computed tomography and the diagnosis … · –zollinger-ellison, prolactinomas ......
TRANSCRIPT

Parathyroid Disease
Frederick S. Rosen, MD
Faculty Advisor: Anna M. Pou, MD
The University of Texas Medical Branch
Department of Otolaryngology
Grand Rounds Presentation
March 2002
2
Calcium Regulation
• 99% of body calcium in skeleton
• Miscible Pool: 40% bound to protein, 13% complexed w/ anions, 47% free ionized
• PTH: Increased Ca, Decreased PO4, Increased Vitamin D
• Vitamin D: Increased Ca, Increased PO4, Decreased PTH (slow)
• Kidney, Bones, GI Tract

3

4
Hyperparathyroidism
• 85% solitary adenoma
• 15% hyperplasia or
multiple adenomata
• <1% parathyroid
carcinoma
•Primary HyperPTH: Most
common; postmenopausal
women
•Secondary HyperPTH:
Usually renal failure
•Tertiary HyperPTH: Chronic
Renal Failure; low or normal
Ca, irrepressible PTH
5
Hyperparathyroidism
• Usually asymptomatic
• Fatigue and weakness – up to ½ resolve
• Bone and joint pain, stones and hematuria (Reflect decreased bone density & nephrolithiasis)
• Osteitis Fibrosa Cystica (Brown tumor) and Nephrocalcinosis rare
• Calciphylaxis

6
Calciphylaxis

7
Hyperparathyroidism: Signs &
Symptoms
• Ca=12 mg/dL-14 mg/dL
• Constitutional: fatigue, wt loss, anorexia
• Musculoskeletal: pain, weakness
• Renal: colic, hematuria
• GI: Pancreatitis, constipation, PUD, nausea
• Neuro: H/A, memory loss, psychosis, insomnia
• Skin: pruritus, brittle nails

8
Hyperparathyroidism
•Slow progression
•75% of asymptomatic patients remain symptom
free
•Risk factors: XRT, chronic Lasix, chronic
lithium, family h/o MEN
9
• Elevated serum Ca X 3
• Elevated PTH
• Other:
– Albumin
– Alkaline Phosphatase
– Phosphorous
– BUN/Cr
– 24-hour urine Ca
– Bone Mineral Density
Hyperparathyroidism: Diagnosis

10
Localization
•4 glands in 87% of patients; range 2-6 glands
•Internal carotid artery to AP window
•Superior parathyroid glands within 1 cm of RLN piercing cricothyroid membrane
11
Localization
• Location of Ectopic glands:
• Paraesophageal (28%)
• Mediastinum (26%)
• Intrathymic (24%)
• Intrathyroidal (11%)
• Carotid sheath (9%)
• High cervical (2%)

12
Localization
• Ultrasound
• CT
• FNA
• MRI
• Angiography w/ or w/o selective venous
sampling (Angioablation)

13
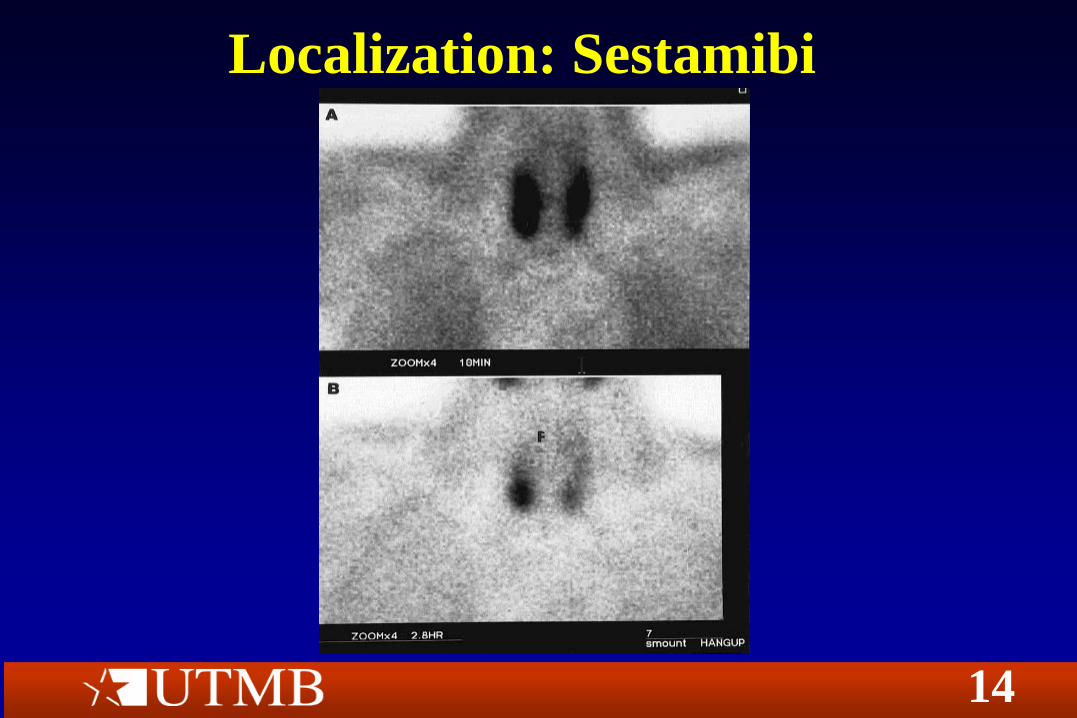
Localization: Sestamibi
• 1989: Cardiac imaging, Technetium derivative
• SPECT imaging
• False Positives: Thyroid nodules
• False Negatives: Small adenomas, hyperplasia
• Cheap
14
Localization: Sestamibi

15
Medical Management
• Q6months
– Ca
– Cr
– U/A
– PTH
•Q12months
–Bone Density
Oral Calcium < 1 g/day

16
Medical Management
• Severe Hypercalcemia:
– Saline-furosemide diuresis
– Bisphosphonates (onset of action 24-48h)
– Calcitonin (immediate onset)
– Hemodialysis

17
Medical Management
• Estrogen in post-menopausal women
• Chronic Renal Failure (Hypo-Vitamin D,
Hyperphosphatemia, HyperPTH)
– Calcium salts
– Vitamin D or analogs
18
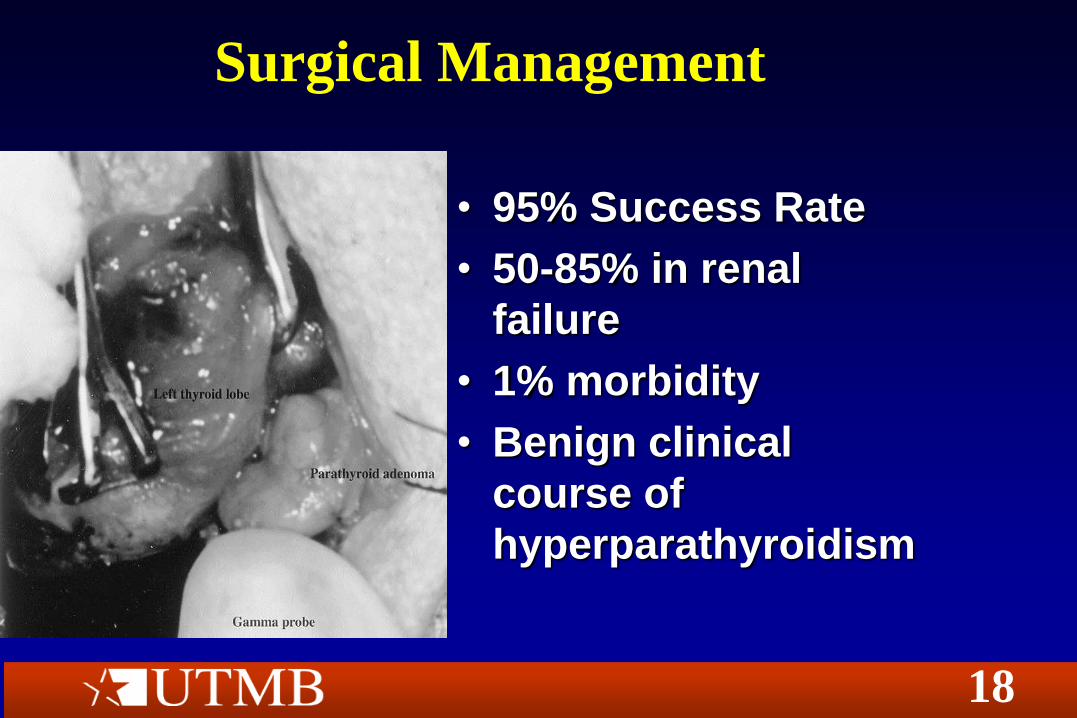
Surgical Management
• 95% Success Rate
• 50-85% in renal
failure
• 1% morbidity
• Benign clinical
course of
hyperparathyroidism
19
Surgical Management • NIH Guidelines (1990)
– Symptomatic HyperPTH
– Serum Ca 1-1.6 mg/dL above normal
– H/o life-threatening hypercalcemic event
– ClCr <70% of expected
– Kidney stones on radiograph
– Elevated urine Ca (>400 mg/dL)
– Z-score>2
– Patient requests surgery
– Consistent followup unlikely
– Complicating comorbid condition
– Age<50 yo

20
Surgical Management
• Renal failure (Unresponsive to medical tx)
– Renal osteodystrophy/pathologic fractures
– Intractable bone pain/pruritus
– Calciphylaxis

21
Surgical Management
• New Tools of the Trade: Minimally Invasive
Surgery
– Pre-operative Sestamibi
– Intraoperative rapid PTH (50%, 80%)
– Hand-held gamma probe
– Methylene blue

22
Surgical Management

23
Surgical Management
• Adenoma
– Unilateral vs. Bilateral Exploration
– rPTH vs. Frozen Section
• Hyperplasia/Multiple adenomata
– Subtotal – less hypocalcemia
– Subtotal w/ autotransplantation – MEN, Renal
Failure
– Total w/ Cryopreservation – up to 1 year

24
Autotransplantation
• Iced saline bath
• 20-30 mg; 10-20 1-2 mm slices
• SCM vs. Brachioradialis
• Pockets marked with clips
• Up to 50% failure rate

25
Surgical Complications
• Failure: missed ectopic adenoma, incomplete
resection in multi-gland dz.
• Hypocalcemia (20-30%)
– Wait for appearance of symptoms
• TVC paralysis (<1%)
• Hematoma
26
Multiple Endocrine Neoplasia • MEN I
– Moderate-severe hyperPTH in 85%
– Zollinger-Ellison, prolactinomas
– Auto Dominant, MEN1(tumor suppressor), Chromosome 11
• MEN IIa
– Mild hyperPTH in 70%
– Medullary Carcinoma 100%
– Pheochromocytoma
– Auto Dominant, RET proto-oncogene
27
Hyperparathyroidism: Miscellany
• Parathyroid carcinoma
– Hi PTH, palpable neck mass, Hi Ca post-op
– Regional/distant mets in 25-30%, Local recurrence 30%
– Surgery: Ipsilateral thyroid lobe, skeletonization of RLN, paratracheal nodes
• Hyperparathyroidism-Jaw Tumor Syndrome
– Severe hypercalcemia in teenager
– Multiple parathyroid adenomas; 10% parathyroid carcinoma

28
Hypocalcemia/Hypoparathyroidism
• Neuro: Paresthesias, fasciculations, muscle spasm, tetany, irritability, movement disorder, SEIZURE, psychosis
• Visual: Cataracts, optic neuritis, papilledema
• Pulmonary: Bronchospasm
• CV: Prolonged QT, CHF, Hypotension
• GI: Dysphagia, abdominal pain, biliary colic
• GU: Preterm labor
29
• Acute Hypocalcemia: Parathyroidectomy
– PTH undetectable at 8 hours
– Normalizes by 30 hours
– Calcium nadir at 20 hours, normal Day 2-3
– Hungry bone syndrome – Old, Labs
• Medications: I-131, Cimetidine, ETOH, Cisplatin,
Digoxin, Ampho-B
– Hypomagnesemia
Hypocalcemia/Hypoparathyroidism
30
Hereditary Hypoparathyroidism
• DiGeorge’s syndrome and velocardiofacial
syndrome – agenesis
• Pseudohypoparathyroidism – peripheral
resistance to PTH
– Short stature, round facies, obesity, mild
MR, dental abscesses, short digits, thickened
calvaria, ectopic calcification
31
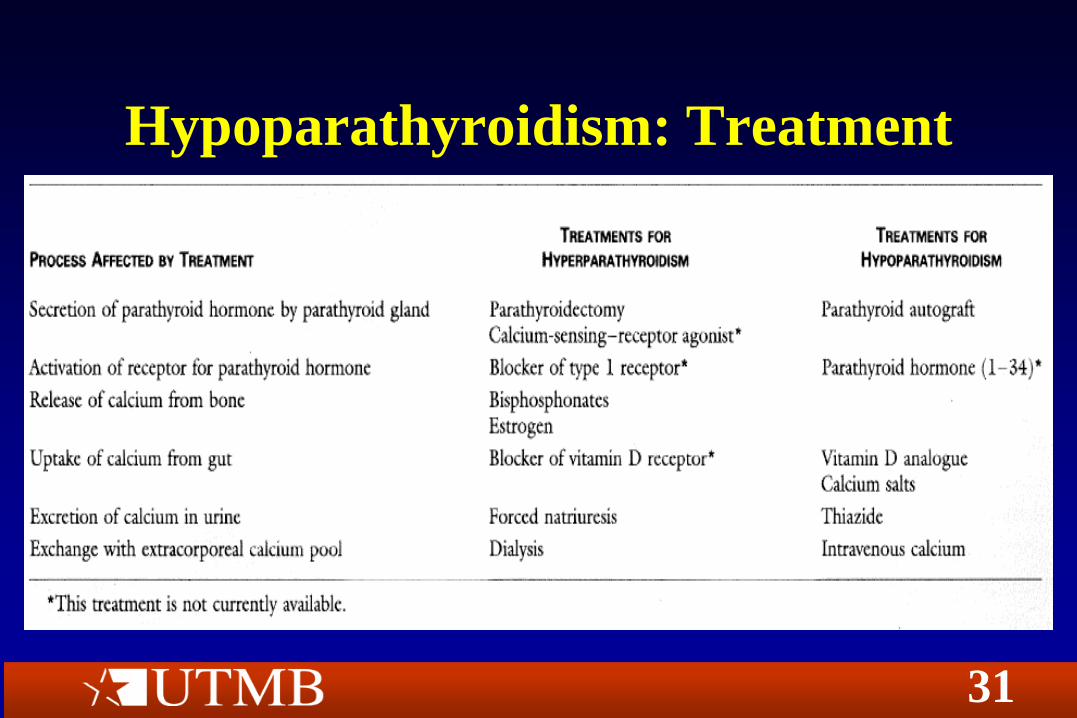
Hypoparathyroidism: Treatment
32
Hypoparathyroidism: Treatment
• Acute severe hypocalcemia
– Check ionized Ca
– 100-300 mg (10-30 ml) 10% Ca-gluconate in 150 cc
D5W over 10 minutes
– Continuous infusion at 0.5 mg/kg/hr
– EKG monitoring
– Check Magnesium
– Check Phosphorous

33
Conclusion: Impress the
Endocrinologist • How big is your Chvostek’s? Grade 1-4
• You say Chvostek’s, I say Weiss
• Su-Su-Sudio:
Pseudopseudohypoparathyroidism
• Clean-up: McLean Hastings Nomogram
(Zaloga 1985)