confidential: for review only · lucena:- descrever as alterações presentes - relatar a...
TRANSCRIPT
Confidential: For Review O
nly
Follow-up head CT scans on a series of 37 children with
congenital Zika syndrome
Journal: BMJ
Manuscript ID BMJ.2017.038478.R2
Article Type: Research
BMJ Journal: BMJ
Date Submitted by the Author: 13-Jul-2017
Complete List of Authors: Petribu, Natacha; Hospital Barão de Lucena, de Fatima Vasco Aragao, Maria; Centro Diagnostico Multimagem, van der Linden, Vanessa ; Association for Assistance of Disabled Children (AACD), Jungmann, Patricia; Universidade de Pernambuco Araújo, Luziany; Hospital Barão de Lucena Abath, Marília; Hospital Barão de Lucena Fernandes, Andrezza; Hospital Barão de Lucena Brainer-Lima, Alessandra; PROCAPE- University of Pernambuco Holanda, Arthur ; Federal University of Pernambuco (UFPE) Mello, Roberto; Federal University of Pernambuco (UFPE), Patology Sarteschi, Camila ; INSTITUTO AGGEU MAGALHAES / FIOCRUZ - RECIFE, PE - BRASIL., Parizel, Paul; Universitair Ziekenhuis Antwerpen
Keywords: Zika Virus, congenital, tomography, brain, calcification, apoptosis
https://mc.manuscriptcentral.com/bmj
BMJ

Confidential: For Review O
nlyHOSPITAL OTÁVIO DE
FREITAS/ SES
PARECER CONSUBSTANCIADO DO CEP
Pesquisador:
Título da Pesquisa:
Instituição Proponente:
Versão:
CAAE:
Achados tomográficos em pacientes recém-nascidos com microcefalia em surtoepidêmico do estado de Pernambuco no ano de 2015.
Natacha Calheiros de Lima Petribu
SECRETARIA DE SAUDE
1
51275815.3.0000.5200
Área Temática:
DADOS DO PROJETO DE PESQUISA
Número do Parecer: 1.337.074
DADOS DO PARECER
Achados tomográficos em pacientes recém-nascidos com microcefalia em surto epidêmico do estado de
Pernambuco no ano de 2015.
Apresentação do Projeto:
Em pacientes recém-nascidos com microcefalia que realizaram tomografia do crânio no Hospital Barão de
Lucena:- Descrever as alterações presentes - Relatar a frequência dos achados -Caracterizar alguma
achado comum ou específico.
Objetivo da Pesquisa:
Mínimo.
Avaliação dos Riscos e Benefícios:
Conhecimento das alterações presentes na tomografia de crânio dos recém-nascidos com microcefalia em
surto atual no Estado de Pernambuco em que a causa ainda é desconhecida.
Comentários e Considerações sobre a Pesquisa:
Encontram-se dentro dos critérios aceitos por este comitê.
Considerações sobre os Termos de apresentação obrigatória:
Financiamento PróprioPatrocinador Principal:
50.920-640
(81)3182-8578 E-mail: [email protected]
Endereço:Bairro: CEP:
Telefone:
Rua Aprígio Guimarães S/NTejipió
UF: Município:PE RECIFEFax: (81)3182-8632
Página 01 de 02
Page 1 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nlyHOSPITAL OTÁVIO DE
FREITAS/ SES
Continuação do Parecer: 1.337.074
Que a pesquisa em tela seja desenvolvida de acordo com o que prediz a mesma.
Recomendações:
Aprovado.
Conclusões ou Pendências e Lista de Inadequações:
Considerações Finais a critério do CEP:
RECIFE, 25 de Novembro de 2015
José Alexandre de Andrade Ferreira(Coordenador)
Assinado por:
Este parecer foi elaborado baseado nos documentos abaixo relacionados:
Tipo Documento Arquivo Postagem Autor Situação
Informações Básicasdo Projeto
PB_INFORMAÇÕES_BÁSICAS_DO_PROJETO_625633.pdf
23/11/201522:20:32
Aceito
Recurso Anexadopelo Pesquisador
TCLE.jpeg 23/11/201522:19:22
Natacha Calheiros deLima Petribu
Aceito
Declaração dePesquisadores
CONFIDENCIALIDADE.jpeg 23/11/201522:18:16
Natacha Calheiros deLima Petribu
Aceito
Projeto Detalhado /BrochuraInvestigador
microcefaliatexto.docx 23/11/201521:49:20
Natacha Calheiros deLima Petribu
Aceito
Outros ANUENCIA.pdf 23/11/201521:46:27
Natacha Calheiros deLima Petribu
Aceito
Folha de Rosto folharosto.pdf 23/11/201521:37:16
Natacha Calheiros deLima Petribu
Aceito
Situação do Parecer:Aprovado
Necessita Apreciação da CONEP:Não
50.920-640
(81)3182-8578 E-mail: [email protected]
Endereço:Bairro: CEP:
Telefone:
Rua Aprígio Guimarães S/NTejipió
UF: Município:PE RECIFEFax: (81)3182-8632
Página 02 de 02
Page 2 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
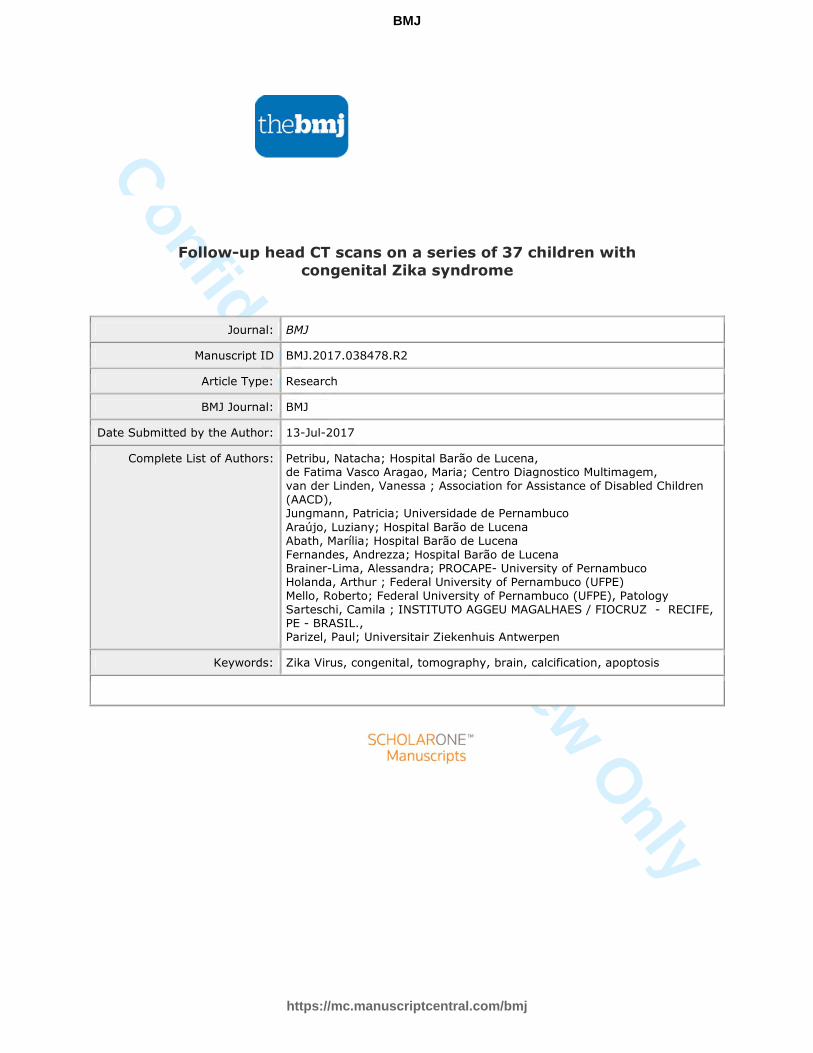
Figure 1. Head CT scans from patients with CZS showing brain calcifications pattern: (A) punctate, (B) coarse and punctate.
89x50mm (150 x 150 DPI)
Page 3 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
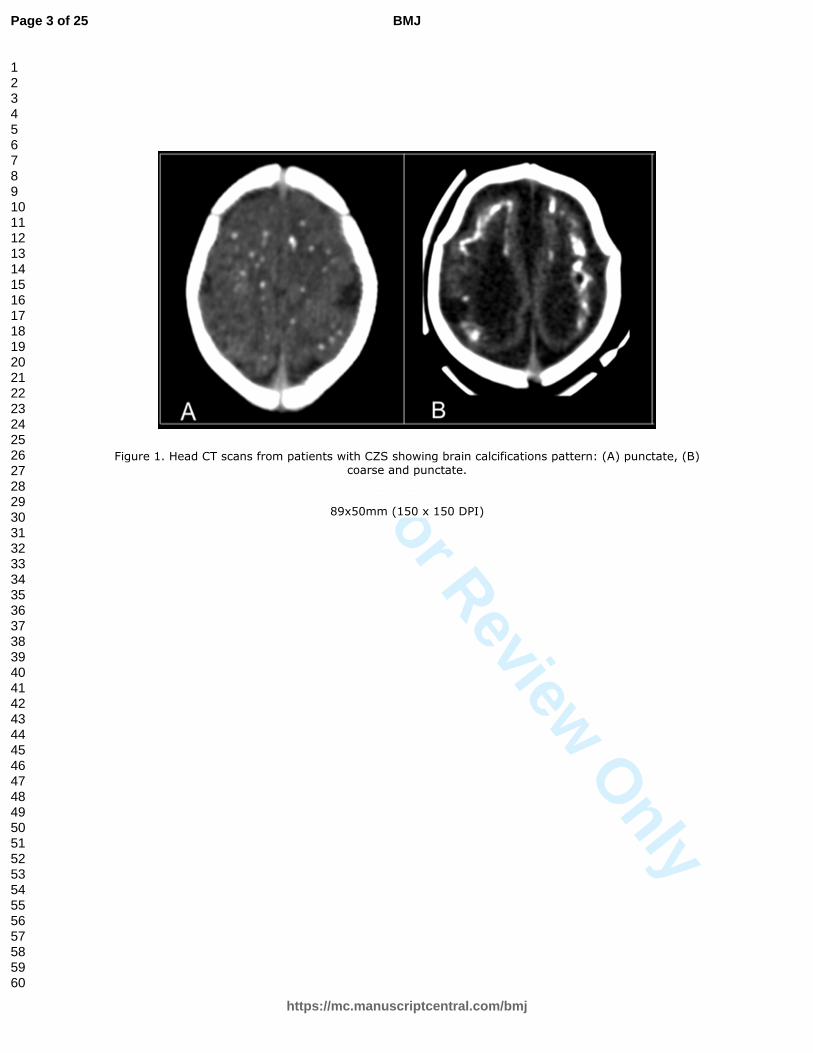
Figure 2. Representative images of head CT scans from six patients (named A, B, C, D, E, F) with CZS who show diminished number, size and/or density intracranial calcifications on follow-up CT scans (bottom line,
named 2) compared with initial CT scans (top line, named 1). Patient A presented punctate cortico-
subcortical junction calcifications in frontal and parietal lobes on initial CT scan (A1) that diminished on follow-up CT scan (A2). Patient B presented punctate cortico-subcortical junction calcifications,
predominating in temporal lobes, and coarse calcifications in basal ganglia and thalamus on initial CT scan (B1) that diminished on follow-up CT scan (B2). Patient C presented on initial CT scan (C1) punctate and
coarse calcifications in cortico-subcortical junction in frontal and parietal lobes, in basal ganglia and thalamus, mostly diminished on follow-up CT scan (C2), remaining only few and tenues punctate
calcifications in basal ganglia and thalamus. Patient D presented punctate and coarse cortico-subcortical junction calcifications in frontal lobes on initial CT scan (D1) that diminished on follow-up CT scan (D2).
Patient E presented on initial CT scan (E1) punctate and coarse calcifications in cortico-subcortical junction in frontal and temporal lobes, in basal ganglia and thalamus that diminished on follow-up CT scan (E2).
Patient F presented on initial CT scan (F1) punctate and coarse calcifications in cortico-subcortical junction in
frontal and temporal lobes, in basal ganglia and thalamus that diminished on follow-up CT scan (F2).
428x170mm (144 x 144 DPI)
Page 4 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
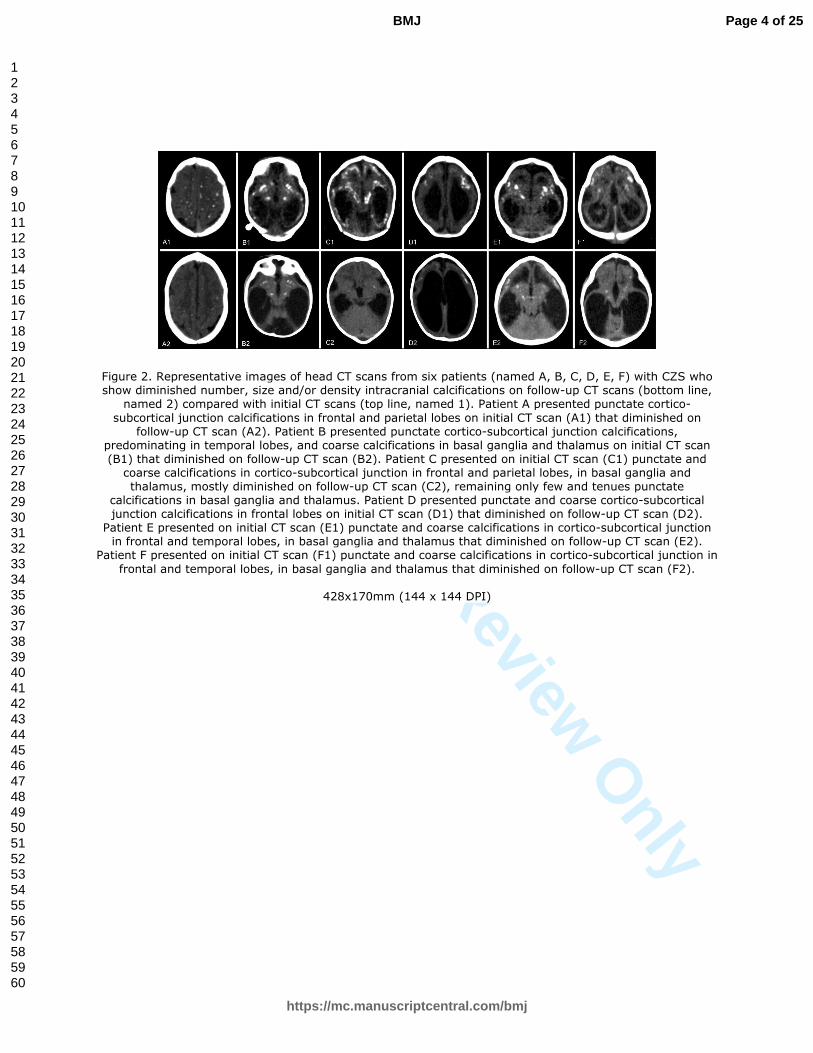
Figure 3. Head CT scans from the only patient with CZS which brain calcifications vanished. Initial CT scan (A) shows tenuous punctate calcifications in cortical-subcortical junction on frontal lobes (arrows). On
follow-up CT scan (B) calcifications vanished.
219x92mm (150 x 150 DPI)
Page 5 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
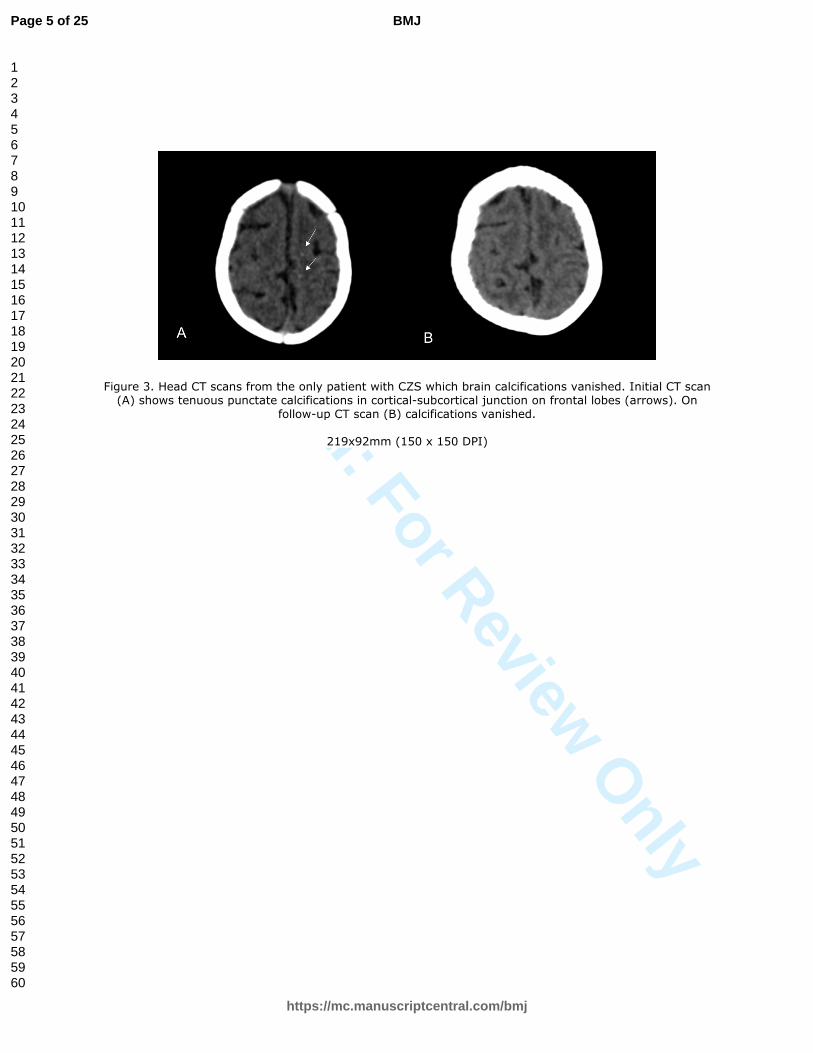
Figure 4. Head CT scans from one patient with CZS. Initial CT scan (A) shows punctate calcifications in cortical-subcortical junction on occipital lobe (arrow). On follow-up CT scan (B) calcifications remains
unchanged.
231x131mm (150 x 150 DPI)
Page 6 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
Figure 5: Brain section of Zika microcephalic fetus: parenchymal (white matter) microcalcifications placed over a non-inflammatory background. In the inset and arrow: non-inflamed blood vessel adjacent to
microcalcifications. HE 50X and inset 100X.[26]
19x9mm (300 x 300 DPI)
Page 7 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
1
Follow-up head CT scans on a series of 37 children with congenital Zika syndrome
Abstract
OBJECTIVE
To compare the initial and follow-up head CT scans in children with congenital Zika
syndrome (CZS), focusing on the evaluation of cerebral calcifications.
DESIGN
Case series study.
SETTING
Barão de Lucena Hospital, Pernambuco (Brazil).
PARTICIPANTS
Thirty-seven children with probable or confirmed CZS, who underwent 2 head CT
scans: the first one shortly after birth (during the microcephaly outbreak), and the
second after about one-year follow-up.
INTERVENTIONS
Comparison of neuroimaging findings between the head CT scans performed shortly
after birth and around one year later, in infants with probable or confirmed CZS.
MAIN OUTCOME MEASURES
Differences regarding cerebral calcification patterns between the initial head CT scan
and the follow-up CT scan after around one year.
RESULTS
Thirty-seven children presenting CZS were evaluated by head CT scan. All patients
presented cerebral calcifications on the initial CT, predominantly located at the cortical-
subcortical junction. The intracranial calcifications diminished in number, size and/or
density on follow-up CT in 34 patients (91.9% - IC95%: 78.7-97.2), vanished in 1 and
remained unchanged in 2 children. No patient had an increase of calcifications. There
Page 8 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
2
was a statistically significant vanished of cortical- subcortical white matter junction
calcifications of the parietal (p = 0,002) and occipital (p= 0,002) lobes.
CONCLUSION
In this series of children with CZS, brain calcifications had diminished in number, size
and/or density on follow-up head CT scans. No patient had an increase of calcifications.
The vanished of cortico-subcortical junction calcifications predominated significantly in
the parietal and occipital lobes. One must be aware that in view of the present data the
detection of encephalic calcification should not be considered a major criterion for late
diagnosis of CZS, nor should its absence be used for excluding it.
Page 9 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
3
Contributors: All authors contributed to the clinical, radiological and pathological
assessment, according to their own specialty, and to the concept and design or analysis
and interpretation of the data and to the draft of final version.
Funding: The study received no external funding.
In our population of children with CZS, calcifications diminished in number, size or
density in most patients on follow-up head CT scans. The diminished of cortico-
subcortical junction calcifications predominated in the parietal and occipital lobes. We
discuss possible theories to explain these findings in light of histopathological findings.
One must be aware that the presence of encephalic calcification should not be
considered a major criterion for late diagnosis of CZS, nor should its absence be used
for excluding it.
What is already known on this topic
Cerebral calcifications at the cortico-subcortical junction are the most remarkable
imaging sign of CZS. However, there are no follow-up studies regarding the
evolution of the calcifications in children with CZS.
What this study adds
• Our study compares head CT scans of children with probable or confirmed
CZS performed shortly after birth with one-year follow-up CT scans.
• The most frequent findings are the partial or complete diminished of cerebral
calcifications. No patient had an increase of number, size and density of
calcifications.
• The presence of cerebral calcifications should not be considered a major
criterion for late diagnosis of CZS (nor should its absence be used for
excluding the diagnosis).
Page 10 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
4
INTRODUCTION
Just over a year ago, an unprecedented outbreak of congenital microcephaly occurred
in Brazil, associated with the Zika virus infection. Since then, significant knowledge has
been gained about the epidemiology and physiopathology of this terrible
disease.[1][2][3][4] The global risk assessment has not changed. Zika virus continues to
spread geographically to areas where competent vectors are present. Although a decline
in number of cases of Zika infection has been reported in some countries, vigilance
needs to remain high.[5] Nowadays, we are faced with a population of children with
congenital Zika virus syndrome (CZS), who present with a broad spectrum of clinical
and radiological presentations, and whose natural histories are still being written.[6][7]
The main findings on head computed tomography (CT) scans of the newborns with
CZS have been widely reported and include: brain calcifications (mainly occurring at
the cortico-subcortical junction), decreased cerebral volume with malformation of
cortical development, ventriculomegaly (mostly colpocephaly; defined as
disproportionate enlargement of the occipital horns of the lateral ventricles), cerebellar
hypoplasia and prominent occipital protuberance.[8][9][10]
In our experience, several children followed-up with CZS are developing
hydrocephalus, even without clinical symptoms, and around 10% had indication for
neurosurgery (ventriculoperitoneal shunt). The pathophysiology of hydrocephalus in
CZS is still unknown. Due to the risk of developing hydrocephalus, many patients did
follow-up CT scans and nowadays, there is a recommendation that at least one brain
imaging control could be done between 10 to 12 months of age.[11] Up to now, there
are no published follow-up studies describing the evolution of the neuroimaging
abnormalities in these infants, so the aim of our investigation was to compare the initial
Page 11 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
5
with the follow-up head CT scans, focusing on the assessment of cerebral calcifications,
in the first 37 children with CZS referred to perform the control brain image.
METHODS
This is a case series study, involving thirty-seven children, convenience sampling, with
probable or confirmed CZS, according to the definition of the Ministry of Health of
Brazil [12]. All subjects underwent a follow-up unenhanced head CT in Recife, from
August 2015 to January 2017.
The brain image reevaluation was indicated when there was clinical suspicion of
hydrocephalus and due to nonspecific symptoms. The most frequent symptoms that
motivated the request of a follow-up CT were: seizures (26 patients/ 70,2%), being
difficult to control in 11 patients (29,7%); irritability (10 patients/ 27%); vomiting (8
patients/ 21,6%); worsening of dysphagia (5 patients/ 13,5%); previous MRI suggestive
of hydrocephalus (4 patients/ 10,8%); HC increase (3 patients/ 8,1%); drowsiness (2
patients/ 5,4%); worsening of hypertonia (1 patient/ 2,7%) and recurrent respiratory
tract infection (1 patient/ 2,7%). These symptoms could be associated. The most
common association, present in 9 patients (24,3%), were the triad: vomiting, irritability
and seizures difficult to control. Despite the harmful effects of ionizing radiation, CT
scan was the exam of choice for investigation these children around 1 year of age
because cranial fontanelles were closed, what precludes the use of transfontanelle
ultrasonography. Magnetic resonance imaging was not choose due to a longer time to
perform the exam, prolonger sedation time and also higher cost.
In the beginning of outbreak in Brazil, the ministry of healthy defined microcephaly as a
head circumference < = 33 cm, a cutoff that decreased 2 times before the establishment
of the current criteria based on the Intergrowth-21st that consider microcephaly when
Page 12 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
6
head circumference (HC) is below 2 standard deviations and severe microcephaly when
is below 3 standard deviations.[13]
All follow-up unenhanced head CT scans were formally requested by the assistant
neuropediatrician. The person responsible for each child signed an informed consent
form for the study to be carried out. Most children did not have to be sedated, they just
needed a physical containment with bands. In the few children who were agitated at the
time of the exam, inhalation sedation according to the weight of each patient was
performed by an experienced anesthetist.
The following inclusion criteria were used for selection of patients:
a) Initial head CT scan performed shortly after birth, according to the protocol
established for investigation of microcephaly during the outbreak in Brazil;[12]
b) Initial head CT scan showed findings suggestive of congenital infection including:
cerebral calcifications, ventriculomegaly, malformation of cortical development,
cerebellar or brainstem hypoplasia, and white matter abnormalities;
c) Laboratory findings excluding STORCH (Syphilis, Toxoplasmosis, Rubella,
Cytomegalovirus and Herpes virus) infections in mother and/or baby.
According to the Brazilian Ministry of Health, probable cases have (a) mother’s rash
during pregnancy, (b) brain imaging suggestive of congenital infection, and (c)
laboratory exclusion of STORCH infections in mother and/or baby. Confirmed cases
have, in addition, (d) laboratory confirmation of ZIKV infection in mother and/or baby
[e.g., real-time reverse transcription polymerase chain reaction (RT-PCR), ZIKV-
specific IgM, plate reduction neutralization test (PRNT) for ZIKV in the CSF and/or
serum].[12]
The initial CT scans were performed during the outbreak in different radiology centers
and with different CT equipment (slice detectors varying from 6 to 64 on initial CT
Page 13 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
7
scan), making it impossible to standardize, but these scanners had similar technical
capabilities. All scans done at Barão de Lucena Hospital were in a Philips Brilliance 6
slice CT. We used a nonenhanced low-dose head CT protocol specific for children,
promoting less ionizing radiation exposure. Patients were placed supine, head first into
the gantry, with the head in the head-holder. Table height was defined when external
auditory meatus (EAM) was at the center of the gantry. The gantry was not angled. The
images were acquired from foramen magnum through top of calvarium with 300 mAs,
90 kVp and 3mm of thickness.
All images were retrieved in the form of CD containing DICOM images and were
carefully analyzed and compared by trained physicians in a workstation. The initial and
follow-up CT images from each patient were analyzed side by side in a workstation,
after adjustments of window, slice thickness and planes, to better equalize the images.
Despite this careful evaluation, there were minimal variations in the images shown, but
they did not compromise the perception of calcifications. It were due to the cranial
deformity that some newborns presented on initial CT scan and the movement of some
patients on follow-up CT scan (because we avoided sedation in most patients)
Four physicians (a neuropediatrician with 19 years of experience, one radiologist with
18 years and two radiologists with 3 years of experience) made the image analyse
together in two meetings. The meetings had a difference of two days between them. At
the first meeting 20 patients were analyzed and 17 patients at the second meeting. The
analyzes was made in two steps as following: (1) In the first step, analysing the initial
CT scans, (a) we answered if there were brain calcifications (yes or no). (b) If the
calcifications were present, they were classified according to their shape in punctate,
coarse or both and, also, (c) we localize where they were in the brain (cerebellum,
brainstem, thalamus, basal ganglia, periventricular, cerebral cortex and in cortico-
Page 14 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
8
subcortical white matter junction). (d) Then, we evaluated specifically cerebral lobes
distribution (frontal, parietal, temporal and occipital) of cortical-subcortical junction
calcifications. (2) In the second step, analysing the follow-up CT scans, (a) we analyzed
what happened with the brain calcifications, if they were increased, unchanged,
diminished (meaning reduced in size, number and/or density) or vanished (completely
disappearance of calcifications). (b) We also registered the location of brain
calcifications vanished (on the cerebellum, brainstem, thalamus, basal ganglia,
periventricular, cerebral cortex and in cortico-subcortical white matter junction). (c)
After that, we evaluated in which cerebral lobes occur the vanished of the cortical-
subcortical junction calcifications (frontal, parietal, temporal and occipital).
The authors agreed on most of the answers, but when there was disagreement, it was
consensually chose the best answer. All the consensus answers were stored in
appropriate spreadsheets for statistical analysis. Until now, there is no CT software for
quantification of brain calcification to our knowledge.
For the statistical analysis, the software SPSS 21.0 (Statistical Package for the Social
Sciences) for Windows and Excel 2010 were used. McNemar test for paired data was
applied to study the behavior of results of initial CT scan with the follow-up CT scan.
Fisher's exact test was used to analyze the association of variables. Additional analyses
included a residual analysis, which examines the association between categories of
variables in a contingency table. Results were considered statistically significant when p
< 0.05.
RESULTS
Thirty-seven children with CZS were evaluated by head CT scans, being 22 (59.5%)
male. We have the information about timing maternal infection from 36 patients, of
Page 15 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
9
which 25 mothers (69.4%) reported rash between 2 and 6 months of gestation, being 18
(50.0%) in the first trimester. The gestational age at birth ranged from 31 to 41 weeks (5
preterm). The measures of head circumference at birth ranged from 23 to 33cm. In this
series, 35 patients (94.6%) presented with microcephaly, classified as severe
microcephaly in 26 cases. Two patients (5.4%) had a normal head circumference at
birth but developed postnatal microcephaly. Among the 37 infants, twenty-nine were
confirmed CZS cases and only eight (21.6%) were probable cases. The probable cases
are quite typical of CZS, and are only not confirmed due to having not been submitted
to the laboratory tests in a timely manner for the serological diagnosis. Fifteen children
(40.5% - IC95%: 26.3-56.5) had diagnosis hydrocephalus by follow-up CT scans and
indication for neurosurgery (ventriculoperitoneal shunt).
On initial head CT scans, the age of the patients ranged from 1 to 138 days, with a
median of 11.5 days. On the follow-up head CT scans, their age ranged from 105 to 509
days, with a median of 415 days.
From 37 patients, 28 performed follow-up CT scans at Barão de Lucena Hospital with
the same parameters for all patients. Nine patients were scanned on the same scanner in
initial and follow-up CT scan.
First Step: Initial CT Scans Results
All patients presented brain calcifications. In relation of the shape, all patients showed
punctate calcifications on the initial CT, and 19 (51.3% - IC95%: 35.9-66.6) patients
also presented coarse calcifications (Figure 1).
In respect of location of brain calcifications, the cortical-subcortical junction was the
most frequent (35/37; 94,6% - IC95%: 82.3% - 98.5%) followed by basal ganglia
(26/37; 70.3% - IC95%: 54.2 - 82.5), thalamus (20/37; 54.1% - IC95%: 38.4 - 68.9),
Page 16 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
10
brainstem (5/37; 13.5% - IC95%: 5.9 - 27.9), periventricular area (4/37; 10.8% -
IC95%: 4.3 - 24.7) and cerebellum (3/37; 8.1% - IC95%: 2.8 - 21.3).
Second Step: Around One-Year Follow-up CT Scans Results
On follow-up CT scans, the intracranial calcifications diminished in number, size and/or
density in 34 patients (91.9% - IC95%: 78.7 - 97.2); (Figure 2), vanished in 1 (Figure 3)
and remained unchanged in 2 children (Figure 4). No patient had an increase of number,
size and density of calcifications.
There was vanished of brain calcifications, but without statistical significance, on
cortico-subcortical junction of all lobes of cerebral hemispheres (1 patient; p = 1.000),
thalamus (2 patients; p = 0.499), brainstem (2 patients; p = 0.501) and periventricular
area (3 patients; p = 0.250). There were no vanished calcifications in basal ganglia and
cerebellum, remaining unchanged in these location (p = 1,000).
Considering only cortico-subcortical calcifications, there were diminished in 32/35
children, vanished in 1/35 child and remained unchanged in 2/35 children. Analyzing in
which cerebral lobes occur the vanished of the cortical-subcortical junction
calcifications, we only found statistically significant in parietal (p = 0.004) and occipital
lobes (p = 0.004). Table 1.
Table 1. Distribution of the cortical-subcortical calcifications in the cerebral lobes
on initial and on follow-up CT scans (n = 35).
CT Inicial CT Follow up p
Yes - n (%) No - n (%) McNemar test
Frontal Yes 32 (94.1) 2 (5.9) 0.999 No 1 (100) 0 (0) Parietal Yes 19 (67.9) 9 (32.1) 0.004*
No 0 (0.0) 7 (100) Temporal Yes 20 (95.2) 1 (4.8) 0.999 No 1 (7.1) 13 (92.9) Occipital
Page 17 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
11
Yes 12 (57.1) 9 (42.9%) 0.004*
No 0 (0) 14 (100) (*) p < 0,05
DISCUSSION
All patients presented brain calcifications on the initial head CT scans; this represents
the most striking tomographic finding in patients with CZS. The cortical-subcortical
junction was the most prevalent location, followed by the basal ganglia, thalamus,
brainstem and cerebellum; these results are in agreement with the existing
literature.[8][9][10]
Surprisingly, on follow-up head CT scans, these intracranial calcifications diminished in
number, size and/or density or vanished in the most of patients. Only in 2 patients, the
calcifications remain unchanged. No patient had an increase of calcifications. The only
patient in whom the calcifications vanished had few and tenues punctate calcifications
on cortical-subcortical junction of frontal lobe, which may have contributed to their
complete disappearance on follow-up CT scan.
The reduction of calcifications does not mean clinical improvement, once these children
were investigated due to clinical worsening, even they did not have hydrocephalus on
follow-up CT scans. The clinical picture was varied, most of them with severe
neurological impairment, with a high incidence of epilepsy and feeding problems. In
addition, we believe that even children who are not yet clinically worsened may also
have reduced cerebral calcifications.
The comprehensive autopsy reports of microcephalic Zika fetuses from Slovenia and
from Washington [2][14] describe disorders of neuronal differentiation, astroglia
reactivity and parenchymal microcalcifications. These authors did not point out any
significant inflammatory reactions in the CNS. The microcalcifications found in these
cases had been described over cell remnants.
Page 18 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
12
A great body of experimental evidence, in vitro, with human neuroprogenitor cells
[15][16] and in vivo, using mice [17] and primate models [18][19], strongly suggests
that the main pathologic mechanism involved in the loss of neural cells in CZS is the
pathologically induced apoptosis of neuroprogenitor cells.[20] Early clinical
observations correlated with gestational and post-natal brain images and CSF analysis
pointed towards a primary teratogenic mechanism not related to a necrotic or
inflammatory lesions in the CNS.[21] In the CZS, the current inflammation-free autopsy
and clinical data point that there is a microglial phagocytic response rather than the
exudative pathway that evolves with the breakdown of the blood brain barrier (BBB)
and the recruitment of peripheral inflammatory cells.[22] Because of these findings, the
pathophysiology of microglia phagocytic response should be elucidated[23], specially
in CZS.
The process of calcium deposition over apoptotic organic matrix is already described in
the literature.[24][25]. Radiologically, the punctate calcifications identified on CT scans
could correspond microscopically to tiny and loose calcium deposits, so far observed,
and the coarse calcifications to bigger aggregates. (Figure 5).[26]
So, taking into account the data on CT scans reported in here, we hypothesized that the
progressive clearance are probably due to an enhanced microglial activity,
disaggregating mineralized microgranules by active phagocytosis and moving them
towards a final destination into the recently described lymphatic system of the CNS
[27][28].
As for the distribution of cortico-subcortical junction calcifications there were a
statistically significant diminution of calcification in the parietal and occipital lobes.
These could be related to brain development, in a similar fashion as what happens with
the myelination process (i.e., from posterior to anterior).[29]
Page 19 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
13
In this study, 40.5% of children evolved with hydrocephalus and neurosurgery
(ventriculoperitoneal shunt). The pathophysiology of hydrocephalus in CZS is still
unknown. However, we hypothesize that may exist an important damage to the cerebral
vascular system, especially in the venous component, leading to cerebral venous
thrombosis and cerebral venous hypertension during intrauterus development and
continuing after birth, as was reported by Aragao et al.[7][30] and Soares de Oliveira-
Szejnfeld[10]. This could explain the development of hydrocephalus in some of the
infants, and also, the presence and the changes of brain calcifications. As the use of
contrast is usually not recommended in infants, no venous contrast was administered at
any initial or follow-up CT scans. Because of this, the frequency of cerebral venous
thrombosis is still unknown in CZS. Future studies with brain Magnetic Resonance
Imaging and brain Magnetic Resonance Venography (unenhanced) may bring additional
information regarding the association of thrombosis with CZS.
Knowing that brain calcifications have diminished over time in most patients of our
study, although being the most expressive image finding in the initial CT scans, we can
no longer consider them as a major criterion when late diagnosis of CZS being under
investigation. The findings described here could explain, in part, how difficult to make
the suspicion and the diagnosis of CZS could be in cases without microcephaly in initial
presentation. [6][30]
A limitation of our study was the subjective way of quantifying cerebral calcifications,
since there is no specific software for this purpose to our knowledge. However, we tried
to minimize subjective bias effects by reading the images jointly in a consensus
analysis.
Finally, this is the first series of infants with CZS where follow-up imaging findings are
described. As we said at the beginning, the CZS natural history is still being written.
Page 20 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
14
Our number of cases under continuous study increases every day, supporting the
validity of these findings. We believe that this study can contribute with new knowledge
about the physiopathology of CZS and add radiological details on the evolution of this
disease in time-line.
CONCLUSION
In this series of children with CZS, brain calcifications had diminished in number, size
and/or density on follow-up head CT scans. No patient had an increase of calcifications.
The vanished of cortico-subcortical junction calcifications predominated significantly in
the parietal and occipital lobes. One must be aware that in view of the present data the
detection of encephalic calcification should not be considered a major criterion for late
diagnosis of CZS, nor should its absence be used for excluding it.
Page 21 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
15
Contributors: All authors contributed to the clinical, radiological and pathological assessment, according to their own specialty, and to the concept and design or analysis and interpretation of the data and to the draft of final version.
Funding: The study received no external funding.
Competing interests: All authors have completed the ICMJE uniform disclosure form at
www.icmje.org/coi_disclosure.pdf and declare: no support from any organization for the
submitted work; no financial relationships with any organizations that might have an interest in
the submitted work in the previous three years; no other relationships or activities that could
appear to have influenced the submitted work.
Ethical approval: This study was approved by the Research Ethical Committee and the
children’s mothers or guardians gave their consent for the publication of the results and images.
Data sharing: Additional information is available from the corresponding author
[email protected] by request.
Transparency: The lead author affirms that the manuscript is an honest, accurate, and
transparent account of the study being reported; that no important aspects of the study have been
omitted; and that any discrepancies from the study as planned have been explained.
This is an open access article distributed in accordance with the Creative Commons Attribution
Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt,
build upon this work non-commercially, and license their derivative works on different terms,
provided the original work is properly cited and the use is non-commercial. See:
http://creativecommons.org/licenses/by-nc/4.0.
Page 22 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
16
BIBLIOGRAPHY
1. Oliveira Melo AS, Malinger G, Ximenes R, Szejnfeld PO, Alves Sampaio S, Bispo de
Filippis AM (2016) Zika virus intrauterine infection causes fetal brain abnormality and
microcephaly: tip of the iceberg? Ultrasound Obstet Gynecol 47:6–7
2. Summ, Mlakar J, Korva M, Tul N, Popović M, Poljšak-Prijatelj M, Mraz J et al. (2016)
Brief Report. New 10:22. Mlakar J, Korva M, Tul N, Popović M, Poljšak-P
3. Martines RB, Bhatnagar J, Keating MK, et al (2016) Notes from the Field : Evidence of
Zika Virus Infection in Brain and Placental Tissues from Two Congenitally Infected
Newborns and Two Fetal Losses — Brazil, 2015. MMWR Morb Mortal Wkly Rep
65:1–2
4. Calvet G, Aguiar RS, Melo ASO, et al (2016) Detection and sequencing of Zika virus
from amniotic fluid of fetuses with microcephaly in Brazil: a case study. Lancet Infect
Dis 16:653–660
5. WHO. Situation report. Zika virus.
http://apps.who.int/iris/bitstream/10665/254507/1/zikasitrep2Feb17-eng.pdf.
6. van der Linden V, Pessoa A, Dobyns W, et al (2016) Description of 13 Infants Born
During October 2015–January 2016 With Congenital Zika Virus Infection Without
Microcephaly at Birth — Brazil. MMWR Morb Mortal Wkly Rep 65:1343–1348
7. Aragao MFVV, Holanda AC, Brainer-Lima AM, et al (2017) Nonmicrocephalic Infants
with Congenital Zika Syndrome Suspected Only after Neuroimaging Evaluation
Compared with Those with Microcephaly at Birth and Postnatally: How Large Is the
Zika Virus “Iceberg”? Am J Neuroradiol. doi: 10.3174/ajnr.A5216
8. Hazin AN, Poretti A, Di Cavalcanti Souza Cruz D, et al (2016) Computed Tomographic
Findings in Microcephaly Associated with Zika Vires. N Engl J Med 374:2193–2195
9. de Fatima Vasco Aragao M, van der Linden V, Brainer-Lima AM, Coeli RR, Rocha
MA, Sobral da Silva P, Durce Costa Gomes de Carvalho M, van der Linden A, Cesario
de Holanda A, Valenca MM (2016) Clinical features and neuroimaging (CT and MRI)
findings in presumed Zika virus related congenital infection and microcephaly:
Page 23 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960

Confidential: For Review O
nly
17
retrospective case series study. Bmj 353:i1901
10. Soares de Oliveira-Szejnfeld P, Levine D, Melo AS de O, et al (2016) Congenital Brain
Abnormalities and Zika Virus: What the Radiologist Can Expect to See Prenatally and
Postnatally. Radiology 281:203–218
11. van der Linden V, Filho ELR, van der Linden A (2017) Congenital Zika Syndrome:
Clinical Aspects. In: Maria de Fátima Viana Vasco Aragão (ed) Zika Focus, First.
Springer International Publishing, Cham, pp 33–45
12. Microcefalia D, Ou E/ (2016) PROTOCOLO DE VIGILÂNCIA E RESPOSTA À
OCORRÊNCIA. http://combateaedes.saude.gov.br/images/sala-de-si
13. Villar J, Ismail LC, Victora CG, et al (2014) International standards for newborn weight,
length, and head circumference by gestational age and sex: the Newborn Cross-Sectional
Study of the INTERGROWTH-21st Project. Lancet 384:857–868
14. Driggers RW, Ho C-Y, Korhonen EM, et al (2016) Zika Virus Infection with Prolonged
Maternal Viremia and Fetal Brain Abnormalities. N Engl J Med 374:2142–2151
15. Tang H, Hammack C, Ogden SC, et al (2016) Zika Virus Infects Human Cortical Neural
Progenitors and Attenuates Their Growth Cell Stem Cell Zika Virus Infects Human
Cortical Neural Progenitors and Attenuates Their Growth. Cell Stem Cell 18:587–590
16. Garcez PP, Loiola EC, Madeiro da Costa R, Higa LM, Trindade P, Delvecchio R,
Nascimento JM, Brindeiro R, Tanuri A, Rehen SK (2016) Zika virus impairs growth in
human neurospheres and brain organoids. Science (80- ) 352:816–818
17. Cugola FR, Fernandes IR, Russo FB, et al (2016) The Brazilian Zika virus strain causes
birth defects in experimental models. Nature. doi: 10.1038/nature18296
18. Adams Waldorf KM, Stencel-Baerenwald JE, Kapur RP, et al (2016) Fetal brain lesions
after subcutaneous inoculation of Zika virus in a pregnant nonhuman primate. Nat Med
22:1256–1259
19. Dudley DM, Aliota MT, Mohr EL, et al (2016) A rhesus macaque model of Asian-
lineage Zika virus infection. Nat Commun 7:12204
20. Russo FB, Jungmann P, Beltrão-Braga PCB (2017) Zika infection and the development
Page 24 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Confidential: For Review O
nly
18
of neurological defects. Cell Microbiol e12744
21. jungmann P, pires P, Araujo júnior E (2017) Early insights into Zika’s microcephaly
physiopathology, from the epicentre of the outbreak: teratogenic apoptosis on the central
nervous system. Acta Obstet Gynecol Scand. doi: 10.1111/aogs.13184
22. Nickerson JP, Richner B, Santy K, Lequin MH, Poretti A, Filippi CG, Huisman TAGM
(2012) Neuroimaging of Pediatric Intracranial Infection-Part 2: TORCH, Viral, Fungal,
and Parasitic Infections. J Neuroimaging 22:e52–e63
23. Marín-Teva JL, Cuadros MA, Martín-Oliva D, Navascués J (2011) Microglia and
neuronal cell death. Neuron Glia Biol 7:25–40
24. Kim KM (1995) Apoptosis and calcification. Scanning Microsc 9:1137-75–8
25. Fujita H, Yamamoto M, Ogino T, Kobuchi H, Ohmoto N, Aoyama E, Oka T, Nakanishi
T, Inoue K, Sasaki J (2014) Necrotic and apoptotic cells serve as nuclei for calcification
on osteoblastic differentiation of human mesenchymal stem cells in vitro. Cell Biochem
Funct 32:77–86
26. Holanda AC MR (2017) Histopathological Findings of Congenital Zika Syndrome. In:
Aragao MFVV (ed) Zika Focus., First. Springer, pp 139–150
27. Louveau A, Smirnov I, Keyes TJ, et al (2015) Structural and functional features of
central nervous system lymphatic vessels. Nature 523:337–341
28. Iliff JJ, Wang M, Liao Y, et al (2012) A paravascular pathway facilitates CSF flow
through the brain parenchyma and the clearance of interstitial solutes, including amyloid
β. Sci Transl Med 4:147ra111
29. Barkovich AJ,Moore KR JB (2007) Diagnostic imaging: pediatric neuroradiology.
AMIRSYS, Salt Lake City, Utah
30. Aragao MFVV, Brainer-Lima AM, Holanda AC de LPN, Holanda AC MR (2017)
Neuroimaging Findings of Congenital Zika Syndrome. In: Aragao MFVV (ed) Zika
Focus. Springer, pp 63–92
Page 25 of 25
https://mc.manuscriptcentral.com/bmj
BMJ
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960