consensus on management of deep vein thrombosis … · upplement to ournal of the association of...
TRANSCRIPT

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 2016 7
Consensus on Management of Deep Vein Thrombosis with Emphasis on NOACs (Non-Vitamin K Antagonist Oral Anticoagulants): Recommendations from Inter-Disciplinary Group of Indian ExpertsWorking Group Leaders: Rajiv Parakh1, Pinjala Rama Krishna2, Pravin Amin3, VS Bedi4, Sanjay Desai5, Harjit Singh Dumra6, PC Gupta7, Vineet Gupta8, Rajesh Hydrabadi9, Dhanesh Kamerkar10, Nalini Mahajan11, Paresh Pai12, Pankaj Patel13, Kumud Rai14, Raghuram Sekhar15, Dheepak Selvaraj16, Ajay Sharma17, SR Subrammaniyan18
1Chairman, Division of Peripheral Vascular and Endovascular Sciences, Medanta Medicity,Gurgaon, 2Head, Department of Vascular and Endovascular Surgery, NIMS, Hyderabad, 3Chief, Department of Critical Care, Bombay Hospital, Mumbai, 4Chairman and Head, Dept. of Vascular and Endovascular Surgery, SGRH, Delhi, 5Head, Department of Vascular and Endovascular Surgery, M.S.Ramaiah Memorial Hospital, Bangalore, 6Consultant, Department of Critical Care, Sterling Hospital, Ahmedabad, 7Consultant Vascular Surgeon, CARE Hospital, Hyderabad, 8Senior Consultant and Head - Medical Oncology and Haematology, Sakra World Hospital, Bangalore, 9Consultant Vascular Surgeon, Sterling Hospital, Ahmedabad, 10Consultant Vascular Surgeon, Ruby Hall Clinic, Pune, 11Clinical Director, Nova IVI Fertility, Delhi, 12Consultant Vascular Surgeon, Lilavati Hospital, Mumbai, 13Consultant Vascular Surgeon, Lilavati Hospital, Mumbai, 14Consultant Vascular Surgeon, Max Super Specialty Hospital, Saket, Delhi, 15Consultant Vascular Surgeon, KDAH, Mumbai, 16Department of Vascular Surgery, Christian Medical College, Vellore, 17Consultant Hematologist, Sir Ganga Ram Hospital, Delhi, 18Department of Vascular Surgery and Endovascular Science, Vijaya Hospital, Chennai
AbstractIt is estimated that around 2.5 lac patients are identified as having an acute venous thrombo-embolic event in India annually. This includes patients with deep vein thrombosis and pulmonary embolism, and is estimated to result in more than 3.7 lacs deaths each year in European countries. The ‘Consensus on Management of Deep Vein Thrombosis with Emphasis on NOACs (Non-Vitamin K Antagonist Oral Anticoagulants): Recommendations from Inter-Disciplinary Group of Indian Experts’ position paper was developed to assist clinicians and institutions with an evidence-based approach to the diagnosis and treatment of acute deep vein thrombosis patients. Key to the evaluation of patients with suspected deep vein thrombosis is the use of the clinician’s clinical evaluation with the help of pre-test probability tools as well as judicious use of objective diagnostic tests. Our hope is that we have supplemented clinicians’ clinical acumen, and assisted them and their health systems in developing best practice approaches to this ever-interesting population of patients.
The Deep Vein Thrombosis Consensus Working Group welcomes your inputs on how improvements might be made on this paper in the future.
Aims1. To improve accurate diagnosis
and treatment of deep vein thrombosis
2. To prevent progress ion or recurrence of thromboembolic disease.
3. To safely use anticoagulants to reduce the likelihood of patients
all races, age groups, and both genders. DVT in the lower extremity can be classified as (a) proximal (the popliteal vein or thigh veins are involved) or (b) distal (the calf veins are involved). And etiologically, it can be classified as provoked (when the risk factor is known) and unprovoked (when the risk factor is unknown).1 Various hereditary as well as acquired factors predispose to the development of VTE (Table 1).2
The global burden of VTE shows overall annual incidences of 0.75-2.69 per 1000 population and 2-7 per 1000 in elderly (≥70 years of age).3 The overall age adjusted incidence rate of VTE is higher for men (114 per 100,000) than women (105 per 100,000) with male to female sex ratio of 1.2:1. 4,5 The true incidence of VTE is hard to estimate because of the often silent nature of the condition. In Prospective Registry on Venous Thromboembolic Events (PROVE) conducted in 19 countries, 667 patients with symptomatic DVT from India were included. In this study, proximal plus calf DVTs were found in 54%, proximal DVT in 17 %, and calf DVT in 13 % of Indian patients, compared with 52,
harm and complicat ions of anticoagulation therapy.
Introduction“Venous thromboembolic (VTE)
disease” is a term used to describe both deep vein thrombosis (DVT) and pulmonary embolism (PE).Venous thromboembolism (VTE) is a global health problem as it affects

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 20168
18, and 24 per cent in the global PROVE population, respectively.6 The SMART study involving 2420 Asian patients undergoing major or thopaedic surger ies without thromboprophylaxis showed that the incidence of symptomatic VTE is comparable to that of the western countries.7 In the ENDORSE study, a multinational cross-sectional survey, out of 68,183 patients in acute hospital beds across 32 countries, 51.8% were at risk for developing VTE according to ACCP guidelines.8 In this study, chronic pulmonary disease, heart failure and complete immobi l izat ion were the most common risk factors before and during hospitalization, respectively.8 The subset of ENDORSE study showed that in India, 53.6% of hospita l ized pat ients [surgical (61.3%), medical (44.7%)] were at-risk for VTE, still >80% of these
patients did not receive American College of Chest Physicians (ACCP) recommended thromboprophylaxis.9 About 30% of VTE patients develop recurrence within next 10 years and is highest within first 6 to 12 months of presentation.10,11
Diagnosis of Deep Vein Thrombosis
Symptoms and signs of DVT (Table 2)12 are not specific and have different possible causes which may warrant further evaluation.13 T h e d i a g n o s i s o f D V T c a n b e often missed, even in high-risk patients, with a history and physical examination alone.13
It is also important to ascertain the diagnosis of DVT accurately to minimize the risk of thromboembolic complications and the potential risk of bleeding due to anticoagulant therapy.14 Studies have shown that only 20–40% of patients presenting with symptoms of DVT, actually have confirmed diagnosis of the condition.15–17 Now, It has been establ ished that a combination of signs, symptoms and clinical prediction rules can be useful to categorise suspected DVT patients as low, moderate or high risk of DVT,and aid further management o f s u c h p a t i e n t s . 1 3 F o l l o w i n g clinical prediction rules can assist in diagnosis of DVT.
Clinical Prediction Rules for Deep Vein Thrombosis
Validated cl inical predict ion rules reliably predict the pre-test probability of DVT, which guide the interpretation of subsequent diagnostic tests. The usefulness of various diagnostic tests and imaging studies in predicting the presence of DVT depends on the likelihood of disease in each risk
group. For example, a negative test may rule out DVT in a low-probability patient but not in a high-probability patient when applied. Many patients have an intermediate probability of DVT, in such cases; clinical judgment plays an important role in making the decision to treat.18 Of the available clinical prediction rules for DVT, modified Wells score seems to be more useful because of its reproducibility in predicting the pre-test probability of DVT in outpatient settings (Table 3).19–21 The pre-test probability of DVT in three risk group category is 5% (low risk), 17% (moderate risk) and 53% (high risk) respectively while in the two risk category it is 6% (DVT unlikely) and 28% (DVT likely) respectively.20,21
M e d i c a l p a t i e n t s h a v e a heterogeneous risk of VTE therefore evaluation of thromboprophylaxis strategies in such patients in two different strata, low risk and high risk is suggested by the guidelines. Several Risk Assessment Models have been proposed to estimate the baseline risk of VTE in hospitalized medical patients. Of which, the Padua prediction score seems to be useful for VTE risk assessment of hospitalized medical patients (Table 4).22 In a prospective observational study, 1180 hospitalized medical patients using this score were, categorized as low risk (<4 points; 60.3% of patients) or high risk ( ≥4 points; 39.7% of patients) for VTE and followed for symptomatic VTE for 90 days. VTE occurred in 11.8% of high-risk patients who did not receive thromboprophylaxis vs 2.2% of high-risk patients who received thromboprophylaxis . . Among 711 low-r i sk pat ients , two (0.3%) developed VTE (1 PE, 1 PE with DVT). The ACCP 9th edition guidelines for ‘Prevention of VTE in Nonsurgical Patients’ mentions that ‘this model provides the best available basis for judging hospitalized patients’ risk.23
In patients undergoing general and abdominal-pelvic surgery, the risk of VTE varies depending o n b o t h p a t i e n t - s p e c i f i c a n d procedure-specif ic factors. The recommendations for deep vein
Table 1: Risk factors for venous thromboembolsm2
Acquired risk factorsSurgeryTrauma (major trauma or lower – extremity injury)Immobility, lower – extremity paresisCancer (active or occult)Cancer therapy (hormonal, chemotherapy, angiogenesis inhibitors, radiotherapy)Venous compression (tumor, hematoma, arterial abnormality)Previous VTEIncreasing agePregnancy and the postpartum periodEstrogen-containing oral contraceptives or hormone replacement therapySelective estrogen receptor modulatorsErythropoiesis-stimulating agentsAcute medical illnessInflammatory bowel diseaseNephrotic syndromeMyeloproliferative disordersParoxysmal nocturnal hemoglobinuriaObesityCentral venous catheterizationInherited risk factorsFactor V Leiden Mutation (most common)Prothrombin gene mutation (20210A)Protein S DeficiencyProtein C Deficiency Antithrombin III DeficiencyHyper-homocysteinemia
Table 2: Clinical features of deep vein thrombosis12
Symptoms PercentagesCalf tenderness 94Calf pain 90Ankle swelling 76Calf swelling 42Dilated superficial veins 33

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 2016 9
profile, electrolyte levels, l iver function tests and kidney function tests.26
D - d i m e r , a d e g r a d a t i o n product of cross-linked fibrin is commonly elevated in patients with thromboembolism. However, one needs to bear in mind that D-dimer test does not necessarily help in diagnosis of VTE, but rather helps in rul ing out thrombotic c o n d i t i o n s . I t s l e ve l s m a y b e e l e va t e d i n o t h e r c o n d i t i o n s l ike mal ignancy, disseminated intravascular coagulation, infection, acute inflammation, stroke, atrial fibrillation, following surgery or trauma.21 In a systematic review, total 217 D-dimer test evaluations for DVT were analysed. In this study, the ELFA (Enzyme Linked I m m u n o f l u o r e s c e n c e A s s a y ) , m i c r o p l a t e E L I S A a n d l a t e x quantitative assays were found to have higher sensitivities (96%, 94% and 93% respectively) compared to the whole-blood D-dimer assay (83%) , la tex semi quant i ta t ive assay (85%) and latex qualitative assay (69%) respectively.27 Based on these data, the ELFA (Enzyme L i n k e d I m m u n o f l u o r e s c e n c e Assay) , microplate ELISA and l a t e x q u a n t i t a t i ve a s s a y s a r e considered as “highly sensitive whereas, the whole-blood D-dimer assay , la tex semi quant i ta t ive assay and latex qualitative assays are considered as “moderately s e n s i t i v e ” D - d i m e r a s s a y s . 2 1 Compression ultrasonography is preferred over venography for the diagnosis of DVT due to its wider availability, non-invasive nature and relatively economical advantage.21 The findings of a meta-analysis do not support the use of magnetic resonance venography over ul trasound as a f i rs t - l ine imaging method; however, it may be useful in the diagnosis of DVT where ultrasound is difficult (e.g. leg casting, excessive subcutaneous tissue or fluid preventing adequate assessment of compressibility) or non-diagnostic.21,28 Similarly, CT venography is also useful to diagnose DVT in such patients.21 Recurrent VTE requires investigations for thrombophil ia . 26 The American
Table 3: Modified Wells score19–21
Parameter ScoreActive cancer (treatment ongoing, or within 6 months or currently receiving palliative treatment)
1
Paralysis, paresis or recent plaster immobilization of lower extremities 1Recently bedridden for ≥3 days or major surgery within past 12 weeks under general or regional anesthesia
1
Localized tenderness along the distribution of the deep venous system 1Entire leg swelling 1Calf swelling more than 3 cm compared with asymptomatic leg 1Pitting edema (greater than asymptomatic leg) 1Previous DVT documented 1Collateral superficial veins (non-varicose) 1Alternative diagnosis (at least as likely as DVT) -2Interpretation:3 risk group: Patients with score 0 to -2 are considered to be at low risk, between 1-2 at moderate and ≥3 are at high risk2 risk group: patients are stratified as DVT unlikely (Wells score < 2) or DVT likely (Wells score > 2).
Table 4: The Padua Prediction Score22
Parameter ScoreActive cancer (local or distant metastases and/or in whom chemotherapy/ radiotherapy in previous 6 months)
3
Previous VTE (with the exclusion of superficial vein thrombosis) 3Reduced mobility (Bed rest with bathroom privileges due to patient’s limitations or on physicians order) for > 3 days.
3
Already known thrombophilic condition(Carriage of defects of Anti-thrombin, Protein C or S, Factor V Leiden, G20210A Prothrombin mutation, Anti-phospholipid syndrome)
3
Recent (<1 month) trauma and/or surgery 2Elderly patient with age >70 years 1Heart and/or respiratory failure 1Acute myocardial infarction or ischemic stroke 1Acute infection and/or rheumatologic disorder 1Obesity (BMI >30kg/m2) 1Ongoing hormonal treatment 1Interpretation:If the score is <4: Low risk of VTEIf the score if ≥4: High risk of VTE
thrombosis risk assessment are summarized in Table 5. Although several models for risk stratification exist, all have important limitations. One such model is the Caprini score, which estimates VTE risk by adding points for various VTE risk factors. With this model, VTE risk is categorized as being very low (0-1 point), low (2 points), moderate (3-4 points), or high (5 points). It is relatively easy to use and appears to
discriminate reasonably well among patients at low, moderate, and high risk for VTE.24,25
Investigations for Deep Vein Thrombosis
Basic laboratory investigations, D-dimer assessment and imaging are useful in diagnosis of DVT. Basic laboratory investigations include complete blood count, coagulation
Table 5: Recommendations for deep vein thrombosis risk assessment
• We suggest the use of Modified Wells Score for pretest probability assessment in outpatients with clinical suspicion of DVT.
• In hospitalized patients considered to be at high risk of DVT, we suggest the use of PADUA score, for DVT risk assessment.
• In patients who are undergoing general and abdominal-pelvic surgery, we suggest the use of Caprini score to assess the risk of DVT.

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 201610
College of Chest Physicians 9th Ed guideline suggests classification of suspected DVT patients into low, moderate and high pretest probability based on the clinical assessment for guiding the diagnostic procedures in case of first lower extremity DVT.21 The recommended diagnostic tests for respective pretest probability are given in Table 6.
Treatment of Acute Deep Vein Thrombosis
Early, accurate diagnosis of DVT is important because treatment with anticoagulants reduces the risk of PE, relieves acute symptoms (e.g., leg pain), prevents DVT in a distal calf vein from extending to proximal veins (e.g., femoral), and may decrease the incidence of PTS29
extension and PE. The anticoagulant t h e r a p y f o r D V T h a s e v o l ve d f rom inpat ient adminis t ra t ion o f in t ravenous unfrac t ionated h e p a r i n ( U F H ) t o o u t p a t i e n t therapy with low molecular weight heparin (LMWH), warfarin and non-Vitamin-K antagonist oral a n t i c o a g u l a n t s ( N O A C s ) . T h e duration of anticoagulant therapy is defined as acute (0-7 days), long term (first 3 months of therapy) and extended therapy (beyond 3 months).30 Heparin and warfarin n e e d r o u t i n e m o n i t o r i n g o f anticoagulation profile through aPTT and INR respectively, hence
limiting their use.
Parenteral Anticoagulation for Acute Deep Vein Thrombosis
Heparin use has been a tradition i n t h e m a n a g e m e n t o f a c u t e DVT episode. Heparin therapy prevents extension of thrombus and subsequently reduces (but doesn’t eliminate) the risk of non-fatal and fatal PE. However, complete clot lysis with heparin therapy has been seen in less than 10% of acute DVT patients in venography studies after treatment. Unfractionated heparin was the standard of care for initial treatment of acute DVT until the introduction of LMWH (Low Molecular Weight Heparin). A meta-analysis of eight clinical trials has shown that subcutaneous UFH is more effective than and a t l eas t as sa fe as cont inuous intravenous UFH administration for the initial treatment of DVT. Low Molecular Weight Heparin provides better anti-Xa activity, has longer half- l i fe , and better predictabi l i ty of ant icoagulant response than UFH. LMWH can be given once or twice daily s.c. without need of aPTT monitoring. Also, the rate of heparin-induced thrombocytopenia with LMWH is less compared to UFH.31 In two meta-analyses, fixed-dose s.c. LMWH was found to be at least as effective and
safe as adjusted-dose intra venous UFH for treatment of patients with acute VTE.32,33 Fondaparinux is a synthetic and selective inhibitor of factor Xa which was found to be at least as effective and safe as enoxaparin in the initial treatment of symptomatic deep vein thrombosis in a randomized controlled trial. The recommendations for parenteral ant icoagula t ion in acute deep vein thrombosis t reatment are summarized in Table 7.34
Bleeding is the most common adverse effect of anticoagulant t he rap y . UF H / LMWH t he rap y may also be associated with non-h a e m o r r h a g i c a d ve r s e e f f e c t s such as HIT (Heparin Induced Thrombocytopenia), osteoporosis. They are caused by the nonspecific protein binding of UFH and are less common with LMWH, owing to decreased molecular charge. Heparin Induced Osteoporosis is an adverse effect of long-term UFH or LMWH therapy.35 This is not a major concern in most patients with DVT, who receive only short-term treatment ; however , long-term heparin therapy may be associated with substantial bone loss.
Oral AnticoagulantsVitamin K Antagonists
Warfar in ac t s by inh ib i t ing v i t a m i n K e p o x i d e r e d u c t a s e (VKORC) responsible for the cyclic inter-conversion of vitamin K1 and vitamin K epoxide. Inhibition of vitamin K epoxide reductase reduces the activation of coagulation factors II, VII, IX, and X production by the liver.36 The structure (racemic mixture) and pharmacokinet ic properties (hepatic metabolism, high protein binding) makes warfarin more prone for the drug interactions. Warfarin has two isomers S-isomer and R-isomer, of which “S” form is more potent. Both the isomers are metabolized primarily by CYP2C9 (S-isomer), and CYP1A2 and 3A4 (R-isomer) isozymes.36 Warfarin has several limitations like slow onset and off set of action, drug-food and drug-drug interactions (Figure 1), genetic polymorphism leading to variable response. Due to such
Table 6: Recommended initial diagnostic tests for acute deep vein thrombosis21
Pretest probability Recommended initial testLow Moderately sensitive D-dimer test (preferred) or compression ultrasound
of proximal veinsModerate Highly sensitive D-dimer test (preferred), proximal compression
ultrasound, or whole-leg ultrasound examinationHigh Proximal compression (preferred) or whole-leg ultrasound examination
Table 7: Recommendations for parenteral anticoagulation in acute deep vein thrombosis treatment
• Initial treatment with parenteral anticoagulant is recommended for patients with acute DVT, over no such treatment.
• We recommend the use of LMWH/fondaparinux over UFH for treatment in patients with acute DVT due to lack of need for routine aPTT monitoring and ease of administration.
• We recommend weight based dosing of LMWH in all patients for the treatment of acute DVT.
• In case intravenous UFH is preferred, we recommend aPTT monitoring every 6 hourly until two consecutive therapeutic levels are achieved and then 24 hourly for the treatment of acute DVT.
• We recommend platelet count monitoring at baseline and every 2 or 3 days between days 4-14 (or until UFH/LMWH is stopped) of UFH/LMWH therapy for early detection and management of HIT (Heparin Induced Thrombocytopenia).

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 2016 11
l imi ta t ions , war far in requi res frequent monitoring with INR to keep balance between effectiveness and safety in clinical practice.36 Warfarin has some issues peculiar to Indians. The dietary habit of Indians di f fer that f rom their Western counterparts because of which they are prone to various drug-food interactions. For example, eating green leafy vegetables like cabbage, cauliflower, spinach and other foods rich with vitamin K in diet would interfere target INR on patients with warfarin/acenocoumarol and cause labile INR values. Habitual intake of over the counter medications [e.g. nonsteroidal anti-inflammatory d r u g s ( N S A I D s ) / t r a m a d o l ] or alternative herbal products/foods (e.g. garlic, fenugreek) for various disorders would increase the OAC action of the VKA and may cause bleeding. Paracetamol i s a f r e q u e n t l y u n r e c o g n i z e d cause of over anticoagulation in India. Concomitant use of anti-tubercular drugs l ike isoniazid (INH) or rifampicin can also alter INR values and result in over or under anticoagulation. Indians with low body weight and body mass index (BMI) require lesser doses of VKA to achieve target INR compared to their Western counterparts and are more prone to bleeding. Smoking a l so causes enzyme induct ion and lowers INR. Another issue in India is INR monitoring on VKA therapy. One Indian study had shown poor outpatient VKA
anticoagulant control with high proportion of sub therapeutic PT/INR values and high complication r a t e s . 3 7 A n o t h e r I n d i a n s t u d y showed unsatisfactory knowledge base of clinicians in terms of OAC targets with a tendency to under coagulate in view of the perceived risk of bleeding.38 To address such challenges with VKAs, Time in Therapeutic Range (TTR) could be a suitable option. TTR is a measure of intensity of anticoagulation control, which estimates the percentage of time INR values within therapeutic range (i .e VTE treatment target INR should be 2-3) for patients on VKAs.39 TTR is calculated by Rosendaal method, and it should be >60 % to be effective for VKAs. TTR helps the physician to maintain the quality of anticoagulation control over a therapeutic period as well as to minimize the risk of adverse events . i .e . thromboembolic or bleeding on VKA therapy.39 In order to achieve better patient compliance and target INR values as per the recommended guidelines for OAC there is a pressing need for better patient education and physician/local practitioner update of the various issues involved.
For venous thrombosis prevention after hip and major gynaecological surgeries, warfarin (INR 2-3) has been found to be effective with modest risk of clinically relevant bleeding.40 In a meta-analysis of LMWH, UFH and warfar in for prophylaxis of thrombo-embolism
in orthopaedic surgery, warfarin had significantly lower risk of minor bleeding compared with LMWH [RR for LMWH vs. warfarin 3.28, p < 0.05].41 For the treatment of acute DVT, initial therapy with VKA alone is not recommended because VKA alone was found to be associated with more recurrent symptomatic and asymptomatic VTE in a randomized trial. When acute VTE is suspected initial parenteral anticoagulation for at least 5 days along with VKA is given and once the INR reaches 2-3, parenteral anticoagulat ion should be discontinued.42 DURAC43 and WODIT trials44 demonstrated that oral anticoagulation therapy with VKA for 6 months and 1 year is better than 6 weeks and 3 months of therapy for prevention of recurrent VTE in patients who had first episode of VTE and idiopathic proximal DVT respectively.Need for Newer Oral Anticoagulants
Need for frequent laboratory moni tor ing i s a cha l l enge for outpatient management with VKAs especia l ly in India . Therefore , an oral anticoagulant with wide therapeutic window without routine laboratory monitoring would be a good alternative to VKAs in the treatment as well as secondary prevention of DVT. Non-Vitamin K Antagonist Oral Anticoagulants (NOACs)
The NOACs are broadly classified into two major categories: direct thrombin (factor IIa) inhibitors and direct Factor Xa inhibitors. Dabigatran is a direct thrombin inhibitor while other three i .e . rivaroxaban, apixaban, and edoxaban are direct factor Xa inhibitors.36 The NOACs offer advantages of predictable pharmacokinetic profile and lesser food and drug interactions compared to warfarin. Moreover NOACs do not require routine monitoring. The NOACs have been extensively studied in the treatment of acute VTE and prevention of VTE. Dabigatran, rivoroxaban, apixaban and edoxaban have shown to be effective and at least comparable in safety with the conventional treatment of acute VTE. They are associated with lower risk of
Fig. 1: Limitations of Vitamin K antagonists
VKA therapy has several limitations
that make it difficult to use in practice
Unpredictable response
Narrow therapeutic window
(INR range 2-3)
Routine coagulation monitoring
Slow onset/offset of action
Intracranial
bleeding
Frequent dose adjustments
Numerous food-drug interactions
Numerous drug-drug interactions
Warfarin resistance
CYP 2C9, VKORC1 genetic polymorphisms

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 201612
Table 8: Pharmacology of NOACs
Dabigatran46 Rivaroxaban49 Apixaban56 Edoxaban55
Mechanism of action
Competitive, direct thrombin inhibitors
Selective inhibitor of FXa
Selective inhibitor of FXa
Selective inhibitor of FXa.
Time to peak concentration (T-max)
1 - 3 hours 2 to 4 hours 3 to 4 hours 1-2 hours
Plasma protein binding
35% 92-95%, Approximately 87%
About 55%
Renal elimination
80% About 51% recovered as inactive metabolites (urine 30 and feces 21%)
Renal excretion is about27% of total clearance
Renalclearance is about 50% of total clearance
Metabolism Not a substrate, inhibitor, or inducer of CYP450
Major metabolism via CYP3A4/5 and CYP2J2 and hydrolysis
Substrate of transport proteins: P-gp
Minimalmetabolism via hydrolysis, conjugation,and oxidation by CYP3A4.
Half-life 12-17 hours 5-9 hours 12 hours 10 to 14 hours
intracranial or intracerebral bleeding compared to warfarin.45 Dabigatran
Dabigatran etexilate, an oral prodrug is rapidly converted by es terases to dabigatran which competitively inhibits both free and fibrin-bound thrombin.36 In 2014, dabigatran received approval in India for the treatment and secondary prevention of DVT and PE in patients who have been treated with a parenteral anticoagulant (UFH or LMWH/fondaparinux) for 5-10 days. Its use is also approved to reduce the risk of recurrence of DVT and PE in patients who have been previously treated and for the prophylaxis of DVT and PE in patients who have undergone hip replacement surgery.46 The approval is based on four clinical trials which examined the effects of dabigatran in venous thromboembolism (VTE). Dabigatran can be given as a simple, fixed-dose regimen without need for routine laboratory monitoring.
The RE-COVER studies compared dabigatran versus warfar in in patients with acute VTE who initially received parenteral anticoagulation therapy.47,48 Dabigatran was found to be non-inferior to warfarin for the primary outcome of recurrent VTE and related deaths, and major bleeding rates were found to be less with dabigatran compared to warfarin in individual studies.47,48
The pooled analysis of RE-COVER
and RE-COVER-II s tudies a lso showed non-inferiority of dabigatran for the primary efficacy outcome of recurrent symptomatic VTE and related deaths, and significantly lower bleeding rates compared to warfarin in the treatment of acute VTE.48
Rivaroxaban
Rivaroxaban is a selective and reversible direct oral FXa inhibitor.36 In 2011 , the USFDA approved rivaroxaban to reduce the risk of DVTs and PEs from occurring after knee or hip replacement surgery. In November 2012, the USFDA approved it for the treatment of acute DVT or PE, and to reduce the risk of recurrent DVT and PE following initial treatment.49,50 Rivaroxaban can be given as a simple, fixed-dose regimen without need for routine laboratory monitoring.51 The efficacy of rivaroxaban was evaluated in the EINSTEIN studies (EINSTEIN-DVT and EINSTEIN-PE) for the treatment of acute DVT/PE respectively.51,52 These studies showed that compared w i t h L M W H / V K A t r e a t m e n t , rivaroxaban was non-inferior for recurrent VTE and had similar or fewer major haemorrhages.51,52 Apixaban
Apixaban is a lso a se lect ive and reversible direct oral factor X a i n h i b i t o r . 3 6 T h e A M P L I F Y study compared apixaban versus subcutaneous enoxaparin, followed by warfarin in the treatment of acute
VTE.53 For primary efficacy outcome of recurrent symptomatic VTE or VTE related death, apixaban was non-inferior to the conventional therapy. For major bleeding and the composite outcome of major bleeding and clinically relevant non-major bleeding, apixaban was superior compared to conventional therapy.53
Edoxaban
Edoxaban is an oral, selective Factor Xa inhibitor.36 Edoxaban is administered once daily and has a rapid onset of action.54 Edoxaban is approved by the USFDA for the treatment of DVT and PE following 5 to 10 days of initial parenteral anticoagulation therapy.55 In the Hokusai -VTE s tudy, edoxaban therapy for 3 to 12 months was compared with warfarin in patients with acute VTE, who had initially received heparin therapy for 5-10 days.54 In this study, it was found to be non- infer ior to warfar in for primary efficacy outcome of recurrent symptomatic VTE.54 The principal safety outcome of major or clinically relevant non-major bleeding was signif icantly less w i t h e d o x a b a n c o m p a r e d t o warfarin.54 Detailed pharmacological characteristics, drug interactions and study characteristics of all NOACs are elucidated in Table 8, 9 and 11, respectively.Drug interactions of NOACs:
N O A C s c a n a l s o i n t e r a c t w i t h o t h e r m e d i c a t i o n s . T h e r e c o m m e n d a t i o n s f o r d o s e adjustment/contraindications are given in Table 9.56
Monitoring NOACs Anticoagulant Effect
R o u t i n e m o n i t o r i n g o f anticoagulant effect of NOAC is not required. However, monitoring of NOAC anticoagulant effect might be useful in certain situations: (i) serious bleeding, (ii) emergency surgery or intervention, ( i i i ) suspected overdose,(iv) patients with renal or hepatic insufficiency, (v) potential drug-drug interactions. Monitoring assays for NOACs are summarized in Table 10.56

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 2016 13
Table 9: Drug interactions46,49,55,56,57
Dabigatran Apixaban Edoxaban RivaroxabanAmiodarone +12-60 % No PK data +40 % Minor effect (use
with caution if CrCl <50 ml/min
Antacids No dose adjustment No dose adjustment No dose adjustment No dose adjustmentAtorvastatin No dose adjustment No data yet No dose adjustment No dose adjustmentClarithromycin/Erythromycin
No dose adjustment No data yet Reduce NOAC dose by 50 %
+30-54 %
Cyclosporin/Tacrolimus
Not recommended No data yet + 73 % Extent of increase unknown
Digoxin No dose adjustment No data yet No dose adjustment No dose adjustmentDiltiazem No dose adjustment +40 % No data yet Minor effect (use
with caution if CrCl 15-50 ml/min
Dronedarone Contraindicated No PK/PD data; caution
Reduce NOAC dose by 50 %
Moderate effect but no PK/PD data: caution and try to avoid
HIV protease inhibitors
No data yet Strong increase No data yet Contraindicated
Ketoconazole, Itraconazole, Voriconazole, Posaconazole
Contraindicated Contraindicated Reduce NOAC dose by 50 %
Contraindicated
Carbamazepine, Phenytoin, Phenobarbitone, Rifampicin
Minus 66 % Minus 54 % Minus 35 % Up to minus 50 %
Quinidine +53 % No data yet +77 % Extent of increase unknown
Verapamil +12-180 % No PK data +53 % (Slow release)
Minor effect (use with caution if CrCl 15-50 ml/min
Contraindicated Dose reduction required
Consider dose reduction if ≥ 2 yellow is present
No dose adjustment required
Reduction in NOAC plasma levels. This may also constitute a contraindication for simultaneous use
Decrease in plasma level but not clinically relevant. Avoid if possible
Acute Treatment of Deep Vein Thrombosis
The efficacy and safety of NOACs have been evaluated in large phase III clinical trials versus warfarin or parenteral anticoagulation plus warfarin (Table 11, Figures 2 and 3) for treatment of acute venous thromboembolism. In these phase III clinical trials, NOACs have been found to be non-inferior in reducing recurrence VTE with less major and major plus clinically relevant non-major bleeding compared to warfarin or parenteral anticoagulant p l u s w a r f a r i n . 4 7 , 4 8 , 5 3 , 5 4 , 5 8 T h e recommendations for OACs in acute deep vein thrombosis treatment are summarized in Table 12.Bleeding Risk Assessment for Patients on Anticoagulation
Various risk stratification tools prepared by considering parameters such as age, comorbid conditions (e.g. renal disease, anemia, liver disease, hypertension, malignancy etc.), past history of bleeding, and anemia are available for assessment of bleeding risk in patients on anticoagulants.
HAS-BLED score: Major bleeds occurred in 11/537 patients (2.0%, 5.2/100 person years, 95% CI 2.8-9.2). Cumulative incidences of major bleeds were 1.3% (95% CI 0.1-2.5) in the non-high (HAS-BLED < 3) and 9.6% (95% CI 2.2-17.0) in the high-risk group (HAS-BLED ≥ 3), (p <0.0001 by Log-Rank test), with a HR of 8.7 (95% CI 2.7-28.4).58
A c u t e V T E p a t i e n t s w i t h a HAS-BLED score ≥ 3 points (Tables 13 and 14) are at increased risk of major bleeding. These results warrant for correction of the potentially reversible risk factors for major bleeding and careful International Normalized Ratio monitoring in acute VTE patients with a high HAS-BLED score.58
Extended Therapy in Deep Vein Thrombosis
T h e d u r a t i o n o f e x t e n d e d anticoagulant therapy in deep vein thrombosis depends on the risk of recurrent VTE (fatal/non-fatal) and bleeding complications. The RIETE
Table 10: Monitoring assays for NOACs57
Dabigatran Rivaroxaban Apixaban EdoxabanaPTT *TT, dTT
ECT
Anti-Fxa assays † ‡ †PT ¶ *INR
*Prolonged, but no known relationship to bleeding risk; †No data on threshold values for bleeding or thrombosis; ‡No data yet; ¶Influenced by rivaroxaban in a dose-dependent way with a close correlation to plasma concentrations only if Neoplastin is used. aPTT = activated partial thromboplastin time; dTT = diluted thrombin time; ECT = ecarin clotting time; FXa = Factor Xa; INR = international normalized ratio; PT = prothrombin time; TT = thrombin time
Table 11: Important clinical trials with NOACs
Dabigatran47,48 Rivoroxaban51,52 Apixaban53 Edoxaban54
Study name RE-COVER I and II
EINSTEIN–DVTEINSTEIN-PE
AMPLIFY Hokusai-VTE
Total number of patients
5128 8282 5400 8292
Dosage Dabigatran 150 mg twice daily for 6 months
Rivaroxaban: 15 mg twice daily for 3 weeks, followed by 20 mgonce daily for 12 months
Apixaban 10 mg twice daily for first7 days, followed by 5 mg twice daily for 6 months
Edoxaban 60 mg once daily, or 30 mg once daily (e.g., Crcl30 to 50 ml per minute or a body weight <60 kg) for 3 to 12 months

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 201614
Table 13: HAS-BLED risk criteria59
HAS-BLED risk criteria ScoreHypertension 1Abnormal renal or liver function (1 point each)
1 or 2
Stroke 1Bleeding 1Labile INRs 1Elderly (e.g. age >65 years) 1Drugs or alcohol (1 point each) 1 or 2INR, international normalized ratio. Hypertension’ is defined as systolic blood pressure >160 mmHg. Abnormal kidney function is defined as the presence of chronic dialysis or renal transplantation or serum creatinine ≥200 mmol/L. Abnormal liver function is defined as chronic hepatic disease (e.g., cirrhosis) or biochemical evidence of significant hepatic derange-ment (e.g., bilirubin 2 _ the upper limit of normal, in association with aspartate aminotransferase/alanine aminotransferase/alkaline phosphatase. 3 _ upper limit normal, etc.). Bleeding refers to previous bleeding history and/or predisposition to bleeding, e.g. bleeding diathesis, anemia, etc. Labile INRs refers to unstable/high INRs or poor time in therapeutic range (e.g. <60%). Drugs/alcohol use refers to concomitant use of drugs, such as antiplatelet agents, nonsteroidal anti-inflammatory drugs, or alcohol abuse, etc.
Table 14: Recommendation for bleeding risk assessment for patients on OAC
We recommend the use of HAS-BLED score for assessing the risk of bleeding in anticoagulated DVT patients.
Fig. 2: Efficacy outcome of NOACs RCTs in the management of acute VTE47,48,53,54,58
registry data of 41,826 patients with mean duration of anticoagulation therapy for 7.8 months showed 16.1% case fatality rate (CFR) of recurrent VTE during first three months compared, to 2.0% beyond this period while the case fatality rate (CFR) of major bleeding was 20.2% during the first three months, compared to 18.2% beyond this period. These f indings suggest reduction in CFR of recurrent VTE over time with no major change in bleeding risk with continued use of anticoagulant.59 In one meta-analysis of seven randomized trials, 2925 patients with a first episode of VTE who received different durations of anticoagulation were followed up for 24 months after stopping the anticoagulation therapy.60 This study showed a higher recurrence of VTE if anticoagulation was stopped at 1.0 or 1. 5 months compared with at 3 months or later, and similar recurrence of VTE if anticoagulation was stopped at 3 months compared with at 6 months or later.61 Current
A C C P 1 0 t h ( A m e r i c a n C o l l e g e of Chest Physicians) guidelines recommend long term (at least 3 months) anticoagulant therapy for patients with DVT (proximal or d is ta l ) or PE over no such therapy.30 Decision to further extend anticoagulant therapy should be at physician’s discretion based on the benefit versus the risk of its continuation considering patients’ profile.Deep Vein Thrombosis Recurrence Risk Assessment
The assessment of risk of VTE recurrence is important because of its potential impact on the duration of anticoagulant treatment. The VTE recurrence risk is more in unprovoked cases compared to those with provoked risk factors, and the duration of treatment is longer in the former cases compared to the later.62
Three scores have been proposed to identify patients who carry a high recurrent risk and require extended anticoagulant treatment, the HERDOO2, the DASH score,
and the Vienna prediction model (Table 15). In all , male sex and elevated D-dimer levels have been identified as important risk factors for recurrence. However, there are some differences among these scoring systems. The HERDOO2 score inc ludes D-dimer leve ls measurement during anticoagulation and age more than 65 as a risk factor for recurrence, whereas the DASH score considers age less than 50 as a higher risk.62 The Vienna Prediction Model is a simple and useful scoring system to assess the recurrence risk in patients with a first unprovoked VTE. It was first validated on a prospective cohort study of 929 patients with a first unprovoked VTE. In this study, a total of 176 patients (18.9%) had recurrent VTE. The risk of recurrence was higher in men vs. women, with proximal DVT and PE vs. distal DVT, and with elevated levels of D-dimer after
Table 12: Recommendations for OACs in acute deep vein thrombosis treatment
• In patients with proximal DVT, at least 3 months anticoagulant therapy is recommended over no therapy and use of NOACs (dabigatran, rivaroxaban, apixaban, or edoxaban) is suggested over VKA therapy.
• In case VKA therapy is considered, concomitant (on the same day) parenteral anticoagulation is recommended in the initial phase of DVT treatment for at least 5 days or till INR >2.
• We recommend percentage TTR (Time in Therapeutic Range) of >60 % in case of VKA therapy.
• If dabigatran or edoxaban is considered, parenteral anticoagulantion for 5-10 days should be used in the initial DVT treatment, with no overlap.
• In case of isolated distal DVT of the leg, if the patient is decided to be treated with anticoagulant, therapy should be given for 3 months.
Symptomatic Recurrent VTE
STUDY
RE-COVER I & II
EINSTEIN
AMPLIFY
Hokusai-VTE
OR(95% CI)
1.09(0.76-1.57)
0.89(0.66-1.19)
0.84(0.60-1.18)
0.89(0.70-1.13)
0.10 0.50 1.0 1.5 5.0<- NOAC Better Warfarin Better ->

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 2016 15
Fig. 3A: Safety outcomes of NOACs RCTs in the management of acute VTE47,48,53,54,58
Fig. 3B: Safety Outcomes of NOACs RCTs in the management of acute VTE47,48,53,54,58
discontinuation of anticoagulation, Based on this study, a nomogram to compute the risk of recurrence has been developed.50 The risk factors along with their assigned points are given in Table 15. The total score is calculated by adding points assigned to each variable which is then mapped against expected cumulative recurrence risk at 12 and 60 months.63
It has been validated externally e n r o l l i n g 9 0 4 o l d e r p a t i e n t s (median age , 68 years ) where it underestimated the observed cumulative recurrence rates at 12 months . 64 The updated Vienna Prediction Model is an improved vers ion of the or iginal Vienna Prediction Model which allows prediction of recurrence at several
different time points after stopping anticoagulation.65 It was developed in a prospect ive cohort of 553 patients with unprovoked VTE with the same clinical parameters (ie, sex, location of VTE, and a quantitative D-dimer level determined by ELISA between 3 weeks and 15 months after discontinuation of anticoagulation) to estimate the risk of recurrent VTE up to 60 months.65
NOACs in Extended Therapy for Deep Vein Thrombosis Prevention
L o n g - t e r m a n t i c o a g u l a n t treatment is effective in the treatment of acute VTE. However, the risk of recurrence remains once the therapy is discontinued. The risk of recurrence can be 5-10 % during the first year.51 Extended therapy with anticoagulants is an option
to reduce risk of recurrence. The extension studies have proved efficacy and safety of NOACs in patients with VTE. All NOACs have been evaluated for extended therapy versus placebo.66–68 They were found to be superior to placebo in reducing the risk of primary efficacy end point of symptomatic recurrent VTE or death from VTE. The incidence of major bleeding was low with all NOACs. However as expected all the NOACs significantly increased the risk of clinically relevant non major bleeds and total bleeds in comparison to placebo. Additionally, dabigatran (150 mg BD) was compared with dose adjusted warfarin (INR 2-3) for extended therapy for VTE prevention in 2866 patients with a longest period of treatment up to 36 months. In this study, less major bleeding, significantly less major or clinically relevant bleeding and signif icantly less any bleeding events were seen with dabigatran with non-inferior rates of VTE and VTE related deaths compared to dose adjusted warfarin.66 One systematic review and network meta-analysis of efficacy and safety of oral anticoagulants and antiplatelets for secondary prevention of VTE showed that oral anticoagulants are more efficacious and safe compared to aspirin or observation alone (Table 16).69 The recommendations for extended therapy in deep vein thrombosis are summarized in Table 17.
Switching between Anticoagulant Regimens
Switching between dif ferent anticoagulant regimens should consider two important things:
Table 15: Vienna prediction model64
Parameter PointsMaleFemale
60 points0 points
Proximal DVT Distal DVT PE
70 points0 points90 points
D-dimer level (0-100 points based on the level)
100 mcg/l- “0” points2000mcg/l- “100” points
*Patients at low risk [rate of recurrence of 4.4% (95% CI 2.7–6.2%)] when points (according to nomogram) are 180 or less.64
Major Bleeding
STUDY
RE-COVER I & II
EINSTEIN
AMPLIFY
Hokusai-VTE
OR(95% CI)
0.60(0.36-0.99)
0.54(0.37-0.79)
0.31(0.17-0.55)
0.84(0.59-1.21)
0.10 0.50 1.0 1.5 5.0<- NOAC Better Warfarin Better ->
Major and Clinically Relevant Non-Major Bleeding
STUDY
RE-COVER I & II
EINSTEIN
AMPLIFY
Hokusai-VTE
OR(95% CI)
0.56(0.45-0.71)
0.93(0.81-1.06)
0.44(0.36-0.55)
0.81(0.71-0.94)
0.10 0.50 1.0 1.5 5.0<- NOAC Better Warfarin Better ->

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 201616
Fig. 4: Switching between anticoagulant regimen36
Table 17: Recommendations for extended therapy in deep vein thrombosis
• At least 3 months treatment with anticoagulant is recommended in patients with venous thromboembolism due to first provoked event while extended therapy is required for patients with a first unprovoked event.
• The risk of ongoing anticoagulation therapy for extended duration should be assessed after every 3 months of therapy to look at the benefit risk profile.
• An unprovoked DVT of the leg requires anticoagulation for at least 3 months after which the patient should be evaluated for the risk-benefit ratio of extended anticoagulant therapy.
• If the first VTE is an unprovoked proximal DVT of the leg with low or moderate bleeding risk, then extended anticoagulant therapy is suggested.
• If the first VTE is an unprovoked proximal DVT of the leg with high bleeding risk, then at least 3 months of anticoagulant therapy is suggested with close monitoring.
• In patients with second unprovoked VTE with low bleeding risk, extended anticoagulant therapy over three months is recommended while for moderate bleeding risk, extended anticoagulant therapy over three months is suggested with close monitoring.
( 1 ) M a i n t e n a n c e o f o p t i m a l a n t i c o a g u l a n t e f f e c t , a n d ( 2 ) Minimizing the bleeding risk at the same time.36 Switching to and from VKA to NOAC
Switching from VKA to NOAC should start with discontinuation of VKA followed by check INRs. Once the INR reaches < 2, NOAC should be started immediately. For INR >2, consider actual INR value and half-life of VKA to calculate the approximate time for INR to
reach below threshold of 2 after which NOAC can be initiated.57 While switching from a NOAC to warfarin, consider bridging with a short-acting parenteral agent (rivaroxaban, apixaban)49,56 or a lower dose (edoxaban)55 of the NOAC. For switching from dabigaran to VKA check creatinine clearance first. If it is ≥50 ml/min, start VKA 3 days before discontinuation of dabigatran, and if CrCL is ≥30-<50 ml/min, start VKA 2 days before the
discontinuation of dabigatran.46
Switching to and from Parenteral Anticoagulant to NOAC
NOAC should be initiated up to 2 h before the next dose of the parenteral agent when transitioning from a parenteral agent to a NOAC and vice versa. The prescribing information of each of the NOACs describes the strategy for switching between these therapies. Figure 4 summarizes the transition between different treatment regimens.36
Approach to pharmacological management of DVT is shown in Figure 5.
Complications of Deep Vein Thrombosis
Complications of DVT include recurrence, pulmonary embolism (i.e. proximal DVT of leg), death due to massive pulmonary embolism, post thrombotic syndrome, chromic t h r o m b o e m b o l i c p u l m o n a r y hypertension (i.e. survivors of acute PE).70,71 Recurrence of VTE may occur in about one third population wi th a decade . 72 Overa l l , VTE results in more than 100,000 deaths every year.73 Pulmonary embolism can lead to three month all-cause mortality rate of up to 30%.73 It is generally believed that proximal DVT in the leg is associated with an increased r isk for PE while calf DVT with post thrombotic syndrome.74 The seriousness of calf DVT lies in the fact that 15- 25% of them may progress to become p r o x i m a l D V T. 7 4 S y m p t o m a t i c chronic thromboembolic pulmonary hypertension (CTEPH) is a common and serious complication of PE which may occur in about 4% patients at 2 years.71
Post-thrombotic Syndrome
Post-thrombotic Syndrome is often ignored, but an important complication of DVT seen in about 30% of patients. Chronic pain and swelling in the affected extremity are the typical clinical features of the post-thrombotic syndrome, formerly known as post-phlebitic syndrome. Post-thrombotic syndrome results in dermatological changes, venous stasis and sometimes venous ulcer and
Table 16: Absolute risk of recurrent VTE and major bleeding per 100 patients treated each year
Placebo or Observation
Vitamin K antagonist
(dose adjusted)
Dabigatran(150 mg BD)
Rivaroxaban(20 mg OD)
Apixaban(5 mg BD)
Aspirin(100 mg/
day)
Absolute risk of recurrent VTE
10/100 1/100 2/100 2/100 2/100 7/100
Absolute risk of major bleeding
1/100 2/100 1/100 6/100 1/100 1/100
Stop VKAs Check INR
INR <2
INR >2.5
Start NOAC
Based on the INR value and t1/2 ofthe VKA (acenocoumarol t1/28-14 hrsand warfarin t1/2 36-42 hrs) ,calculate the likely time required todrop INR value below <2.5
Continuous infusion of UFH to NOACsParenteral to NOACs
*without overlapping
Start NOAC at the time of
discontinuation of continuous infusion
Start NOAC up to 2 hours before next parenteral drug
dose*

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 2016 17
Result
Positive?
Clinical suspicion of DVT
Determine clinical pretest probability
(Well’s Score)
DVT likely(Well’s Score ≥2)
DVT unlikely
(Well’s Score <2)
D-Dimer test
Perform duplex ultrasound
(with compression)
DVT excludedResult
Positive?
DVT confirmed
Repeat duplexUltrasound (with compression) in 1 week
Parenteral anticoagulation≥5 days
Oral anticoagulation
f/b Vit. K Antagonist- Warfarin, acenocumarol (INR 2-3) for at least 3 months
f/b Dabigatran etexilate (150 mg BID) for at least 3 months
f/b Edoxaban 60mg OD for at least 3 months
Rivaroxaban 15mg BID for 21 days followed by 20mg OD for at least 3months
Apixaban 10mg BID for 7 days followed by 5mg BID for at least 3 months
YesNo
Yes
No
Perform duplex ultrasound (with compression)
DVT confirmed
Positive
Negative
DVT excluded
Negative
D-Dimer test
Positive
Fig. 5: DVT Management Protocol21,30

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 201618
leads to impaired quality of life.73,75 It has been estimated that about half of the people with DVT develop post-thrombotic syndrome.72 Deep vein thrombosis should be prevented by pharmacologic or mechanical thromboprophylaxis in high risk patients to avoid development of PTS. The recommendations for the management of PTS (post-thrombotic syndrome) are summarized in Table 18.
Interventions in Deep Vein Thrombosis TreatmentSystemic Thrombolysis for Deep Vein Thrombosis Treatment
Intravenous streptokinase and recombinant tissue plasminogen a c t i v a t o r ( r t - PA) h a v e b e e n studied in the treatment of DVT.76 T h r o m b o l y s i s c a n r e d u c e t h e long-term complications like post-thrombotic syndrome.77 An updated C o c h r a n e a n a l y s i s e x a m i n i n g thrombolysis and anticoagulation versus anticoagulation for acute DVT has confirmed that the use of thrombolytics plus anticoagulation c a n r e s u l t i n c o m p l e t e c l o t lysis or better improvement in venous patency more often and significantly less occurrence of post-thrombotic syndrome compared to anticoagulation alone; however, s i g n i f i c a n t l y m o r e b l e e d i n g complications resulted from this therapy.78 Streptokinase infusion is not commonly used in the clinical practice because of higher bleeding complications.76
Catheter Directed Thrombolysis for Deep Vein Thrombosis Treatment
Catheter-directed thrombolysis (CDT) receives greater acceptance w i t h t h e t r e a t i n g p h y s i c i a n s a s c o m p a r e d t o i n t r a v e n o u s thrombolysis78 and there has been a
steady rise in its use in the United States for the treatment of inferior vena cava thrombosis. The data from the Nationwide Inpatient Sample Database (2005 to 2011) comparing CDT plus anticoagulation versus anticoagulation alone showed no significant difference in mortality between two groups. However, CDT group had more bleeding events and resource uti l ization compared to anticoagulation.79 A recent study by Enden et al has shown that long term outcome after CDT plus anticoagulation in acute i l io-femoral deep vein thrombosis as measured by PTS at 24 months and ilio-femoral patency at 6 months was significantly better than conventional therapy.80 Allergy may also occur in some patients.81
Catheter directed thrombolysis can be performed in patients having no contraindications for treatment.81 Patients with extensive thrombosis, for e.g., ilio-femoral thrombosis have the most to gain in terms of preserving venous function.78 Patient selection is important to provide maximum benefit and to keep low risk of bleeding in patients.78 From an Indian perspective, catheter-directed thrombolysis has limited acceptance due to perceived risks, time required for lysis, and cost involved. Catheter assisted thrombus removal should be done only by an expert in the presence of resources for acute PE associated with hypotension and high risk of bleeding risk, failed systemic thrombolysis, or severe shock likely to cause death within hours.78
Mechanical Thrombectomy for Deep Vein Thrombosis Treatment
M e c h a n i c a l t h r o m b e c t o m y requires less time for clot lysis compared to catheter directed thrombolysis.82 In recent times use
of mechanical thrombolysis as endovascular therapy is increasing. However, it also requires expertise and resources. There are no full-fledged sufficiently powered studies available to provide evidence for the use of mechanical thrombectomy for deep vein thrombosis.IVC Filters for Deep Vein Thrombosis Treatment
The use of for vena cava filters in treatment of VTE is controversial. In the absence of strong evidence of efficacy in preventing DVT, high cost and difficulty in predicting which pat ients might benef i t , prophylactic IVC filters cannot be recommended. However , some selected patients in very high-risk category might be benefited with optional IVC filters.83 In patients with absolute contraindications for the use of anticoagulation and a high risk of VTE recurrence, IVC filters might be tried. 84 Recommendations for intervent ions in deep vein thrombosis treatment are given in Table 19.
Compression Devices for Deep Vein Thrombosis Treatment
Three types of compress ion devices are available for prevention of DVT. Compression stockings with graduated pressure (highest at the ankle and lower proximally) prevent venous stasis due to pressure d i f ference . Al ternate inf la t ion and deflation of the cuffs used in intermittent pneumatic compression are another type of compression devices to prevent venous stasis. The third type of compression device is mechanical foot pumps, which by intermittent plantar compression (IPC) increases the flow of blood in leg veins (Table 20).85
Upper Extremity Deep Vein Thrombosis
U p p e r e x t r e m i t y d e e p ve i n thrombosis (UEDVT) comprises 5-10% of VTE. It is either due to primary cause (unprovoked with or without thrombophilia, effort-related and thoracic outlet syndrome)
Table 18: Recommendations for management of post-thrombotic syndrome75
Patient category Recommendations/suggestionsPatients with DVT Routine use of elastic compression stockings (ECS)
is not recommended for prevention of PTS Leg swelling due to acute DVT-related Trial of ECS may be given. Established PTS Daily use of 20-30 mm Hg knee-length ECS
(stronger pressure stockings, if ineffective)Moderate-to-severe PTS with inadequate control of symptoms with ECS
Intermittent compression devices/pneumatic compression sleeve
Patients who can tolerate exercise Supervised exercise training program for >6 months may be tried

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 2016 19
and secondary cause (provoked b y c e n t r a l v e n o u s c a t h e t e r s , pacemakers,or cancer ) . UEDVT usually occurs in subclavian, axillary or brachial veins and may involve brachiocephalic vein, superior vena cava or internal jugular vein. UEDVT may lead to complications l ike symptomatic PE (5%), recurrence (8% at 5 years) and PTS of the arm (20%) (Table 21).30,86
Superficial Vein Thrombosis
Superficial veins of the upper extremity include cephalic vein, basilic vein, median cubital vein, accessory cephalic vein, superficial median vein of the forearm, palmar venous plexus , pa lmar dig i ta l veins whereas superficial veins of the lower extremity include great
saphenous vein, small saphenous vein, dorsal venous arch. Superficial vein thrombosis (SVT) characterized by thrombosis and inflammation in a superficial vein most commonly affects the great saphenous vein, sometimes small saphenous vein and rarely upper extremity veins. T h e e t i o l o g y o f S V T i n c l u d e s trauma or haematolgic changes. The complications of SVT include suppuration, thrombosis at different sites, hypercoagulable state87 and increased risk of DVT and PE.88
The treatment of SVT is directed at alleviation of pain and inflammation and prevention of complications. The treatment approach includes removal of predisposing factors, symptomatic treatment with anti-inflammatory drugs, and warm compress ion . Super f i c ia l ve in thrombosis close to saphenofemoral or saphenopopliteal junction may require anticoagulant treatment while varicose veins and reflux may require surgery.86 In a randomized double blind study fondaparinux at a dose of 2.5 mg S.C. once a day for 45 days in patients with acute superficial vein thrombosis of lower extremity was found to be effective with serious side effects (Figure 6).89
Special Population and Deep Vein Thrombosis Elderly Patients
Age is an important risk factor for VTE and VTE recurrence. The risks for DVT and PE are 4 to 6 times higher in patients above 70 years old compared to younger patients,90,91 and this risk doubles with each decade of aging. 92 Importantly, e lder ly pat ients a lso exhibi t a higher case-fatality rate due to more frequent fatal PE (odds ratio in patients aged >75 years 2.31)93 and coexistent comorbidities. The diagnosis of VTE in the elderly also poses particular challenges, as an atypical presentation and a reduced sensitivity and specificity of both clinical scoring systems and laboratory parameters may impede a timely diagnosis.94In patients treated with warfarin, the rate of VTE recurrence was higher in patients aged ≥75, with a pooled risk ratio of
Table 19: Recommendations for interventions in deep vein thrombosis treatment
Interventions RecommendationsSystemic Thrombolysis
• Routine use of systemic thrombolysis for treatment of acute proximal DVT is not recommended.
• We suggest use of anticoagulant therapy alone over systemic thrombolysis in patients with acute proximal DVT.
• Intravenous thrombolysis can be considered in the following:- Iliofemoral DVT- Symptoms <14 days- Good functional status- Life expectancy of ≥1 year, and- Low risk of bleeding
Catheter Directed Thrombolysis
• Routine use of Catheter Directed Thrombolysis is not recommended for treatment of acute proximal DVT..
• We suggest use of anticoagulant therapy alone over Catheter Directed Thrombolysis in patients with acute proximal DVT.
• Catheter Directed thrombolysis can be considered in the following :- Iliofemoral DVT- Symptoms <14 days- Good functional status- Life expectancy of ≥1 year, and- Low risk of bleeding
• Catheter directed thrombolysis should be done only by experienced interventionists and in the facilities where resources for management of complications are available
Mechanical Thrombectomy
• Routine use of Mechanical thrombectomy is not recommended for treatment of acute proximal DVT.
• We suggest use of anticoagulation therapy alone over mechanical thrombectomy in patients with acute proximal DVT.
• Mechanical thrombectomy can be considered in the following :- Iliofemoral DVT- Symptoms <7 days- Good functional status- Life expectancy of ≥1 year, and- Resources and expertise are available
IVC filters • In patients with acute DVT treated with anticoagulants, use of an inferior vena cava (IVC) filter is not recommended.
• We recommend use of an IVC filter in patients with acute proximal DVT of the leg and contraindication to anticoagulation.
Table 20: Recommendation for compression devices for deep vein thrombosis treatment
In patients with acute DVT of the leg, routine use of compression stockings to prevent PTS is not suggested.
Table 21: Recommendation for upper extremity deep vein thrombosis treatment
We suggest anticoagulant therapy alone over thrombolysis in patients with acute UEDVT that involves the axillary or more proximal veins.

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 201620
1.47 compared to warfarin-treated patients <75 years. In contrast , patients ≥75 treated with NOACs did not have an increased recurrence compared to younger patients. Thus, in a meta-analysis of all patients ≥ 75, NOACs were found to be more effective compared to warfarin.95
Patients with Heparin-Induced Thrombocytopenia
Heparin-induced thrombocyto-penia (HIT) is a clinic-pathological syndrome,96 its diagnosis is based on characteristic clinical events and concurrent laboratory detection of HIT antibodies in the setting of
recent heparin therapy. As a result of which there could be increased thrombin generation, which may be associated with arterial or venous thrombosis.96 Thrombocytopenia that typically occurs 5 to 10 days after heparin exposure, though it may develop more rapidly in patients previously exposed to heparin within the preceding 100 days.96 A decline of 50% from the basel ine plate let count should raise clinical suspicion for HIT.(96)
In patients receiving heparin for treatment, both antibody formation and clinical HIT are more common
with UFH than LMWH.97 Alternate anticoagulation should be con-sidered if a patient develops HIT. LMWH is not an optimal alternative to UFH because of a high risk of clinically significant cross-reactivity with the HIT antibodies. Warfarin may cause micro thrombosis in patients with HIT. These patients typically present with an interna-tional normalized ratio (INR) greater than 4, which corresponds to severe protein C depletion. Initiation of warfarin should be postponed until substantial platelet recovery. Prefer-ably, warfarin should not be started before the platelet count exceeds 150 x 109/L.26,97 If warfarin has already been started, vitamin K should be given.98
Thrombophilia, Anti-phospholipid Antibody Syndrome, and Deep Vein Thrombosis
Thrombophilia is a known risk factor for the development of VTE. In the MAISTHRO registry, out of 1490 patients analysed at the time of first VTE, 50.1% patients had at least one thrombophilia.99 The hereditary thrombophilia was less common in elderly people compared to younger population. Thrombophilia was more commonly o b s e r ve d i n u n p r o v o k e d V T E compared with r isk-associated VTE (57·7% vs. 47·7%; P = 0·001).99 positivity for anti-phospholipid antibody syndrome (APLAS) are at higher risk for development of thrombotic events.99 At the moment, the best anticoagulation regimen for these patients is unknown. Aspirin use as an add-on to low dose warfarin does not provide benefits while short term therapy with warfarin is less useful.100 In patients with APLAS and DVT, long-term warfarin (INR 3.0-4.0) may seem to be superior compared to warfarin (INR 2.0-3.0).100 A post-hoc subgroup analysis of thrombophilia patients within the RE-MEDY trial showed that efficacy of dabigatran vs dose adjusted warfarin was not affected by the presence of thrombophilia at baseline.101 Patients with Renal Impairment
Renal impairment was associated with an increased risk of recurrence
Fig. 6: Superficial vein thrombosis management protocol86
RECOMMENDATION FOR MANAGEMENT OFSUPERFICIAL VEIN THROMBOSIS OF LOWER EXTREMITY
Patient presents with signs/symptoms of superficial vein thrombosisObtain duplex ultrasound to confirm diagnosis
Treat according to therecommendations for
Treatment of DVT
Duplex Positive for DVTDuplex Negative for DVT
and Positive for SVT
No to all
Yes to any
YesNo
Treat with VTE Prophylaxis
Superficial thrombus is > 5 cm and / orwithin 3-5 cm from spheno-femoral junction
• Fondaparinux 2.5 mg SQ daily (unless contraindicated) x 45 days (preferred unless contraindicated by CrCl < 50 ml/min)
• LMWH SQ daily for 45 days
1. Repeat duplex scan at 7-10 days and
treat according to the recommendations
for treatment of DVT if DVT or significant
extension of SVT is detected.
2. Consider oral non-steroid anti-
inflammatory agent for symptom relief
3. Consider referral to Vascular Surgery if
varicose
Through shared decision
making, patient prefers
VTE Prophylaxis
Through shared decision
making, patient prefers
repeat duplex strategy
Review risk of VTE vs risk / benefit
of prophylactic anticoagulation
Evaluate for VTE Risk Factors
History of VTE Known Thrombophilia
Male Pregnancy
Chronic venous insufficiency
Recent surgery, trauma or injury
Recent hospital admission
Active malignancy ± active cancer treatment
Ongoing use of oral contraceptives or
hormone replacement therapy
Absence of varicose veins

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 2016 21
53% reduction in recurrent VTE with LMWH with minor difference in the rate of major bleeding.47,103
Data on the use of NOACs in cancer patients receiving chemotherapy is limited. The pooled data from two large randomized trials in acute VTE (RECOVER and RECOVER-II showed similar benefits with dabigatran as warfarin. No significant difference in efficacy was seen for cancer at baseline or diagnosed during the study.51 Patients taking Anti-platelet Agents
The NOAC VTE treatment trials a l lowed low-dose concomitant aspirin, and dual antiplatelet therapy was al lowed in the dabigatran and rivaroxaban trials. The rate of low-dose aspirin use ranged from 8 to 14 % for dabigatran, rivaroxaban, and apixaban, and was not reported in the edoxaban trial.47,48,51–54 The receommendations for deep vein thrombosis treatment in special population are summarized in Table 22.Deep Vein Thrombosis and Pregnancy
The risk of VTE in pregnancy is five to ten times higher than non-pregnant women of similar age group. During the postpartum period the risk of VTE is even more (15-35 times higher ) compared to non-pregnant women of the same age. The risk of VTE is greatest during the first 3 to 6 weeks after delivery.105 Overall, the rate of VTE in pregnancy ranges between 0.5–2.2 per 1000 deliveries based on different population studies and can result in significant maternal morbidity and mortality.105–112 Treatment and prevention of deep vein thrombosis in pregnancy is of concern due to two reasons. First, the risk involved for mother and the fetus due to both the VTE and drugs used in i ts management and secondly, absence of high quality pregnancy specific data causing difficulty in providing recommendations. The recommendations are mostly based on observational studies and data extrapolated from non-pregnant patients. Vitamin K antagonists cross the placenta and can cause t e r a t o g e n i c i t y , m i s c a r r i a g e , fetal bleeding, and neurological
in the warfarin-arms of all trials. Although not significant in most individual trials, pooled data show a s ignif icant 71% risk increase in patients with reduced renal clearance. A similar increase in recurrence was noted in patients with reduced renal function treated with apixaban or rivaroxaban, but not in patients treated with dabigatran or edoxaban. A pooled analysis showed no significant difference in relative efficacy between NOACs and warfarin in patients with renal dysfunction.102
Patients with Active Cancer
Malignancy is well known risk fac tor for the development o f VTE. Different factors including
h y p e r c o a g u l a b l e s t a t e d u e t o interaction between tumor and host cells, venous stasis, endothelial dysfunction, age of the patient and treatment related components contribute to the risk of VTE. The risk of VTE in active cancer is up to 8-fold higher compared to general population. VTE adversely affect the survival outcome in patients with cancer.103
A landmark study comparing dalteparin with an oral anticoagulant therapy in malignancy showed 52% reduction in recurrent VTE without major differences in the rates of major bleeding or mortality.104 A recent Cochrane review of seven randomized clinical trials comparing LMWH versus VKA therapy showed
Table 22: Recommendations for deep vein thrombosis treatment in special population
Special Population RecommendationsElderly (≥ 75 Yrs) Based on the currently available evidence, we suggest the use of NOACs
over VKA therapy in patients’ ≥75 years.HIT (Heparin Induced Thrombocytopenia)
In patients with prior history of HIT who have DVT and normal renal function, we suggest the use of fondaparinux as an initial anticoagulation therapy until transition to VKA therapy.
Thrombophilia The screening for hereditary thrombophilia in VTE patients should be done based on age and other risk factors.Thrombophilia workup may be done for
DVT occurring at a younger age (i.e. < 45 years)Unprovoked DVT Recurrent DVT Thrombosis at an unusual site (splanchnic, sinus/cerebral, or renal veins) Unusually extensive spontaneous DVT Family history of DVT
Thrombophilia work up to be doneActivated protein C resistanceProthrombin gene mutationsProtein S, C, and antithrombin III deficiencyAntiphospholipid antibodiesFactor V Leiden mutationHomocysteine levels
Renal impairment VKA is the preferred anticoagulant for patients with renal disease and creatinine clearance <30 mL/min. NOACs and LMWH are contraindicated in patients with severe renal insufficiency (creatinine clearance <30 mL/min). Assess renal function of the patient before starting NOACs.
Hepatic impairment Avoid NOACs in moderate to severe hepatic dysfunction.Active Cancer In cancer patients having DVT of the leg, long-term (first 3 months)
anticoagulant therapy is recommended.LMWH is preferred over VKA or NOACs (dabigatran, rivaroxaban, apixaban or edoxaban) in cancer associated thrombosis. Extended anticoagulant therapy is recommended in patients without high bleeding risk.
Concomitant antiplatelet use
We suggest avoiding concomitant antiplatelet therapy during NOAC therapy unless the potential benefit clearly justifies the increased bleeding risk.

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 201622
Table 23: Recommendations for treatment of deep vein thrombosis during pregnancy/peripartum/brest feeding
Recommendations for treatment of DVT during pregnancy• Women of child bearing potential should avoid pregnancy during treatment with
NOACs (dabigatran, rivaroxaban, apixaban, edoxaban) and Vitamin K antagonists, and if pregnancy is planned, use appropriate contraception or switch over to LMWH/UFH as early as possible.
• When pregnant, NOACs (dabigatran, rivaroxaban, apixaban, edoxaban) should be used only if the potential benefit outweighs the potential risk to the mother and fetus.
• Vitamin K antagonists should be avoided during pregnancy because of their known potential risk to the mother and fetus. If pregnant, discontinue VKA and switch to LMWH/UFH before the 6th week of gestation or consider for medical termination of pregnancy according to the potential risk to the mother and fetus.
• LMWH (dalteparin 200 units/kg once daily or 100 units/kg 12 hourly; tinzaparin 175 units/kg once daily; enoxaparin 1 mg/kg 12 hourly; nadroparin 86 units/kg 12 hourly or 171 units/kg once daily) is the drug of choice for treatment and prevention of VTE in pregnancy and postpartum period, except in cases with history or presence of heparin induced thrombocytopenia, or significant kidney dysfunction. In patients with significant kidney dysfunction (GFR < 30 ml/min), UFH is preferred.
• Danaparoid or fondaparinux may be used in pregnant women with severe skin allergies to UFH or LMWH or history or presence of heparin induced thrombocytopenia.
• Outpatient treatment can be considered in clinically stable patients and those having good cardiorespiratory reserve, no major risk factors for bleeding and good social support with easy access to medical care.
Recommendations for treatment of DVT during peripartum period • Anticoagulant therapy should be discontinued at the onset of spontaneous labor.• LMWH should be discontinued at least 24 hours before the expected time of epidural
analgesia or delivery in case of planned delivery.• Intravenous UFH should be discontinued at least 4-6 hours before the expected time of
epidural analgesia or delivery with check aPTT in case of planned delivery.• Subcutaneous UFH should be discontinued preferably 24 hours before the expected time of
epidural analgesia or delivery with check aPTT in case of planned delivery.• LMWH/intravenous UFH may be initiated/reinitiated 24 hours after delivery or as soon as
haemostasis is achieved.Recommendation for treatment of DVT in breastfeeding Women• NOACs (dabigatran, rivaroxaban, apixaban, edoxaban) should be avoided in breastfeeding
women, and other alternative anticoagulants i.e. LMWH/UFH/warfarin/acenocoumarol should be considered.
Recommendation for duration of anticoagulation therapy for DVT in pregnancy and postpartum period • Anticoagulation therapy should continue throughout pregnancy and at least 6 weeks
postpartum. Decision to further continue anticoagulation therapy should be based on risk of recurrent VTE versus risk of bleeding.
Table 24: Recommendations for anticoagulation therapy in deep vein thrombosis associated with ART
• No routine thromboprophylaxis for women undergoing ovulation induction needed.• We recommend thromboprophylaxis with LMWH for woman at increased risk (e.g.
previous h/o VTE, h/o asymptomatic thrombophilia, family history of symptomatic thrombophilia and pregnancy related risk factors) of VTE undergoing ART at the time of ovarian stimulation. It has to be stopped 24-48 hrs prior to OPU (oocyte pick-up) and restarted 24 hrs after OPU (oocyte pick-up).- In case pregnancy ensues – then continue for first 6 weeks of pregnancy.- In absence of pregnancy – can be stopped at a negative UPT (Urine Pregnancy Test).
• In case of severe OHSS due to ART, we recommend thromboprophylaxis with LMWH for at least 8-12 weeks after the resolution of the syndrome.
• We recommend therapeutic anticoagulation for a minimum 3 months for woman with VTE in association with the use of ART who do not conceive in that cycle.
• We recommend therapeutic anticoagulation for a minimum 3 months for woman with VTE in association with the use of ART who conceive in that cycle. After which anticoagulation intensity can be decreased to intermediate or prophylactic dose for the remainder of the pregnancy and for at least 6 weeks postpartum.
developmental defects. Pregnant women were excluded from all
non-vi tamin K antagonist oral anticoagulants (e.g. dabigatran,
rivaroxaban, apixaban, edoxaban) clinical trials.46,49,55,56 These agents are likely to cross the placenta and their risks during pregnancy use are not known.46,49,55,56 Fondaparinux crosses placenta in small amount, and its use during pregnancy has been found to be safe.113–120LMWH, UFH and danaparoid do not cross the placenta and have a better safety profile in pregnancy.121–124 UFH can be used during pregnancy for both prevention and treatment o f t h r o m b o e m b o l i s m t h o u g h LMWH has a better safety profile than UFH in such patients.125 The recommendations for treatment of deep vein thrombosis during pregnancy / peripartum / breast feeding are summarized in Table 23.Assisted Reproductive Technology and Deep Vein Thrombosis
T h e r e i s l i m i t e d d a t a o n epidemiology and management of VTE related to Assisted Reproductive Technology (ART). According to a retrospective analysis of data from 2748 in vitro fertil ization (IVF) cycles, the risk of thromboembolism in women undergoing IVF is 0.11% per cycle. And in the presence of OHSS (Ovarian Hyper stimulation Syndrome), the risk of thrombosis is as high as 0.78% per cycle involving upper extremity in majority of cases.126,127 The VTE risk in OHSS ( O v a r i a n H y p e r s t i m u l a t i o n Syndrome) may remain for weeks or months even after the resolution of the OHSS. In women with high risk of VTE, thromboprophylaxis might be started at the start of ovarian stimulation, and continued till the completion of ART. In case pregnancy occurs, thromboprophylaxis should be continued during the antepartum period. If the woman undergoing IVF does not have risk factors for the development of VTE, routine thromboprophylaxis is not required. However if she develops severe OHSS, thromboprophylaxis should be used.127 The recommendations for anticoagulation therapy in deep vein thrombosis associated with ART are summarized in Table 24.
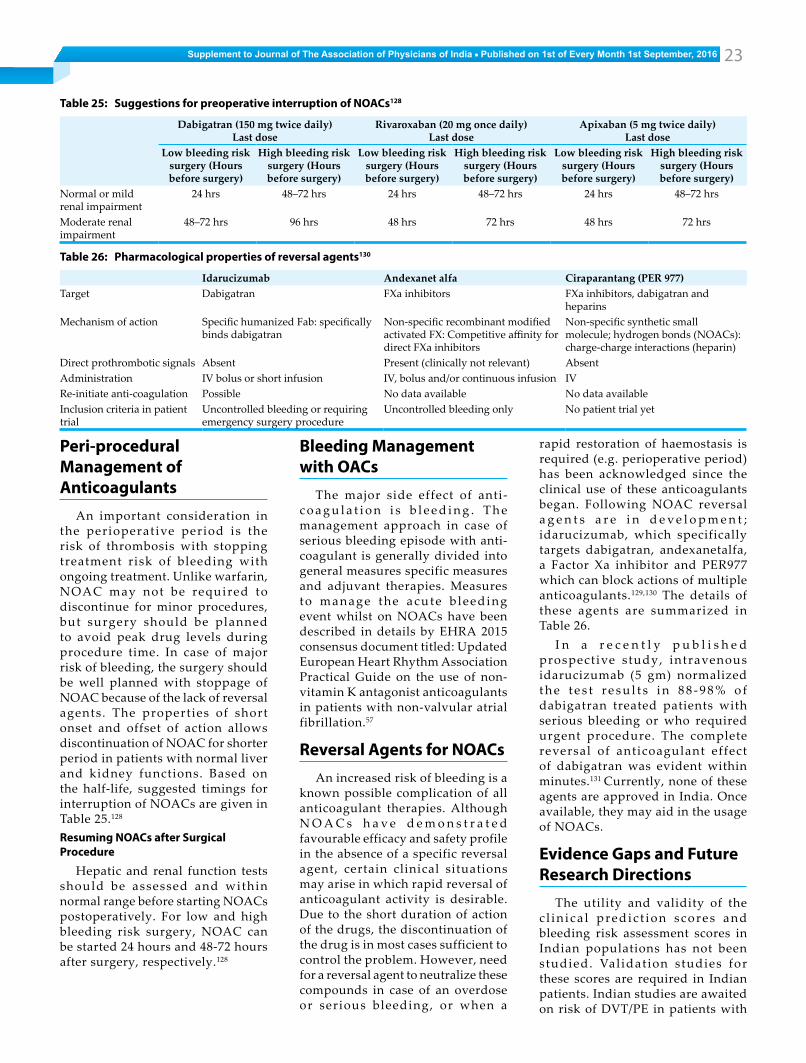
Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 2016 23
rapid restoration of haemostasis is required (e.g. perioperative period) has been acknowledged since the clinical use of these anticoagulants began. Following NOAC reversal a g e n t s a r e i n d e v e l o p m e n t ; idarucizumab, which specifically targets dabigatran, andexanetalfa, a Factor Xa inhibitor and PER977 which can block actions of multiple anticoagulants.129,130 The details of these agents are summarized in Table 26.
I n a r e c e n t l y p u b l i s h e d prospective study, intravenous idarucizumab (5 gm) normalized t h e t e s t r e s u l t s i n 8 8 - 9 8 % o f dabigatran treated patients with serious bleeding or who required urgent procedure. The complete reversal of anticoagulant effect of dabigatran was evident within minutes.131 Currently, none of these agents are approved in India. Once available, they may aid in the usage of NOACs.
Evidence Gaps and Future Research Directions
The utility and validity of the c l in ica l predic t ion scores and bleeding risk assessment scores in Indian populations has not been studied. Val idation studies for these scores are required in Indian patients. Indian studies are awaited on risk of DVT/PE in patients with
Peri-procedural Management of Anticoagulants
An important consideration in the perioperative period is the risk of thrombosis with stopping treatment risk of bleeding with ongoing treatment. Unlike warfarin, NOAC may not be required to discontinue for minor procedures, but surgery should be planned to avoid peak drug levels during procedure time. In case of major risk of bleeding, the surgery should be well planned with stoppage of NOAC because of the lack of reversal agents. The properties of short onset and offset of action allows discontinuation of NOAC for shorter period in patients with normal liver and kidney functions. Based on the half-life, suggested timings for interruption of NOACs are given in Table 25.128
Resuming NOACs after Surgical Procedure
Hepatic and renal function tests should be assessed and within normal range before starting NOACs postoperatively. For low and high bleeding risk surgery, NOAC can be started 24 hours and 48-72 hours after surgery, respectively.128
Bleeding Management with OACs
The major side effect of anti-c o a g u l a t i o n i s b l e e d i n g . T h e management approach in case of serious bleeding episode with anti-coagulant is generally divided into general measures specific measures and adjuvant therapies. Measures to manage the acute b leeding event whilst on NOACs have been described in details by EHRA 2015 consensus document titled: Updated European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist anticoagulants in patients with non-valvular atrial fibrillation.57
Reversal Agents for NOACsAn increased risk of bleeding is a
known possible complication of all anticoagulant therapies. Although N O A C s h a v e d e m o n s t r a t e d favourable efficacy and safety profile in the absence of a specific reversal agent, certain clinical situations may arise in which rapid reversal of anticoagulant activity is desirable. Due to the short duration of action of the drugs, the discontinuation of the drug is in most cases sufficient to control the problem. However, need for a reversal agent to neutralize these compounds in case of an overdose or serious bleeding, or when a
Table 25: Suggestions for preoperative interruption of NOACs128
Dabigatran (150 mg twice daily)Last dose
Rivaroxaban (20 mg once daily)Last dose
Apixaban (5 mg twice daily)Last dose
Low bleeding risk surgery (Hours before surgery)
High bleeding risk surgery (Hours before surgery)
Low bleeding risk surgery (Hours before surgery)
High bleeding risk surgery (Hours before surgery)
Low bleeding risk surgery (Hours before surgery)
High bleeding risk surgery (Hours before surgery)
Normal or mild renal impairment
24 hrs 48–72 hrs 24 hrs 48–72 hrs 24 hrs 48–72 hrs
Moderate renal impairment
48–72 hrs 96 hrs 48 hrs 72 hrs 48 hrs 72 hrs
Table 26: Pharmacological properties of reversal agents130
Idarucizumab Andexanet alfa Ciraparantang (PER 977)Target Dabigatran FXa inhibitors FXa inhibitors, dabigatran and
heparinsMechanism of action Specific humanized Fab: specifically
binds dabigatranNon-specific recombinant modified activated FX: Competitive affinity for direct FXa inhibitors
Non-specific synthetic small molecule; hydrogen bonds (NOACs): charge-charge interactions (heparin)
Direct prothrombotic signals Absent Present (clinically not relevant) AbsentAdministration IV bolus or short infusion IV, bolus and/or continuous infusion IVRe-initiate anti-coagulation Possible No data available No data availableInclusion criteria in patient trial
Uncontrolled bleeding or requiring emergency surgery procedure
Uncontrolled bleeding only No patient trial yet

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 201624
superficial venous thrombosis.
Conflicts of InterestThe authors are on the advisory
panel of multiple pharmaceutical organisations including Boehringer Ingelheim (India) Pvt. Ltd.
FundingSupported by an educational
grant from Boehringer Ingelheim (India) Pvt. Ltd.
AcknowledgementsAu t h o r s a c k n o w l e d g e t h e
sc ient i f ic support extended by following doctors. East
D. Prabhakar, Hyderabad Devender Singh, HyderabadC. Chandra Sekhar, HyderabadNihar Ranjan Pradhan, HyderabadSandeep Mohapatra, HyderabadWest
M.V. Reddy, MumbaiN.P.Mishra, BhopalTanveer Ali, MumbaiVijay Mandora, PuneNorth
Alok Agarwal, DelhiGaurav Bhardwaj, DelhiNaveen Chobdar, DelhiPankaj Aneja, DelhiRajat Agarwal, DelhiRajeev Thukral, DelhiSandeep Agarwal, DelhiSanjay Gogia, DelhiSuhail Bukhari, DelhiVibhor Singhal, GurgaonVineet Arya, DelhiSouth
J. Amalorpavanathan, ChennaiM. Rajkumar, ChennaiPrakash Ramamurthy, CoimbatoreRajesh S, BangaloreSaurabh Rai, BangaloreSunder Narasimhan, BangaloreSunil Bohra, BangaloreBoehringer Ingelheim India Pvt. Ltd
Gaurav Chaudhry, Mumbai
Nirad Acharya, HyderabadPrashant Rana, MumbaiRohit Kodagali, MumbaiShraddha Bhure, MumbaiSonesh Kalra, DelhiViraj Suvarna, MumbaiPlasma Medical Services
Anant Patil
References1. Kesieme E, Kesieme C, Jebbin N, Irekpita E, Dongo
A. Deep vein thrombosis: a clinical review. J Blood Med 2011; 2:59–69.
2. Geerts WH, Bergqvist D, Pineo GF, Heit JA, Samama CM, Lassen MR, et al. Prevention of venous thromboembolism: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest 2008; 133(6 Suppl):381S–453S.
3. Raskob GE, Angchaisuksiri P, Blanco AN, Buller H, Gallus A, Hunt BJ, et al. Thrombosis: a major contributor to global disease burden. Arterioscler Thromb Vasc Biol 2014; 34:2363–71.
4. Silverstein MD, Heit JA, Mohr DN, Petterson TM, O’Fallon WM, Melton LJ. Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med 1998; 158:585–93.
5. Heit J, Petterson T, Farmer S, Bailey K, Melton L. Trends in Indicdence of deep vein thrombosis and pulmonary embolism: a 35-year population-based study. Blood 2006; 108.
6. Turpie, AGG, the PROVE Investigators. A Characterization of Patients with Symptomatic DV T in India. Journal of Thrombosis and Haemostasis volume 3 supplement 1 ISSN: 1740-3340;
7. Leizorovicz A, Turpie AGG, Cohen AT, Wong L, Yoo MC, Dans A, et al. Epidemiology of venous thromboembolism in Asian patients undergoing major orthopedic surgery without thromboprophylaxis. The SMART study. J Thromb Haemost JTH 2005; 3:28–34.
8. Cohen AT, Tapson VF, Bergmann J-F, Goldhaber SZ, Kakkar AK, Deslandes B, et al. Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE study): a multinational cross-sectional study. Lancet Lond Engl 2008; 371:387–94.
9. Pinjala R, ENDORSE-India investigators. Venous thromboembolism risk and prophylaxis in the acute hospital care setting (ENDORSE), a multinational cross-sectional study: results from the Indian subset data. Indian J Med Res 2012; 136:60–7.
10. Heit JA, Mohr DN, Silverstein MD, Petterson TM, O’Fallon WM, Melton LJ. Predictors of recurrence after deep vein thrombosis and pulmonary embolism: a population-based cohort study. Arch Intern Med. 2000; 160:761–8.
11. Schulman S, Lindmarker P, Holmström M, Lärfars G, Carlsson A, Nicol P, et al. Post-thrombotic syndrome, recurrence, and death 10 years after the first episode of venous thromboembolism treated with warfarin for 6 weeks or 6 months. J Thromb Haemost JTH 2006; 4:734–42.
12. Paolo Prandoni Pier Mannuccio Mannucci. Deep vein thrombosis of the lower limbs: Diagnosis and management. Baillières Clin Haematol 1994; 7:693–712.
13. Wells PS. Advances in the diagnosis of venous thromboembolism. J Thromb Thrombolysis 2006; 21:31–40.
14. Kahn SR. The clinical diagnosis of deep venous thrombosis: integrating incidence, risk factors,
and symptoms and signs. Arch Intern Med 1998; 158:2315–23.
15. Haeger K. Problems of acute deep venous thrombosis. I. The interpretation of signs and symptoms. Angiology 1969; 20:219–23.
16. Heijboer H, Büller HR, Lensing AW, Turpie AG, Colly LP, ten Cate JW. A comparison of real-time compression ultrasonography with impedance plethysmography for the diagnosis of deep-vein thrombosis in symptomatic outpatients. N Engl J Med 1993; 329:1365–9.
17. Ginsberg JS, Wells PS, Hirsh J, Panju AA, Patel MA, Malone DE, et al. Reevaluation of the sensitivity of impedance plethysmography for the detection of proximal deep vein thrombosis. Arch Intern Med. 1994;154:1930–3.
18. Ramzi DW, Leeper KV. DVT and pulmonary embolism: Part I. Diagnosis. Am Fam Physician 2004; 69:2829–36.
19. Wells PS, Anderson DR, Bormanis J, Guy F, Mitchell M, Gray L, et al. Value of assessment of pretest probability of deep-vein thrombosis in clinical management. Lancet Lond Engl 1997; 350:1795–8.
20. Hargett CW, Tapson VF. Clinical probability and D-dimer testing: how should we use them in clinical practice? Semin Respir Crit Care Med. 2008; 29:15–24.
21. Bates SM, Jaeschke R, Stevens SM, Goodacre S, Wells PS, Stevenson MD, et al. Diagnosis of DVT: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012; 141(2 Suppl):e351S–418S.
22. Barbar S, Noventa F, Rossetto V, Ferrari A, Brandolin B, Perlati M, et al. A risk assessment model for the identification of hospitalized medical patients at risk for venous thromboembolism: the Padua Prediction Score. J Thromb Haemost 2010; 8:2450–7.
23. Kahn SR, Lim W, Dunn AS, Cushman M, Dentali F, Akl EA, et al. Prevention of VTE in nonsurgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141(2 Suppl):e195S–226S.
24. Caprini JA. Thrombosis risk assessment as a guide to quality patient care. Dis--Mon DM 2005; 51:70–8.
25. Gould MK, Garcia DA, Wren SM, Karanicolas PJ, Arcelus JI, Heit JA, et al. Prevention of VTE in nonorthopedic surgical patients: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012; 141(2 Suppl):e227S–77S.
26. Ramzi DW, Leeper KV. DVT and pulmonary embolism: Part II. Treatment and prevention. Am Fam Physician. 2004; 69:2841–8.
27. Di Nisio M, Squizzato A, Rutjes AWS, Büller HR, Zwinderman AH, Bossuyt PMM. Diagnostic accuracy of D-dimer test for exclusion of venous thromboembolism: a systematic review. J Thromb Haemost JTH. 2007; 5:296–304.
28. Abdalla G, Fawzi Matuk R, Venugopal V, Verde F, Magnuson TH, Schweitzer MA, et al. The diagnostic accuracy of magnetic resonance venography in the detection of deep venous thrombosis: a systematic review and meta-analysis. Clin Radiol 2015; 70:858–71.
29. McRae SJ, Ginsberg JS. Initial treatment of venous thromboembolism. Circulation 2004; 110(9 Suppl 1):I3-9.
30. Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, et al. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest 2016; 149:315–52.
31. Green D, Hirsh J, Heit J, Prins M, Davidson B, Lensing AW. Low molecular weight heparin: a critical analysis of clinical trials. Pharmacol Rev

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 2016 25
1994; 46:89–109. 32. Gould MK, Dembitzer AD, Doyle RL, Hastie TJ,
Garber AM. Low-molecular-weight heparins compared with unfractionated heparin for treatment of acute deep venous thrombosis. A meta-analysis of randomized, controlled trials. Ann Intern Med 1999; 130:800–9.
33. Dolovich LR, Ginsberg JS, Douketis JD, Holbrook AM, Cheah G. A meta-analysis comparing l o w - m o l e c u l a r - w e i g h t h e p a r i n s w i t h unfractionated heparin in the treatment of venous thromboembolism: examining some unanswered questions regarding location of treatment, product type, and dosing frequency. Arch Intern Med 2000; 160:181–8.
34. Büller HR, Davidson BL, Decousus H, Gallus A, Gent M, Piovella F, et al. Fondaparinux or enoxaparin for the initial treatment of symptomatic deep venous thrombosis: a randomized trial. Ann Intern Med 2004; 140:867–73.
35. Hirsh J, Warkentin TE, Shaughnessy SG, Anand SS, Halperin JL, Raschke R, et al. Heparin and low-molecular-weight heparin: mechanisms of action, pharmacokinetics, dosing, monitoring, efficacy, and safety. Chest 2001; 119(1 Suppl):64S–94S.
36. Dalal J, Bhave A, Oomman A, Vora A, Saxena A, Kahali D, et al. The Indian consensus guidance on stroke prevention in atrial fibrillation: An emphasis on practical use of nonvitamin K oral anticoagulants. Indian Heart J 2015; 67, Supplement 2:S13–34.
37. Kakkar N, Kaur R, John M. Outpatient oral anticoagulant management--an audit of 82 patients. J Assoc Physicians India. 2005; 53:847–52.
38. Kakkar N, Kaur R. Knowledge base of clinicians regarding oral anticoagulant therapy in a teaching institution--a questionnaire survey. J Assoc Physicians India 2004; 52:868–72.
39. Ansell J, Hirsh J, Hylek E, Jacobson A, Crowther M, Palareti G, et al. Pharmacology and management of the vitamin K antagonists: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008; 133(6 Suppl):160S–198S.
40. Hirsh J, Fuster V, Ansell J, Halperin JL, American Heart Association, American College of Cardiology Foundation. American Heart Association/American College of Cardiology Foundation guide to warfarin therapy. Circulation 2003; 107:1692–711.
41. Palmer AJ, Koppenhagen K, Kirchhof B, Weber U, Bergemann R. Efficacy and safety of low molecular weight heparin, unfractionated heparin and warfarin for thrombo-embolism prophylaxis in orthopaedic surgery: a meta-analysis of randomised clinical trials. Haemostasis 1997; 27:75–84.
42. Wells PS, Forgie MA, Rodger MA. Treatment of venous thromboembolism. JAMA 2014; 311:717–28.
43. Schulman S, Rhedin AS, Lindmarker P, Carlsson A, Lärfars G, Nicol P, et al. A comparison of six weeks with six months of oral anticoagulant therapy after a first episode of venous thromboembolism. Duration of Anticoagulation Trial Study Group. N Engl J Med 1995; 332:1661–5.
44. Agnelli G, Prandoni P, Santamaria MG, Bagatella P, Iorio A, Bazzan M, et al. Three months versus one year of oral anticoagulant therapy for idiopathic deep venous thrombosis. Warfarin Optimal Duration Italian Trial Investigators. N Engl J Med 2001; 345:165–9.
45. Pipilis A. Management of Bleeding with Newer Anticoagulants. Hosp Chron 2014; 9(1 Sup):54–6.
46. PRADAXA® (dabigatran etexilate mesylate) Prescribing information. Boehringer Ingelheim; 2015.
47. Schulman S, Kearon C, Kakkar AK, Mismetti P, Schellong S, Eriksson H, et al. Dabigatran versus warfarin in the treatment of acute venous thromboembolism. N Engl J Med 2009;
361:2342–52. 48. Schulman S, Kakkar AK, Goldhaber SZ, Schellong
S, Eriksson H, Mismetti P, et al. Treatment of acute venous thromboembolism with dabigatran or warfarin and pooled analysis. Circulation 2014; 129:764–72.
49. XARELTO (rivaroxaban) tablets. Prescribing information. 2013.
50. Press Announcements - FDA expands use of Xarelto to treat, reduce recurrence of blood clots [Internet]. [cited 2016 Mar 16]. Available from: http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm326654.htm
51. EINSTEIN Investigators, Bauersachs R, Berkowitz SD, Brenner B, Buller HR, Decousus H, et al. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med 2010; 363:2499–510.
52. EINSTEIN–PE Investigators, Büller HR, Prins MH, Lensin AWA, Decousus H, Jacobson BF, et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med 2012; 366:1287–97.
53. Agnelli G, Buller HR, Cohen A, Curto M, Gallus AS, Johnson M, et al. Oral apixaban for the treatment of acute venous thromboembolism. N Engl J Med 2013; 369:799–808.
54. Hokusai-VTE Investigators, Büller HR, Décousus H, Grosso MA, Mercuri M, Middeldorp S, et al. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N Engl J Med 2013; 369:1406–15.
55. SAVAYSA (Edoxaban) tablets. USFDA Prescribing information. Daiichi-Sankyo; 2015.
56. ELIQUIS (apixaban) tablets. Prescribing information. 2012.
57. Heidbuchel H, Verhamme P, Alings M, Antz M, Diener H-C, Hacke W, et al. Updated European Heart Rhythm Association Practical Guide on the use of non-vitamin K antagonist anticoagulants in patients with non-valvular atrial fibrillation. Eur Eur Pacing Arrhythm Card Electrophysiol J Work Groups Card Pacing Arrhythm Card Cell Electrophysiol Eur Soc Cardiol 2015; 17:1467–507.
58. Prins MH, Lensing AW, Bauersachs R, van Bellen B, Bounameaux H, Brighton TA, et al. Oral rivaroxaban versus standard therapy for the treatment of symptomatic venous thromboembolism: a pooled analysis of the EINSTEIN-DVT and PE randomized studies. Thromb J 2013; 11:21.
59. Kooiman J, van Hagen N, Iglesias Del Sol A, Planken EV, Lip GYH, van der Meer FJM, et al. The HAS-BLED Score Identifies Patients with Acute Venous Thromboembolism at High Risk of Major Bleeding Complications during the First Six Months of Anticoagulant Treatment. PloS One 2015; 10:e0122520.
60. Lecumberri R, Alfonso A, Jiménez D, Fernández Capitán C, Prandoni P, Wells PS, et al. Dynamics of case-fatalilty rates of recurrent thromboembolism and major bleeding in patients treated for venous thromboembolism. Thromb Haemost 2013; 110:834–43.
61. Boutitie F, Pinede L, Schulman S, Agnelli G, Raskob G, Julian J, et al. Influence of preceding length of anticoagulant treatment and initial presentation of venous thromboembolism on risk of recurrence after stopping treatment: analysis of individual participants’ data from seven trials. BMJ 2011; 342:d3036.
62. Poli D, Palareti G. Assessing recurrence risk following acute venous thromboembolism: use of algorithms. Curr Opin Pulm Med 2013; 19:407–12.
63. Eichinger S, Heinze G, Jandeck LM, Kyrle PA. Risk assessment of recurrence in patients with unprovoked deep vein thrombosis or pulmonary embolism: the Vienna prediction model. Circulation 2010; 121:1630–6.
64. Marcucci M, Iorio A, Douketis JD, Eichinger S, Tosetto A, Baglin T, et al. Risk of recurrence after
a first unprovoked venous thromboembolism: external validation of the Vienna Prediction Model with pooled individual patient data. J Thromb Haemost 2015; 13:775–81.
65. Tritschler T, Méan M, Limacher A, Rodondi N, Aujesky D. Predicting recurrence after unprovoked venous thromboembolism: prospective validation of the updated Vienna Prediction Model. Blood 2015; 126:1949–51.
66. Schulman S, Kearon C, Kakkar AK, Schellong S, Eriksson H, Baanstra D, et al. Extended use of dabigatran, warfarin, or placebo in venous thromboembolism. N Engl J Med 2013; 368:709–18.
67. Romualdi E, Donadini MP, Ageno W. Oral r ivaroxaban after symptomatic venous thromboembolism: the continued treatment study (EINSTEIN-extension study). Expert Rev Cardiovasc Ther 2011; 9:841–4.
68. Agnelli G, Buller HR, Cohen A, Curto M, Gallus AS, Johnson M, et al. Apixaban for extended treatment of venous thromboembolism. N Engl J Med 2013; 368:699–708.
69. Castellucci LA, Cameron C, Le Gal G, Rodger MA, Coyle D, Wells PS, et al. Efficacy and safety outcomes of oral anticoagulants and antiplatelet drugs in the secondary prevention of venous thromboembolism: systematic review and network meta-analysis. BMJ 2013; 347:f5133.
70. Deep Venous Thrombosis: Practice Essentials, Background, Anatomy. 2016 Feb 26 [cited 2016 Mar 16]; Available from: http://emedicine.medscape.com/article/1911303-overview
71. Pengo V, Lensing AWA, Prins MH, Marchiori A, Davidson BL, Tiozzo F, et al. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism. N Engl J Med 2004; 350:2257–64.
72. CDC USA. Health, United States 2014 [Internet]. [cited 2016 Mar 16]. Available from: http://www.cdc.gov/nchs/data/hus/hus14.pdf#020
73. Conklin P, Soares GM, Dubel GJ, Ahn SH, Murphy TP. Acute deep vein thrombosis (DVT): evolving treatment strategies and endovascular therapy. Med Health R I 2009; 92:394–7.
74. Ray G, Behera M. Venous Thromboembolism - Indian Perspective. Med Update 2010; 20:329–34.
75. Kahn SR, Galanaud J-P, Vedantham S, Ginsberg JS. Guidance for the prevention and treatment of the post-thrombotic syndrome. J Thromb Thrombolysis 2016; 41:144–53.
76. Popuri RK, Vedantham S. The role of thrombolysis in the clinical management of deep vein thrombosis. Arterioscler Thromb Vasc Biol 2011; 31:479–84.
77. Watson LI, Armon MP. Thrombolysis for acute deep vein thrombosis. Cochrane Database Syst Rev 2004;(4):CD002783.
78. Watson L, Broderick C, Armon MP. Thrombolysis for acute deep vein thrombosis. Cochrane Database Syst Rev 2014;1:CD002783.
79. Alkhouli M, Zack CJ, Zhao H, Shafi I, Bashir R. Comparative outcomes of catheter-directed thrombolysis plus anticoagulation versus anticoagulation alone in the treatment of inferior vena caval thrombosis. Circ Cardiovasc Interv 2015; 8:e001882.
80. Enden T, Sandvik L, Kløw N-E, Hafsahl G, Holme PA, Holmen LO, et al. Catheter-directed Venous Thrombolysis in acute iliofemoral vein thrombosis--the CaVenT study: rationale and design of a multicenter, randomized, controlled, clinical trial (NCT00251771). Am Heart J 2007; 154:808–14.
81. Davies J, Tippet R, Watson A, Metcalfe J. Systemic inflammatory response syndrome following catheter-directed thrombolysis of acute iliofemoral deep venous thrombosis. Phlebol Venous Forum R Soc Med 2016 Feb 8;
82. Murphy KD. Mechanical thrombectomy for DVT. Tech Vasc Interv Radiol 2004; 7:79–85.

Supplement to Journal of The Association of Physicians of India ■ Published on 1st of Every Month 1st September, 201626
83. Wehrenberg-Klee E, Stavropoulos SW. Inferior vena cava filters for primary prophylaxis: when are they indicated? Semin Interv Radiol 2012; 29:29–35.
84. Mayer O, Poklopová Z. [Usefulness of vena cava filters from clinicians view]. Vnitraní Lékaraství. 2015; 61:799–804.
85. Narani KK. Deep vein thrombosis and pulmonary embolism - Prevention, management, and anaesthetic considerations. Indian J Anaesth 2010; 54:8–17.
86. Kearon C, Akl EA, Comerota AJ, Prandoni P, Bounameaux H, Goldhaber SZ, et al. Antithrombotic therapy for VTE disease: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141(2 Suppl):e419S–94S.
87. Litzendorf ME, Satiani B. Superficial venous thrombosis: disease progression and evolving treatment approaches. Vasc Health Risk Manag 2011; 7:569–75.
88. Di Minno MND, Ambrosino P, Ambrosini F, Tremoli E, Minno GD, Dentali F. Prevalence of deep vein thrombosis and pulmonary embolism in patients with superficial vein thrombosis: a systematic review and meta-analysis. J Thromb Haemost 2016.
89. Decousus H, Prandoni P, Mismetti P, Bauersachs RM, Boda Z, Brenner B, et al. Fondaparinux for the treatment of superficial-vein thrombosis in the legs. N Engl J Med 2010; 363:1222–32.
90. Anderson FA, Wheeler HB, Goldberg RJ, Hosmer DW, Patwardhan NA, Jovanovic B, et al. A population-based perspective of the hospital incidence and case-fatality rates of deep vein thrombosis and pulmonary embolism. The Worcester DVT Study. Arch Intern Med 1991; 151:933–8.
91. Stein PD, Hull RD, Kayali F, Ghali WA, Alshab AK, Olson RE. Venous thromboembolism according to age: the impact of an aging population. Arch Intern Med 2004; 164:2260–5.
92. Heit JA, Mohr DN, Silverstein MD, Petterson TM, O’Fallon WM, Melton LJ. Predictors of recurrence after deep vein thrombosis and pulmonary embolism: a population-based cohort study. Arch Intern Med 2000; 160:761–8.
93. Laporte S, Mismetti P, Décousus H, Uresandi F, Otero R, Lobo JL, et al. Clinical predictors for fatal pulmonary embolism in 15,520 patients with venous thromboembolism: findings from the Registro Informatizado de la Enfermedad TromboEmbolica venosa (RIETE) Registry. Circulation 2008; 117:1711–6.
94. Bauersachs RM. Use of anticoagulants in elderly patients. Thromb Res 2012; 129:107–15.
95. Geldhof V, Vandenbriele C, Verhamme P, Vanassche T. Venous thromboembolism in the elderly: efficacy and safety of non-VKA oral anticoagulants. Thromb J 2014; 12:21.
96. W a r k e n t i n T E . H e p a r i n - i n d u c e d t h ro m b o c y to p e n i a : p at h o g e n e s i s a n d management. Br J Haematol 2003; 121:535–55.
97. Warkentin TE. Platelet count monitoring and laboratory testing for heparin-induced thrombocytopenia. Arch Pathol Lab Med 2002; 126:1415–23.
98. Linkins L-A, Dans AL, Moores LK, Bona R, Davidson BL, Schulman S, et al. Treatment and prevention of heparin-induced thromboc ytopenia: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012; 141(2 Suppl):e495S–530S.
99. Weingarz L, Schwonberg J, Schindewolf M, Hecking C, Wolf Z, Erbe M, et al. Prevalence
of thrombophilia according to age at the first manifestation of venous thromboembolism: results from the MAISTHRO registry. Br J Haematol 2013; 163:655–65.
100. Brunner HI, Chan W-S, Ginsberg JS, Feldman BM. Longterm anticoagulation is preferable for patients with antiphospholipid antibody syndrome. result of a decision analysis. J Rheumatol 2002; 29:490–501.
101. Paper: Influence of Thrombophilia on the Efficacy of Dabigatran Versus Warfarin for the Extended Treatment of Acute Venous Thromboembolism in RE-MEDYTM [Internet]. [cited 2016 Jul 5]. Available from: https://ash.confex.com/ash/2014/webprogram/Paper75822.html
102. Falgá C, Capdevila JA, Soler S, Rabuñal R, Sánchez Muñoz-Torrero JF, Gallego P, et al. Clinical outcome of patients with venous thromboembolism and renal insufficiency. Findings from the RIETE registry. Thromb Haemost 2007; 98:771–6.
103. Akl EA, Kahale L, Barba M, Neumann I, Labedi N, Terrenato I, et al. Anticoagulation for the long-term treatment of venous thromboembolism in patients with cancer. Cochrane Database Syst Rev 2014;7:CD006650.
104. Schulman S, Goldhaber SZ, Kearon C, Kakkar AK, Schellong S, Eriksson H, et al. Treatment with dabigatran or warfarin in patients with venous thromboembolism and cancer. Thromb Haemost 2015; 114:150–7.
105. Heit JA, Kobbervig CE, James AH, Petterson TM, Bailey KR, Melton LJ. Trends in the incidence of venous thromboembolism during pregnancy or postpartum: a 30-year population-based study. Ann Intern Med 2005; 143:697–706.
106. Gherman RB, Goodwin TM, Leung B, Byrne JD, Hethumumi R, Montoro M. Incidence, clinical characteristics, and timing of objectively diagnosed venous thromboembolism during pregnancy. Obstet Gynecol 1999; 94(5 Pt 1):730–4.
107. Lindqvist P, Dahlbäck B, Marŝál K. Thrombotic risk during pregnancy: a population study. Obstet Gynecol 1999; 94:595–9.
108. Simpson EL, Lawrenson RA, Nightingale AL, Farmer RD. Venous thromboembolism in pregnancy and the puerperium: incidence and additional risk factors from a London perinatal database. BJOG Int J Obstet Gynaecol 2001; 108:56–60.
109. James AH, Jamison MG, Brancazio LR, Myers ER. Venous thromboembolism during pregnancy and the postpartum period: incidence, risk factors, and mortality. Am J Obstet Gynecol 2006; 194:1311–5.
110. Andersen BS, Steffensen FH, Sørensen HT, Nielsen GL, Olsen J. The cumulative incidence of venous thromboembolism during pregnancy and puerperium--an 11 year Danish population-based study of 63,300 pregnancies. Acta Obstet Gynecol Scand 1998; 77:170–3.
111. Jacobsen AF, Skjeldestad FE, Sandset PM. Incidence and r isk patterns of venous t h r o m b o e m b o l i s m i n p r e g n a n c y a n d puerperium--a register-based case-control study. Am J Obstet Gynecol 2008; 198:233.e1-7.
112. McColl MD, Ramsay JE, Tait RC, Walker ID, McCall F, Conkie JA, et al. Risk factors for pregnancy associated venous thromboembolism. Thromb Haemost 1997; 78:1183–8.
113. Dempfle C-EH. Minor transplacental passage of fondaparinux in vivo. N Engl J Med 2004; 350:1914–5.
114. Harenberg J. Treatment of a woman with lupus and thromboembolism and cutaneous intolerance to heparins using fondaparinux during pregnancy. Thromb Res 2007; 119:385–8.
115. Mazzolai L, Hohlfeld P, Spertini F, Hayoz D, Schapira M, Duchosal MA. Fondaparinux is a safe alternative in case of heparin intolerance during pregnancy. Blood 2006; 108:1569–70.
116. Wi jes i r iwardana A, Lees DAR, Lush C . Fondaparinux as anticoagulant in a pregnant woman with heparin allergy. Blood Coagul Fibrinolysis Int J Haemost Thromb 2006; 17:147–9.
117. Gerhardt A, Zotz RB, Stockschlaeder M, Scharf RE. Fondaparinux is an effective alternative anticoagulant in pregnant women with high risk of venous thromboembolism and intolerance to low-molecular-weight heparins and heparinoids. Thromb Haemost 2007; 97:496–7.
118. Winger EE, Reed JL. A retrospective analysis of fondaparinux versus enoxaparin treatment in women with infertility or pregnancy loss. Am J Reprod Immunol N Y N 1989. 2009; 62:253–60.
119. Knol HM, Schultinge L, Erwich JJHM, Meijer K. Fondaparinux as an alternative anticoagulant therapy during pregnancy. J Thromb Haemost 2010; 8:1876–9.
120. Elsaigh E, Thachil J, Nash MJ, Tower C, Hay CRM, Bullough S, et al. The use of fondaparinux in pregnancy. Br J Haematol 2015; 168:762–4.
121. Clark NP, Delate T, Witt DM, Parker S, McDuffie R. A descriptive evaluation of unfractionated heparin use during pregnancy. J Thromb Thrombolysis 2009; 27:267–73.
122. Forestier F, Daffos F, Capella-Pavlovsky M. Low molecular weight heparin (PK 10169) does not cross the placenta during the second trimester of pregnancy study by direct fetal blood sampling under ultrasound. Thromb Res 1984; 34:557–60.
123. Forestier F, Daffos F, Rainaut M, Toulemonde F. Low molecular weight heparin (CY 216) does not cross the placenta during the third trimester of pregnancy. Thromb Haemost 1987; 57:234.
124. Lindhoff-Last E, Kreutzenbeck H-J, Magnani HN. Treatment of 51 pregnancies with danaparoid because of heparin intolerance. Thromb Haemost 2005; 93:63–9.
125. Weitz JI. Low-Molecular-Weight Heparins. N Engl J Med 1997; 337:688–99.
126. Mára M, Koryntová D, Rezábek K, Kaprál A, Drbohlav P, Jirsová S, et al. [Thromboembolic complications in patients undergoing in vitro fertilization: retrospective clinical study]. Ceská Gynekol Ceská Lékarská Spolecnost J Ev Purkyne. 2004; 69:312–6.
127. Chan W-S, Rey E, Kent NE, VTE in Pregnancy Guideline Working Group, Chan W-S, Kent NE, et al. Venous thromboembolism and antithrombotic therapy in pregnancy. J Obstet Gynaecol Can JOGC J Obstétrique Gynécologie Can JOGC 2014; 36:527–53.
128. Tran H, Joseph J, Young L, McRae S, Curnow J, Nandurkar H, et al. New oral anticoagulants: a practical guide on prescription, laboratory te s t i n g a n d p e r i - p ro ce d u ra l / b l e e d i n g management. Australasian Society of Thrombosis and Haemostasis. Intern Med J 2014; 44:525–36.
129. Sarich TC, Seltzer JH, Berkowitz SD, Costin’ J, Curnutte JT, Gibson CM, et al. Novel oral a n t i c o a g u l a n t s a n d r e v e r s a l a g e n t s : Considerations for clinical development. Am Heart J 2015; 169:751–7.
130. Dalal J, Bhave A, Chaudhry G, Rana P. Reversal agents for NOACs: Connecting the dots. Indian Heart J [Internet]. [cited 2016 Mar 16]; Available from: http://www.sciencedirect.com/science/article/pii/S0019483215008810
131. Pollack CV, Reilly PA, Eikelboom J, Glund S, Verhamme P, Bernstein RA, et al. Idarucizumab for Dabigatran Reversal. N Engl J Med 2015; 373:511–20.