conjoint smoking and drinking: a case for dual-substance intervention among young emergency...
TRANSCRIPT
1126 SMOKING & DRINKING Horn et al. • CONJOINT SMOKING AND DRINKING
Conjoint Smoking and Drinking: A Case forDual-substance Intervention among Young
Emergency Department Patients
KIMBERLY HORN, EDD, XIN GAO, MS, JANET WILLIAMS, MD,JIM HELMKAMP, PHD, MIKE FURBEE, MA, WILLIAM MANLEY, RN
Abstract. Objectives: To better understand con-joint smoking and drinking among young adult emer-gency department (ED) patients, the purposes of thisinvestigation were: 1) to assess the prevalence of con-joint use; 2) to determine the factors associated withconjoint alcohol use and smoking; and 3) to addressthe implications for future ED-based investigation ofdual-substance intervention. Methods: Data for thisinvestigation were obtained from a battery of ques-tionnaires administered to the routine-care patientsduring an alcohol screening in the ED, which waspart of a larger alcohol intervention study. Results:
Study findings revealed that a majority of patientswith self-reported alcohol-related problems weresmokers. In fact, drinkers who smoked were likely to
be pack-a-day smokers. Among the study sample, be-ing female, having low education levels (e.g., highschool education or less), having some emotionalproblems, and currently using marijuana were riskfactors for conjoint smoking and drinking. Conclu-
sions: Conjoint users were identifiable through briefscreening. Given the prevalence of conjoint smokingand alcohol use among the ED sample and a specificset of risk factors, tailored intervention for alcoholand nicotine dependence may be an important andopportunistic clinical ED service. Key words: alcoholuse; smoking; substance abuse; intervention; emer-gency medicine. ACADEMIC EMERGENCY MEDI-CINE 2000; 7:1126–1134
BOTH smoking and alcohol use are stronglyassociated with increased morbidity and
mortality.1,2 In fact, more than 25% of long-timesmokers die directly as a result of smoking, andthose who die prematurely will lose, on average,20 years of life.3 Studies have found that the syn-ergistic health risks associated with smoking anddrinking are estimated to be 50% higher than thesum of their independent risks.4 Frequently, pa-tients recover from alcohol dependence only to dieprematurely from tobacco-related illnesses.5,6
More specifically, alcohol consumption com-bined with cigarette smoking increases the metab-olism and activation of tobacco chemical carcino-gens in users, leading to an increased risk ofcancer.7,8 Cancers most often found among individ-uals who are dependent on both cigarettes and al-cohol are in the upper digestive tract, such as themouth, pharynx, esophagus, and larynx.1,7,9 Con-
From West Virginia University, Robert C. Byrd Health Sci-ences Center, School of Medicine, Morgantown, WV (KH, XG,JW, JH, MF, WM).Received January 31, 2000; revision received June 5, 2000; ac-cepted June 14, 2000.Address for correspondence and reprints: Dr. Kimberly Horn,West Virginia University, Robert C. Byrd Health Sciences Cen-ter, Department of Community Medicine, Office of Drug AbuseIntervention Studies, P.O. Box 9190, Morgantown, WV 26506.Fax: 304-293-8624; e-mail: [email protected]
joint drinkers and smokers are also at greater riskthan the general population for cardiovascular dis-ease,1 hypertension, gastrointestinal bleeding, sud-den death, and spontaneous abortions.7 Also, pan-creatitis appears tenfold among alcohol-dependentsmokers and cirrhosis is three times more likely.6
Individuals who are the heaviest smokers alsoare the heaviest drinkers, and vice versa.3,6,10–12
The relative risk of alcohol dependence amongsmokers is estimated to be ten times that of non-smokers. Moreover, individuals with alcohol-re-lated problems may represent at least one fourthof all smokers.13 This relationship is so strong thatheavy smoking is considered a strong predictor ofunrecognized alcoholism.14 According to Bobo andcolleagues,11 regular smoking precedes the devel-opment of alcohol dependence by many years.
The physiologically addicting natures of bothnicotine and alcohol,15–17 coupled with psychologi-cal and behavioral conditioning processes,18,19
make smoking and drinking negative health be-haviors that are extremely resistant to change.While some efforts have been made to address nic-otine addiction in alcohol intervention,5,6 standardalcohol intervention rarely addresses smoking, andvice versa. In fact, alcohol-dependent individualsoften are warned to avoid the stress of quittingsmoking while trying to abstain from or reduce al-cohol use.1 Common rationales are that 1) abstain-

ACADEMIC EMERGENCY MEDICINE • October 2000, Volume 7, Number 10 1127
ing from smoking while receiving alcohol interven-tion adversely affects alcohol abstinence6; 2) nico-tine is a drug that alcohol-dependent individualscan use safely3; 3) cigarette smoking is the lesserof two evils20,21; and 4) alcohol-dependent individ-uals are neither interested in abstaining nor mo-tivated to abstain from smoking.20
However, studies show that conjoint users areinterested in quitting smoking20 and that smokingintervention in conjunction with alcohol interven-tion may have a positive effect on alcohol absti-nence.21 For example, Irving and colleagues20 foundthat 77.4% of alcohol-dependent inpatients wantedto abstain from smoking. Burling and colleaguesfound that alcoholic-dependent individuals who re-ceived smoking and alcohol intervention concur-rently had a higher rate of alcohol abstinence thanindividuals who did not receive smoking interven-tion.21 These findings support the belief that absti-nence from smoking may actually contribute to theinitiation and maintenance of alcohol abstinence.
Emergency medicine has an increasingly im-portant role in disease prevention and health pro-motion, and emergency departments (EDs) havebecome primary purveyors of a variety of healthprograms and services for patients. Increasingly,ED practitioners are recognizing that selected clin-ical prevention and intervention services, such asimmunizations and domestic violence screening,are feasible and appropriate in the ED, particu-larly for non-critically injured or ill patients.22 In-tervention for alcohol and nicotine dependencemay be another important ED service. Emergencydepartments, particularly public hospital EDs,serve as a primary source of ambulatory care for asubstantial proportion of uninsured and underin-sured persons—groups that receive the least pre-ventive care in the United States23–25 and that arevulnerable to substance misuse.26
In fact, the ED is often a frequent source offrontline health care services for persons with al-cohol problems.26 Many of these persons, who arepredominantly young or middle-aged, present withmedical conditions unrelated to alcohol use. How-ever, more commonly there is a clear associationbetween harmful drinking and the presentingproblems. It also is likely that a majority of thesepatients are smokers. In fact, research shows thatthe rate of smoking among alcohol-dependentadults is between 75% and 95%4,11—a rate aboutthree times that of the general adult population.6,11
Early detection of negative health behaviors, suchas mild-to-moderate alcohol problems and smok-ing, is important because patients who receive helpearly in their use or dependence are more likely tobe helped by simple efficient interventions thanare patients with longstanding addictions.27 Thus,it is crucial to assess health behavior in adoles-
cence and young adulthood. Emergency depart-ments may be the only potential source of sub-stance use intervention for many individuals,particularly high-risk groups of dual-substanceusers.
To further understand the merit of dual-sub-stance intervention in the ED, it is necessary toexplore the prevalence of conjoint alcohol use andsmoking among ED patients, the relationship be-tween smoking and alcohol use, and the social-sit-uational factors that encompass both behaviors.28
Given the current need for better understandingabout conjoint smoking and drinking among youngadult patients in the ED, the purposes of this in-vestigation were 1) to assess the prevalence of con-joint use; 2) to determine the factors associatedwith conjoint alcohol use and smoking; and 3) toaddress implications for future investigation ofED-based dual-substance intervention.
METHODS
Study Design. This was a prospective study ofED patients, using questionnaires to assess theprevalence of smoking and drinking. All patientssigned a written consent form approved by the in-stitutional review board for human subjects.
Study Setting and Population. Study partici-pants were drawn from a larger alcohol screeningand intervention study conducted with patientswho presented for treatment in the university hos-pital ED. Participants were eligible for the studyif they 1) were 18–29 years old, 2) consumed al-cohol in the preceding 12 months, 3) provided writ-ten informed consent, and 4) had positive screen-ing results for alcohol problems (AUDIT score >5;AUDIT is discussed in detail under ‘‘Alcohol Prob-lems’’). Participants were excluded if they 1) ar-rived in police custody, 2) had severe communica-tion deficits, 3) were deemed mentally incompetentby staff, 4) had life- or limb-threatening conditions,or 5) posed a threat to the ED staff. Eligibility wasdetermined during face-to-face interviews by staffin the ED waiting area or treatment rooms. Pa-tient information was collected between August1998 and February 1999 (Fig. 1). The normal shifttime for project personnel was from 12 PM to 1 AM.
Study Protocol. Data for this investigation wereobtained from a battery of questionnaires admin-istered to the participants during their initial al-cohol screening in the ED. To enhance efficiency,reliability, and validity of the self-reported data,questionnaires were read aloud to patients by atrained staff member. The screening, which in-cluded about 5.7 minutes for consent, lasted about14 minutes total. Excluding consent for research

1128 SMOKING & DRINKING Horn et al. • CONJOINT SMOKING AND DRINKING
Screened negativen = 669 (57%)
Screened positiven = 500 (43%)
Refusedn = 177 (13%)
Consentedn = 1,169 (87%)
Excludedn = 710 (35%)
Met inclusion criterian = 1,346 (65%)
Patients not approachedn = 699 (25%)
Patients approachedn = 2,056 (75%)
Eligible patientsn = 2,755
Figure 1. The process of patient inclusion.
participation, the screening itself took about 8minutes.
Using the existing questionnaires, the relation-ship between alcohol use and smoking was ex-plored by examining the following domains: 1) con-joint use status; 2) alcohol severity; 3) drugcomorbidity; 4) other health-related risk factors;and 5) demographic information. In total, 15 fac-tors were examined from the questionnaires usedin this investigation (Table 1).
Alcohol Problems. The Alcohol Use DisordersIdentification Test (AUDIT)29–34 was used to assessalcohol problems. The AUDIT is comprised of tenitems. Chronbach’s alpha reliability and item-totalcorrelations are typically 0.80.30,33 Questions 1–8were scored using 0, 1, 2, 3, or 4 (i.e., never,<monthly, monthly, weekly, or daily/almost daily).Questions 9 and 10 were scored using 0 or 4 (i.e.,no or yes). In all questions, 0 indicated less sever-ity. For instance, questions 1–3 measured alcoholconsumption (i.e., How often in the past year haveyou had 5 [male]/4[female] or more drinks on oneoccasion?), 4–6 measured dependence symptomsand tolerance (i.e., How often in the past year haveyou failed to do what was normally expected of youbecause of drinking?), and 7–10 measured alcohol-related harm or consequences (i.e., Have you orsomeone else been injured in the past year as aresult of your drinking?).31–33 The standard totalAUDIT score range is between 0 and 40. Thehigher the score, the greater the likelihood that apatient has alcohol problems. A score of 6 or moreindicated a likelihood of hazardous or harmfuldrinking in this study, and was a primary inclusioncriterion. The AUDIT scores also were used to as-
sess severity of alcohol problems. For exploratorypurposes, a score of >20 represented severe alcoholproblems in this study.
Smoking Status. Smoking status was deter-mined by asking participants ‘‘Do you currentlysmoke cigarettes?’’ Patients who answered ‘‘yes’’were classified as current smokers. Current smok-ers also were probed about occasional or dailysmoking, and if they were daily smokers, howmany cigarettes they smoked every day. Conjointuse was determined by self-reported current smok-ing and an AUDIT score >5.
Drug Comorbidity. The Drug Co-MorbidityQuestionnaire examined the frequency of past yearuse of medications, including sleeping pills, dietpills, tranquilizers, cough medications, antidepres-sants, laxatives, indigestion medications, and pre-scription and over-the-counter pain medications.In addition, the use of illicit drugs such as heroin,cocaine or crack, marijuana, LSD, amphetamines,and methadone was examined. All items werescored as 1, 2, 3, 4, or 5, representing responsecategories of never, rarely, monthly, weekly, anddaily, respectively. This measure was developedspecifically for this study; therefore, no previouspsychometric properties are available.
Health-related Risk Factors. The status of threehealth-related risk factors was assessed using aHealth Risk Survey: 1) overeating; 2) undereating;and 3) emotional/nervous problems. Patients re-sponded by indicating either ‘‘yes’’ or ‘‘no’’ to havingproblems in these health areas in the precedingyear.

ACADEMIC EMERGENCY MEDICINE • October 2000, Volume 7, Number 10 1129
TABLE 1. The 15 Factors Explored
Dependent variable:
• Conjoint use status (drinker [AUDIT > 5] 1 current smoker[self-reported ‘‘yes’’ to current smoking])
Independent variables:
• Alcohol problem severity1. Severity category
• Drug comorbidity2. Over-the-counter medication3. Antidepressant4. Marijuana5. Other illicit drug use
• Health-related risk factors6. Overeating7. Undereating8. Emotional problems
• Demographic factors9. Age
10. Gender11. Employment status12. Marital status13. Roommate status14. Educational level15. Current student status
Demographic Information. Demographic varia-bles included the following: 1) gender; 2) age; 3)employment status; 4) marital or partner cohabi-tation status; 5) educational level; 6) current stu-dent status; and 7) roommate status. All demo-graphic variables except for age and educationallevel were dichotomous.
Data Analysis. The initial analysis included acalculation of the prevalence of conjoint use status:number of current smokers/number who screenedpositive for alcohol problems. Next, following a lit-erature review on predictors of conjoint use, sev-eral factors were selected. Fifteen factors (Table 1)were used as independent variables in the predic-tion model, including demographic factors, alcoholseverity, drug comorbidity, and health-relatedrisks. Drinkers who were not current smokers con-stituted the comparison group.
Initially, general comparisons were made be-tween conjoint users (i.e., patients who currentlysmoke cigarettes and are problem drinkers) anddrinkers only (i.e., patients who are problem drink-ers, but do not currently smoke) on the factorsshown in Table 1. Chi-square analysis was used tofurther explore important or significant relation-ships between the explanatory variables and con-joint use. Next, to determine the extent to whichthe study variables explained and predicted con-joint use when the other variables were controlled,a multiple logistic regression model using a step-wise method was conducted. In order to increasethe reliability of the model and facilitate clinicalinterpretation, continuous data were transformedinto dichotomous data using ‘‘dummy’’ or indicatorcoding. The exception was the age variable. Fac-tors were scaled as dichotomous, using 0 or 1 todefine the absence or presence of a particular at-tribute, respectively.
For instance, alcohol problem severity was as-sessed using AUDIT scores. Patients with AUDITscores between 0 and 20 were classified into thelow-severity group (i.e., not severe), and those hav-ing scores more than 20 were classified into thehigh-severity group (i.e., severe). These categoriesare more clinically meaningful than a single score.Next, drug comorbidity was recoded. These itemswere collapsed into four distinct categories: over-the-counter (OTC)/routine medications, antide-pressants/antianxiety medication (including tran-quilizers), marijuana, and other illicit drugs. TheOTC/routine medication category included dietpills, sleeping pills, cough medicine, laxatives, in-digestion aids, and pain medications. Other illicitdrugs included heroin, cocaine, LSD, ampheta-mines, and methadone. Patients who responded‘‘never’’ or ‘‘rarely’’ were classified as nonusers andpatients who reported monthly, weekly, or daily
were identified as users. The final recoding issueinvolved education. The options were coded to formtwo exclusive categories: ‘‘no college’’ (high schooldegree or less) and ‘‘some college.’’
The regression model coefficients for indepen-dent factors were transformed to odds ratios (ORs).This approach provided a comparison of the uniquecontribution of each factor to the model. Exami-nation of the data revealed no evidence of a prob-lematic level of multicolinearity among predic-tors.35 All Pearson correlation coefficients amongpredictors were <0.50.
RESULTS
Sample Characteristics. Two thousand sevenhundred fifty-five patients were available duringstudy shift time, 2,056 were approached by theproviders, 1,346 met the inclusion criteria, and1,169 consented for participation.
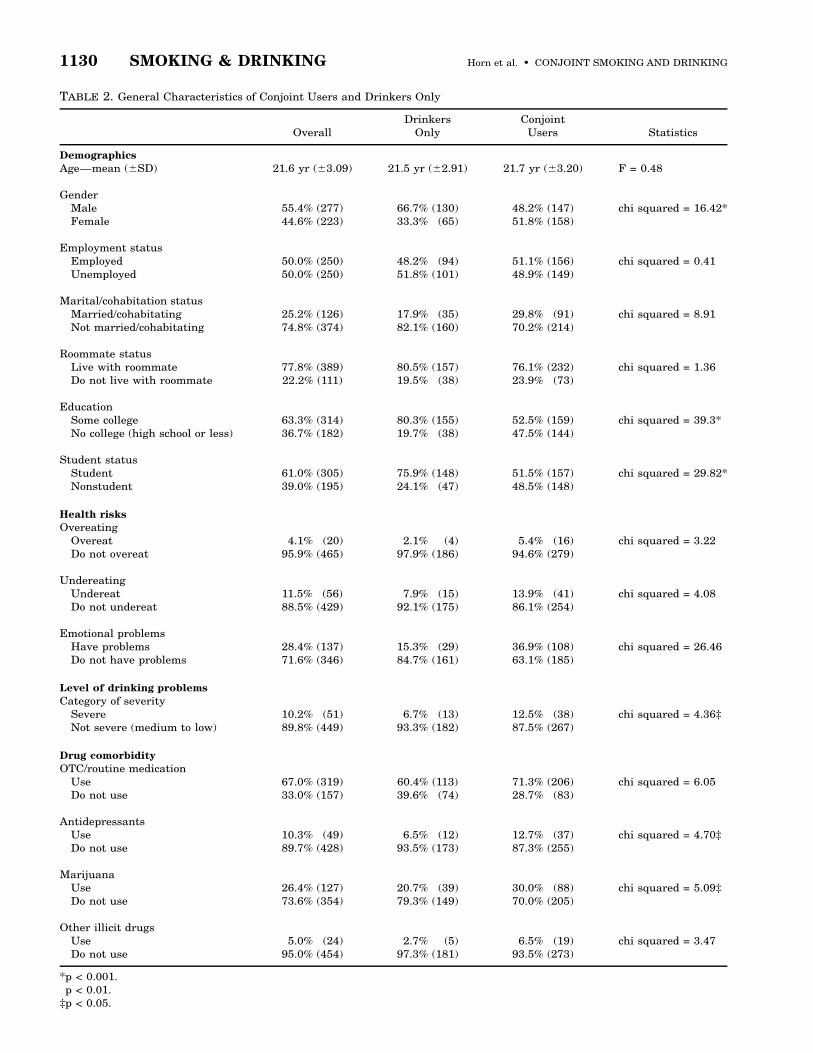
Among the patients who consented for partici-pation (n = 1,169), 500 (43%) screened positive foralcohol problems with an AUDIT score higher than5 (M = 11.9); this constituted the study sample.Characteristics of the groups are provided in Table2. Ninety two percent of participants were whiteand 61% were college students.
Among the 500 study patients who screenedpositive for alcohol problems, 61% were currentsmokers, with 83% of that group being daily smok-ers. Conjoint users who were daily smokers
1130 SMOKING & DRINKING Horn et al. • CONJOINT SMOKING AND DRINKING
TABLE 2. General Characteristics of Conjoint Users and Drinkers Only
OverallDrinkers
OnlyConjoint
Users Statistics
Demographics
Age—mean (6SD) 21.6 yr (63.09) 21.5 yr (62.91) 21.7 yr (63.20) F = 0.48
GenderMale 55.4% (277) 66.7% (130) 48.2% (147) chi squared = 16.42*Female 44.6% (223) 33.3% (65) 51.8% (158)
Employment statusEmployed 50.0% (250) 48.2% (94) 51.1% (156) chi squared = 0.41Unemployed 50.0% (250) 51.8% (101) 48.9% (149)
Marital/cohabitation statusMarried/cohabitating 25.2% (126) 17.9% (35) 29.8% (91) chi squared = 8.91†Not married/cohabitating 74.8% (374) 82.1% (160) 70.2% (214)
Roommate statusLive with roommate 77.8% (389) 80.5% (157) 76.1% (232) chi squared = 1.36Do not live with roommate 22.2% (111) 19.5% (38) 23.9% (73)
EducationSome college 63.3% (314) 80.3% (155) 52.5% (159) chi squared = 39.3*No college (high school or less) 36.7% (182) 19.7% (38) 47.5% (144)
Student statusStudent 61.0% (305) 75.9% (148) 51.5% (157) chi squared = 29.82*Nonstudent 39.0% (195) 24.1% (47) 48.5% (148)
Health risks
OvereatingOvereat 4.1% (20) 2.1% (4) 5.4% (16) chi squared = 3.22Do not overeat 95.9% (465) 97.9% (186) 94.6% (279)
UndereatingUndereat 11.5% (56) 7.9% (15) 13.9% (41) chi squared = 4.08Do not undereat 88.5% (429) 92.1% (175) 86.1% (254)
Emotional problemsHave problems 28.4% (137) 15.3% (29) 36.9% (108) chi squared = 26.46†Do not have problems 71.6% (346) 84.7% (161) 63.1% (185)
Level of drinking problems
Category of severitySevere 10.2% (51) 6.7% (13) 12.5% (38) chi squared = 4.36‡Not severe (medium to low) 89.8% (449) 93.3% (182) 87.5% (267)
Drug comorbidity
OTC/routine medicationUse 67.0% (319) 60.4% (113) 71.3% (206) chi squared = 6.05†Do not use 33.0% (157) 39.6% (74) 28.7% (83)
AntidepressantsUse 10.3% (49) 6.5% (12) 12.7% (37) chi squared = 4.70‡Do not use 89.7% (428) 93.5% (173) 87.3% (255)
MarijuanaUse 26.4% (127) 20.7% (39) 30.0% (88) chi squared = 5.09‡Do not use 73.6% (354) 79.3% (149) 70.0% (205)
Other illicit drugsUse 5.0% (24) 2.7% (5) 6.5% (19) chi squared = 3.47Do not use 95.0% (454) 97.3% (181) 93.5% (273)
*p < 0.001.†p < 0.01.‡p < 0.05.

ACADEMIC EMERGENCY MEDICINE • October 2000, Volume 7, Number 10 1131
TABLE 3. Results from the Multiple Logistic RegressionAnalysis for Conjoint Users (Compared with Drinkers Only)*
Risk Factor OR† 95% CI‡ p-value
Educational level (havinghigh school education orless) 2.74 1.60, 4.69 0.0003
Gender—being female 2.56 1.65, 3.94 <0.0001Marijuana use—using
marijuana 2.34 1.42, 3.86 0.0008Emotional problems—
having problems 2.21 1.33, 3.68 0.0023Student status—being
nonstudent 1.93 1.14, 3.27 0.0148
*The goodness of fit was 485.69, and the LL was 2267.94. Thechi-square of the model was significant (x2 = 84.77, p < 0.001).†Odds ratio (OR) using coefficients obtained from logistic re-gression.‡95% confidence interval.
smoked almost a pack of cigarettes per day (M =17.6, SD 6 10.9). This resulted in two groups: 305conjoint users and 195 drinkers only. General com-parisons between conjoint users and drinkers onlyare presented in Table 2.
Overall, women were far more likely to be con-joint users (51.8%) than drinkers only (33.3%), andwomen (51.8%) represented slightly more of theconjoint users than men. Conjoint users were morelikely than drinkers only to have high school orless education. Among conjoint users with highschool or less education, 54.9% were men and45.1% were women. Conjoint users also were morelikely than drinkers only to have emotional prob-lems. Almost 58% of conjoint users with emotionalproblems were women, compared with 41.4% ofwomen who were drinkers only. Conjoint users(48.5%) also were more likely than drinkers only(24.1%) to be nonstudents. More male conjointusers (54.7%) than females were in the nonstudentcategory. However, a much higher percentage(78.7%) of male drinkers only were nonstudents.Marijuana use was more common among conjointusers than drinkers only. Among conjoint userswho smoked marijuana, a majority (60.2%) weremen. The same held true for drinkers only whoused marijuana—66.7% were men. Only a smallpercentage in either group (#5%) reported prob-lems with overeating or undereating. Further, il-licit drug use was not problematic for either group.
Multiple logistic regression revealed that five ofthe 15 factors explored in this study were indepen-dently associated with conjoint alcohol and tobaccouse (Table 3). The factors that provided a uniquecontribution were 1) educational level (OR = 2.74);2) gender (OR = 2.56); 3) marijuana use (OR =2.34); 4) emotional problems (OR = 2.21); and 5)student status (OR = 1.93). Coefficients, ORs, andrelated statistics are shown in Table 3. The overallpercentage accuracy classification was 68.10%.
DISCUSSION
This study revealed that 1) it is possible to screenand identify conjoint users in an ED setting; 2)problem drinking and smoking prevalence appearto be high among young adult ED patients; 3) sev-eral risk factors are jointly related to smoking anddrinking; and 4) being female significantly in-creases the odds of being a conjoint user.
Identification and Prevalence. Providers wereable to recruit and obtain consent from a majorityof ED patients available during the shift time. Us-ing the AUDIT and a single question about currentsmoking status, conjoint users were efficientlyidentified. Findings revealed a high prevalence ofconjoint alcohol use and smoking among the target
population. Among patients who consented for par-ticipation, almost half screened positive for alcoholproblems. A majority of those patients were cur-rent smokers, with most being regular daily smok-ers. As anticipated, the current smoking rate forthe study sample was substantially higher thansmoking among the general ED adult populationof the same age cohort, which is approximately27%.36 It is also higher than the 41% smoking ratefound in a study of an urban ED population.37
Factors Associated with Conjoint Alcohol Use
and Smoking. Findings suggest that patterns ofsmoking and drinking differ across factors of gen-der, student status, marital/cohabitation status,educational levels, emotional problems, alcohol useseverity, uses of some medications, and marijuana.Overall, results revealed that educational level,gender, marijuana use, emotional problems, andstudent status were significant determinants ofconjoint use of alcohol and tobacco. Analysisshowed that conjoint users were correctly classifiedgiven these five factors with high accuracy (68%),illustrating the capacity of this model for predict-ing conjoint use.
Interestingly, females were more likely thanmales to use both alcohol and tobacco. In fact, theodds for conjoint smoking and alcohol use were al-most three times greater for females than males.Our results were similar to a previous ED studythat found 37% of female drinkers met the criteriafor alcohol problems.38 Another study found that47% of females were conjoint users.39 Studentstatus and gender showed no interactive effects onconjoint use. That is, being female remained a sig-nificant determinant of conjoint use, regardless ofstudent status. Having emotional problems alsowas predictive of conjoint use. More specifically,

1132 SMOKING & DRINKING Horn et al. • CONJOINT SMOKING AND DRINKING
patients who reported emotional problems weretwice as likely to be conjoint users than drinkersonly. The majority of conjoint users with emotionalproblems were women. Past studies have shown40
that women are more likely than men to attributetheir drinking or dependence symptoms as anxietyor depression.
The use of sleeping pills, diet pills, tranquiliz-ers, cough medications, laxatives, indigestion med-ications, and prescription and pain medicationswas not predictive of conjoint use. Furthermore,most of the illicit drugs examined in this studysuch as heroin, cocaine, LSD, amphetamines, andmethadone were unrelated to conjoint use. Mari-juana use was the only drug significantly predic-tive of the risk of conjoint smoking and drinking.The findings are comparable to a study conductedby Schorling and colleagues,41 who found that cig-arette smoking was significantly associated withbinge drinking and marijuana use. Men were morelikely than women to be marijuana users amongdrinkers only and conjoint users.
Lack of education was also a risk factor for con-joint use of alcohol and tobacco. That is, individu-als with low educational levels (e.g., high school orless education) were almost two times more likelyto drink and smoke. Interestingly, the percentagesof males who were less educated and who werenonstudents were dramatically higher than fe-males in the drinkers-only category. However, thepercentage of less-educated women increased inthe conjoint use category. The percentage of less-educated males decreased in the conjoint category.This finding suggests that education may be an im-portant risk factor to explore, particularly amongfemale conjoint users.
Although conjoint users had significantlyhigher AUDIT scores than drinkers only, the auditscore did not appear to be a reliable determinantof conjoint use. This may be due to both conjointusers and drinkers only having uniformly high AU-DIT scores. In addition, although more conjointusers than drinkers only were married or livingwith a partner, marital/cohabitation status was nota significant risk factor. This finding may be ex-plained, in part, by the fact that patients’ marital/cohabitation status was negatively related to theirstudent status (Pearson r = 20.46, p < 0.001) andeducational level (Pearson r = 20.31, p < 0.001).The variance in the grouping variable (conjointusers or drinkers only) accounted for by maritalstatus may come from the correlation between stu-dent status and education. The unique varianceexplained by marital status may be insignificant.Specifically, being married or living with a partnerwas associated with nonstudent status and low ed-ucation—two significant predictors for conjointusers. Overall, the groups were equivalent or sim-
ilar in age, employment status, roommate status,eating habits, and illicit drug use.
Implications for ED-based Investigation of
Dual-substance Intervention. The finds of thisstudy are important because they suggest that in-stituting conjoint or sequential intervention withindividuals who both smoke and drink may be ap-propriate and necessary in an ED setting. Specifi-cally, results show that 1) it is possible to identifyconjoint users and 2) there are a set of jointly as-sociated risk or predictive factors. Appropriatelydeveloped and delivered dual-intervention ap-proaches should assume strategies that addressunderlying issues, risk factors, and related lifeproblems of both substances.42 Past research showsthat such approaches may be more likely to pro-duce enduring gains than those focusing solely onone problem or dependence.5 Although this conclu-sion cannot be drawn from the data, past researchshows that intervention for one dependence maygeneralize to and lead to positive changes in otherlife habits and behaviors.11,28 If the risk factorsjointly associated with drinking and smoking areconsidered, dual-substance intervention effortsmay be enhanced.
Given the prevalence of conjoint use among thestudy sample, relative amounts (units) of interven-tion should be considered for both smoking and al-cohol use with conjoint users. However, given in-dividual differences, patterns, and risks associatedwith conjoint use, a single intervention formulamay not be appropriate for drinkers who smoke vsdrinkers who do not smoke.43 Careful attentionshould be given to factors such as gender (i.e., be-ing female), emotional problems, low educationallevels, and marijuana use when considering inter-vention context and content. These ‘‘red flags’’ mayhelp to design and tailor interventions.
For example, emphasis on stress managementand coping skills may be particularly important forfemale conjoint users.40 This is consistent with thesocial learning models of addiction, which assertthat people come to rely on alcohol use or smokingto deal with stress. Past research indicates thatstress, social situations, and negative emotionsprecede smoking and drinking behaviors and alsoimplicate alcohol as an antecedent to smoking.44 Assuch, smoking may be a means for coping in high-risk alcohol-related situations,44 particularly for fe-males. Another example for tailoring may relate toeducation. For instance, if conjoint users in an EDsetting are likely to have low educational levels,the presentation and writing levels of the materi-als presented should be carefully planned anddelivered. For this population it may be useful toconsider materials developed for low-literacy indi-viduals.

ACADEMIC EMERGENCY MEDICINE • October 2000, Volume 7, Number 10 1133
The target age group was young adults (18–29years-old), who may not yet suffer from irreversi-ble, medical effects of smoking12 and drinking. Infact, only a minority of patients were classified ashaving ‘‘severe’’ alcohol problems. A comprehensiveED response to minimize injuries, disease, andother hazards associated with conjoint alcohol andtobacco use calls for both primary preventionthrough education and public policy and secondaryprevention programs that enable problem drinkersand smokers to be identified and treated early.Early identification and intervention of both sub-stance issues may offer our best hope for cessation.
Although it is not appropriate for EDs to be-come substance ‘‘treatment’’ facilities, there arenew approaches that may be both feasible and ef-fective for EDs. As used to screen and identify pa-tients in the larger study, one potential strategy foraddressing conjoint use in the ED may be screen-ing and brief intervention (SBI). The SBI approachis an innovative, secondary prevention strategythat links new screening technologies to inexpen-sive and often opportunistic interventions that canbe offered in EDs.29,45,46 This type of approach in-cludes minimal demands on providers’ time and re-sources, emphasizes self-help and behavioral self-management techniques, and has showneffectiveness with reducing hazardous drinkingand smoking cessation. In fact, recent studies showthat brief interventions are at least as effective asother treatment methods for mild-to-moderate al-cohol problems and are clearly superior to no treat-ment.45,46 Colby and colleagues38 recently con-ducted an ED-based brief smoking interventionstudy with teen patients. They found ‘‘high ratesof recruitment, retention, and quit attempts andlong periods of continuous abstinence.’’38 Dual-sub-stance intervention using the SBI approach maybe feasible for dual-substance intervention in theED.
LIMITATIONS AND FUTURE QUESTIONS
Our study has three primary limitations that war-rant mention. First, the study was conducted in arural university setting with a homogeneous sam-ple of young adults. Thus, findings may not gen-eralize to urban-metropolitan and/or diverse set-tings. Second, the study was limited to a specificage group (18–29), and it is possible that predic-tors of conjoint use and patterns of drinking andsmoking may differ with an older population ofadults. Third, because this investigation was partof a larger feasibility study, the sample was not arandom sample of the general ED population.
Before emergency medicine can move forwardon widespread implementation of dual-substanceintervention, much research is needed. Develop-
ment of such interventions may benefit from con-sideration of the conjoint user profile found in thisstudy and current SBI strategies. Future studiesshould consider 1) the target population’s interestin quitting smoking and their willingness to re-ceive intervention in a clinical ED setting, 2) ap-propriate inclusion criteria for dual-substance in-tervention, 3) the most appropriate ED deliverysystem for intervention, and 4) the feasibility andeffectiveness of ED-based intervention.
CONCLUSIONS
Overall, study data suggest that smoking is prev-alent among the target population of young adultED patients who have alcohol problems. Moreover,drinkers who smoke are likely to be pack-a-daysmokers. Among the study sample, young femaleswho had low educational levels (e.g., high schooleducation or less), were not currently students,had some emotional problems, and/or currentlyused marijuana were at high risk of conjoint smok-ing and drinking. By examining the differencesand similarities between conjoint users and drink-ers only, and the jointly associated risk factors, itmay be possible to develop brief interventions39 tomeet the specific needs of ED patients who areboth drinkers and smokers. Although the findingsof this study provide insight about the prevalenceand risk of conjoint use, additional study is neededto examine the merit, utility, and feasibility of ED-based dual-substance intervention, as well as thewillingness of patients to receive it.
References
1. Sees KL, Clark HW. When to begin smoking cessation insubstance abusers. J Subst Abuse Treat. 1993; 10:189–95.2. U.S. Department of Health and Human Services. TheHealth Benefits of Smoking Cessation. Bethesda, MD:USDHHS, Public Health Service, National Institutes ofHealth, NIH Publication No. 94-1647; 1990.3. Hoffman AL, Slade J. Following the pioneers: addressingtobacco in chemical dependency treatment. J Subst AbuseTreat. 1993; 10:153–60.4. Bien TH, Burge R. Smoking and drinking: a review of theliterature. Int J Addict. 1990; 25:1429–54.5. Hughes JR. Combining behavioral therapy and pharma-cotherapy for smoking cessation: an update. In: Onken LS,Blaine JD, Boren JJ (eds). Integrating Behavior Therapieswith Medication in the Treatment of Drug Dependence. NIDAResearch Monograph. Washington, DC: U.S. GovernmentPrinting Office, 1995; 150, pp 92–109.6. Hurt RD, Eberman KM, Slade J, Karan L. In: Orleans CT,Slade J (eds). Nicotine Addiction: Principles and Management.New York: Oxford University Press, 1993, pp 310–26.7. Johnson KA, Jennison KM. The drinking-smoking syn-drome and social context. Int J Addict. 1992; 27:749–92.8. McCoy GD, Wynder EL. Etiological and preventive impli-cations in alcohol carcinogenesis. Cancer Res. 1979; 39:2844–50.9. U.S. Department of Health and Human Services. TheHealth Consequences of Smoking: Nicotine Addiction. A Reportof the Surgeon General. USDHHS Publication (CDC) 88-8406.Washington, DC: U.S. Government Printing Office, 1988.10. Bobo JK, Davis CM. Cigarette smoking cessation and al-

1134 SMOKING & DRINKING Horn et al. • CONJOINT SMOKING AND DRINKING
cohol treatment. Addiction. 1993; 88:405–12.11. Bobo JK, Gilchrist LD, Schilling RF II, Noach B, SchinkeSP. Cigarette smoking cessation attempts by recovering alco-holics. Addict Behav. 1987; 12:209–15.12. Joseph AM. Nicotine treatment at the drug dependencyprogram of the Minneapolis VA Medical Center. J Subst AbuseTreat. 1993; 10:147–52.13. DiFranza JR, Guerrera MP. Alcoholism and smoking. JStud Alcohol. 1990; 51:130–5.14. Vaillant GE, Schnurr PP, Baron JA, Gerber PD. A pro-spective study of the effect of cigarette smoking and alcoholabuse on mortality. J Gen Intern Med. 1991; 6:299–304.15. American Psychiatric Association. Diagnostic and Statis-tical Manual of Mental Disorders-IV. Washington, DC: APA,1994.16. Benowitz NL. Pharmacologic aspects of cigarette smokingand nicotine addiction. N Engl J Med. 1988; 319:1318–30.17. Henningfield JE, Keenan RM. The anatomy of nicotine ad-diction. Health Values. 1993; 17(2):12–9.18. Fisher EB Jr, Lichtenstein E, Haire-Joshu D, Morgan GD,Rehberg HR. Methods, successes, and failures of smoking ces-sation programs. Annu Rev Med. 1993; 44:481–513.19. Lando HA. Formal quit smoking treatments. In: OrleansCT, Slade J (eds). Nicotine Addiction: Principles and Manage-ment. New York: Oxford University Press, 1993, pp 221–44.20. Irving LM, Seinder AL, Burling TA, Thomas RG, BrennerGF. Drug and alcohol abuse in patients’ attitudes about smok-ing cessation. J Subst Abuse. 1994; 6:267–78.21. Burling TA, Marshall GD, Seinder AL. Smoking cessationfor substance abuse inpatients. J Subst Abuse. 1991; 3:269–76.22. Rodriquez RM, Kreider NJ, Baraff LJ. Need and desire forpreventive care measures in emergency department patients.Ann Emerg Med. 1995; 26:615–20.23. Horne A, Ros SP. Telephone follow-up of patients dis-charged from the emergency department: how reliable? PediatrEmerg Care. 1995; 11:173–5.24. Maio RF. Alcohol and injury in the emergency department:opportunities for intervention. Ann Emerg Med. 1995; 26:221–3.25. Longabaugh R, Minugh PA, Nirenberg TD, Clifford P,Becker B, Woolard R. Injury as a motivator to reduce thinking.Acad Emerg Med. 1995; 2:817–25.26. Institute of Medicine. Broadening the Base of Treatmentfor Alcohol Problems. Washington, DC: National AcademyPress, 1990, pp 142–62, 211–78.27. U.S. Preventive Services Task Force. Guide to Clinical Pre-ventive Services: An Assessment of the Effectiveness of 169Interventions. Baltimore, MD: William & Wilkins, 1989.28. Zimmerman RS, Warheit GJ, Ulbrich PM, Auth JB. Therelationship between alcohol use and attempts and success atsmoking cessation. Addict Behav. 1990; 15:197–207.29. Fleming MF, Barry KL, Manwell LB, Johnson K, LondonR. Brief physician advice for problem alcohol drinkers: a ran-
domized controlled trial in community-based primary carepractices. JAMA. 1997; 277:1039–45.30. Allen JP, Litten RZ, Fertig JB, Babor T. A review of re-search on the Alcohol Use Disorders Identification Test (AU-DIT). Alcohol Clin Exp Res. 1997; 21:613–9.31. Conigrave KM, Hall WD, Saunders JB. The AUDIT ques-tionnaire: choosing a cut-off score. Addiction. 1995; 90:1349–56.32. Schmidt A, Barry KL, Fleming MF. Detection of problemdrinkers: the Alcohol Use Disorders Identification Test (AU-DIT). South Med J. 1995; 88:52–9.33. Saunders JB, Aaslund OG, Babor TF, de la Fuente JR,Grant M. Development of the Alcohol Use Disorders Identifi-cation Test (AUDIT): WHO collaborative project on early de-tection of persons with harmful alcohol consumption—II. Ad-diction. 1993; 88:791–804.34. Barry KL, Fleming MF. The Alcohol Use Disorders Iden-tification Test (AUDIT) and the SMAST-13: predictive validityin a rural primary care sample. Alcohol Alcohol. 1993; 28:33–42.35. Licht MH. Multiple regression and correlation. In: GrimmLG, Yarnold PR (eds). Reading and Understanding Multivar-iate Statistics. Washington, DC: American Psychological As-sociation, 1994.36. Centers for Disease Control and Prevention. BehavioralRisk Factor Surveillance Survey (BRFSS) Summary Preva-lence Report. Atlanta: CDC, 1997.37. Lowenstein SR, Tomlinson D, Koziol-McLain J, ProchazkaA. Smoking habits of emergency department patients: an op-portunity for disease prevention. Acad Emerg Med. 1995; 2:165–71.38. Colby SM, Monti PM, Barnett DJ. Brief motivational in-terviewing in a hospital setting for adolescent smoking: a pre-liminary analysis. J Consult Clin Psychol. 1998; 66:574–8.39. Weisner C, Schmidt L. Gender disparities in treatment foralcohol problems. JAMA. 1992; 268:1872–6.40. Bradley K, Boyd-Wickizer J, Powell S, Burman M. Alcoholscreening questionnaires in women: a critical review. JAMA.1998; 280:166–71.41. Schorling JB, Gutgesell M, Klas P, Smith D, Keller A. To-bacco, alcohol and other drug use among students. J SubstAbuse. 1994; 6:105–15.42. Botvin GJ, Botvin EM. Adolescent tobacco, alcohol, anddrug abuse: prevention strategies, empirical findings, and as-sessment issues. J Dev Behav Pediatr. 1992; 13:290–6.43. Sobell LC, Sobell MB. Alcohol abuse and smoking: dualrecoveries. Alcohol44. Health Res. World. 1996; 20:124–7.45. Abrams DB, Rohsenow DJ, Niaura RS, et al. Smoking andtreatment outcome for alcoholics: effects on coping skills, urgeto drink, and drinking rates. Behav Ther. 1992; 23:283–97.46. Miller WR. Increasing motivation for change. In: HesterRK, Miller WR (eds). Handbook of Alcoholism Treatment Ap-proaches, 2nd Ed. New York: Allyn & Bacon, 1995, pp 89–104.