common problems in gastroenterology for internal...
TRANSCRIPT

Common problems in Gastroenterology for Internal medicine
Julajak Limsrivilai
Siriraj Hospital
Outline : GI tract
Upper tract Dyspepsia
H. pylori infection
PancreaticobiliaryGall stone and CBD stone
Acute cholecystitis
Ascending cholangitis
Lower tract IBS
C. difficile infection
CRC screening GI bleeding
NSAIDs and prophylaxis of bleeding
Antiplatelet, anticoagulant, DOAC and GI bleeding
Occult GI bleeding: FOBT/IDA

Outline : Liver disease
Chronic liver disease Viral hepatitis
Alcoholic hepatitis
NAFLD
Autoimmune liver disease
Cirrhosis Portal hypertension
Variceal bleeding
Ascites and complication
Hepatorenal syndrome
Hepatocellular carcinoma

Dyspepsia: Thailand Guidelines 2018
Pittayanon R, J Neurogastroenterol Motil 2019

Dyspepsia: Thailand Guidelines 2018
Pittayanon R, J Neurogastroenterol Motil 2019

Etiology
Functional dyspepsia Organic dyspepsia
Normal Nonerosive gastritis
Polyp
Erosive/Hemorrhagic gastritis Peptic ulcer
Gastric cancer
Normal finding

Etiology : other causes of upper abdominal pain
Chronic pancreatitisPancreatic cancer
Gall stone
Liver tumor

Dyspepsia: Thailand Guidelines 2018
Pittayanon R, J Neurogastroenterol Motil 2019

Alarming features
3.Dysphagia
1.GI blood loss• IDA • Hematemesis/Mele
na
2.Weight loss 4.Persistent vomiting
5. Significant early satiety
6. Family Hx of gastric cancer

Dyspepsia: Thailand Guidelines 2018
Pittayanon R, J Neurogastroenterol Motil 2019

Dyspepsia: Thailand Guidelines 2018
Pittayanon R, J Neurogastroenterol Motil 2019

Dyspepsia: Thailand Guidelines 2018
Pittayanon R, J Neurogastroenterol Motil 2019


H. pylori: Indication for eradication
การใช้ยา NSAIDs และ แอสไพรนิ ร่วมกบัยาต้านการแข็งตวัของเลือด (anticoagulant), clopidogrel หรือ corticosteroids

H. pylori: Diagnosis
12
3

H. pylori: Treatment

Outline : GI tract
Upper tract Dyspepsia
H. pylori infection
PancreaticobiliaryGall stone and CBD stone
Acute cholecystitis
Ascending cholangitis
Lower tract IBS
C. difficile infection
CRC screening GI bleeding
Antiplatelet, anticoagulant, DOAC and GI bleeding
NSAIDs and prophylaxis of bleeding
Occult GI bleeding: FOBT/IDA

Gut 2018; 67:405-417

Recommendation in GIB
Single antiplatelet agent Withholding aspirin before endoscopy
Do not recommend platelet transfusion
Resume ASA in 3-5 D after endoscopic hemostasis
DAPT Withholding clopidogrel, continue ASA (controversial)
Resume clopidogrel or other new P2Y12 receptor inhibitors (prasugrel and ticagrelor) in 5 days (2-3 d for ticagrelor)

Warfarin Withholding warfarin
4-factor prothrombin complex concentrate (PCC) plus low-dose vit. K for life-threatening bleeding with an INR above 2.5
Not recommend higher doses of vit. K (>5 mg) in high thromboembolic risk
Do not recommend delaying endoscopy for life-threatening bleeding until normalisation of INR
Rechecking INR after reversal therapy is not mandatory before endoscopy
In high thromboembolic risk, Resume warfarin once adequate haemostasis is achieved.
Bridging anticoagulation with unfractionated heparin
Recommendation in GIB
• Non-valvular atrial fibrillation with a CHA2DS2-VASc score >5*
• Metallic mitral valve • Prosthetic valve with atrial fibrillation • <3 months after VTE • Severe thrombophilia (protein C or
protein S deficiency, antiphospholipid syndrome)

Direct oral anticoagulants (DOACs) Withholding DOACs
Activated charcoal for life-threatening bleeding if the last dose of DOAC is taken within 3 hours
Idarucizumab for the treatment of life-threatening bleeding in patients on dabigatran
Do not recommend vitamin K for treatment of bleeding associated with DOACs
Resuming DOACs after adequate haemostasis is achieved
Do not recommend bridging therapy in patients on DOACs
Recommendation in GIB

NSAID and Peptic ulcer

NSAID and Peptic ulcer
Melcarne L et al, EXPERT REVIEW OF GASTROENTEROLOGY & HEPATOLOGY, 2016
Relative risk for GI events
Relative risk for CV events

NSAID and Peptic ulcer
Low GI risk High GI risk
Low CV risk Non-selective NSAIDs Non-selective NSAIDs + PPICelecoxib + PPI (several risk factors) Eradicate H. pylori
High CV risk Naproxen; add PPI if patient is taking ASA
No NSAIDsNaproxen + PPI Low-dose celecoxib + ASA + PPI
Lanas A, Lancet 2017
GI risk Age > 60 years History of peptic ulcers Concomitant medication with antiplatelet agents, anticoagulants, corticosteroids, or SSRIs
Cardiovascular riskUse risk charts (eg, Framingham risk scores or the European SCORE system) History of cardiovascular events or diabetes

NSAID and Peptic ulcer
Low GI risk High GI risk
Low CV risk Non-selective NSAIDs Non-selective NSAIDs + PPICelecoxib + PPI (several risk factors) Eradicate H. pylori
High CV risk Naproxen; add PPI if patient is taking ASA
No NSAIDsNaproxen + PPI Low-dose celecoxib + ASA + PPI
Lanas A, Lancet 2017
GI risk Age > 60 years History of peptic ulcers Concomitant medication with antiplatelet agents, anticoagulants, corticosteroids, or SSRIs
Cardiovascular riskUse risk charts (eg, Framingham risk scores or the European SCORE system) History of cardiovascular events or diabetes

NSAID and Peptic ulcer
Low GI risk High GI risk
Low CV risk Non-selective NSAIDs Non-selective NSAIDs + PPICelecoxib + PPI (several risk factors) Eradicate H. pylori
High CV risk Naproxen; add PPI if patient is taking ASA
No NSAIDsNaproxen + PPI Low-dose celecoxib + ASA + PPI
Lanas A, Lancet 2017
GI risk Age > 60 years History of peptic ulcers Concomitant medication with antiplatelet agents, anticoagulants, corticosteroids, or SSRIs
Cardiovascular riskUse risk charts (eg, Framingham risk scores or the European SCORE system) History of cardiovascular events or diabetes

NSAID and Peptic ulcer
Low GI risk High GI risk
Low CV risk Non-selective NSAIDs Non-selective NSAIDs + PPICelecoxib + PPI (several risk factors) Eradicate H. pylori
High CV risk Naproxen; add PPI if patient is taking ASA
No NSAIDsNaproxen + PPI Low-dose celecoxib + ASA + PPI
Lanas A, Lancet 2017
GI risk Age > 60 years History of peptic ulcers Concomitant medication with antiplatelet agents, anticoagulants, corticosteroids, or SSRIs
Cardiovascular riskUse risk charts (eg, Framingham risk scores or the European SCORE system) History of cardiovascular events or diabetes

FOBT

Question
Which of the following statements about gFOBT (guiac test) is true?
1. Avoid Fe supplement before testing
2. Lower sensitivity than immunohistochemistry FOBT for upper GI bleeding
3. More than one sample of stools can increased test sensitivity
4. Vitamin C ingestion causes false-positive result
5. is recommended for annually surveillance in HNPCC family

FOBT
Hb
globin Heme
Reabsorption in prox intestine
porphyrins iron
pancreatic protease gastric pepsin protease
Pancreatic & intestinal protease
digestion
colonic bacteria
intestinal converted fractionColonic bacteria(1-99%)
15%
Have peroxidase activity
No peroxidase activity
Yamada. Principle of clinical gastroenterology. 2008
GuaiacImmuno-chemical
Heme-porphyrin

Fecal occult blood
Rockey. Gastroenterol Clin N Am 2005
Guaiac Heme-Porphyrin
iFOBT
False positives
• Animal Hb ++++ ++++ 0
• Dietary peroxidase
+++ 0 0
False negatives
• Vitamin C ++ 0 0
High false +ve and –ve

FOBT and bleeding site
Rockey DC, NEJM 1999

Fecal occult blood test : indication
Colorectal cancer screening :Decreased mortality from CRC
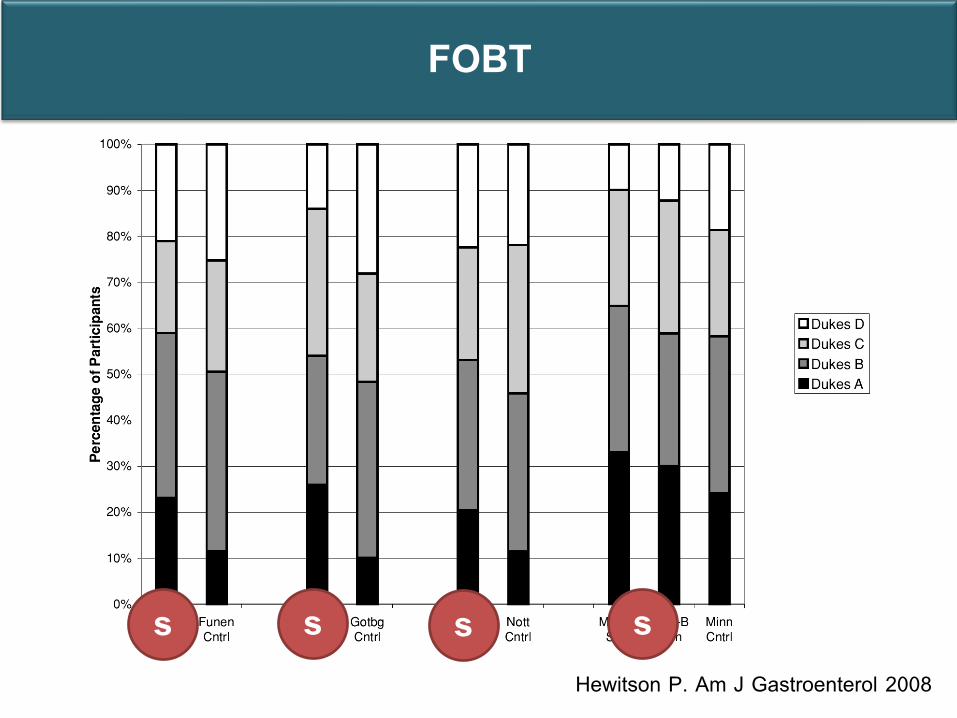
FOBT
Hewitson P. Am J Gastroenterol 2008
s s s s

Fecal occult blood test : indication
Colorectal cancer screening :Decreased mortality from CRC
Not indicate in symptomatic patients : IDA, abdominal pain
Low sensitivity Low specificity
iFOBT >> gFOBT

Role of FOBT in patients with IDA
Sensitivity
CA colon
gFOBT 33-50%
iFOBT 50-75%
Sensitivity
60 cc blood ingestion
gFOBT 16%
iFOBT 2%
Lieberman DA. NEJM 2009Rockey DC, Am J Gastroenterol 1999
No role of FOBT in the evaluation of IDA

Goddard AF, Gut 2013

Question
Which of the following statement about gFOBT (guiac test) is true?
1. Avoid Fe supplement before testing
2. Lower sensitivity than immunohistochemistry FOBT for upper GI bleeding
3. More than one sample of stools can increased test sensitivity
4. Vitamin C ingestion causes false-positive result
5. is recommended for annually surveillance in HNPCC family

Outline : GI tract
Upper tract Dyspepsia
H. pylori infection
PancreaticobiliaryGall stone and CBD stone
Acute cholecystitis
Ascending cholangitis
Acute pancreatitis
Lower tract IBS
C. difficile infection
CRC screening GI bleeding
NSAIDs and prophylaxis of bleeding
Antiplatelet, anticoagulant, DOAC and GI bleeding
Occult GI bleeding: FOBT/IDA

Irritable bowel syndrome

Irritable bowel syndrome: Rome IV
Recurrent abdominal pain, on average, at least 1 day/wk in the last 3 months, associated with 2 or more of the following criteria:
Related to defecation
Associated with a change in frequency of stool
Associated with a change in form (appearance) of stool
Symptoms must be present for the last 3 months, with onset at least 6 months before diagnosis
Lacy BE, et al. Gastroenterology 2016:150;1393

Differential diagnosis
Adapted from Furman DL & Cash BD, Gastroenterol Clin North Am 2011

Differential diagnosis
CA colon Chronic colitis eg. IBD, infection• Age > 50 yr or have Familial Hx of
CRC • Bloody diarrhea, bowel habit change • Anemia • Weight loss
• Mucous bloody diarrhea • Fever • Anemia • Weight loss

Alarming features
New onset of symptoms at 50 years or older
Severe or progressively worsening symptoms
Nocturnal diarrhea
Bloody stools
Unexplained IDA
Unintentional weight loss
Family history of colon cancer or IBD
Chey WD et al, JAMA 2015

Investigation
Alarming features
• Blood test : CBC, serum chemistries, TFT
• Stool test : ova, parasite
Diarrhea Constipation
Colonoscopy BE or colonoscopy

Treatment
Lacy BE, et al. Gastroenterology 2016:150;1393

C. difficile infection

Crobach MJT, Clin Microbiol Infect 2016Putsathit P, New Microbe and New Infect 2017
C. difficile infection: Diagnosis
Test in Unexplained and new-onset ≥ 3 unformed stools in 24 hours
Gold standard: Toxigenic culture (TC), Cell cytotoxicity neutralization assay (CCNA) (expensive, need special media, take 48 hr)
Pooled sensitivity Pooled specificity ราคา
CCNA TC CCNA TC
Enzyme immunoassay for toxin A/B
83% 57% 99% 99% 500 บาท
Glutamate dehydrogenase (GDH)
94% 96% 90% 96%
Nucleic acid amplification test (NAAT)
96% 95%(SI 68.6%)
94% 98%(SI 95.1%)
1,400 บาท

C. difficile infection: Diagnosis
Ma J, Pol Arc Int Med 2018

C. difficile: treatment
Consult Sx

Colon cancer screening

Question
A 57 year-old man, has recently been diagnosed advance stage colon cancer. He concerns that this malignant disease might be inherited. What would you recommend to his 30 yr-old son?
1. Colonoscopy now 2. Colonoscopy at age 40 3. Colonoscopy at age 504. FOBT at age 40 5. FOBT at age 50

Average risk
High risk
Colon cancer screening

Test USPSTF 2016 Multi-society
Joint 2017Asia Pacific 2014
gFOBT (3 samples) 1 yr 1 yr Not recommend
iFOBT (1-2 samples) 1 yr 1 yr 1 yrSigmoidoscopy 5 yr 5 - 10 yr 5 yr Colonoscopy 10 yr 10 yr 10 yr CT colonography 5 yr 5 yr Not recommend
Average risk
Screening period: 50 to 75-85 years

High risk
Familial colorectal cancer
Hereditary colorectal cancer
History of adenoma
History of colorectal cancer
Inflammatory bowel disease
Colonoscopy

Familial colorectal cancer
Lipton. Clin Gastroenterol Hepatol 2004Johns. Am J Gastroenterol 2001

Familial colorectal cancer
RR Age to begin Test Comment
Either CRC or AP in • 1st degree < 60 yr or • 2 or more 1st degree at
any age
4x • 40 years, or • 10 years
before the youngest
Colonoscopy Every 5 years
Either CRC or AP in • 1st degree age > 60 yr
2-2.5x • 40 years Screening options as recommended for average-risk
Rex DK, Gastroenterol 2017

Hereditary colon cancer
Who should be screen Age to begin Tool for screening and age to stop
FAP -mutation carrier-family members at 50% risk if no mutation identified
Age 10 to 12 years -Annual FSIG or colonoscopy until age 30 years, -every 3-5 years thereafter until age 60
HNPCC -mutation carrier-family members at 50% risk if no mutation identified
Age 20 to 25 years, or 2-5 years before the youngest case
-At least biennial colonoscopy, until age 40 years, -annually thereafter to age 70-75 years or until co-morbidity makes it clinically inappropriate
AD pattern

Hereditary colon cancer
Who should be screen Age to begin Tool for screening and age to stop
FAP -mutation carrier-family members at 50% risk if no mutation identified
Age 10 to 12 years -Annual FSIG or colonoscopy until age 30 years, -every 3-5 years thereafter until age 60
HNPCC -mutation carrier-family members at 50% risk if no mutation identified
Age 20 to 25 years, or 2-5 years before the youngest case
-At least biennial colonoscopy, until age 40 years, -annually thereafter to age 70-75 years or until co-morbidity makes it clinically inappropriate
AD pattern

Hereditary colon cancer
Who should be screen Age to begin Tool for screening and age to stop
FAP -mutation carrier-family members at 50% risk if no mutation identified
Age 10 to 12 years -Annual FSIG or colonoscopy until age 30 years, -every 3-5 years thereafter until age 60
HNPCC -mutation carrier-family members at 50% risk if no mutation identified
Age 20 to 25 years, or 2-5 years before the youngest case
-At least biennial colonoscopy, until age 40 years, -annually thereafter to age 70-75 years or until co-morbidity makes it clinically inappropriate
AD pattern

HNPCC: How to diagnose?
Clinical criteria
Tumor testing
Germline testing

Clinical criteria: Amsterdam II
Amsterdam II criteria• 3 or more relatives with HNPCC-associated cancer (i.e. CRC, endometrial, renal
pelvis, SB, ureteral cancers), one of whom is a first degree relative of the other two
• Cancer in at least 2 generations of the same family
• At least one cancer case Dx before the age of 50
• FAP should be excluded
Major limitation = low sensitivity: 22% High specificity 98%

Clinical criteria: revised Bethesda guidelines
1. Colorectal cancer diagnosed in age < 50 years2. Presence of synchronous, metachronous colorectal, or other HNPCC-associated tumors, regardless of age. 3. Colorectal cancer with the MSI-H-like histology diagnosed in a age < 60 years. 4. Colorectal cancer diagnosed in a patient +
1 first-degree relatives with an HNPCC-related tumor at age < 505. Colorectal cancer diagnosed in a patient +
2 first- or second-degree relatives with HNPCC-related tumors,regardless of age.
J Natl Cancer Inst 2004; 96:261
Presence of tumor infiltrating lymphocytes. Crohn's-like lymphocytic reaction, mucinous/signet-ring differentiation, or medullary growth pattern
Sensitivity: 82% Specificity; 77%
If meet, MSI and or IHC should be evaluated

Suspected HNPCC
Analyse tumor MSI or IHC
MSS/MSI-low or Intact prot by IHC
Most likely not HNPCC
But if strong suspicious →genetic testing
Exclude FAP/AFAP
MSI-H or loss protein by IHC
Genetic germline testing
Germline MMR gene mutation
Dx HNPCC and genetic counseling
No germline mutation detected
MLH1 methylation studies and/or BRAF assessment if MLH1 loss by IHC
Hypermethylationor BRAF mutation
Not HNPCC
Normal
Most likely undetectable mutation

Question
A 57 year-old man, has recently been diagnosed advance stage colon cancer. He concerns this malignant disease might be inherited. What would you recommend to his 30 yr-old son?
1. Colonoscopy now 2. Colonoscopy at age 40 3. Colonoscopy at age 504. FOBT at age 40 5. FOBT at age 50

Outline : GI tract
Upper tract Dyspepsia
H. pylori infection
PancreaticobiliaryGall stone and CBD stone
Acute cholecystitis
Ascending cholangitis
Lower tract IBS
C. difficile infection
CRC screening GI bleeding
NSAIDs and prophylaxis of bleeding
Antiplatelet, anticoagulant, DOAC and GI bleeding
Occult GI bleeding: FOBT/IDA

Gall stone and complications

Question
A 40 year-old woman presents with acute epigastric pain for 4 hr. LFTs : TB 0.6, DB 0.4, AST 350, ALT 320, ALP 120, A/G 4.4/2.6. U/S reveals gall stone, no biliary duct dilatation
What’s the most appropriate next management?
1. check for HAV, HBV, and HEV infection
2. LC
3. ERCP
4. Endoscopic ultrasonography

Gall stone and complications

Asymptomatic GS60-80%

Biliary pain20%

Acute cholecystitis10%

Biliary pain(with AST/ALT)
Obstructive jaundiceCholangitis
5%

GS pancreatitis<5%

Gallstone and CBD stone

Stone in GB : cholycystectomy in …
Do only in symptomatic cases
Kimura Y, J Hepatobiliary Pancreast Sci 2013
Acute cholecystitis 0-3%Jaundice 0-2%
Acute cholecystitis 5.8-11.4%Jaundice 3-7.5%

Cholecystectomy in asymptomatic gallstone
Special subgroups Comments
Chronic hemolytic syndromes - Sickle cell anemia and hereditary ovalocytosis
- Onset in younger age - ↑life-time risk of complication - Prophylactic LC at the time of
splenectomy
GB cancer - Porcelain GB- GB polyp ≥ 1 cm- [Large gallstones (≥ 3 cm)]
EASL guideline 2016

CBD stone
Difficult to diagnose
up to 50% developing complication Removal
Test SensitivityTransabdominalU/S
75% dilated ducts 50% non-dilated
CT scan 70-75%
MRCP 88-92% all comers90-95% dilated ducts
EUS 90-97%

CBD stone : clinical predictors in who have GS
Predictor
Very strong
CBD stone on US
clinical ascending cholangitis
bilirubin > 4 mg/dL
Strong
dilated CBD on US (>6 mm)
bilirubin 1.8-4 mg/dL
Moderate
abnormal LFT other than bilirubin
age > 55 yr
GS pancreatitis
Presence of any very strong High
Presence of both strong High
No predictors present Low
All other patients Intermediate
ASGE guideline 2010
Obstruction
ALP
AST or ALT

CBD stone
Symptomatic ptwith GS
Likelihood of CBD stone
Low Intermediate High
LC LC with IOC or
Preop EUS/MRCP ERCP
ASGE guideline 2010

Acute cholecystitis

Acute cholecystitis
RUQ pain , RUQ tenderness 90%
Fever 50%
prior history of biliary colic 75%
Murphy’s sign Sens 20-65%Spec 87%
Jaundice • Sepsis• CBD stone • Mirizzi’s syndrome
20%

Cholecystitis: Diagnosis
Item Signs Details
A Local signs of inflammation Murphy’s sign
RUQ mass/pain/tenderness
B Systemic sign of inflammation
Fever
Elevated CRP (> 3 mg/dl)
Elevated WBC (>10,000 mm3/dl)
C Imaging findings Characteristic of acute cholecystitis
Suspected diagnosis : A + B
Definite diagnosis : A + B + C
Sens 91.2%, Spec 96.9%Yokoe M, J
Hepatobiliary Pancreas Sci 2018

Cholecystitis : Diagnosis
US Sens 81%, Spec 83%
US Murphy sign Sens 63%, Spec 94%
Distention (8*4 cm) ,
Wall thickening (4 mm), Fat strand,
Pericholecystic fluid
Tc-HIDA scanSensitivity 80-90%
False positive 10-20%: (fasting, s/p
sphincterotomy)

Cholecystitis: Complications
Gangrenous cholecystitis
• Irregular wall thickening• Poor contrast enhancement
(interrupted rim sign), • intraluminal fap
Emphysematous cholecystitis
Gas in lumen or wall of gallbladder

Cholecystitis : Treatment
IV ATB and supportive
care
Specific Rx
Cholecys-tostomy
Cholecys-tectomy
Center experiencePatients surgical risk status

Acute cholecystitis : management
Grade II : 1/4 ofDuration > 72 hr,
palpable tender mass, WBC > 18,000/mm3,
Mark local inflam by image (presence of complications)
Grade I : mild
Okamoto K, J Hepatobiliary Pancreas Sci 2018
In pt with high Sx riskCCS ≥ 6, ASA ≥ 3
Percutaneuos cholecystostomy
ATB and general support care
ATB and general support care
Urgent/early GB drainage
Observation
Early LC
Delayed/ elective LC
Advanced LC technique available, low risk Sx
Successful Rx, high risk Sx
Failure Rx

Acute cholecystitis : management
Grade III : organ failure
Okamoto K, J Hepatobiliary Pancreas Sci 2018
Percutaneuoscholecystostomy
ATB and general support care
Urgent/early GB drainage
Early LC
Delayed/ elective LC
No negative predictive factor and presence of favorable organ system failure
Presence of negative
predictive factors and/or no FOSF
observation
Advanced centerGood PS
Not advanced centerpoor PS
poor PS
good PS
Negative predictive factors for withstanding LC: neurological dysfunction, respiratory dysfunction, and coexistence of jaundice (TB> 2)Favorable organ system failure: renal and CVS dysfunction

Ascending cholangitis

Ascending cholangitis
1.Fever 95%
2.RUQ tenderness 90%
3.Jaundice 80%
4.Confusion 15%
5.Hypotension 15%
1+2+3 = Charcot’s triad (20-70% of patients)1+2+3+4+5 = Reynolds’ pentad

Ascending cholangitis : Diagnosis Item Signs Details
A Systemic inflammation Fever (> 38 c) and/or shaking chills
Laboratory data evidence of inflammation (WBC < 4000 or > 10000/mcl, CRP ≥ 1 mg/dL)
B Cholestasis Jaundice (> 2 mg/dL)
Abnormal LFTs (AST,ALT,ALP,GGT > 1.5x STD)
C Imaging findings Biliary dilatation
Evidence of the etiology on imaging (stricture, stone, stent, etc.)
Suspected diagnosis : A + (B or C)
Definite diagnosis : A + B + CKiriyama S, J Hepatobiliary Pancreas Sci 2018

Cholangitis : Treatment
IV ATB and supportive
care
Specific Rx
PTBDERCP
Surgery

Ascending cholangitis : Treatment
Grade II : 2/5 ofAge≥75 yr, T ≥ 39°C,
TB ≥ 5mg/dl, Alb ≤ STD*0.7
WBC <4,000 or >12,000
Grade III : Any organ failure
Grade I : not grade II/III
Yokoe M, J Hepatobiliary Pancreas Sci 2018Kiriyama S, J Hepatobiliary Pancreas Sci 2018
ERCP, PTBD, Sx
ATB and general support care
Early (24-48 hr) biliary drainage
ATB and general support care
Urgent (ASAP) biliary drainage
Organ support, ATB
Finish course of
ATB
Biliary drainage
Treatment for etiology if still
needed (endoscopic Rx,
percutaneous Rx, or surgery)

Outline : Liver disease
Chronic liver disease Viral hepatitis
Alcoholic hepatitis
NAFLD
Autoimmune liver disease
Metabolic liver disease
Cirrhosis Portal hypertension
Variceal bleeding
Ascites and complications
Hepatorenal syndrome
Hepatocellular carcinoma

Outline : Liver disease
Chronic liver disease Viral hepatitis
Alcoholic hepatitis
NAFLD
Autoimmune liver disease
Metabolic liver disease
Cirrhosis Portal hypertension
Variceal bleeding
Ascites and complications
Hepatorenal syndrome
Hepatocellular carcinoma

Question
Who should be started anti-HBV treatment?
1. 30 year-old man with HBsAg and HBeAg +ve, HBV VL > 170,000,000 IU/L, ALT 20, US – normal liver
2. 30 year-old man with HBsAg and HBeAg +ve, HBV VL 20,000 IU/L, ALT 50, US – normal liver
3. 50 year-old man with HBsAg +ve, HBeAg –ve, HBV VL 1,500 IU/L, ALT 30, US – cirrhotic liver
4. 40 year-old man with HBsAg +ve, HBeAg –ve, HBV VL < 10 IU/L, ALT 80, US – fatty liver

HBeAg positive HBeAg negative
Phase 1 Phase 2 Phase 3 Phase 4 Phase 5
Chronic HBV
infection
Chronic
hepatitis B
Chronic HBV
infection
Chronic
hepatitis B
Resolved HBV
infection
HBsAg HighHigh/
intermediateLow Intermediate Negative
HBeAg Positive Positive Negative Negative Negative
HBV DNA >107 IU/mL 104–107 IU/mL <2,000 IU/mL* >2,000 IU/mL <10 IU/mL‡
ALT Normal Elevated Normal Elevated† Normal
Liver disease None/minimalModerate/
severeNone
Moderate/
severeNone§
Old
terminologyImmune tolerant
Immune reactive
HBeAg positiveInactive carrier
HBeAg negative
chronic hepatitis
HBsAg negative
/anti-HBc
positive
New nomenclature for chronic phases
*HBV DNA levels can be between 2,000 and 20,000 IU/mL in some patients without signs of chronic hepatitis;†Persisitently or intermittently, based on traditional ULN (~40 IU/L). ‡cccDNA can frequently be detected in the liver;§Residual HCC risk only if cirrhosis has developed before HBsAg loss.
EASL CPG HBV. J Hepatol 2017;67:370–98
• The natural history of chronic HBV infection has been schematically divided
into five phases
Chronic HBV
infection
Chronic
hepatitis B

Indications for treatment
*Defined by HBV DNA >2,000 IU/ml, ALT >ULN and/or at least moderate liver necroinflammation or fibrosis;†Defined by persistently normal ALT and high HBV DNA levels;‡ Even if typical treatment indications are not fulfilled
EASL CPG HBV. J Hepatol 2017;67:370–98
• Primarily based on the combination of 3 criteria
– HBV DNA, serum ALT and severity of liver disease
Recommendations
Should be treated
• Patients with HBeAg-positive or -negative chronic hepatitis B* I 1
• Patients with cirrhosis, any detectable HBV DNA, regardless of
ALT levelI 1
• Patients with HBV DNA >20,000 IU/mL and ALT >2x ULN,
regardless of severity of histological lesionsII-2 1
May be treated
• Patients with HBeAg-positive chronic HBV infection†
>30 years old, regardless of severity of liver histological lesions
III 2
Can be treated
• Patients with HBeAg-positive or -negative chronic HBV infection
and family history of HCC or cirrhosis and extrahepatic
manifestations‡
III 2
Grade of evidence Grade of recommendation

Monitoring of patients currently not treated
EASL CPG HBV. J Hepatol 2017;67:370–98
• Patients with no current indication of antiviral therapy should
be monitored
– Periodical assessments of serum ALT, HBV DNA and non-invasive
markers for liver fibrosis
Recommendations
Follow-up at least every 3–6 months
• HBeAg-positive chronic HBV infection, <30 years oldII-2 1
Follow-up at least every 6–12 months
• HBeAg-negative chronic HBV infection and serum HBV DNA
<2,000 IU/ml
II-2 1
Follow-up every 3 months for the first year and every 6 months
thereafter
• HBeAg-negative chronic HBV infection, serum HBV DNA
≥2,000 IU/ml
III 1
Grade of evidence Grade of recommendation

Discontinuation of NA treatment
EASL CPG HBV. J Hepatol 2017;67:370–98
• Long-term therapy with NAs is usually required
– HBV eradication is not usually achieved
Recommendations
NAs should be discontinued
• After confirmed HBsAg loss (± anti-HBs seroconversion)II-2 1
NAs can be discontinued
• In HBeAg-positive patients, without cirrhosis, who
achieve stable HBeAg seroconversion and undetectable
HBV DNA and complete ≥12 months of consolidation
therapy
Close post-NA monitoring is warranted
II-2 2
NAs may be discontinued
• In selected HBeAg-negative patients, without cirrhosis,
who achieve long-term (≥3 years) virological
suppression, if close post-NA monitoring can be
guaranteed
II-2 2
Grade of evidence Grade of recommendation

Special patient groups: HIV or HDV co-infection
EASL CPG HBV. J Hepatol 2017;67:370–98
• The risk of fibrosis progression, cirrhosis and HCC is
greater in patients also infected with HDV or HIV
Recommendations (HIV)
All HIV-positive patients with HBV co-infection should start
antiretroviral therapy (ART) irrespective of CD4 cell count II-2 1
HIV/HBV co-infected patients should be treated with a TDF- or
TAF-based ART regimen
I (TDF)
II-1 (TAF)1
Recommendations (HDV)
PegIFN for at least 48 weeks is the current treatment of choice
in HDV/HBV co-infected patients with compensated liver disease I 1
In HDV/HBV co-infected patients with ongoing HBV DNA
replication, NA therapy should be consideredII-2 1
PegIFN treatment can be continued until Week 48 irrespective
of on-treatment virological response if well tolerated II-2 2
Grade of evidence Grade of recommendation

Special patient groups: patients undergoing immunosuppressive therapy or chemotherapy
EASL CPG HBV. J Hepatol 2017;67:370–98
Recommendations
All candidates for chemotherapy and immunosuppressive
therapy should be tested for HBV markers prior to
immunosuppression
I 1
All HBsAg-positive patients should receive ETV, TDF, or
TAF as treatment or prophylaxis II-2 1
HBsAg-negative, anti-HBc-positive subjects should
receive anti-HBV prophylaxis if they are at high risk of HBV
reactivation
II-2 1
Grade of evidence Grade of recommendation

Question
Who should be started anti-HBV treatment?
1. 30 year-old man with HBsAg and HBeAg +ve, HBV VL > 170,000,000 IU/L, ALT 20, US – normal liver
2. 30 year-old man with HBsAg and HBeAg +ve, HBV VL 20,000 IU/L, ALT 50, US – normal liver
3. 50 year-old man with HBsAg +ve, HBeAg –ve, HBV VL 1,500 IU/L, ALT 30, US – cirrhotic liver
4. 40 year-old man with HBsAg +ve, HBeAg –ve, HBV VL < 10 IU/L, ALT 80, US – fatty liver

Viral hepatitis C

Acute alcoholic hepatitis

Management of alcoholic hepatitis: Definition and diagnosis
*Ascites and/or encephalopathy; †Defined histologically by steatosis, hepatocyte ballooning, and an inflammatory infiltrate with polymorphonuclear neutrophils
EASL CPG ALD. J Hepatol 2018;69:154–81
• Clinical
– Recent jaundice ± other signs of liver decompensation* in patients with ongoing
alcohol abuse
• Cardinal sign is a progressive jaundice, often associated with fever, malaise, weight loss
and malnutrition
• Histological
– Steatohepatitis†
• Laboratory
– Neutrophilia
– Hyperbilirubinaemia (>50 μMol/L)
– AST >2 x ULN and AST/ALT ratio typically greater than 1.5–2.0
– Severe: prolonged PT, hypoalbuminaemia, and decreased platelet count
Recommendations
A recent onset of jaundice in patients with excessive alcohol
consumption should prompt clinicians to suspect AH A 1
Grade of recommendation Level of evidence

Management of suspected alcoholic hepatitis: Treatment algorithm
*Particularly in null responders (Lille score ≥0.56).
EASL CPG ALD. J Hepatol 2018;69:154–81
Stop treatment* and assessment for early liver transplantation in
highly selected patients
Continue treatment for 28 days
Lille score ≥0.45Lille score <0.45
mDF <32 and GAHS <9
Assess treatment response at Day 7 (Lille score)
Prednisolone 40 mg/day ± NAC No specific therapy
mDF ≥32 or GAHS ≥9
Assessment of disease severity (prognostic scores)
• Systematic evaluation of nutritional status and energy intake
• Daily target 35–40 kcal/kg BW• Prefer oral route as first-line intervention• Supplementation with B-complex
vitamins
Consider liver biopsy if diagnosis is uncertain
Perform systematic extensive screening for infection
Treatment of alcohol dependence
Clinical diagnosis of AH
Absence of
infection

Management of alcoholic hepatitis: Evaluation of severity
*Modified version (mDF) cut-off value of 32 identifies patients with severe AH and is usually the threshold used for initiating
specific therapy
EASL CPG ALD. J Hepatol 2018;69:154–81
• Different prognostic models aim to identify patients at high risk of early death
– Often incorporate the same variables and have similar efficacy in predicting
short-term survival
• Lille model can predict pattern of response to corticosteroid treatment
– Based on pre-treatment data plus the response of serum bilirubin
Score Bilirubin PT/INR
Creatinine/
urea Leucocytes Age Albumin
Change in
bilirubin
(Day 0 to 7)
Maddrey
DF*+ + – – – – –
MELD + + + – – – –
GAHS + + + + + – –
ABIC + + + – + + –
Lille + + + – + + +

Management of suspected alcoholic hepatitis: Treatment algorithm
*Particularly in null responders (Lille score ≥0.56).
EASL CPG ALD. J Hepatol 2018;69:154–81
Stop treatment* and assessment for early liver transplantation in
highly selected patients
Continue treatment for 28 days
Lille score ≥0.45Lille score <0.45
mDF <32 and GAHS <9
Assess treatment response at Day 7 (Lille score)
Prednisolone 40 mg/day ± NAC No specific therapy
mDF ≥32 or GAHS ≥9
Assessment of disease severity (prognostic scores)
• Systematic evaluation of nutritional status and energy intake
• Daily target 35–40 kcal/kg BW• Prefer oral route as first-line intervention• Supplementation with B-complex
vitamins
Consider liver biopsy if diagnosis is uncertain
Perform systematic extensive screening for infection
Treatment of alcohol dependence
Clinical diagnosis of AH
Absence of
infection

Non alcoholic fatty liver disease (NAFLD)
Cirrhosis
Hepatocellularcarcinoma
Liver-relateddeath
NASH
20-25%
40% ?
Fatty liverrare
Metabolic syndrome

NAFLD : Noninvasive Diagnosis of Liver Fibrosis in NAFLD
Score Serum markersAge BMI FBS TG AST ALT PLT ALB
FIB-4 O O O O
NAFLD fibrosis score
O O O O O O O
BARD O O O O
BAAT O O O O

NAFLD : Noninvasive Diagnosis of Liver Fibrosis in NAFLD
Transient elastrography
(fibroscan)
MR elastrography

NAFLD : Treatment
Treatment Recommen-dation
Comment
Weight reduction Yes • 3-5 % : improve steatosis• 10% : improve necroinflammation
Metformin No 6-12 mo of MF did not improve aminotransferases or liver histology
Pioglitazone Yes Improve histology in biopsy-proven NASH, in both with and without DM
Vitamin E Yes Dose 800 IU/d improves histology in non-diabetic adults with biopsy-proven NASH
UDCA No No histological effect
Omega-3 fatty acid N/A May be 1st line agent to Rx hyperTg in NAFLD
Statin Can be used to Rx dyslipidemia in NAFLD AASLD guideline 2018

Autoimmune liver disease
Liver parenchyma :
AIH Small duct : PBC
Large duct : PSC

AIH : Clinical clues
Type 1 Type 2
Clinical presentation• Acute hepatitis on top chronic hepatitis 40-50%• Chronic hepatitis 40-50%• Acute hepatitis 10%

AIH : Investigation
Antibody Type Prevalence ANA 1 60-80%SMA 1 60-80%
LKM-1 2 4%
Plasma cell infiltration
Interface hepatitis
Hepatocyte rosette formation

AIH : diagnosis
Pretreatment aggregate score : Definite Dx > 15
Probable Dx 10-15Posttreatment aggregate score :
Definite Dx > 17Probable Dx 12-17

IAIHG simplified scoring system (2008)
Hennes EM, et al. Hepatology 2008;48:169–76; EASL CPG AIH. J Hepatol 2015;63:971–1004
Feature/parameter Discriminator Score
Antibodies (max 2 points)
ANA or SMA+
ANA or SMA+
or LKM+
or SLA/LP+
≥1:40
≥1:80
≥1:40
Any titre
(0−2 points total)
+1
+2
+2
+2
IgG or γ-globulins level>ULN
>1.1x ULN
+1
+2
Liver histology
(evidence of hepatitis is required)
Compatible with AIH
Typical of AIH
Atypical
+1
+2
0
Absence of viral hepatitis No
Yes
0
+2
Score ≥7 = Definite AIH
Score ≥6 = Probable AIH
• Diagnostic criteria for routine clinical use

AIH treatment

Therapeutic algorithm
*Treatment probably no longer indicated in decompensated, burned-out cirrhosis, unless high inflammatory score on liver biopsy
EASL CPG AIH. J Hepatol 2015;63:971–1004
Diagnosis of AIH
Advanced fibrosis/
cirrhosis*
Active disease
(HAI ≥ 4/18)
Mild disease
(ALT <3x ULN; HAI <4/18)
and no advanced fibrosis
Treatment optional
Individual decision based on:
• Age
• Co-morbidities
• Patient preference
• Serology
Treatment
required
If no treatment, monitor every
3 months (ALT, IgG)
Follow-up liver biopsy if there is
increase of ALT and/or IgG
Induction
therapy

AIH treatment

Primary biliary cirrhosis (PBC)
Small duct (interlobular bile ducts) destruction
by autoimmune inflammatory process

PBC : Clinical
Finding Frequency (%)Fatigue 21-85
Pruritus 19-55
Jaundice 3-10
Right upper quadrant pain 8
Hyperpigmentation 25
Hepatomegaly 25
Splenomegaly 15
Xanthelasma 10
None (ALP elevation) 25-61

PBC : Diagnosis
• AMA +ve• ALP > 1.5x • AST < 5x
PPV > 98%DuctopeniaGranuloma

PBC : Treatment
UDCA 13-15
mg/kg/d
Cirrhosis complication
Cholestatic complication • Pruritus : Cholestyramine,
rifacimin, opiod antagonist• Steatorrhea : MCT• Bone disease : Vit D + Ca• Coagulopathy : Vit K
Add 2nd line:• obeticholic acid 5 mg• fibrate
Inadequate response

Primary sclerosing cholangitis
Large duct destruction
by autoimmune inflammatory process

PSC : Clinical features
Intermittent biliary obstruction
Secondary biliary cirrhosis

PSC : Treatment
UDCA
Immunosuppressive and other agents
ERCP and endoscopic therapy
Liver transplantation
Less benefit

Outline : Liver disease
Chronic liver disease Viral hepatitis
Alcoholic hepatitis
NAFLD
Autoimmune liver disease
Metabolic liver disease
Cirrhosis Portal hypertension
Variceal bleeding
Ascites and complications
Hepatorenal syndrome
Hepatocellular carcinoma

Question
Which condition can cause varix only at fundus of stomach?
1. Primary biliary cirrhosis
2. Essential thrombocytosis with portal vein thrombosis
3. Chronic pancreatitis
4. Budd-Chiari syndrome
5. Schistosomiasis

Portal hypertension
Left sided portal HT : Isolated fundal varices
Caput medusa : Cirrhosis

Portal hypertension : Etiologies
Prehepatic• Portal V thrombosis• Splenic V thrombosis
Posthepatic• Budd-Chiari syndrome• Constrictive pericarditis • Rt-sided HF
Intrahepatic • Presinusoidal :
Schistosomiasis• Sinusoidal : cirrhosis • Postsinusoidal : VOD
Variceal bleeding Variceal bleedingAscites (low prot)
Variceal bleedingAscites (high prot)
hepatomegaly

Question
Which condition can cause varix only at fundus of stomach?
1. Primary biliary cirrhosis
2. Essential thrombocytosis with portal vein thrombosis
3. Chronic pancreatitis
4. Budd-Chiari syndrome
5. Schistosomiasis

Variceal bleeding

No varices
Small varicesNo hemorrhage
Med/Large varicesNo hemorrhage
Varicealhemorrhage
Recurrenthemorrhage
8% per year
8% per year
5-15% per year
60%
Variceal bleeding
V = I x R
↑Resistance to portal flow
↑Portal pressure
↑Variceal growth →rupture
Splanchnic vasodilatation
↑Portal blood flow
cirrhosis↑NO
TIPS, Shunt
EVL
Somatostatin, telipressin,
Non-select BB
OLT
T = tp x rw

AASLD guideline 2017
No varices
Small varicesNo hemorrhage
Med/Large varicesNo hemorrhage
Varicealhemorrhage
Recurrenthemorrhage
8% per year
8% per year
5-15% per year
60%
Variceal bleeding• Prevent variceal formation : no benefit • Prevent variceal progression : BB in
CTP-C or presence of red wale sign• Repeat EGD :
No varices: 2 y (active), 3 y (quiescent) Small varices:1 y(active),2 y (quiescent)
BB
• Prevent variceal rupture
BB or EVL
• Stop variceal bleeding
Somatostatin/telipressin + EVL, if fail → TIPS or OLT
• Prevent rebleedingBB & EVL, if fail → TIPS or OLT
EGD in all cirrhosis except in pt with LS < 20 kPa and Plt > 150,000

Ascites

Ascites : What’s SAAG
Exudate VS TransudateHigh protein Low protein
Right-sided CHF : High protein SBP : Low protein

Ascites : What’s SAAG
Sinusoid (S)
Peritoneal Cavity (PC)
Hs
Hpc
Os
Opc
SH – SO = PCH - PCO
SH = SO+ PCH - PCO
Portal pressure = Serum Alb – Ascites Alb

Ascites
Cirrhotic ascitesCardiac ascites
Peritoneal malignancy
1.1
4.
0
3.
0
2.
0
1.
0
0
Serum –
ascites
albumin
gradient
(g/dL)
(75)
Ascitic fluid
total protein
(g/dL)
7.
0
5.
0
3.
02.
0
0
2.5
Runyon, Ann Intern Med 1992; 117:215
97% accuracy

Ascites
Low gradient < 1.1 gm/dl▪ Peritoneal disease▪ Peritoneal carcinomatosis▪ TB peritonitis▪ Pancreatic ascites▪ Bowel obstruction /infarction▪ Biliary ascites▪ Postop lymphatic leak▪ Serositis in CNT diseases
▪ Nephrotic syndrome
High gradient > 1.1 g/dl▪ Sinusoid ▪ Cirrhosis▪ Alcoholic hepatitis▪ Mixed ascites
▪ Post sinusoid ▪ Veno-occlusive diseaseBudd-
Chiari syndrome▪ Cardiac ascites
▪ Myxedema
Runyon BA. Ann Intern Med 1992;117:215

Ascites
False low SAAG Different in time
Hypoalbuminemia < 1.1 mg/dl
Hyperglobulinemia : glob contribute to serum oncotic P
Hypotension : decrease portal pressure
False high SAAG Chylous ascites : lipid interfere with albumin measurement

Treatment of cirrhotic ascites
Grade Definition Treatment
1 Only detectable by US No treatment
2 Moderate symmetrical distension of abdomen
Restriction of salts and diuretic
3 Large or gross ascites with marked abdominal distention
LVP
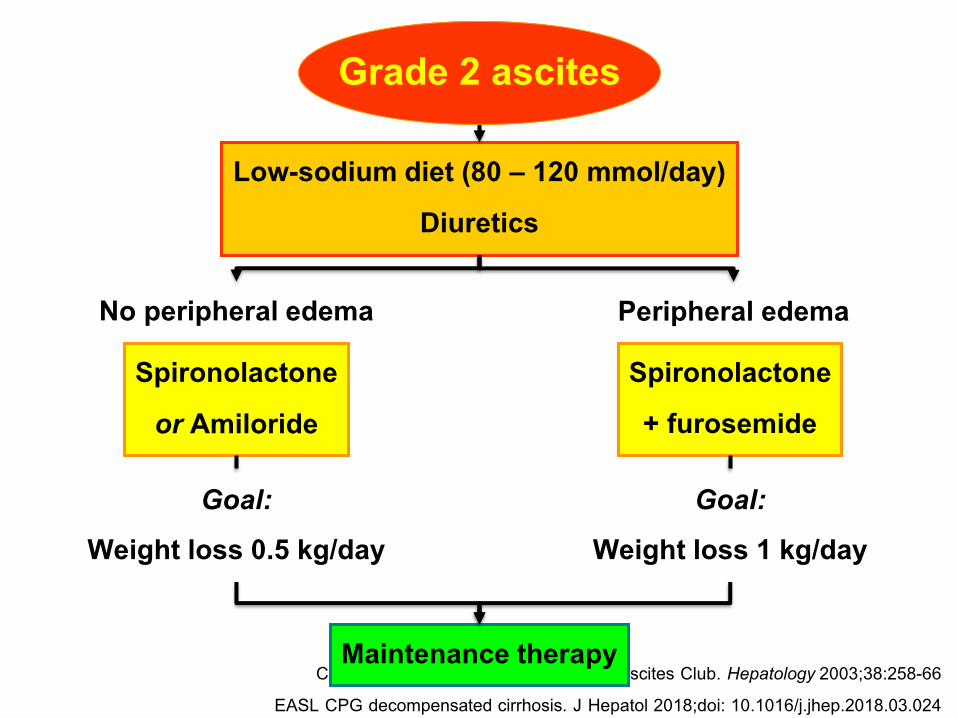
Consensus Report of the International Ascites Club. Hepatology 2003;38:258-66EASL CPG decompensated cirrhosis. J Hepatol 2018;doi: 10.1016/j.jhep.2018.03.024
Grade 2 ascites
No peripheral edema
Low-sodium diet (80 – 120 mmol/day)Diuretics
Maintenance therapy
Spironolactone+ furosemide
Peripheral edema
Spironolactoneor Amiloride
Goal:Weight loss 0.5 kg/day
Goal:Weight loss 1 kg/day

Grade 3 ascites
< 5 L
Large-volumeParacentesis/TIPS
> 5 LSynthetic plasma expanders
Low sodium diet (70-90 mEq/day)Diuretics
Albumin(6-8 g/L of ascites tapped)
Consensus Report of the International Ascites Club. Hepatology 2003;38:258-66EASL CPG decompensated cirrhosis. J Hepatol 2018;doi: 10.1016/j.jhep.2018.03.024
↓ Post paracentesiscirculatory dysfunction

Ascites infection
Type of infection PMN (/mm3)
Culture result Treatment
Spontaneous bacterial peritonitis
≥ 250 Positive
(usually 1 Organism)
ATB + alb
Culture-negative neutrocytic ascites
≥ 250 Negative ATB + alb
Monomicrobial nonneutrocytic bacterascites
< 250 Positive
(1 Organism)
Symp : as SBP
Asymp : repeat
Secondary bacterial peritonitis
≥ 250 Positive (polymicrobial)
Surgery

SBP : Albumin infusion
• 1.5 g/kg within 6 hr and 1 g/kg on day 3
• ↓ type I HRS (30%->10%) and MR (29%->10%)• Indicated in
1. Cr >1mg/dL
2. BUN >30 mg/dL
3. TB > 4mg/dL

Ascites infection
Type of infection PMN (/mm3)
Culture result Treatment
Spontaneous bacterial peritonitis
≥ 250 Positive
(usually 1 Organism)
ATB + alb
Culture-negative neutrocytic ascites
≥ 250 Negative ATB + alb
Monomicrobial nonneutrocytic bacterascites
< 250 Positive
(1 Organism)
Symp : as SBP
Asymp : repeat
Secondary bacterial peritonitis
≥ 250 Positive (polymicrobial)
Surgery

Ascites infection
TREATMENTINDICATED
PMN>250?
Culture Positive?
TREATMENT NOT INDICATED
NO
Repeat Paracentesis
YES
PMN>250?
Culture Positive?
NO
NO
YES
YES
YESNO

Ascites infection
Type of infection PMN (/mm3)
Culture result Treatment
Spontaneous bacterial peritonitis
≥ 250 Positive
(usually 1 Organism)
ATB + alb
Culture-negative neutrocytic ascites
≥ 250 Negative ATB + alb
Monomicrobial nonneutrocytic bacterascites
< 250 Positive
(1 Organism)
Symp : as SBP
Asymp : repeat
Secondary bacterial peritonitis
≥ 250 Positive (polymicrobial)
Surgery

Primary VS Secondary peritonitis
*Only for free perforation
Ascitic profiles Sensitivity* Specificity*
2/3 of• Total protein > 1g/dL• LDH > ULN of serum LDH • Glucose < 50 mg/dL
100 45
• CEA > 5 ng/mL or• ALP > 240 units/L
92 88
Akriviadis EA, Runyon BA. Gastroenterology 1990Wu SS et al. J Hepatol 2001

Hepatorenal syndrome
Functional renal failure in cirrhosis ↑NO, CO, endogenous canabinoids
Decompensated cirrhosis
Splanchnic vasodilatation
↓effective circulatory volume
Renal failure
RAAS → Renal vasoconstriction
Infection : SBP, UTI
Type 1
Liver function
Type 2

Renal impairment: definitions of kidney disease
EASL CPG decompensated cirrhosis. J Hepatol 2018;doi: 10.1016/j.jhep.2018.03.024
• KDIGO group definitions
Definition Functional criteria Structural criteria
AKI
Increase in sCr ≥50% within 7 days,
OR
increase in sCr ≥0.3 mg/dl within 2 days
No criteria
AKD
GFR <60 ml/min per 1.73m2 for <3 months,
OR
decrease in GFR ≥35% for <3 months,
OR
increase in sCr ≥50 % for <3 months
Kidney damage
for <3 months
CKD GFR <60 ml/min per 1.73 m2 for ≥3 monthsKidney damage
for ≥3 months
Stage 1A (sCr <1.5mg/dl)*
Stage 1B (sCr ≥1.5mg/dl)*

ICA management algorithm for AKI in cirrhosis
*Initial AKI stage is defined as AKI stage at the time of first fulfilment of the AKI criteria;†Treatment of spontaneous bacterial peritonitis should include albumin infusion according to current guidelines
Adapted from Angeli P, et al. J Hepatol 2015;62:968–74;
EASL CPG decompensated cirrhosis. J Hepatol 2018;doi: 10.1016/j.jhep.2018.03.024
• Investigation and management should begin immediately
Initial AKI* stage 1A Initial AKI* stage >1A
Close monitoring
Remove risk factors (withdrawal of nephrotoxic
drugs, vasodilators and NSAIDs, taper/withdraw
diuretics and β-blockers, expand plasma volume,
treat infections† when diagnosed)
Withdrawal of diuretics (if not yet
applied) and volume expansion with
albumin (1 g/kg) for 2 days
Persistance ProgressionResolution
Further treatment of
AKI decided on a
case-by-case basics
Close follow-up
Response
YES NO
Does AKI meet
criteria of HRS?
NO
Specific treatment for
other AKI phenotypes
YES
Vasoconstrictors
and albumin

Hepatorenal syndrome : Diagnosis
1. Cirrhosis with ascites2. Serum creatinine > 1.5 mg/dL3. No improvement after at least 2 days with diuretic withdrawal and
volume expansion with albumin (1g/kg/d, max 100 g/d)4. Absence of other causes
1. shock2. recent treatment with nephrotoxic drugs3. parenchymal renal disease (proteinuria > 0.5 g/d, rbc > 50/HF, abnormal U/S)
Type 1 Rapidly progressive (Cr >2.5 mg/dL or
Ccr <20 ml/min in 2 wk)
Type 2 Slow (months)
Refractory ascites

Hepatorenal syndrome : Treatment Treatment Type I Type II
Correct precipitating factor +++
Vasoactive drugs plus albumin +++ +
Renal replacement therapy +
TIPS + +
Liver dialysis +
Liver transplantation +++ +++• Vasoactive agents : Terlipressin (1 mg q 6 hr, titrate q 2 days,
max 12 mg/d), Norepinephrine, Midodrine • 20%Albumin: IV 20 – 40 g/d

Hepatocellular carcinoma

Hepatocellular carcinoma
US + AFP q 6 months
• Cirrhosis CTP-A,B• Cirrhosis CTP-C if on
transplantation waiting list • Chronic HBV infection
• Asian male > 40 yr • Asian female > 50 yr• Family history of HCC
• Non-cirrhotic F3, based on an individual risk
Screening
Bruix J, AASLD practice guideline 2010Heimbach JK, AASLD practice guideline 2018, EASL guideline 2018

Diagnosis
Bruix J, AASLD practice guideline 2010EASL guideline 2018
Cirrhosis/CH-B with liver nodule
< 1cm
Repeat US q 4 mo
Growing Stable for 1 yr
Ix according to size
Routine surveillance
> 1cm
4-phase MDCT/ dynamic CE MRI
Typical lesion

Typical HCC on 3-phase CT
A phase 30 sec V phase 80 sec
V. or delayed phase wash outA. hypervascular
AND

Diagnosis
Bruix J, AASLD practice guideline 2010EASL 2018
Cirrhosis/CH-B with liver nodule
< 1cm
Repeat US q 3 mo
Growing Stable for 2 yr
Ix according to size
Routine surveillance
> 1cm
4-phase MDCT/ dynamic CE MRI
Typical lesion
HCC Other CE study
Bx
Y
YN
N

Modified BCLC staging system and treatment strategy
*Child–Pugh A without ascites. Applies to all treatment options apart from LT; †PS 1; tumour-induced modification of performance
capacity; ‡Multiparametric evaluation: compensated Child–Pugh class A liver function with MELD score <10, matched with grade
of portal hypertension, acceptable amount of remaining parenchyma and possibility to adopt a laparoscopic/minimally invasive
approach; §The stage migration strategy applies; ‖Sorafenib has been shown to be effective in first line, while regorafenib is
effective in second line in case of radiological progression under sorafenib. Lenvatinib has been shown to be non-inferior to
sorafenib in first line, but no effective second-line option after lenvatinib has been explored. Cabozantinib has been demonstrated
to be superior to placebo in 2nd or 3rd line with an improvement in OS. Nivolumab has been approved in second line by FDA but
not EMA based on uncontrolled Phase 2 data. Please see notes for full details.
EASL CPG HCC. J Hepatol 2018; doi: 10.1016/j.jhep.2018.03.019
Very early stage (0)
Single <2 cm
Preserved liver
function*
PS 0
Early stage (A)
Solitary or
2–3 nodules <3 cm
Preserved liver
function*
PS 0
Intermediate stage (B)
Multinodular,
unresectable
Preserved liver
function*
PS 0
Advanced stage (C)
Portal invasion/
extrahepatic spread
Preserved liver
function*
PS1†–2
Terminal stage (D)
Not transferable HCC
End-stage
liver function
PS 3–4
Prognostic
stage
Solitary2–3 nodules
≤3 cm
Optimal surgical
candidate‡
Yes No
Yes No
Transplant
candidate
Treatment§
Survival >5 years >2.5 years ≥10 months 3 months
Chemoembolization Systemic therapy‖ BSCAblation Resection Transplant
HCC in cirrhotic liver
Ablation

Thank you for your attentions