complications of radiation therapy for childhood...
TRANSCRIPT

COMPLICATIONS OF RADIATION THERAPYFOR
CHILDHOOD CANCERS
Siddhartha LaskarAssociate Professor
Department of Radiation OncologyTata Memorial Hospital, Mumbai
INDIA([email protected], www.tatamemorialcenter.com)
S Laskar ICARO 2009

* WHO Projection - 2005
YEAR GLOBAL DEVELOPING WORLD PERCENT.(Millions) (Millions) OF GLOBAL
1985 7.6 3.9 52%1990 8.1 4.1 51%2000 10.1 5.4 53%
2020* 20.0 14.0 70%
CANCER BURDENCANCER BURDENCANCER BURDEN
NEW CASES OF CANCER
“Paediatric Malignancies account for 3-5% of the burden”
S Laskar ICARO 2009

AVERAGE ANNUAL INCIDENCE OF CHILDHOOD CANCERS
IARC 2005S Laskar ICARO 2009

RELATIVE FREQUENCIES OF MAJOR TUMOUR TYPES
IARC 2005S Laskar ICARO 2009

ROLE OF RADIOTHERAPY IN CHILDHOOD CANCERS
Hodgkin’s LymphomaEarly StageAdvanced Stage
> 90%Poor Prognostic Group
Nasopharyngeal Carcinoma 100%
CNS Tumors > 90%
Ewings Sarcoma/ PNETDefinitivePost Operative
40%30-40%
Rhabdomyosarcoma IRS Gr III, Unfav. Histology
NR- Soft Tissue Sarcoma > 80%
Wilms Tumor Stage III FH, All UH
Retinoblastoma Non Amenable to Focal Th.Vitreous Seeding
Leukemia (CNS Prophylaxis) Depends upon type of CTh
Neuroblastoma Residual, Unfavourable
S Laskar ICARO 2009
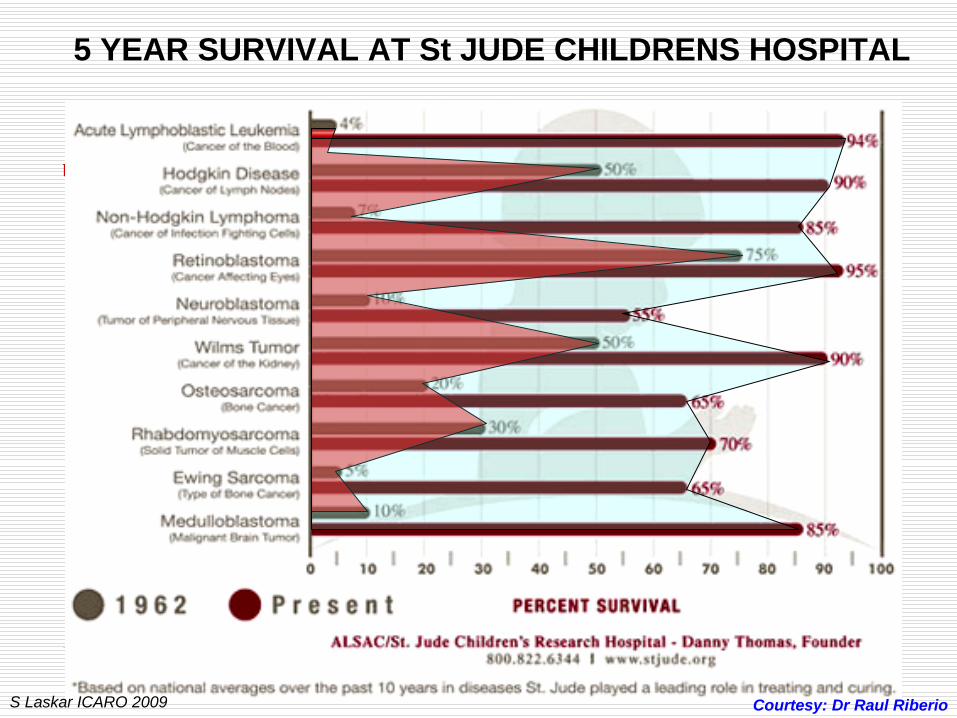
5 YEAR SURVIVAL AT St JUDE CHILDRENS HOSPITAL
Courtesy: Dr Raul RiberioS Laskar ICARO 2009

UNITED STATES DATA
1 in 640 persons between the ages of 20 and 39years is a childhood cancer survivor (~300,000)
Courtesy: Dr Raul RiberioS Laskar ICARO 2009

ACUTE TOXICITIES
S Laskar ICARO 2009

Dermatitis
Mucositis
Enteritis
Cystitis
Dysphagia
Xerostomia
Impaired Taste
Hoarseness of Voice
Headache
Nausea & Vomiting
Hematological
Radiation Dose: 50-60Gy @ 1.8-2.0Gy/ fr
Potentiating Factors:Skin Condition/ Connective Tissue DisordersPrior Interventions: Surgery/ ChemotherapyConcurrent ChemotherapyPoor Nutrition & HyegienePoor Orodental HyegienePoor Skin Care
Management:Optimal Sequencing with Chemo Optimal Dose/ Fractionation & RT Volume Optimal Radiotherapy Plan (skin dose)Skin CareMaintain Nutrition & HyegieneMaintain Orodental Hyegiene
S Laskar ICARO 2009

RADIOTHERAPYPrimary: 66 – 70 GyNeck: 50 Gy/ 25 fr
CHEMOTHERAPYNeoadjuvantConcomittant
Adjuvant
CARCINOMA OF NASOPHARYNX
S Laskar ICARO 2009

IMRT CONVENTIONAL RT
DOSIMETRIC COMPARISION OF TREATMENT PLANS
S Laskar ICARO 2009

PTV70 (70.2Gy/ 33# @ 2.12Gy/#)
PTV59.4 (59.4Gy/ 33# 1.8Gy/#)
PTV52.8 (52.8Gy/ 33# 1.6Gy/#)
PTV70
PTV59.4
PTV52.8
IMRT FOR CA NASOPHARYNX
S Laskar NPX IMRT 03

IJROBP DEC 2008S Laskar ICARO 2009

42.8
53.447.2
52
32.1
55.4
41.9
57.4
0
10
20
30
40
50
60
Dos
e in
Gy
Spinal Cord Brain stem ContralateralParotid
IpsilateralParotid
IMRTConventional RT
COMPARATIVE DVH FOR CRITICAL ORGANS
Laskar, IJROBP Dec 2008S Laskar ICARO 2009

Laskar, IJROBP Sept 2008S Laskar ICARO 2009

TIME TO DEVELOPMENT OF GRADE II TOXICITY
Laskar, IJROBP Dec 2008S Laskar ICARO 2009

HELICAL TOMOTHERAPY
Significant Improvement in Normal Tissue SparingS Laskar ICARO 2009

S Laskar ICARO 2009

PHOTON IMRT PROTON IMRT
S Laskar ICARO 2009

LATE TOXICITIES
S Laskar ICARO 2009

Cardiovascular
Visual
Psychosocial
Dental
Musculoskeletal Pulmo
nary
Gastrointestinal
Genitourinary
SecondTumor
Endocrine
Auditory
Neurocognitive
LateEffects
S Laskar ICARO 2009

CHRONIC CONDITIONS IN ADULT SURVIVORS OF CHILDHOOD CANCER
Condition Relative Risk of Grade 3 or 4 Complication as Compared to
Siblings
Major Joint Replacement 54. 0
Congestive Heart Failure 15.1
Second malignant neoplasm 14.8
Cognitive dysfunction, severe 10.5
Coronary artery disease 10.4
Cerebrovascular Accident 9.3
Renal failure or dialysis 8.9
Hearing loss not corrected by aid 6.3
Legally blind or loss of eye 5.8
Ovarian failure 3.5
Oeffinger et al, NEJM 2006S Laskar ICARO 2009

CAUSE OF MORTALITY IN SURVIVORS CANCER
Recurrent
Cancer
Second
Malignancy/
Neoplasm
Cardiac
Toxicity
Pulmonary
Disease
Other
Sequelae
Non‐
Treatment
Related
Childhood
Cancer
Survivor Study
N = 2823
57% 15% 7% 2% 4% 15%
Piedmont
Region, Italy
N = 143
62.2% 12.6% 1.4% NA 8.4% 15.4%
British
Columbia,
Canada
N = 181
69.1% 7.7% 4.4% 2.2% 5.5% 11.1%
S Laskar ICARO 2009

TIMELINE OF LATE EFFECTS
Paulino AC, IJROBP 2004S Laskar ICARO 2009

EFFECT OF RT ON MUSCULOSKELETAL DEVELOPMENT
Factors Influencing Growth
• Chronological age at treatment• RT volume• Total RT dose• RT dose per fraction• Site of treatment• Homogeneity of growth plate irradiated• Surgery• Chemotherapy
S Laskar ICARO 2009

RELATIVE LOSS OF ADULT HEIGHT
• 7.7% (13cm) with RT dose > 33Gy, Entire spine (pre-pubertal age)• No clinically significant loss of height with low dose RT • IFRT associated with clinically insignificant height loss• No disproportion between sitting & standing height
William KY, IJROBP 1993;28:85StanfordS Laskar ICARO 2009

HEIGHT DEFICIT FROM RADIOTHERAPY
Age at treatment (yrs)
Height deficit (cm) after 10Gy
Height deficit (cm) after 20Gy
Height deficit (cm) after 30Gy
2 2.4 4.8 7.2
4 1.8 3.5 5.3
6 1.2 2.4 3.6
8 0.8 1.5 2.3
Hogeboom et al, Med Pediar Oncol 2001S Laskar ICARO 2009

• Hypoplasia of right flank secondary to hemiabdomen RT at age 3 years for FH Wilms’ tumor
• Dose: 36Gy in 20 fractions
S Laskar ICARO 2009

BOWEL OBSTRUCTION
• 131 of 1,910 children (6.9%) enrolled in NWTS-3 at median follow-up of 5.1 years
• Etiology was bowel adhesions in 104, intussusception in 17, internal hernia in 2
• Risk factors: higher local tumor stage, extrarenal intravascular involvement, en bloc resection of other organs
• Postoperative RT not a risk factor
Ritchey ML et al, Ann Surg 1993S Laskar ICARO 2009

BOWEL OBSTRUCTION
• At University of Iowa, SBO was seen in 6 of 42 children who received RT with median follow-up of 15.1 years for Wilms’ tumor
• 5 yrs:9.5%
• 10 yrs:13%
• 15 yrs:17%
• Time from surgery to RT borderline significant (< 10 days vs. > 10 days)
Paulino et al, IJROBP 2000S Laskar ICARO 2009
PNEUMONITIS: NWTS-3 EXPERIENCE
• 153 pts with Stage IV, FH received whole lung RT
• 19 (13%) developed diffuse interstitial pneumonitis
• 15 unknown etiology, 3 pneumocystis, 1 varicella
• Only 4 of 15 (27%) with pneumonia of unknown etiology survived
Green DM et al, Cancer 1989

CARDIOVASCULAR LATE EFFECTS
STANFORD(1960-1995)
2498 Pts. 754 Deaths 16% CV disease
JCRT(1969-1996)
794 Pts. 124 Deaths 14%CV disease
EORTC(1963-1986)
1449 Pts. 240 Deaths 7%CV disease
BNLI 1043 Pts. 43 Deaths 14%CV disease
Decreasing CV deaths with improving therapy (CT & RT)
Stage I & II at Stanford (CV deaths after 15yrs of treatment)1962 - 1980: 812 pts. ------ 5.4%1980 – 1996: 628 pts. ------ 0.8%
S Laskar ICARO 2009

No of pts No of pts with renal failure
Incidence of Renal Failure (%)
2 years 4 years 16 years
Unilateral 5312 15 0.1 0.2 0.6
Bilateral - - - - -
NWTS-1 41 7 9.8 9.8 16.6
NWTS-2 43 7 14.6 14.6 22.3
NWTS-3 181 18 6.6 8.3 12.7
NWTS-4 177 7 2.6 5.8 _
RENAL FAILURE
Ritchey ML et al, Med Pediatr Oncol, 1996S Laskar ICARO 2009

PREGNANCY OUTCOME
• Increased frequency of following were seen in female patients who have received prior flank or tumor bed RT on NWTS 1-4
Fetal malpositionPremature laborOffspring with low birthweight, premature birth (< 36 weeks of gestation) and congenital anomalies
Green DM et al, JCO 2002S Laskar ICARO 2009

Hong et al., IJROBP 2004
3D-CRT vs. IMRT FOR EXTREMITY SARCOMAS
S Laskar ICARO 2009

CAX
10cm SUP
3D-CRT IMRT
Hong et al., IJROBP 2004S Laskar ICARO 2009

Reduction of Volumes receiving 100% dose using IMRTFemur: 57%Normal Soft Tissue: 78%Normal Skin: 45%Mean Skin Dose: Decreased by 14%
Hong et al., IJROBP 2004S Laskar ICARO 2009

a) 3D CRT b) IMRT c) PROTONS
3D CRT vs. IMRT vs. PROTONS FOR PELVIC SARCOMA
Lee et al, IJROBP 2005S Laskar ICARO 2009
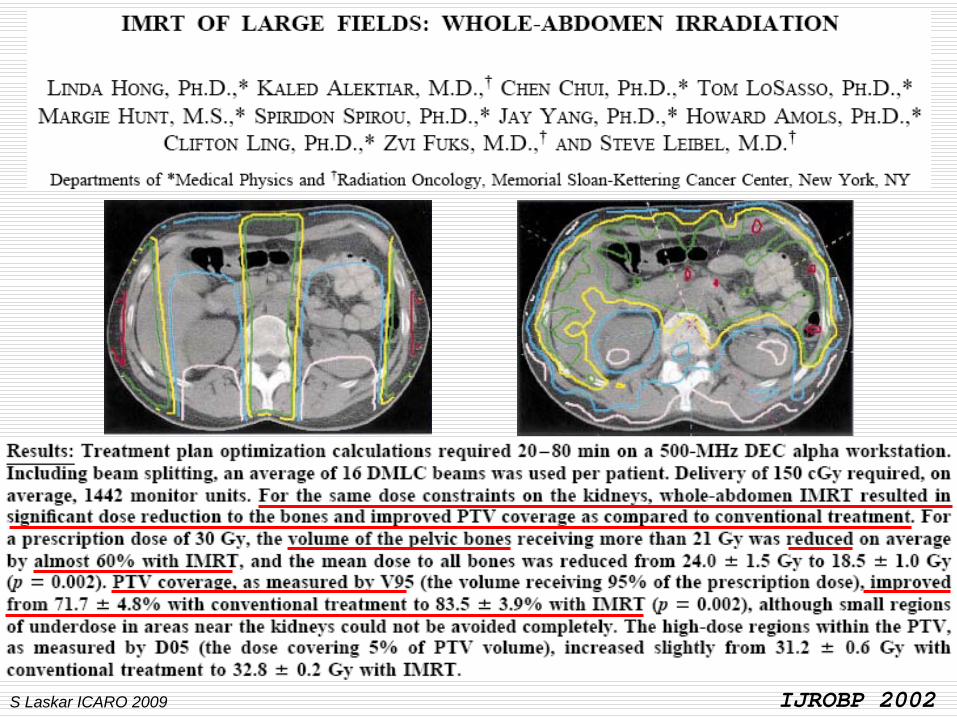
IJROBP 2002S Laskar ICARO 2009

Significant Reduction in Volume of Bony Wall of Orbit inHigh Dose Region
S Laskar ICARO 2009

2002 2008
S Laskar STS CRT S Laskar ICARO 2009

2004
2008
S Laskar STS Brachy 04S Laskar ICARO 2009

TYPE/ SITE RELATIVE RISK ABSOLUTE RISK /10,000 pts,Per Yr.
RELATIVE RISKIn 10yr survivor
ABSOLUTE RISK In 10yr survivor Per 10,000 pts,Per Yr.
All cancers 3.5 (3.1 – 3.8) 56.2 4.7 (3.8 – 5.7) 111.7
Leukemia 32.4 (25.5 – 40.6) 16.8 16.2 (6.5 – 33.3) 9.9
NHL 18.6 (13.8 – 24.6) 10.7 32.7 (19.7 – 51.1) 27.8
Solid tumorsFemale breastLung
2.4 (2.1 – 2.7)2.5 (1.8 – 3.4)4.2 (3.3 – 5.2)
29.3 11.3 13.5
3.6 (2.8 – 4.6)4.6 (3.0 – 6.6)7.3 (4.7 – 10.6)
74.439.533.8
RISK OF SECOND CANCERS
Van Leeuwen FE, J Clin Oncol 1994;12:312Swerdlow AJ, Br Med J 1992;304:1137Tucker MA, NEJM 1988;318:76
S Laskar ICARO 2009

SECOND CANCERS ??????????????????
IJROBP 2003S Laskar ICARO 2009

Its 15 Years after the first clinical use of IMRT“NO REPORT OF 2ND MALIGNANCIES TILL DATE”
S Laskar ICARO 2009

Lancet Oncology 2006S Laskar ICARO 2009

Lancet Oncology 2005S Laskar ICARO 2009

ISSUES……………..
Exact mechanism of radiation induced second cancers
Which is more harmful ??Low Dose RadiationHigh Dose Radiation
Who is the culprit ??RadiationChemotherapy
S Laskar ICARO 2009

IMRT!!
S Laskar ICARO 2009

SUMMARY
Radiation therapy associated with both acute & late sequlae
Severity influenced by:Patient Related/ Tumor Related/ Treatment Related Factors
RT Related Acute Sequelae: Self Limiting
RT Related Late Sequelae: Site Irradiated, Volume, Dose, FractionationConcurrent Therapies
Optimal Sequencing Essential for Favorable Outcome
S Laskar ICARO 2009

Thank YouS Laskar ICARO 2009