Episcopal Church on Chicago’s West
Side, holds marriage counseling ses-sions to insure that those who want to get married at Saint Martin’s are psychologically ready to say “I do.”
But one counseling session involv-ing two lesbian partners sparked a conversation much bigger than the pending marriage.
“I usually hold three marriage counseling sessions before a couple gets married just to make sure they are really ready,” Griffin said. “At the time, one of the ladies’ fathers had died and she was grieving, but her partner just didn’t understand why.
When I asked her why she wasn’t un-derstanding of the grief her partner was feeling, she replied, ‘Because I don’t have love for my father,’ ” Grif-fin said. “I then asked her why she felt that way? She said, ‘Because my daddy raped me when I was young.’ ”
“That was the first time that she had ever said what her father had done to her,” Griffin said. Griffin was able to find professional help for the couple to resolve their issues, which, if left unaddressed, would have add-ed additional stress to the marriage.
Griffin notwithstanding, black ministers playing the role of psycho-therapists to their parishioners is controversial among mental health
professionals and some members of their flock. That’s because most pastors are not trained to treat their parishioners suffering from mental illness, and they don’t know where to direct them for help.
There is no easy solution to this problem.
African-Americans seek help from their ministers because they don’t trust the medical commu-nity, which historically has used scientific evidence against them, Griffin said. Only 2 percent of social workers, who employ talk therapy to resolve issues, and 2 percent of psychiatrists, who may prescribe medication as part of treatment, in the United States are African-Amer-ican, according to the book “Social Work with African American Males,” by Waldo E. Johnson, Ph.D., of the University of Chicago School of Social Service Administration. Only 2 percent of psychologists are Afri-can-American, Johnson added.
In addition, many African-Ameri-cans don’t know how to find a psy-chiatrist or a therapist and many can’t afford to pay them. Charges are often $100 and up an hour, even with sliding scales.
N’Dana Carter, lead mental health organizer for Southside Together Organizing for Power (STOP), has organized workshops to educate African-American ministers about mental health.
When asked if someone should go to a minister instead of a therapist, she replied: “It can only be helpful if the minister uses more than just prayer. He or she has to provide other help.”
"The church can be a good place to go for people in the black commu-nity," she added. "Sometimes there is no place for some people to go to receive that therapy they need.”
‘Take it to the Lord’In the black community, the minister often doubles as a therapist, offering prayer instead of treatment
By Brandon SpencerUrban Prep Academy, West Campus
Tanya Auguste, a doctoral student in criminal psychology at the Illinois Institute of Technology, cautions that not all members of the clergy have any training in mental health.

7
Father Christopher Griffin of St. Martin's Episcopal Church on the West Side talks to visitors after Sunday service. "African-Americans seek help from their ministers because they don't trust the medical community," he said.
A band-aid approach?Tanya Auguste, a doctoral student
in forensic psychology who works with children 3 to 12 years old, also has strong views about the role black ministers can and cannot play help-ing parishioners with mental illness. “Some religious leaders receive psychological training, but some don’t. So when people come to these leaders who aren’t trained, they are receiving a band-aid rather than the true help that is needed,” Auguste said.
Carter’s and Auguste’s viewpoints resonated with the audience who attended the theatrical production “Coming Home,” about the stigma of mental illness in the African-Ameri-can community.
During a Q&A following the play, audience members agreed the church has a role helping with men-tal illness, but they said there needs to be more help available including medication.
An audience member at the play chanted: “Prayer, patience and pills.”
Auguste said professional thera-py could help end beliefs that hurt the black community. For example,
there is an iron-clad rule in much of the black community that “what happens in this house stays in the house.”
“This is the complete opposite of bringing ‘positive communication around the child," Auguste said. She also says that to truly move on from a mental health problem or an in-stance of abuse, “you have to steadily work on the problem,” meaning that you have to address what has or is happening with someone, Auguste said. For people who cannot afford or find a clinician, ministers can play that role. Griffin notes that minis-ters have a strong role in the Afri-can-American community.
“A lot of people will not tell some-one they had been raped or molested until they are around someone who is a man of God, which is why you see more of a trend of pastors and ministers going back to school to receive a degree in psychology so that they can help those who come to them with these problems,” he said.
A spokesperson at the University of Chicago School of Social Service Administration said that while it is not a growing trend, some students
are seeking dual degrees in social work and theology.
Like the theatrical productions, there are other efforts to help minis-ters and the community understand mental illness. For example, STOP Chicago has sponsored workshops to educate African-American minis-ters and the black community about mental health.Ministers fill a void
People usually meets with min-isters in their neighborhoods and they aren't charged for counseling sessions. People feel comfortable opening up to ministers, and these meetings can serve as a gateway to additional treatment outside the church.
Griffin will talk to parishioners several times in counseling sessions before referring them to a therapist for another level of service. So min-isters can be of some help to their parishioners, but not every problem can be solved with a series of conver-sations and prayer, especially for the most severe mental disorders.

8
Racial and ethnic minorities underutilize mental health services for a variety of
reasons, including the stigma about mental health and the inability to reach those facilities. And without adequate care, mental illness can lead to incarceration for many peo-ple.
Miwa Yasui, assistant professor at the University of Chicago’s School of Social Service Administration, said that since the 1970s' data have indi-cated that racial and ethnic minori-ties tend to not use these services despite clinical need. “And here we are in 2015 and still these disparities continue to exist,” she said.
As organizations and programs face closure and cuts while the state budget crisis continues in Spring-field, things could get even worse for people living with mental illness. While there has been attention to the looming impact of the budget cuts, the public spotlight still has not been shone on the difficulties that minori-ties have in accessing services. The stigma lingers
“In some cultures, mental health is something that is still largely stigma-tized,” Yasui said. “This actually goes back to the disparities in that there's a huge aspect of mental health dis-parity that is related to stigma.”
Advocates say mental health care should be just as standard as going to the doctor for a checkup, but un-fortunately the shame surrounding mental illness acts as a barrier.
“In some cultures, if you are seeking mental health services, that means that there is something very wrong with you ... that you're crazy, that you can't be changed, that there's something incurable in you. There is something genetically wrong,” Yasui said. “Unfortunately, this leads to stigmatization of those who have mental health problems and also those who are seeking mental health services.”
There are also other obstacles to minorities, especially lower-income people, in accessing mental health care. Location and immediate access are important, and are often a barrier for people in minority or low-income neighborhoods.
“Some families would take three buses to come because they wanted services for their kids,” Yasui said. “If you think about a single mom, working, and she is taking three bus-es with a child who needs services, I think that’s so much effort on that mom’s part. Oftentimes the reality is that many families are not able to do that…[especially] in the middle of winter.”
On the South Side, there are fewer mental health providers than on the North Side or areas with higher income patients. This leaves those in need to travel long distances or forgo necessary treatment. “So for those who do make it into the mental health services, it really speaks a lot to their motivation and their desire and their strength to come in,” Yasui said.
Preconceived notions and discrim-ination also play a role in what and
Stigma, criminal justice and social service: A look at mental health in Chicago
By Solomon DavisMarist High School
Dr. Nneka Jones Tapia, executive director of the Cook County Jail. Some members of the I-Team met with Dr. Jones in her office and she took the team on a tour of Division II, where patients with mental illness are held.
Photo By Rosemary Lambin

9
where services are available. Yasui uses the lack of a trauma center at the University of Chicago as an ex-ample of the biases in the healthcare industry that are also found in the mental health field.Trauma center opens, finally
“We have a very fragmented health-care system that unfortunately I be-lieve does have systematic biases to-ward ethnic minorities, families and youth,” Yasui said. “Here we have had to rally to try and have a trauma center and yet we don't despite the fact that we’re enclosed in a neigh-borhood where there are a lot of shootings and that we may have a lot of people who have gunshot wounds who may need immediate access.” (Since this story was reported, the University of Chicago and the Sinai Health System announced a new joint Level 1 adult trauma center at Holy Cross Hospital at 68th Street and California Avenue.)
Youth can be especially affected by the lack of healthcare resourc-es. Unaddressed mental health problems can often cause behav-ioral and social problems for youth. Yasui worked with her advisor from graduate school and advocates his intervention program, which used teacher screening assessments to find troubled youth. Teachers rate the students on certain behaviors and intervention staff target certain students and reach out to their fami-lies as a result.
“Unfortunately, there are sever-al factors I think that lead to the disparities,” Yasui said. “Obviously discrimination is a huge factor that does play a big role in terms of how even, for example, African-American boys would be identified as being at risk just because of certain stereo-types that schools or teachers may have.”
Biases can mean that Afri-can-American teens in particular don’t get access to the resources they need.
“Youth who tend to be stereotyped as being a lot more delinquent . . . are not serviced into mental health services,” Yasui said. “They end up in the justice system and that's so un-fortunate because if you think about
the services that can be provided to these youth they are not getting those services and they are actually getting punished for having a clinical need.”
In 2012, Chicago closed six of its 12 public mental health clinics. The closures gave relief to the city’s tight budget but at the cost of patients left without services and the resources they needed.
“A lot of the reasons these people come here is because of the cut-backs in mental health,” said Abdon Pallasch, director of public affairs for Cook County Sheriff Tom Dart. “Some of these folks might not have come to our jail if they went to their normal clinics.”
According to the Cook County Sher-iff ’s website, 36 percent of arrestees self-identified as mentally ill during intake on Aug. 4, 2015. “We have to pick up the slack [from providers] because one-third of our detainees identify as mentally ill at intake,” Pallasch said.Zip code bias
Juliana Stratton is the former exec-utive director of Cook County Jus-tice for Children, which promotes transparency and accountability of the Cook County juvenile court. She said trauma and the related mental health impacts play a key role in youth ending up in detention.
“We know that there are certain communities in this city, certain zip codes in this city, where we see disproportionately higher rates of violence," she explained.
"In those communities there are young people that are experiencing and seeing violence both in their homes and in their communities. They're losing friends to violence and that trauma puts them at greater risk of ending up perpetrating an act of violence.”
Stratton has worked in the legal field for more than 20 years, and fresh out of law school, worked for a law firm that handled child abuse and neglect cases. After she became a mediator, Stratton created her own service where she trained students on conflict resolution skills in school systems. She also worked on cases involving keeping young people out
of the justice system by resolving a dispute rather than going to court.
“There I became very involved in re-storative justice and I was trained as a peace circle keeper,” Stratton said. “This concept saw justice as a way to address the harm that has been done to a community, to young people as a result of crime, rather than just looking at prosecution.”
She has “devoted my entire life to look at the harm that is done by our juvenile justice system and recog-nizing there is a need for reform and working on different projects and initiatives to try to find alternatives for our young people.”
Jail officials said that individuals may commit a petty crime to go to jail or return to the security of being in jail. Stratton said families told her that the only way their child has re-ceived the services they needed was by getting arrested. “Anyone would agree that we don't want young people to get arrested so they can get therapy and counseling or any of the other services they may need,” Stratton said. “We want to see those services being provided in advance to keep young people out of the system.”
Stratton emphasized that under-standing the culture around mental health is crucial. In communities of color, talking about mental health needs is often taboo.
“That perpetuates this stigma of saying “well I’ll just have to man up,’ " Stratton said. “ ‘Yes, I saw my friend get shot in the face, yes, I’ve seen this happen in my home but we just have to man up and deal with it,’ ” Stratton said. “That certainly does not help when we are talking about how to heal the trauma that many young people experience.”Capacity to rehabilitate
Two important things have changed in juvenile justice over time. In the 1980s justice was tough on young people because they were viewed as “super-predators.” Within the last decade, there has been a shift to the original focus. When Jane Addams created the first juvenile court, it was based on the belief that young people needed to be treated differently and that they had the capacity to rehabilitate. “So the goal

10
is not to punish. The goal is to try and help them get back on the path so that once they are adults they can live out their lives,” Stratton said.
Dr. Nneka Jones Tapia (who holds a doctorate in clinical psychology) took over as head of Cook County Jail in May of 2015. Jones Tapia, the first person with this educational background to hold this top job, aims to continue mental health work -- a mission that Cook County Sheriff Tom Dart started when he took office in 2006. “The crisis has not mended, we are seeing it at its worst,” Jones Tapia said.
Jones Tapia hopes to have more cu-mulative services and more collabo-ration so providers are not stepping on each others’ toes. Previously after an inmate was released, he would have gotten two weeks of medica-tion which was not enough time to connect with the services and care they needed. Now it is standard for him or her to get a month’s supply and a renewal option for 30 more days. Jones Tapia also stressed the importance of overcoming this
shameful label, and getting access to the services and the needed support. “The best thing to do is get help for you and your loved ones,” Jones Tapia said. “There is really no place for the stigma.”A new look at the mentally ill
Among the efforts of Sheriff Dart and his staff are a pre-bond initiative at the Markham Courthouse which aims to identify those in need of ser-vices and to make sure that judges, lawyers and prosecutors are aware of the presence of any mental health needs. The Markham Courthouse also offers individual and group case management with participants vol-unteering, not being court-ordered. “My team screens everyone before bond court to see if they are suffering from mental illness and we make re-ferrals immediately,” said Elli Petac-que Montgomery, deputy director of mental health policy and advocacy for the Cook County Sheriff's Office. Montgomery also oversees a pre-bond screening program at the Cook
County Jail. Ideally Montgomery said she'd like
to see individuals who are charged with a crime of survival avoid jail. For example, the system could find other ways of dealing with someone charged with stealing $30 worth of food to eat or feed a family.
Ultimately, Montgomery is mod-estly optimistic about better ways to deal with mental illness. But more is needed and funding is always a prob-lem, especially with current state budget cuts.
“A lot of people are in support but we have a governor who doesn’t view mental health as a priority,” Montgomery said. “Unfortunately there is still a stigma around men-tal illness. We are doing our best to de-stigmatize it, but we have a lot more to do.”
Photo By Rosemary Lambin
The visitor's entrance to Cook County Jail.

11
Growing up in a difficult family sit-uation with experiences that she said traumatized her, Kaylaa Velazquez, a 16-year-old Northside College Prep junior, fell “into a never-ending chasm of low self-esteem.” Carrying with her an “overwhelming sadness and panic for years,” it wasn’t un-til she was in sixth grade that the reason she was suffering from these intense feelings became clearer, she said.
But it seemed that her school at the time, O.A. Thorp Academy, a North Side public school, had a much more difficult time understanding. Af-ter years of counseling and failed attempts for seeking help, Kaylaa Velazquez is just now receiving some of the support she needs -- support she believes came “far too late.”
(For more about Kaylaa Velazquez in her own words, see pages 18-20.)
Hidden beneath the conspicuous issues of funding, academic success and class size in the Chicago Public Schools lies the under-reported, yet equally glaring, dilemma of juvenile mental health.
While mental health conditions -- including depression, anxiety, bi-polar disorder and PTSD -- affect 20 percent of teens nationwide, many feel CPS continues to treat the prob-lem as an afterthought. Because of improper staffing, a lack of resources and intense pressure on teachers, counselors and students alike, the
Failing grade Chicago Public Schools don’t meet mental health needs of students
problem of mental health remains largely unaddressed, experts and advocates contend.
Velazquez -- who says she still struggles every day with bipolar disorder, manic depression, PTSD and anxiety -- knows these issues far too well. Without adequate resources, she went to the police by herself seeking help. She bought over-the-counter medication and even attempted suicide, resulting in a week-long hospital stay. The cries for help were there, but CPS coun-selors “didn’t really understand” or made her “feel even worse,” she said. CPS students claim no support
Velazquez does not blame the counselors, however, and said that they “work tirelessly” at their jobs. In fact, counselors and school staff often find their hands tied in trying to deal with students’ mental health issues. They say that they don’t have the support or resources they need to help students with mental health. And CPS budget cuts have eliminat-ed these key positions.
Susan Hickey is a recently retired social worker, having served many CPS schools, including Mitchell Ele-mentary and Pritzker. If her 21-year-experience has taught her anything, it is that the problems relating to mental health run the gamut. And CPS is not meeting the challenge.
“Mental health is the last thing
[CPS] thinks about,” she said. School social workers, Hickey said,
are responsible for “1,100 students at any given time.” Recent cuts -- “20 school workers and 20 psychologists, being replaced by no one” -- are es-timated to yield an “expected ratio of one to 1,500” social workers to stu-dents in the fall, Hickey said, citing Chicago Teachers Union data. (CPS did not respond to repeated requests for comment and Freedom of Infor-mation Act requests.)
Perhaps most startling of all is what “CPS considers sufficient,”Hickey said, a 1:500 social worker to student ratio. Facing astounding numbers of students, Hickey added, “you do what you can...use the band-aid approach.”
With the overwhelming number of students that social workers are assigned, social workers say they should be given ample resources and workspace. But the reality is far different. Explaining that having “no space to do the job right” was one of the most glaring issues she faced, Hickey described her workspace for over a year as a tiny room she shared with the school engineer, with urine dripping in through the walls from the adjacent boys’ restroom.
“[CPS] doesn’t give us what we need,” she said.
Lacking in resources, many social workers do what they can to go the extra mile for students in need. But
By Christian ThorsbergNorthside College Prep

12
it’s still nearly impossible for them to meet all the needs of the students they serve.
“Basic needs come first,” said Hick-ey. “It is very hard for them to focus on their education.”
For example, Hickey’s daily work included helping a girl from a broken home and also assisting the move of a family with a gang-affiliated father. Providing for these exceptionally troubled students takes time away from others. Meanwhile, mental health problems are often not obvi-ous and may be triggered by various factors, so some students aren't noticed so they don't get treatment. When schools contribute to ills
Ironically, in addition to not giving proper help to students with mental illness, often schools themselves contribute to students’ mental health problems. Depression and anxiety, what Hickey describes as the “most common mental health issues,” stem in part from the pres-sures, expectations and testing in today's educational system.
A 17-year-old senior at Northside College Prep, who prefers to remain anonymous, suffers from what she describes as “a constant anorexic mindset,” brought on by “extreme amounts of stress.” Driven internally and externally to achieve educa-tional success, she is a member of more than 10 clubs, sports and dance groups, on top of the daily honors and AP classes.
“It was just an extreme amount of pressure and stress,” she said. “I don’t think I was truly happy most of the year. Oftentimes I would just start crying for no reason.”
The student initially was very re-luctant to seek help, feeling she “had an image...to uphold.” However, after receiving help from a friend, she was able to talk to a counselor and receive some support.
“I definitely did get a lot of help from my counselor as well as the social worker. However, it was also the school itself and the stress that caused my case to worsen and caused me to have to seek out aid.”
With an always-stressful senior year remaining, likely followed by even more stressful higher educa-
tion, the student still worries about her future.
“It is almost a guarantee that I will experience the same thing next school year as a senior, possibly much worse. The summer has given me a little bit of breathing room, but not much...college will prove to be interesting.”
Velazquez expresses other con-cerns.
“Schools that punish children for being late, not showing up, or not doing their work instead of working with them to fix this make it really difficult for everyone,” she said.
John Gianoulis recently completed his first year as a school counselor at Taft High School, one of the largest CPS schools, located on the North-west Side. Coming from an intern-ship at Highland Park High School, a public high school in the north suburbs, he quickly saw the dispar-ities in CPS regarding access to and availability of mental health help.
Highland Park High School, a school of just over 2,000 students, “has four social workers and four psychologists, but there’s also a lot of money in the area. Taft has one psy-chologist, two social workers.” Taft High School has more than 3,200 students.A need for more counselors
And Gianoulis considers Taft fortu-nate, saying, “Could we use a couple more? Definitely. But other schools have a lot less. A lot of schools don’t even have access to a social worker. It’s pretty unfortunate.”
This is one problem that Valerie Wiley is attempting to tackle head-on.
Having worked seven years at vari-ous CPS high schools as a counselor and therapist, Wiley saw “so many kids who needed attending to,” who, due to lack of resources, did not receive proper help.
Thus, Wiley founded The Schools Group in 2009 -- a not-for-profit organization that provides clinical counseling services, with no charge to the school.
“The mission is two-fold...provide services, and provide them for free,” she stated.
Working tirelessly as the “found-
er and director” of this “one-man thing,” Wiley’s remarkable head-quarters are her own home, where she trains and teaches four counsel-ing and clinical psychology graduate students, placing them in three to four CPS elementary schools a year. Most recently, she has worked with Swift, Hayt and Field elementary schools on the North Side. At just these three small schools, the lack of attention to mental health is ex-tremely apparent to Wiley.
“They’re always calling for more counselors. With testing, teaching evaluations, there is so much pres-sure to advance kids, and meet their standards. So much testing is going on now that it’s frustrating for people who want to teach and take care of kids. Classes are too large, there are huge disparities of abilities within one classroom...Teachers are under a lot of pressure, the way they are being evaluated.”
As a result of these issues, too many kids are not receiving proper aid or even noticed as being at risk, she said.
“You always worry about the quiet kids - if you don’t draw attention to yourself...who knows?”
The Schools Group works to imple-ment a more unique type of therapy, one that the client directs, hopefully by talking out their feelings and personal needs, rather than acting out and being punished. In this way, “the kids fully respond to it” and feel “fully empowered,” said Wiley.
Nonetheless, the largest gaps be-tween students and support in CPS, according to Wiley, is the system’s stubborn viewpoints toward chang-ing their approaches.Daily recess shows merit
“All the research shows that kids benefit from activity. Recess is critical....Figure it out! Let a kid get up and walk around the classroom. Take current research and apply it! You’re shooting yourself in the foot [if you don’t]," said Wiley. "If we could change that punitive mindset of, ‘Well, if you give a kid an inch, it’s gonna take a mile’...In some ways, that’s the largest mental health gap -- the educational system does not seem to be in sync with current re-

13
search….The system is large, lumber-ing and cumbersome.”
Said Gianoulis, who too feels the weight of the system: “I can’t dis-agree with that.”Listening to students pays off
With a lack of school social work-ers, counselors often find their hands extremely full - often too full. Though most do all they can to give proper help, many people forget that the role of the counselor primarily involves college applications, career planning, finding scholarships and writing letters of recommendation. According to Gianoulis, counselors spend “probably 20 percent of our time dealing with social or emotion-al problems...Some students want to talk about their problems, and need to, but the unfortunate thing is, as a counselor, you don’t have the time in a day.”
With that being said, however, stu-dents who approach counselors are almost always heard out.
“If we know there’s a student in need, while we may not have the time, we can refer the student to outside resources. If I were in a situ-ation where a student really needed something, we would...find the time.”
Yet while counselors like Gianoulis work diligently at their professions, the lack of help leaves them at times with no other option than having to “weigh how serious the issue is.” In fact, it has even gotten to the point where, according to Gianoulis, school workers “may think there’s an issue and don’t address it, because it could open a can of worms that could be extremely time-consuming.”
Here in Chicago, it is difficult to dis-cuss mental health among juveniles
without mentioning one particular condition - posttraumatic stress disorder (PTSD). Steve Bogira, a journalist with more than 40 years of experience writing about poverty, vi-olence and mental health in Chicago, has seen and reported on the drastic impact of PTSD. Bogira is the author of "Courtroom 302: A Year Behind the Scenes in an American Criminal Courthouse."Trauma takes its toll on students
“PTSD has become a popular subject, for good reason, but it’s not a youth phenomenon. It’s been a problem for poor families in violent neighborhoods forever. We’re just now realizing the toll it takes,” he said.
Inside the classroom, as Bogira describes, the toll this condition is taking hits extremely hard.
“When people are exposed to vio-lence, directly or indirectly, it trig-gers the fight or flight impulse, and puts people on edge, makes people more likely to respond more quickly to what they perceive as a threat,” he explained. “It’s very hard for kids to focus at school, when they’re not only consciously concerned about threats to them, family, or friends, but subconsciously as well - their systems are always on guard.”
In terms of creating solutions, Bogira too sees a lack of help coming from the Chicago Public Schools.
“Schools are a great platform of intervention for kids who could use help,” he said. “What is stopping us from getting [help] in more schools? There’s a host of problems. We need a host of programs.”
A third CPS student, who also wanted to remain anonymous,
knows firsthand how the lack of proper help hinders her ability as a student. Struggling with panic dis-order, she at times is unable to focus on the material in class, instead preoccupied by worrying about a potential upcoming panic attack. Her depression can spark irritability and a lack of patience when it comes to homework.
However, she doesn’t see her condi-tions as an entirely negative deal.
“It caused me to try to fight it and taught me the lesson of vulnerabil-ity in which you shouldn't be afraid of it,” said the 16-year-old junior. “I believe I'm a stronger person today because of these mental illnesses.”
While the vast majority of mental health help in schools is dependent on CPS itself and its policies, it was evident to all three students that among their peers, awareness is de-veloping, tackling perhaps one of the biggest challenges of all.
“Awareness is finally being raised, and more and more teens are becom-ing open-minded and supportive of their peers,” said Kaylaa Velazquez.
“I feel like a lot of the older genera-tions won't believe it, but it's becom-ing more accepted by the younger generations,” said the 17-year-old Northside senior.
“People are starting to realize that depression, anxiety, etcetera don't make you entirely different. We're all human and we all have flaws,” said the 16-year-old junior.
When it comes to mental health, teens are sparking a movement of acceptance and potential solutions. CPS needs to move in the same direction.

14
She is secretly meeting another teen who is known for selling Atten-tion Deficit Hyperactivity Disor-der (ADHD) drugs at their school. The teens check to see if anyone is looking, then close and lock the door behind them. The teen quickly ex-changes her money for a small bag of about a dozen pills. Then they leave the scene with one teen carrying a plastic bag of pills and the other with a pocket filled with the profits from the sale.
This drug deal, witnessed by anoth-er 15-year-old student at the Chica-go Academy for the Arts, is happen-ing in high schools all across the city with troubling frequency, students and treatment professionals say. This teen, who asked his name not be used, has witnessed more than 10 cases of teens buying and selling ADHD medications at school, this year alone.
According to the federal Substance Abuse and Mental Health Services Administration (SAMHSA), every day about 4,000 12-17-year-olds use prescription and illegal drugs for the first time, which makes this teen one of many encountering opportunities to abuse harmful substances.
Juveniles are illegally buying and selling ADHD drugs to other teens at a profit, but the widespread sale of the drug used to treat one of the most common psychiatric disorders among children is hardly noticed by
The ABC’s of AdderallHigh school teens are illegally buying and selling ADHD medications
By Kiersten Lofton Illinois Mathematics and Science Academy
parents and officials at the schools where most of the drug sales occur.
Drug-dealing teens stimulate the market by offering two-for-one specials and free trials to encourage other students to first try and later buy ADHD drugs, students say. In addition to the sophisticated mar-keting techniques teens are using to sell the drugs, there is also peer pressure that encourages drug use.
A teen who has bought ADHD medications from another teen said, “The medications made me happy, hyper and attentive--but people looked at me and acted differently around me. It was a way of dealing with depression, peer pressure and
in general a method to escape.” Despite the fact that teens and
experts say much of the buying and selling goes on in schools, it appears school administrators are doing little to address the problem. Roch-ester High School in Rochester, Ill., The Independent Schools Associa-tion of the Central States and Chi-cago Public Schools (CPS) did not return calls or declined to answer questions about the issue. CPS also did not respond to several Freedom of Information Act requests filed about the issue.
Teens who reported selling or buying ADHD medication said that school officials had never done anything about the issue. Many school policies include disciplinary measures for misusing or abusing prescription drugs, but students say there is little enforcement.
A growing problemA 2009 study in Cincinnati found
that calls to emergency rooms related to teen ADHD medication abuse rose by 76 percent from 1998 to 2005. The study, conducted by Dr. Jennifer Setlik, Dr. G. Randall Bond, and Mona Ho, who has a master’s in emergency medicine, showed ADHD abuse calls rising faster than any other substance abuse-related calls for all age groups.
The National Institute on Drug Abuse (NIDA) also found that after marijuana and alcohol, ADHD med-ications are the substances most
Information from Child Mind Institute Children’s Mental Health Report

15
abused by Americans 14 and older. With these numbers skyrocketing, it is crucial that we find a way to prevent the misuse of these pre-scription drugs. However, before we’re able to find out how to prevent ADHD medication abuse from oc-curring, we have to find out why it’s happening in the first place.
According to the NIDA, 62 percent of teens misuse prescription drugs due to the fact that they are easy to access in medicine cabinets. In fact, 54.2 percent of teens get the medica-tions from friends or family, accord-ing to NIDA.
However, medicine cabinets are not the only way teens are acquiring these meds. Many online “pharma-cies” are selling prescription med-ications, without needing to have a prescription. For example, the sites trustedonlinepills.org and 7day-pharmacy.net offer medication for ADHD and a host of other illnesses without a prescription.
With thousands of these sites ex-isting and teens being so interested in technology, it’s crucial to beware of the dangers associated with these online pharmacies. The Food and Drug Administration has found that many of these sites sell medications that are expired, have dangerous ingredients, or are counterfeit. Some of the sites also disclose the con-sumer’s personal information such as credit card numbers, according to the FDA. The FDA says any websites offering prescription drugs online should be reported to the agency at
this link: http://www.fda.gov/Safe-ty/ReportaProblem/ucm059315.htm.
Cultural influenceFifteen-year-old Sona Fokum
believes that the top three reasons teens misuse ADHD medications are to do better in school, because they are addicted, and to deal with stress.
When asked about the topic, Sona instantly mentioned the TV show “90210” which depicts teens sell-ing ADHD medications. This show is the sequel to the well-known 1990s show, “Beverly Hills, 90210.” “90210” is a drama about a group of friends who go down many differ-ent paths such as college, singing careers and business careers. On the show, many students buy and sell various drugs; some are prescription drugs. In fact, one of the characters, Dixon Wilson, suffers from an addic-tion to Adderall, the most misused ADHD medication. Millions of teens can see this show online. In fact, many popular shows and movies in-cluding “Orange Is the New Black,” “Degrassi,” “Side Effects” and “XIII: The Series” portray it as hip and acceptable to abuse prescription drugs.
In addition to the countless num-ber of shows exposing teens to sub-stance abuse, there are also many songs making drugs seem like a smart coping mechanism. The song “Habits” by singer Tove Lo is about
a girl experiencing a breakup and trying to get over her ex. During the process, she abuses drugs, alcohol and makes other bad decisions. The lyrics read: “You’re gone and I gotta stay high all the time, to keep you off my mind...Gotta stay high all my life to forget I’m missing you.”
The artist portrays the substanc-es to be an appropriate way to get over her feelings for her ex. She also expresses the “positive” effects that come with taking the drugs: “Loosen up the frown, make them feel alive...Staying in my play pretend, where the fun ain’t got no end.” Tove Lo admitted that “Habits” is an autobi-ographical song. For teen listeners, it could be easy to get the wrong impression from songs like these and make poor decisions.
The dangers of the medications In reality, the feelings that Tove
Lo described in her song “Habits” aren't what most people experience while constantly misusing prescrip-tion drugs. Seth Eisenberg, M.D., an adolescent psychiatrist and medical director at the Illinois Department of Human Services Division of Alcoholism and Substance Abuse (DASA), said that the drugs play tricks on people’s minds. Eisenberg said that there is no proof that the drugs can actually enhance per-formance. “The drugs do make you aggressive, so for sports like foot-ball that may be helpful--but does aggressiveness mean that you’re
Information from Child Mind Institute Children’s Mental Health Report

16
how to stop the misuse of the medication
It is difficult for teens to stop abusing prescription medications if many of their friends are also doing so. For teens trying to treat their addiction to prescription medications, it’s unhealthy and an unfriendly reminder of their past to be around people misusing the medica-tions. A solution for parents with children recovering from prescription medication abuse would be to find a center designed for teens conquering substance abuse.
This way, the teen can be around people who understand what they’ve been through, set a good example and encourage them to quit. Since these medications are so powerful and addictive, it is advised to decrease the amount of medications teens are taking by 20 percent each use, rather than quitting cold turkey.
For teens who have been misusing prescription medication, contact a doctor or any substance abuse treatment center for help. Teens seeking help do not have to reveal their names under confidentiality laws; teens can simply say they are suffering from prescription medication abuse and give the details of the situation. Another option is to call 1-800-662-HELP (4357), which is a confidential ho-tline run by the federal Substance Abuse and Mental Health Services Adminis-tration. More treatment information can be found at findtreatment.samhsa.gov.

17
winning?”Some experts say that for children
with ADHD, it can be dangerous to take these strong psychoactive drugs. Taking the medications with-out having the condition and with-out medical supervision could cause even more detrimental side effects.
At first, ADHD medication reduc-es the intensity of emotional pain, shame and anxiety and gives you a feeling of well-being. Abusers of the medication say the high that the pills offer is similar to the feeling associated with using cocaine. ADHD medications like Ritalin even make things that you usually don’t find interesting to be very appealing, users say. However, these emotions typically only last for around four hours. For the first year of use, the experience may be great for teens. But later, there can be extreme con-sequences.
For teens who misuse ADHD medications, the side effects can be destructive to their health. The fact that the medication works for people with ADHD causes teens to believe the medicine could be bene-ficial to their health as well. People diagnosed with ADHD use the med-ications to balance the neurotrans-mitters in their brains. The medica-tion also affects the frontal lobe and executive functions in the brain.
Using the medication without suf-fering from the condition can cause minor issues leading to more seri-ous, long-term conditions, according to experts including Dr. Teri Collins, executive director of Maine Com-munity Youth Assistance Founda-tion, a Des Plaines substance abuse prevention organization. In fact, Dixon Wilson from “90210” eventu-ally was diagnosed with a heart de-fect after struggling with the abuse of Adderall for so long. The minor side effects of taking someone else’s ADHD medications include nausea, headaches, dry mouth and uncon-trollable shaking. Some of the major side effects are seizures, weakness or numbness of limbs, hallucination, blistering skin and difficulty breath-ing or swallowing.
There are also risks for teens who sell or give away their own pre-
scribed ADHD medication instead of taking it. For teens who have been taking ADHD medication for valid medical reasons, suddenly stop-ping can cause problems including feelings of social alienation leading to depression and possibly suicide, impulsive behavior and withdrawal symptoms. There can also be phys-ical problems from restarting the medications too quickly.
Apart from the physical and mental risks of misusing ADHD medica-tions, teens buying, selling or using the medication without a prescrip-tion could also face incarceration, probation, expulsion from school or academic failure. Teens caught misusing or selling their medica-tion might also have trouble getting needed prescriptions in the future, once medical providers become suspicious.
Teens selling their ADHD medica-tion might also become dependent on the money, causing other social problems or enabling them to buy and abuse other drugs. An Illinois therapist, who asked that her name not be used, said she witnessed a pa-tient become dependent on money made from selling ADHD medica-tions. The patient was prescribed Adderall and Clonidine but didn’t like taking his medications.
He later realized that he could profit from selling the medicine. Making $1,200 a month, the patient was able to help his family pay bills. Eventually he started using some of that money to purchase the anxiety medication Norco and selling it as well. To substitute for his ADHD and anxiety pills, he used marijua-na. One night the patient decided to snort Adderall, smoke marijuana and downed a “handful” of Norcos and Clonidine, the therapist said. The patient experienced a psychotic episode with suicidal ideations.
What can parents do?
Although parents can’t monitor their children at all times, there are steps a parent can take to prevent their teen from misusing prescrip-tion medications, or stop them if they’ve already started.
Emily Gilliam, a senior mental health family therapist from Rose-crance Berry Campus, a child and adolescent mental health treatment facility in Rockford, Ill., suggests that children of all ages should have parental supervision while taking medications. It is also important to keep prescription drugs in a safe place and properly dispose any un-used medicines.
Eisenberg suggests that parents have continuous open communi-cation with their child about all types of substance abuse and life in general. It is also important that the child trusts the parents and feels comfortable asking questions. If the child feels as if the parents judge him or her, that child may not turn to their parents while facing sub-stance abuse issues. “Teens don’t always think clearly, so parents need to guide them.”
With ADHD drugs being addictive and powerful, it’s important that teens don’t get the chance to misuse these medications, Gilliam said. If a child asks for more of their medi-cation or parents haven’t physically seen them take the medication in a while, that should immediately raise a red flag, Gilliam said.
A few other signs of ADHD medica-tion misuse are staring eyes, mood changes such as irritability, secre-tive behaviors such as whispering on the phone at night, having a greater or lesser amount of money than usu-al (greater goes with selling, lesser goes with buying), grades going significantly up or down and the in-ability to sleep at night while instead sleeping during the daytime.
The misuse of these medications has nothing to do with race, gender or socioeconomic status. However, it can sometimes be related to one’s environment. The misuse of pre-scription medication in general is more of an issue in high schools than in earlier grades. Collins found that most teens begin using these medi-cations just to experiment and have fun. Teens will experiment in groups of friends and not think about the consequences.

18
Reporter Christian Thorsberg interviewed high school student
Kaylaa Velaquez about her struggles with mental illness. She is a junior at
Northside College Prep.
Christian Thorsberg: What personal experience have you had or do you still have with mental health?
Kaylaa Velaquez: I struggle every day with bipolar disorder, manic depression, PTSD and anxiety. My grandmother had schizophrenia and my mother had post-partum depression. Many of my close friends suffer from depression and/or anxiety disorders.
How long was it before you realized you had a problem?
I had felt this overwhelming sadness and panic for years. No one realized until I finally told someone about my suicidal ideation and self-harm.
Did you have this mental health trou-ble while at a CPS school?
Yes, I do. I've suffered from this since sixth grade. I went to O.A. Thorp Scho-lastic Academy and am currently at Northside College Prep
At your school, regardless if it was CPS, did you feel you had adequate personnel (counselors, therapists, etc.) that you could feel comfortable openly talking to? Did you even try to seek help at the school - why or why not?
The counselors at my old school worked tirelessly to try to help me, though they didn't really understand. At
Talking with CPS students about mental health
Northside, my assigned counselor made me feel even worse, until I met the social worker who accepted me, opened up to me and cared for me. I finally got help because of him and I truly believe he saved my life.
Who do you see as some of the more approachable people at the school to talk to about your mental health?
Mostly teachers that I was close with, and social workers at the school. Currently I talk to my therapist and my friends because they understand where I'm coming from and support me fully.
How did this mental health problem affect your school work, relationships with others, daily lives?
Depression made it extremely difficult to get out of bed, let alone go to school. Paying attention in class got extremely difficult and I began having panic attacks over tests and assignments. My PTSD could only be quelled by medication that put me to sleep, not allowing me to finish my work. I felt constantly suicidal, isolating myself from everyone I loved. It was increasingly difficult to find the energy to even cry over the stress.
What did you do once you came to this realization?
When I found out I immediately went to my mother and begged her to take me to the doctor. She didn't believe me and so I purchased some over-the-counter supplements to try to make the ideation go away. When that didn't work I ended up trying to take my life, which sent
me to a hospital for a week. After the hospital, I was finally able to receive treatment
To this day, do you feel you have received adequate help? If so, from where? If not, why not?
I do believe I received help, but far too late. I still struggle with my mental health and have to take medication and go to a regular appointment with my psychiatrist every week. Though I do this, there are still so many bad days and even weeks. My social worker at Northside and my mother pushed things along to get me the help I have now.
From your experience,is your school doing a good job with helping you with your mental health troubles?
Yes. Northside has incredible social workers and counselors who make sure that I am accommodated in all of my classes. My teachers do their part as well. Checking in with me every class and being understanding when I need extensions.
What have you seen as some of the biggest problems surrounding mental health and teens?
It's the stigma. Teens don't want to have that label attached to themselves. Feeling it makes them inferior to their peers. They don't want to stand out or make their friends view them differently. They see it as taboo.
What are some of the biggest suc-cesses surrounding mental health and teens?
Awareness is finally being raised, and more and more teens are becoming open minded and supportive of their peers. The stigma regarding medication is slowly being taken apart
By Christian ThorsbergNorthside College Prep

19
From what you have experienced, with CPS in general, what remain the largest problems, in terms of giving help to students with mental health issues?
The largest problem is teachers that are not educated on the subject, struggles and feelings of someone with mental health issues. Schools that punish chil-dren for being late, not showing up, or not doing their work instead of working with them to fix this make it really diffi-cult for everyone.
What personal experience have you had or do you still have with mental
health?My largest struggles would have to be
having eating issues and having an ex-treme amount of stress. The stress prob-ably set off the eating issues, but I'm not too sure where stress falls on the mental health spectrum. And this year is going to be so stressful. I don't like to catego-rize my eating habits as anorexia due to the fact that I don't think it escalated to that point, however I would call it having an constant anorexic mindset. Would they be considered the same thing? I'm not too sure but I'd like to think they're
not. I still face issues with my body and with eating, and, to be honest, if I didn't have a hawk-like mother, I would be in a much worse situation right now, which is why college will prove to be interest-ing.
What contributed to your mental health trouble?
Schoolwork, extracurriculars and applying to college. Most of the time I could ignore the little voices in my head telling me not to eat, that I wasn't thin enough. But then junior year hit and it was hell. I was loaded with all of these things going on - or more like too many things going on. On top of taking the ACT, APs, SAT subject tests, swim team, Student Council, yearbook, Samulnori, Isang Hakbang, Soran, NHS, Spanish Honor Society, Math Honor Society and PIECE, I still had to keep my grades up. It was the idea that I wouldn't get into college, so I just piled up more onto my plate. Not only that, but I felt like I had to keep up my image - or something of the sort. It was just an extreme amount of pressure and stress. I don't think that I was truly happy most of the year. Often
times I would just start crying for no rea-son. I started watching what I ate more, and I was just too worn out to tell that little voice in my head "no." I thought that if I became thinner or prettier, then people might also like me more.
How long was it before you know real-ized you/they had a problem?
I never thought of it as a 'problem,' but one day my mom and I got into a big heated discussion of my eating habits, and then the week after I kind of realized it. My case wasn't as severe as other people due to the fact that I most of the time was able to still eat normally even though I felt terrible, and to be honest it still is kind of weird to think that it's a problem because I've always been this way, but I think I'm slowly accepting it more. I'm not too sure what to call stress and anxiety and unhappiness though; it's definitely something, but I don't know whether to call it a problem or just life. Maybe I just haven't hit my realization for that yet.
Did you have this mental health trou-ble while at a CPS school?
In my suburban middle school -- I moved to Chicago for high school from Arlington Heights -- I would say that I experienced something closer to depression due to bullying. But while at Northside College Prep, a CPS school, I experienced stress/anxiety and eating issues during junior year mainly, some of freshman year, and it is almost a guaran-tee that I will experience the same thing next school year as a senior, possibly much worse. The summer has given me a little bit of breathing room, but not much.
At your school, regardless if it was CPS, did you feel you had adequate personnel (counselors, therapists, etc.) that you could feel comfortable openly talking to? Did you even try to seek help at the school - why or why not?
I was scared to go to the school coun-selor, so I had to have a friend take me and go with me. The only inconvenient thing is that the whole ebb and flow thing happens randomly, so once I felt miserable in the middle of orchestra, but it's not like I can just ditch class to go to the counseling office. What ended up happening was that I just stood in the back of the classroom with a box of

20
tissues and just cried. When I hit my breaking point, most of the time I go to talk to a counselor, but sometimes he's unavailable or talking to someone else. I don't really talk to anyone at school about my eating habits.
Who do you see as some of the more approachable people at the school to talk to about your mental health?
The only person I am completely hon-est with is my friend. Once, in the middle of Samulnori practice, I locked myself in the bathroom for a half hour and then when I came out he gave me tissues and sat with me while I cried. Sometimes he's not too sure how to react. I don't blame him either, I would be too. Or other times he's not available, but when I really need him, he's always there for me, and for that I am so grateful.
How did this mental health problem affect your school work, relationships with others, daily life?
School work not too much; it was a struggle but I maintained all of my grades. What was more impacted would probably have been my relationships with others. While I felt like everyone else was so happy, I felt miserable all of the time, like I was two seconds away from bursting into tears, tired all of the time, and constantly feeling sick. But I couldn't tell anyone that. I felt like peo-ple didn't like me as much as before, and I felt distant from a lot of people. Even though I feel like I know many people and am friends with them, I'm really only honest with my friend, and some-times it can feel a little isolating because it seems like no one else would under-stand or accept me. But don't get me wrong. I definitely had so many happy moments last year and lots of fun!!! For some, every day is a battle. For me, it was more ebb and flow, like a wave.
What did you do once you came to this realization?
The week after said big argument with the eagle mother, I made a status about it on Facebook (I think this was around mid-June this year) and while I was typ-ing it, my fingers were shaking. I didn't want people to judge me and for them to change their opinion of me, because I had this image that I wanted to uphold, and I was scared to show people how imperfect I really was. I wanted to keep
quiet about it, but if people can't love me for who I am, then they aren't true friends. If even one person could learn from my experiences, then no matter how scared I felt, it would be worth it. People's view of me probably changed a lot, but that's okay. I don't need the whole world to like me, and it's okay if they don't!
To this day, do you feel you have received adequate help? If so, from where? If not, why not?
I think it'll always be something that I struggle with. I don't think it's some-thing that will ever really go away, but the key is to be able to ignore it and to be able to live your life without it taking control. I think that I did get adequate help, but at the same time I think it's also a very personal thing and each person has to come to a realization by them-selves, because no matter how much they're preached at, it won't necessarily make them accept it.
From your experience, is your school doing a good job with helping you with your mental health troubles?
I would definitely say that my counsel-or really did help me a lot throughout the year, but that was because I sought him out freshman year and felt comfortable doing so. I feel like if you're not comfort-able getting assistance when you need it, it would be a lot harder getting the necessary aid.
What have you seen as some of the biggest problems surrounding mental health and teens?
I think that it's a lot of different things. There are definitely resources, but I would say that most people don't feel comfortable accessing them, as well as the fact that a lot of people don't talk about their mental health. Mental health isn't something that can just be taken care of by itself, but rarely do you see people talk about their mental health at lunch or in the hallways. When people socialize, they feel the need to show their best self, and I think that we have to come to the realization that it's okay not to be happy 100 percent of the time. There's also this stigma that if you go to the social worker, you're crazy and need help when that's not even the case. The social worker is just an adult friend, but not everyone can see it that way.
What are some of the biggest suc-cesses surrounding mental health and teens?
Probably the fact that society and people are accepting that mental health is just as important as physical health. A lot of people think that it's unnecessary, or a common view that people have is that if you're depressed, just go out and do something that makes you happy or just stop being gloomy. The thing is, it doesn't work like that, and while I feel like a lot of the older generations won't believe it, it's becoming more accepted by the younger generations. For in-stance, my when my parents found out that I talked to my counselor, they were very unsupportive of it, while my sister definitely supported me a lot more.
From what you have experienced, with CPS in general, what remain the largest problems, in terms of giving help to students with mental health issues?
I think CPS has done a lot, but at the same time a lot more could be done. At Northside we talk about mental health a lot, but I feel like not enough. We have an awareness week and the bulletin board outside the social worker's office changes every month, but other than that, not much is done. Why not have an assembly? Why not have a spirit week? Student Council did a stress-free week a few years back and handed out stress balls and tea, but why should it have to be the council who does it? Why can't the administration? Also, why is the social worker's office so hard to find? It should be more easily accessible.
Is there anything else you would like to add regarding your mental health experience, and specifically, mental health in CPS?
I can only speak from my experience at Northside, but I definitely did get a lot of help from my counselor as well as the social worker. On another note, howev-er, it was also the school itself and the stress that caused my case to worsen and caused me to have to seek out aid. I feel like CPS has all of the basics of mental health down; social workers, counselors, mandatory mental health assignments done in advisory. But I feel like it needs to be taken a step further.

21
In her article, "Minority Youth: Needs for Mental Health Ser-vices Grow with Population,"
Miwa Yasui, Ph.D., discusses how minorities are often not able to find and/or utilize proper mental health treatment. Among a variety of caus-es, including stigma, logistics and lack of money, Yasui cites one other reason that many would find more surprising: minorities underutilizing services that are available. It was not until speaking with Yasui that this problem became much more clear, and it’s true weight, evident.
While it “has taken decades for [mental health] needs to be brought to attention,” said Yasui, in 2015, the newest “goal is reducing the dispar-ity.”
There is a disparity in resources, knowledge, but most importantly, the workplace. According to Yasui, the mental health care profession has been dominated previously by white males, and now, white fe-males. This fact stems directly from social inequalities.
As Yasui described, “to be a [men-tal health] provider, you have to get an advanced degree,” and of course when it comes to college, “certain races are definitely favored. There are more resources -- college plan-ning, school, money -- for some, and
less for others.” Thus, there is a selection bias when
it comes to graduate school, and professional training, resulting in an ethnically one-sided distribution of mental health care professionals. With a lack of role models in the profession whom minorities can relate to, the powerful stigma regard-ing mental health in many minority cultures is increasingly augmented.
“The stigma in some cultures prevents youth from seeking men-tal health, psychology and social services,” said Yasui. In turn, mi-nority youth who aspire to study and become a mental health care professional are quickly shrinking in numbers. If seeking help is consid-ered taboo, giving help would be seen as even stranger. Consequently, what Yasui calls “generational distrust” continues. And, as Yasui wrote, with the number of minority youth greatly increasing by the decade, the cyclicality of this issue will not be slowed, and the number of mental health care providers will continue to decrease.
So, what needs to be done to in-spire minority youth to be more open about mental health, and not be afraid to venture into the study of a topic seen by their culture as foreign? There “needs to be a part-
nership between communities and providers.," said Yasui. "It would be nice to see providers determined to cater to the needs of their own communities. There would be less of a stigma and a dissemination of information.”
Whether it has been publically accepted or not, the minorities of today will soon be the majority of tomorrow. It is up to those first few brave souls to pave the way for their cultures, reducing the stigma of mental health, and raise awareness of the importance and significance of the topic.
Lack of diversity in mental health profession leads to generational distrust
By Christian ThorsbergNorthside College Prep
Miwa Yasui, Ph.D., assistant professor at the University of Chicago’s School of Social Ser-
vice Administration, met with members of the I-Team in her office at the University Chicago.
She discussed the growing need for mental health services for minority youth.

22
Many students, teachers and advocates feel Illinois schools lack the proper
resources to help teens coping with substance abuse and related mental health issues. Maine Township hap-pens to be one of the communities fortunate enough to have a well-re-garded program to prevent and treat substance abuse among teens.
In 2001, Steven Snider, superinten-dent of District 207 at the time, and Rose Garlasco, assistant principal of Maine South High School, created a program called Maine Community Youth Assistance Foundation.
MCYAF serves all of Maine Town-ship, which is around 135,000 people. According to Theresa “Teri” Collins, Ph.D., executive director of MCYAF, the organization looks for solutions that can change the en-tire community. Since the program serves thousands of people, it was given a 10-year drug-free community federal grant from the White House.
Since then, MCYAF has continued to grow, relying on federal, state and private funds.
MCYAF informs teens of the dangers of substance abuse through youth group events, going into schools and communities, town hall meetings, summer programs and various other methods. Although their focus is on substance abuse prevention, they also help teens dealing with substance abuse issues. MCYAF partners with churches, po-lice departments, park districts and schools. Through these partnerships, they are able to provide teens facing substance abuse issues the proper treatment.
“When people hear the term mental illness, they think of schizophrenia, but substance abuse is one as well,”
said Collins. Commonly abused substances interfere with the way neurons send, receive and process information. Substance abuse is of-ten a way that people self-medicate the symptoms of mental illness. The National Bureau of Economic Re-search reports that people diagnosed with a mental illness are responsible for 84 percent of the consumption of cocaine. Experts believe that one triggers the other. Many substances such as alcohol can trigger depres-sion. However, a patient with de-pression may use marijuana for pain relief.
Collins believes that teens tend to abuse certain substances due to the perception that these substances are not harmful.
Misunderstood substances include marijuana and prescription medi-cations. With the use of marijuana being legal for recreational and med-ical purposes in more than 20 states, Collins says that teens are getting
Just say know!With substance abuse and mental illness, one can trigger the other
Profile: Maine Community Youth Assistance Foundation
By Kiersten Lofton Illinois Mathematics and Science Academy

23
the impression that marijuana is healthy and safe.
The same thoughts are associated with the misuse of prescription med-ications. People may also believe that smoking marijuana or other sub-stances through hookah pens is not harmful because they are inhaling water vapor. Certain hookah pens have flavor names like Jungle Juice and Crazy Apple that suggest they are made for kids. Some people even believe that hookah pens are similar to ice cream since they share a com-mon ingredient, propylene glycol.
Instead of punishing teens who make the wrong decisions about these harmful substances, MCYAF educates them. Collins says that MCYAF believes in the “Just Say Know” approach, rather than the old philosophy, “Just Say No.”
The organization has teamed
up with police officers to create a program for teens who are caught with substances. Teens can either choose to pay $1,000, get their li-cense revoked, and have the incident reported to the Secretary of State, or they can participate in educational classes at MCYAF. Collins said that 80 percent of teens have chosen the option to go to MCYAF and become educated.
Collins believes that parents should talk to their kids regularly about sub-stance abuse, be around them and pay attention to them. “Too many children die or become severely injured before a parent ever notices their child is suffering from sub-stance abuse,” she said. “Since the symptoms from certain substanc-es aren’t always noticeable in the beginning, it is important you watch your teen.”
Many teens tend to experiment with substances for fun with their friends, so parents should also be active in their child’s social life. Knowing where their child is, who they’re with and who is supervising is essential when trying to prevent a child from using substances.
If you or a teen you know is coping with substance abuse, or for general information about MCYAF, call or text (847) 858-7090 or visit their website at www.mcyaf.com.
Theresa “Teri” Collins, Ph.D., executive director of Maine Community Youth Assistance Foundation (MCYAF), said that teens tend to abuse cer-tain substances due to the perception that these substances are not harmful.

24
Depression is a mental illness that affects 20 percent of teens. It can lead to sub-
stance abuse, eating disorders and suicide--the second leading cause of death for 15-to-24-year-olds.
But depression can also result in a resilient character.
According to Families for De-pression Awareness, more than 85 percent of teens improve from depression with a combination of medication and therapy. Paige Gesic-ki, a 26-year-old clinical intern at the National Alliance on Mental Illness (NAMI), was one of the people fortunate enough to receive proper treatment for depression.
“Everyone has their own dreams and expectations that maybe you’re putting on yourself or your parents are putting on you,” she said. “High school is a hotbed for that--what college are you going to go to? What are you going to do? [My dream] was to go to Notre Dame. My sister had gone there and it was important for my family to go there. I thought I would get in, so when I didn’t get in, it felt like a big blow to my ego.”
Paige instead went to Wake Forest University in Winston-Salem, N. C.,
for her freshman year of college.Already disappointed in herself,
Paige experienced complete culture shock at Wake Forest.
“I went from knowing everyone in this tiny school where I’m from in New Jersey, being confident, good at basketball, and feeling good about myself, to going to college. It was a really hard transition for me. I didn’t know anybody. I didn’t fit in at all. I also felt like my friends at home were having a great time at college. We’d come home to share our stories from college and I’d wonder why I didn’t have those experiences. I felt so lone-ly and weird at school.”
Paige started using negative cop-ing skills in order to mask what was really going on inside. She partied, stayed out late and turned to harmful substances, only making her symp-toms worse. Paige began to feel as if her life was plummeting. Eventually, ashamed of her actions, Paige went through a period of social isolation.
“I really liked to talk and was out-going, but after my partying stage, I became an unrecognizable version of myself,” she said. “Any social thing was completely beyond my energy level. I stopped going to the dining
hall; and not because I was scared of gaining weight or anything, but be-cause food didn’t taste like anything to me anymore. I also didn’t want to have to deal with talking to anybody, so if I didn’t leave my room no one
'Mom, I think I'm depressed'
By Kiersten Lofton Illinois Mathematics and Science Academy
How Paige Gesicki fought mental illness
Paige Gesicki, a graduate student at Loyola University, suffered
from mental illness in college. Last summer she worked as an
intern for the National Alliance on Mental Illness in Chicago.

25
'Mom, I think I'm depressed'
could see me.”Paige went to see the movie “Elf ”
with friends right before Christmas break. “Everyone was pumped be-cause they got to go home and school was over.” They ordered wings and had a small celebration.
“But I just could not stop crying.” She was sobbing badly and “it got
so normal to [her] that [she] thought it was OK to just sit in a room filled with people and cry like that.”
Paige remembered that one of her Wake Forest friends asked in a hostile tone: “What is wrong with you? We’re going home, we have no school, you have nothing to stress out about in your life. What is wrong with you?” Depression sets in
Paige felt betrayed and upset with her friend, and didn’t know how to express what she was feeling. “I don’t know what’s wrong with me. I wish I did,” she said.
The feeling reminded Paige of a moment from high school, when her Spanish teacher opened up to the class about depression.
“[The teacher] was really funny and eccentric and after class we’d all be like, ‘Oh my god, did you hear what she said in class today?’ She would always just say really funny things. One day she just stopped class in Spanish and started speaking in English; it was a really intense class that day. She wanted us to under-stand what she meant. She talked about this loneliness that she had, and disconnection with the world around her. And she called that the dark night of the soul. I didn’t think about that again, but the way she described it felt so intense to me and the words she put on it had such gravity. I didn’t think about it again until I was in college.”
Spurred by that memory, Paige called her mom and said, “I think I’m depressed.” Since mental illness runs in Paige’s family, she was able to use that language without worrying about her mom not understanding or being judgmental. Her mom was accepting and said that once she got home, she would take care of her.
Paige’s plan was to go home for a while, then once she felt better she would return to Wake Forest. When she got off the plane, arriving in New Jersey, her parents looked at her and said ,“Who is this zombie version of my daughter?” Paige remembered. Paige had lost 15 pounds and didn’t have the will to smile or engage with anyone.
She explained that being depressed had been so unbearable that she picked a particular bench out at school and fantasized dying on it. “I don’t know why. It was kind of in a quiet part of campus and I just had this fantasy of going there and just laying down and dying. My plan was just like, ‘I can’t keep doing this be-cause this is so painful and it would be better if I wasn’t here because I don’t want everyone else to have to deal with whatever this is.’”
Paige’s mother helped her get care, and at age 19, Paige was diagnosed with depression. She went through a long process of going to different doctors, counselors and psychi-atrists in order to find the right treatment.
Paige and her mother ultimately decided that medication would be the best method for her. They went to New York City to see a specialist. Waiting for drugs to kick in
“What happens with medications is that it takes a long time to work out how to get the right fit for you. Some ones they try and just don’t work out. I will never forget this one. I felt terrible side effects where you felt like your skin was crawling, which is a terrible image to have. I remem-ber being in the back of the car and telling my mom, ‘My skin is crawling. Take me to the hospital!’ ”
Eventually, however, Paige got med-ication that worked began recover-ing.
“The getting better process-- I don’t even remember. It was that intense,” she said. “Your mind actually blocks all of it out. Like apparently I was sleeping on the couch for two weeks or so in this huge puffy jacket, be-cause I just wanted to disappear. So
I would just sleep there in and out of waking up and crying and in and out of consciousness. And apparently my friends came and visited me and I really just don’t remember this. But, I slowly did get better with the right medication and with time. I didn’t have the luxury of saying, ‘Eh, I have time, I can wait.’ I had to be like, ‘It’s go time. Let’s do it.’ ”Moving on after treatment
Although she never went back to Wake Forest, Paige still keeps in contact with friends there. “My par-ents drove down, withdrew me and moved everything out of my room. I had to tell all of my friends that I wasn’t coming back and I don’t think they were surprised.” Paige ended up going to a nearby school so she could commute from home and go to the doctor.
Paige got her social life back with friends from her hometown, and she was able to get back on routines such as her sleep pattern. She got a gym membership and started working out which was a big step for her.
Paige decided that it was time for her to reapply to Notre Dame. Her sister and her brother were there at the time. Paige ending up getting in and since she had a support system and felt better, she decided to go. “It was a huge thing of my life that I end-ed up getting into Notre Dame.”
Paige currently lives in Chicago and is studying for a master’s degree in social work. She is living a pro-ductive and vivid life -- “I laugh all the time.” Her goals are to be a mom, a social worker and to finish getting her master’s degree.
“If you would’ve met me when I was at Wake, you wouldn’t have recog-nized me for the person I am today. And also if I hadn’t asked my mom for help, there would probably be someone else here from NAMI giv-ing you this speech because I don’t think I was going to make it if I didn’t ask for help.”
If you or someone you know is strug-gling with depression, call the NAMI hotline at (800) 950-NAMI (6264) or text “ANSWER” to 839863.

26
Many people think they understand mental illness. But they often have the wrong ideas about what it is and how it affects people.
Because of stigmas and stereotypes that surround mental illnesses, many people look down on those who suffer from mental illness, instead of being understand-ing and giving a helping hand. But, the majority of stig-mas and stereotypes around mental health are based upon opinion rather than fact. That leads to discrimi-nation against people with mental illness. The National Alliance on Mental Illness (NAMI) notes that sudden feelings of being overwhelmed, severe mood swings, drastic changes in behavior or feelings of hopelessness are all signs of a possible mental imbalance. Here are some of the major myths and realities surrounding different mental illnesses. Bipolar disorder
Myths:• Everyone who deals with bipolar disorder is a tick-
ing time bomb, and they are not safe to be around.• Bipolar disorder is a very rare health condition.• Bipolar disorder is just another way to say that
someone has mood swings.Reality:• People who suffer from Bipolar Disorder are not
overly aggressive, though they can have manic periods.
• Bipolar disorder affects about 5.7 million Ameri-can adults, or about 2.6 percent of the U.S. popula-tion 18 and older, according to the National Insti-tute of Mental Health.
• The mood swings that come with bipolar disorder are completely different from the mood swings that many healthy people experience.
PTSDMyths:• Everyone who goes through a very life-threatening
event will get PTSD (posttraumatic stress syn-drome).
• Only soldiers who have fought in a war get PTSD. • Those who suffer from PTSD cannot function at
all. Reality:• Most people who are exposed to a traumatic event
will not get PTSD at all, and many see a natural decrease in symptoms over the months following an incident. The number of people who receive a diagnosis after a PTSD-level event is less than 10 percent, according to WebMD.
• PTSD is not as common as many people think; about 7 to 8 percent of people may experience PTSD during their lifetime, according to the U.S. Department of Veterans Affairs.
• Even though the symptoms can be severe, people with PTSD can still live a regular life.
DepressionMyths:• Staying busy by doing very tedious work can help
someone dealing with depression.• Depression is not a real illness, and those who
claim they have it are just seeking attention.• Depression is nothing but self-pity or regular
sadness.Reality:• Doing extra work to keep busy does not help de-
pression; it can actually hinder recovery if you are avoiding what is really going on.
• Depression is in fact a real illness, and it is one of the top sicknesses for American adults, according to WebMD.
AnxietyMyths:• If a person hyperventilates they are suffering from
Anxiety.• If you eat right, exercise, avoid caffeine and live a
healthy lifestyle, your anxiety will go away.Reality:• Anxiety goes beyond symptoms like hyperventilat-
ing; it is an ongoing debilitating feeling of anxiety that can come and go.
• Exercise, avoiding caffeine and other healthy lifestyle choices can help someone dealing with Anxiety but it won’t cure the condition.
Schizophrenia spectrumMyths:• If your parents have schizophrenia (hallucinations
or disorganized thinking), you will likely have it also.
• Those who suffer from schizophrenia are the epit-ome of mental illness and need to be in a mental health institution or “asylum.”
Reality:• It is not always common for a child to have schizo-
phrenia just because his or her parents may suffer from it. In some cases these disorders will skip generations and may not even get passed down.
• Schizophrenia is usually made to seem as though it is the most common mental illness, while it is actually one of the rarest.
Mental illness: Myths vs. realityBy Brandon SpencerUrban Prep Academy, West Campus

27
Approximately 1 in 5 youth aged 13–18 (21.4%) experiences a severe mental disorder at some point during their life. For children aged 8–15,
the estimate is 13%.
An estimated 26% of homeless adults staying in shelters live with serious mental illness and an estimated 46% live with severe mental
illness and/or substance use disorders.
Approximately 20% of state prisoners and 21% of local jail prisoners have “a recent history” of a mental health condition.
70% of youth in juvenile justice systems have at least one mental health condition and at least 20% live with a serious mental illness.11
Only 41% of adults in the U.S. with a mental health condition received mental health services in the past year. Among adults with a serious men-
tal illness, 62.9% received mental health services in the past year.
Just over half (50.6%) of children aged 8-15 received mental health services in the previous year.
African-Americans and Hispanic-Americans used mental health services at about one-half the rate of Caucasian-Americans in the past year and
Asian Americans at about one-third the rate.
Half of all chronic mental illness begins by age 14; three-quarters by age 24. Despite effective treatment, there are long delays—some-
times decades—between the first appearance of symptoms and when people get help.
Did you know? Facts about mental health
Source: NAMI (National Alliance on Mental Illness

28
Some of Chicago's school children may face cognitive deficits and possible future
trouble with the law because of lead poisoning, which causes neurolog-ical problems including lower IQs and attention-deficit disorder.
"In Chicago, the number of children with lead poisoning is four times the national average, and the problem is concentrated in our most-distressed neighborhoods," Anne Evens, former director of lead poisoning prevention at the Chicago Department of Public Health, wrote in a blog published August 4th. "Exposure to lead can cause brain damage which can lead to learning disabilities and violent behavior later in life."
The Illinois Department of Public Health reported in 2013 that 278,000 children were tested for lead poi-soning and 20,100 had blood lead levels higher than 5 micrograms per deciliter (µg/dL), which the Centers for Disease Control uses as a refer-ence level. In 2013, 1,000 Chicago children were diagnosed with high levels of lead.
This is such a serious national problem that the U.S. Centers for Disease Control and Prevention (CDC) holds a National Lead Poisoning Prevention Week annu-ally. This year's observance occurred
October 25-31, 2015.The National Institute of Environ-
mental Health Sciences funded a study that reported that lead expo-sure lowers children's IQs, said Kim-berly Gray, Ph.D., a NIEHS health science administrator.
Evens and her co-authors analyzed the lead tests and test scores of 58,000 Chicago children. The tests showed that lead exposure in early childhood significantly increased the chance of failing at reading and math.
The blog notes that a University of Cincinnati study found that as teens, children exposed to lead were more likely to commit crimes.50 children die in Chicago
The late Chicago Alderman Leon M. Despres devoted a chapter to lead poisoning in his book, "Challenging the Daley Machine: A Chicago Alder-man's Memoir."
The chapter is titled "Chicago Children Die from Lead Poisoning." Despres wrote in the late 1960s that 50 children had died from ingesting sweet-tasting lead-based paint flakes in their homes. Their parents were unaware that the paint was causing a slow death and mental-health prob-lems for their children. He called the
deaths an epidemic.Despres and other alderman intro-
duced an ordinance declaring lead-based paint a public nuisance. If the ordinance had passed, the buildings' tenants or the city could then compel the owner to abate the lead.
However, the legislation was sent to committee where it died after Sam-uel Andelman, M.D., commissioner of the Chicago Department of Public Health, said it would be difficult to determine the amount of lead in paint products.
Later, the city council passed a weaker ordinance, which didn't declare buildings with lead paint a nuisance, but did allow CDPH employees to gather and test paint samples. City officials can inspect private homes and buildings for lead under the Lead Laws of the City of Chicago, which are intended to prevent and reduce the occurrence of lead poisoning among Chicago children.Freddie Gray
The awareness of the effects of lead-paint poisoning burst on the na-tional scene this year although many did not realize it. Freddie Gray’s April death while in Baltimore police custody sparked days of violence in
Lead paint poisoning threatens students’ academic achievement and livesChicago has high levels of lead paint because of its old housing stock
By Frederick H. LoweI-Team Project Manager
Freddie Gray, who died while in Baltimore police custody, suffered from lead paint poisoning as a child.
Cou
rtes
y Fa
lcon
& M
urph
y /
MG
N

29
Charm City. It was later revealed that Gray suffered from lead poison-ing, according to a 2008 lawsuit filed in Baltimore Circuit Court.
In the home where Gray lived from 1992 to 1996, the windowsills shed white chips of paint. The area most affected by paint flakes was the living room where Gray slept, the Washington Post reported.
Gray, who was often suspended from school, didn't complete high school. He suffered ADHD (attention deficit hyperactivity disorder). His siblings were also either diagnosed with ADHD or ADD (attention defi-cit disorder), according to the law-suit. The family sued the building's owner and the lawsuit was settled out of court.Landlord goes to prison
One of the first legal cases against a property manager who used lead-based paint occurred in Manchester, N.H., when James T. Aneckestein and his company, JTA Real Estate Brokerage and Property Manage-ment, pled guilty to a number of charges, including failing to provide prospective tenants with lead-based paint disclosure information as required by federal law, according to
the U.S. Environmental Protection Agency.
The federal government charged Aneckestein in 2000 following the death of Sunday Abek, a two-year-old Sudanese girl who lived with her family in one of the buildings man-aged by Aneckestein's company.
The NIEHS warns that young chil-dren under the age of five are partic-ularly vulnerable because their bod-ies, brains and metabolic processes are still developing. Two-year-olds tend to have the highest blood-lev-el concentration because they put many things into their mouth, in-cluding toys and other products that contain lead. Sunday played on her apartment's building's wood porch, where she often ate paint chips, ac-cording to legal documents. Aneck-estein was ultimately ordered to pay Mary Alorout, Sunday's mother, $700,000. He also was sentenced to 15 months in federal prison.Mental health problems
The NIEHS at one time reported that adverse health effects in both children and adults occur at blood levels below 10 µg/dL and some below 5 µg/dL.
In a 2014 study, NIEHS said the
CDC now uses a reference level of 5 µg/dL to identify children with blood lead levels that are much higher than normal.
"Emotional and behavioral prob-lems show up even with low expo-sure to lead and as blood lead levels increase in children so do their problems," NIEHS reported.
When he was 22 months old, Fred-die Gray had 37 micrograms of lead per deciliter in his blood. Lead hides in older buildings
In addition to paint in the interior and exterior of buildings constructed before 1978, lead can be found in the soil, drinking water, some imported toys, old toys, lead-glazed pottery, plaster and some artist paints. The U.S. Product Safety Commission banned lead in paint, a popular and inexpensive additive, in 1978 for use in house-painting.
So why does Chicago still have a significant lead-poisoning problem?
Emile Jorgensen, an epidemiologist at the Chicago Department of Public Health, wrote in an email that it's because Chicago has old housing stock especially on the South and West Sides.
Homes built prior to 1978 have lead-based paint, according to the Illinois Lead Program 2013 Annual Surveillance Report. The surveil-lance report noted that 3.4 million homes were constructed in Chicago prior to 1978. Some 2.1 million had lead paint and 1.4 million had signifi-cant lead paint.
In fiscal year 2014, the CDC gave Chicago $347,375 for lead abate-ment, said Eddy Kaka, the program’s contact person.
The Illinois Department of Public Health notes that Illinois has re-ceived $4.4 million from the CDC’s Healthy Homes and Lead Poisoning Prevention Program, but the funds have been declining each year lead-ing to cuts in services.
In her blog, Evens notes that Chi-cago has one of the strongest lead-based paint ordinances on paper. But, she complains, "inspections are few and enforcement is spotty.”
Info
rmat
ion
from
Nat
iona
l Ins
titut
e of
Env
iron
men
tal S
cien
ces

30
In the spring of 2015, newspa-pers had written the obituary for Community Counseling Cen-
ters of Chicago, or C4, for weeks. But CountyCare -- Cook County's
Health & Hospitals System's Medic-aid health plan -- took C4, provider of outpatient psychiatric services for adults and children, off the obituary page and put it on the news page.
Community Counseling, or C4, was scheduled to close at the end of May be-cause of financial problems, but a deal with CountyCare, gave C4 new life.
The deal expanded C4's patient coverage. In addition, C4 named a new interim executive director.
In a published statement, Coun-tyCare said, "In light of a the new agreement, C4 will remain open and continue to provide services to both the new CountyCare popula-tion served under the agreement, as well as to its current consumers."
C4, one of the largest providers of mental health services in Cook Coun-ty, was founded in 1972 to help people released from psychiatric hospitals
Once financially troubled C4 can now see a future
into Chicago's neighborhoods Edge-water and Uptown. The organization provides mental health counseling, crisis counseling, substance abuse treatment, and it is the largest pro-vider of crisis services for children.
C4's philosophy is, "People with men-tal illness recover best in the commu-nity, not institutions, where they can be supported by family and friends."
The facility, which has four locations, serves 10,000 low-income clients annually. More than two-thirds are African-American and Hispanic. Fifty-two percent are children.
The deal’s financial as-pects are not known.
C4 officials, however, sent letters to nine state lawmakers pleading for $1 million to remain open, ac-cording to several news reports. During fiscal year 2013, C4's an-nual budget was $17.1 million.
"This (funding) comes at a criti-cal time for our consumers and our employees. The agreement pro-vides C4 the opportunity to serve an expanded patient base through
CountyCare," said Eileen Durkin, who was C4's CEO at the time.
CountyCare was established in 2013 as a health plan for adults newly eligible for Medicaid under the Affordable Care Act. CountyCare recently expanded to include tradi-tional Medicaid populations, includ-ing children, adults with dependents and seniors with disabilities.
In the coming months, C4 plans to expand its behavioral health capacity by finding innovative ways to serve clients through a network of provid-ers commensurate with that growth.
"The deal also provides the sta-bility we need to serve our current consumers, as well as continuing to be able support our dedicat-ed employees," said Durkin.
Chris Carroll, who was named C4's interim executive director, replaced Durkin on July 13, 2015. Carroll is not new to C4. He has served its consumers in many capacities for over 25 years.
He began his career at C4 in 1990 as a crisis worker for the organiza-tion's Screening Assessment Support Services program (SASS). Later, he became SASS program director. He also was vice president of Crisis and Justice Services. In that role, he headed the largest program for children and adolescents in Illinois.
In addition, Carroll served as direc-tor of C4's Adult Emergency Services' on-call team for overnight crisis services, according to a news release issued by the center. He also helped C4 develop long-term relationships with many of the area's hospitals.
“The C4 model is widely respected and something we hope to replicate throughout the county to serve all CountyCare members and ultimate-ly all of our patients,” said John Jay Shannon, M.D., and CEO of Cook County Health & Hospitals System.Chris Carroll was named C4’s (Community Counseling Centers of Chicago) interim
executive director.
Courtesy Community Counseling Centers of Chicago
By Frederick H. LoweI-Team Project Manager
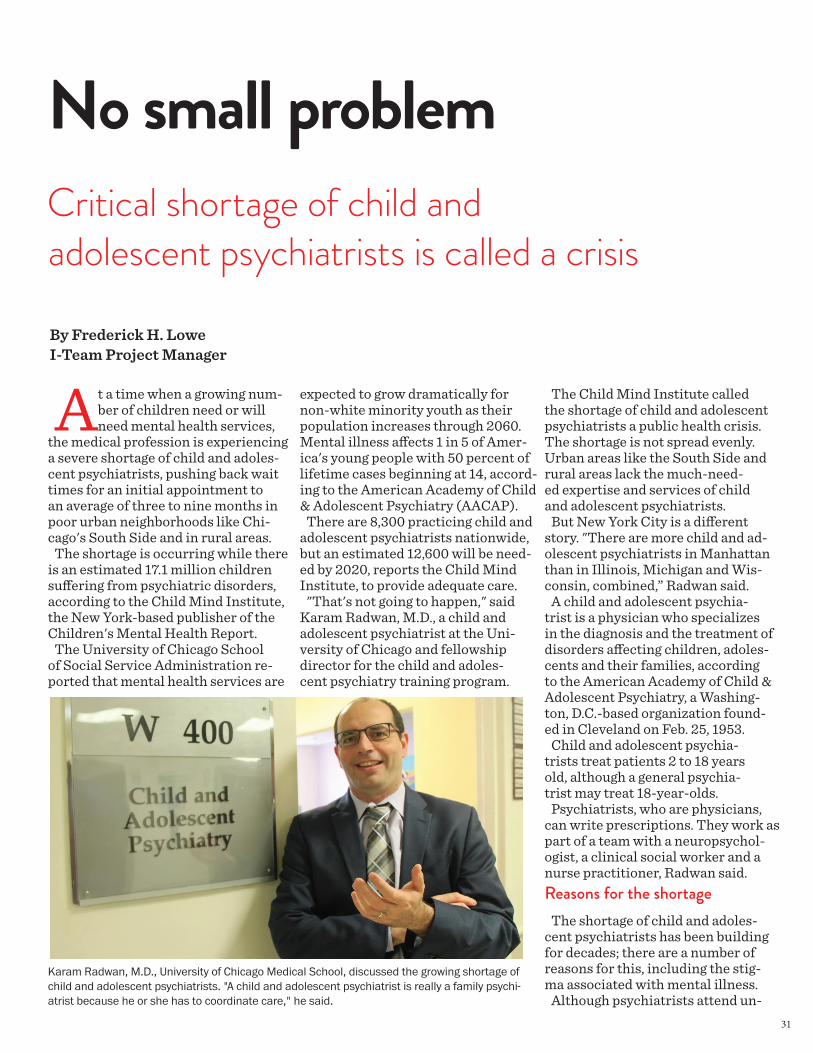
31
At a time when a growing num-ber of children need or will need mental health services,
the medical profession is experiencing a severe shortage of child and adoles-cent psychiatrists, pushing back wait times for an initial appointment to an average of three to nine months in poor urban neighborhoods like Chi-cago's South Side and in rural areas.
The shortage is occurring while there is an estimated 17.1 million children suffering from psychiatric disorders, according to the Child Mind Institute, the New York-based publisher of the Children's Mental Health Report.
The University of Chicago School of Social Service Administration re-ported that mental health services are
No small problem
expected to grow dramatically for non-white minority youth as their population increases through 2060. Mental illness affects 1 in 5 of Amer-ica's young people with 50 percent of lifetime cases beginning at 14, accord-ing to the American Academy of Child & Adolescent Psychiatry (AACAP).
There are 8,300 practicing child and adolescent psychiatrists nationwide, but an estimated 12,600 will be need-ed by 2020, reports the Child Mind Institute, to provide adequate care.
"That's not going to happen," said Karam Radwan, M.D., a child and adolescent psychiatrist at the Uni-versity of Chicago and fellowship director for the child and adoles-cent psychiatry training program.
The Child Mind Institute called the shortage of child and adolescent psychiatrists a public health crisis. The shortage is not spread evenly. Urban areas like the South Side and rural areas lack the much-need-ed expertise and services of child and adolescent psychiatrists.
But New York City is a different story. "There are more child and ad-olescent psychiatrists in Manhattan than in Illinois, Michigan and Wis-consin, combined,” Radwan said.
A child and adolescent psychia-trist is a physician who specializes in the diagnosis and the treatment of disorders affecting children, adoles-cents and their families, according to the American Academy of Child & Adolescent Psychiatry, a Washing-ton, D.C.-based organization found-ed in Cleveland on Feb. 25, 1953.
Child and adolescent psychia-trists treat patients 2 to 18 years old, although a general psychia-trist may treat 18-year-olds.
Psychiatrists, who are physicians, can write prescriptions. They work as part of a team with a neuropsychol-ogist, a clinical social worker and a nurse practitioner, Radwan said.Reasons for the shortage
The shortage of child and adoles-cent psychiatrists has been building for decades; there are a number of reasons for this, including the stig-ma associated with mental illness.
Although psychiatrists attend un-
Critical shortage of child and adolescent psychiatrists is called a crisis
Karam Radwan, M.D., University of Chicago Medical School, discussed the growing shortage of child and adolescent psychiatrists. "A child and adolescent psychiatrist is really a family psychi-atrist because he or she has to coordinate care," he said.
By Frederick H. LoweI-Team Project Manager

32
dergraduate school, medical school and four-year psychiat-ric residency, they are not highly regarded by others within the medical profession, Radwan said.
The years it takes to become a child and adolescent psychiatrist also discourages some physicians from entering the profession.
It takes four years of undergraduate work, four years of medical school and four years psychiatric residency to become a general psychiatrist.
A person who wants to become a child and adolescent psychiatrist must spend an additional two years getting pediatric psychiatric train-ing. A general psychiatrist cannot treat children because they don't have the training, although they may treat 18-year-olds, Radwan said.
"After completing training, they have to pay $750 to $1,000 to take the state exam to be certified to practice in Illinois," said Karen Taylor-Crawford, a child and ado-lescent psychiatrist who practices in Palos Heights, a Chicago suburb.
Radwan admits the additional two years discourages prospec-tive candidates from entering the field. "Some feel they are los-ing two years of work and it will take 10 years for them to make up for the lost wages," he said.
Each year, AACAP holds an advo-cacy day (the last one was held April 23-24, 2015) in which they lobby Congress to pass legislation to pro-vide loan forgiveness to encourage medical students to enter the profes-
sion. So far, that has not happened. "In response to the primary care
workforce shortage, Congress is reauthorizing worthy programs such as the National Health Service Corps. This program can provide medical education loan debt relief for physicians who have success-fully completed general pediatrics or general psychiatry residency training programs," AACAP said in a statement. "Trainees, who go on to subspecialize in child and ado-lescent psychiatry, pediatric neu-rology or pediatric rheumatology, etc., do not have this option through the current NHSC program."A difficult job
Being a child and adolescent psy-chiatrist is also very difficult, com-plicated by family dynamics. For ex-ample, a general psychiatrist works with adults. He or she asks adult-pa-tient questions to get answers. But a child and adolescent psychiatrist is involved with the patient, both par-ents and possibly the child's school.
If the parents are separated or divorced, they may disagree about their child's treatment."If the family is not intact, there can be custody battles," Radwan said.
In addition, a child's school may subpoena the psychiatrist's med-ical records to learn what type of medication the child is taking.
"A child and adolescent psychi-atrist is really a family psychi-atrist because he or she has to coordinate care," Radwan said.
Some psychiatrists don't want to become child and adolescent psychiatrists because they are concerned about prescribing med-ication to children, whose brains are still developing, said Dan Bad-er, a therapist with the Chicago Department of Public Health.
"I wouldn't say it is a ma-jor factor," Radwan said.Finally, there's the pay
Although many assume that once a person has the letters "M.D." after his or her name, he or she is on the road to a comfortable life. Even-tually, this may be the case. But child and adolescent psychiatrists who treat low-income patients are reimbursed only $35 to $45 through Medicaid for each visit.
Their salary during child and adolescent psychiatric residency is about $57,000 annually, which is about what residents in other medical specialties earn as well. The difficulty is that their practice earns less than other specialties once they have advanced beyond residency.
Merritt Hawkins, an Irving, Texas, company, which monitors physicians' salaries, reported that orthopedic surgeons in the Mid-west potentially can earn $700,000 annually. On the other hand, child and adolescent psychiatrists in the Midwest can earn a potential income of $250,000 annually.
As a result, child and adolescent psychiatrists go into private practice where they don't accept any insur-
Information from Child Mind Institute Children’s Mental Health Report

33
ance. They often charge $270 cash for an assessment and $140 cash for each follow up visit, Radwan said.Common mental illnesses in children
Some of the most common dis-orders diagnosed in children and adolescents are anxiety disorders, attention-deficit/hyperactivity disorder (ADHD) disruptive behav-ior, depression, bipolar disorder and eating disorders. Other ailments include autism spectrum disorders.
The lack of access to a child and adolescent psychiatrist often can lead to children, especially black boys, being aggressive, medicat-ed or turned over to the police.
The Child Mind Institute re-ported that mental illness cost $202 billion in lost productiv-ity and crime by Americans under 24 years old in a year.
While mental health issues of-
ten lead to law enforcement in-volvement, what the child and his family really need is thera-py to learn what dynamics are taking place, Radwan said.
The National Institutes of Health reported in June that boys ranging in age from 10 to 18 are more like-ly to be prescribed antipsychotic drugs for treatment of ADHD.
Maladaptive aggression is com-mon in ADHD, NIH said.
The report noted that "Among young people receiving antipsychot-ic prescriptions, fewer than half had any medical visit that included a mental disorder diagnosis. That may be in part due to stigma about mental illness, or because prima-ry care providers are concerned about reimbursement for treat-ment related to such diagnoses."
In 2003, the American Acad-emy of Child and Adolescent Psychiatry launched a task force
on workforce needs, which led to a recruitment initiative.
The University of Chicago Pritz-ker School of Medicine encourages medical students to become child and adolescent psychiatrists.
Some 320 fellows annually join the pool to become child and adolescent psychiatrists, Radwan said. They graduate after two years of training and are paid by the medical school.
"Every year, we welcome a di-verse body of fellows, reflected by their unique academic back-grounds, talents, strengths and viewpoints," Radwan wrote in a message to students. "We believe that it is through such diversity that our program is strengthened."
Information from Child Mind Institute Children’s Mental Health Report

34
Be an advocate: Access LivingSave community-based mental health services!
Supporting people with mental health issues is one of the most important things we can do to make Illinois a great place to live. Anyone can have a mental health issues or crisis of some kind. Anyone can also have a loved one struggling with mental health. Preventative supports save MILLIONS of dollars in hospitalization costs. Access Living, a Chicago-based disabil-ity advocate, offers an easy form to fill out to send a letter to your legislator about the need for funding for Illinois mental health programs.
Thresholds, a Chicago-based nonprofit, believes that it is vital to invest in a strong community behavioral health safety net, both to save lives and to save money.
Thresholds
• The state’s failure to invest in an adequate behavioral health safety net costs the state millions every year in expensive and preventable hospitalizations, emergency room visits, institutionalizations, inappropriate incarcerations, and homelessness. Both the human cost and the public costs are extraordinary.
• Illinois received a “D” report card rating by the National Al-liance on Mental Illness (NAMI) due to significant inadequa-cies in its community-based safety net for people living with a mental illness or substance use disorder. The state’s lack of essential community behavioral health services has resulted in a number of lawsuits and consent decrees, mandating the state to invest in an adequate community behavioral health infrastructure.
• People with a severe mental illness die 25 years younger than the general population, not due to their mental illness, but due to undiagnosed medical conditions because of a lack of access to healthcare.
• Over 23 million Americans, including more than 3 million Illinoisans, need treatment for a substance use disorder yet 90% of them go without any treatment. In 2011, there were 5.1 million emergency room visits nationwide, fully 49% of which were attributed to drug misuse or abuse.
Visit: http://www.capwiz.com/accessliving/issues/alert/?alertid=64119526&type=ST
See more at: http://www.thresholds.org/advocacy/our-platform/#sthash.pBVJJPmd.dpuf
Problem: Thousands of individuals living with a mental illness or substance use disorder cannot get necessary care due to repeated state cuts to services.
Solution: Access to care enables wellness and recovery, and saves money.
• Community-based care is the most cost-effective approach to recovery for individuals with a mental illness or substance use disorder.
• Community-based care combined with stable housing works: Between 70% and 90% of indi-viduals living with a mental illness or substance use disorder see a reduction in symptoms, better health, and an improved quality of life with the appropriate community treatment. Recovery leads to wellness, lower health care costs, independent living, and employment.
• Illinois must follow through on its commitment to rebalance the behavioral health system to reduce preventable hospitalizations and institutionaliza-tions.
• Successful and sustainable community-based care will only be achieved through comprehensive and collaborative approaches that break down the divisions that exist between funding, regulatory agencies, and public and private providers across the full continuum of care
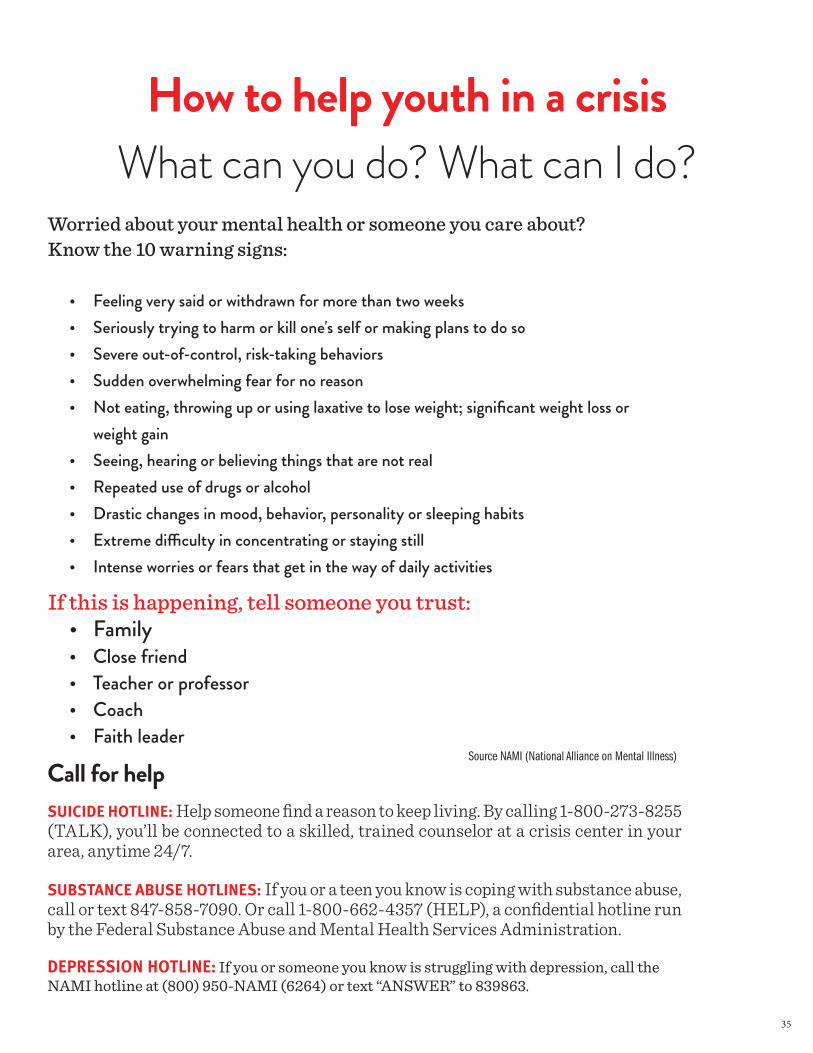
35
SUICIDE HOTLINE: Help someone find a reason to keep living. By calling 1-800-273-8255 (TALK), you’ll be connected to a skilled, trained counselor at a crisis center in your area, anytime 24/7.
SUBSTANCE ABUSE HOTLINES: If you or a teen you know is coping with substance abuse, call or text 847-858-7090. Or call 1-800-662-4357 (HELP), a confidential hotline run by the Federal Substance Abuse and Mental Health Services Administration.
DEPRESSION HOTLINE: If you or someone you know is struggling with depression, call the NAMI hotline at (800) 950-NAMI (6264) or text “ANSWER” to 839863.
Worried about your mental health or someone you care about? Know the 10 warning signs:
• Feeling very said or withdrawn for more than two weeks• Seriously trying to harm or kill one's self or making plans to do so• Severe out-of-control, risk-taking behaviors• Sudden overwhelming fear for no reason• Not eating, throwing up or using laxative to lose weight; significant weight loss or
weight gain• Seeing, hearing or believing things that are not real• Repeated use of drugs or alcohol• Drastic changes in mood, behavior, personality or sleeping habits• Extreme difficulty in concentrating or staying still• Intense worries or fears that get in the way of daily activities
If this is happening, tell someone you trust:• Family• Close friend• Teacher or professor• Coach• Faith leader
How to help youth in a crisisWhat can you do? What can I do?
Call for helpSource NAMI (National Alliance on Mental Illness)

www.columbialinks.org