contentseickemeyerveterinary.com/product_documents/4802560 - stephens...6 designed to be versatile,...
TRANSCRIPT
Contents
Page
The Stephens Anaesthetic Machine - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 5
Stephens Universal Vapouriser - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 6
A Simple Method to Ensure Fresh Working Soda Lime - - - - - - - - - - - - - - - - 8
An Introduction to In-circle Closed Circuit Anaesthesia - - - - - - - - - - - - - - - 9
Induction of Anaesthesia With The Stephens Machine
1. Mask Induction - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 11
2. Intravenous Induction - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 12
Operation of Stephens Anaesthetic Apparatus in
Small Animals without Pre-Anaesthetic Drugs - - - - - - - - - - - - - - - - - - - - - 13
Mask Induction of Anaesthesia in Small Animals
without Pre-Anaesthetic Drugs - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 13
Problems of Maintenance - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 14
Operational Hints - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 15
Care and Maintenance of the Stephens Equipment - - - - - - - - - - - - - - 15
Accessories for the Stephens Anaesthetic Apparatus - - - - - - - - - - - - - - - - 16
Stephens Floor Stand & Wall Mount - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 16
Storage of Anaesthetic Agents - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 17
Face Masks - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - 17
Stephens Anaesthetic Apparatus Parts List - - - - - - - - - - - - - - - - - - - - - - - 18
3

4
THE STEPHENS ANAESTHETIC MACHINE
Fig.1
Fig.2
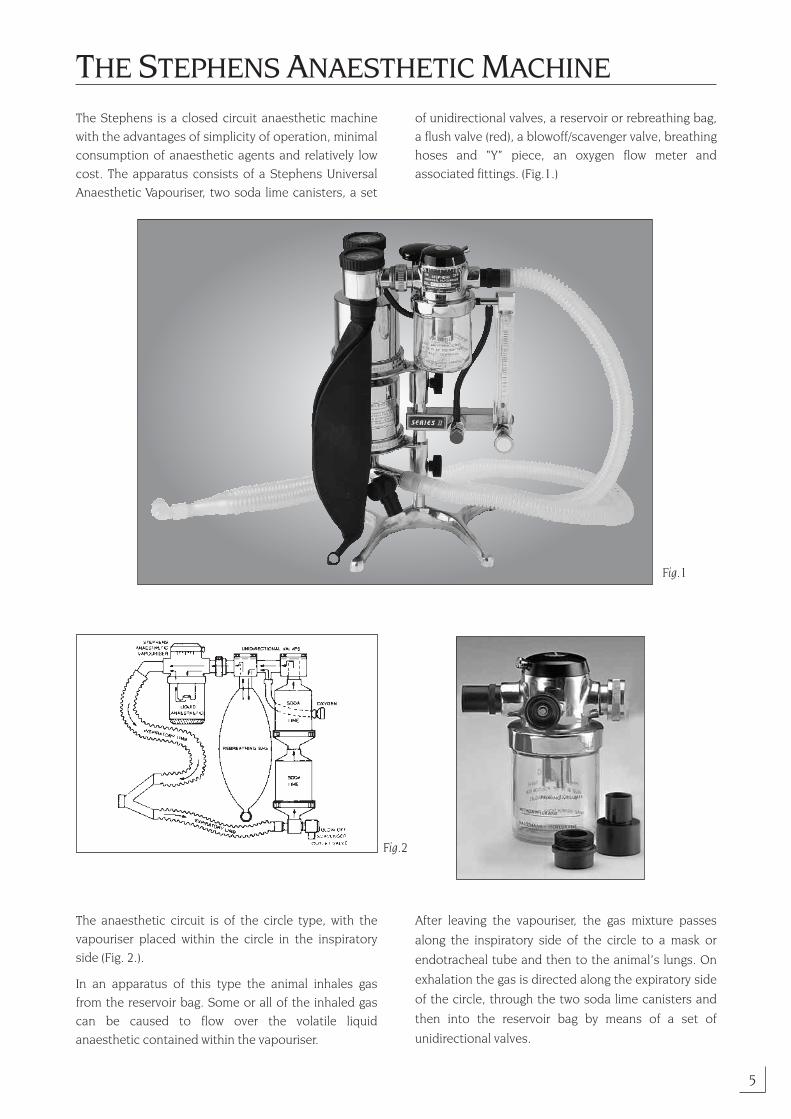
The Stephens is a closed circuit anaesthetic machinewith the advantages of simplicity of operation, minimalconsumption of anaesthetic agents and relatively lowcost. The apparatus consists of a Stephens UniversalAnaesthetic Vapouriser, two soda lime canisters, a set
of unidirectional valves, a reservoir or rebreathing bag,a flush valve (red), a blowoff/scavenger valve, breathinghoses and “Y” piece, an oxygen flow meter andassociated fittings. (Fig.1.)
The anaesthetic circuit is of the circle type, with thevapouriser placed within the circle in the inspiratoryside (Fig. 2.).
In an apparatus of this type the animal inhales gasfrom the reservoir bag. Some or all of the inhaled gascan be caused to flow over the volatile liquidanaesthetic contained within the vapouriser.
After leaving the vapouriser, the gas mixture passes
along the inspiratory side of the circle to a mask or
endotracheal tube and then to the animal’s lungs. On
exhalation the gas is directed along the expiratory side
of the circle, through the two soda lime canisters and
then into the reservoir bag by means of a set of
unidirectional valves.
5

66
Designed to be versatile, the Stephens vapouriser is verycompact and is readily adapted for use with any volatileanaesthetic agent, i.e., halothane, methoxyflurane andisoflurane.
The main control on the vapouriser provides a smoothincrease in concentration between OFF and ON. Inaddition to this, there is a metal sleeve on the innercircular port, which extends into the glass anaestheticjar. By raising or lowering this sleeve, the vapourconcentration delivered may be decreased orincreased to suit the clinical requirements. (Fig. 3C.)
In contrast to most vapourisers, an exceptionally wideand constant bore is maintained throughout themechanism, regardless of the concentration setting onthe main control. This is a unique feature, and isachieved by the use of a special port design in thevapouriser head. The bore is equivalent to a diameterof 7/8” (22mm). Back pressure and turbulence are thuskept to an absolute minimum.
The bowl of the vapouriser enables the anaesthetist toquickly check the levels of anaesthetic agent remainingin the vapouriser. The priming volume required issmaller than used in most other vapourisers, e.g., 8-12mLs of halothane or isoflurane and sevoflurane. Thesepriming (filling) volumes should never be exceeded.
As the anaesthetic vapouriser is located within thecircuit, the mass of anaesthetic delivered to the animal(at a particular setting of the vapouriser) changes withthe variations in the minute volume of respiration. Ifthe depth of anaesthesia increases, the decrease inminute volume which results is followed by a decreasein the rate of vapourisation of the anaesthetic.Conversely, the rate of vapourisation of theanaesthetic increases as the depth of anaesthesiadecreases. Because changes in the depth ofanaesthesia are automatically followed bycompensating changes in the mass of anaestheticdelivered to the animal, the system is to some extentself-regulating.
STEPHENS UNIVERSAL VAPOURISER
Fig.3A
Fig.3B
Fig.3C
Fig.3D
Stephens Universal Vapouriser fitted to an Ohio machine. Sleeve is in the DOWN position for mask induction with a cat.
The Vapouriser can be readily fitted to other machines as illustratedin the above photographs.

In those cases in which intermittent positive pressureventilation is used, the vapouriser setting should bereduced. The flow of oxygen into the system should beincreased to slightly above the metabolic requirementsof the animal. This higher oxygen inflow ensures thatthe rebreathing bag will slowly overfill and that periodicemptying of excess gas will tend to prevent thepossibility of a build-up of concentration ofanaesthetic or CO2 within the system.
The adjustable metal sleeve is normally used in the UPposition for maintenance of anaesthesia. It may beadvantageous to lower the sleeve for induction of
animals in cold climates or when anaesthetising catsand other lightweight animals to enable a higherconcentration to be achieved during induction. Oncethis is accomplished, the sleeve is returned to the UPposition. The sleeve gives the vapouriser greatversatility and enables it to be used in a variety ofdifferent climates, with a number of differentanaesthetic agents, and for the production of varyingdepths of surgical anaesthesia in animals.
The vapouriser locks in the OFF position. To turn it onpull the knob out and turn clockwise.
7
Soda Lime Canisters
Soda Lime Canisters are used to absorb the exhaledcarbon dioxide from the animal’s lungs. They aredesigned to produce minimum channelling of theexpired respiratory gases through the soda limecontained within each canister. (Fig.4.) The carbondioxide chemically reacts with the soda lime producingheat and water.
Two canisters are placed in the expiratory limb of theanaesthetic apparatus, thus any resistance caused bythe soda lime occurs on the passive expiratory phaseof the respiration and there is little resistance duringinspiration. (Fig.5.) During the absorption of carbondioxide by the soda lime, heat is produced and this isused as an indicator of absorptive efficiency. (Fig.7.)
The soda lime canister nearest to the expiratory limbof the circle is always the first canister to becomeexhausted (i.e., lower canister). When the soda lime inthe lower canister is exhausted, the canister is cold tothe touch and may be removed temporarily from thecircuit and refilled with fresh soda lime. (Fig.6.)
Fig.4
Fig.5
Fig.4A

It should then be placed in the upper position, and thetop canister is placed nearest to the animal (in thelower position). By doing this it is assured there isalways one soda lime canister containing fresh sodalime within the circle at all times. (Fig.7.)
When the anaesthetic apparatus is to be stored for anylength of time it is advisable to place a cork firmly in
the “Y” piece of the apparatus, thus sealing the systemand preventing the slow decomposition of the sodalime by the carbon dioxide contained in theatmosphere. An approximate estimation of thetime to exhaust one canister is 7.5 hours per each260gm canister with a 25kg/55lb dog.
8
A SIMPLE METHOD TO ENSURE FRESH WORKING SODA LIME:Change your lower canister every Monday or second Monday morning – this will be governed by duration, size of patient and number of anaesthetics for a week. Ref. Fig. 6 & 7.
Unidirectional Valves
The unidirectional valves are manufactured in one unitembodying two one-way valves and provision for an inletfor fresh gases.(Fig.8.) Fresh gas enters the systemthrough the inletport and fills therebreathing bag.The unidirectionalvalves have atendency to makea “clicking” noiseduring operatingwhich is anadvantage to theveterinarian whomay be workingalone. The noise produces an auditory indication of theanimals’ respiratory rate. The valve assembly is readilydismantled for cleaning by unscrewing the valve covers.
Flowmeter The apparatus is supplied with a specially constructed“rotameter” type oxygen flow meter as shown in Fig.1.
This flow meter has a maximum measurable output of600cc per minute. We suggest the use of a 4 litre bag as ithas less resistance than some smaller bags. The new latexbags of 2 litres or less have acceptable low resistance.When using the apparatus for very small animals whosemetabolic requirements for oxygen are small, make sureoxygen is set at 5mL/kg body weight oxygen entering thesystem to prevent the uneconomical wastage ofanaesthetic vapour. Wastage will occur with the loss ofvapourised anaesthetic into the atmosphere followingover-filling of the rebreathing bag, if too high an oxygeninflow is used. If excess gas flows into the system it caneasily be removed by opening the blowoff/pop off valvesituated near the lower canister, and squeezing the excessgas from the rebreathing bag. The rebreathing bag shouldalways contain sufficient gas so that the maximuminspiratory effort made by the animal will not completelyempty the bag. However, it should not be so full of gasthat a maximum expiration by the patient will over-distend the bag.
Fig.6 Fig.7
Fig.8
Unidirectional Valves
REBREATHINGBAG

Low Flow and Closed Circuit Anaesthesia
Circle systems are classified by the ratio of fresh gas flowto the minute volume uptake of the inhaled gases. If thefresh gases are provided at a rate exactly equal to therate at which the body takes them up, then the systemby definition is a closed circuit. If the flow of fresh gasesis higher than the uptake, but not so high as to preventrebreathing, the system by definition is semi-closed. Ifthe flow of fresh gases is so high that rebreathing doesnot occur, the system is a non-rebreathing one.Assuming an approximate oxygen consumption of5mL/kg/min for a dog or cat, then an oxygen flow of5mL/kg/min would result in a closed circuit. If the oxygenflow was higher than 5mL/kg/min but less than200mL/kg/min then the system is semi-closed. If theflow is 200mL/kg/min or greater then the system is non-rebreathing. The most economical way of administeringinhaled anaesthetic is with a closed circuit.
Vapouriser Position
Vapourisers may be positioned in-the-circuit or out-of-the-circuit. In general, vapourisers used out-of-the-circuit are intricate, expensive, heavy and deliver aknown concentration of anaesthetic agent. Vapourisersused in-the-circuit are less expensive, lighter, andcannot be calibrated for the delivered anaestheticconcentration, as the rebreathed gases re-cycledthrough the vapouriser already contain anaestheticagent and can only be calibrated when used with freshgases. Ideally, in-circuit vapourisers should maintain arelatively constant temperature, not be subject to largeconcentration fluctuations associated with surging gasflows which occur with spontaneous respiration, andhave low internal resistance. The Stephens meetsthese criteria.
Neither type of vapouriser is absolutely superior to theother and each has certain advantages anddisadvantages. Neither type is more difficult to usethan the other. The most important factor in the use ofeither, is to understand the effects of the fresh gas flow(oxygen) on the inspired concentration of the inhaledanaesthetic and the effects of intermittent positivepressure ventilation on the inhaled anaestheticconcentration.
It is important to understand and differentiatebetween the anaesthetic concentration delivered fromthe vapouriser and the actual inspired concentration.The inspired concentration is the concentration being
inspired by the patient from the inspiratory limb of thecircuit. Sometimes these two concentrations aresimilar and sometimes they are very different. In theout-of-circuit vapouriser with oxygen fresh gas flows of2L/min, the inspired concentration will be close to thedial setting. With low fresh gas flows of 2-500cc/min,the inspired concentration will be substantially lessthan the dial setting. With in-circuit vapourisers, theinspired concentration will be lower with high oxygenfresh gas flows than with lower fresh gas flows.
Guidelines
There are many variations in techniques for usinginhalant anaesthetics, however, the most commonmethod in the dog is to administer an anticholinergicdrug such as atropine with a tranquilliser or a narcotic.After a few minutes, anaesthesia is induced with anintravenous thiobarbiturate such as thiopental orthiamylal. Following this the animal is then intubatedand inhalant anaesthesia begun. The followingguidelines for using the Stephens Anaesthetic Machineare based on using the above technique. As with any anaesthetic technique dosages, flows andconcentrations need to be varied from any guidelinesor recommendations depending on the responses ofeach individual patient. If other techniques are usedthen these guidelines need to be modified for theparticular circumstance. If a healthy animal is to beinduced and maintained with only an inhaledanaesthetic then the induction and maintenanceconcentrations will need to be higher than those inthese guidelines. On the other hand if the animal isvery ill then a much lower concentration may beneeded or the patient may not be able to tolerate thechosen agent at all. Oxygen flows used commonly, varygreatly. Those listed here are not the only ones whichcan be used but are just suggestions for a veryeconomical approach, however they too need to bemodified depending on the circumstances of aparticular patient.
Regardless of the oxygen flow chosen it is of the utmostimportance that the operator understand the effects ofthe oxygen flow on the inspired anaestheticconcentration and the oxygen requirements of the patient.
These guidelines are for healthy dogs given amoderately sedative pre-anaesthetic and which aregoing to be anaesthetised with halothane or isoflurane.
9
AN INTRODUCTION TO IN-CIRCLE CLOSEDCIRCUIT ANAESTHESIA

Intermittent Positive Pressure Ventilation
Because the Stephens Vapouriser is positioned in-the-circuit it is important to understand the effects of IPPVon the inspired concentration. IPPV may increase theinspired anaesthetic concentration from that recordedwith spontaneous ventilation therefore the vapourisersettings need to be lower with positive pressureventilation than those used with spontaneousbreathing. Guidelines for vapouriser settings withpositive pressure ventilation are: for inhalationinduction; vapouriser set at 2 or 3 eighths; formaintenance, vapouriser set at 1 or 2 eighths. If IPPV isstarted the vapouriser setting should be decreased by50%. The patient should be re-assessed after a fewminutes and the vapouriser control re-adjusted if necessary.
The oxygen flow for maintenance may have to behigher than that used with spontaneous breathing ifthe machine has not been checked for leaks aroundthe endotracheal tube cuff, face mask, or any othercircumstances, which will allow gas to escape from themachine or the patient.
Should the patient require positive pressureventilation because of respiratory arrest due to asuspected drug overdose – medical condition, etc.,etc., then commence with the vapouriser turned offuntil the cause of the respiratory arrest has beendetermined.
Our thanks to Professor Alan M. Klide, University ofPennsylvania for help in the preparation of theseadditional notes.
NOTEThe use of pre-anaesthetic drugs, such as Ace Promazine will
substantially potentiate anaesthetic agents. Ideally Ace should be administered 1 hour prior to the commencement of Anaesthesia for
its effect to be adequate. If given 15 minutes before anaesthesia, the animal will often go deeper 30 minutes into the anaesthetic when the full effect of the
Ace takes place. The original vapouriser setting which was adequate for theinitial and subsequent maintenance phase of the anaesthetic, will now,
due to a deepening of the anaesthetic plane-be too high.
THERE IS NO SUBSTITUTE FOR ADEQUATE PATIENT MONITORING.
If pre-anaesthetic agents are used – all settings should be drastically reduced,(usually by up to 30%) more often than not, settings of 1/4 to 3/8
may be all that is necessary.
10

11
INDUCTION OF ANAESTHESIA WITH THESTEPHENS MACHINE
The Stephens anaesthetic machine can be used in oneof two ways to complete induction of anaesthesia:
1. Mask Induction
Particularly valuable in old or debilitated patients inwhich intravenous induction agents (e.g. barbiturates)may be poorly tolerated. Also of value in Caesariansection and where rapid recovery is required (e.g.outpatient anaesthetics). If necessary, the patient maybe premedicated with an opioid and/or sedative tominimize patient resistance during induction. Theaddition of an anticholinergic, such as atropine, to thepreanaesthetic drug regime will reduce salivation to aminimum and protect against vagally-mediatedbradycardia.
Doses of Premeds:
Acepromazine 0.05mg/kg IM
Butorphanol 0.2mg/kg IM
Atropine 0.04mg/kg IM
In a healthy patient all the above agents may be givensimultaneously (mixed in the same syringe if desired). A30 minute interval is required between premedicationand mask induction for the full effect of the drugs tobecome apparent. In debilitated or elderly patients thedose of acepromazine should be reduced by half oracepromazine can be omitted. In patients which are sodepressed that no resistance to mask induction isanticipated, atropine may be all that is required.
The animal (dog or cat) should be handled gentlythroughout the induction process. The Stephensmachine should be primed with oxygen and a snugfitting face mask should be attached at the Y-piece ofthe breathing tubes. The flowmeter should be set todeliver 10mL/Kg/minute of oxygen and at this point the
vapouriser should be set in the OFF position. The facemask should be applied to the animal’s snoutand the animal should be permitted to breathe oxygenfor a few breaths or until it has become accustomed tothe mask. At this point the vapouriser can be“cracked”. An initial dial set of #1 will permit theanimal to become accustomed to the odour of theanaesthetic. When the animal is comfortably breathingthe low concentration of anaesthetic which results,say, after 5 good breaths, the vapouriser setting shouldbe increased to #2. After another 5 breaths or 30seconds later the vapouriser setting can be increasedto #3 or #4 depending on the patient’s response.Usually a further increment to setting of #5 or #6 willbe necessary, especially in healthy patients, beforeinduction is complete. Even if induction takes a fewminutes longer with this incremental approach, thetechnique is safer than using supramaximalconcentrations to expedite the induction process. Inthe event of the patient struggling during induction,the incremental increases may be made in earliersuccession to get more rapid control of the patient.
The end point of the induction is when spontaneoushead, neck and limb movements have ceased; the jawis relaxed; tongue curing, tongue retraction andswallowing have ceased; the eyes are rotated ventrally;breathing is regular and automatic. At this pointintubation should be accomplished. For shortprocedures, say less than 40 minutes, in previouslyfood deprived animals, maintenance by facemask isoften satisfactory (providing the face mask fits well and is closely applied to prevent leaks). Followinginduction the dial setting should be reduced to #2 or#3 depending on the anaesthetic depth of the patient.Oftentimes, in healthy patients which have receivedsedative premedication, a dial setting of #2 or #21/2 isrequired to maintain anaesthetic. In depressedpatients lower settings will maintain anaesthesia.
By Dr Nicholas Dodman, Professor of Anaesthesia School of VeterinaryMedicine, Tufts University, Massachusetts, U.S.A.

12
2. Intravenous Induction
In healthy patients, intravenous induction ofanaesthesia is safe and more expeditious than maskinduction. Agents used include thiobarbiturates,methobarbiturates and propofol. The latter two areassociated with much quicker recoveries and are idealfor outpatient work. The dose of the induction agentswill depend on the level of central nervous systemactivity of the patient. This, in turn, depends onwhether premedication has been given (see earlier) andon the physical state of the patient. Induction drugs arebest given slowly and to effect. Sedative premedicationis almost mandatory with methobarbiturates tominimize excitatory phenomena during induction. The
end point of induction is as described above under theheading “mask induction”. Once again, intubation isoptional. Indications for intubation are governed byoperative factors and patient factors. In either case, theStephens anaesthetic machine should be primed withoxygen ready for inhalational maintenance ofanaesthesia. An oxygen flow rate of 10 mL/kg/minute isrecommended and an initial dial setting of #3 is usuallysatisfactory (again, depending on the patient’sanaesthetic depth following induction). After thetransition form intravenous to inhalation anaesthesiathe dial setting can often be reduced to #2.
Our thanks to
Professor Nicholas Dodman,
Tufts University for help in
the preparation of these
additional notes.
13
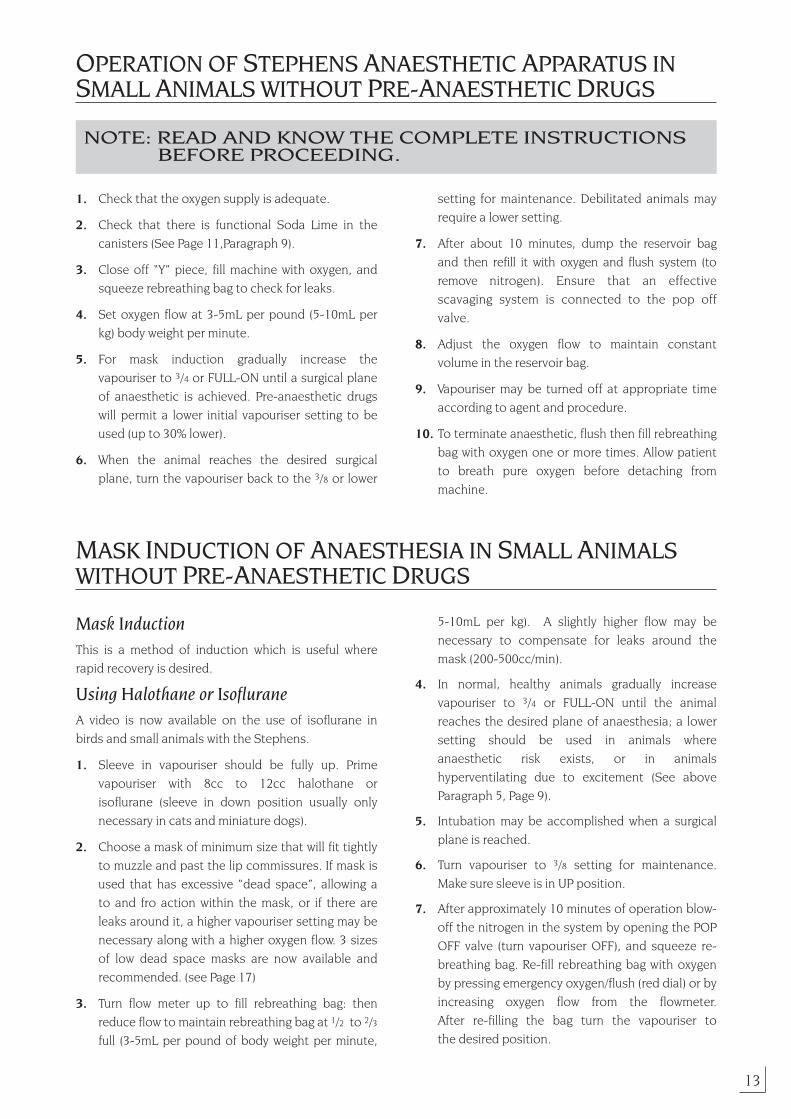
OPERATION OF STEPHENS ANAESTHETIC APPARATUS INSMALL ANIMALS WITHOUT PRE-ANAESTHETIC DRUGS
NOTE: READ AND KNOW THE COMPLETE INSTRUCTIONS BEFORE PROCEEDING.
1. Check that the oxygen supply is adequate.
2. Check that there is functional Soda Lime in the canisters (See Page 11,Paragraph 9).
3. Close off “Y” piece, fill machine with oxygen, andsqueeze rebreathing bag to check for leaks.
4. Set oxygen flow at 3-5mL per pound (5-10mL perkg) body weight per minute.
5. For mask induction gradually increase thevapouriser to 3/4 or FULL-ON until a surgical planeof anaesthetic is achieved. Pre-anaesthetic drugswill permit a lower initial vapouriser setting to beused (up to 30% lower).
6. When the animal reaches the desired surgical plane, turn the vapouriser back to the 3/8 or lower
setting for maintenance. Debilitated animals mayrequire a lower setting.
7. After about 10 minutes, dump the reservoir bagand then refill it with oxygen and flush system (toremove nitrogen). Ensure that an effectivescavaging system is connected to the pop offvalve.
8. Adjust the oxygen flow to maintain constantvolume in the reservoir bag.
9. Vapouriser may be turned off at appropriate timeaccording to agent and procedure.
10. To terminate anaesthetic, flush then fill rebreathingbag with oxygen one or more times. Allow patientto breath pure oxygen before detaching frommachine.
MASK INDUCTION OF ANAESTHESIA IN SMALL ANIMALSWITHOUT PRE-ANAESTHETIC DRUGS
Mask InductionThis is a method of induction which is useful whererapid recovery is desired.
Using Halothane or IsofluraneA video is now available on the use of isoflurane inbirds and small animals with the Stephens.
1. Sleeve in vapouriser should be fully up. Primevapouriser with 8cc to 12cc halothane orisoflurane (sleeve in down position usually onlynecessary in cats and miniature dogs).
2. Choose a mask of minimum size that will fit tightlyto muzzle and past the lip commissures. If mask isused that has excessive “dead space”, allowing ato and fro action within the mask, or if there areleaks around it, a higher vapouriser setting may benecessary along with a higher oxygen flow. 3 sizesof low dead space masks are now available andrecommended. (see Page 17)
3. Turn flow meter up to fill rebreathing bag: thenreduce flow to maintain rebreathing bag at 1/2 to 2/3full (3-5mL per pound of body weight per minute,
5-10mL per kg). A slightly higher flow may benecessary to compensate for leaks around themask (200-500cc/min).
4. In normal, healthy animals gradually increasevapouriser to 3/4 or FULL-ON until the animalreaches the desired plane of anaesthesia; a lowersetting should be used in animals whereanaesthetic risk exists, or in animalshyperventilating due to excitement (See aboveParagraph 5, Page 9).
5. Intubation may be accomplished when a surgicalplane is reached.
6. Turn vapouriser to 3/8 setting for maintenance.Make sure sleeve is in UP position.
7. After approximately 10 minutes of operation blow-off the nitrogen in the system by opening the POPOFF valve (turn vapouriser OFF), and squeeze re-breathing bag. Re-fill rebreathing bag with oxygenby pressing emergency oxygen/flush (red dial) or byincreasing oxygen flow from the flowmeter. After re-filling the bag turn the vapouriser to the desired position.

14
NOTE: DO NOT MAINTAIN THE ANIMAL WITH THE SLEEVEIN THE DOWN POSITION.
The sleeve of the vapouriser must be in the UP positionwhen using halothane or isoflurane, a wick is fitted foruse with methoxyflurane. The vapouriser is turned tothe 1/2 or higher setting after a barbiturate inductionuntil a surgical plane is reached.
The maintenance setting for anaesthesia withhalothane or isoflurane and oxygen in temperateclimates 60° - 70° F is 1/8 to 3/8 open. In warmerclimates or with very toxic animals a setting of between1/8 to 2/8 may be sufficient. Very small animals such ascats and very small dogs may need the vapouriser at aslightly higher setting.
At the completion of the procedure the animal maysimply be disconnected from the machine (followingpurging and allowed to breath pure oxygen).
Problems of Maintenance
Animal too deeply anaesthetised:
Check:
1. Position of sleeve in vapouriser (should be in theUP position).
2. Setting on vapouriser control ( may be too high).
3. Vapouriser over-full (above designated level for agent).
4. Lime exhausted.
Animal too light:
Check:
1. Is endo tube correctly positioned and inflated?
2. Does vapouriser contain anaesthetic liquid?
3. Is setting of vapouriser main control correct?
4. Excess leakage from the system due to a looseconnection.
5. Oxygen flow too high causing dilution of anaesthetic concentration.
With the Stephens excess O2 flow is the single greatestcause of poor maintenance of a surgical plane ofanaesthesia. Check flow – it should be approximately6-10mL/kg body weight.
In the out-of-circuit system the fresh gas (oxygen)carries the anaesthetic agent to the patient. In thevapouriser-in-circuit system, the patient’s breathingcarries the anaesthetic agent. Too high an O2 flow willdilute the anaesthetic mixture when a rate in excess ofbasal O2 requirement is used.
Bag Overfills:
1. Excessive oxygen inflow.
2. Kink or obstruction has occurred in breathing hoseor endo tube.
3. A fall in body temperature with a resulted decreasein oxygen consumption.
4. A fall in cardiac output with a resulted decrease inoxygen uptake.Fig.10
Read the flowmeter fromthe top of the O2 bobbin

15
Operational Hints
1. If high oxygen flow is required to keep bag atconstant size, look for leaks in the system at:
a) connections (especially around the vapouriser).
b) cuff deflation on the endotracheal tube.
2. To speed anaesthetic recovery, turn vapouriser offbefore the end of the anaesthetic.
3. To terminate anaesthetic, turn off vapouriser, flushwith oxygen to clear machine of anaesthetic andallow animal to breath oxygen for a short whilebefore detaching from machine.
4. Remove endotracheal tube when the swallowingreflex reappears.
5. Whenever the animal seems unduly depressed atthe regular maintenance setting or with animalsthat are toxic, anaemic, dehydrated, debilitated, inshock or a breed known to be anaestheticsensitive, always try to maintain them at a lowervapouriser setting. If they are light wriggle at thispoint. Increase the vapouriser setting until thedesired depth of anaesthetic is reached, thenreturn to the lower maintenance setting.
6. On very small animals where basal oxygen flow may be difficult to regulate, fill the rebreathingbag 2/3 full and almost shut off the oxygen flow.Refill the bag when the animal’s needs havereduced the bag to less than 1/2 full.
7. If very small animals (under 5 pounds/2kg) are to be routinely anaesthetised, it may be desirableto purchase and use a paediatric set containingbreathing hoses and “Y” piece.
8. When filling the soda lime canisters, tap them gently to remove any dust from the soda lime,before attaching to the machine.
9. Soda lime gives off heat while it is absorbing CO2.To determine if a canister is exhausted, feel it whenin operation. The lower canister will exhaust first. Ifit is cold to the touch it may be removed from thecircuit and refilled (Fig. 7.), even during operation,and re-connect the expiratory hose to the uppercanister. (Fig.6.) When returning the fresh canisterto the machine, always put it in the upper position.
10. Cork off the”Y” mount when machine is not in useto prevent loss of soda lime activity.
11. After a long duration anaesthetic, the machineshould be dried to remove the water vapour,particularly with large dogs. This is due to theabsorption of carbon dioxide within the soda limecanisters which produces both heat and moisture.
Care and Maintenance of the StephensEquipment
All parts of this machine in contact with soda lime oranaesthetic agents are constructed of materialsresistant to corrosion.
1. Metal fittings are connected by pushing themtogether while turning them 1/2 turn and should becleaned regularly by washing in warm, soapy waterand drying thoroughly. Do not wash flowmeter.
2. Petroleum jelly (Vasoline) should be used on alljoints and “O” rings.

16
STEPHENS FLOOR STAND & WALL MOUNT
Floor Stand (Code: S8760)
An optional floor stand is available for the StephensAnaesthetic Apparatus. The stand comes completewith castor wheels and will accommodate a ‘D’ sizeoxygen bottle.

17
Storage of Anaesthetic Agents
As the Stephens Vapouriser can be used with allcommon volatile anaesthetic agents, a vapouriser Jar
Sealing Cap is now available for the storage of theparticular anaesthetic agent in the jar. Make sure each
jar and cap is identified with the agent containedwithin. Care should be taken to ensure eachanaesthetic agent is kept according to themanufacturers prescribed storage conditions.
A large face mask (dog), Long Nose dog breeds and asmall face mask (small dog and cat) are now available
in see through unbreakable plastic for mask induction.Attaches directly to ‘‘Y’’piece.
Sealing cap being used to seal vapouriser jar.Fig.12
Four face masks are available for mask inductionsCat Small Dog Large Dog Long Nose
D1930 D1920 D1890 D1870
Fig.13
Face Masks (Low Dead Space – designed especially for the Stephens)
18
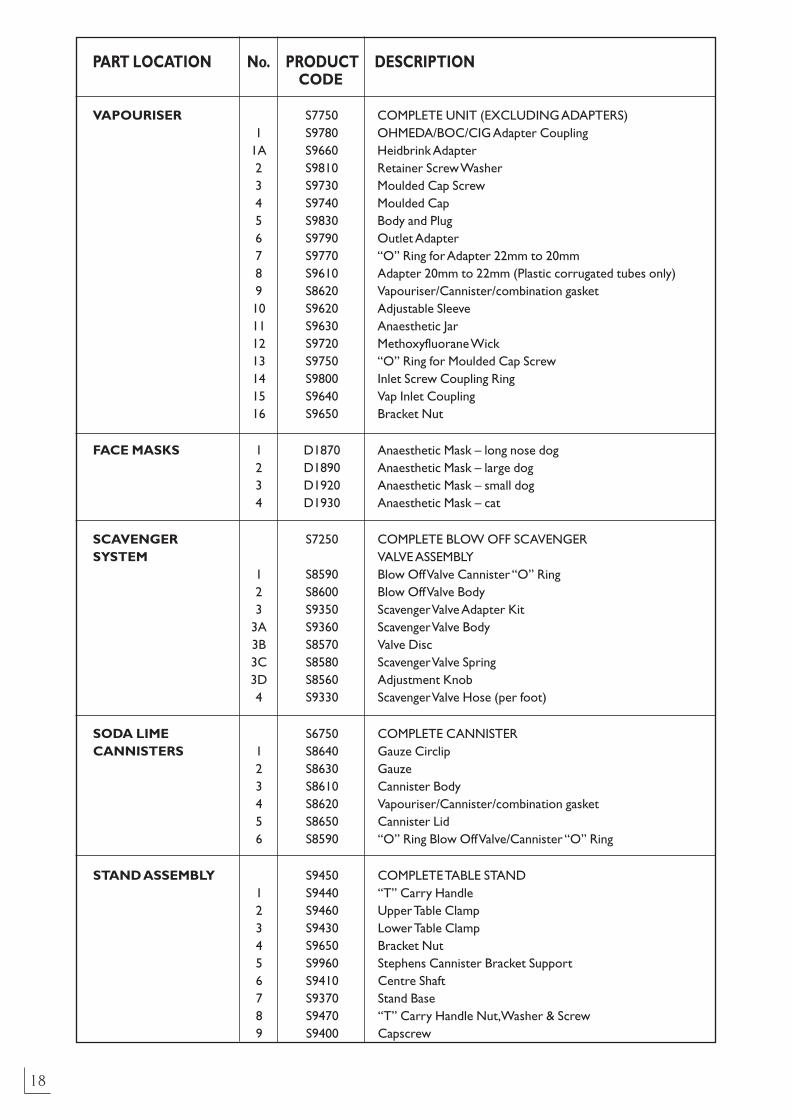
PART LOCATION No. PRODUCT DESCRIPTIONCODE
VAPOURISER S7750 COMPLETE UNIT (EXCLUDING ADAPTERS)1 S9780 OHMEDA/BOC/CIG Adapter Coupling
1A S9660 Heidbrink Adapter 2 S9810 Retainer Screw Washer 3 S9730 Moulded Cap Screw 4 S9740 Moulded Cap 5 S9830 Body and Plug 6 S9790 Outlet Adapter 7 S9770 “O” Ring for Adapter 22mm to 20mm 8 S9610 Adapter 20mm to 22mm (Plastic corrugated tubes only) 9 S8620 Vapouriser/Cannister/combination gasket 10 S9620 Adjustable Sleeve 11 S9630 Anaesthetic Jar 12 S9720 Methoxyfluorane Wick 13 S9750 “O” Ring for Moulded Cap Screw 14 S9800 Inlet Screw Coupling Ring 15 S9640 Vap Inlet Coupling16 S9650 Bracket Nut
FACE MASKS 1 D1870 Anaesthetic Mask – long nose dog 2 D1890 Anaesthetic Mask – large dog 3 D1920 Anaesthetic Mask – small dog4 D1930 Anaesthetic Mask – cat
SCAVENGER S7250 COMPLETE BLOW OFF SCAVENGER SYSTEM VALVE ASSEMBLY
1 S8590 Blow Off Valve Cannister “O” Ring 2 S8600 Blow Off Valve Body 3 S9350 Scavenger Valve Adapter Kit
3A S9360 Scavenger Valve Body 3B S8570 Valve Disc 3C S8580 Scavenger Valve Spring 3D S8560 Adjustment Knob 4 S9330 Scavenger Valve Hose (per foot)
SODA LIME S6750 COMPLETE CANNISTER CANNISTERS 1 S8640 Gauze Circlip
2 S8630 Gauze 3 S8610 Cannister Body 4 S8620 Vapouriser/Cannister/combination gasket 5 S8650 Cannister Lid 6 S8590 “O” Ring Blow Off Valve/Cannister “O” Ring
STAND ASSEMBLY S9450 COMPLETE TABLE STAND 1 S9440 “T” Carry Handle 2 S9460 Upper Table Clamp 3 S9430 Lower Table Clamp 4 S9650 Bracket Nut 5 S9960 Stephens Cannister Bracket Support 6 S9410 Centre Shaft 7 S9370 Stand Base 8 S9470 “T” Carry Handle Nut,Washer & Screw 9 S9400 Capscrew