complex regional pelvic pain syndrome . time for a new paradigm
TRANSCRIPT

COMPLEX REGIONAL COMPLEX REGIONAL PELVIC PAIN SYNDROMEPELVIC PAIN SYNDROME ……..
TIME FOR A NEW PARADIGMTIME FOR A NEW PARADIGM
Alain Alain WatierWatier mdmd, LMCC, FRCP, LMCC, FRCPProfessorProfessorofof GastroenterologyGastroenterologyPelvicPelvic FloorFloor UnitUnitCHUS, QuCHUS, Quéébec, Canadabec, Canada

PELVIPELVI --PERINEAL PERINEAL PAINPAIN

BLADDER PAIN SYNDROMEBLADDER PAIN SYNDROME
TESTICULAR PAINTESTICULAR PAIN
VULVODYNIAVULVODYNIA VESTIBULITISVESTIBULITIS
URETHRAL SYNDROMEURETHRAL SYNDROME
LEVATOR ANI SYNDROMELEVATOR ANI SYNDROME
PROCTALGIA FUGAX
IBSIBS
CRONIC PELVIC PAIN IN MANCRONIC PELVIC PAIN IN MAN
ENDOMETRIOSISENDOMETRIOSIS
DYSMENORRHEADYSMENORRHEA
PUDENDAL NEURALGIAPUDENDAL NEURALGIACLUNEAL NEUROPATHYCLUNEAL NEUROPATHY

PELVIC ORGAN CROSS SENSITIZATIONPELVIC ORGAN CROSS SENSITIZATIONNEUROPATHIC PAINNEUROPATHIC PAINCOMPLEX REGIONAL PAIN SYNDROMECOMPLEX REGIONAL PAIN SYNDROMEFIBROMYALGIAFIBROMYALGIAPOST TRAUMATIC STRESS SYNDROMEPOST TRAUMATIC STRESS SYNDROME
As As specialistsspecialistsin in pelvipelvi--perinealperineal pain pain whatwhat cancan wewe learnlearn fromfrom ……
IBS TMD CFS !!!!IBS TMD CFS !!!!ENDOMETRIOSIS !!!!!ENDOMETRIOSIS !!!!!

VestibulitisVestibulitis/CPP//CPP/urethralurethral obstruction/IBSobstruction/IBS/constipation/constipation
CPP/CPP/dyspareuniadyspareunia//urologicalurological problemsproblems/IBS/IBS
IBS/IBS/DyspareuniaDyspareunia//UrethralUrethral problemsproblems/CPP/CPP
UrethralUrethral syndrome/syndrome/dyspareuniadyspareunia/IBS//IBS/abdominal painabdominal pain
CPP/CPP/unexplainedunexplainedgenitalgenital pain/pain/bladderbladder outletoutletobstruction/obstruction/prostatodyniaprostatodynia

FibromyalgiaFibromyalgia/IBS//IBS/vestibulitisvestibulitis
PenismusPenismus//anismusanismus/IBS/IBS
IC/IC/ headacheheadache/FM/IBS//FM/IBS/ depressiondepression//vulvodyniavulvodynia

PELVIC ORGAN CROSSPELVIC ORGAN CROSS--SENSITIZATIONSENSITIZATION

PELVIC PAIN ASSESSMENT FORMPELVIC PAIN ASSESSMENT FORM

Information about painInformation about painPain Pain mapsmapsSurgicalSurgical historyhistoryMedicationsMedicationsObstetricalObstetrical historyhistoryFamilyFamily historyhistoryMedicalMedical historyhistoryHealthHealth habit habit ((SleepSleephabit)habit)MenstrualMenstrual historyhistory ((dysmenorrheadysmenorrhea, , endometriosisendometriosis))GI / GI / EatingEating / / Rome III Rome III criteriacriteria IBSIBSUrinaryUrinary symptomssymptoms(IC)(IC) ((KidneyKidney stones)stones)SexualSexual/ / PhysicalPhysicalabuse abuse historyhistoryPelvicPelvic varicosityvaricosity pain syndromepain syndromeFibromyalgiaFibromyalgiaImpact Impact ofof pain on pain on sexualsexualactivitiesactivitiesCopingCoping mecanismsmecanismsShort Short FormForm McGillMcGill questionnairequestionnaire

Posture, Posture, gaitgait, , backback, abdomen, , abdomen, lowerlower extremitiesextremitiesSacroiliacSacroiliac jointsjointsChanges Changes ofof skin sensation, skin sensation, numbnessnumbness, , tendernesstendernessChanges in Changes in temperaturetemperature, , colourcolourFibromyalgiaFibromyalgiaExternalExternal genitaliagenitaliaQ Q tiptip testtestVaginaVaginaUnimanualUnimanual examinationexaminationMuscle Muscle tendernesstendernessTrigger pointsTrigger pointsBimanualBimanual examinationexaminationAdnexalAdnexal examinationexaminationSpeculumSpeculumexaminationexaminationRectovaginalRectovaginalexaminationexaminationAbdominal Abdominal examinationexaminationRectoscopyRectoscopyPelvicPelvic floorfloor exam by a exam by a trainedtrained PTPT
NEUROPATHIC PAINNEUROPATHIC PAIN

CUTANEOUS NOCICEPTIVE HYPERSENSITIVITYCUTANEOUS NOCICEPTIVE HYPERSENSITIVITY
PERIPHERAL SENSITIZATIONPERIPHERAL SENSITIZATION
CENTRAL SENSITIZATIONCENTRAL SENSITIZATION
ACTIVATION OF DESCENDING FACILITATIONACTIVATION OF DESCENDING FACILITATION
ALTERED INTRACELLULAR SIGNALINGALTERED INTRACELLULAR SIGNALING
ALTERED ION CHANNEL EXPRESSIONALTERED ION CHANNEL EXPRESSION
ABNORMAL FIRING OR AFFERENT AND EFFERENT PAIN PATHW AYSABNORMAL FIRING OR AFFERENT AND EFFERENT PAIN PATHW AYS
ALTERED PHENOTYPE OF LARGE NERVE FIBERSALTERED PHENOTYPE OF LARGE NERVE FIBERS
AUGMENTED INLAMMATORY RESPONSEAUGMENTED INLAMMATORY RESPONSE
IMMUNE SYSTEM INVOLMENT (MICROGLIA)IMMUNE SYSTEM INVOLMENT (MICROGLIA)
GENETIC VARIATIONGENETIC VARIATION
PATHOPHYSIOLOGY OF NEUROPATHICPATHOPHYSIOLOGY OF NEUROPATHICPAINPAIN

ALLODYNIAALLODYNIADYSESTHESIADYSESTHESIAHYPERALGESIAHYPERALGESIAHYPERPATHYHYPERPATHYPARESTHESIAPARESTHESIACAUSALGIACAUSALGIA
SPECIFIC NEUROPATHIC PAIN QUESTIONNAIRESSPECIFIC NEUROPATHIC PAIN QUESTIONNAIRES
QUANTITATIVE SENSORY TESTING (QST)QUANTITATIVE SENSORY TESTING (QST)
GivesGivesa a phenotypicphenotypic mappingmapping andand maymay definedefine patientspatientsthatthat are more are more proneprone to to respondrespondto certain to certain therapeutictherapeuticagents.agents.
BouhassiraBouhassira

QUANTITATIVE SENSORY TESTING (QST)QUANTITATIVE SENSORY TESTING (QST)
SensorySensorythresholdsthresholds for pain, for pain, touchtouch, vibration, , vibration, heatheat, cold., cold.
AA--deltadelta fibersfibers: cold + : cold + coldcold pain pain thresholdsthresholdsCC--fibersfibers: : heatheat + + heatheat pain pain detectiondetection thresholdsthresholdsAA--betabeta fibersfibers: vibration : vibration detectiondetection thresholdsthresholds
PermitsPermits to to definedefine differentdifferent somatosensorysomatosensoryphenotypesphenotypes
DoesDoesitit help help thethe pain pain clinicianclinician ????

NSAIDsNSAIDs
Inhibition Inhibition ofof serotoninserotonin andand NE NE uptakeuptake((TCAsTCAs, , TramadolTramadol, , DuloxetineDuloxetine, , VenlafaxineVenlafaxine))
BlockageBlockageofof voltage voltage dependantdependantNa Na channelschannels((TCAsTCAs, , LamotrigineLamotrigine , , CarbamazepineCarbamazepine, , oxcarbazepineoxcarbazepine))
Modulation Modulation ofof NMDA NMDA receptorsreceptorsandand/or glutamate/or glutamaterelease release ((TCAsTCAs, , LamotrigineLamotrigine ))
BlockageBlockageofof voltage voltage gatedgatedCaCa channelchannelsubunitsubunit((TCAsTCAs, , GabapentinGabapentin, , PregabalinPregabalin))
Modulation Modulation ofof opioidsopioids receptorsreceptors((opioidsopioids))

CANNABINOIDSCANNABINOIDS

Inhibition Inhibition ofof voltage voltage gatedgatedNa Na channelschannelsLocal Local anesthesicsanesthesics((LidocaineLidocaine, , lidocainelidocaine 5% gel 5% gel andand patch)patch)
Inhibition Inhibition ofof CaCa channelchannel functionfunction + + reductionreduction in in membrane membrane excitabilityexcitabilityTetrazoleTetrazole
Modulation Modulation ofof alphaalpha--2 2 adrenoreceptoradrenoreceptorClonidineClonidine ((creamcream / / transdermaltransdermal patch)patch)
Blocage Blocage ofof adenosineadenosineuptakeuptakeTCAsTCAs ((amitritylineamitrityline 2% + 2% + kkéétaminetamine 1%) (1%) (DoxepinDoxepin 3%)3%)
TRPV1 TRPV1 receptorreceptor agonistagonist ((CapsaicinCapsaicin0.025%0.025%--0.075%)0.075%)(gel / (gel / creamcream ) ) CapsaicinCapsaicindermaldermal patch 8%)patch 8%)

Amitriptyline 2-7 %
Clonidine 0,05-0,2 %
Gabapentine 4-6 %
Baclofène 2-5 %
Ibuprofène 2,5-10%
Cyclobenzaprine 1%
Lidocaine gel 2 %
Lidocaine onguent 5 %
Lidocaïne 10%/kétamine1% (autres [[[[ ]]]] selon condition)

Nitroglycérine 0,2-0,8 % + Lidocaine 10 % ou Morphine 0,2-0,5 %
Kétamine 1 à 10% (+ Morphine 0,2-0,5%)(+ Hydromorphone 0,04-0,1%)
Diltiazem 2%
Nabilone topique(Cannabinoïdes)
Misoprostol 0,0024%- 0,015%

FIBROMYALGIAFIBROMYALGIA



CENTRALCENTRALSENSITIZATIONSENSITIZATION




FIBROMYALGIEFIBROMYALGIE IBSIBS
CRPSCRPS VULVODYNIAVULVODYNIA
PTSDPTSD

THE DESCENDING PAIN CONTROLTHE DESCENDING PAIN CONTROLSYSTEM SHOULD BE ACCESSIBLESYSTEM SHOULD BE ACCESSIBLEBY BOTH BY BOTH BEHAVIORALBEHAVIORAL AND AND PHARMACOLOGICALPHARMACOLOGICAL TREATMENTSTREATMENTS
CAN DESCENDING PAIN CONTROLCAN DESCENDING PAIN CONTROLIMPROVE WITH PRACTICE ?IMPROVE WITH PRACTICE ?
PREDICTIVE OF POSTPREDICTIVE OF POST --OP PAIN ???OP PAIN ???POSTPOST--HYSTERECTOMY ?HYSTERECTOMY ?

WhatWhat about about thethe descendingdescendingpain controlpain controlsystemsystemin in womenwomenwithwith a a historyhistory ofofphysicalphysical / / sexualsexualabuse ???abuse ???


SLEEP DISORDERSSLEEP DISORDERS
FMFMIBSIBSCRPSCRPS
QUESTIONNAIREQUESTIONNAIRE

PHYSICAL/SEXUALPHYSICAL/SEXUALABUSES ANDABUSES AND
PELVIPELVI --PERINEALPERINEALPAINPAIN

SexualSexualabuse abuse historyhistory: : PrevalencePrevalence, , HealthHealth effectseffects,,MediatorsMediators, , andand PsychologicalPsychologicaltreatmenttreatment..Jane Jane LessermanLessermanPsychomaticPsychomaticMedicineMedicine 67: 90667: 906--915 (2005915 (2005))
LongLong--termterm effectseffectsofof childhoodchildhood abuse on abuse on thethe qualityquality ofoflifelife andand healthhealth ofof olderolder peoplepeople: : ResultsResultsfromfrom thethedepressiondepressionandand earlyearly preventionprevention ofof suicide in suicide in generalgeneralpractivepractive projectproject..Brian Draper et Brian Draper et alal..GeriatrGeriatr Soc 56: 262Soc 56: 262--271, 2008271, 2008
SexualSexualabuse abuse andand lifetimelifetime diagnosisdiagnosisofof somaticsomaticdisordersdisordersA A systematicsystematicreviewreview andand metameta--analysisanalysisMollyMolly L. ParasL. ParasJamaJama August 5, 2009August 5, 2009--Vol 302 # 5Vol 302 # 5

A comparaison A comparaison ofof chronicchronic pain patients pain patients andand controlscontrolson on traumatictraumatic eventseventsin in childhoodchildhood..Richard T. Richard T. GoldbgergGoldbgerg et et alal..DisabilityDisability andand rehabilitationrehabilitation ,2000: Vol 22 No. 17, 756,2000: Vol 22 No. 17, 756--763763
ChildhoodChildhood sexualsexualabuse abuse isis associatedassociatedwithwith physicalphysicalillnessillnessburdenburden andand functioningfunctioning in in psychiatricpsychiatric patientspatients50 50 yearsyearsofof age age andand olderolder..Nancy L Nancy L talbottalbot et et alal..PsychosomPsychosomMedMed 2009 May; 71(4): 4172009 May; 71(4): 417--422422
ChildhoodChildhood trauma, trauma, attachmentattachment, , andand abuse by multipleabuse by multiplepartnerspartners..Pamela C. AlexanderPamela C. AlexanderPsychologicalPsychologicalTrauma: Trauma: TherapyTherapy, , researchresearchandand policypolicy. 2009. Vol 1 # 1, 78. 2009. Vol 1 # 1, 78--8888
ChronicChronic pain syndromes pain syndromes andand theirtheir relation to relation to childhoodchildhoodabuse abuse andand stressfulstressful lifelife eventsevents..Astrid Lampe et Astrid Lampe et alalJournal Journal ofof PaychosomaticPaychosomaticResearchResearch54 (2003) 36154 (2003) 361--367367

WE MUST STOP TO PRETENDWE MUST STOP TO PRETEND

THE PHENOMENA DOES EXISTTHE PHENOMENA DOES EXIST

Évaluation complète musculo-squelettiqueMobilisation des tissus mous interne (vaginal-rectal) et externeRelâchement myofascialManipulation articulaireTraitement des trigger pointsStimulation électriqueExercices thérapeutiquesEntraînement de la musculature pelvi-périnéaleUltra-son thérapeutiqueTENSDilatation vaginaleEMG de surfaceBiofeedbackMichel GuérineauElizabeth Rummer / Stéphanie Prendergast (San Francisco)« Headache in the pelvis »Stimulation du nerf tibial postérieur
INTERVENTION THÉRAPEUTIQUEINTERVENTION THÉRAPEUTIQUE
PUDENDAL NEURALGIAPUDENDAL NEURALGIA
TherapeuticTherapeutic targetstargetsMultiple types of Multiple types of medicationmedicationTopicalTopical creamscreams
STATE OF THE ART 2009STATE OF THE ART 2009
PelvicPelvic floorfloor reeducationreeducation
INFILTRATIONSINFILTRATIONS
DECOMPRESSIONDECOMPRESSIONCHIRURGICALECHIRURGICALE
NEUROMODULATION PUDENDALENEUROMODULATION PUDENDALE
BOTOXBOTOX
PharmacologicalPharmacologicalapproachapproach

Those Those whowho do do notnotrespondrespondto to conventionalconventionaltherapiestherapiesusuallyusually havehavea a severeseverehistoryhistory ofofsexualsexualabuseabuse

PTSD COMPLEXPTSD COMPLEX

PSYCHOPSYCHO--NEURONEURO--IMMUNOLOGYIMMUNOLOGY

STRESSSTRESS
HYPOTHALAMUSHYPOTHALAMUS
CRF
LOCUS CERULEUSLOCUS CERULEUS
NENE
AUTONOMOUS NERVOUS SYSTEMAUTONOMOUS NERVOUS SYSTEM

ALLOSTATIC LOADALLOSTATIC LOAD
The price the The price the body pays for wear of body pays for wear of tear tear on on its systemsits systems, , secondarysecondaryto to chronic psychological chronic psychological stress. stress. PhysiologicalPhysiologicalarousal arousal and the and the persistent release of stress hormonespersistent release of stress hormonesor or ««mediatorsmediators»», , sleep deprivationsleep deprivation, , poor dietpoor diet, , and otherand otherhealthhealth--damaging behaviors can result from damaging behaviors can result from feelingfeeling««stressed stressed outout»» with resultant psysiological with resultant psysiological changes. changes. ItItisis possible possible that that stress stress induced disturbances induced disturbances of endocrineof endocrineand neurological systems underlie the ultimate and neurological systems underlie the ultimate expressionexpressionof of diseasedisease

CAN WE HELP THEMCAN WE HELP THEM


FOCUSINGFOCUSING
EugeneEugeneGendlinGendlin PermitsPermits awarenessawarenessof of emotionsemotions..TransformTransform a vague a vague internalinternalsensation sensation intointo a a physicalphysicalsensationsensation

SUGGESTIONSSUGGESTIONS
METAPHORESMETAPHORES
ERICKSONIANERICKSONIANHYPNOSEHYPNOSE

A new A new wayway of of treatingtreating informationsinformationsPermitsPermits thethe spontaneousspontaneousemergenceemergenceof new associations, new of new associations, new emotionsemotions,,awarenessawareness

ART THERAPY

PSYCHOBIOLOGIC TRANSDUCTIONPSYCHOBIOLOGIC TRANSDUCTION
HypnoseHypnoseEMDREMDRBriefBrief therapytherapy
A.A. WeitzenhofferWeitzenhofferB.B. M.H M.H EricksonEricksonC.C. F. ShapiroF. ShapiroD.D. E.L.RossiE.L.Rossi

COMPLEX REGIONALCOMPLEX REGIONALPAIN SYNDROMEPAIN SYNDROME



A NEUROPATHIC (?) PAIN A NEUROPATHIC (?) PAIN DISORDER ASSOCIATED WITHDISORDER ASSOCIATED WITHSIGNIFICANT AUTONOMICSIGNIFICANT AUTONOMICINVOLVEMENTINVOLVEMENT

A A completecompletefunctionalfunctional losslossof of cutaneouscutaneoussympatheticsympatheticvasoconstrictorvasoconstrictoractivityactivityin an in an earlyearly stage, stage, withwith recoveryrecovery. This . This autonomicautonomic dysfunctiondysfunction originatesoriginates in in thethe CNSCNS
A spinal component to A spinal component to microcirculatorymicrocirculatory abnomalitiesabnomalitieswhichwhich appearedappearedto to manifestmanifestitselfitself throughthrough a neural a neural antidromicantidromic mechanismmechanism
A positive feedback circuit, A positive feedback circuit, consistingconsistingofof primaryprimary afferentafferent neuronneuron, spinal , spinal cordcordneuronsneurons, , sympatheticsympatheticneuronsneurons, , andand a a pathologicpathologic synpatheticsynpatheticcouplingcoupling
SNS SNS andand vascularvascular abnormalitiesabnormalities
ExageratedExageratedregionalregional inflammation inflammation responseresponse
ImpairmentImpairment ofof highhigh--energyenergyphosphate phosphate metabolismmetabolism
AbnormalAbnormal oxidativeoxidative stressstress
AfterAfter a partial nerve a partial nerve lesionlesion, excessive , excessive antidromicantidromic activation activation ofof undamagedundamagedafferentafferent C C fibersfibers andand neuropeptide release, neuropeptide release, leadingleading toto acute vasodilatation acute vasodilatation withinwithinthethe innervation innervation territoryterritory ofof thethe affectedaffectednerve has been nerve has been demonstrateddemonstrated
FrequentFrequent presencepresenceofof humanhuman lymphocyte antigenlymphocyte antigen--DQ1DQ1

AutoimmuneAutoimmune diseasedisease
Cortical changesCortical changesOngoingOngoing pain pain altersalters somatosensorysomatosensoryprocessingprocessingCortical Cortical hyperexcitabilityhyperexcitabilityCortical Cortical reorganizationreorganization

**********
CouplingCoupling betweenbetweenthethe sympatheticsympatheticandand afferentafferent neuronsneurons

BRADYKININBRADYKININ

NANA
SUBSTANCE PSUBSTANCE P

SKIN TEMPERATURESKIN TEMPERATURESUDOMOTOR FUNCTION TESTINGSUDOMOTOR FUNCTION TESTINGELECTRODIAGNOSTIC STUDIESELECTRODIAGNOSTIC STUDIESQUANTITATIVE SENSORY TESTINGQUANTITATIVE SENSORY TESTINGLASER DOPPLER IMAGING LASER DOPPLER IMAGING (Test skin (Test skin autonomicautonomic reflexesreflexes))
ShouldShould wewe test test somesomeofof ourour patients patients withwithpain an pain an autonomicautonomic manifestationsmanifestations

In In somesomecases cases pelvipelvi--perinealperineal pain pain seemsseemsto to bebe out out ofof proportion to identifiable causesproportion to identifiable causesofof pain. pain. ((AllodyniaAllodynia , , hyperpathyhyperpathy)) Variations Variations in skin in skin colorcolor andand temperaturetemperature andand abnormalabnormalsweatingsweatinghashasalsoalsobeenbeendescribeddescribed
CRPS OF THE PELVIC FLOORCRPS OF THE PELVIC FLOOR

GANGLION IMPAR BLOCKGANGLION IMPAR BLOCK

SympatheticSympatheticbloc bloc atat thethelevellevel ofof L2L2
ICICPerinealPerineal painpainIBSIBS

DESENSITIZATIONDESENSITIZATION
TheoreticallyTheoretically basedbasedon on thethe abilityability ofof bodybody’’ sstissues to tissues to adaptadapt in in responseresponseto to demanddemand
SufficientSufficient intensityintensity andand durationduration to to provideprovideadequateadequateinput to change input to change thethe abnormalabnormalCNS CNS activityactivity

SELFSELF--REGULATIONREGULATION
InnateInnate abilityability to to learnlearn to to modifymodify andand modumodu--latelate ««autonomicautonomic»» responseresponseto to reachreach aahealthierhealthier homeostatichomeostaticstatestate
TechnonologyTechnonologyassistedassistedselfself--modulationmodulation::NeuromotorNeuromotor + + otherother learninglearning withwith BFBBFB
TryTry to to reducereducethethe perception perception ofof pain viapain viamodification modification ofof thethe autonomicautonomic componentscomponents
HeartHeart beat Skin beat Skin temperaturetemperatureRespiratoryRespiratory rate rate SweatSweatresponseresponseType Type ofof breathingbreathing VasospasmVasospasmBloodBlood pressure Vasodilatationpressure VasodilatationBrainBrain wavewavepatterns patterns MuscularMuscular spasmsspasmsElectroElectro--dermaldermal responseresponse

REFLECTIONS, IMAGERY, ANDREFLECTIONS, IMAGERY, ANDILLUSIONS: THE PAST, PRESENTILLUSIONS: THE PAST, PRESENTAND FUTURE OF TRAINING THE AND FUTURE OF TRAINING THE BRAIN IN COMPLEX REGIONALBRAIN IN COMPLEX REGIONALPAIN SYNDROMEPAIN SYNDROME
Dr G. Dr G. LorimerLorimer MoseleyMoseley
GRADED MOTOR IMAGERY (MIRROR THERAPY)GRADED MOTOR IMAGERY (MIRROR THERAPY)
InducingInducing thethe illusion illusion thatthat thethe affectedaffected limblimb isissmallersmaller thanthan itit reallyreally isis reducesreducesthethe pain pain andandswellingswelling causedcausedby by movementmovementofof thethe limblimb
IMPLICATIONS IN PELVIIMPLICATIONS IN PELVI --PERINEAL PAIN !!!!!PERINEAL PAIN !!!!!


«« AUTONOMIC NERVOUS SYSTEMAUTONOMIC NERVOUS SYSTEMDYSFUNCTION DYSFUNCTION »»
Wilfrid Wilfrid JJäänignig

THE SYNPATHETICTHE SYNPATHETICNERVOUS SYSTEMNERVOUS SYSTEMAND BODY PROTECTION,AND BODY PROTECTION,INFLAMMATION, PAIN,INFLAMMATION, PAIN,AND HYPERALGESIAAND HYPERALGESIA

IBS & AUTONOMIC NERVOUS SYSTEMIBS & AUTONOMIC NERVOUS SYSTEM

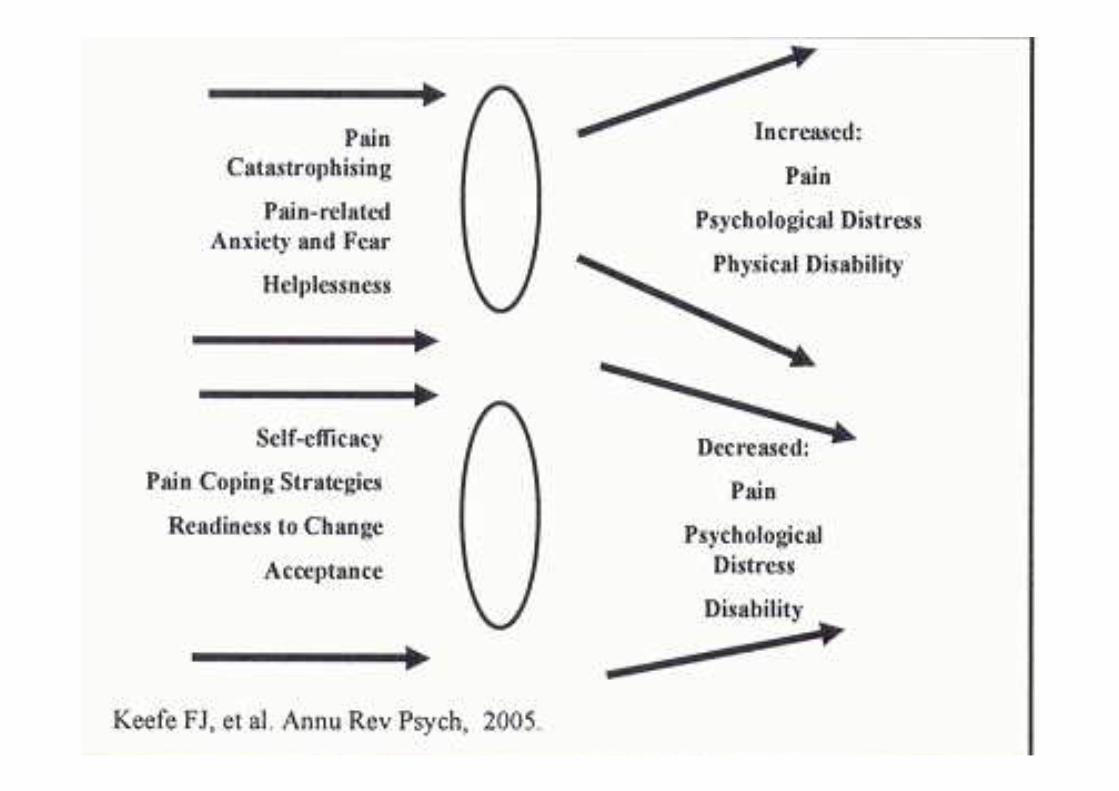
PSYCHOLOGY PSYCHOLOGY ANDAND
CHRONIC PAINCHRONIC PAIN

THE EFFECT OF PERSONNALITY ON CENTRALTHE EFFECT OF PERSONNALITY ON CENTRALPAIN PROCESSINGPAIN PROCESSING
RESILIENCERESILIENCE
PAIN ACCEPTANCEPAIN ACCEPTANCE
CATASTROPHYSINGCATASTROPHYSING
HYPERVIGILENCEHYPERVIGILENCE

TraumaticTraumatic lifelife eventseventsscreeningscreeningquestionnairequestionnaireTrauma Trauma scalescaleofof DavidsonDavidsonResilienceResiliencescalescaleChronicChronic pain pain acceptanceacceptancequestionnairequestionnaireFearFear avoidanceavoidancebeliefsbeliefsquestionnairequestionnairePain Pain andand catastrophysingcatastrophysingscalescalePain vigilance Pain vigilance andand awarenessawarenessquestionnairequestionnaireHospitalHospital anxietyanxiety andand depressiondepressionscalescalePain Pain intensityintensity questionnairequestionnaireTheThe impairmentimpairment andand functionningfunctionning inventoryinventoryDisabilityDisability andand functioningfunctioning inventoryinventory

AND WHAT ABOUT THEAND WHAT ABOUT THE
SUFFERINGSUFFERING
OF THESE PATIENTSOF THESE PATIENTS

WHAT ABOUTWHAT ABOUT ……....
MOTIVATIONAL ENHANCEMENTMOTIVATIONAL ENHANCEMENTTHERAPYTHERAPY
OPTIMISM INTERVENTIONOPTIMISM INTERVENTION

SOMATOSENSORY LANGUAGESOMATOSENSORY LANGUAGEWhereWhere isis thethe pain ?pain ?How How isis thethe sensation sensation perceivedperceived??WhatWhat cancan I do to I do to makemake thethe pain stop ?pain stop ?
LIMBIC LANGUAGELIMBIC LANGUAGEWhatWhat pain pain meansmeansto me ?to me ?How How isis thethe pain pain changingchanging thethe lifelife I I hadhadbeforebefore thethe pain ?pain ?WhatWhat cancan I do to I do to recoverrecover mymy lifelife ??

IN CONCLUSIONIN CONCLUSION

OverlapOverlap ofof patient patient andand healthyhealthy populationspopulations……..HowHow do do youyou becomebecomea a chronicchronic patientspatients……....
VisceroViscero--somaticsomaticsensitivitysensitivityPeripheralPeripheral andand central central sensitizationsensitizationLimbicLimbic systemsystemresponsivenessresponsivenessAutonomicAutonomic nervousnervoussystemsystemactivityactivity
Neurocognitive Neurocognitive factorsfactorsSelectiveSelectiveattention to attention to bodilybodily sensationssensationsCatastrophysingCatastrophysingSymptomsSymptomsrelatedrelated worriesworriesIllnessIllness behaviorbehaviorPsychologicalPsychologicalstressorsstressors

GreaterGreater prevalenceprevalencein in womenwomen
HistoryHistory ofof adverse adverse earlyearly lifelife eventseventsandand stressstresssensitivitysensitivity
ComorbidityComorbidity withwith disordersdisorders ofof moodmood andand affectaffect
ResponseResponseto to centrallycentrally actingacting therapiestherapies((DuloxetineDuloxetine MilnacipranMilnacipran , , TCaTCa, SSRI), SSRI)

EvidenceEvidencefor for alteredaltered pain perception pain perception andand processingprocessing
HypersensitivityHypersensitivity to to experimentalexperimental stimulistimuli
CompromisedCompromiseddiffuse diffuse noxiousnoxious inhibitoryinhibitorycontrol ( DNIC) control ( DNIC) (FM, IBS, (FM, IBS, VulvodyniaVulvodynia, CRPS), CRPS)
EvidenceEvidencefromfrom brainbrain imagingimaging studiesstudiesofofalteredaltered pain pain processingprocessingandand modulationmodulation
EvidenceEvidenceofof structural structural brainbrain abnormalitiesabnormalities(Changes in (Changes in greygrey mattermatter densitydensity or cortical or cortical thicknessthicknessin FM, IBS,in FM, IBS,headacheheadache))
EvidenceEvidenceofof alteredaltered neurocognitive neurocognitive functionfunction(FM, (FM, lowlow backback pain, IBS,PTSD)pain, IBS,PTSD)
EvidenceEvidenceofof increasedincreasedactivityactivity in central arousalin central arousalcircuits circuits andand sympatheticsympatheticnervousnervoussystemsystemactivityactivity((EnhanceEnhancestress stress responsivenessresponsiveness) ( FM, IBS, TMJD, PTSD)) ( FM, IBS, TMJD, PTSD)
EvidenceEvidenceofof commoncommongeneticgeneticsusceptibilitysusceptibility(Pain amplification (Pain amplification andand psychologicalpsychologicaldistressdistress))

WHEREWHEREARE WEARE WESTANDINGSTANDINGNOW !!!!!NOW !!!!!

FunctionalFunctional pain syndromes pain syndromes shouldshould notnotbebe individualizedindividualized
WeWe shouldshould stop stop treatingtreating justjust thethe ««organorgan»»((endend--organorgan--specificspecificsyndrome) BUT syndrome) BUT wewemust must integrateintegrate thethe pain syndromepain syndrome
PeripheralPeripheral ««organicorganic»» etiologyetiology ofof symptomssymptomsare possible but a more are possible but a more integratedintegrated psychopsycho--sociosocio--neurobiologicneurobiologic approachapproach isis mandatorymandatory

•• Alain Alain WatierWatier mdmd, LMCC, FRCP, LMCC, FRCP•• ProfessorProfessorofof GastroenterologyGastroenterology•• DirectorDirector ofof PelvicPelvic FloorFloor UnitUnit•• PelvicPelvic FloorFloor reeducationreeducation(Lyon)(Lyon)•• FacultFacultéé de mde méédecine et des Sciences de la Santdecine et des Sciences de la Santéé
de lde l’’ UniversitUniversitéé de Sherbrookede Sherbrooke•• CHUSCHUS--HôtelHôtel--DieuDieu•• 580 580 BowenBowenSud Sherbrooke QuSud Sherbrooke Quéébec Canada J1G2E8bec Canada J1G2E8•• 819819--346346--1110 1110 [email protected]@abacom.com